
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg. , 06 March 2023
Sec. Surgical Oncology
Volume 10 - 2023 | https://doi.org/10.3389/fsurg.2023.1064145
This article is part of the Research Topic Neuroendocrine Tumours of the Gastrointestinal Tract, Liver and Pancreas: Current management and treatment strategies View all 11 articles
 Apostolos Koffas1*†
Apostolos Koffas1*† Alexandros Giakoustidis2,†
Alexandros Giakoustidis2,† Apostolis Papaefthymiou3
Apostolis Papaefthymiou3 Petros Bangeas2
Petros Bangeas2 Dimitrios Giakoustidis2
Dimitrios Giakoustidis2 Vasileios N Papadopoulos2
Vasileios N Papadopoulos2 Christos Toumpanakis4
Christos Toumpanakis4
Neuroendocrine neoplasms (NENs) are a heterogeneous group of neoplasms ranging from well-differentiated, slowly growing tumors to poorly differentiated carcinomas. These tumors are generally characterized by indolent course and quite often absence of specific symptoms, thus eluding diagnosis until at an advanced stage. This underscores the importance of establishing a prompt and accurate diagnosis. The gold-standard remains histopathology. This should contain neuroendocrine-specific markers, such as chromogranin A; and also, an estimate of the proliferation by Ki-67 (or MIB-1), which is pivotal for treatment selection and prognostication. Initial work-up involves assessment of serum Chromogranin A and in selected patients gut peptide hormones. More recently, the measurement of multiple NEN-related transcripts, or the detection of circulating tumor cells enhanced our current diagnostic armamentarium and appears to supersede historical serum markers, such as Chromogranin A. Standard imaging procedures include cross-sectional imaging, either computed tomography or magnetic resonance, and are combined with somatostatin receptor scintigraphy. In particular, the advent of 111In-DTPA-octreotide and more recently PET/CT and 68Ga-DOTA-Octreotate scans revolutionized the diagnostic landscape of NENs. Likewise, FDG PET represents an invaluable asset in the management of high-grade neuroendocrine carcinomas. Lastly, endoscopy, either conventional, or more advanced modalities such as endoscopic ultrasound, capsule endoscopy and enteroscopy, are essential for the diagnosis and staging of gastroenteropancreatic neuroendocrine neoplasms and are routinely integrated in clinical practice. The complexity and variability of NENs necessitate the deep understanding of the current diagnostic strategies, which in turn assists in offering optimal patient-tailored treatment. The current review article presents the diagnostic work-up of GEP-NENs and all the recent advances in the field.
Neuroendocrine neoplasms (NEN) are rare and heterogeneous tumors that are phenotypically similar and derive from the diffuse neuroendocrine cell system. These neoplasms demonstrate a rising prevalence and incidence. This is likely a result of the deeper and better understanding of these tumors, but also of the advent and integration of more advanced diagnostic means (1–4). In general, NENs exhibit slow growth and often absence of specific symptoms, which may in turn delay the diagnosis until at an advanced stage, when overt symptoms may develop. Among the several distinct sites of origin, gastroenteropancreatic NENs (GEP NENs) represent the commonest subtype, accounting for nearly 60% of all NENs. Among these, small bowel- (SBNEN) and pancreatic- NENs (pNEN) are the most frequent (5–8).
In addition to the variable primary sites, tumor heterogeneity is also evident by their variable biologic behavior. Often these tumors run a “benign” course with no ostensible disease progression and excellent prognosis. However, non-uncommonly, they may also be truly malignant, associated with an aggressive course, poor prognosis and a very limited life expectancy, mimicking other cancers (9).
This complexity and variability of NENs necessitate the deeper and better understanding of the current diagnostic armamentarium and strategic approach, and integration in clinical practice of all novel diagnostic tools. This in turn is pivotal to determine the optimal (tailored) treatment, including accurate selection of surgical candidates. The diagnostic cascade should be initiated once there is clinical suspicion. Initial work-up involves assessment of serum Chromogranin A and, in selected patients, measurement of gut peptide hormones. Recently, the measurement of multiple NEN-related transcripts or the detection of circulating tumor cells has been introduced and will play a key role, and seems to be superior to historical serum markers, such as Chromogranin A. Cross-sectional imaging, combined with somatostatin receptor scintigraphy and PET scan will complement the diagnostic approach and assist in disease stratification. Ultimately, the gold-standard of the diagnosis remains histopathology. The present review discusses the diagnostic work-up of GEP-NENs and presents all the novel diagnostic means that emerged over the last years. Table 1 summarizes current diagnostic modalities and their clinical utility.
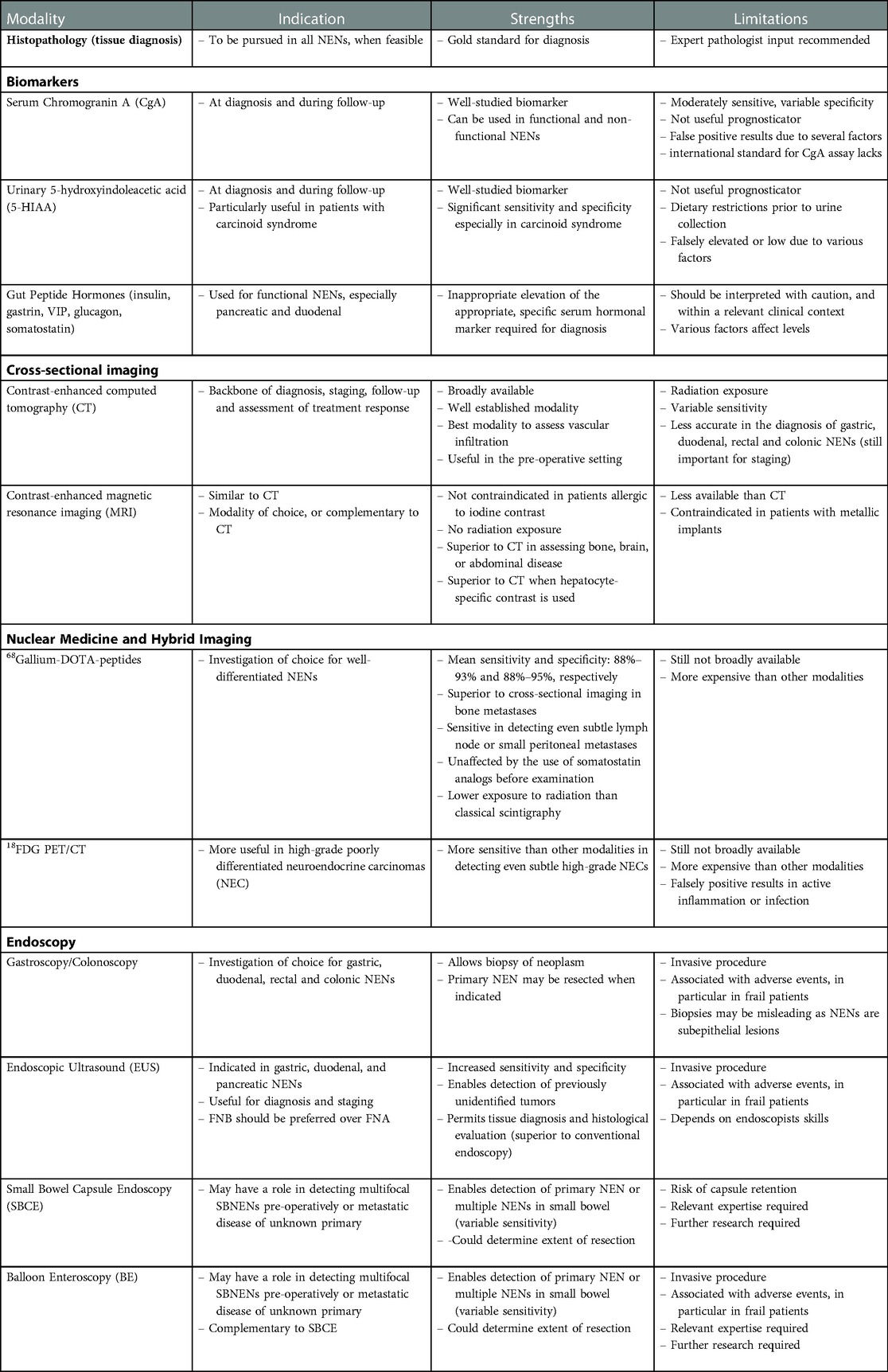
Table 1. Current diagnostic tools in neuroendocrine neoplasms (NENs).
Not uncommonly, GEP-NENs are incidentally discovered. The rate of such presentation varies; for instance, in pNENs not producing hormones incidental diagnosis can exceed 50% (10), whereas it can be as high as 80% in the case of appendiceal NENs (11). Often NENs cause non-specific symptoms, such as abdominal pain or discomfort, weight loss, change in bowel habits or diarrhea. These symptoms are often attributed to other causes, such as gastritis, irritable bowel syndromes, or other relevant disorders, before a diagnosis is established. In contrast to such presentation, however, NENs may also overproduce hormones, such as 5-hydroxytryptamine (5-HT, serotonin), that results is associated symptoms. Such tumors are termed functional NENs, in contrast to non-functional NENs. For instance, the “carcinoid syndrome” is a syndrome that is mostly present in SBNENs, in the presence of hepatic or retroperitoneal metastases. This is caused due to 5-HT reaching the systemic circulation. As a result, patients present with a variety of symptoms, often precipated by a variety of foods, alcohol, stress, ot other triggers. Most commnonly subjects present with paroxysmal flushing, chronic diarrhea, wheezing and less frequently carcinoid heart disease (CHD), among others. Analogous to this, the secretion of other hormones by this subgroup of NENs, termed functionally active, such as insulin, gastrin, vasoactive intestinal peptide, glucagon, somatostatin, and others, can lead to specific syndromes, which are discussed later in more detail (6, 8). Table 2 summarizes functional pNENs and their respective presentation.
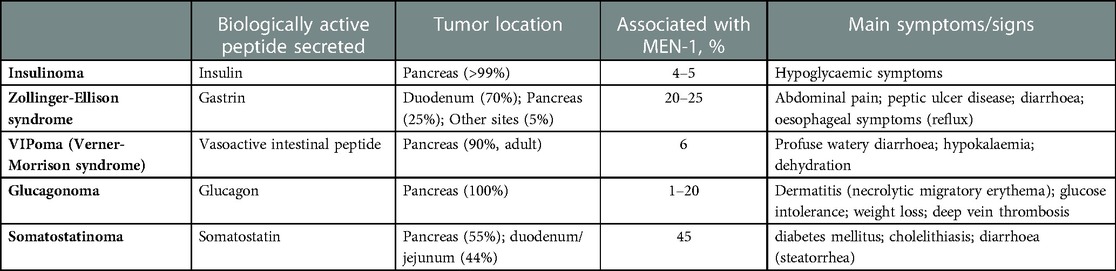
Table 2. Functional pancreatic neuroendocrine tumor syndromes.
Histopathological confirmation represents the gold standard for the diagnosis of NENs and is recommended by the European Neuroendocrine Tumor Society (ENETS) (12). Tissue diagnosis should be pursued when clinically feasible. It should be noted that a biopsy is deemed superior to a fine needle aspirate (FNA) when, this is feasible (12, 13). This is of particular interest in the context of Endoscopic Ultrasound (EUS), where if not enough material is available, there is a risk of under-grading the tumor (6, 14, 15). In a recent study by our study group, data of patients who underwent EUS-guided tissue sampling of suspicious pancreatic lesions over a 13-year period were analyzed. Lesions underwent EUS-FNA or FNB sampling, or a combination of the two, and the accuracy and safety of different EUS-guided sampling methods for confirmed pNENs were investigated. Diagnostic yield of EUS-FNA and EUS-FNB alone, including the inadequate specimens, was 77.5 % (95 % CI: 68.9 %– 86.2 %) and 85.4 % (95 % CI: 74.6% – 96.2 %), respectively, whereas the combination of both sampling modalities established the diagnosis in over 95% of cases. Diagnostic sensitivity among the adequate samples for EUS-FNA, EUS-FNB and for the combination of the two methods was 88.4 % (95 % CI: 80.9% – 96.0 %), 94.3 % (95 % CI: 86.6% – 100 %) and 100 % (95 % CI: 100 %– 100%). These findings clearly illustrated that EUS-FNB improves diagnostic sensitivity and provides further information than cytological assessment alone, in patients with pNENs (16).
When a NEN is considered or clinically suspected, in addition to the conventional histopathological analysis, immunohistochemistry should be performed, to assess the tumor phenotype and Ki-67. Immunohistochemical staining with synaptophysin, and Chromogranin A (CgA) is also required. Ki-67 is a cell proliferation–associated nuclear marker, that is critical in assessing the differentiation of NENs, and as a result their respective course. CgA is a protein commonly secreted by neuroendocrine tumor cells (17).
The AJCC (American Joint Committee on Cancer), ENETS, UICC (International Union for Cancer Control), WHO (World Health Organization) developed a series of systems to classify NENs. Similar to other neoplasms, these classification systems are used to stage the disease, and are essential for treatment selection and prognostication (18–25). In particular, the WHO proposes a universal definition system for neuroendocrine neoplasia based on differentiation and proliferative grading. Table 3 summarises the novel WHO NEN classification.It integrates the mitotic count, and most importantly the nuclear antigen Ki-67, as markers of the proliferation activity of these neoplasms. Ki67 is more accurate and reproducible than the mitotic index (24, 25). Historically, a Ki-67 > 20% was believed to define poorly differentiated neoplasms, indicating an overall unfavorable prognosis. However, emerging evidence indicated that there is a distinct category of well-differentiated grade 3 neuroendocrine tumors (NETs), that is clearly different from the very aggressive poorly differentiated grade 3 neuroendocrine carcinomas (NECs), the latter associated with an unfavorable prognosis (19–21). More recently, the 5th edition of the WHO Classification of Endocrine Tumors was published, termed Classification of Endocrine and Neuroendocrine Tumors. This up-to-date classification system integrates this emerging evidence. In particular, the novel WHO 2022 system describes NECs, epithelial poorly differentiated neoplasms, composed of cells with severe cellular atypia and severely deranged molecular/genetic profiles, that broadly retain neuroendocrine markers. These NECs are further subclassified in small or large cell types, and Ki-67 is >20%, often >70%. This is in contrast to well differentiated grade 3 NETs. This is shown to have clinical implications on prognosis: Grade 3 NECs for instance were shown to have a 4 months' shorter median survival than G3 NETs and responded better to platinum-based chemotherapy (26, 27).
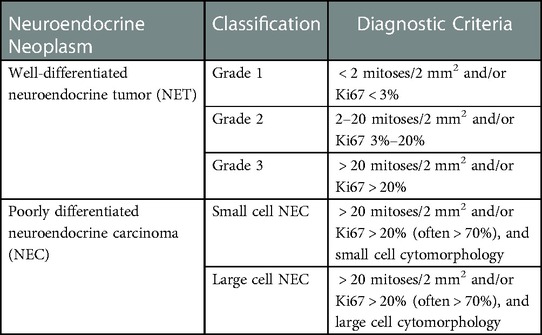
Table 3. WHO 2022 classification system for neuroendocrine tumors.
Over the years, a considerable number of biomarkers have been integrated in clinical practice, and are used for diagnostic purposes, but also to follow-up patients with established disease. The most important among them is the general serum biomarker CgA. This is an acid glycoprotein present in the secretory dense core granules of most neuroendocrine cells. It is also secreted from neuroendocrine-derived tumors, including GEP-NENs, pheochromocytomas, and others. Of note, both functional and non-functional NENs may result in elevated CgA levels (28). CgA is a moderately sensitive marker, whereas specificity largely relies upon the type and tumor burden (for instance, specificity of approximately 100% has been reported in metastatic tumors). In particular, specificity of assays ranges from 68 to 100% and sensitivity ranges from 42%–93%, depending upon tumor primary site, grade, or disease burden (29). Significantly elevated CgA levels are unlikely to be encountered in other disease than NENs, with the exception maybe of patients receiving protein pump inhibitors (PPIs) (30–34). Although this is a marker that has been well validated for diagnostic and follow-up purposes, CgA cannot steadily be used for prognostication (35, 36).
In addition, CgA should be interpreted with caution as several conditions may lead to falsely positive elevation. Reasons for false positive CgA elevation include renal disease, Parkinson disease, uncontrolled hypertension, pregnancy, hypergastrinemia, chronic atrophic gastritis, among others. In addition, treatment with antisecretory medications, especially PPIs have been associated with falsely elevated CgA levels, and PPIs should be interrupted, leaving a clearance of at least 3 half-lives, prior to testing, where this is possible and safe for the patient. Analogous to this, steroid treatment or glucocorticoid excess can lead to upregulation of CgA. A limitation of CgA is also the fact that a recognized international standard for CgA assay is not available and variations in assay types may influence results. It is thus recommended that reference laboratories should be preferred when available, and that serial measurements should be performed using the same assay (28).
As already discussed, NENs may secrete 5-hydroxytryptamine (5-HT, serotonin) and other hormones, and in some subjects particularly with SBNENs this may mediate the carcinoid syndrome. Urinary 5-hydroxyindoleacetic acid (5-HIAA) is the urinary metabolite, following breakdown of 5-HT. Urinary 5-HIAA has proven of great value, and has been integrated in the diagnosis and follow-up of patients with carcinoid syndrome (28). The sensitivity and specificity of this marker has been reported to be 70% and 90%, respectively. Midgut NENs, such as SBNENs, produce more serotonin than the rest of the NENs, and it is when 5-HIAA is most useful. It should also be noted that urinary 5-HIAA levels depend upon the respective volume of the neoplasm and thus could be normal in individuals with no metastases (37, 38). Like CgA, there is no sound scientific evidence supporting the role of urinary 5-HIAA for prognosis. To increase accuracy, specific dietary restrictions should be followed prior to urine collection. Falsely low urinary 5-HIAA levels may be encountered in cases of impaired kidney function or on haemodialysis. Lastly, one needs to consider that urinary 5-HIAA levels may be falsely elevated in cases of malabsorptive disease, not treated. Examples include untreated coeliac disease, tropical sprue, Whipple disease, etc (28).
A less common manifestation of carcinoid syndrome is CHD, which affects nearly 20% of patients with “carcinoid syndrome”. In CHD, plaque-like, fibrous endocardial thickening of the cardiac valves develops. Patients with CHD have a poor prognosis. This is due to the gradual development of heart valve dysfunction and finally progressive heart failure. CHD is believed to be caused by this same tumor secretion of vasoactive hormonal products. Bhattacharyya et al. prospectively followed-up more than two hundred fifty patients with carcinoid syndrome for a median follow-up of 29 months. 44 of the included individuals either developed de novo CHD or exhibited deterioration in the pre-existing valvular dysfunction. This was associated with a synchronous elevation in the median levels of urinary 5-HIAA 5-HIAA levels of more than 300 μmol/24 h were reported to independently predict CHD development or progression, among other factors (39).
N-terminal pro-brain natriuretic peptide (NT-proBNP) is a natriuretic peptide, and it is an established diagnostic test for heart failure and its management. In the context of NENs, it should be used to screen for CHD, with proven and well-established value (40). Bhattacharyya et al. reported that in patients with carcinoid syndrome and valvular involvement, NT–proBNP was significantly higher than in patients without CHD. A cutoff level of 260 pg/ml was reported to be 92% sensitive and 91% specific to diagnose CHD in subjects with carcinoid syndrome (41). It is recommended that this biochemical marker should be routinely included in the diagnostic assessment and subsequent follow-up of patients with NENs and carcinoid syndrome.
In functional tumors, measurement of specific hormones is appropriate [glucagon in glucagonoma, vasoactive intestinal peptide (VIP) in VIPoma, gastrin in gastrinoma, insulin in insulinoma, etc.]. There are two distinct clinical syndromes that need to be exceptionally presented: gastrinoma and Zollinger Ellison Syndrome (ZES); and insulinoma.
Gastrinomas are usually located in the duodenum or pancreas, secrete gastrin, and cause a clinical syndrome known as ZES. This results from hyperproduction of gastric acid by the parietal cells of the stomach, triggered by gastrin hypersecretion from the NEN. This in turn causes peptic ulcer disease, abdominal pain and chronic diarrhoea and malabsorption. The most common presentation of ZES is with duodenal ulcers, peptic ulcer symptoms, GERD symptoms or ulcer complications and diarrhea. Conversely, multiple ulcers or ulcers in unusual locations are a less frequent presenting feature than in the past. ZES should be suspected in cases of recurrent, severe or familial peptic ulcer disease, in particular when H. pylori is not detected or other risk factors are absent. In addition, peptic ulcer disease that is resistant to treatment, or associated with severe GORD or severe complications, should also prompt the physician to consider ZES (42). It should be noted that hypergastrinemia can occur much more frequently outside the context of a ZES cause, such as hypo- or achlorhydria secondary to chronic atrophic gastritis, pernicious anaemia, helicobacter pylori, or due to the use of proton-pump inhibitors (8). For ZES to be confidently diagnosed, inappropriately elevated fasting serum gastrin (FSG) level should be shown in the presence of gastric acid secretion. ZES can be diagnosed when FSG is more that 10-fold elevated and the gastric pH <2. However, in about 60% these requirements are not present (43), and additional tests are required, i.e., secretin test (44). It is acknowledged that the diagnosis of ZES is becoming more challenging, primarily due to increasing unreliability of commercial gastrin assays; the lack of availability of secretin to perform secretin provocative tests, where indicated; and the widespread use of PPIs (8).
Insulinoma is a rare pancreatic NEN (pNEN) that secretes insulin. This secretion is not properly regulated by glucose, and as a result Insulinomas continuously and inappropriately secrete insulin causing hypoglycaemia. Typically, patients with such tumors develop hypoglycaemia while fasting or during exercise, which improve by eating (8). In a consensus report from the US Endocrine Society, the proposed criteria for the diagnosis of Insulinoma were as follows: endogenous hyperinsulinism documented by the finding of symptoms, signs, or both; with plasma concentrations of glucose <55 mg/dl (3.0 mmol/litre), insulin ≥ 3.0 μU/ml (18 pmol/litre), C-peptide ≥0.6 ng/ml (0.2 nmol/litre), and proinsulin ≥5.0 pmol/litre (45).
Most pNENs occur sporadically in a non-inherited fashion. Nevertheless, a variable proportion of them can emerge as part of an inherited syndrome. Multiple Endocrine Neoplasia type 1 (MEN1) is the most important inherited syndrome that accounts for up to 30% of gastrinomas and <5% of Insulinomas. This is an autosomal-dominant genetic condition involving the development of multiple tumors, arising from neuroendocrine cells. These tumors more frequently occur in endocrine glands, mainly the parathyroids, GEP system and pituitary gland (8). The diagnosis of MEN1 in patients with a functional pNEN is frequently markedly delayed (5–9.5 years) (46, 47). Patient diagnosed with ZES should be routinely screened for MEN1, due to the association between the two conditions. Relevant guidelines recommend that parathormone level in the serum, ionized calcium levels and prolactin are routinely performed at diagnosis, and then annually in these patients. Additionally, if a patient is diagnosed with insulinoma before the age of 20 or with multiple insulinomas at any age, MEN1 should also be suspected, and patient screened (8, 42). Overall, we would recommend that all patients with functional pNENs are screened, as above, despite some paucity of relevant data.
Computed Tomography (CT) with contrast of the neck-chest-abdomen and pelvis, including three-phase CT of the liver, represents the cornerstone for the diagnosis, staging and follow-up of NENs. Magnetic resonance imaging (MRI) with contrast should be the examination of choice to assess the liver, pancreas, brain and bone, when possible. It is recommended that somatostatin receptor imaging is used for staging, follow-up, and on a pre-operative basis; 68Ga-DOTATATE is recommended when available. Lastly, 18FDG-PET/CT is of greater value in cases of higher glucose metabolism and less somatostatin receptor expression. Therefore, we recommend that 18FDG-PET/CT is considered for high grade NENs, mainly G3 tumors (48–52).
CT scan represents the backbone of the NEN diagnosis; and is also broadly used for staging, surveillance and monitoring treatment response. Its' use is well-established as a result of its diagnostic accuracy and broad and steady availability. CT is the best modality to assess vascular infiltration and is very helpful in the pre-operative setting. The sensitivity and specificity for CT to diagnose individuals with NEN ranges from 61 to 93% and 71 to 100%, respectively (48).
In particular, the diagnostic accuracy of CT for the diagnosis of pNEN ranges from 69%–94% (53–56). For the diagnosis of small bowel NENs, CT enteroclysis exhibits sensitivity of up to 85% and 97%, respectively (57–59). CT enterography is similar to CT enteroclysis, primarily differing in the method of contrast administration. The sensitivity of both methods is comparable (60). Gastric (gNENs), duodenal (dNENs), rectal (rNENs) and NENs of the colon are often diagnosed by endoscopy, either conventional or EUS. Therefore, CT has a limited role for the diagnosis of these tumors, but should be used for staging (48). CT sensitivity and specificity for diagnosing liver metastases ranges from 75%–100% and 83%–100%, respectively (61–64). Careful consideration is required, however, as CT scan cannot steadily differentiate NEN liver metastases from liver metastases originating from other malignancies (48). Additionally, CT is less accurate in detecting smaller lesions (< 1cm) and bone metastases (sensitivity <60%) and this limitation needs to be considered (65–67).
MRI is increasingly available and has the advantage of no exposure to radiation. Additionally, as is the case of other types of cancer, MRI appears superior to CT in assessing bone, brain, or abdominal disease, and may be preferred as the imaging modality of choice, or complementary to CT. In particular, MRI has higher tissue resolution than CT and should be preferred for assessing bone metastases. In addition, on patients who are allergic to iodine contrast agents, MRI should also be the preferred modality (68). Furthermore, diffusion weighted imaging (DW imaging) allows detection of subtle neoplastic tissue changes and is highly sensitive in detecting NEN-related liver metastases (48).
In the assessment of pNENs, tumor volume affects the accuracy of MRI. In particular, it is 70% sensitive for primary NENs larger than 2.5 cm, and this sensitivity decreases for lesions < 1.5 cm (69, 70). The accuracy of DW-MRI for the detection of primary NENs and metastatic disease is comparable to PET/CT (71–73). MRI is helpful in surgical planning and assessment of the relationship of the tumor to the main pancreatic duct if enucleation is planned (74). Several features of the neoplasms, such as its size and shape; enhancement pattern, vascular invasion, and involvement of lymph nodes can assist in determining tumor grade (74). MRI also enables additional sequences for pancreatic neoplasms; and in particular MRCP should be used to determine the anatomical relationship between the tumor and the pancreatic and common bile ducts (48).
The use of hepatocyte-specific contrast media renders MRI scan superior to CT in characterizing liver lesions (48, 74). In a prospective study that compared MRI, CT, and somatostatin receptor scintigraphy (SRS), MRI was reported to detect more metastasic sites compared to the other modalities. In particular, the respective sensitivity for detecting liver metastases was 95.2%, 78%, and 49.3% (75). If hepatic surgery is considered, MRI of the liver should be considered for better assessment of the hepatic tumor load prior to the surgical intervention.
Lastly, in the assessment of SBNENs, a recent study by Dohan et al., reported that the overall sensitivity of MR-enterography for small bowel NENs detection was 74% (95% CI: 54%–89%) on a per-lesion basis and 95% (95% CI: 74%–100%) on a per-patient basis, providing direct evidence of the diagnostic value of MRI in this setting too (76).
Echocardiography (ECHO) is of paramount importance in the diagnosis of CHD and is the gold standard in determining severity of the condition. It is a prerequisite that only physicians experienced in its use are involved. Diffuse thickening of the valve leaflets; isolated thickening of a single valve leaflet without significant reduction in leaflet mobility; or the development of valvular regurgitation, may all be seen in CHD. 3-dimensional trans-thoracic-ECHO or trans-oesophageal ECHO may be preferred to examine the pulmonary and tricuspid valves (41). ENETS recommend echocardiography to be performed at baseline and then six monthly to annually in relevant patients (77).
Cardiac magnetic resonance imaging (CMRI) and cardiac computed tomography (CCT) are useful additional modalities, and can complement ECHO. The former is an excellent tool when echocardiographic windows are poor or when structures such as the pulmonary valve cannot be visualised. It also allows measurement of heart metastases and provides information on invasion of extra-cardiac structures (41). CCT can assist in examining the heart valves and right ventricular size and function; the coronary arteries before heart surgery; and depict myocardial metastases and their relationship with the affected valve(s) (78, 79).
Somatostatin is a cyclic peptide that exerts strong regulatory effects in the body. The action of this protein is mediated through membrane-bound receptors. These receptors are expressed in high volumes in neuroendocrine cells, and currently five subclasses 1–5 have been cloned (sst1–sst5). These somatostatin receptors are also expressed in high volumes in NENs (80, 81). The landscape was revolutionised following the advent of PET/CT; and novel tracers have been developed, including somatostatin analogs (SSAs), such as 68Ga-DOTA, and metabolic markers, such as 18F-FDG (82, 83). DOTATOC OTANOC, and DOTATATE are the main DOTA-peptides that bind to somatostatin receptors. As a result, they are currently broadly used both in the diagnostic/staging cascade, but also for therapeutic purposes, i.e. Peptide receptor radionuclide therapy (PRRT) (84, 85). PET/CT with 68Ga-DOTA-peptides is more sensitivity than cross-sectional imaging with CT or classical scintigraphy for detecting well-differentiated tumors (52, 86). Conversely, 18F-FDG PET/CT is used for less differentiated NETs, due to the presence of increased glucose in these tumors. This also illustrates the increased propensity for more aggressive course and poor prognosis (87).
Historically, 111In-pentetreotide (Octreoscan™) represented the mainstay of SRS. 68Ga-DOTA-SSAs has superseded and replaced classical scintigraphy in an increasing number of healthcare settings, owing to the greater accuracy and lower exposure to radiation, and it is now considered the investigation of choice for well-differentiated NENs. Nevertheless, primarily due to financial limitations, Octreoscan™ still represents the backbone of scintigraphy in many centers, especially in healthcare settings with restricted resources. At present, we recommend that SRS should only be used only when PET/CT imaging is unavailable. Overall, the sensitivity of 111In-pentetreotide scintigraphy for the detection of these neoplasms ranges from 60%–80% and the specificity from 92%–100% (88–92). Conversely, 68Ga-DOTA-SSAs exhibits greater diagnostic accuracy, albeit small variations reported in the literature. In recent systematic reviews and meta-analyses comprising overlapping studies, mean sensitivities and specificities for NEN detection varied from 88%–93% and 88%–95%, respectively. 68Ga-DOTA-SSAs is superior to cross-sectional imaging in the detection of bone metastases, that are often subtle. Likewise, lymph node metastases may be characterised, and the detection of small peritoneal metastases is facilitated by 68Ga-DOTA-SSAs (93–96).
Yang et al. in their metanalysis included ten studies comprising 416 patients with NENs. The pooled sensitivity and sensitivity of 68Ga-DOTATOC in the diagnosis of NENs was 93% (95% confidence interval [CI] 89%–96%) and 85% (95% CI 74%–93%), respectively. The pooled sensitivity and specificity of 68Ga-DOTATATE PET in diagnosing NENs was 96% (95% CI 91%–99%) and 100% (95% CI 82%–100%), respectively (93). In a recent retrospective study of patients with pNENs across three tertiary UK NET referral centers 68Ga-DOTA PET/CT was assessed. It was reported that the findings of 68Ga-DOTA PET/CT imaging provided extra information in more than 50% of the studied subjects and had an impact on management decisions in nearly 40% (97). These studies clearly illustrate that 68Ga-DOTA PET/CT significantly upgraded and enhanced our diagnostic armamentarium. The quality of this diagnostic modality was also found to be unaffected by the use of SSAs before the examination, a key advantage. Thus, it is recommended against discontinuing short-acting SSAs before the examination (98).
In contrast to 68Ga-DOTA PET/CT imaging, 18FDG PET/CT is generally better in the context of high-grade disease, indicating likely a more aggressive course. With increasing tumor proliferation, somatostatin receptor expression declines and so does uptake on SRS or 68Gallium-DOTA-SSAs (99, 100). Conversely, these lesions generally become more avid on 18FDG PET/CT with increasing proliferation. Therefore, 18FDG PET/CT is more appropriate for high-grade poorly differentiated G3 tumors, which generally have higher glucose metabolism. 18FDG PET/CT has been reported to be 37%–72% sensitive for the detection of these high-grade tumors. In general, findings of 18FDG-positive tumors at PET/CT are indicative of unfavorable prognosis (87, 101–104).
MEN1 syndrome may be associated with tumors developing in several sites, more frequently in the parathyroids, GEP tract and pituitary gland (8). In fact, 90% of patients with MEN1 develop primary hyperparathyroidism before the age of 50. Parathyroid imaging is of paramount importance in the management of parathyroid disease and its aim is to localise all sites of excess hormone secretion before surgery. The spectrum of parathyroid imaging comprises single-photon scintigraphy with Tc-99m-Sestamibi, or dual tracer Tc-99m-pertechnetate and Tc-99m-sestamibi with or without SPECT or SPECT/CT. Combination of cross-sectional imaging and molecular imaging enables optimisation of our diagnostic potential, and grants the ability to have concrete structural and functional information in a single investigation (105).
Conventional endoscopy is pivotal in detecting and treating NENs in the upper or lower GI tract (106). More recently, the introduction of EUS in clinical practice enhanced out diagnostic potential. Lastly, small bowel capsule endoscopy (SBCE) and balloon enteroscopy have also emerged as novel and helpful techniques.
Upper gastrointestinal endoscopy with careful appraisal of tumors and background gastric mucosa is still the gold standard in diagnosing gastric and duodenal NENs. In the case of gNENs, gastroscopy establishes the diagnosis. It is critical that multiple biopsies are taken from the antrum and gastric body and fundus, in addition to the largest lesions/polyps (107). dNENs are commonly incidentally found during endoscopy for other indications. As the duodenum is within the reach of conventional endoscopy, histological evaluation and staging, and even curative endoscopic treatment are enabled. Gastroscopy with biopsies can accurately diagnose dNEN, whereas EUS can solidify the diagnosis and complete (local) staging, as discussed later. Some dNENs, such as gastrinomas causing ZES, may be missed on both conventional endoscopy and EUS, and these are diagnosed by hormone assays as described in detail in a previous section (108). Although beyond the scope of this review article, it should be noted that endoscopic management also represents the first line treatment for localized type 1 gNENs, followed by active surveillance. This approach ascertains acceptable oncologic outcomes combined with peri-procedural safety. Classic polypectomy, endoscopic mucosal resection (EMR), or endoscopic submucosal dissection (ESD) modalities are used in clinical practice. Any gNEN > 10mm should be considered for endoscopic treatment, unless suspicion or confirmation exists of muscularis propria invasion or lymph node metastasis, when surgical resection should be considered (106).
In analogy to this, most rNENs are diagnosed incidentally during colonoscopy performed for other indications. rNENs are small, usually 10mm lesions, that resemble benign hyperplastic rectal polyps. Commonly, the endoscopist resects the “hyperplastic polyp”, which proves to be a rNEN on histopathology. This emphatically illustrates why endoscopists should be familiarised with the identification of such lesions. It is also important to be able to distinct NENs from other subepithelial lesions, such as lipomas, which usually do not require treatment. Endoscopic biopsies could be misleading as rNENs are submucosal lesions frequently escaping the diagnosis when biopsies with conventional endoscopy are taken. In addition, random biopsies can cause tissue fibrosis, which may challenge subsequent endoscopic resection (109). This underscores why biopsies should not be taken routinely if a rNEN is strongly suspected, and the critical role of EUS is evident.
The role of SBCE in the diagnosis of SBNENs is not yet well established, in contrast to other endoscopic modalities, and consensus guidelines recommend its use upon local expertise (7). At present, it seems that SBCE may be of value in detecting multifocal SBNENs, in particular in the pre-operative setting to determine the extent of resection. Additionally, the use of SBCE could be considered in cases of metastatic disease of unknown origin before laparotomy. Occasionally, the primary site may remain unclear despite thorough investigations (110). On surgical exploration, most such tumors are detected in the small bowel (111). Nevertheless, one should consider that in NENs of unknown primary, SBCE is 75% sensitive, and only 38% specific compared to laparotomy (112). Additionally, in SBCE contractions of the small bowel or extrinsic compression may give the (false) impression of lesions. Likewise, when a true mass is detected, localization may be inaccurate and additional procedures, such as balloon enteroscopy, may be required for confirmations and pathological evaluation.
The diagnostic yield of bowel enteroscopy (BE) for all small bowel masses varies in different studies (113, 114). In individuals with suspected NENs but inconclusive initial investigations, the diagnostic yield is estimated approximately 33% (115). In a recent study, BE was reported to have 88% sensitivity for the detection of the primary SBNEN, compared to approximately 60% for CT, 54% for MRI, and 56% for somatostatin receptor imaging. In this study, 21.2% of the patients had their primary tumors missed on imaging. Notably, 92.3% of those who had BE, had their primary tumor ultimately identified (116). Similar to SBCE, this modality can identify multifocal NENs pre-operatively. In a retrospective study of subjects who had small bowel resection, pre-operative BE was shown to detect additional lesions in over 50% of patients, compared to 18% with capsule endoscopy (117). The mail limitation of BE would be the fact that it is only or primarily available in referral centres. Considering this, the North American (NANETS) guidelines recommend that multifocal tumors may be most accurately identified at the time of surgery, by examining the entire bowel (118). Overall, the use of BE should be reserved only for centers where it is available and relevant expertise exists.
Overall, BE has the advantage of being an invasive modality, enabling the performance of biopsies, among others. In cases of suspected small bowel lesions, SBCE is usually performed first-line, followed by BE in the case of positive findings (119). Sound relevant evidence or guidance lack in the diagnostic cascade of neuroendocrine neoplasms. Where local expertise does exist, and in an appropriate clinical context as outlined above, these two modalities should have a role, and we believe this is complementary, similar to other small bowel lesions.
The advent of EUS revolutionised the field. In particular, it enables detection of previously unidentified tumors; contributes to staging of GEP-NETS, and finally permits tissue diagnosis and histological evaluation.
In particular, it seems that EUS is the most sensitive method for pNENs, being 82%–93% sensitive and 86%–95% specific in this context (120–122). In a series of studies involving more than 200 patients, the detection rate of EUS was ranging from 75 to 97% (55, 99, 100, 123–128). Notably, in a recent review by Ishi et al., tumor grading between EUS-FNA and surgical samples showed a concordance rate of 77.5% (95% CI = 0.59–0.71, p < 0.01). (129). Likewise, intraoperative US (IOUS) was also shown to sensitive for pNEN, having a detection rate of 74 to 96% (99, 130–132).
For dNENs and lymph node metastases, the detection rate of EUS was 63% in 2 studies comprising 59 patients (99, 126). Forceps biopsy during standard endoscopic examination can diagnose most dNENs, and not uncommonly, endoscopy can offer a curative option for small sporadic dNENs. Nevertheless, for larger tumors over 1 cm, local staging by EUS is recommended before resection. Duodenal NENs are typically submucosal lesions, but they can rarely extend beyond this layer. EUS can accurately establish the degree of submucosal involvement. EUS can accurately assess locoregional lymph node metastases, and this is of particular importance as dNENs can be associated with such metastases in up to 40%–60%, especially gastrinomas. All the above are critical to determine optimal treatment, and candidacy for endoscopic or surgical treatment. Lastly, the pancreas can also be fully interrogated for small tumors, that can be linked to MEN-1 (133–135).
Lastly, gNENs can be classified into three subtypes: type 1 g-NETs which are the most frequent and develop due to hypergastrinaemia in the context of autoimmune atrophic gastritis; type 2 that are linked to increased gastric secretion, in the context of gastrin-secreting tumors, often in patients with MEN-1 and as part of a ZES; lastly, type 3 tumors are sporadic and usually poorly differentiated, mimicking malignant neoplasms of the stomach (136). EUS is recommended for type 1 gNENs > 1 cm prior to endoscopic resection. Similarly, for patients suspected to have type 2 neoplasms, this modality assesses for the presence of dNENs or pNENs. Lastly, for the assessment of type 3 gNENs, EUS evaluates the depth of invasion into the mucosal layers or beyond, and the presence of lymph nodes in the gastro-hepatic and peri-gastric areas (137).
Regarding the role of EUS in the management of rNENs, according to the current ENETS consensus, EUS should follow endoscopic evaluation of a suspected rNEN (138). EUS can accurately assess tumor size, depth of invasion and locoregional lymph node metastases. This can be of paramount importance when determining surgical candidates, and can assist in determining appropriate treatment (109, 139).
Most of the aforementioned biomarkers, widely used to date, fail to capture the biologic complexity of a NEN; and even the historical Ki67 appears to have some limitations. There is an emerging need to embrace advances in the field and integrate molecular genomic tools into clinical practice. The argument is that contrary to the current biomarkers, multianalyte analysis assess the tumor molecular genomic mechanism. Multianalyte biomarkers include tumor-derived components such as ctDNA, circulating tumor cells (CTCs), miRNA, extracellular vesicles, and “tumor-educated” platelets (140). Key novel biomarkers are summarised in Table 4.
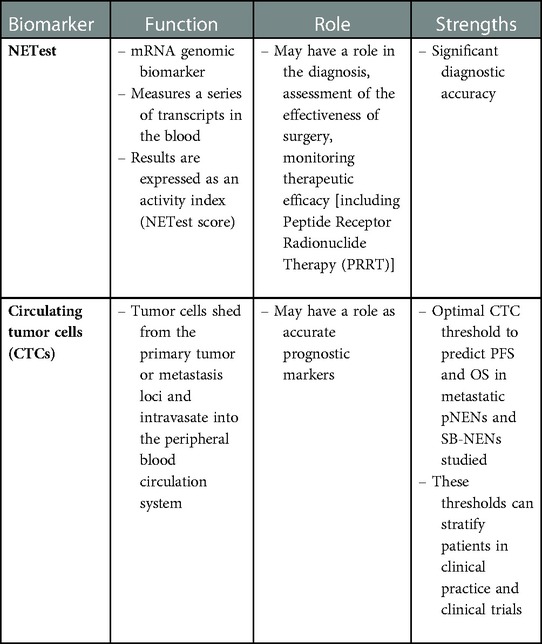
Table 4. Novel biomarkers for the diagnosis of neuroendocrine neoplasms (NENs).
The NETest is the most successful multianalyte biomarker assessed to date in the management of NENs. This mRNA genomic biomarker measures a series of relevant transcripts in the blood, which is considered the biological signature of the neoplasm. It is considered a liquid biopsy procedure, assessing the circulating expression level of genes involved in oncogenesis, cell proliferation, signalling and metastasis formation through a peripheral blood real-time polymerase chain reaction (RT-PCR). The respective results are expressed as an activity index (NETest score), ranging between 0 and 100. A score ranging from 21 to 40% represents “stable” disease, whereas a score > 40% reflects “progressive” disease (140). Oberg et al. in their recent meta-analysis reported that the diagnostic accuracy of this tests is approximately 96%. The diagnostic accuracy of this test to differentiate between stable and progressive disease was reported to be between 84.5% and 85.5%. The NETest was 91.5%–97.8% accurate as a marker of natural history and 93.7%–97.4% accurate as an interventional/response biomarker (141).
PRRT is a very effective treatment modality for patients with metastatic and/or inoperable NENs. A radionuclide linked to a SSA is used, and this allows to accurately deliver radiotherapy to somatostatin receptor–expressing neoplasms, such as the great majority of NENs (142). Bodei et al. prospectively evaluated NETest as a surrogate biomarker for Response Evaluation Criteria in Solid Tumors (RECIST). Notably, in over a hundred subjects assessed, NETest significantly decreased in patients who responded to treatment, as per RECIST criteria, and remained elevated in those who did not “respond” to PRRT. Notably, the reported accuracy of treatment response was 98% (143). Similar to the NETest, NEN transcript expression in blood integrated with tumor grade provides a PRRT predictive quotient (PPQ) which also stratifies patients who “respond” to PRRT from those who do not. PPQ response prediction was accurate in 97% with a 99% accurate positive and 93% accurate negative prediction. NETest significantly decreased in PPQ-predicted “responders” and remained elevated or even further increased in PPQ-predicted patients who did not respond to treatment. Interestingly, CgA did not correlate that well with the outcome of PRRT, decreasing in only 38% of treatment “responders” (143).
CTC measurement has also been assessed in several malignancies. In particular, the CellSearch platform was approved by the US Food and Drug Administration for use in several malignancies, after trials reported the prognostic value of CTCs at defined thresholds (144–146). Although CTCs are also detectable in patients with NENs, studies on the measurement of CTCs in the diagnosis of NENs are not equally enthusiastic (140). On the contrary, CTCs appear more accurate as prognostic markers (147, 148). Interestingly, Mandair et al. defined optimal prognostic CTC thresholds in pNENs and midgut NENs. They used CellSearch to enumerate CTCs in almost 200 subjects with metastatic NENs, as above. These subjects were then followed-up for at least 3 years or until death. CTCs were detected in 33% of patients with pNEN and 51% of midgut NENs. In the multivariate Cox hazard regression analysis for progression free survival (PFS) in subjects with pNEN, 1 or greater CTC had a hazard ratio (HR) of 2.6, whereas 2 or greater CTCs had an HR of 2.25 in midgut NENs. In the multivariate Cox hazard regression analysis for overall survival (OS) in pNEN, 1 or greater CTCs had an HR of 3.16 and in midgut NENs, 2 or greater CTCs had an HR of 1.73 (149).
The quantitative analysis of medical images data and the extraction of imaging features, also called “radiomics”, represent an emerging approach in personalized medicine and advanced diagnostics, especially for disease characterization or outcome prediction. Similar to other neoplasia, this appears to be a promising tool in the context of NENs. A recent study by Mori et al. evaluated preoperative CT radiomic features as a predictor of tumor grade, the presence of lymph nodes metastases or distant metastases, and microvascular invasion of pNENs. This retrospective study included over 100 patients who underwent surgery for pNEN. They showed that combining few radiomic and clinic-radiological features resulted in presurgical prediction of histological characteristics of pNENs (150). In a different study by Chiti et al., the authors assessed whether CT scan radiomics analysis could predict GEP-NEN grade according to the recent WHO classification; they also concluded that CT-radiomics analysis may contribute to differentiating the histological grade for these tumors (151). Although these studies, among others, illustrate that radiomics may be an invaluable tool in the future, further studies will be required to validate the results.
Insulinomas are rare functional pNENs that secrete insulin arbitrarily, as already discussed. Surgery remains the preferred treatment modality, whenever possible, being linked to cure rate exceeding 98% (152–157). Surgical treatment of insulinomas may be challenged due to difficulties in localizing it using conventional diagnostic modalities, however. In <5%–10% of such individuals, investigations can be negative and non-conclusive (8). Even highly sophisticated and advanced 68Gallium-DOTA-SSAs are positive in less than 30% (158). Conversely, insulinomas exhibit a very high density of glucagon-like peptide-1 receptors (GLP-1R). As a result, receptor scintigraphy with radiolabelled GLP-1 receptor analogues is a very promising modality, albeit hampered by its limited availability so far (159–162). In one of the first relevant studies, Christ et al. tested the 111In-labeled GLP-1R agonist 111In-DOTA-exendin-4 in localizing insulinomas. They found that the GLP-1R scans successfully detected the insulinomas and contributed to the successful surgical resection of insulinomas in all subjects (162).
Recent studies explored whether combining 68Gallium-DOTA-SSAs and 18F-FDG PET/CT would enhance our ability to determine prognosis. A recent study by Hayes et al. investigated the prognostic utility of a classification system combining the findings of 68Ga-DOTATATE and 18F-FDG PET/CT and the researchers reported that such a classification tool could indeed correlate with prognosis (163). In addition, Panagiotidis et al. investigated whether 68Ga-DOTATATE and 18F-FDG PET/CT could influence treatment decisions. The results changed the therapeutic plan in 80.8% of patients. In approximately 21%, 18F-FDG PET/CT affected the decision-making, prompting mostly the initiation of chemotherapy. In nearly 50% the treatment cascade was influenced by 68Ga-DOTATATE, resulting in consideration of PRRT (164). More recently, a multicentre study assessed and aimed to validate the NETPET score as a prognostic biomarker in metastatic GEP-NENs. The combination of 68Gallium-DOTA-SSAs and 18F-FDG PET/CT, i.e., “dual PET imaging”, provides a comprehensive overview of the status of the disease. The NETPET score, a 5-point scoring system for dual PET reporting in subjects with metastatic NENs, summarises the information provided by the two modalities into a single parameter. The NETPET score correlated with histological grade (p < 0.001), and importantly it was significantly associated with overall survival and time to progression on univariate and multivariate analysis (p < 0.01) (165).
The advent of pre-clinical models appears to be promising for the design, assessment and evolution of genuinely tailored personalised treatment. In particular, primary culture cells originating from solid neoplasms, have gained significant importance in individualised anti-cancer treatment. In analogy to this, patient-derived xenografts (PDXs) in mice represent an in vivo model for the development of individualised precision medicine. To produce PDXs, tumors collected following surgical resection or biopsy, are inoculated as pieces or single-cell suspensions subcutaneously usually into the flank of an animal model (166). More recently, zebrafish PDX (zPDX) emerged as a promising option (167). In the former case, the main advantage is the potential to assess the efficacy of different anti-tumor treatment options in a short time, and also to perform preliminary pre-clinical studies for the identification of novel molecular targets (168, 169). In the latter case, it is anticipated that the effects of antitumor compounds on tumor-induced angiogenesis, invasiveness, metastatic dissemination and tumor cell proliferation can be assessed within very few days after implantation.
Although some of the novel revolutionary techniques presented in the current review are currently in the developmental pipeline, it is surely an insight into the future and illustrate the major paradigm shift currently taking place in medical oncology. Accurate and early diagnosis is critical, whereas there has been some progress, and we definitely believe that the research focus should be in establishing robust prognosticators and prognostic scores.
It is evident that NENs are complex and heterogeneous tumors, and as such require a sophisticated diagnostic approach. This is critical, as early and accurate diagnosis and staging largely influence prognosis and patient outcomes. Pathology still represents and will likely remain the gold standard in the foreseeable future. Likewise, cross-sectional imaging is still the backbone in the diagnosis and staging of these tumors, and in addition, the advances in CT and MRI have also improved the diagnostic yield. Nevertheless, the genuine revolution in the field follows the advances in nuclear medicine, and the emergence of novel biomarkers assessing the tumor molecular genomic mechanisms. The former, comprising 68Ga-DOTA PET/CT exhibits unprecedented diagnostic accuracy, and has been shown to influence and update management in a significant number of patients (97, 164), limited primarily by its high-cost and consequent limited availability. Likewise, multianalyte biomarkers appear promising tools also leading to new horizons. The NETest in particular provides accurate information about the diagnosis, completeness of surgical resection and the presence of residual disease in patients with NENs; it can also predict the therapeutic efficacy of SSAs and PRRT; and lastly it is standardized, reproducible and not influenced by age, gender, ethnicity, fasting or other medications (141, 170, 171). It is evident that we do live in exciting times. Our deeper understanding of these rare neoplasms, the progress already made in the diagnosis and treatment of NENs, and finally these new promising developments, all bring us one step closer to tailored treatment and improved outcomes.
AK, AG, AP, PB, DG, VNP, CT: conception and design; AK, AK, AP: article draft; AK, AG, AP, PB, DG, VNP, CT: critical revision for important intellectual content, final approval of the article. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ameri P, Ferone D. Diffuse endocrine system, neuroendocrine tumors and immunity: what's New? Neuroendocrinology. (2012) 95:267–76. doi: 10.1159/000334612
2. Lawrence B, Gustafsson BI, Chan A, Svejda B, Kidd M, Modlin IM. The epidemiology of gastroenteropancreatic neuroendocrine tumors. Endocrinol Metab Clin North Am. (2011) 40:1–18. vii. doi: 10.1016/j.ecl.2010.12.005
3. Fraenkel M, Kim M, Faggiano A, de Herder WW, Valk GD. Knowledge NETwork. Incidence of gastroenteropancreatic neuroendocrine tumours: a systematic review of the literature. Endocr Relat Cancer. (2014) 21:R153–63. doi: 10.1530/ERC-13-0125
4. Dasari A, Shen C, Halperin D, Zhao B, Zhou S, Xu Y, et al. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. (2017) 3:1335–42. doi: 10.1001/jamaoncol.2017.0589
5. O’Toole D, Kianmanesh R, Caplin M. ENETS 2016 Consensus guidelines for the management of patients with digestive neuroendocrine tumors: an update. Neuroendocrinology. (2016) 103:117–8. doi: 10.1159/000443169
6. Pape U-F, Perren A, Niederle B, Gross D, Gress T, Costa F, et al. ENETS Consensus guidelines for the management of patients with neuroendocrine neoplasms from the jejuno-ileum and the appendix including goblet cell carcinomas. Neuroendocrinology. (2012) 95:135–56. doi: 10.1159/000335629
7. Niederle B, Pape U-F, Costa F, Gross D, Kelestimur F, Knigge U, et al. ENETS Consensus guidelines update for neuroendocrine neoplasms of the Jejunum and ileum. Neuroendocrinology. (2016) 103:125–38. doi: 10.1159/000443170
8. Falconi M, Eriksson B, Kaltsas G, Bartsch DK, Capdevila J, Caplin M, et al. ENETS Consensus guidelines update for the management of patients with functional pancreatic neuroendocrine tumors and non-functional pancreatic neuroendocrine tumors. Neuroendocrinology. (2016) 103:153–71. doi: 10.1159/000443171
9. Herrera-Martínez AD, Hofland J, Hofland LJ, Brabander T, Eskens FALM, Gálvez Moreno MA, et al. Targeted systemic treatment of neuroendocrine tumors: current options and future perspectives. Drugs. (2019) 79:21–42. doi: 10.1007/s40265-018-1033-0
10. Gorelik M, Ahmad M, Grossman D, Grossman M, Cooperman AM. Nonfunctioning incidental pancreatic neuroendocrine tumors. Surg Clin North Am. (2018) 98:157–67. doi: 10.1016/j.suc.2017.09.014
11. Alabraba E, Pritchard DM, Griffin R, Diaz-Nieto R, Banks M, Cuthbertson DJ, et al. The impact of lymph node metastases and right hemicolectomy on outcomes in appendiceal neuroendocrine tumours (aNETs). Eur J Surg Oncol. (2021) 47:1332–8. doi: 10.1016/j.ejso.2020.09.012
12. Perren A, Couvelard A, Scoazec J-Y, Costa F, Borbath I, Delle Fave G, et al. ENETS Consensus guidelines for the standards of care in neuroendocrine tumors: pathology: diagnosis and prognostic stratification. Neuroendocrinology. (2017) 105:196–200. doi: 10.1159/000457956
13. Vinayek R, Capurso G, Larghi A. Grading of EUS-FNA cytologic specimens from patients with pancreatic neuroendocrine neoplasms: it is time move to tissue core biopsy? Gland Surg. (2014) 3:222–5. doi: 10.3978/j.issn.2227-684X.2014.07.03
14. Larghi A, Capurso G, Carnuccio A, Ricci R, Alfieri S, Galasso D, et al. Ki-67 grading of nonfunctioning pancreatic neuroendocrine tumors on histologic samples obtained by EUS-guided fine-needle tissue acquisition: a prospective study. Gastrointest Endosc. (2012) 76:570–7. doi: 10.1016/j.gie.2012.04.477
15. Weynand B, Borbath I, Bernard V, Sempoux C, Gigot J-F, Hubert C, et al. Pancreatic neuroendocrine tumour grading on endoscopic ultrasound-guided fine needle aspiration: high reproducibility and inter-observer agreement of the ki-67 labelling index. Cytopathology. (2014) 25:389–95. doi: 10.1111/cyt.12111
16. Eusebi LH, Thorburn D, Toumpanakis C, Frazzoni L, Johnson G, Vessal S, et al. Endoscopic ultrasound-guided fine-needle aspiration vs fine-needle biopsy for the diagnosis of pancreatic neuroendocrine tumors. Endosc Int Open. (2019) 07:E1393–9. doi: 10.1055/a-0967-4684
17. Lloyd RV. Practical markers used in the diagnosis of neuroendocrine tumors. Endocr Pathol. (2003) 14:293–301. doi: 10.1385/ep:14:4:293
18. Rindi G, Petrone G, Inzani F. The 2010 WHO classification of digestive neuroendocrine neoplasms: a critical appraisal four years after its introduction. Endocr Pathol. (2014) 25:186–92. doi: 10.1007/s12022-014-9313-z
19. Lloyd R, Osamura R, Kloppel G. World health organization, international agency for research on cancer. WHO Classification of tumours of endocrine organs, ed 4. Geneva, World Health Organization. (2017).
20. Tang LH, Basturk O, Sue JJ, Klimstra DS. A practical approach to the classification of WHO grade 3 (G3) well-differentiated neuroendocrine tumor (WD-NET) and poorly differentiated neuroendocrine carcinoma (PD-NEC) of the pancreas. Am J Surg Pathol. (2016) 40:1192–202. doi: 10.1097/PAS.0000000000000662
21. Klöppel G, Klimstra D, Hruban R. Pancreatic neuroendocrine tumors: update on the new world health organization classification. AJSP Rev Rep. (2017) 22:233–9.
22. Kruljac I, Pape U. The classification of neuroendocrine neoplasms: “neuroendocrine carcinomas” revisited – a 2017 update and future perspectives. Endocr Oncol Metab. (2017) 3:37–42. doi: 10.21040/eom/2017.3.1.2
23. Rindi G, Klöppel G, Couvelard A, Komminoth P, Körner M, Lopes JM, et al. TNM Staging of midgut and hindgut (neuro) endocrine tumors: a consensus proposal including a grading system. Virchows Arch. (2007) 451:757–62. doi: 10.1007/s00428-007-0452-1
24. Rindi G, Klöppel G, Alhman H, Caplin M, Couvelard A, de Herder WW, et al. TNM Staging of foregut (neuro)endocrine tumors: a consensus proposal including a grading system. Virchows Arch. (2006) 449:395–401. doi: 10.1007/s00428-006-0250-1
25. Rindi G, Falconi M, Klersy C, Albarello L, Boninsegna L, Buchler MW, et al. TNM Staging of neoplasms of the endocrine pancreas: results from a large international cohort study. J Natl Cancer Inst. (2012) 104:764–77. doi: 10.1093/jnci/djs208
26. Rindi G, Mete O, Uccella S, Basturk O, la Rosa S, Brosens LAA, et al. Overview of the 2022 WHO classification of neuroendocrine neoplasms. Endocr Pathol. (2022) 33:115–54. doi: 10.1007/s12022-022-09708-2
27. Sorbye H, Welin S, Langer SW, Vestermark LW, Holt N, Osterlund P, et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): the NORDIC NEC study. Ann Oncol. (2013) 24:152–60. doi: 10.1093/annonc/mds276
28. Oberg K, Couvelard A, Delle Fave G, Gross D, Grossman A, Jensen RT, et al. ENETS Consensus guidelines for standard of care in neuroendocrine tumours: biochemical markers. Neuroendocrinology. (2017) 105:201–11. doi: 10.1159/000472254
29. Malczewska A, Kidd M, Matar S, Kos-Kudła B, Bodei L, Oberg K, et al. An assessment of circulating chromogranin A as a biomarker of bronchopulmonary neuroendocrine neoplasia: a systematic review and meta-analysis. Neuroendocrinology. (2020) 110:198–216. doi: 10.1159/000500525
30. Sanduleanu S, de Bruïne A, Stridsberg M, Jonkers D, Biemond I, Hameeteman W, et al. Serum chromogranin A as a screening test for gastric enterochromaffin-like cell hyperplasia during acid-suppressive therapy. Eur J Clin Invest. (2001) 31:802–11. doi: 10.1046/j.1365-2362.2001.00890.x
31. Sobol RE, Memoli V, Deftos LJ. Hormone-negative, chromogranin A-positive endocrine tumors. N Engl J Med. (1989) 320:444–7. doi: 10.1056/NEJM198902163200707
32. O’Connor DT, Pandlan MR, Carlton E, Cervenka JH, Hslao RJ. Rapid radioimmunoassay of circulating chromogranin A: in vitro stability, exploration of the neuroendocrine character of neoplasia, and assessment of the effects of organ failure. Clin Chem. (1989) 35:1631–7. doi: 10.1093/clinchem/35.8.1631
33. Eriksson B, Arnberg H, Oberg K, Hellman U, Lundqvist G, Wernstedt C, et al. A polyclonal antiserum against chromogranin A and B--a new sensitive marker for neuroendocrine tumours. Acta Endocrinol (Copenh). (1990) 122:145–55. doi: 10.1530/acta.0.1220145
34. Zatelli MC, Torta M, Leon A, Ambrosio MR, Gion M, Tomassetti P, et al. Chromogranin A as a marker of neuroendocrine neoplasia: an Italian multicenter study. Endocr Relat Cancer. (2007) 14:473–82. doi: 10.1677/ERC-07-0001
35. Turner NC, Strauss SJ, Sarker D, Gillmore R, Kirkwood A, Hackshaw A, et al. Chemotherapy with 5-fluorouracil, cisplatin and streptozocin for neuroendocrine tumours. Br J Cancer. (2010) 102:1106–12. doi: 10.1038/sj.bjc.6605618
36. Bergestuen DS, Aabakken L, Holm K, Vatn M, Thiis-Evensen E. Small intestinal neuroendocrine tumors: prognostic factors and survival. Scand J Gastroenterol. (2009) 44:1084–91. doi: 10.1080/00365520903082432
37. Meijer WG, Kema IP, Volmer M, Willemse PH, de Vries EG. Discriminating capacity of indole markers in the diagnosis of carcinoid tumors. Clin Chem. (2000) 46:1588–96. doi: 10.1093/clinchem/46.10.1588
38. Janson ET, Holmberg L, Stridsberg M, Eriksson B, Theodorsson E, Wilander E, et al. Carcinoid tumors: analysis of prognostic factors and survival in 301 patients from a referral center. Ann Oncol. (1997) 8:685–90. doi: 10.1023/a:1008215730767
39. Bhattacharyya S, Toumpanakis C, Chilkunda D, Caplin ME, Davar J. Risk factors for the development and progression of carcinoid heart disease. Am J Cardiol. (2011) 107:1221–6. doi: 10.1016/j.amjcard.2010.12.025
40. Koffas A, Toumpanakis C. Managing carcinoid heart disease in patients with neuroendocrine tumors. Ann Endocrinol (Paris). (2021) 82:187–92. doi: 10.1016/j.ando.2020.12.007
41. Bhattacharyya S, Toumpanakis C, Caplin ME, Davar J. Usefulness of N-terminal pro–brain natriuretic peptide as a biomarker of the presence of carcinoid heart disease. Am J Cardiol. (2008) 102:938–42. doi: 10.1016/j.amjcard.2008.05.047
42. Jensen RT, Cadiot G, Brandi ML, de Herder WW, Kaltsas G, Komminoth P, et al. ENETS Consensus guidelines for the management of patients with digestive neuroendocrine neoplasms: functional pancreatic endocrine tumor syndromes. Neuroendocrinology. (2012) 95:98–119. doi: 10.1159/000335591
43. Berna MJ, Hoffmann KM, Serrano J, Gibril F, Jensen RT. Serum gastrin in zollinger-ellison syndrome: i. Prospective study of fasting serum gastrin in 309 patients from the national institutes of health and comparison with 2229 cases from the literature. Med (Baltimore). (2006) 85:295–330. doi: 10.1097/01.md.0000236956.74128.76
44. Bradley EL, Galambos JT. Diagnosis of gastrinoma by the secretin suppression test. Surg Gynecol Obstet. (1976) 143:784–8.982259
45. Cryer PE, Axelrod L, Grossman AB, Heller SR, Montori VM, Seaquist ER, et al. Evaluation and management of adult hypoglycemic disorders: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. (2009) 94:709–28. doi: 10.1210/jc.2008-1410
46. Ito T, Igarashi H, Uehara H, Berna MJ, Jensen RT. Causes of death and prognostic factors in multiple endocrine neoplasia type 1: a prospective study: comparison of 106 MEN1/zollinger-ellison syndrome patients with 1613 literature MEN1 patients with or without pancreatic endocrine tumors. Medicine (Baltimore). (2013) 92:135–81. doi: 10.1097/MD.0b013e3182954af1
47. Yamazaki M, Suzuki S, Kosugi S, Okamoto T, Uchino S, Miya A, et al. Delay in the diagnosis of multiple endocrine neoplasia type 1: typical symptoms are frequently overlooked. Endocr J. (2012) 59:797–807. doi: 10.1507/endocrj.ej12-0071
48. Sundin A, Arnold R, Baudin E, Cwikla JB, Eriksson B, Fanti S, et al. ENETS Consensus guidelines for the standards of care in neuroendocrine tumors: radiological, nuclear medicine and hybrid imaging. Neuroendocrinology. (2017) 105:212–44. doi: 10.1159/000471879
49. Koopmans KP, de Vries EGE, Kema IP, Elsinga PH, Neels OC, Sluiter WJ, et al. Staging of carcinoid tumours with 18F-DOPA PET: a prospective, diagnostic accuracy study. Lancet Oncol. (2006) 7:728–34. doi: 10.1016/S1470-2045(06)70801-4
50. Ruf J, Schiefer J, Furth C, Kosiek O, Kropf S, Heuck F, et al. 68Ga-DOTATOC PET/CT of neuroendocrine tumors: spotlight on the CT phases of a triple-phase protocol. J Nucl Med. (2011) 52:697–704. doi: 10.2967/jnumed.110.083741
51. Veit-Haibach P, Schiesser M, Soyka J, Strobel K, Schaefer NG, Hesselmann R, et al. Clinical value of a combined multi-phase contrast enhanced DOPA-PET/CT in neuroendocrine tumours with emphasis on the diagnostic CT component. Eur Radiol. (2011) 21:256–64. doi: 10.1007/s00330-010-1930-4
52. Gabriel M, Decristoforo C, Kendler D, Dobrozemsky G, Heute D, Uprimny C, et al. 68Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: comparison with somatostatin receptor scintigraphy and CT. J Nucl Med. (2007) 48:508–18. doi: 10.2967/jnumed.106.035667
53. Fidler JL, Fletcher JG, Reading CC, Andrews JC, Thompson GB, Grant CS, et al. Preoperative detection of pancreatic insulinomas on multiphasic helical CT. AJR Am J Roentgenol. (2003) 181:775–80. doi: 10.2214/ajr.181.3.1810775
54. Ichikawa T, Peterson MS, Federle MP, Baron RL, Haradome H, Kawamori Y, et al. Islet cell tumor of the pancreas: biphasic CT versus MR imaging in tumor detection. Radiology. (2000) 216:163–71. doi: 10.1148/radiology.216.1.r00jl26163
55. Gouya H, Vignaux O, Augui J, Dousset B, Palazzo L, Louvel A, et al. CT, endoscopic sonography, and a combined protocol for preoperative evaluation of pancreatic insulinomas. AJR Am J Roentgenol. (2003) 181:987–92. doi: 10.2214/ajr.181.4.1810987
56. Procacci C, Carbognin G, Accordini S, Biasiutti C, Bicego E, Romano L, et al. Nonfunctioning endocrine tumors of the pancreas: possibilities of spiral CT characterization. Eur Radiol. (2001) 11:1175–83. doi: 10.1007/s003300000714
57. Johanssen S, Boivin M, Lochs H, Voderholzer W. The yield of wireless capsule endoscopy in the detection of neuroendocrine tumors in comparison with CT enteroclysis. Gastrointest Endosc. (2006) 63:660–5. doi: 10.1016/j.gie.2005.11.055
58. Pilleul F, Penigaud M, Milot L, Saurin J-C, Chayvialle J-A, Valette P-J. Possible small-bowel neoplasms: contrast-enhanced and water-enhanced multidetector CT enteroclysis. Radiology. (2006) 241:796–801. doi: 10.1148/radiol.2413051429
59. Kamaoui I, De-Luca V, Ficarelli S, Mennesson N, Lombard-Bohas C, Pilleul F. Value of CT enteroclysis in suspected small-bowel carcinoid tumors. AJR Am J Roentgenol. (2010) 194:629–33. doi: 10.2214/AJR.09.2760
60. Paulsen SR, Huprich JE, Fletcher JG, Booya F, Young BM, Fidler JL, Johnson CD, Barlow JM, Earnest F. CT Enterography as a diagnostic tool in evaluating small bowel disorders: review of clinical experience with over 700 cases. Radiographics. (2006) 26:641–57; discussion 657-62. doi: 10.1148/rg.263055162
61. Chiti A, Fanti S, Savelli G, Romeo A, Bellanova B, Rodari M, et al. Comparison of somatostatin receptor imaging, computed tomography and ultrasound in the clinical management of neuroendocrine gastro-entero-pancreatic tumours. Eur J Nucl Med. (1998) 25:1396–403. doi: 10.1007/s002590050314
62. Dahdaleh FS, Lorenzen A, Rajput M, Carr JC, Liao J, Menda Y, et al. The value of preoperative imaging in small bowel neuroendocrine tumors. Ann Surg Oncol. (2013) 20:1912–7. doi: 10.1245/s10434-012-2836-y
63. Kumbasar B, Kamel IR, Tekes A, Eng J, Fishman EK, Wahl RL. Imaging of neuroendocrine tumors: accuracy of helical CT versus SRS. Abdom Imaging. (2004) 29:696–702. doi: 10.1007/s00261-003-0162-3
64. Hubalewska-Dydejczyk A, Fröss-Baron K, Mikołajczak R, Maecke HR, Huszno B, Pach D, et al. 99mTc-EDDA/HYNIC-octreotate Scintigraphy, an efficient method for the detection and staging of carcinoid tumours: results of 3 years’ experience. Eur J Nucl Med Mol Imaging. (2006) 33:1123–33. doi: 10.1007/s00259-006-0113-7
65. Hofland J, Kaltsas G, de Herder WW. Advances in the diagnosis and management of well-differentiated neuroendocrine neoplasms. Endocr Rev. (2020) 41:371–403. doi: 10.1210/endrev/bnz004
66. Pavel M, Öberg K, Falconi M, Krenning EP, Sundin A, Perren A, et al. Gastroenteropancreatic neuroendocrine neoplasms: eSMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2020) 31:844–60. doi: 10.1016/j.annonc.2020.03.304
67. Putzer D, Gabriel M, Henninger B, Kendler D, Uprimny C, Dobrozemsky G, et al. Bone metastases in patients with neuroendocrine tumor: 68 ga-DOTA-tyr 3 -octreotide PET in comparison to CT and bone scintigraphy. J Nucl Med. (2009) 50:1214–21. doi: 10.2967/jnumed.108.060236
68. Baumann T, Rottenburger C, Nicolas G, Wild D. Gastroenteropancreatic neuroendocrine tumours (GEP-NET)–imaging and staging. Best Pract Res Clin Endocrinol Metab. (2016) 30:45–57. doi: 10.1016/j.beem.2016.01.003
69. Lee L, Ito T, Jensen RT. Imaging of pancreatic neuroendocrine tumors: recent advances, current status, and controversies. Expert Rev Anticancer Ther. (2018) 18:837–60. doi: 10.1080/14737140.2018.1496822
70. Howe JR, Merchant NB, Conrad C, Keutgen XM, Hallet J, Drebin JA, et al. The North American neuroendocrine tumor society consensus paper on the surgical management of pancreatic neuroendocrine tumors. Pancreas. (2020) 49:1–33. doi: 10.1097/MPA.0000000000001454
71. Farchione A, Rufini V, Brizi MG, Iacovazzo D, Larghi A, Massara RM, et al. Evaluation of the added value of diffusion-weighted imaging to conventional magnetic resonance imaging in pancreatic neuroendocrine tumors and comparison with 68Ga-DOTANOC positron emission tomography/computed tomography. Pancreas. (2016) 45:345–54. doi: 10.1097/MPA.0000000000000461
72. Etchebehere ECS de C, Santos A dO, Gumz B, Vicente A, Hoff PG, Corradi G, et al. 68Ga-DOTATATE PET/CT, 99mTc-HYNIC-octreotide SPECT/CT, and whole-body MR imaging in detection of neuroendocrine tumors: a prospective trial. J Nucl Med. (2014) 55:1598–604. doi: 10.2967/jnumed.114.144543
73. d’Assignies G, Fina P, Bruno O, Vullierme M-P, Tubach F, Paradis V, et al. High sensitivity of diffusion-weighted MR imaging for the detection of liver metastases from neuroendocrine tumors: comparison with T2-weighted and dynamic gadolinium-enhanced MR imaging. Radiology. (2013) 268:390–9. doi: 10.1148/radiol.13121628
74. Lo GC, Kambadakone A. MR Imaging of pancreatic neuroendocrine tumors. Magn Reson Imaging Clin N Am. (2018) 26:391–403. doi: 10.1016/j.mric.2018.03.010
75. Dromain C, de Baere T, Lumbroso J, Caillet H, Laplanche A, Boige V, et al. Detection of liver metastases from endocrine tumors: a prospective comparison of somatostatin receptor scintigraphy, computed tomography, and magnetic resonance imaging. J Clin Oncol. (2005) 23:70–8. doi: 10.1200/JCO.2005.01.013
76. Dohan A, el Fattach H, Barat M, Guerrache Y, Eveno C, Dautry R, et al. Neuroendocrine tumors of the small bowel: evaluation with MR-enterography. Clin Imaging. (2016) 40:541–7. doi: 10.1016/j.clinimag.2015.12.016
77. Grozinsky-Glasberg S, Davar J, Hofland J, Dobson R, Prasad V, Pascher A, et al. European Neuroendocrine tumor society (ENETS) 2022 guidance paper for carcinoid syndrome and carcinoid heart disease. J Neuroendocrinol. (2022) 34:e13146. doi: 10.1111/jne.13146
78. Rajiah P, Kanne JP, Kalahasti V, Schoenhagen P. Computed tomography of cardiac and pericardiac masses. J Cardiovasc Comput Tomogr. (2011) 5:16–29. doi: 10.1016/j.jcct.2010.08.009
79. Guo Y, Gao H, Zhang X, Wang Q, Yang Z, Ma E. Accuracy and reproducibility of assessing right ventricular function with 64-section multi-detector row CT: comparison with magnetic resonance imaging. Int J Cardiol. (2010) 139:254–62. doi: 10.1016/j.ijcard.2008.10.031
80. Frilling A, Sotiropoulos GC, Radtke A, Malago M, Bockisch A, Kuehl H, et al. The impact of 68Ga-DOTATOC positron emission tomography/computed tomography on the multimodal management of patients with neuroendocrine tumors. Ann Surg. (2010) 252:850–6. doi: 10.1097/SLA.0b013e3181fd37e8
81. Reubi JC. Regulatory peptide receptors as molecular targets for cancer diagnosis and therapy. Q J Nucl Med. (1997) 41:63–70. doi: 10.1210/er.2002-0007
82. Panagiotidis E, Bomanji J. Role of 18F-fluorodeoxyglucose PET in the study of neuroendocrine tumors. PET Clin. (2014) 9:43–55. doi: 10.1016/j.cpet.2013.08.008
83. Ramage JK, Ahmed A, Ardill J, Bax N, Breen DJ, Caplin ME, et al. Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs). Gut. (2012) 61:6–32. doi: 10.1136/gutjnl-2011-300831
84. Pettinato C, Sarnelli A, di Donna M, Civollani S, Nanni C, Montini G, et al. 68Ga-DOTANOC: biodistribution and dosimetry in patients affected by neuroendocrine tumors. Eur J Nucl Med Mol Imaging. (2008) 35:72–9. doi: 10.1007/s00259-007-0587-y
85. Shastry M, Kayani I, Wild D, Caplin M, Visvikis D, Gacinovic S, et al. Distribution pattern of 68Ga-DOTATATE in disease-free patients. Nucl Med Commun. (2010) 31:1025–32. doi: 10.1097/MNM.0b013e32833f635e
86. Kowalski J, Henze M, Schuhmacher J, Mäcke HR, Hofmann M, Haberkorn U. Evaluation of positron emission tomography imaging using [68Ga]-DOTA-D phe(1)-tyr(3)-octreotide in comparison to [111In]-DTPAOC SPECT. First results in patients with neuroendocrine tumors. Mol Imaging Biol. (2003) 5:42–8. doi: 10.1016/s1536-1632(03)00038-6
87. Binderup T, Knigge U, Loft A, Federspiel B, Kjaer A. 18F-fluorodeoxyglucose Positron emission tomography predicts survival of patients with neuroendocrine tumors. Clin Cancer Res. (2010) 16:978–85. doi: 10.1158/1078-0432.CCR-09-1759
88. van Binnebeek S, Vanbilloen B, Baete K, Terwinghe C, Koole M, Mottaghy FM, et al. Comparison of diagnostic accuracy of (111)In-pentetreotide SPECT and (68)Ga-DOTATOC PET/CT: a lesion-by-lesion analysis in patients with metastatic neuroendocrine tumours. Eur Radiol. (2016) 26:900–9. doi: 10.1007/s00330-015-3882-1
89. Sainz-Esteban A, Olmos R, González-Sagrado M, González ML, Ruiz MÁ, García-Talavera P, et al. Contribution of 111In-pentetreotide SPECT/CT imaging to conventional somatostatin receptor scintigraphy in the detection of neuroendocrine tumours. Nucl Med Commun. (2015) 36:251–9. doi: 10.1097/MNM.0000000000000239
90. Pfeifer A, Knigge U, Binderup T, Mortensen J, Oturai P, Loft A, et al. 64Cu-DOTATATE PET for neuroendocrine tumors: a prospective head-to-head comparison with 111In-DTPA-octreotide in 112 patients. J Nucl Med. (2015) 56:847–54. doi: 10.2967/jnumed.115.156539
91. Perri M, Erba P, Volterrani D, Lazzeri E, Boni G, Grosso M, Mariani G. Octreo-SPECT/CT imaging for accurate detection and localization of suspected neuroendocrine tumors. Q J Nucl Med Mol Imaging. (2008) 52:323–33.18480741
92. Wong KK, Cahill JM, Frey KA, Avram AM. Incremental value of 111-in pentetreotide SPECT/CT fusion imaging of neuroendocrine tumors. Acad Radiol. (2010) 17:291–7. doi: 10.1016/j.acra.2009.08.015
93. Yang J, Kan Y, Ge BH, Yuan L, Li C, Zhao W. Diagnostic role of gallium-68 DOTATOC and gallium-68 DOTATATE PET in patients with neuroendocrine tumors: a meta-analysis. Acta Radiol. (2014) 55:389–98. doi: 10.1177/0284185113496679
94. Johnbeck CB, Knigge U, Kjær A. PET Tracers for somatostatin receptor imaging of neuroendocrine tumors: current status and review of the literature. Future Oncol. (2014) 10:2259–77. doi: 10.2217/fon.14.139
95. Geijer H, Breimer LH. Somatostatin receptor PET/CT in neuroendocrine tumours: update on systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. (2013) 40:1770–80. doi: 10.1007/s00259-013-2482-z
96. Treglia G, Castaldi P, Rindi G, Giordano A, Rufini V. Diagnostic performance of gallium-68 somatostatin receptor PET and PET/CT in patients with thoracic and gastroenteropancreatic neuroendocrine tumours: a meta-analysis. Endocrine. (2012) 42:80–7. doi: 10.1007/s12020-012-9631-1
97. Cuthbertson DJ, Barriuso J, Lamarca A, Manoharan P, Westwood T, Jaffa M, et al. The impact of 68Gallium DOTA PET/CT in managing patients with sporadic and familial pancreatic neuroendocrine tumours. Front Endocrinol (Lausanne). (2021) 12:654975. doi: 10.3389/fendo.2021.654975
98. Haug AR, Rominger A, Mustafa M, Auernhammer C, Göke B, Schmidt GP, et al. Treatment with octreotide does not reduce tumor uptake of (68)Ga-DOTATATE as measured by PET/CT in patients with neuroendocrine tumors. J Nucl Med. (2011) 52:1679–83. doi: 10.2967/jnumed.111.089276
99. de Angelis C, Carucci P, Repici A, Rizzetto M. Endosonography in decision making and management of gastrointestinal endocrine tumors. Eur J Ultrasound. (1999) 10:139–50. doi: 10.1016/s0929-8266(99)00054-3
100. Glover JR, Shorvon PJ, Lees WR. Endoscopic ultrasound for localisation of islet cell tumours. Gut. (1992) 33:108–10. doi: 10.1136/gut.33.1.108
101. Has Simsek D, Kuyumcu S, Turkmen C, Sanlı Y, Aykan F, Unal S, et al. Can complementary 68Ga-DOTATATE and 18F-FDG PET/CT establish the missing link between histopathology and therapeutic approach in gastroenteropancreatic neuroendocrine tumors? J Nucl Med. (2014) 55:1811–7. doi: 10.2967/jnumed.114.142224
102. Bahri H, Laurence L, Edeline J, Leghzali H, Devillers A, Raoul J-L, et al. High prognostic value of 18F-FDG PET for metastatic gastroenteropancreatic neuroendocrine tumors: a long-term evaluation. J Nucl Med. (2014) 55:1786–90. doi: 10.2967/jnumed.114.144386
103. Kayani I, Conry BG, Groves AM, Win T, Dickson J, Caplin M, et al. A comparison of 68Ga-DOTATATE and 18F-FDG PET/CT in pulmonary neuroendocrine tumors. J Nucl Med. (2009) 50:1927–32. doi: 10.2967/jnumed.109.066639
104. Squires MH, Volkan Adsay N, Schuster DM, Russell MC, Cardona K, Delman KA, et al. Octreoscan versus FDG-PET for neuroendocrine tumor staging: a biological approach. Ann Surg Oncol. (2015) 22:2295–301. doi: 10.1245/s10434-015-4471-x
105. Morris MA, Saboury B, Ahlman M, Malayeri AA, Jones EC, Chen CC, et al. Parathyroid imaging: past, present, and future. Front Endocrinol (Lausanne). (2022) 12:760419. doi: 10.3389/fendo.2021.760419
106. Papaefthymiou A, Laskaratos F-M, Koffas A, Manolakis A, Gkolfakis P, Coda S, et al. State of the art in endoscopic therapy for the management of gastroenteropancreatic neuroendocrine tumors. Curr Treat Options Oncol. (2022) 23:1014–34. doi: 10.1007/s11864-022-00986-w
107. Annibale B, Azzoni C, Corleto VD, di Giulio E, Caruana P, D’Ambra G, et al. Atrophic body gastritis patients with enterochromaffin-like cell dysplasia are at increased risk for the development of type I gastric carcinoid. Eur J Gastroenterol Hepatol. (2001) 13:1449–56. doi: 10.1097/00042737-200112000-00008
108. Delle Fave G, Kwekkeboom DJ, van Cutsem E, Rindi G, Kos-Kudla B, Knigge U, et al. ENETS Consensus guidelines for the management of patients with gastroduodenal neoplasms. Neuroendocrinology. (2012) 95:74–87. doi: 10.1159/000335595
109. Maione F, Chini A, Milone M, Gennarelli N, Manigrasso M, Maione R, et al. Diagnosis and management of rectal neuroendocrine tumors (NETs). Diagnostics. (2021) 11:771. doi: 10.3390/diagnostics11050771
110. Bellizzi AM. Assigning site of origin in metastatic neuroendocrine neoplasms: a clinically significant application of diagnostic immunohistochemistry. Adv Anat Pathol. (2013) 20:285–314. doi: 10.1097/PAP.0b013e3182a2dc67
111. Wang SC, Parekh JR, Zuraek MB, Venook AP, Bergsland EK, Warren RS, et al. Identification of unknown primary tumors in patients with neuroendocrine liver metastases. Arch Surg. (2010) 145:276–80. doi: 10.1001/archsurg.2010.10
112. Furnari M, Buda A, Delconte G, Citterio D, Voiosu T, Ballardini G, et al. The role of wireless capsule endoscopy (WCE) in the detection of occult primary neuroendocrine tumors. J Gastrointestin Liver Dis. (2017) 26:151–6. doi: 10.15403/jgld.2014.1121.262.wce
113. Partridge BJ, Tokar JL, Haluszka O, Heller SJ. Small bowel cancers diagnosed by device-assisted enteroscopy at a U.S. Referral center: a five-year experience. Dig Dis Sci. (2011) 56:2701–5. doi: 10.1007/s10620-011-1640-z
114. Mitsui K, Tanaka S, Yamamoto H, Kobayashi T, Ehara A, Yano T, et al. Role of double-balloon endoscopy in the diagnosis of small-bowel tumors: the first Japanese multicenter study. Gastrointest Endosc. (2009) 70:498–504. doi: 10.1016/j.gie.2008.12.242
115. Bellutti M, Fry LC, Schmitt J, Seemann M, Klose S, Malfertheiner P, et al. Detection of neuroendocrine tumors of the small bowel by double balloon enteroscopy. Dig Dis Sci. (2009) 54:1050–8. doi: 10.1007/s10620-008-0456-y
116. Manguso N, Gangi A, Johnson J, Harit A, Nissen N, Jamil L, et al. The role of pre-operative imaging and double balloon enteroscopy in the surgical management of small bowel neuroendocrine tumors: is it necessary? J Surg Oncol. (2018) 117:207–12. doi: 10.1002/jso.24825
117. Gangi A, Siegel E, Barmparas G, Lo S, Jamil LH, Hendifar A, et al. Multifocality in small bowel neuroendocrine tumors. J Gastrointest Surg. (2018) 22:303–9. doi: 10.1007/s11605-017-3586-8
118. Howe JR, Cardona K, Fraker DL, Kebebew E, Untch BR, Wang Y-Z, et al. The surgical management of small bowel neuroendocrine tumors: consensus guidelines of the North American neuroendocrine tumor society. Pancreas. (2017) 46:715–31. doi: 10.1097/MPA.0000000000000846
119. Abul-Hajj YJ, Cisek PL. Catechol estrogen adducts. J Steroid Biochem. (1988) 31:107–10. doi: 10.1016/0022-4731(88)90212-9
120. Rösch T, Lightdale CJ, Botet JF, Boyce GA, Sivak MV, Yasuda K, et al. Localization of pancreatic endocrine tumors by endoscopic ultrasonography. N Engl J Med. (1992) 326:1721–6. doi: 10.1056/NEJM199206253262601
121. Ardengh JC, de Paulo GA, Ferrari AP. EUS-guided FNA in the diagnosis of pancreatic neuroendocrine tumors before surgery. Gastrointest Endosc. (2004) 60:378–84. doi: 10.1016/s0016-5107(04)01807-3
122. Anderson MA, Carpenter S, Thompson NW, Nostrant TT, Elta GH, Scheiman JM. Endoscopic ultrasound is highly accurate and directs management in patients with neuroendocrine tumors of the pancreas. Am J Gastroenterol. (2000) 95:2271–7. doi: 10.1111/j.1572-0241.2000.02480.x
123. Zimmer T, Ziegler K, Bäder M, Fett U, Hamm B, Riecken EO, et al. Localisation of neuroendocrine tumours of the upper gastrointestinal tract. Gut. (1994) 35:471–5. doi: 10.1136/gut.35.4.471
124. Zimmer T, Stölzel U, Bäder M, Koppenhagen K, Hamm B, Buhr H, et al. Endoscopic ultrasonography and somatostatin receptor scintigraphy in the preoperative localisation of insulinomas and gastrinomas. Gut. (1996) 39:562–8. doi: 10.1136/gut.39.4.562
125. Zimmer T, Scherübl H, Faiss S, Stölzel U, Riecken EO, Wiedenmann B. Endoscopic ultrasonography of neuroendocrine tumours. Digestion. (2000) 62(Suppl 1):45–50. doi: 10.1159/000051855
126. Proye C, Malvaux P, Pattou F, Filoche B, Godchaux JM, Maunoury V, Palazzo L, Huglo D, Lefebvre J, Paris JC. Noninvasive imaging of insulinomas and gastrinomas with endoscopic ultrasonography and somatostatin receptor scintigraphy. Surgery (1998) 124:1134–43; discussion 1143-4. doi: 10.1067/msy.1998.93109
127. Ruszniewski P, Amouyal P, Amouyal G, Grangé JD, Mignon M, Bouché O, et al. Localization of gastrinomas by endoscopic ultrasonography in patients with zollinger-ellison syndrome. Surgery. (1995) 117:629–35. doi: 10.1016/s0039-6060(95)80005-0
128. Fujimori N, Osoegawa T, Lee L, Tachibana Y, Aso A, Kubo H, et al. Efficacy of endoscopic ultrasonography and endoscopic ultrasonography-guided fine-needle aspiration for the diagnosis and grading of pancreatic neuroendocrine tumors. Scand J Gastroenterol. (2016) 51:245–52. doi: 10.3109/00365521.2015.1083050
129. Ishii T, Katanuma A, Toyonaga H, Chikugo K, Nasuno H, Kin T, et al. Role of endoscopic ultrasound in the diagnosis of pancreatic neuroendocrine neoplasms. Diagnostics (Basel). (2021) 11:316. doi: 10.3390/diagnostics11020316
130. Pitre J, Soubrane O, Palazzo L, Chapuis Y. Endoscopic ultrasonography for the preoperative localization of insulinomas. Pancreas. (1996) 13:55–60. doi: 10.1097/00006676-199607000-00007
131. Huai JC, Zhang W, Niu HO, Su ZX, McNamara JJ, Machi J. Localization and surgical treatment of pancreatic insulinomas guided by intraoperative ultrasound. Am J Surg. (1998) 175:18–21. doi: 10.1016/s0002-9610(97)00235-3
132. Hiramoto JS, Feldstein VA, LaBerge JM, Norton JA. Intraoperative ultrasound and preoperative localization detects all occult insulinomas. Arch Surg (2001) 136:1020–5. doi: 10.1001/archsurg.136.9.1020
133. Hoffmann KM, Furukawa M, Jensen RT. Duodenal neuroendocrine tumors: classification, functional syndromes, diagnosis and medical treatment. Best Pract Res Clin Gastroenterol. (2005) 19:675–97. doi: 10.1016/j.bpg.2005.05.009
134. Yu F, Venzon DJ, Serrano J, Goebel SU, Doppman JL, Gibril F, et al. Prospective study of the clinical course, prognostic factors, causes of death, and survival in patients with long-standing zollinger-ellison syndrome. J Clin Oncol. (1999) 17:615–30. doi: 10.1200/JCO.1999.17.2.615
135. Weber HC, Venzon DJ, Lin JT, Fishbein VA, Orbuch M, Strader DB, et al. Determinants of metastatic rate and survival in patients with zollinger-ellison syndrome: a prospective long-term study. Gastroenterology. (1995) 108:1637–49. doi: 10.1016/0016-5085(95)90124-8
136. Rindi G, Luinetti O, Cornaggia M, Capella C, Solcia E. Three subtypes of gastric argyrophil carcinoid and the gastric neuroendocrine carcinoma: a clinicopathologic study. Gastroenterology. (1993) 104:994–1006. doi: 10.1016/0016-5085(93)90266-f
137. Pavel M, de Herder WW. ENETS Consensus guidelines for the standard of care in neuroendocrine tumors. Neuroendocrinology. (2017) 105:193–5. doi: 10.1159/000457957
138. Caplin M, Sundin A, Nillson O, Baum RP, Klose KJ, Kelestimur F, et al. ENETS Consensus guidelines for the management of patients with digestive neuroendocrine neoplasms: colorectal neuroendocrine neoplasms. Neuroendocrinology. (2012) 95:88–97. doi: 10.1159/000335594
139. Park SB, Kim DJ, Kim HW, Choi CW, Kang DH, Kim SJ, et al. Is endoscopic ultrasonography essential for endoscopic resection of small rectal neuroendocrine tumors? World J Gastroenterol. (2017) 23:2037. doi: 10.3748/wjg.v23.i11.2037
140. Öberg K. Molecular genomic blood biomarkers for neuroendocrine tumors: the long and winding road from berzelius and bence jones to a neuroendocrine destination. Neuroendocrinology. (2021) 111:297–303. doi: 10.1159/000508488
141. Öberg K, Califano A, Strosberg JR, Ma S, Pape U, Bodei L, et al. A meta-analysis of the accuracy of a neuroendocrine tumor mRNA genomic biomarker (NETest) in blood. Ann Oncol. (2020) 31:202–12. doi: 10.1016/j.annonc.2019.11.003
142. Kipnis ST, Hung M, Kumar S, Heckert JM, Lee H, Bennett B, et al. Laboratory, clinical, and survival outcomes associated with peptide receptor radionuclide therapy in patients with gastroenteropancreatic neuroendocrine tumors. JAMA Netw Open. (2021) 4:e212274. doi: 10.1001/jamanetworkopen.2021.2274
143. Bodei L, Kidd MS, Singh A, van der Zwan WA, Severi S, Drozdov IA, et al. PRRT Neuroendocrine tumor response monitored using circulating transcript analysis: the NETest. Eur J Nucl Med Mol Imaging. (2020) 47:895–906. doi: 10.1007/s00259-019-04601-3
144. Cristofanilli M, Budd GT, Ellis MJ, Stopeck A, Matera J, Miller MC, et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med. (2004) 351:781–91. doi: 10.1056/NEJMoa040766
145. de Bono JS, Scher HI, Montgomery RB, Parker C, Miller MC, Tissing H, et al. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res. (2008) 14:6302–9. doi: 10.1158/1078-0432.CCR-08-0872
146. Cohen SJ, Punt CJA, Iannotti N, Saidman BH, Sabbath KD, Gabrail NY, et al. Relationship of circulating tumor cells to tumor response, progression-free survival, and overall survival in patients with metastatic colorectal cancer. J Clin Oncol. (2008) 26:3213–21. doi: 10.1200/JCO.2007.15.8923
147. Khan MS, Tsigani T, Rashid M, Rabouhans JS, Yu D, Luong TV, et al. Circulating tumor cells and EpCAM expression in neuroendocrine tumors. Clin Cancer Res. (2011) 17:337–45. doi: 10.1158/1078-0432.CCR-10-1776
148. Khan MS, Kirkwood A, Tsigani T, Garcia-Hernandez J, Hartley JA, Caplin ME, et al. Circulating tumor cells as prognostic markers in neuroendocrine tumors. J Clin Oncol. (2013) 31:365–72. doi: 10.1200/JCO.2012.44.2905
149. Mandair D, Khan MS, Lopes A, Furtado O’Mahony L, Ensell L, Lowe H, et al. Prognostic threshold for circulating tumor cells in patients with pancreatic and midgut neuroendocrine tumors. J Clin Endocrinol Metab. (2021) 106:872–82. doi: 10.1210/clinem/dgaa822
150. Mori M, Palumbo D, Muffatti F, Partelli S, Mushtaq J, Andreasi V, et al. Prediction of the characteristics of aggressiveness of pancreatic neuroendocrine neoplasms (PanNENs) based on CT radiomic features. Eur Radiol. (2022). doi: 10.1007/s00330-022-09351-9. [Epub ahead of print]
151. Chiti G, Grazzini G, Flammia F, Matteuzzi B, Tortoli P, Bettarini S, et al. Gastroenteropancreatic neuroendocrine neoplasms (GEP-NENs): a radiomic model to predict tumor grade. Radiol Med. (2022) 127:928–38. doi: 10.1007/s11547-022-01529-x
152. Crippa S, Partelli S, Zamboni G, Scarpa A, Tamburrino D, Bassi C, et al. Incidental diagnosis as prognostic factor in different tumor stages of nonfunctioning pancreatic endocrine tumors. Surgery. (2014) 155:145–53. doi: 10.1016/j.surg.2013.08.002
153. Peranteau WH, Palladino AA, Bhatti TR, Becker SA, States LJ, Stanley CA, et al. The surgical management of insulinomas in children. J Pediatr Surg. (2013) 48:2517–24. doi: 10.1016/j.jpedsurg.2013.04.022
154. Mehrabi A, Fischer L, Hafezi M, Dirlewanger A, Grenacher L, Diener MK, et al. A systematic review of localization, surgical treatment options, and outcome of insulinoma. Pancreas. (2014) 43:675–86. doi: 10.1097/MPA.0000000000000110
155. Knigge U, Hansen CP. Surgery for GEP-NETs. Best Pract Res Clin Gastroenterol. (2012) 26:819–31. doi: 10.1016/j.bpg.2012.12.005
156. Su A-P, Ke N-W, Zhang Y, Liu X-B, Hu W-M, Tian B-L, et al. Is laparoscopic approach for pancreatic insulinomas safe? Results of a systematic review and meta-analysis. J Surg Res. (2014) 186:126–34. doi: 10.1016/j.jss.2013.07.051
157. Guo Q, Wu Y. Surgical treatment of pancreatic islet cell tumor: report of 44 cases. Hepatogastroenterology. (2013) 60:2099–102.24719954
158. Sharma P, Arora S, Karunanithi S, Khadgawat R, Durgapal P, Sharma R, et al. Somatostatin receptor based PET/CT imaging with 68Ga-DOTA-Nal3-octreotide for localization of clinically and biochemically suspected insulinoma. Q J Nucl Med Mol Imaging. (2016) 60:69–76.24740163
159. Laidlaw DA, Smith PE, Hudgson P. Orbital pseudotumour secondary to giant cell arteritis: an unreported condition. Br Med J. (1990) 300:784. doi: 10.1136/bmj.300.6727.784
160. Cases AI, Ohtsuka T, Fujino M, Ideno N, Kozono S, Zhao M, et al. Expression of glucagon-like peptide 1 receptor and its effects on biologic behavior in pancreatic neuroendocrine tumors. Pancreas. (2014) 43:1–6. doi: 10.1097/MPA.0b013e3182a71537
161. Eriksson O, Velikyan I, Selvaraju RK, Kandeel F, Johansson L, Antoni G, et al. Detection of metastatic insulinoma by positron emission tomography with [(68)ga]exendin-4-a case report. J Clin Endocrinol Metab. (2014) 99:1519–24. doi: 10.1210/jc.2013-3541
162. Christ E, Wild D, Forrer F, Brändle M, Sahli R, Clerici T, et al. Glucagon-like peptide-1 receptor imaging for localization of insulinomas. J Clin Endocrinol Metab. (2009) 94:4398–405. doi: 10.1210/jc.2009-1082
163. Hayes AR, Furtado O’Mahony L, Quigley A-M, Gnanasegaran G, Caplin ME, Navalkissoor S, et al. The combined interpretation of 68Ga-DOTATATE PET/CT and 18F-FDG PET/CT in metastatic gastroenteropancreatic neuroendocrine tumors: a classification system with prognostic impact. Clin Nucl Med. (2022) 47:26–35. doi: 10.1097/RLU.0000000000003937
164. Panagiotidis E, Alshammari A, Michopoulou S, Skoura E, Naik K, Maragkoudakis E, et al. Comparison of the impact of 68 ga-DOTATATE and 18 F-FDG PET/CT on clinical management in patients with neuroendocrine tumors. J Nucl Med. (2017) 58:91–6. doi: 10.2967/jnumed.116.178095
165. Chan DL, Hayes AR, Karfis I, Conner A, Furtado O’Mahony L, Mileva M, et al. Dual [68Ga]DOTATATE and [18F]FDG PET/CT in patients with metastatic gastroenteropancreatic neuroendocrine neoplasms: a multicentre validation of the NETPET score. Br J Cancer. (2022). doi: 10.1038/s41416-022-02061-5. [Epub ahead of print]
166. Gaudenzi G, Dicitore A, Carra S, Saronni D, Pozza C, Giannetta E, et al. MANAGEMENT OF ENDOCRINE DISEASE: precision medicine in neuroendocrine neoplasms: an update on current management and future perspectives. Eur J Endocrinol. (2019) 181:R1–R10. doi: 10.1530/EJE-19-0021
167. Gaudenzi G, Albertelli M, Dicitore A, Würth R, Gatto F, Barbieri F, et al. Patient-derived xenograft in zebrafish embryos: a new platform for translational research in neuroendocrine tumors. Endocrine. (2017) 57:214–9. doi: 10.1007/s12020-016-1048-9
168. Mitra A, Mishra L, Li S. Technologies for deriving primary tumor cells for use in personalized cancer therapy. Trends Biotechnol. (2013) 31:347–54. doi: 10.1016/j.tibtech.2013.03.006
169. Grozinsky-Glasberg S, Shimon I, Rubinfeld H. The role of cell lines in the study of neuroendocrine tumors. Neuroendocrinology. (2012) 96:173–87. doi: 10.1159/000338793
170. Ćwikła JB, Bodei L, Kolasinska-Ćwikła A, Sankowski A, Modlin IM, Kidd M. Circulating transcript analysis (NETest) in GEP-NETs treated with somatostatin analogs defines therapy. J Clin Endocrinol Metab. (2015) 100:E1437–45. doi: 10.1210/jc.2015-2792
Keywords: neuroendocrine tumor, ki67 proliferation index, chromogranin A, gut peptide hormones, NETest, somatostatin receptor scintigraphy, 68-gallium-DOTA-Octreotate
Citation: Koffas A, Giakoustidis A, Papaefthymiou A, Bangeas P, Giakoustidis D, Papadopoulos VN and Toumpanakis C (2023) Diagnostic work-up and advancement in the diagnosis of gastroenteropancreatic neuroendocrine neoplasms. Front. Surg. 10:1064145. doi: 10.3389/fsurg.2023.1064145
Received: 7 October 2022; Accepted: 7 February 2023;
Published: 6 March 2023.
Edited by:
Roberto Valente, Umeå University, SwedenReviewed by:
Francesco Panzuto, Sapienza University of Rome, Italy© 2023 Koffas, Giakoustidis, Papaefthymiou, Bangeas, Giakoustidis, Papadopoulos and Toumpanakis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Apostolos Koffas YXBvc3RvbG9zX2tvZmZhc0Bob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Specialty Section: This article was submitted to Surgical Oncology, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.