 Fabio Medas1*†
Fabio Medas1*† Enrico Moroni2
Enrico Moroni2 Simona Deidda1Luigi Zorcolo1Angelo Restivo1
Simona Deidda1Luigi Zorcolo1Angelo Restivo1 Gian Luigi Canu1
Gian Luigi Canu1 Federico Cappellacci1
Federico Cappellacci1 Pietro Giorgio Calò1Stefano Pintus2
Pietro Giorgio Calò1Stefano Pintus2 Giovanni Fantola2
Giovanni Fantola2
- 1Department of Surgical Sciences, University of Cagliari, Cagliari, Italy
- 2Obesity Surgery Unit, Surgical Department, “ARNAS G. Brotzu” Hospital, Cagliari, Italy
Introduction: Superobesity (SO) is defined as a BMI > 50 Kg/m2, and represents the extreme severity of the disease, resulting in a challenge for the surgeons.
Methods: In this retrospective study we aimed to compare the outcomes of SO patients compared to morbidly obese (MO) patients.
Results: We included in this study 154 MO patients, with a median preoperative BMI of 40.8 kg/m2, and 19 SO patients with median preoperative BMI of 54.9 kg/m2. The MO patients underwent sleeve gastrectomy (SG) in 62 (40.3%) cases, laparoscopic Roux-and-Y gastric bypass (LRYGBP) in 85 (55.2%) cases and One-Anastomosis Gastric Bypass (OAGB) in 7 (4.5%) cases. underwent OAGB. The patients in the SO group were submitted to SG in 11 (57.9%) cases, LRYGBP in 5 (26.3%) cases, and OAGB in 3 (15.8%). At 24-month follow-up, an excess weight loss (EWL) >50% was achieved in 129 (83.8%) patients in the MO group and in 15 (78.9%) in the SO group (p = 0.53). A BMI < 35 kg/m2 was achieved in 137 (89%) patients in the MO group and from 8 (42.2%) patients in the SO group (p < 0.001). The total weight loss was significantly directly related to the initial BMI. Superobesity was identified as independent risk factor for surgical failure when considering the outcome of BMI < 35 kg/m2.
Discussion: Our study confirms that, although SO patients tend to gain a greater weight loss than MO patients, they less frequently achieve the desired BMI target. In this setting, it should be necessary to re-consider malabsorptive procedures as first choice.
Introduction
Super obesity (SO) is defined as a Body Mass Index (BMI) > 50 kg/m2, and represents the extreme severity of the disease, resulting in an increase in morbidity and mortality, and in poorer quality of life compared with morbid obesity (BMI > kg/m2 35 and <50 kg/m2).
Although bariatric surgery is proven to exceed medical treatment regarding weight loss and obesity-related morbidity resolution (1), in SO patients bariatric surgery may present suboptimal and less predictable results (2, 3). Furthermore, in this class of patients, surgery presents an increase in operative risks and is technically challenging (2, 4), Conventional methods, such as Laparoscopic Roux-and-Y Gastric Bypass (LRYGBP) and Laparoscopic Sleeve Gastrectomy (SG), gain different results in SO patients, with different weight-loss trends during the first two years after surgery (2), Conversely, One-Anastomosis Gastric Bypass (OAGB) seems to result in better middle- and long-term weight-loss (4, 5), Another important issue is to define success, insufficient weight loss or weight regain after surgery (6–9); indeed SO patients frequently need revision or second step surgery to achieve optimal results.
Several studies have demonstrated that after bariatric surgery less weight was achieved at 12–24 months (10–12); thus, 24 months should be considered the threshold to define a surgical result.
Excess Weight Loss (EWL)% represents a common measure used to define the success of bariatric interventions: surgical success is defined by an EWL greater than 50% (EWL > 50%) (7). Usually, EWL > 50% is achieved more easily in morbidly obese (MO) than SO patients, independent of the surgical procedure. Another target commonly used to define surgical success, particularly in SO patients, is represented by a BMI <35 kg/m2.
In this study, we aimed to evaluate the outcomes of bariatric surgery in SO patients compared to MO patients, and to assess patients' and surgical factors associated with bariatric success.
Patients and methods
Study design
This is a unicentric, retrospective study. Data were extracted from a prospectively maintained database of all morbidly obese patients undergoing bariatric surgery in our institution.
Inclusion criteria
We included in our study all the patients who underwent bariatric surgery from January 2018 to July 2020 at our institution. The indications for bariatric surgery were assigned according to IFSO criteria (13, 14), and all the cases were discussed and endorsed in a local interdisciplinary consensus meeting comprising surgeons, endocrinologists, nutritionists, and psychologists.
Exclusion criteria
All patients who underwent revisional surgery and patients without at least 12 and 24 months of postoperative follow-up were excluded.
Preoperative evaluation
Preoperative clinical evaluation was performed to detect patient characteristics (sex, age), biometric values (weight, height and BMI), and comorbidities, including diabetes, metabolic, cardiac or cerebrovascular diseases, gastroesophageal reflux disease (GERD), arthrosis and Obstructive Sleep Apnea Syndrome (OSAS). Serological blood tests according to IFSO guidelines (14), lower US-doppler and esophagogastroscopy with research of Helicobacter pylori infection were performed in all patients. Pneumological counselling, spirometry and polysomnography were performed in cases of positive pneumological disease or in cases of a score at stop-bang test ≥3. A nutritional evaluation was performed in all the patients to obtain preoperative weight loss, according to the ERAbS (Enanched Recovery after bariatric Surgery) protocol (15) and to reduce anaesthesia and surgery-associated risks. Psychological evaluation was performed to identify a history of eating disorder/behavior, anxiety or depression.
Type of procedure
LRYGBP was usually recommended in patients who suffered from severe GERD or type 2 diabetes (T2DM), or in patients with severe sweet eating behavior. SG was the favourite procedure in case of patients younger than 30 years old, large incisional hernia or severe small bowel adhesions. OAGB was not performed routinely and was indicated only in patients with severe dyslipidemia or diabetes.
LRYGBP was performed with the creation of a gastric pouch of approximately 30 cc, with a biliopancreatic limb of 75 cm, and an alimentary limb of 100–150 cm. SG was performed with gastric section 5 cm from the pylorus and 40 Fr bougie. OAGB was performed and 40 Fr bougie gastric pouch (>10 cm) and 150–180 cm biliopancreatic limb.
Follow-up
All patients were evaluated 1,3, 6, 12, 18, 24 months after surgery. Postoperative assessment included clinical, nutritional, or psychological evaluation, and serological blood test.
Endpoints
The primary endpoint was surgical success at 24 months, defined as a) BMI < 35 kg/m2, and b) EWL > 50%.
As secondary endpoints were evaluated as predictive and protective factors for surgical success (EWL < 50% and BMI < 35 kg/m2).
Statistical analysis
Patients were divided into two groups according to preoperative BMI (>50 kg/m2 and ≤50 kg/m2). The Chi-squared test or the Fisher's exact test was used to compare categorical variables, while Student's t-test or Mann–Whitney's U test was employed for continuous variables based on the data distribution. Data are presented as medians with 95% confidence intervals or means with standard deviations (SD) as appropriate.
An exploratory analysis was conducted to identify any correlations and redundancies between independent variables and to choose what models to test should be made. Multivariate logistic regression was used to evaluate factors associated with surgical failure, defined as EWL > 50% and BMI < 35 kg/m2 at 24 months. The correlation coefficient was calculated to determine whether the TWL was significantly associated with superobese or morbid obese status.
Statistical significance was defined as p < 0.05. Statistical analyses were performed with MedCalc version 20.105.
Results
A total of 332 patients underwent primary bariatric surgery during the study period. Among them, 173 (52.1%) patients had a complete postoperative follow-up at 12 and 24 months after surgery and were then included in the study.
The MO group included 154 patients with a mean age of 45.4 ± 11.2 years and median preoperative BMI of 40.8 kg/m2. The SO group included 19 patients with a mean age of 41.6 ± 10.5 years and median preoperative BMI of 54.9 kg/m2.There were 30 (19.5%) male patients in the MO group and 4 (21.1%) in the SO group. Regarding comorbidities, OSAS was present in 52 (33.8%) patients in the MO group and in 11 (57.9%) the SO group, high blood pressure in 82 (53.2%) cases in the MO group and in 8 (42.1%) in the SO group, osteoarthrosis in 93 (60.4%) patients in the MO group and in 13 (68.4%) in the SO group, GERD in 70 (45.5%) in the MO group and in 4 (21.1%) in the SO group, diabetes mellitus in 23 (14.9%) in the MO group and in 3 (15.8) in the SO group. In univariate analysis, preoperative weight and BMI were significantly higher in the SO groups (p < 0.001), and the incidence of OSAS and osteoarthrosis was higher in SO group (p = 0.0398 and p = 0.0404, respectively). Full preoperative data, including comorbidities, are reported in Table 1.
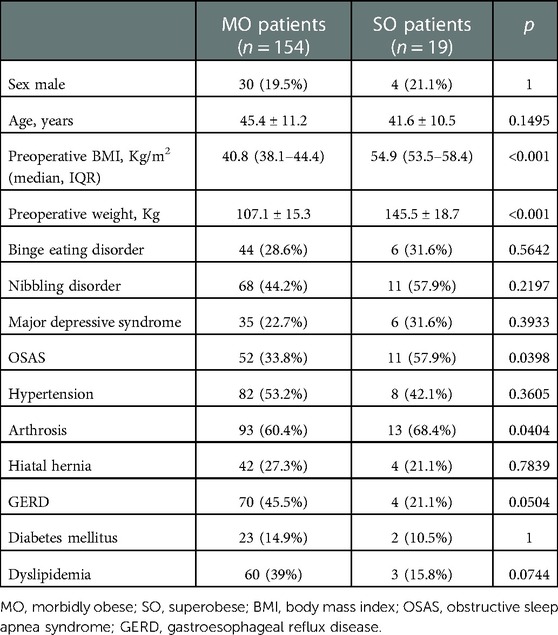
Table 1. Preoperative features.
As reported in Table 2, among the MO group, 62 (40.3%) patients underwent SG, 85 (55.2%) underwent LRYGBP and 7 (4.5%) underwent OAGB. The patients in the SO group were submitted to SG in 11 (57.9%) cases, LRYGBP in 5 (26.3%) cases, and OAGB in 3 (15.8%). The mean postoperative stay was 3.4 ± 1.5 days in the MO group and 3 ± 1.2 in the SO group. Postoperative complications were observed in 21 (13.6%) patients in the MO group and in 2 (10.5%) cases the in SO group.
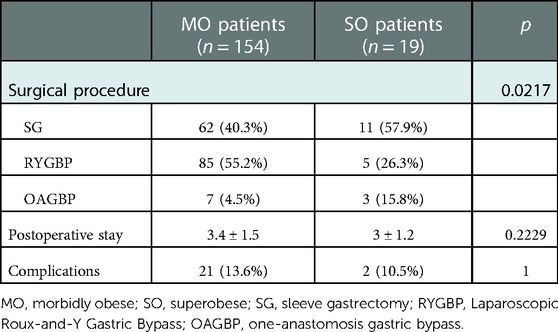
Table 2. Surgical management and postoperative complications.
The outcomes after 24 months of follow-up are reported in Table 3. The median BMI was 28.7 kg/m2 in the MO group and 36.4 kg/m2 in the SO group (p < 0.001). The TWL was 31.1 ± 11.7 Kg in the MO group, and 51.9 ± 18.3 Kg in the SO group (p < 0.001). The correlation test demonstrated that SO was significantly associated with a higher TWL (correlation coefficient = 0.4914; p < 0.001); the scatter diagram is reported in Figure 1.
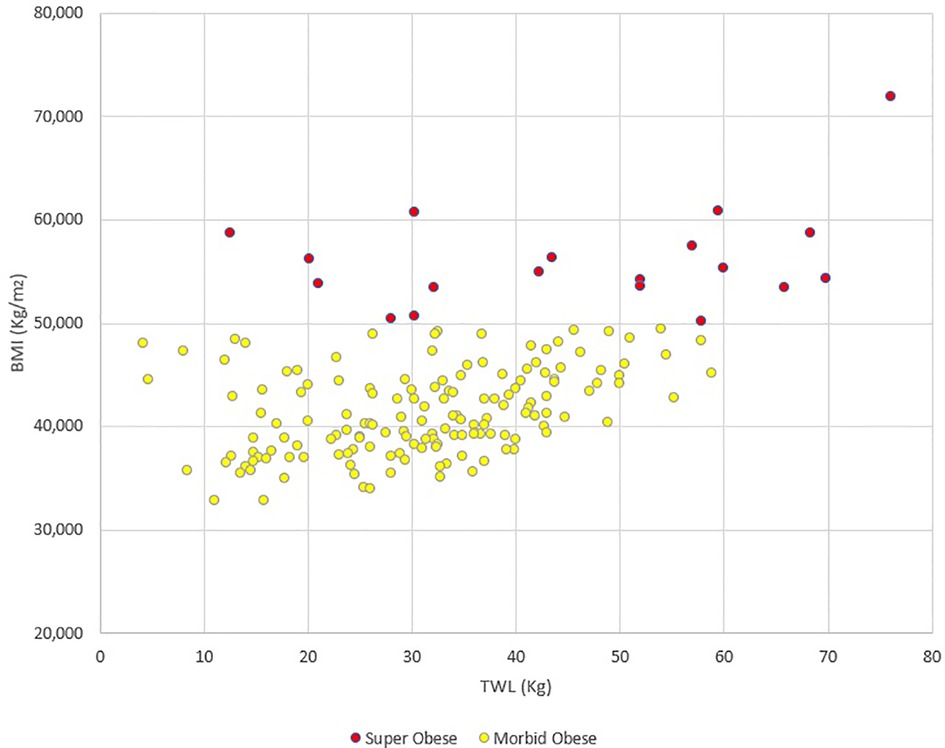
Figure 1. Scatter diagram representing the correlation between preoperative BMI and total weight loss (TWL). The correlation test demonstrated that preoperative BMI > 50 Kg/m2 was significantly associated with a higher TWL (correlation coefficient = 0.4914; p < 0.001).
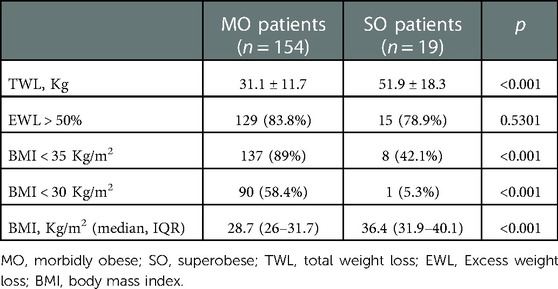
Table 3. Results at 24-month follow-up.
When considering an EWL > 50%, surgical success was achieved in 129 (83.8%) patients in the MO group and in 15 (78.9%) in the SO group (p = 0.53). A BMI < 35 kg/m2 was achieved in 137 (89%) patients in the MO group and from 8 (42.2%) patients in the SO group (p < 0.001); a BMI < 30 kg/m2 was reached from 90 (58.4%) patients in the MO group and in 1 (5.3%) case in the SO group (p < 0.001).
At multivariate analysis (Figure 2), when considering surgical success as EWL > 50%, the only significant predictive factor for failure was SG (OR = 2.816; 95%CI = 1.0741–7.3837; p = 0.0353); indeed, when considering surgical success as BMI < 35, superobesity was an independent predictive factor for failure (OR = 14.04; p = 0.002).
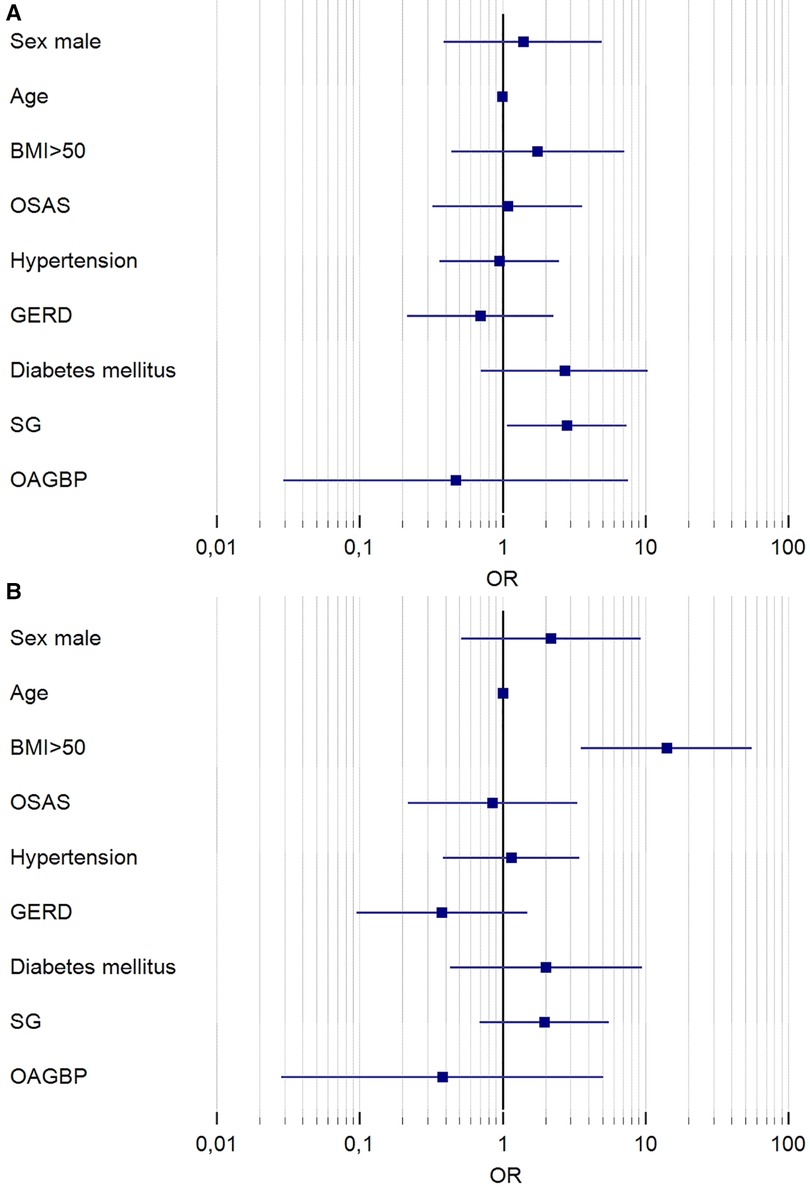
Figure 2. Forest plot of results of multivariate analysis. Results are reported in logarithmic scale. In (A) are reported the results of logistic regression considering the outcome of EWL > 50% at 24 months; the only significant variable predictive of surgical failure was SG (OR = 2.816; 95%CI = 1.0741–7.3837; p = 0.0353). In (B) are reported the results of logistic regression considering the outcome of BMI < 35 Kg/m2 at 24 months. The only significant variable predictive of surgical failure was superobesity (OR = 14.04; 95%CI = 3.5443–55.6861 p = 0.002). OR, odds ratio; OSAS, obstructive sleep apnea syndrome; GERD, gastroesophageal reflux disease; SG, sleeve gastrectomy; OAGBP, one-anastomosis gastric bypass.
Full comorbidity-related outcomes are reported in Table 4. Complete or partial resolution of OSAS was observed in 35 (67.3%) MO patients, and in 6 (54.5%) SO patients. Hypertension was completely or partially resolved in 36 (43.9%) MO patients, and in 3 (37.5%) SO patients. There were no significant differences among the groups.

Table 4. Partial or complete resolution of comorbidities at 24-month follow-up.
Finally, we performed a comparison of the outcomes at 24 months of follow-up of patients that underwent SG (Table 5). The TWL and the EWL were significantly higher in the SO group, whereas no significant differences were observed regarding the EWL > 50%. Conversely, the BMI targets <35 Kg/m2 and <30 Kg/m2 were reached significantly more frequently by the MO group. The median BMI at 24 months was 30.3 (27.1–32.2) Kg/m2 in the MO group, and 38.4 (36.5–41.1) Kg/m2 in the SO group (p < 0.0001).
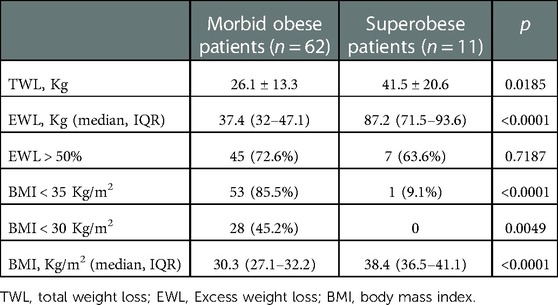
Table 5. Comparison of outcomes at 24 months of patients that underwent sleeve gastrectomy.
Discussion
In one of the most famous paradoxes of Zeno of Elea, Achilles, famous for his speed, will never reach the tortoise after granting her a head start. This narration appears to be similar to what happens to SO patients: in fact, SO patients start with a handicap (a greater BMI), run faster than MO patients (gaining a greater weight loss), but lose the race against them, rarely reaching the finish line of the BMI target <30 kg/m2.
In fact, our study confirmed that SO patients may present suboptimal results in terms of weight loss after bariatric surgery compared to MO patients. Our comparative analysis showed that SO patients significantly gained more weight loss during the first two years after surgery, but this was not enough to achieve surgical success in terms of BMI < 35 kg/m2: in fact, only 8 (42.1%) out of 19 SO patients reached this result, compared to 137 out of 154 (89%) MO patients. When considering the target of BMI < 30 kg/m2, only one SO patient (5.3%) reached the result, compared to 90 (58.4%) in the MO group. Furthermore, in our study, superobesity was identified as an independent risk factor for failure when considering the outcome of BMI < 35 kg/m2 at 24 months. However, we should note that, considering the outcome of EWL > 50% at 24 months, the results were not significantly different between the two groups. This result raises the issue whether EWL > 50% is a proper target to evaluate bariatric surgery failure, or if it would be better to consider the final BMI.
According to our results, several studies in which patients were stratified by obesity category showed that a higher baseline BMI was associated with a lower %EWL (2, 16, 17).
Our study did not show an increased risk of postoperative complications in SO patients. In this regard, the literature is still contrasting and inconclusive. Verhoeff reported five years of MBSAQIP data for SO patients (3). In his study, which included 751,952 obese patients who underwent obesity surgery, 173,110 (23%) SO patients had a small but significant increase in postoperative complications in nearly all measured domains, including serious complications (3.7% SO vs. 3.2% non-SO, p < 0.001) and mortality (0.17% SO vs. 0.07% non-SO, p < 0.001).
Tien-Chou Soong reported data of SO patients who underwent LRYGBP, OAGB, and SG: LRYGBP was associated with a higher major 30-day complication rate (4.8%) than other procedures (0.8% OAGB, p = 0.041; and 0.5% SG, p = 0.023) (4). Conversely, a recent meta-analysis compared SG and LRYGBP in SO patients, showing no difference in 30-day complications (2). Bettencourt-Silva did not report a difference in the 30-day morbidity rate comparing SG, LRYGBP and adjustable gastric banding (10). Only one study reported severe major adverse events in LRYGBP, even if this study showed no difference in 30-day complications (17).
Our univariate analysis on patients that underwent SG demonstrated that this type of intervention was associated to a lower success-rate in SO patients than in MO patients; furthermore, at multivariate analysis, we demonstrated that SG was an independent risk factor for surgical failure. SG is the most common procedure performed worldwide 18 in SO and non-SO patients. Verhoeff reported in the last five years that SG was used in 70% of SO patients and in 74.7% of non-SO patients (p < 0.001), and LRYGBP was used in 30% of SO patients and in 25.3% of non-SO patients (p < 0.001) (3).
A recent meta-analysis compared SG and LRYGBP in SO patients and showed that considerable weight loss was achieved following both procedures, but LRYGBP accomplished a higher %EWL (mean 59.73%) at 12 months (2). Although this tendency was already present at 6 months, a significant difference was not shown after 24 months; perhaps this result could be explained by the loss of patients at follow-up. Bettencourt-Silva included 213 SO patients in his study, performing 127 RYGB, 67 SG and 19 adjustable gastric banding procedures (10). At 12 and 24 months, the median %EWL was higher in LRYGBP (67.5% and 72.19%, respectively; p < 0.001) than in SG (58.7% and 59.9%) and adjustable gastric banding (38.7% and 48.3%). At 12 and 24 months, the median BMI was lower in LRYGBP (34.5 and 33.2 kg/m2) than in SG and adjustable gastric banding (p < 0.001). Tien-Chou Soong reported data on 498 SO patients, who underwent 62 RYGB, 190 SG, and 246 OAGB procedures (4). Five years after surgery, 64.6% of all the patients achieved a BMI < 35 kg/m2: 56.1% in the SG, 58.6% in the LRYGBP, and 71.8% in the OAGB group. Interestingly, the authors described LRYGBP with biliopancreatic limb of 100 cm and alimentary limb of 250–300 cm without common channel measurement, and OAGB with biliopancreatic limb of 250–350 cm without common channel measurement.
The choice of surgical procedure in SO patients should always be carefully evaluated and should be addressed based on surgical perioperative risk and surgical results (weight-loss, resolution of obesity-related complications, and quality of life). Considering weight-regain as the most common bariatric surgery failure in SO patients, reoperation could achieve better improvement in primary SG than primary RYGB, despite new procedures were promising (18).
Furthermore, it would be necessary to reconsider malabsorptive procedures as long limb LRYGBP, distal OAGB, single anastomosis gastro-ileal bypass (SAGI), single anastomosis duodeno-ileal bypass (SADI-S).
Furthermore, it would be necessary to reconsider mixed (restrictive and malbsorbitive) procedures as long limb LRYGBP, distal OAGB, single anastomosis gastro-ileal bypass (SAGI), single anastomosis duodeno-ileal bypass (SADI-S).
Our study has some limitations. First, this was a retrospective study. Then, the number of patients in the SO group was limited, and it is likely that the number was not sufficient to reach the statistical power to detect significant differences between the two groups regarding some aspects, including postoperative complications and comorbidity resolution. Furthermore, in our multivariate analysis SG was an independent risk factor for surgical failure, but the analysis was conducted considering both the SO and MO patients. For these reasons, the results of our study should be prudently considered.
Conclusion
The management of SO patients is an important issue. Our study confirmed that, after surgery, patients with BMI > 50 kg/m2 tend to lose more weight than MO patients, but less frequently reach the goal of BMI < 35 kg/m2. Even if our study has several limitations, mainly the limited number of SO patients, SG seems to be associated with an increased risk of surgical failure, particularly in SO patients. In this setting, it could be necessary to re-consider mixed procedures; however, the type of intervention should be chosen based on the patient's characteristics, according to the rule that “one size does not fit all”.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comitato Etico Indipendente AOU Cagliari. The patients/participants provided their written informed consent to participate in this study.
Author contributions
FM: study conception and design, acquisition of data, analysis and interpretation of data, drafting of the article, final approval of the version to be submitted, EM: acquisition of data, drafting of the article, final approval of the version to be submitted, SD: analysis and interpretation of data, final approval of the version to be submitted, LZ: analysis and interpretation of data, revision of the article for important content, final approval of the version to be submitted, AR: acquisition of data, analysis and interpretation of data, final approval of the version to be submitted, GLC: analysis and interpretation of data, revision of the article for important content, final approval of the version to be submitted, FC: study conception and design, acquisition of data, drafting of the article, final approval of the version to be submitted, PGC: revision of the article for important content, final approval of the version to be submitted, SP: study conception and design, acquisition of data, drafting of the article, final approval of the version to be submitted. GF: study conception and design, acquisition of data, drafting of the article, final approval of the version to be submitted. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Schauer PR, Bhatt DL, Kirwan JP, Wolski K, Aminian A, Brethauer SA, et al. Bariatric surgery versus intensive medical therapy for diabetes - 5-year outcomes. N Engl J Med. (2017) 376:641–51. doi: 10.1056/NEJMoa1600869
2. Gomes-Rocha SR, Costa-Pinho AM, Pais-Neto CC, de Araújo Pereira A, Nogueiro JPM, Carneiro SPR, et al. Roux-en-Y gastric bypass vs sleeve gastrectomy in super obesity: a systematic review and meta-analysis. Obes Surg. (2022) 32:170–85. doi: 10.1007/s11695-021-05745-8
3. Verhoeff K, Mocanu V, Dang J, Purich K, Switzer NJ, Birch DW, et al. Five years of MBSAQIP data: characteristics, outcomes, and trends for patients with super-obesity. Obes Surg. (2022) 32:406–15. doi: 10.1007/s11695-021-05786-z
4. Soong TC, Lee MH, Lee WJ, Almalki OM, Chen JC, Wu CC, et al. Long-term efficacy of bariatric surgery for the treatment of super-obesity: comparison of SG, RYGB, and OAGB. Obes Surg. (2021) 31:3391–9. doi: 10.1007/s11695-021-05464-0
5. Parmar CD, Bryant C, Luque-de-Leon E, Peraglie C, Prasad A, Rheinwalt K, et al. One anastomosis gastric bypass in morbidly obese patients with BMI ≥ 50 kg/m2: a systematic review comparing it with roux-en-Y gastric bypass and sleeve gastrectomy. Obes Surg. (2019) 29:3039–46. doi: 10.1007/s11695-019-04034-9
6. Mason EE, Amaral J, Cowan GS, Deitel M, Gleysteen JJ, Oria HE. Standards for reporting results. Obes Surg. (1994) 4:56–65. doi: 10.1381/096089294765558944
7. Guidelines for reporting results in bariatric surgery. Standards committee, American society for bariatric surgery. Obes Surg. (1997) 7:521–2. doi: 10.1381/096089297765555322
8. Grover BT, Morell MC, Kothari SN, Borgert AJ, Kallies KJ, Baker MT. Defining weight loss after bariatric surgery: a call for standardization. Obes Surg. (2019) 29:3493–9. doi: 10.1007/s11695-019-04022-z
9. van de Laar A, de Caluwé L, Dillemans B. Relative outcome measures for bariatric surgery. Evidence against excess weight loss and excess body mass index loss from a series of laparoscopic Roux-en-Y gastric bypass patients. Obes Surg. (2011) 21:763–7. doi: 10.1007/s11695-010-0347-0
10. Bettencourt-Silva R, Neves JS, Pedro J, Guerreiro V, Ferreira MJ, Salazar D, et al. Comparative effectiveness of different bariatric procedures in super morbid obesity. Obes Surg. (2019) 29:281–91. doi: 10.1007/s11695-018-3519-y
11. Thereaux J, Corigliano N, Poitou C, Oppert JM, Czernichow S, Bouillot JL. Comparison of results after one year between sleeve gastrectomy and gastric bypass in patients with BMI ≥ 50 kg/m2. Surg Obes Relat Dis. (2015) 11:785–90. doi: 10.1016/j.soard.2014.11.022
12. Gonzalez-Heredia R, Sanchez-Johnsen L, Valbuena VSM, Masrur M, Murphey M, Elli E. Surgical management of super-super obese patients: Roux-en-Y gastric bypass versus sleeve gastrectomy. Surg Endosc. (2016) 30:2097–102. doi: 10.1007/s00464-015-4465-6
13. Fried M, Yumuk V, Oppert JM, Scopinaro N, Torres AJ, Weiner R. Interdisciplinary European guidelines on metabolic and bariatric surgery. Obes Facts. (2013) 6:449–68. doi: 10.1159/000355480
14. Busetto L, Dicker D, Azran C, Batterham RL, Farpour-Lambert N, Fried M, et al. Practical recommendations of the obesity management task force of the European association for the study of obesity for the post-bariatric surgery medical management. Obes Facts. (2017) 10:597–632. doi: 10.1159/000481825
15. Fantola G, Agus M, Runfola M, Podda C, Sanna D, Fortunato F, et al. How can lean thinking improve ERAS program in bariatric surgery? Surg Endosc. (2021) 35:4345–55. doi: 10.1007/s00464-020-07926-5
16. Jain D, Sill A, Averbach A. Do patients with higher baseline BMI have improved weight loss with Roux-en-Y gastric bypass versus sleeve gastrectomy? Surg Obes Relat Dis. (2018) 14:1304–9. doi: 10.1016/j.soard.2018.05.014
17. Serrano OK, Tannebaum JE, Cumella L, Choi J, Vemulapalli P, Scott Melvin W, et al. Weight loss outcomes and complications from bariatric surgery in the super super obese. Surg Endosc. (2016) 30:2505–11. doi: 10.1007/s00464-015-4509-y
18. De Luca M, Piatto G, Sartori A, Zese M, Lunardi C, Targa S, et al. Single Anastomosis Jejuno-ileal (SAJI): a new model of malabsorptive revisional procedure for insufficient weight loss or weight regain after Roux-en-Y gastric bypass. Obes Surg. (2022) 32(9):3194–204. doi: 10.1007/s11695-022-06174-x
Keywords: obesity surgery, superobesity, morbidly obese patients, laparoscopic sleeve gastrectomy, laparoscopic Roux-and-Y gastric bypass
Citation: Medas F, Moroni E, Deidda S, Zorcolo L, Restivo A, Canu GL, Cappellacci F, Calò PG, Pintus S and Fantola G (2023) The paradox of Zeno in bariatric surgery weight loss: Superobese patients run faster than morbidly obese patients, but can't overtake them. Front. Surg. 10:1100483. doi: 10.3389/fsurg.2023.1100483
Received: 16 November 2022; Accepted: 16 January 2023;
Published: 2 February 2023.
Edited by:
Maurizio Gentile, Federico II University Hospital, Italy© 2023 Medas, Moroni, Deidda, Zorcolo, Restivo, Canu, Cappellacci, Calò, Pintus and Fantola. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabio Medas ZmFiaW9tZWRhc0B1bmljYS5pdA==
†ORCID Fabio Medas orcid.org/0000-0002-9546-0178
Specialty Section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery