 Yu Cheng
Yu Cheng Taicheng Li
Taicheng Li Qin Ling
Qin Ling Xiaoyi Yuan
Xiaoyi Yuan Shengfei Xu
Shengfei Xu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Surg. , 20 September 2022
Sec. Genitourinary Surgery and Interventions
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.986679
Purpose: We conducted the first meta-analysis to determine the diagnostic value of non-invasive methods for diagnosing bladder outlet obstruction (BOO) in men with lower urinary tract symptoms (LUTS).
Methods: We searched a range of databases for relevant publications up to June 2022, including PubMed, Embase, Web of Science, and the Cochrane Library. Retrieved studies were then reviewed for eligibility and data were extracted. The risk of bias (RoB) was assessed using the QUADAS-2 tool. We then performed a formal meta-analysis to evaluate the accuracy of various non-invasive methods for diagnosing BOO in men.
Results: We identified 51 eligible studies including 7,897 patients for meta-analysis. The majority of the studies had a low overall RoB. Detrusor wall thickness (DWT) (pooled sensitivity (SSY): 71%; specificity (SPY): 88%; diagnostic odds ratio (DOR): 17.15; area under curve (AUC) 0.87) and the penile cuff test (PCT) (pooled SSY: 87%; SPY: 78%; DOR: 23.54; AUC: 0.88) showed high accuracy for diagnosing BOO. Furthermore, data suggested that DWT had the highest pooled SPY (0.89), DOR (32.58), and AUC (0.90), when using 2 mm as the cut-off.
Conclusion: Of the non-invasive tests tested, DWT and PCT had the highest levels of diagnostic accuracy for diagnosing BOO in men with LUTS. DWT, with a 2 mm cut-off, had the highest level of accuracy. These two methods represent good options as non-invasive tools for evaluating BOO in males.
Lower urinary tract symptoms (LUTS) can be very troublesome for both male and female patients and can cause a reduction in their quality of life. Most patients seek medical help due to bothersome LUTS, especially when they develop bladder outlet obstruction (BOO) as this can result in severe urinary difficulty (1). BOO is mainly caused by benign prostatic hyperplasia (BPH) and usually requires surgical treatment. Therefore, it is very important that we can determine whether LUTS is due to BOO if we are to optimize patient management (2). Over recent years, the evaluation of LUTS/BPH has depended heavily on pressure-flow study (PFS) of urodynamic study (UDS) as the gold standard diagnostic tests for BOO (3). However, UDS has several disadvantages. First, PFS requires transurethral intubation and may cause urinary symptoms, such as hematuria and urinary tract infections. Furthermore, PFS can be unpleasant and is commonly associated with anxiety and embarrassment (4). In addition, UDS is expensive, time consuming, and requires delicate instruments and specific expertise.
Given the invasive nature and side effects associated with conventional invasive PFS, a variety of non-invasive diagnostic methods have been developed (5). Although these novel and non-invasive diagnostic methods were designed to improve the quality of life in patients with LUTS by promoting earlier diagnosis and treatment, and do show significant potential (6), there is some conflict with regards to their specific clinical outcomes. Previous authors have evaluated and summarized the diagnostic value of these non-invasive methods (5, 7–14); nevertheless, researchers have yet to perform a meta-analysis to investigate the diagnostic accuracy for these approaches in a quantitative manner.
The aim of the present meta-analysis was to re-evaluate and determine the diagnostic accuracy of non-invasive methods for the diagnosis of BOO in men with LUTS by assessing sensitivity (SSY), specificity (SPY), diagnostic odds ratio (DOR) and area under curve (AUC). This was the first meta-analysis to quantitatively compare the diagnostic value of different non-invasive methods for BOO.
This meta-analysis was conducted based on Preferred Reporting Items for a Systematic Review and Meta-Analysis (PRISMA). Neither ethical approval or informed consent was required for this study.
We searched a range of databases for relevant publications up to June 2022, including PubMed, Embase, Web of Science, and the Cochrane Library. The search strategy was (“uroflowmetry” OR “flow rate” OR “intravesical prostat* protrusion” OR “intravesical protrusion” OR “penile cuff” OR “urocuff” OR “detrusor wall thickness” OR “detrusor thickness” OR “bladder wall thickness” OR “bladder thickness” OR “external condom catheter” OR “doppler ultrasound” OR “resistive index” OR “velocity ratio” OR “bladder weight” OR “prostate volume” OR “international prostat* symptom* score” OR “IPSS” OR “residual urine” OR “post-void* residual urine” OR “RUV” OR “PVR” OR “prostat* specific antigen” OR “PSA” OR “near-infrared spectroscopy” OR “noninvasive” OR “non-invasive” OR “noninvasively” OR “non-invasively”) AND (“bladder obstruction” OR “benign prostatic obstruction” OR “bladder outlet obstruction” OR “bladder outflow obstruction” OR “BOO” OR “BPO” OR “infravesical obstruction”). To achieve a comprehensive literature search, we also reviewed the reference lists of the retrieved literature. The articles included in this study were restricted to human subjects and those published in English. Two researchers carried out the same literature screening protocols; any disagreements were resolved by a third researcher.
Following the removal of duplicate articles, two researchers independently reviewed the titles and abstracts of the retrieved studies. To be eligible for analysis, the articles needed to meet our specific inclusion criteria: (1) population: patients with LUTS aged ≥18 years; (2) index test: non-invasive methods. The following noninvasive tests were eligible for inclusion in meta-analysis: the penile cuff test (PCT), near-infrared spectrum (NIRS), ultrasonography of post-voided residual (PVR), intravesical prostatic protrusion (IPP), detrusor wall thickness (DWT), bladder wall thickness (BWT), resistive index (RI), prostate volume (PV), and free uroflowmetry, a detailed description of each index test is included in the Supplementary Material; (3) reference standard: invasive PFS; (4) outcome: diagnostic accuracy for the diagnosis of BOO; (5) study design: any type, including comparative studies, clinical trials, retrospective or prospective studies; (6) complete data: all data could be obtained directly or calculated and included true positive (TP), false positive (FP), true negative (TN), and false negative (FN) data. The exclusion criteria were as follows: (1) failure to meet the inclusion criteria; (2) duplicated publications; (3) reviews, case reports, conference abstracts, letters and editorials; (4) non-English and non-human studies.
All data extraction was completed by two researchers independently and manually according to the inclusion criteria, any inconsistency was resolved by a third researcher. We extracted a range of data from eligible publications, including: (a) author-year; (b) study design; (c) mean age; (d) country; (e) sample size; (f) index test; (g) cut-off value; (h) TP; (i) FP; (j) TN; and (k) FN.
The quality of all studies included in this meta-analysis was assessed by two researchers in accordance with the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) tool (15). This tool was used to evaluate the risk of bias (RoB) on the basis of the following criteria: patient selection, index test, reference standard, flow and timing, and assessing applicability concerns by patient selection, index test, reference test.
To determine the diagnostic accuracy of non-invasive tests for the diagnosis of BOO, we adopted pooled SSY, SPY, DOR and AUC of summary receiver operating characteristics (SROC) as the primary indicators. Because these four indicators can well illustrate the diagnostic ability of the index tests (16–18). The SSY represents the ability to detect disease and the SPY represents the ability to exclude a disease. The DOR is a measure for the discriminative power of a diagnostic test: the ratio of the odds of a positive test result among diseased to the odds of a positive test result among the non-diseased. SROC curves are used to determine test performances and present the tradeoff between the SSY and SPY of non-invasive tests. A two-by-two contingency table (consisting of TP, FP, FN and TN) was then constructed based on the data extracted from each study included in the meta-analysis. If a study used different cut-off values for the same index test, we adopted data for the most common cut-off value to conduct the meta-analysis. A bivariate model was then used to calculate the pooled SSY, SPY, DOR and AUC, along with 95% confidence intervals (CIs) (19). Pooled data was displayed using forest plots and summary receiver operating characteristics (SROC) plots. The heterogeneity of the pooled data was assessed by Cochrane's Q test and I2 test (20). If the data showed little heterogeneity (P ≥ 0.1 and I2 < 50%), a fixed-effect model was used; otherwise, a random-effect model was adopted. A threshold effect was determined by calculating Spearman's correlation coefficient between SSY and the false positive rate (1-SPY) (18); a strong positive correlation was considered a significant threshold effect. Sensitivity analysis and meta-regression were also conducted to explore the sources of heterogeneity relating to non-threshold effects. Publication bias was evaluated with Deeks’ funnel plots and an associated regression test of asymmetry (21). Data were analyzed by STATA version 14.0 (StataCorp LP, College Station, TX, USA) using midas commands. Spearman's correlation coefficient was calculated by MetaDiSc 1.4 (Universidad Complutense, Madrid, Spain). Quality assessment was performed by RevMan 5.3 (Cochrane Collaboration, Oxford, UK). P < 0.05 was considered statistically significant.
We conducted a comprehensive literature search of the PubMed, Embase, Web of Science and the Cochrane Library databases following an established search strategy. We identified a total of 10,058 articles. After the removal of duplicates, reviews, case reports, conference abstracts, letters, and editorials, 2,937 articles were left for screening. Then, 2,886 studies were removed following abstract and full-text evaluation and by insufficient data. For BWT, one study resulted in a significant increase in heterogeneity, after excluding this study, the final number of studies was not enough to perform meta-analysis. For NIRS, the method and calculation in each of the study was different from the other and far from being standard, Therefore, we did not include these two index tests. Finally, 51 articles were eligible for meta-analysis (22–72). Full details of the screening process are shown in Figure 1.
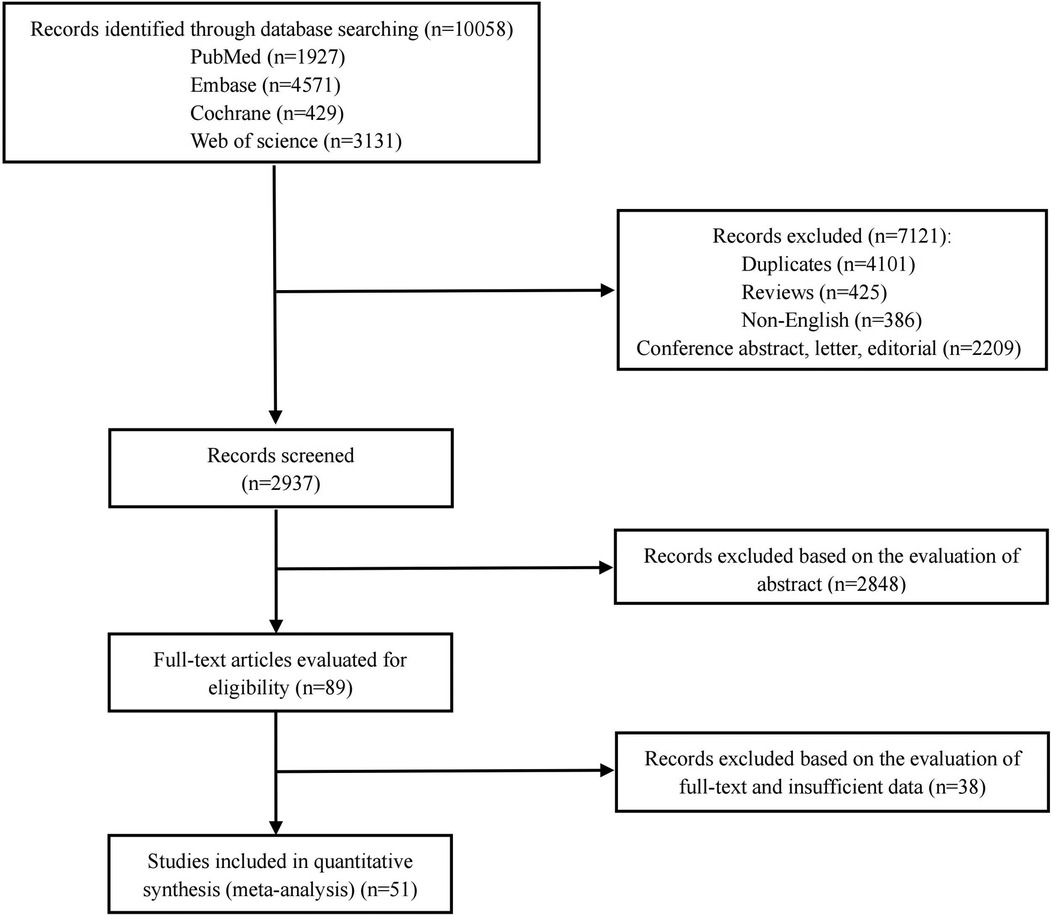
Figure 1. The screening flow diagram of the retrieval studies.
Of the 51 studies included in this meta-analysis, the publication year ranged from 1994 to 2021. These studies involved 21 countries and a total of 7,897 participants. All of the 51 studies were non-randomized trials (NRT); 22 studies were prospective, two were retrospective; 14 studies were blinded, 13 were not blinded; and the remaining studies did not describe their specific design. All 51 studies examined the accuracy of non-invasive methods for the diagnosis of BOO in men with LUTS, using PFS as the gold standard. For specific descriptions of the included studies, see Table 1.
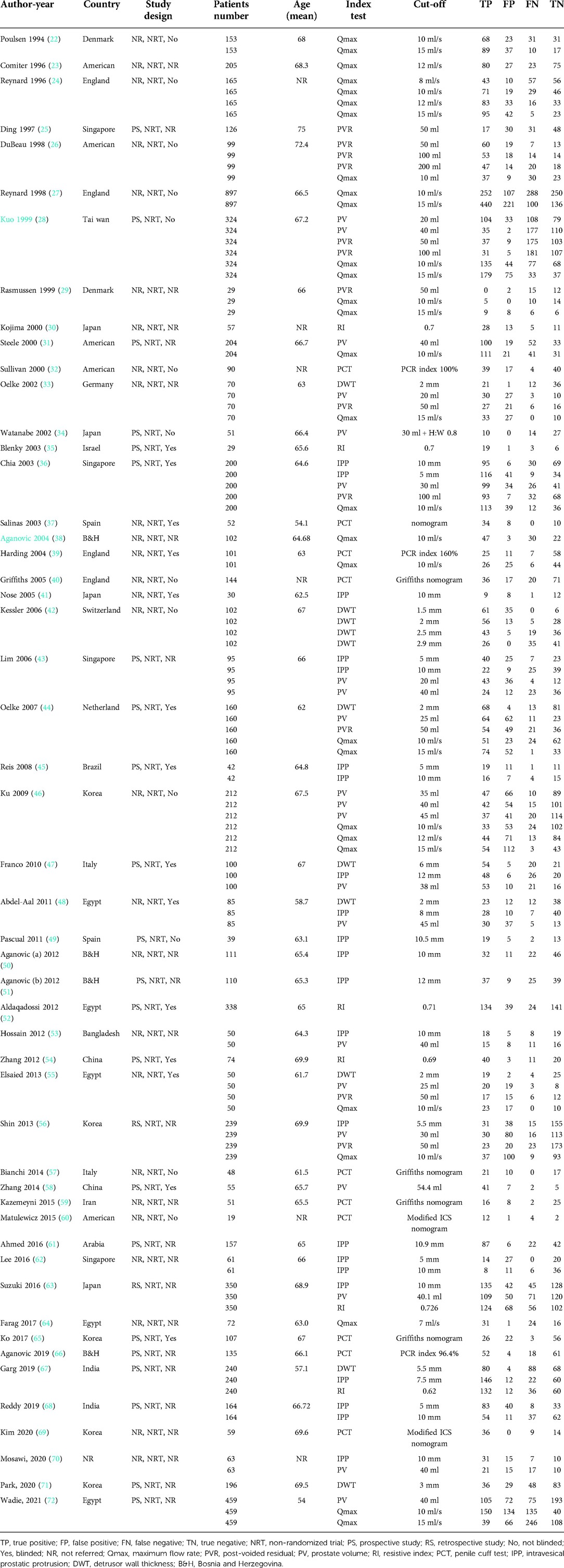
Table 1. Characteristics of the included studies.
Outcomes relating to quality assessment and RoB are shown in Figure 2. Overall, the RoB was generally low for most studies. In the patient selection domain, three studies were classified as high risk due to inappropriate inclusion or exclusion criteria. Twenty-three studies had an unclear risk because it was unknown as to whether they adopted consecutive patients or random samples. In the index test domain, 6 studies showed high risk because the results of the index test were interpreted with knowledge of the reference standard. Nine studies were associated with an unclear risk. In the reference standard domain, 12 studies had a high risk due to knowledge of the results of index tests when interpreting the results of the reference standard; the other 20 studies were at an unclear risk. In the flow and timing domain, only two studies had a high risk; this was due to an inappropriate interval between the index test and the reference standard. In terms of applicability concern, the majority of the publications were at low risk, thus indicating that the patients, index test, and reference standard, for most studies were representative of clinical routine practice.

Figure 2. Risks of bias of the included studies based on QUADAS-2 tool.
With regards to the index tests (DWT, PCT, RI, IPP, Qmax, PV, PVR), we conducted quantitative analysis (meta-analysis) for these tests. The data extracted or calculated from published studies are presented in Table 1.
Outcomes for pooled SSY, SPY, DOR, and AUC of SROC curve are shown in Figures 3–5. Figure 3 shows the pooled SSY and SPY. Across these tests, the pooled SSY ranged from 71% to 87% and the pooled SPY ranged from 74% to 88%. PCT had the highest pooled SSY at 87% (95% CI: 77%–93%) (Figure 3B), followed by RI at 79% (95% CI: 73%–84%) (Figure 3C). DWT had the highest pooled SPY at 88% (95% CI: 78%–93%) (Figure 3A), followed by IPP at 79% (95% CI: 74%–83%) (Figure 3D). The pooled DOR, as presented by forest plots, are shown in Figure 4, ranging from 9.94 to 23.54. PCT exhibited the optimal DOR (23.54, 95% CI: 13.56–40.85) (Figure 4B), followed by DWT at 17.15 (95% CI: 7.09–41.46) (Figure 4A). Due to a significant threshold effect was found for PCT, Qmax and PV, thus we only fit SROC curve and calculate the area under ROC curve for these three tests. SROC curves indicated that DWT and PCT had a relatively better diagnostic power, with AUCs of 0.87 (95% CI: 0.84–0.90) and 0.88 (95% CI: 0.85–0.91) respectively. These indicators are summarized in Table 2. In brief, DWT and PCT showed high levels of diagnostic accuracy; the pooled SSY and SPY exceeded 70%, DORs were the highest and the pooled AUCs exceeded 0.85.
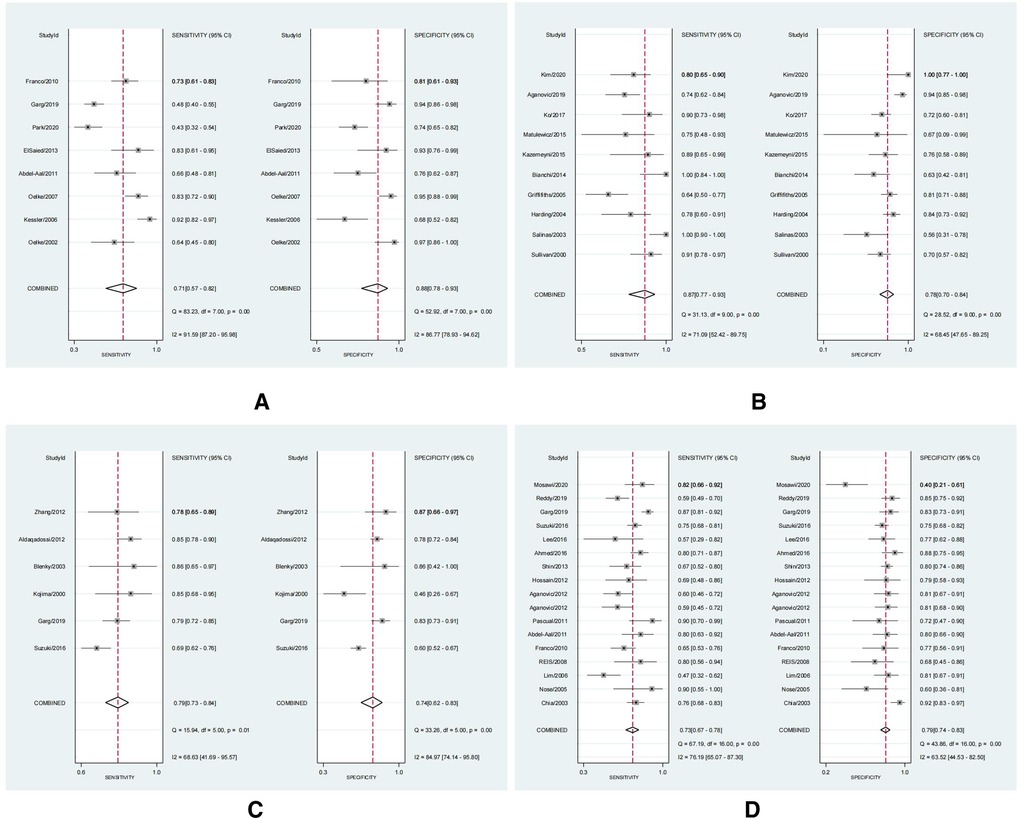
Figure 3. The forest plots of the sensitivity (SSY) and specificity (SPY) with a 95% confidence interval for DWT (A), PCT (B), RI (C), IPP (D) in the diagnosis of BOO in men.
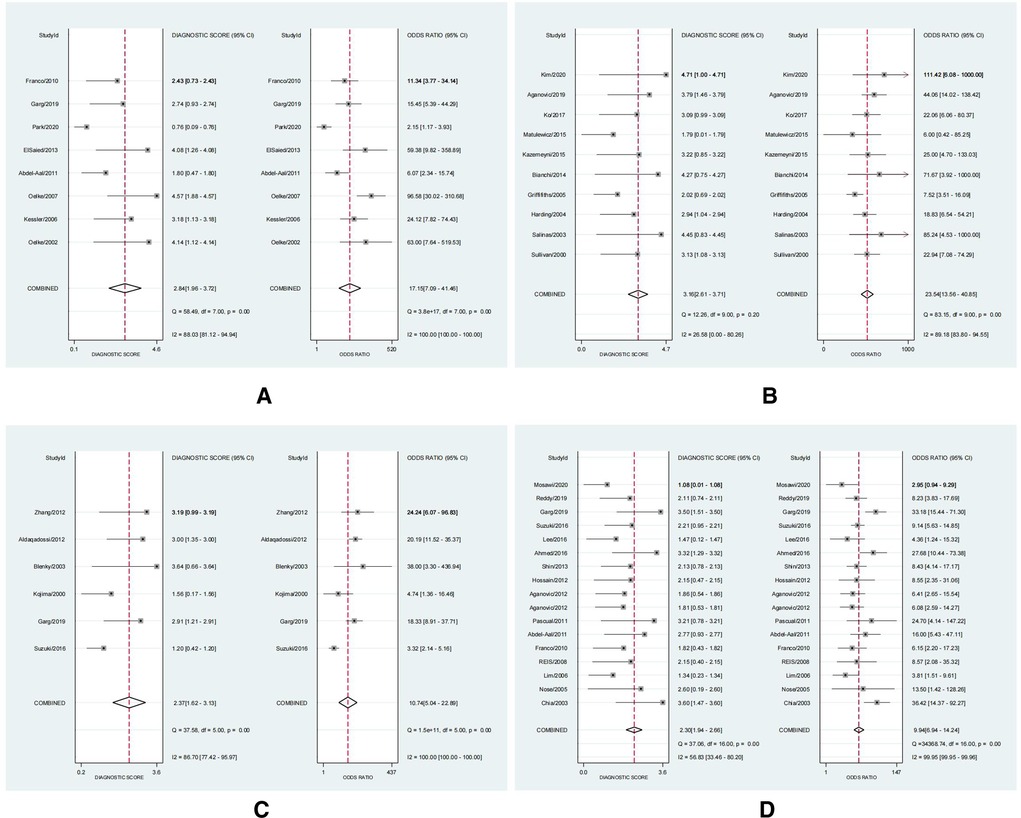
Figure 4. The forest plots of diagnostic odds ratio (DOR) with a 95% confidence interval for DWT (A), PCT (B), RI (C), IPP (D) in the diagnosis of BOO in men.
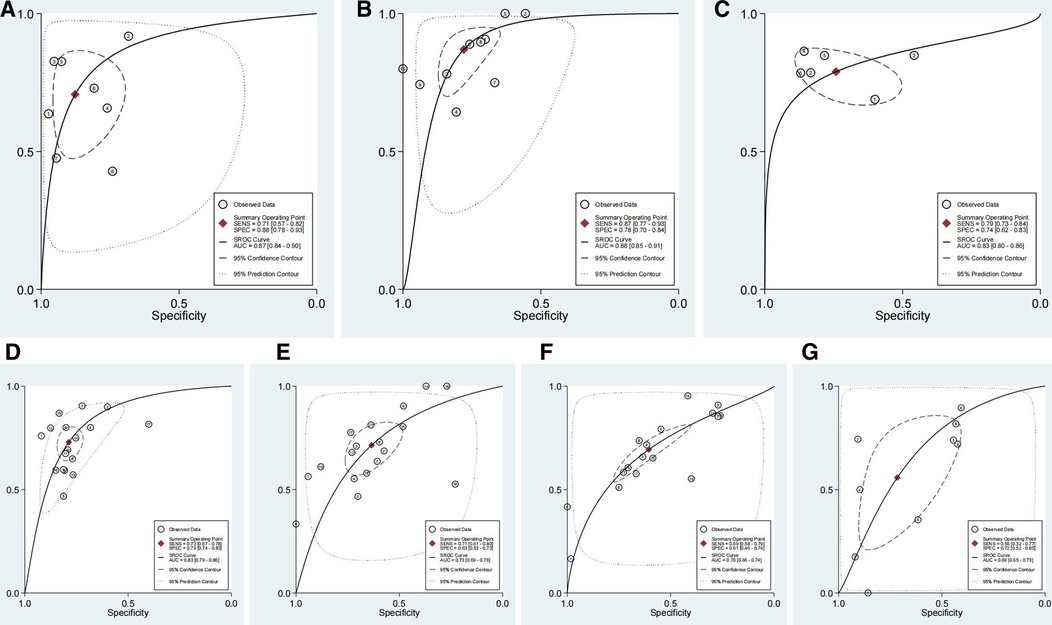
Figure 5. The summary of receiver operator characteristic (SROC) with a 95% confidence interval for DWT (A), PCT (B), RI (C), IPP (D), Qmax (E), PV (F) and PVR (G) in the diagnosis of BOO in men.
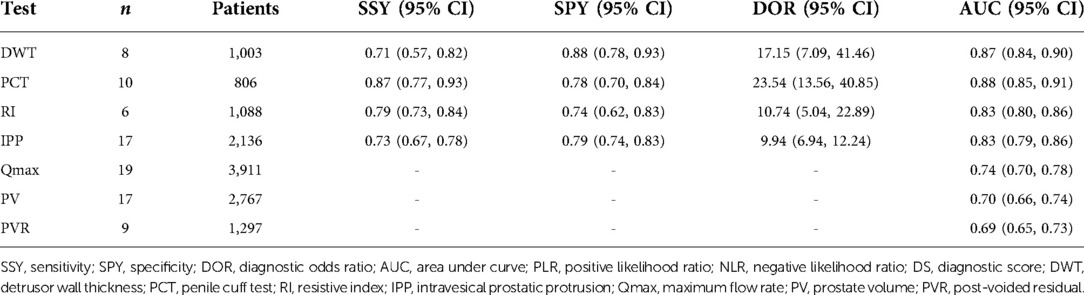
Table 2. Summary of the pooled data for each type of the index test.
We selected the most commonly used threshold values for each test to perform further analysis. We found that DWT (using 2 mm as the cut-off) possessed the greatest diagnostic accuracy for diagnosing BOO in men across these index tests, with a pooled SSY of 0.79 (95% CI: 0.68–0.88), SPY of 0.89 (95% CI: 0.75–0.96), DOR of 32.58 (95% CI: 12.04–88.17), and an AUC of 0.90 (95% CI: 0.87–0.92). PCT (using Griffith's nomogram as the diagnostic criteria) had the second-best diagnostic accuracy, with a pooled SSY of 0.89 (95% CI: 0.67–0.97), SPY of 0.73 (95% CI: 0.65–0.81), DOR of 22.98 (95% CI: 6.76–77.76) and an AUC of 0.81 (95% CI: 0.78–0.85). Table 3 shows a summary of results for each type of index test using the most commonly threshold values.
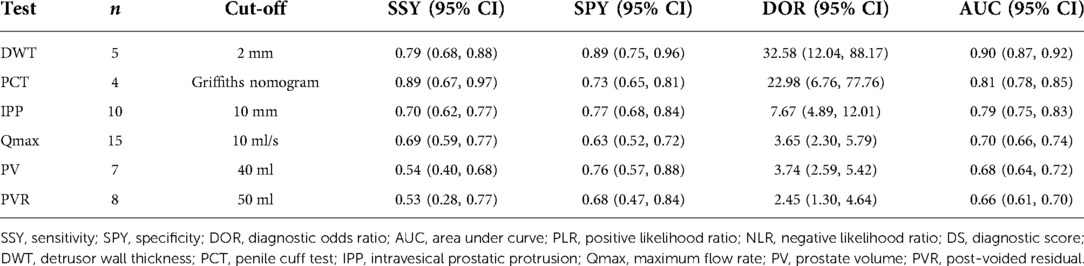
Table 3. Summary of the pooled data for each type of index test using the most commonly used threshold values.
The heterogeneity between studies included threshold effects and non-threshold effects. The threshold effect was assessed by Spearman's correlation coefficient, with values of 0.119 (P = 0.779) for DWT, 0.673 (P = 0.033) for PCT, 0.029 (P = 0.957) for RI, 0.383 (P = 0.129) for IPP, 0.527 (P = 0.025) for Qmax, 0.813 (P = 0.000) for PV, and 0.583 (P = 0.099) for PVR. Therefore, a statistically significant threshold effect was found for PCT, Qmax and PV and we only fit SROC curve and calculate the area under ROC curve for these three tests (Figures 5E–G; Table 2). The heterogeneity of the non-threshold effect was assessed by Cochrane's Q test and I2 test. Forest plots showed that the heterogeneity for the pooled SSY, SPY and DOR for all of these index tests were generally high (P < 0.1 for Cochrane's Q test and I2 > 50% for I2 test). Therefore, a random effect model was applied when pooling the data. To investigate the potential sources of heterogeneity, we conducted sensitivity analysis and meta-regression analysis.
We conducted sensitivity analysis to evaluate the effect of each individual study on the pooled DOR by removing the eligible study one by one for each of the index tests. The pooled data was not changed substantially by removing any of the eligible studies for these index tests (Figure 6).

Figure 6. The sensitivity analysis with a 95% confidence interval for DWT (A), PCT (B), RI (C), IPP (D), Qmax (E), PV (F) and PVR (G) in the diagnosis of BOO in men.
Next, we performed meta-regression analysis to further identify the sources of heterogeneity, including publication year (pre-2010 vs. post-2010), mean age (≤65 vs. >65), sample size (≤100 vs. >100) and cut-off (most common vs. not). The results of meta-regression analysis are presented in Figure 7. Analysis indicated that some of these four factors may represent the source of heterogeneity for these index tests and that the origin of heterogeneity would be different for different tests.
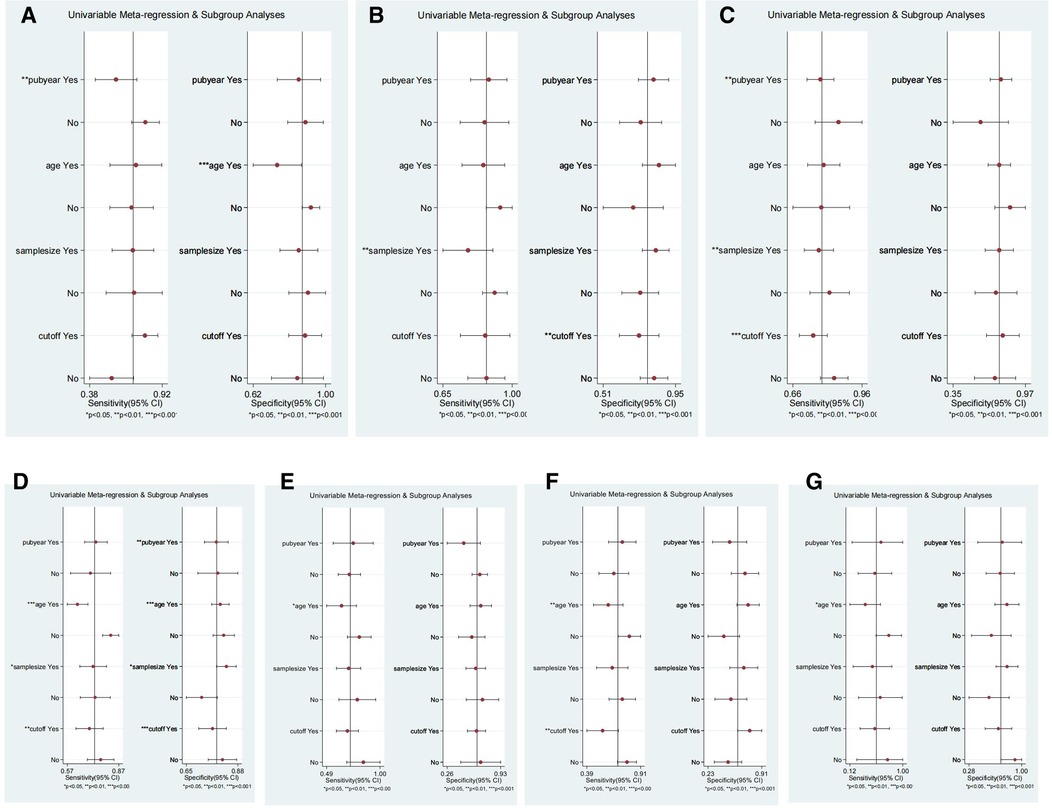
Figure 7. The meta-regression for DWT (A), PCT (B), RI (C), IPP (D), Qmax (E), PV (F) and PVR (G) in the diagnosis of BOO in men. Meta-regression was performed according to whether the publication year was after 2010, the mean age was over 65, the sample size was over 100 and to use the most commonly used cut-off.
Finally, publication bias was evaluated with a Deeks’ funnel plot and an associated regression test for asymmetry. Funnel plots showed that studies relating to DWT, PCT, RI, IPP, PV and PVR were all evenly distributed on both sides of the regression line (P > 0.05; Figure 8). A significant publication bias was identified for studies involving Qmax (P < 0.05).
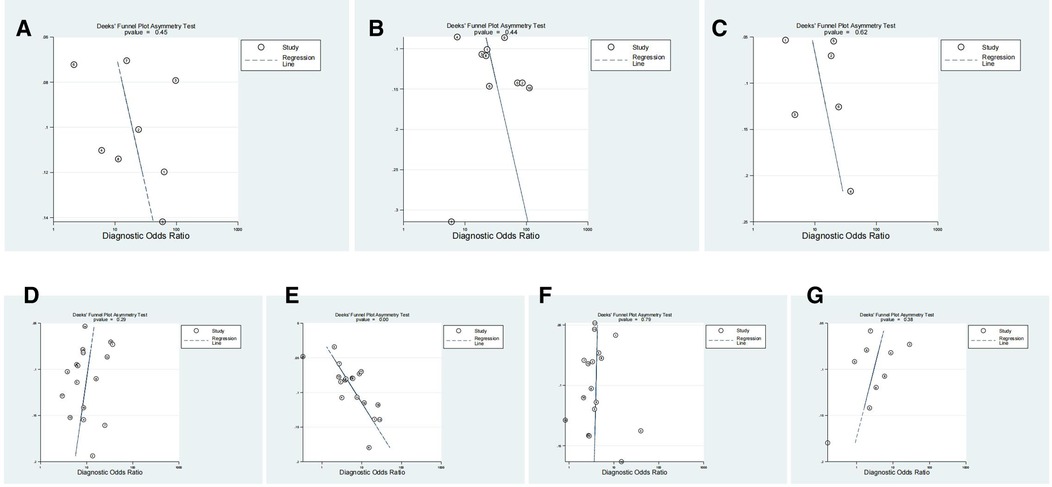
Figure 8. The Deek’s funnel plot for the assessment of publication bias for DWT (A), PCT (B), RI (C), IPP (D), Qmax (E), PV (F) and PVR (G) in the diagnosis of BOO in men.
There are several limitations to the use of UDS to diagnose BOO in men, including the invasive nature of this technique, high costs, and side effects. Consequently, there is significant interest in the development of non-invasive methods to diagnose BOO. Over recent years, several different methods have been developed. However, no meta-analysis has been performed to evaluate the diagnostic accuracy of these new non-invasive tests for diagnosing BOO in men. Therefore, we conducted the first meta-analysis to investigate the diagnostic accuracy of seven non-invasive tests by pooling the data and performing quantitative analysis.
Previous studies have investigated the accuracy of non-invasive tools for the diagnosis of BOO in men; however, conclusions remain inconsistent. A previous systematic review reported that PCT, DWT and NIRS had the highest median SSYs ranging from 82% to 85.7% (5). The highest median NPVs ranged from 84% to 89% when using the most common cut-offs. The findings of our present meta-analysis are consistent with these earlier findings in that systematic review-DWT and PCT were the two most promising non-invasive tests.
Our results indicated that the pooled DORs for DWT and PCT were 17.15 (95% CI: 7.09–41.46) and 23.54 (95% CI: 13.56–40.85) respectively. Furthermore, DWT (using 2 mm as the cut-off) exhibited the highest DOR value (32.58, 95% CI: 12.04–88.17). The DOR is one of the most primary indicators for test accuracy and combines data from SSY and SPY into a single number (73). These data suggested that DWT and PCT had the highest accuracies for the diagnosis of BOO in men when compared among the seven non-invasive methods, especially with DWT using the most commonly used cut-off. Furthermore, the SPY (0.89, 95% CI: 0.75–0.96) and AUC (0.90, 95% CI: 0.87–0.92) values for DWT were also the highest. Unlike a conventional ROC curve, which observes the effect of varying cut-offs on SSY and SPY in a single study, each data point represents an individual study in a SROC curve (18). Our results showed that DWT and PCT had a relatively better diagnostic power, with AUCs of 0.87 (95% CI: 0.84–0.90) and 0.88 (95% CI: 0.85–0.91) respectively.
A vital aspect of meta-analysis is to identify the sources of heterogeneity (74). In the present study, heterogeneity tests showed that PCT, Qmax, and PV, had a significant threshold effect. The heterogeneity of the pooled data caused by non-threshold effects was generally high. We did not find that any single study had a significant influence on the pooled data for each type of non-invasive method. However, in our meta-regression analysis, we found that publication year had a significant influence on the SSY of DWT, RI and the SSY of IPP. The mean age exerted an effect on the SSY of IPP, Qmax, PV and PVR. Sample size had an effect on the SSY of PCT, RI, IPP, and the SPY of IPP. The cut-off exerted impact on the SSY of RI, IPP, PV and the SPY of PCT and IPP, thus indicating that researchers need to unify the publication year, mean age, sample size, and/or cut-offs for the corresponding tests affected by these factors in future studies. In addition to this, although the risk of bias was generally low across most domains in most of the studies included in the present analysis, it is worth noting that all of the included studies were non-randomized trials. Only 14 studies applied the blinding methods, the remaining studies were unblinded or unknown. Furthermore, some studies adopted varying thresholds for the same index test and several studies applied different standards to define BOO in men. Therefore, blinding, study design, and the definitions used for BOO may also cause bias in the pooled data.
This was the first meta-analysis to explore the accuracy of non-invasive methods for diagnosing BOO in men. We performed a more comprehensive literature search to provide a newer and more complete dataset so that we could perform quantitative analysis. Nevertheless, there were several limitations. Firstly, we generally observed high levels of heterogeneity in the included studies for each type of index test. Secondly, all of the included studies were non-randomized trials, some were retrospective or were unblinded; this may have induced bias. Thirdly, some of the included studies adopted varying cut-offs or definitions for BOO, this may cause bias. Finally, only studies that were written in English were included; whether studies in other languages could have influenced our results remains unknown.
This meta-analysis provided relatively good evidence for the diagnostic accuracy of some non-invasive tests, this evidence is not sufficient to provide a new gold standard. However, larger studies, with more stringent methodological standards and larger sample sizes, are now required to better evaluate their value in the diagnosis of BOO in men with LUTS. Of the non-invasive tests tested, DWT and PCT had the highest levels of diagnostic accuracy for diagnosing BOO in men with LUTS. DWT, with a 2 mm cut-off, had the highest level of accuracy. These two methods represent good options as non-invasive tools for evaluating BOO in males.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
SX and YC performed the experiment and wrote the paper. TL, XW, QL, KR, XY, ZC and GD performed the research and analyzed data. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer MX declared a shared affiliation, with no collaboration, with the authors at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2022.986679/full#supplementary-material.
1. Hutchison A, Farmer R, Chapple C, Berges R, Pientka L, Teillac P, et al. Characteristics of patients presenting with LUTS/BPH in six European countries. Eur Urol. (2006) 50:555–61. doi: 10.1016/j.eururo.2006.05.001
2. Radomski SB, Herschorn S, Naglie G. Acute urinary retention in men: a comparison of voiding and nonvoiding patients after prostatectomy. J Urol. (1995) 153:685–8. doi: 10.1016/S0022-5347(01)67686-9
3. Nitti VW. Pressure flow urodynamic studies: the gold standard for diagnosing bladder outlet obstruction. Rev Urol. (2005) 7(Suppl 6):S14–21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1477621/pdf/riu007006_S014.pdf16986024
4. Shaw C, Williams K, Assassa PR, Jackson C. Patient satisfaction with urodynamics: a qualitative study. J Adv Nurs. (2000) 32:1356–63. doi: 10.1046/j.1365-2648.2000.01627
5. Malde S, Nambiar AK, Umbach R, Lam TB, Bach T, Bachmann A, et al. European association of urology non-neurogenic male LUTS guidelines panel. Systematic review of the performance of noninvasive tests in diagnosing bladder outlet obstruction in men with lower urinary tract symptoms. Eur Urol. (2017) 71:391–402. doi: 10.1016/j.eururo.2016.09.026
6. Swavely NR, Speich JE, Stothers L, Klausner AP. New diagnostics for male lower urinary tract symptoms. Curr Bladder Dysfunct Rep. (2019) 14:90–7. doi: 10.1007/s11884-019-00511-0
7. Belal M, Abrams P. Noninvasive methods of diagnosing bladder outlet obstruction in men. Part 1: nonurodynamic approach. J Urol. (2006) 176:22–8. doi: 10.1016/S0022-5347(06)00569-6
8. Belal M, Abrams P. Noninvasive methods of diagnosing bladder outlet obstruction in men. Part 2: noninvasive urodynamics and combination of measures. J Urol. (2006) 176:29–35. doi: 10.1016/S0022-5347(06)00570-2
9. Griffiths CJ, Pickard RS. Review of invasive urodynamics and progress towards non-invasive measurements in the assessment of bladder outlet obstruction. Indian J Urol. (2009) 25:83–91. doi: 10.4103/0970-1591.45544
10. Mangera A, Chapple C. Modern evaluation of lower urinary tract symptoms in 2014. Curr Opin Urol. (2014) 24:15–20. doi: 10.1097/MOU.0000000000000013
11. Mangera A, Osman NI, Chapple CR. Assessment of BPH/BOO. Indian J Urol. (2014) 30(2):177–80. doi: 10.4103/0970-1591.126902
12. Parsons BA, Bright E, Shaban AM, Whitehouse A, Drake MJ. The role of invasive and non-invasive urodynamics in male voiding lower urinary tract symptoms. World J Urol. (2011) 29:191–7. doi: 10.1007/s00345-009-0488-8
13. Pickard R, Griffiths C. Noninvasive methods of diagnosing bladder outlet obstruction. Indian J Urol. (2009) 25:81–2. doi: 10.4103/0970-1591.45543
14. Sahai A, Seth J, Aa FVD, Panicker J, Ridder D, Dasgupta P. Current state of the art in non-invasive urodynamics. Curr Bladder Dysfunct Rep. (2013) 8:83–91. doi: 10.1007/s11884-013-0181-z
15. Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. (2011) 155:529–36. doi: 10.7326/0003-4819-155-8-201110180-00009
16. Irwig L, Tosteson AN, Gatsonis C, Lau J, Colditz G, Chalmers TC, et al. Guidelines for meta-analyses evaluating diagnostic tests. Ann Intern Med. (1994) 120:667–76. doi: 10.7326/0003-4819-120-8-199404150-00008
17. Moses LE, Shapiro D, Littenberg B. Combining independent studies of a diagnostic test into a summary ROC curve: data-analytic approaches and some additional considerations. Stat Med. (1993) 12:1293–316. doi: 10.1002/sim.4780121403
18. Devillé WL, Buntinx F, Bouter LM, Montori VM, de Vet HC, van der Windt DA, et al. Conducting systematic reviews of diagnostic studies: didactic guidelines. BMC Med Res Methodol. (2002) 2:9. doi: 10.1186/1471-2288-2-9
19. Reitsma JB, Glas AS, Rutjes AW, Scholten RJ, Bossuyt PM, Zwinderman AH. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J Clin Epidemiol. (2005) 58:982–90. doi: 10.1016/j.jclinepi.2005.02.022
20. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Br Med J. (2003) 327:557. doi: 10.1136/bmj.327.7414.557
21. Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol. (2005) 58:882–93. doi: 10.1016/j.jclinepi.2005.01.016
22. Poulsen AL, Schou J, Puggaard L, Torp-Pedersen S, Nordling J. Prostatic enlargement, symptomatology and pressure/flow evaluation: interrelations in patients with symptomatic BPH. Scand J Urol Nephrol Suppl. (1994) 157:67–73. https://www.scopus.com/record/display.uri?eid=2-s2.0-0028183089/origin=inward7524143
23. Comiter CV, Sullivan MP, Schacterle RS, Yalla SV. Prediction of prostatic obstruction with a combination of isometric detrusor contraction pressure and maximum urinary flow rate. Urology. (1996) 48:723–9. doi: 10.1016/S0090-4295(96)00420-7
24. Valentini FA, Nelson PP, Besson GR, Zimmern PE. Challenging the maximum flow rate: a new index of voiding dysfunction in men with benign prostatic enlargement. BJU Int. (2008) 101:995–9. doi: 10.1111/j.1464-410X.2008.07460.x
25. Ding YY, Lieu PK, Choo PW. Is the bladder “an unreliable witness” in elderly males with persistent lower urinary tract symptoms? Geriatr Nephrol Urol. (1997) 7:17–21. doi: 10.1023/a:1008299528728
26. DuBeau CE, Yalla SV, Resnick NM. Improving the utility of urine flow rate to exclude outlet obstruction in men with voiding symptoms. J Am Geriatr Soc. (1998) 46:1118–24. doi: 10.1111/j.1532-5415.1998.tb06650.x
27. Reynard JM, Yang Q, Donovan JL, Peters TJ, Schafer W, Rosette JJ, et al. The ICS-'BPH’ study: uroflowmetry, lower urinary tract symptoms and bladder outlet obstruction. Br J Urol. (1998) 82:619–23. doi: 10.1046/j.1464-410x.1998.00813.x
28. Kuo HC. Clinical prostate score for diagnosis of bladder outlet obstruction by prostate measurements and uroflowmetry. Urology. (1999) 54:90–6. doi: 10.1016/s0090-4295(99)00092-8
29. Bøtker-Rasmussen I, Bagi P, Jørgensen JB. Is bladder outlet obstruction normal in elderly men without lower urinary tract symptoms? Neurourol Urodyn. (1999) 18:545–51. doi: 10.1002/(sici)1520-6777(1999)18:6%3C545::aid-nau2%3E3.0.co;2-1
30. Kojima M, Ochiai A, Naya Y, Okihara K, Ukimura O, Miki T. Doppler resistive index in benign prostatic hyperplasia: correlation with ultrasonic appearance of the prostate and infravesical obstruction. Eur Urol. (2000) 37:436–42. doi: 10.1159/000020165
31. Steele GS, Sullivan MP, Sleep DJ, Yalla SV. Combination of symptom score, flow rate and prostate volume for predicting bladder outflow obstruction in men with lower urinary tract symptoms. J Urol. (2000) 164:344–8. doi: 10.1016/S0022-5347(05)67356-9
32. Sullivan MP, Yalla SV. Penile urethral compression-release maneuver as a non-invasive screening test for diagnosing prostatic obstruction. Neurourol Urodyn. (2000) 19:657–69. doi: 10.1002/1520-6777(2000)19:6%3C657::aid-nau3%3E3.0.co;2-r
33. Oelke M, Höfner K, Wiese B, Grünewald V, Jonas U. Increase in detrusor wall thickness indicates bladder outlet obstruction (BOO) in men. World J Urol. (2002) 19:443–52. doi: 10.1007/s00345-001-0238-z
34. Watanabe T, Miyagawa I. New simple method of transabdominal ultrasound to assess the degree of benign prostatic obstruction: size and horizontal shape of the prostate. Int J Urol. (2002) 9(4):204–9. doi: 10.1046/j.1442-2042.2002.00450.x
35. Belenky A, Abarbanel Y, Cohen M, Yossepowitch O, Livne PM, Bachar GN. Detrusor resistive index evaluated by Doppler ultrasonography as a potential indicator of bladder outlet obstruction. Urology. (2003) 62:647–50. doi: 10.1016/s0090-4295(03)00510-7
36. Chia SJ, Heng CT, Chan SP, Foo KT. Correlation of intravesical prostatic protrusion with bladder outlet obstruction. BJU Int. (2003) 91:371–4. doi: 10.1046/j.1464-410x.2003.04088.x
37. Salinas J, Vírseda M, Arredondo F. Validity of cuff-uroflow as a diagnostic technique for bladder outlet obstruction in males. Scand J Urol Nephrol. (2003) 37:316–21. doi: 10.1080/00365590310001610
38. Aganovic D. The role of uroflowmetry in diagnosis of infravesical obstruction in the patients with benign prostatic enlargement. Med Arh. (2004) 58:109–11. https://www.scopus.com/record/display.uri?eid=2-s2.0-2542477308/origin=inward
39. Harding CK, Robson W, Drinnan MJ, Griffiths CJ, Ramsden PD, Pickard RS. An automated penile compression release maneuver as a noninvasive test for diagnosis of bladder outlet obstruction. J Urol. (2004) 172:2312–5. doi: 10.1097/01.ju.0000144027.75838.60
40. Griffiths CJ, Harding C, Blake C, McIntosh S, Drinnan MJ, Robson WA, et al. A nomogram to classify men with lower urinary tract symptoms using urine flow and noninvasive measurement of bladder pressure. J Urol. (2005) 174:1323–6. doi: 10.1097/01.ju.0000173637.07357.9e
41. Nose H, Foo KT, Lim KB, Yokoyama T, Ozawa H, Kumon H. Accuracy of two noninvasive methods of diagnosing bladder outlet obstruction using ultrasonography: intravesical prostatic protrusion and velocity-flow video urodynamics. Urology. (2005) 65:493–7. doi: 10.1016/j.urology.2004.10.014
42. Kessler TM, Gerber R, Burkhard FC, Studer UE, Danuser H. Ultrasound assessment of detrusor thickness in men-can it predict bladder outlet obstruction and replace pressure flow study? J Urol. (2006) 175:2170–3. doi: 10.1016/S0022-5347(06)00316-8
43. Lim KB, Ho H, Foo KT, Wong MY, Fook-Chong S. Comparison of intravesical prostatic protrusion, prostate volume and serum prostatic-specific antigen in the evaluation of bladder outlet obstruction. Int J Urol. (2006) 13:1509–13. doi: 10.1111/j.1442-2042.2006.01611.x
44. Oelke M, Höfner K, Jonas U, Rosette JJ, Ubbink DT, Wijkstra H. Diagnostic accuracy of noninvasive tests to evaluate bladder outlet obstruction in men: detrusor wall thickness, uroflowmetry, postvoid residual urine, and prostate volume. Eur Urol. (2007) 52:827–34. doi: 10.1016/j.eururo.2006.12.023
45. Reis LO, Barreiro GC, Baracat J, Prudente A, D'Ancona CA. Intravesical protrusion of the prostate as a predictive method of bladder outlet obstruction. Int Braz J Urol. (2008) 34:627–33. doi: 10.1590/s1677-55382008000500012
46. Ku JH, Cho SY, Oh SJ. Residual fraction as a parameter to predict bladder outlet obstruction in men with lower urinary tract symptoms. Int J Urol. (2009) 16:739–44. doi: 10.1111/j.1442-2042.2009.02354.x
47. Franco G, De Nunzio C, Leonardo C, Tubaro A, Ciccariello M, De Dominicis C, et al. Ultrasound assessment of intravesical prostatic protrusion and detrusor wall thickness–new standards for noninvasive bladder outlet obstruction diagnosis? J Urol. (2010) 183:2270–4. doi: 10.1016/j.juro.2010.02.019
48. Abdel-Aal A, El-Karamany T, Al-Adl AM, Abdel-Wahab O, Farouk H. Assessment of noninvasive predictors of bladder outlet obstruction and acute urinary retention secondary to benign prostatic enlargement. Arab J Urol. (2011) 9:209–14. doi: 10.1016/j.aju.2011.09.003
49. Pascual EM, Polo A, Morales G, Soto A, Rogel R, García G, et al. Usefulness of bladder-prostate ultrasound in the diagnosis of obstruction/hyperactivity in males with BPH. Arch Esp Urol. (2011) 64:897–903. https://www.scopus.com/record/display.uri?eid=2-s2.0-82155197316/origin=inward
50. Aganovic D, Hasanbegovic M, Prcic A, Kulovac B, Hadziosmanovic O. Which is a better indicator of bladder outlet obstruction in patients with benign prostatic enlargement–intravesical protrusion of prostate or bladder wall thickness? Med Arch. (2012) 66:324–8. doi: 10.5455/medarh.2012.66.324-328
51. Aganovic D, Prcic A, Hadziosmanovic O, Hasanbegovic M. Does the combination of intravesical prostatic protrusion and bladder outlet obstruction number increase test accuracy according to benign prostatic obstruction at the individual level? Acta Inform Med. (2012) 20:160–6. doi: 10.5455/aim.2012.20.160-166
52. Aldaqadossi HA, Elgamal SA, Saad M. The value of measuring the prostatic resistive index vs. pressure-flow studies in the diagnosis of bladder outlet obstruction caused by benign prostatic hyperplasia. Arab J Urol. (2012) 10:186–91. doi: 10.1016/j.aju.2011.12.011
53. Hossain AK, Alam AK, Habib AK, Rashid MM, Rahman H, Islam AK, et al. Comparison between prostate volume and intravesical prostatic protrusion in detecting bladder outlet obstruction due to benign prostatic hyperplasia. Bangladesh Med Res Counc Bull. (2012) 38:14–7. doi: 10.3329/bmrcb.v38i1.10446
54. Zhang X, Li G, Wei X, Mo X, Hu L, Zha Y, et al. Resistive index of prostate capsular arteries: a newly identified parameter to diagnose and assess bladder outlet obstruction in patients with benign prostatic hyperplasia. J Urol. (2012) 188:881–7. doi: 10.1016/j.juro.2012.04.114
55. ElSaied W, Mosharafa A, ElFayoumy H, Elghoniemy M, Ziada A, Elghamrawy H. Detrusor wall thickness compared to other non-invasive methods in diagnosing men with bladder outlet obstruction: a prospective controlled study. Afr J Urol. (2013) 19:160–64. doi: 10.1016/j.afju.2013.03.003
56. Shin SH, Kim JW, Kim JW, Oh MM, Moon du G. Defining the degree of intravesical prostatic protrusion in association with bladder outlet obstruction. Korean J Urol. (2013) 54:369–72. doi: 10.4111/kju.2013.54.6.369
57. Bianchi D, Di Santo A, Gaziev G, Miano R, Musco S, Vespasiani G, et al. Correlation between penile cuff test and pressure-flow study in patients candidates for trans-urethral resection of prostate. BMC Urol. (2014) 14:103. doi: 10.1186/1471-2490-14-103
58. Zhang M, Fu S, Zhang Y, Tang J, Zhou Y. Elastic modulus of the prostate: a new non-invasive feature to diagnose bladder outlet obstruction in patients with benign prostatic hyperplasia. Ultrasound Med Biol. (2014) 40:1408–13. doi: 10.1016/j.ultrasmedbio.2013.10.012
59. Kazemeyni SM, Otroj E, Mehraban D, Naderi GH, Ghadiri A, Jafari M. The role of noninvasive penile cuff test in patients with bladder outlet obstruction. Korean J Urol. (2015) 56:722–8. doi: 10.4111/kju.2015.56.10.722
60. Matulewicz RS, Hairston JC. The urocuff test: a non-invasive alternative to pressure flow studies in adult males with lower urinary tract symptoms secondary to bladder outlet obstruction. Can J Urol. (2015) 22:7896–901. https://www.scopus.com/record/display.uri?eid=2-s2.0-84939183162/origin=inward
61. Ahmed AF, Bedewi M. Can bladder and prostate sonomorphology be used for detecting bladder outlet obstruction in patients with symptomatic benign prostatic hyperplasia? Urology. (2016) 98:126–31. doi: 10.1016/j.urology.2016.08.033
62. Lee A, Lee HJ, Lim KB, Huang HH, Ho H, Foo KT. Can intravesical prostatic protrusion predict bladder outlet obstruction even in men with good flow? Asian J Urol. (2016) 3:39–43. doi: 10.1016/j.ajur.2015.10.002
63. Suzuki T, Otsuka A, Ozono S. Combination of intravesical prostatic protrusion and resistive index is useful to predict bladder outlet obstruction in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Int J Urol. (2016) 23:929–33. doi: 10.1111/iju.13188
64. Farag F, Elbadry M, Saber M, Badawy AA, Heesakkers J. A novel algorithm for the non-invasive detection of bladder outlet obstruction in men with lower urinary tract symptoms. Arab J Urol. (2017) 15:153–8. doi: 10.1016/j.aju.2017.01.002
65. Ko KJ, Suh YS, Kim TH, Sung HH, Ryu GH, Lee KS. Diagnosing bladder outlet obstruction using the penile cuff test in men with lower urinary tract symptoms. Neurourol Urodyn. (2017) 36:1884–9. doi: 10.1002/nau.23203
66. Aganovic D, Kulovac B, Bajramovic S, Kesmer A. Penile compression release Index revisited: evaluation and comparison with other noninvasive tools in the prediction of bladder outlet obstruction in men with benign prostatic enlargement. Med Arch. (2019) 73:81–6. doi: 10.5455/medarh.2019.73.81-86
67. Garg G, Sankhwar SN, Goel A, Pandey S, Sharma D, Parihar A. Evaluation of resistive index of the prostate and bladder sonomorphologic parameters as replacements for urodynamics to predict bladder outlet obstruction in patients with lower urinary tract symptoms suggestive of benign prostatic hyperplasia. Low Urin Tract Symptoms. (2019) 11:163–8. doi: 10.1111/luts.12256
68. Reddy SVK, Shaik AB. Non-invasive evaluation of bladder outlet obstruction in benign prostatic hyperplasia: a clinical correlation study. Arab J Urol. (2019) 17:259–64. doi: 10.1080/2090598X.2019.1660071
69. Kim KS, Choi YS, Bae WJ, Cho HJ, Lee JY, Hong SH, et al. Comparison of penile cuff test and conventional urodynamic study prior to photoselective vaporization of prostate for benign prostate hyperplasia using a 120 W greenlight high performance system laser. J Clin Med. (2020) 9:1189. doi: 10.3390/jcm9041189
70. Al-Mosawi HQ, Al-Aridy HM, Hameed HG. Accuracy of intravesical prostate protrusion measured by trans-abdominal ultrasound in predicting bladder outlet obstruction. Int J Pharm Res. (2020) 12:1150. doi: 10.31838/ijpr/2020.12.02.0170
71. Park J, Suh J, Yoo S, Cho MC, Son H. Bladder wall thickness and detrusor wall thickness can help to predict the bladder outlet obstruction in men over the age of 70 years with symptomatic benign prostatic hyperplasia. Investig Clin Urol. (2020) 61:491–7. doi: 10.4111/icu.20190376
72. Wadie BS. How correlated is BOO with different objective parameters commonly used in evaluation of BPH: a prospective study. Int Urol Nephrol. (2021) 53:635–40. doi: 10.1007/s11255-020-02707-4
73. Glas AS, Lijmer JG, Prins MH, Bonsel GJ, Bossuyt PM. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol. (2003) 56:1129–35. doi: 10.1016/s0895-4356(03)00177-x
Keywords: lower urinary tract symptoms, bladder outlet obstruction, non-invasive methods, diagnosis, meta-analysis
Citation: Cheng Y, Li T, Wu X, Ling Q, Rao K, Yuan X, Chen Z, Du G and Xu S (2022) The diagnostic value of non-invasive methods for diagnosing bladder outlet obstruction in men with lower urinary tract symptoms: A meta-analysis. Front. Surg. 9:986679. doi: 10.3389/fsurg.2022.986679
Received: 5 July 2022; Accepted: 5 September 2022;
Published: 20 September 2022.
Edited by:
Petros Sountoulides, Aristotle University of Thessaloniki, GreeceReviewed by:
Mingxing Xie, Huazhong University of Science and Technology, China© 2022 Cheng, Li, Wu, Ling, Rao, Yuan, Chen, Du and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shengfei Xu c2Z4dUB0amgudGptdS5lZHUuY24=
Specialty Section: This article was submitted to Genitourinary Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.