
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 30 January 2023
Sec. Thoracic Surgery
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1102352
 Yu Han1,2
Yu Han1,2 Qiduo Yu1,2
Qiduo Yu1,2 Qianli Ma1,2
Qianli Ma1,2 Jin Zhang1,2Yuhui Shi1,2Zhenrong Zhang1,2
Jin Zhang1,2Yuhui Shi1,2Zhenrong Zhang1,2 Guangliang Qiang1,2Fei Xiao1,2*Chaoyang Liang1,2*
Guangliang Qiang1,2Fei Xiao1,2*Chaoyang Liang1,2*
Objective: A large number of patients with pulmonary ground-glass opacities (GGOs) have anxiety and depression. However, the contributing factors and effects of anxiety and depression on postoperative outcomes are still unclear.
Methods: Clinical data for patients undergoing surgical resection for pulmonary GGOs were collected. We prospectively evaluated levels and risk factors for anxiety and depression in patients with GGOs before surgery. The relationship between psychological disorders and postoperative morbidity was evaluated. Quality of life (QoL) was also assessed.
Results: A total of 133 patients were enrolled. Prevalence rates of preoperative anxiety and depression were 26.3% (n = 35) and 18% (n = 24), respectively. Multivariate analysis revealed depression [odds ratio(OR) = 16.27, p < 0.001] and multiple GGOs (OR = 3.146, p = 0.033) to be risk factors for preoperative anxiety. Anxiety (OR = 52.166, p < 0.001), age > 60 (OR = 3.601, p = 0.036), and unemployment (OR = 8.248, p = 0.006) were identified as risk factors for preoperative depression. Preoperative anxiety and depression were associated with lower QoL and higher postoperative pain scores. Our results also revealed that the incidence of postoperative atrial fibrillation was higher in patients with than in those without anxiety.
Conclusions: In patients with pulmonary GGOs, comprehensive psychological assessment and appropriate management are required before surgery to improve QoL and reduce postoperative morbidity.
Over the past decades, low-dose computed tomography (LDCT) has been widely applied in lung cancer screening for high-risk patients (1). As a result, an increasing number of pulmonary ground glass opacities (GGOs) have been identified (2, 3). It has been proven that pulmonary nodules manifest as GGOs that enlarge slowly and are associated with excellent survival after resection (4, 5). However, due to the fear of being diagnosed with lung cancer and undergoing surgery, a large number of patients have psychological disorders, most commonly anxiety and depression (6, 7).
Previous studies have shown that 20.9-65.0% of patients with lung cancer have anxiety symptoms, and the incidence of depression ranges from 38.9%–65% (8–11). The prevalence of anxiety and depression in lung cancer patients is influenced by a variety of factors, including age, sex, social support, comorbidities, tumor stage and other factors (12–14). Until now, however, the psychological status and risk factors for anxiety and depression in patients with pulmonary GGOs who have not been diagnosed with lung cancer have remained unclear.
It has been revealed that anxiety and depression are associated with lower QoL in patients with lung cancer (15, 16). Preoperative anxiety has also been proven to be related to higher morbidity and mortality after cardiovascular surgery (17). Furthermore, depressive emotion has even been associated with worse survival in patients with lung cancer (18). Nevertheless, the association of preoperative anxiety and depression with postoperative outcomes of pulmonary resection is still unclear.
In this article, we describe psychological assessments of patients with pulmonary GGOs before surgery, the QoL of those patients, and the occurrence of postoperative outcomes. We aimed to investigate the prevalence of and contributing factors for preoperative psychological disorders in patients with pulmonary GGOs and whether anxiety and depression have adverse effects on QoL and postoperative outcomes in these patients.
From October 2020 to August 2022, 133 patients who underwent thoracoscopic pulmonary resection in China-Japan Friendship Hospital for pulmonary GGOs were included in this study (Figure 1). The patients selected for this research met the following criteria: (1) pulmonary GGOs suspected to be malignant with indications for minimally invasive surgery; (2) clinical stages judged to be cT1N0M0 according to the 8th edition of the AJCC TNM staging system; and (3) not undergoing pathological biopsy before surgery. The exclusion criteria were as follows: (1) a history of mental or psychological diseases; (2) a history of lung cancer or other malignant tumors; and (3) refusal to participate in the study. Patient-controlled intravenous analgesia (PCIA) combined with intercostal nerve block was used for postoperative analgesia. Written informed consent was obtained from all patients before surgery. This study was approved by our institutional review board (2022-KY-127).
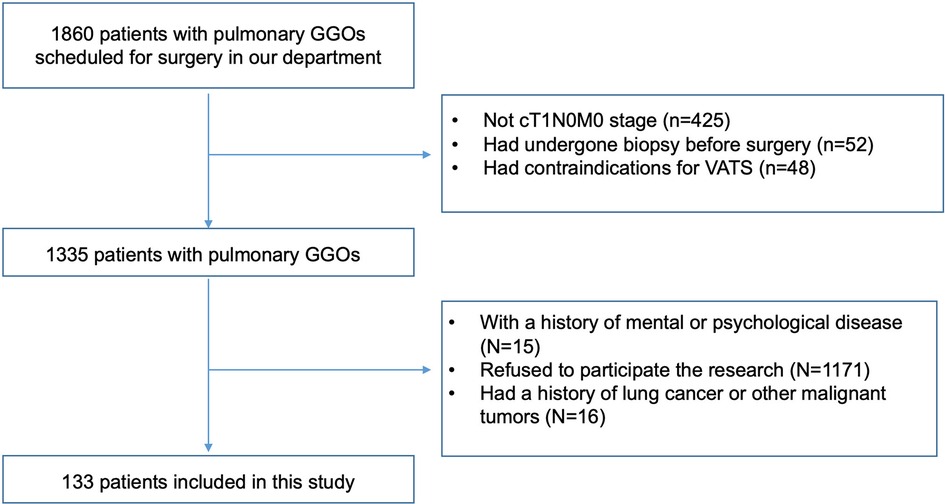
Figure 1. Flow chart of the study.
All patients received psychological evaluations with the Hospital Anxiety Depression Scale (HADS) questionnaire during hospitalization before surgery. The HADS is a widely utilized self-report questionnaire designed to screen for anxiety and depression states in patients (19). The questionnaire consists of the HADS-A and HADS-D, which are designed to detect anxious and depressive states, respectively. Each subscale contains seven items, and each question is scored from 0 to 3 points. Higher scores represent higher levels of anxious or depressive states, and the total scores can range from 0 to 21 in each subgroup. HADS scores ≥8 were defined as anxiety or depression in this study (20).
QoL was assessed with the EORTC QLQ-C30 questionnaire (21), which is the most widely utilized cancer-specific Health-Related Quality-of-Life instrument. The EORTC QLQ-C30 consists of five functional dimensions on physical, role, emotional, cognitive and social functioning, three symptom items (pain, nausea/vomiting, fatigue), six single items including dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial impact, and a global health scale. The scoring procedures were performed as previously described (22).
Statistical analysis was performed using SPSS (version 23, IBM Inc., Chicago, IL, USA). Categorical variables were compared using the chi-square test or Fisher's exact test. Student's t test or the Wilcoxon rank-sum test was used to analyze continuous variables. A p value less than 0.05 was considered statistically significant. A binary logistic regression test was performed to detect risk factors for anxiety and depression status. Variables with a p value less than 0.15 in univariate analysis were then included in multivariate analysis. A p value less than 0.05 was regarded as statistically significant for both univariate and multivariate analyses.
The basic patient characteristics are shown in Table 1. A total of 133 patients with pulmonary GGOs met the inclusion criteria. The case series consisted of 41 (30.8%) men and 92 (69.2%) women, with an average age of 51.5 ± 11.7 years. Sixty-four patients (48.1%) had low levels of education (middle school and below). One hundred and five patients (78.9%) were married, and 70 patients (52.6%) were employed. Twenty-seven patients (20.3%) had a history of alcohol consumption, and 14 patients (10.5%) were smokers. Hypertension was the most common comorbidity (21.1%) in this case series; other common comorbidities included diabetes mellitus (9.0%), pulmonary diseases (6.0%), and cardiac diseases (5.3%). Most of the nodules were malignant (87.2%), and 98.5% were stage I. Overall postoperative morbidity was 15.8%, and no patient died within 30 days postoperatively. The median postoperative length of hospitalization (LOH) was 4 days (IQR: 3–4 days).
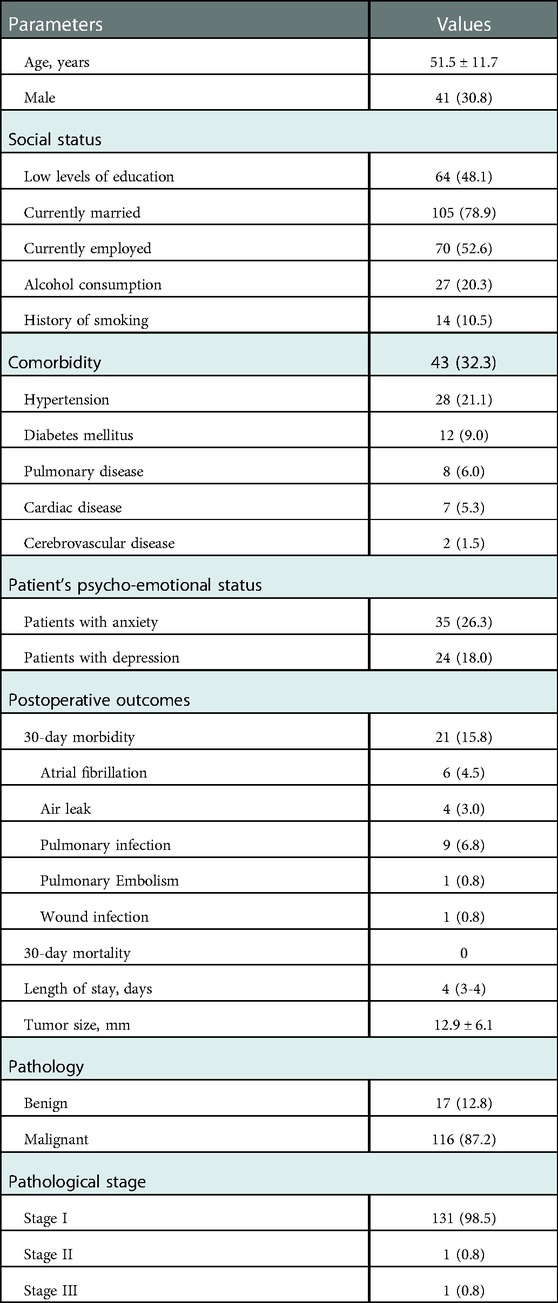
Table 1. Basic patient characteristics and perioperative outcomes.
Based on HADS scores, 41 patients (30.8%) had anxiety or depression. Thirty-five patients (26.3%) had anxiety, and 24 patients (18.0%) had depression before surgery. Moreover, 18 patients (13.5%) were identified as having from both anxiety and depression. All patients with HADS scores ≥8 were recommended to receive psychiatric counselling before surgery. However, only 12 patients (29.3%) agreed to visit the mental health clinic. Among those patients, 6 (50.0%) were diagnosed with adjustment disorder, 4 (33.3%) with anxiety disorder and 2 (16.7%) with depression disorder, and supportive psychotherapy or psychiatric medication was provided.
We further analyzed risk factors for preoperative anxiety and depression (Table 2). Patients with multiple GGOs were more likely to have anxiety than those with a single lesion (p = 0.010). Moreover, preoperative depression was another risk factor associated with anxiety (p < 0.001). Conversely, no significant differences between the two groups were observed in terms of sex, age, education level, marital status, employment status, history of chronic disease, or GGO image size (p > 0.05). After univariable analysis, sex, number of lesions, and preoperative depression were qualified for multivariable analysis. Based on multivariable analysis, preoperative depression (p < 0.001) and the number of lesions (p = 0.033) were identified as risk factors for preoperative anxiety (Table 3).
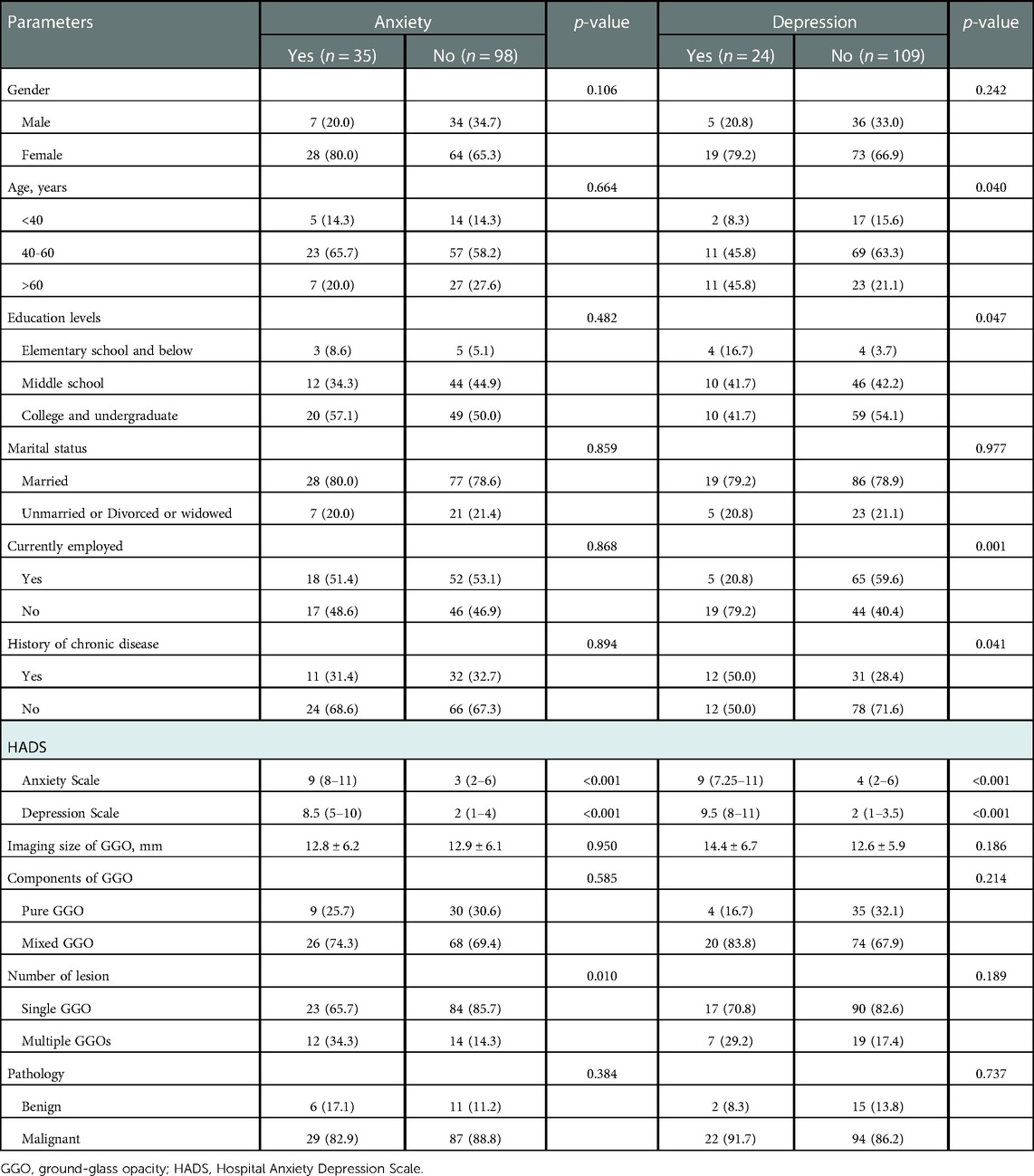
Table 2. Analysis of risk factors of anxiety and depression for patients with pulmonary GGO.
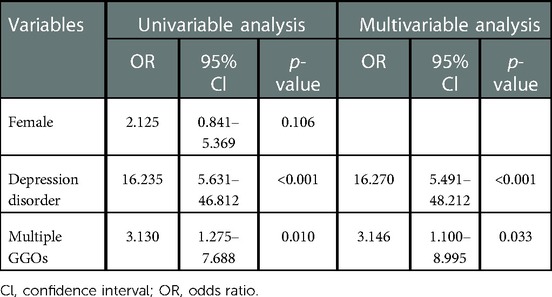
Table 3. Univariable and multivariable risk factor analyses for anxiety.
In univariate analysis, the variables related to preoperative depression were anxiety disorder (p < 0.001), age > 60 (p = 0.008), low education level (p = 0.068), current unemployment (p = 0.001), and history of chronic diseases (p = 0.041). Furthermore, anxiety disorder (p < 0.001), age > 60 (p = 0.036), and current unemployment (p = 0.006) were significantly associated with preoperative depression in multivariate analysis (Table 4).
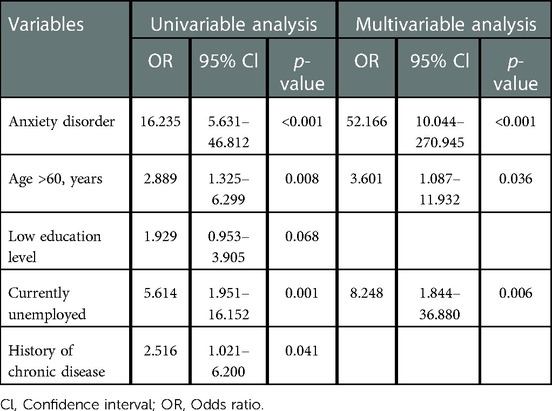
Table 4. Univariable and multivariable risk factor analyses for depression.
Compared with those without anxiety or depression, patients with anxiety and depression had lower scores on all aspects of QoL (physical, role, emotional, cognitive, and social functioning) and global health. There were significant differences between the anxiety and nonanxiety groups regarding insomnia (p = 0.015) and appetite loss (p = 0.012). Additionally, patients with preoperative depression had lower scores of QoL in terms of fatigue (p = 0.021), pain (p = 0.033), insomnia (p = 0.039) and appetite loss (p = 0.006). Detailed score reports of the EORTC QLQ-30 are shown in Table 5.
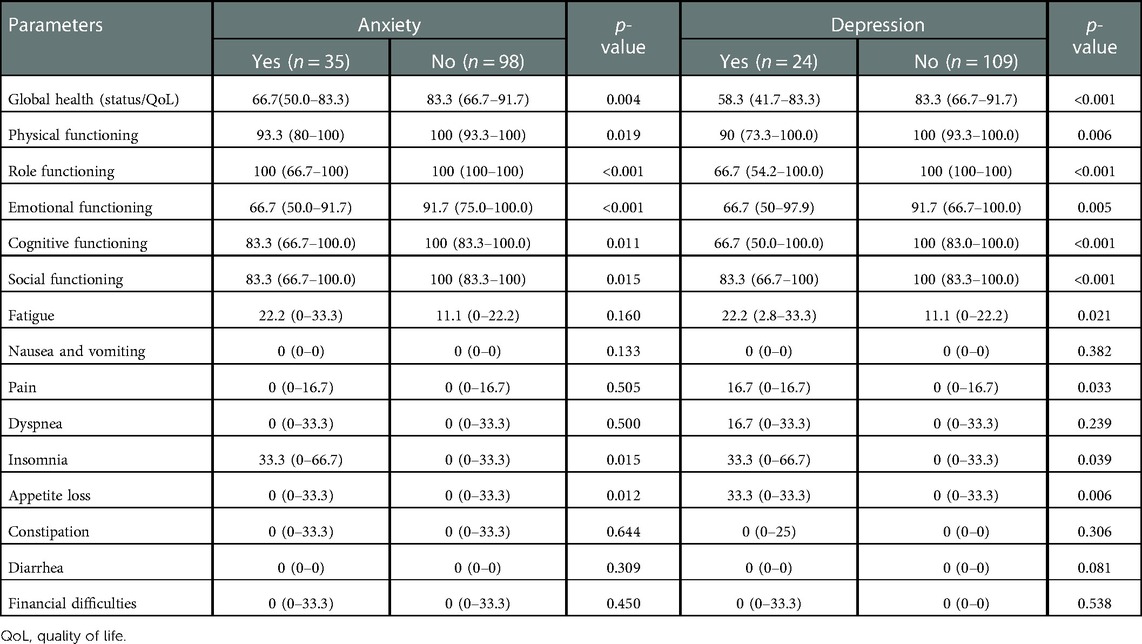
Table 5. Quality of life of the patients with pulmonary GGO before surgery.
The surgical approaches were comparable among the different groups (Table 6). We further investigated the association of preoperative anxiety and depression with postoperative outcomes among different subgroups (Table 6). Pain scores were significantly higher in the anxiety group at postoperative Day 1 (5 [interquartile range (IQR), 4–6] vs. 4 [IQR, 3–5], p < 0.001), POD 2 (3 [IQR, 3–4] vs. 2 [IQR, 2–3], p < 0.001), and POD 3 (2 [IQR, 1–2] vs. 1.5 [IQR, 1–2], p = 0.012). The incidence of atrial fibrillation was also higher in patients with preoperative anxiety than in those without anxiety (11.4% vs. 2.0%, p = 0.041). However, other postoperative outcomes were comparable between the two groups, as were chest tube duration (p = 0.412) and length of stay (p = 1.000).
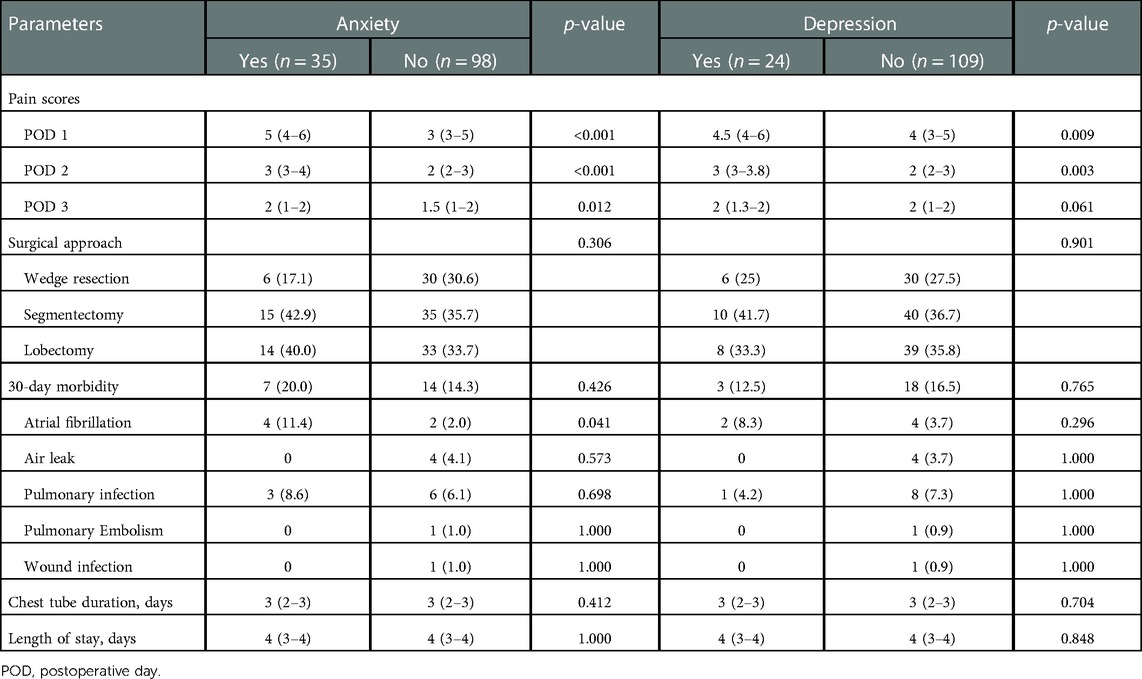
Table 6. Effects of anxiety and depression on postoperative outcomes.
Postoperative pain at POD 1 (4.5 [IQR, 4–6] vs. 4 [IQR, 3–5], p = 0.009) and POD 2 (3 [IQR, 3–3.8] vs. 2 [IQR, 2–3], p = 0.003) was also significantly higher in patients with than in those without depression. However, no significant differences were observed between the depression and non-depression groups regarding other postoperative outcomes, including chest tube duration (p = 0.704) and length of stay (p = 0.848).
With the wide implementation of lung cancer screening, an increasing number of early-stage NSCLC cases have been identified, usually manifesting as GGOs (3, 4). However, few studies have focused on the psychologic status of these patients. This study aimed to elucidate the prevalence and risk factors for anxiety and depression in patients with pulmonary GGOs. QoL and postoperative outcomes were also investigated in our research.
Based on our evaluation, a large number of patients with GGOs have anxiety or depression disorder (30.8%). Moreover, the occurrence rate of anxiety (26.3%) was higher than that of depression (18.0%). Li and colleagues (13) also revealed that 31.8% of patients with incidental pulmonary nodules have anxiety and that 19.4% have depression disorder. These findings indicate that anxiety and depression widely exist in patients with pulmonary GGOs and should not be ignored.
In our research, the number of GGOs was identified as a risk factor for preoperative anxiety. Compared to a single lesion, the treatment strategy for multiple GGOs is more complex and difficult, which may cause nervousness and anxiety. Anxiety and depression are also linked to social-economical factors and support from the institutions (23). We demonstrated that low levels of education and current unemployment are risk factors for depression. Older patients (>60 years) were also more vulnerable to depression than younger patients based on our research.
We found that preoperative depression is an independent risk factor for anxiety disorder and that preoperative anxiety is a risk factor for depression. Comorbidities of anxiety and depression in patients with lung cancer have been found in other studies (24, 25). Furthermore, preoperative anxiety and depression were associated with worse QoL in the patients with GGOs in our study. Hence, to improve QoL and postoperative outcomes, it is important to identify patients with anxiety or depression preoperatively and to offer professional psychological counselling and management.
Acute postoperative pain is an important problem after thoracic surgery and may increase pulmonary and cardiac complications and decrease quality of life. De Cosmo et al. found that patients with preoperative anxiety and depression had higher pain intensities after laparoscopic cholecystectomy (26). Our study revealed that preoperative anxiety and depression both significantly increased postoperative pain in patients who underwent thoracoscopic pulmonary resection. Therefore, special attention should be given to whether such patients experience severe postoperative pain, and adequate analgesics should be administered in a timely manner.
Preoperative anxiety and depression disorders have been considered to be strongly associated with extended LOS and increased complications after complex surgery, including colectomy, total hip arthroplasty, and lung resection (27). Our study found that the incidence of postoperative atrial fibrillation (AF) was higher in patients with preoperative anxiety. Anxiety may cause postoperative AF by increasing sympathetic tone, as based on other studies (28).
Several limitations of our study should be considered. First, postoperative psychological disorders were not evaluated, which may have changed when the patients were informed of the pathology. A dynamic evaluation of anxiety and depression would be more helpful to understand the psychological state of patients. Second, although patients with anxiety and depression were identified in our study, few of them followed advice for psychological counseling or therapy. Third, the surgical approaches had been planned and discussed with patients before admission in our study, patients who scheduled for lobectomy may suffer higher levels of anxiety or depression than patients who scheduled for wedge resection due to different risks of surgery. Furthermore, because anxiety and depression are perceived differently according to the patients beliefs and country of origin. All the patients came from China in our study. We think patients with different beliefs and countries should be included in further studies so that the conclusions in our study could be generalized. Finally, further studies are needed to eliminate preoperative anxiety and depression in patients with GGOs by popularizing medical knowledge and cooperating with professional psychologists to provide multidisciplinary care.
In conclusion, anxiety and depression are common psychological disorders among patients with pulmonary GGOs. Based on our study, preoperative anxiety and depression are related to lower QoL, severe postoperative pain, and a higher occurrence of postoperative AF. Psychological assessment and appropriate management are required for patients with GGOs who have anxiety or depression.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by The ethic committee of China-Japan Friendship Hospital. The patients/participants provided their written informed consent to participate in this study.
YH, FX and CL conceived and designed the study. QY, QM, JZ and YS contributed to the data collection. ZZ, GQ and YH contributed to statistical analysis. All authors contributed to the article and approved the submitted version.
We appreciate all the team members from China-Japan Friendship Hospital, the Department of Thoracic Surgery for their help. We also thank CT, from the Department of Psychiatry, China-Japan Friendship Hospital for helping with psychological counselling in our study.
This study was supported by the National High Level Hospital Clinical Research Funding (2022-NHLHCRF-YS-04), the Elite Medical Professionals Project of China-Japan Friendship Hospital (NO.ZRJY2021-QM23) and the Elite Medical Professionals Project of China-Japan Friendship Hospital (NO.ZRJY2021-GG07).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Humphrey LL, Deffebach M, Pappas M, Baumann C, Artis K, Mitchell JP, et al. Screening for lung cancer with low-dose computed tomography: a systematic review to update the US preventive services task force recommendation. Ann Intern Med. (2013) 159(6):411–20. doi: 10.7326/0003-4819-159-6-201309170-00690
2. Kummer S, Waller J, Ruparel M, Duffy SW, Janes SM, Quaife SL. Psychological outcomes of low-dose CT lung cancer screening in a multisite demonstration screening pilot: the Lung Screen Uptake Trial (LSUT). Thorax. (2020) 75(12):1065–73. doi: 10.1136/thoraxjnl-2020-215054
3. Zhang Y, Jheon S, Li H, Zhang H, Xie Y, Qian B, et al. Results of low-dose computed tomography as a regular health examination among Chinese hospital employees. J Thorac Cardiovasc Surg. (2020) 160(3):824–31. e824. doi: 10.1016/j.jtcvs.2019.10.145
4. Zhang Y, Fu F, Chen H. Management of ground-glass opacities in the lung cancer spectrum. Ann Thorac Surg. (2020) 110(6):1796–804. doi: 10.1016/j.athoracsur.2020.04.094
5. Aokage K, Miyoshi T, Ishii G, Kusumoto M, Nomura S, Katsumata S, et al. Influence of ground glass opacity and the corresponding pathological findings on survival in patients with clinical stage I non-small cell lung cancer. J Thorac Oncol. (2018) 13(4):533–42. doi: 10.1016/j.jtho.2017.11.129
6. Signorelli MS, Surace T, Migliore M, Aguglia E. Mood disorders and outcomes in lung cancer patients undergoing surgery: a brief summery. Future Oncol. (2020) 16(16s):41–4. doi: 10.2217/fon-2018-0835
7. Slatore CG, Golden SE, Ganzini L, Wiener RS, Au DH. Distress and patient-centered communication among veterans with incidental (not screen-detected) pulmonary nodules. A cohort study. Ann Am Thorac Soc. (2015) 12(2):184–92. doi: 10.1513/AnnalsATS.201406-283OC
8. Jung JY, Lee JM, Kim MS, Shim YM, Zo JI, Yun YH. Comparison of fatigue, depression, and anxiety as factors affecting posttreatment health-related quality of life in lung cancer survivors. Psychooncology. (2018) 27(2):465–70. doi: 10.1002/pon.4513
9. Su CH, Liu Y, Hsu HT, Kao CC. Cancer fear, emotion regulation, and emotional distress in patients with newly diagnosed lung cancer. Cancer Nurs. (2022). doi: 10.1097/NCC.0000000000001150. [Epub ahead of print]35984922
10. Wang X, Ma X, Yang M, Wang Y, Xie Y, Hou W, et al. Proportion and related factors of depression and anxiety for inpatients with lung cancer in China: a hospital-based cross-sectional study. Support Care Cancer. (2022) 30(6):5539–49. doi: 10.1007/s00520-022-06961-3
11. Chabowski M, Polanski J, Jankowska-Polanska B, Janczak D, Rosinczuk J. Is nutritional status associated with the level of anxiety, depression and pain in patients with lung cancer? J Thorac Dis. (2018) 10(4):2303–10. doi: 10.21037/jtd.2018.03.108
12. Lee Y, Lin PY, Lin MC, Wang CC, Lu HI, Chen YC, et al. Morbidity and associated factors of depressive disorder in patients with lung cancer. Cancer Manag Res. (2019) 11:7587–96. doi: 10.2147/CMAR.S188926
13. Li L, Zhao Y, Li H. Assessment of anxiety and depression in patients with incidental pulmonary nodules and analysis of its related impact factors. Thorac Cancer. (2020) 11(6):1433–42. doi: 10.1111/1759-7714.13406
14. Park S, Kang CH, Hwang Y, Seong YW, Lee HJ, Park IK, et al. Risk factors for postoperative anxiety and depression after surgical treatment for lung cancerdagger. Eur J Cardiothorac Surg. (2016) 49(1):e16–21. doi: 10.1093/ejcts/ezv336
15. Arrieta O, Angulo LP, Nunez-Valencia C, Dorantes-Gallareta Y, Macedo EO, Martinez-Lopez D, et al. Association of depression and anxiety on quality of life, treatment adherence, and prognosis in patients with advanced non-small cell lung cancer. Ann Surg Oncol. (2013) 20(6):1941–8. doi: 10.1245/s10434-012-2793-5
16. Polanski J, Chabowski M, Chudiak A, Uchmanowicz B, Janczak D, Rosinczuk J, et al. Intensity of anxiety and depression in patients with lung cancer in relation to quality of life. Adv Exp Med Biol. (2018) 1023:29–36. doi: 10.1007/5584_2017_50
17. Hernandez-Palazon J, Fuentes-Garcia D, Falcon-Arana L, Roca-Calvo MJ, Burguillos-Lopez S, Domenech-Asensi P, et al. Assessment of preoperative anxiety in cardiac surgery patients lacking a history of anxiety: contributing factors and postoperative morbidity. J Cardiothorac Vasc Anesth. (2018) 32(1):236–44. doi: 10.1053/j.jvca.2017.04.044
18. Walker J, Magill N, Mulick A, Symeonides S, Gourley C, Toynbee M, et al. Different independent associations of depression and anxiety with survival in patients with cancer. J Psychosom Res. (2020) 138:110218. doi: 10.1016/j.jpsychores.2020.110218
19. Annunziata MA, Muzzatti B, Bidoli E, Flaiban C, Bomben F, Piccinin M, et al. Hospital Anxiety and Depression Scale (HADS) accuracy in cancer patients. Support Care Cancer. (2020) 28(8):3921–6. doi: 10.1007/s00520-019-05244-8
20. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. (2002) 52(2):69–77. doi: 10.1016/S0022-3999(01)00296-3
21. Machingura A, Taye M, Musoro J, Ringash J, Pe M, Coens C, et al. Clustering of EORTC QLQ-C30 health-related quality of life scales across several cancer types: validation study. Eur J Cancer. (2022) 170:1–9. doi: 10.1016/j.ejca.2022.03.039
22. Fayers PM. Interpreting quality of life data: population-based reference data for the EORTC QLQ-C30. Eur J Cancer. (2001) 37(11):1331–4. doi: 10.1016/S0959-8049(01)00127-7
23. Yan X, Chen X, Li M, Zhang P. Prevalence and risk factors of anxiety and depression in Chinese patients with lung cancer: a cross-sectional study. Cancer Manag Res. (2019) 11:4347–56. doi: 10.2147/CMAR.S202119
24. Brown Johnson CG, Brodsky JL, Cataldo JK. Lung cancer stigma, anxiety, depression, and quality of life. J Psychosoc Oncol. (2014) 32(1):59–73. doi: 10.1080/07347332.2013.855963
25. Rutkowski J, Szymanik M, Blok M, Kozaka J, Zaucha R. Prospective evaluation of anxiety, depression and quality of life in medically inoperable early stage non-small cell lung cancer patients treated with stereotactic ablative radiotherapy. Rep Pract Oncol Radiother. (2017) 22(3):217–22. doi: 10.1016/j.rpor.2017.01.002
26. De Cosmo G, Congedo E, Lai C, Primieri P, Dottarelli A, Aceto P. Preoperative psychologic and demographic predictors of pain perception and tramadol consumption using intravenous patient-controlled analgesia. Clin J Pain. (2008) 24(5):399–405. doi: 10.1097/AJP.0b013e3181671a08
27. Paredes AZ, Hyer JM, Diaz A, Tsilimigras DI, Pawlik TM. The impact of mental illness on postoperative outcomes among medicare beneficiaries: a missed opportunity to help surgical patients? Ann Surg. (2020) 272(3):419–25. doi: 10.1097/SLA.0000000000004118
Keywords: ground-glass opacity, anxiety, depression, morbidity, quality of life, tumor
Citation: Han Y, Yu Q, Ma Q, Zhang J, Shi Y, Zhang Z, Qiang G, Xiao F and Liang C (2023) Assessment of preoperative anxiety and depression in patients with pulmonary ground-glass opacities: Risk factors and postoperative outcomes. Front. Surg. 10:1102352. doi: 10.3389/fsurg.2023.1102352
Received: 18 November 2022; Accepted: 9 January 2023;
Published: 30 January 2023.
Edited by:
Alfonso Fiorelli, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Beatrice Leonardi, Sapienza University of Rome, Italy© 2023 Han, Yu, Ma, Zhang, Shi, Zhang, Qiang, Xiao and Liang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chaoyang Liang Y2hhb3lhbmdsaWFuZ0Bob3RtYWlsLmNvbQ== Fei Xiao c2hhd2JqbXVAMTYzLmNvbQ==
Specialty Section: This article was submitted to Thoracic Surgery, a section of the journal Frontiers in Surgery
Abbreviations GGO, ground-glass opacity; LDCT, low-dose computed tomography; HADS, Hospital Anxiety Depression Scale; QoL, quality of life; POD, postoperative day; Cl, confidence interval; OR, odds ratio; EORTC, The European Organization for Research and Treatment of Cancer; AJCC, American Joint Committee on Cancer; TNM, tumor, node, metastasis.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.