 Hui Wang1
Hui Wang1 Xiao Liang
Xiao Liang Jiaxin Xu
Jiaxin Xu Dalong Yang
Dalong Yang Weishi Li
Weishi Li Wenyuan Ding
Wenyuan Ding
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 13 February 2023
Sec. Orthopedic Surgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1116590
This article is part of the Research Topic Advances in Research of Degenerative Orthopedic Conditions: from Basic to Clinical Research View all 32 articles
Objective: To assess the intra- and interobserver reliability by observer training level used for selecting the end vertebra (EV), neutral vertebra (NV), stable vertebra (SV), and first coronal reverse vertebrae (FCRV) in degenerative lumbar scoliosis (DLS) patients.
Methods: Fifty consecutive upright long-cassette radiographs and CT examination of operative cases of DLS were evaluated by three surgeons at various levels of training. For each iteration, the observers attempted to identify the UEV, NV and SV from x-ray, and FCRV from the CT examination. Intra- and interobserver reliability was assessed by means of Cohen's Kappa correlation coefficient, and raw percentages of agreement were recorded.
Results: Intraobserver reliability was excellent for determining FCRV (Ka = 0.761–0.837), fair to good for determining UEV (Ka = 0.530–0.636), fair to good for determining SV (Ka = 0.519–0.644), and fair to good for determining NV (Ka = 0.504–0.734), respectively. Additionally, we also noted a trend towards better intraobserver reliability with increasing levels of experience. Interobserver reliability was poor between observers beyond chance for UEV, NV, SV (Ka = 0.105–0.358), and good reliability for FCRV (Ka = 0.581–0.624). All three observers agreed on the same level of the FCRV in 24 patients of the time, which presented less Coronal imbalance type C compared to the other 26 patients.
Conclusion: Experience and training level of the observers are important factors affecting the accurate identification of these vertebrae in DLS, intraobserver reliability increases along with increasing levels of observer experience. FCRV is superior to UEV, NV, and SV in the accuracy of identification, Type C coronal malalignment could affect the accurate identification of FCRV.
Selection of upper instrumented vertebrae (UIV) has been proved to be closely related to the postoperative proximal adjacent segment degeneration and proximal scoliosis progression followed posterior lumbar fusion for degenerative lumbar scoliosis (DLS), which are common radiological findings but may progressed to adjacent segment disease that required revision surgery (1–4). Bridwell et al. (5) stated that choosing proximal fusion level requires identification of the stable vertebra (SV), neutral vertebra (NV), upper end vertebrae (UEV) from the x-ray examination. This process is a prerequisite for achieving both maximal curve correction and a stable, well-balanced spine while fusing as few motion segments as possible (6). For determination of the optimal proximal fusion level, Wang et al. defined a new concept named first coronal reverse vertebrae (FCRV) based on Hounsfield unit (HU) measurement from computed tomography (CT) examination, which is the first vertebrae that presents opposite orientation of asymmetric HU ratio from the other vertebrae within the major curve (7, 8). Proximal fusion level above FCRV could decrease the risk of postoperative proximal scoliosis progression in DLS when compared to the SV.
FCRV represents the transitional point of the mechanical load and may be within a more stable condition than SV measured from radiographs, the reliability and accuracy of vertebra HU measurement are not affected by the posture, it is reasonable to believe that FCRV is more reliable and objective than SV in the preoperative evaluation of UIV for DLS patients (7, 8). However, no previous study has attempted to assess the reliability and reproducibility in determining the FCRV, SV, NV, UEV in DLS patients, little study specifically focus on the superiority of FCRV in the identification and interpretation. The purpose of the present investigation was to assess the intra- and interobserver reliability of selecting the SV, NV, UEV, and FCRV among three surgeons with varying levels of training based on standing posterior anterior preoperative x-ray examination and CT examination.
This retrospective study was approved by the Institutional Review Board of the Third Hospital of HeBei Medical University (H2022206056). Before data collection and analysis, each patient provided informed consent.
Inclusion criteria: (1) DLS patients with age older than 50 years. (2) Full-spine Postero-Anterior (P/A) x-ray. (3) Lumbar CT was available for HU measurement. Exclusion criteria: (1) Previous surgery for degenerative lumbar disease. (2) Spinal infections or metabolic disease that may potentially affect accuracy of HU measurements. (3) The anatomical identification was difficult to recognize for radiological measurement.
Fifty consecutive upright long-cassette radiographs and CT examination of operative cases of DLS were evaluated on the same occasion by three surgeons at various levels of training [fellowship-trained spine surgeon (observer 1; JX), fellow in-training (observer 2; JS), orthopaedic surgery resident (observer 3; XL)]. The radiograph order was scrambled between each measurement iteration by each observer. For each iteration, the observers attempted to identify the upper end vertebrae (UEV), neutral vertebrae (NV) and stable vertebrae (SV) from x-ray, and first coronal reverse vertebrae (FCRV) from the CT examination.
The UEV is defined as the most tilted vertebrae (that which subtended the greatest Cobb angle) at the cephalad end of the main curve. The NV is defined as the most cephalad vertebrae with apparently neutral rotation as assessed by pedicle symmetry within the radiographic silhouette of the corresponding vertebrae. The SV is the most cephalad vertebra closest to the end vertebra of the main curve that is most nearly bisected by the central sacral vertical line (CSVL) (Figure 1). When two adjacent levels were felt to equally satisfy the above criteria (e.g., the CSVL perfectly bisected the disc between, but not the bodies of, two adjacent vertebrae), the observers were instructed to select the more proximal level. The FCRV is defined as the first vertebrae that presents opposite orientation of asymmetric Hounsfield unit (HU) ratio from the other vertebrae within major curve (Figure 2).
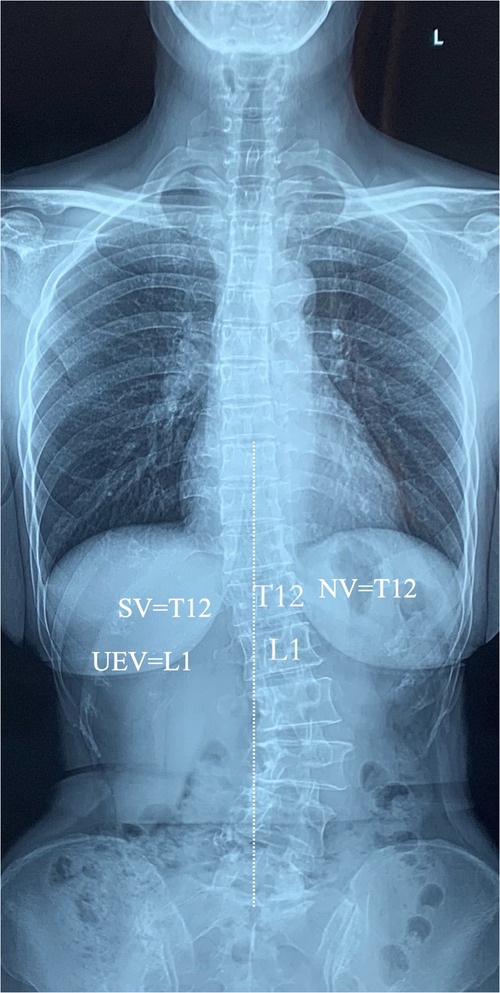
Figure 1. Schematic demonstrating the upper end vertebra, neutral vertebra (not rotated; pedicles and body symmetric, spinous process midline), and stable vertebra (CSVL bisects pedicles).
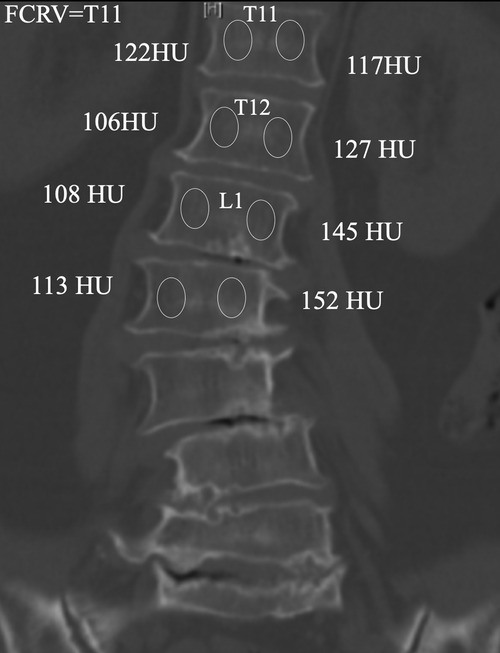
Figure 2. Schematic diagram of FCRV measurement, which is defined as the first vertebrae that presents opposite orientation of asymmetric hounsfield unit (HU) ratio from the other vertebrae within major curve.
All the patients were divided into two groups according to the agreement for FCRV. Age, gender, and bone mineral density (BMD) were recorded. Cobb's angle is measured between the most tilted vertebrae. Coronal balance distance (CBD) is the distance between C7 plumb line and CSVL. Coronal malalignment are classified based on the CBD: Type A, CBD < 3 cm; Type B, CBD > 3 cm and C7PL shifted to the concave side of the curve; Type C, CBD > 3 cm and C7PL shifted to the convex side (Figure 3). All radiographic parameters were measured by two independent observers (first and second author), and were averaged to give a mean value for statistical analysis.
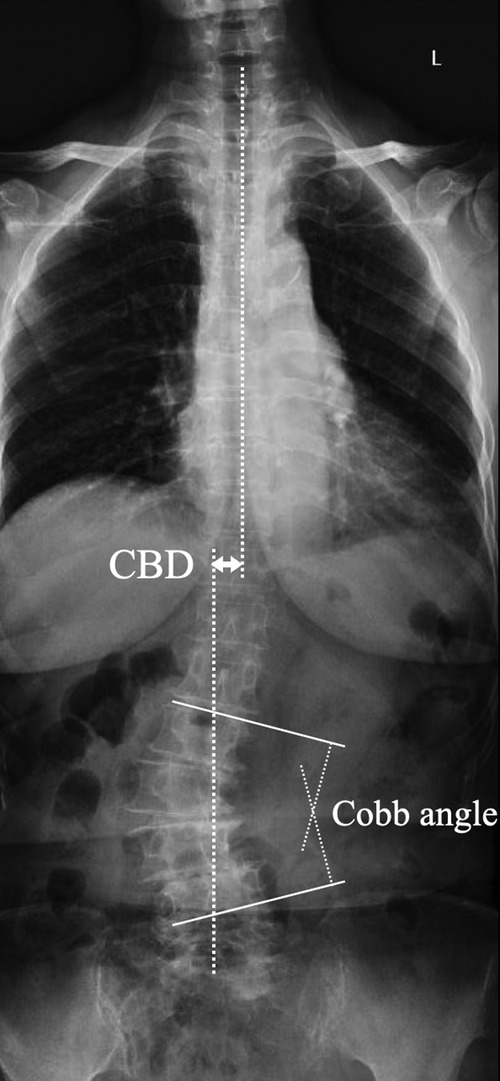
Figure 3. Schematic diagram of coronal spinal parameters measurement. Cobb's angle was measured between the most tilted vertebrae. CBD was the distance between C7 plumb line and CSVL.
Data were analyzed using Statistical Product and Service Solutions software (version 17; SPSS, Chicago, IL). Three-way Cohen's Kappa correlation coefficients were calculated to assess the intra- and interobserver reliability for determining the UEV, NV, SV and FCRV, respectively. We also adopted Ka value of 0.75 and above to represent excellent agreement, 0.55–0.74 good agreement, 0.40–0.54 fair agreement, and 0.39 and below poor agreement beyond chance. Continuous variables were recorded as mean ± standard deviation, and categorical variables were expressed as frequency or percentages. An independent t test was used to analyze the difference of continuous variables. An χ2 analysis and Fisher's exact test were used to examine the differences among categorical variables. The statistical significance was set at p < 0.05.
Among the 50 patients included in the current study, 12 males and 38 females, with mean age of 61.7 ± 8.3 years. Coronal imbalance type A was detected in 31 patients, type B was detected in 9 patients, type C was detected in 10 patients. 27 patients presented apex orientation toward left and 23 patients presented apex orientation toward right. The mean Cobb angle was 23.6 ± 5.6 degrees.
The Ka values were excellent for determining the FCRV (Ka = 0.761–0.837), fair to good for determining the UEV (Ka = 0.530–0.636), fair to good for determining the SV (Ka = 0.519–0.644), and fair to good for determining the NV (Ka = 0.504–0.734). Additionally, we also noted a trend towards better intraobserver reliability with increasing levels of experience; observer 1 demonstrated average Ka value of 0.713 versus 0.671 for observer 2, and 0.579 for observer 3 (Table 1).

Table 1. Intraobserver reliability of SV, NV, UEV, FCRV identification among three surgeons.
For the first measurement by each observer, the Ka values demonstrated poor reliability for agreement between observers beyond chance for UEV, NV, SV (Ka = 0.105–0.358), and good reliability for FCRV (Ka = 0.581–0.624). All three observers agreed on the exact level of the UEV 14% of the time, the NV 8% of the time, the SV 12% of the time, and the FCRV 48% of the time. Conversely, all three observers disagreed (each selected a different vertebral level) for 6% of EV, 12% of NV, 10% of SV, and 2% of FCRV.
For the first measurement by each observer, all three observers agreed on the same level of the FCRV in 24 patients of the time, they were enrolled as the High agreement group, the other 26 patients were enrolled as the Low agreement group. There were significant difference in the Coronal imbalance type between the two groups, Coronal imbalance type C was more common in Low agreement group when compared to the High agreement group (Table 2).

Table 2. Comparison of clinical and radiological data between high and low agreement groups.
The experience and training level of the three observers appeared to be an important factor affecting the identification of the end, neutral, stable vertebra, and FCRV, with a trend towards improved reliability of vertebral level assessment with increased experience, which is partly consistent with the finding by Benjamin et al. (9). The inherent difficulties in radiographic landmark identification and human error attributable to the “level ambiguity” that occurs when two (or even three) vertebrae nearly, could result in the discrepancies in the observer-selected levels (9). The UEV is defined as the most tilted vertebrae at the cephalad end of the main curve, human error attributable to the “level ambiguity” that occurs when two vertebrae nearly, but imperfectly, meet the criteria for the UEV could not be completely avoided (10). The NV is defined as the most cephalad vertebrae with apparently neutral rotation as assessed by pedicle symmetry within the radiographic silhouette of the corresponding vertebrae, human error in the “vertebrae rotation identification” is unavoidable when adjacent vertebrae are extremely close in rotation (9). The SV is the most cephalad vertebra caudal to the end vertebra of the main curve that is most nearly bisected by the CSVL, but there maybe a certain error in drawing the line erected vertically from the midpoint of S1, especially when the sacral anatomy is illegible (11). The FCRV is defined as the first vertebrae that presents opposite orientation of asymmetric HU ratio from the other vertebrae within major curve. For each measurement, the largest possible elliptical region of interest was drawn, but excluding the cortical margins to prevent volume averaging is a technically demanding manipulation, which may result in certain impact on measurement results. The accurate identification of radiographic landmark for the above vertebra is the embodiment of experience.
This is the first study to assess and compare the reproducibility and reliability of UEV, NV, SV, and FCRV interpretation in DLS patients, the intraobserver reliability was excellent for determining the FCRV, fair to good for determining the UEV, NV, and SV. FCRV is superior to UEV, NV, and SV in the accuracy of interpretation, two possible reasons may account for the difference. Firstly, in the identification of FCRV from CT examination, the measurement was performed within the concave and convex sides separately at three different regions of the vertebrae on coronal plane: immediately posterior to the anterior vertebrae margin, in the middle of the vertebral body, and anterior to the posterior vertebrae margin (7). Although excluding the cortical margins to prevent volume averaging is a technically demanding manipulation, it seems that the repeated measurement from different regions of the vertebrae could minimize measurement error when compared to UEV, NV, SV, which were measured only once from x-ray, while human errors attributable to the “level ambiguity”, “vertebrae rotation identification” should not be underestimated. Secondly, from a methodological point of view, the largest possible elliptical region of interest was drawn in the determination of FCRV, which is simple and rarely interfered by other factors (11–14). Contrarily, vertebrae rotation, osteoporosis, aortic calcification, and osteophyte hyperplasia, which may increase measurement difficulty and error in radiographic landmark identification, and would affect the accuracy of identification of UEV, NV, SV (15–17).
Benjamin et al. (9) demonstrated good to excellent intraobserver reliability in the radiographic determination of the EV, NV, and SV in adolescent idiopathic scoliosis (AIS) patients, which present more satisfactory results than the findings in the current study. The characteristics of the two different scoliosis render that there are bound to be differences in the identification of the vertebrae mentioned above. DLS is typically diagnosed in patients older than 40 years and without a history of AIS, the curves typically have an L2–3 apex and are associated with lateral olisthesis, rotatory subluxation, and structural vertebral deformity, which inevitably increase the difficulty in the identification of the EV, NV, and SV (18–20). Osteoporosis is also an important feature of DLS that distinguishing from AIS, and may obscure the radiographic landmark identification of the upper endplate and the pedicles of the vertebrae, finally lead to the variability in the identification of UEV, NV, SV that measured on x-ray (21, 22).
FCRV provides a meaningful reference in the selection of UIV for DLS patients, UIV above FCRV is superior to SV in reducing the incidence of proximal adjacent segment degeneration for DLS patients that received posterior fusion surgery (7, 8). The strength of the current study is that we firstly demonstrate FCRV is superior to UEV, NV, and SV in the accuracy of interpretation. Moreover, type C coronal malalignment, defined as CBD > 3 cm and a C7PL shifted to the convex side of the curve, is detected to be an important factor affecting the accuracy of FCRV identification. The alignment of the vertebrae proximal to the apex present smooth or flat in patients with Coronal imbalance type C, the difference of HU values between the convex and concave sides of these vertebrae is little, which may inevitably lead to a certain error in the identification of FCRV.
There are several limitations in the current study. First, the number of enrolled patients is relatively small, and from a single center, the number of Coronal malalignment type B and type C is relatively smaller when compared to type A, more DLS cases need to be included to verify this conclusion in the next study. Second, the subjects selected are all Chinese Han individuals, whether the conclusion is applicable to other ethnic groups needs to be further investigated in the future.
Experience and training level of the observers are important factors affecting the accurate identification of these vertebrae in DLS, intraobserver reliability increases along with increasing levels of observer experience. FCRV is superior to UEV, NV, and SV in the accuracy of identification, Type C coronal malalignment could affect the accurate identification of FCRV.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
HW: manuscript draft. XL: data collection. JX, JS: data analysis. WL and WD: manuscript design. All authors contributed to the article and approved the submitted version.
This work was supported by the Natural Science Foundation of Hebei Province (H2022206056).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Alentado VJ, Lubelski D, Healy AT, Orr RD, Steinmetz MP, Benzel EC, et al. Predisposing characteristics of adjacent segment disease after lumbar fusion. Spine. (2016) 41(14):1167–72. doi: 10.1097/BRS.0000000000001493
2. Wang H, Ma L, Yang D, Wang T, Yang S, Wang Y, et al. Incidence and risk factors for the progression of proximal junctional kyphosis in degenerative lumbar scoliosis following long instrumented posterior spinal fusion. Medicine. (2016) 95(32):e4443. doi: 10.1097/MD.0000000000004443
3. Lee N, Yi S, Shin DA, Kim KN, Yoon do H, Ha Y. Progression of coronal Cobb angle after short-segment lumbar interbody fusion in patients with degenerative lumbar stenosis. World Neurosurg. (2016) 89:510–6. doi: 10.1016/j.wneu.2016.01.051
4. Phan K, Xu J, Maharaj MM, Li J, Kim JS, Di Capua J, et al. Outcomes of short fusion versus long fusion for adult degenerative scoliosis: a systematic review and meta-analysis. Orthop Surg. (2017) 9(4):342–9. doi: 10.1111/os.12357
5. Bridwell KH. Selection of instrumentation and fusion levels for scoliosis: where to start and where to stop. Invited submission from the joint section meeting on disorders of the spine and peripheral nerves, march 2004. J Neurosurg Spine. (2004) 1(1):1–8. doi: 10.3171/spi.2004.1.1.0001
6. Zhang Z, Liu T, Wang Y, Wang Z, Zheng G. Factors related to preoperative coronal malalignment in degenerative lumbar scoliosis: an analysis on coronal parameters. Orthop Surg. (2022) 14(8):1846–52. doi: 10.1111/os.13379
7. Wang H, Zou D, Sun Z, Wang L, Ding W, Li W. Hounsfield unit for assessing vertebral bone quality and asymmetrical vertebral degeneration in degenerative lumbar scoliosis. Spine. (2020) 45(22):1559–66. doi: 10.1097/BRS.0000000000003639
8. Wang H, Sun Z, Wang L, Zou D, Li W. Proximal fusion level above first coronal reverse vertebrae: an essential factor decreasing the risk of adjacent segment degeneration in degenerative lumbar scoliosis. Global Spine J. (2023) 13(1):149–55. doi: 10.1177/2192568221994082
9. Potter BK, Rosner MK, Lehman RA Jr, Polly DW Jr, Schroeder TM, Kuklo TR. Reliability of end, neutral, and stable vertebrae identification in adolescent idiopathic scoliosis. Spine. (2005) 30(14):1658–63. doi: 10.1097/01.brs.0000170290.05381.9a
10. Guo J, Deng XC, Ling QJ, Yin ZX, He EX. Reliability analysis of cobb measurement in degenerative lumbar scoliosis using endplate versus pedicle as bony landmarks. Postgrad Med. (2017) 129(7):762–7. doi: 10.1080/00325481.2017.1343645
11. Zhu Y, Wang K, Wang B, Wang H, Jin Z, Zhu Z, et al. Selection of proximal fusion level for degenerative scoliosis and the entailing proximal-related late complications. Int J Clin Exp Med. (2015) 8(4):5731–8.26131158
12. Schreiber JJ, Hughes AP, Taher F, Girardi FP. An association can be found between hounsfield units and success of lumbar spine fusion. HSS J. (2014) 10(1):25–9. doi: 10.1007/s11420-013-9367-3
13. Lee S, Chung CK, Oh SH, Park SB. Correlation between bone mineral density measured by dual-energy x-ray absorptiometry and hounsfield units measured by diagnostic CT in lumbar spine. J Korean Neurosurg Soc. (2013) 54(5):384–9. doi: 10.3340/jkns.2013.54.5.384
14. Silva IM, Freitas DQ, Ambrosano GM, Bóscolo FN, Almeida SM. Bone density: comparative evaluation of hounsfield units in multislice and cone-beam computed tomography. Braz Oral Res. (2012) 26(6):550–6. doi: 10.1590/S1806-83242012000600011
15. Tribus CB. Degenerative lumbar scoliosis: evaluation and management. J Am Acad Orthop Surg. (2003) 11(3):174–83. doi: 10.5435/00124635-200305000-00004
16. Xu L, Sun X, Huang S, Zhu Z, Qiao J, Zhu F, et al. Degenerative lumbar scoliosis in Chinese han population: prevalence and relationship to age, gender, bone mineral density, and body mass index. Eur Spine J. (2013) 22(6):1326–31. doi: 10.1007/s00586-013-2678-8
17. Faraj SS, Holewijn RM, van Hooff ML, de Kleuver M, Pellisé F, Haanstra TM. De novo degenerative lumbar scoliosis: a systematic review of prognostic factors for curve progression. Eur Spine J. (2016) 25(8):2347–58. doi: 10.1007/s00586-016-4619-9
18. Akbik OS, Ban VS, MacAllister MC, Aoun SG, Bagley CA. Genetic and serum markers in adult degenerative scoliosis: a literature review. Spine Deform. (2022) 10(3):479–88. doi: 10.1007/s43390-021-00451-y
19. Wollschläger LM, Nebelung S, Schleich C, Müller-Lutz A, Radke KL, Frenken M, et al. Evaluating lumbar intervertebral disc degeneration on a compositional level using chemical exchange saturation transfer: preliminary results in patients with adolescent idiopathic scoliosis. Diagnostics. (2021) 11(6):934. doi: 10.3390/diagnostics11060934
20. Dehnokhalaji M, Golbakhsh MR, Siavashi B, Talebian P, Javidmehr S, Bozorgmanesh M. Evaluation of the degenerative changes of the distal intervertebral discs after internal fixation surgery in adolescent idiopathic scoliosis. Asian Spine J. (2018) 12(6):1060–8. doi: 10.31616/asj.2018.12.6.1060
21. Pickhardt PJ, Pooler BD, Lauder T, del Rio AM, Bruce RJ, Binkley N. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications. Ann Intern Med. (2013) 158(8):588–95. doi: 10.7326/0003-4819-158-8-201304160-00003
22. Lee SJ, Binkley N, Lubner MG, Bruce RJ, Ziemlewicz TJ, Pickhardt PJ. Opportunistic screening for osteoporosis using the sagittal reconstruction from routine abdominal CT for combined assessment of vertebral fractures and density. Osteoporos Int. (2016) 27(3):1131–6. doi: 10.1007/s00198-015-3318-4
Keywords: degenerative lumbar scoliosis, first coronal reverse vertebrae, intraobserver reliability, coronal malalignment, observer training level
Citation: Wang H, Liang X, Xu J, Sun J, Yang D, Li W and Ding W (2023) Reliability of end, stable, neutral, first coronal reverse vertebrae identification in degenerative lumbar scoliosis: Intra- and interobserver consistency analysis. Front. Surg. 10:1116590. doi: 10.3389/fsurg.2023.1116590
Received: 5 December 2022; Accepted: 17 January 2023;
Published: 13 February 2023.
Edited by:
Fang Fang Yu, Zhengzhou University, ChinaReviewed by:
Keyi Yu, Peking Union Medical College Hospital (CAMS), China© 2023 Wang, Liang, Xu, Sun, Yang, Li and Ding. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenyuan Ding ZGluZ3d5bWFudXNjcmlwdEAxNjMuY29t Weishi Li d2Vpc2hpbGkyMDE5QDEyNi5jb20=
Specialty Section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.