 Francesca Salamanna1
Francesca Salamanna1 Deyanira Contartese1*
Deyanira Contartese1* Matilde Tschon1
Matilde Tschon1 Veronica Borsari1
Veronica Borsari1 Cristiana Griffoni2Alessandro Gasbarrini2
Cristiana Griffoni2Alessandro Gasbarrini2 Milena Fini3
Milena Fini3
- 1Complex Structure Surgical Sciences and Technologies, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy
- 2Spine Surgery, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy
- 3Scientific Direction, IRCCS Istituto Ortopedico Rizzoli, Bologna, Italy
In the last decade, numerous studies analyzed and described the surgical outcomes in male and female patients submitted to orthopedic surgery. Although this, the impact of sex/gender on spinal fusion surgery clinical outcomes is still poorly defined. This review systematically maps and synthesizes the scientific literature on sex/gender differences in postoperative outcomes for patients undergoing spinal fusion surgery. The search was performed in PubMed, Scopus, and Web of Science in the last 22 years. Clinical studies evaluating potential sex/gender differences in postoperative outcomes and/or complications, as primary or secondary aim, were included and analyzed. Out of the 1,885 records screened, 47 studies were included. These studies comprised a total of 1,158,555 patients (51.31% female; 48.69% male). About 77% of the analyzed studies reported sex/gender-related differences in postoperative outcomes. Most studies treated patients for lumbar degenerative diseases and more than 55% of them reported a worse postoperative outcome in female patients in terms of pain, disability, health-related quality of life questionnaires, and complications. Differently, a significant heterogeneity across studies on patients treated for cervical and sacral degenerative diseases as well as for spinal deformity and traumatic spinal fracture prevented the understanding of specific sex/gender differences after spinal fusion surgery. Despite this, the present review highlighted those female patients treated for lumbar degenerative spine diseases could require more clinical awareness during postoperative care. The understanding of how sex/gender differences can really affect clinical outcomes after spinal fusion surgeries is mandatory for all spinal pathological conditions to drive clinical research toward oriented and personalized protocols.
Introduction
In the last decade, sex/gender differences attracted considerable interest in several specialties, including cardiothoracic and trauma surgery (1). These differences are key issues for a personalized treatment. The National Institutes of Health (NIH) promotes investigators to design their studies in a way that allows the participants to self-identify their sex or gender (2). By sex, we mean the biological character of male and female as opposed to gender, which reflects societal roles and expectations (2). Although, sex and gender are two different concepts, in medicine they are often linked, and, in the review, they were used as synonyms. Within orthopedic surgery, a patient's sex/gender is thought to influence outcomes after total joint arthroplasty (manly in total knee arthroplasty), after rotator cuff repair, and after anterior shoulder surgical stabilization (3). Sex-based differences in spinal disease incidence have been previously described in several studies, such as lumbar degenerative disc disease (4), lumbar radiculopathy (5), and cauda equina syndrome (6). Nevertheless, Taylor et al. (7) highlighted that male patients generally receive more recommendations than female ones for spine surgery despite similar underlying disorders (7). The impact of male or female sex/gender on clinical outcomes in spinal fusion surgery is less well defined. This is in part because most of the studies do not consider patient sex when examining demographic trends in outcomes, reporting “sex-adjusted” statistics, or using sex-matched groups. Despite this, some data demonstrated individual differences in the postoperative outcomes between male and female patients after spinal fusion surgery. In detail, several clinical trials found a better global and functional outcome after lumbar spine fusion for males than for females. A retrospective study by Gehrchen et al. (8) reported that the female gender is an independent risk factor for nonoptimal outcomes after lumbar fusion; a randomized controlled trial (9) observed that the female gender was also associated with worse postoperative results (10). However, a prospective clinical study on 4,780 patients in the Swedish National Spine Register with lumbar degenerative disc disease and chronic low back pain showed that female patients had worse pain and function preoperatively but improved more than males after surgery (11). These conflicting results are due to the fact that several of the studies are limited to small samples size, which has insufficient power to reach accurate conclusions. Regarding complications, there are several hypothetical reasons for male and female differences after spinal surgery. Differences in anthropomorphic parameters, body mass index, and comorbidity may contribute to differences in complications and mortality risks between females and males after spine surgery (12–14). Additionally, specific differences in tobacco and alcohol use/abuse as well as in unhealthy lifestyles (malnutrition, unhealthy diet, drug abuse, etc.) might also increase the odds of postoperative death or the development of specific complications, such as surgical site infection (SSI) (15).
The number of studies suggesting that sex/gender may affect patient outcomes after a spinal fusion procedure begets the need for a comprehensive examination of these data. Thus, we performed a systematic review of the literature to better understand sex/gender-based differences in spinal fusion surgery outcomes. These aspects are of key interest for both physician and patient thus, to be informed about predictive gender and sex-related differences. This information could also have a prognostic value, playing a critical role in the decision-making process.
Methods
Eligibility criteria
The PICOS model (Population, Intervention, Comparison, Outcomes, Study design) was used to design this study: (1) studies that considered female and male patients (Population) submitted to, (2) spinal fusion surgery (Interventions), (3) with a comparison between them (female and male) (Comparisons), (4) that reported postoperative clinical and/or functional outcomes of spinal fusion surgery (Outcomes), in (5) randomized, retrospective, prospective and case series studies (Study design). Studies from May 2000 to May 2022 were included in this review if they met the PICOS criteria. We excluded studies that evaluated (1) surgeries other than the spine, (2) patients undergoing spine surgery with other severe pathological conditions (genetic and rare diseases, diffuse metastases, advanced neurodegenerative disorders), and (3) articles with incomplete outcomes or data. Additionally, we excluded reviews, case reports, letters, comments to editors, in vivo and in vitro studies, pilot studies, meta-analyses, editorials, protocols and recommendations, guidelines, and articles not written in English.
Search strategies
Our literature review involved a systematic search conducted in May 2022. We performed our review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (16). The search was carried out on three databases: PubMed, Scopus, and Web of Science Core Collection. The following combination of terms was used (spinal fusion OR spinal arthrodesis OR vertebral fusion OR vertebral arthrodesis) AND (gender differences OR sex differences OR gender-specific OR sex-specific), and for each of these terms, free words, and controlled vocabulary specific to each bibliographic database were combined using the operator “OR.” The combination of free-vocabulary and/or Medical Subject Headings (MeSH) terms for the identification of studies in PubMed, Scopus, and Web of Science Core Collection were reported in Supplementary Table S1.
Selection process
After submitting the articles to a public reference manager (Mendeley Desktop 1.19.8) to eliminate duplicates, possible relevant articles were screened using the title and abstract by three reviewers (FS, DC, and MT). Studies that did not meet the inclusion criteria were excluded from review and any disagreement was resolved through discussion until a consensus was reached, or with the involvement of a fourth reviewer (MF). Subsequently, the remaining studies were included in the final stage of data extraction.
Data collection process and synthesis methods
The data extraction and synthesis process started with cataloging the studies' details. To increase validity and avoid omitting potentially findings for the synthesis, three authors (MT, VB, and CG) extracted and performed tables taking into consideration: the study design, female and male patients' number and age, type of surgery (indication and operation types), presence of comorbidities, complications, main objectives related to sex/gender, follow-up, assessment measures, pre-and postoperative quantitative measures, complications, and outcomes/endpoints (specific sex/gender differences).
Assessment of methodological quality
The methodological quality of the selected studies was independently assessed by two reviewers (DC and FS), using the Cochrane risk-of-bias tool RoB for randomized trials and the Cochrane risk of bias ROBINS-I for nonrandomized studies of interventions (17). The tool for randomized trials included five domains, which assessed the possible sources of bias: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in the measurement of the outcome, and bias in the selection of the reported result. For each domain were assigned one of three levels: low risk of bias, some concerns, or high risk of bias until an overall bias risk judgment is reached. The tool for nonrandomized trials included seven domains, which assessed the possible sources of bias: bias due to confounding, bias in the selection of participants into the study, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in the measurement of the outcome, and bias in the selection of the reported result. For each domain were assigned one of three levels: low risk of bias, moderate risk of bias, or high risk of bias until an overall bias risk judgment is reached. In case of disagreement, the reviewers attempted to reach a consensus by discussion; if this failed, a third reviewer (MF) was consulted to make the final decision.
Results
Study selection and characteristics
The initial literature search retrieved 1,885 studies. Of those, 798 studies were identified using PubMed, 435 using Scopus, and 652 were found in the Web of Science Core Collection. Articles were screened for title and abstract and 100 articles were selected. Subsequently, these articles were submitted to a public reference manager to eliminate duplicates. The resulting 77 complete articles were then reviewed to establish whether the publications met the inclusion criteria, and 47 studies were considered eligible for this review. Search strategy and study inclusion and exclusion criteria are detailed in Figure 1. Of these articles, 33 were retrospective studies, 12 were prospective studies, 1 was a case series, and another 1 was a randomized clinical trial (RCT).
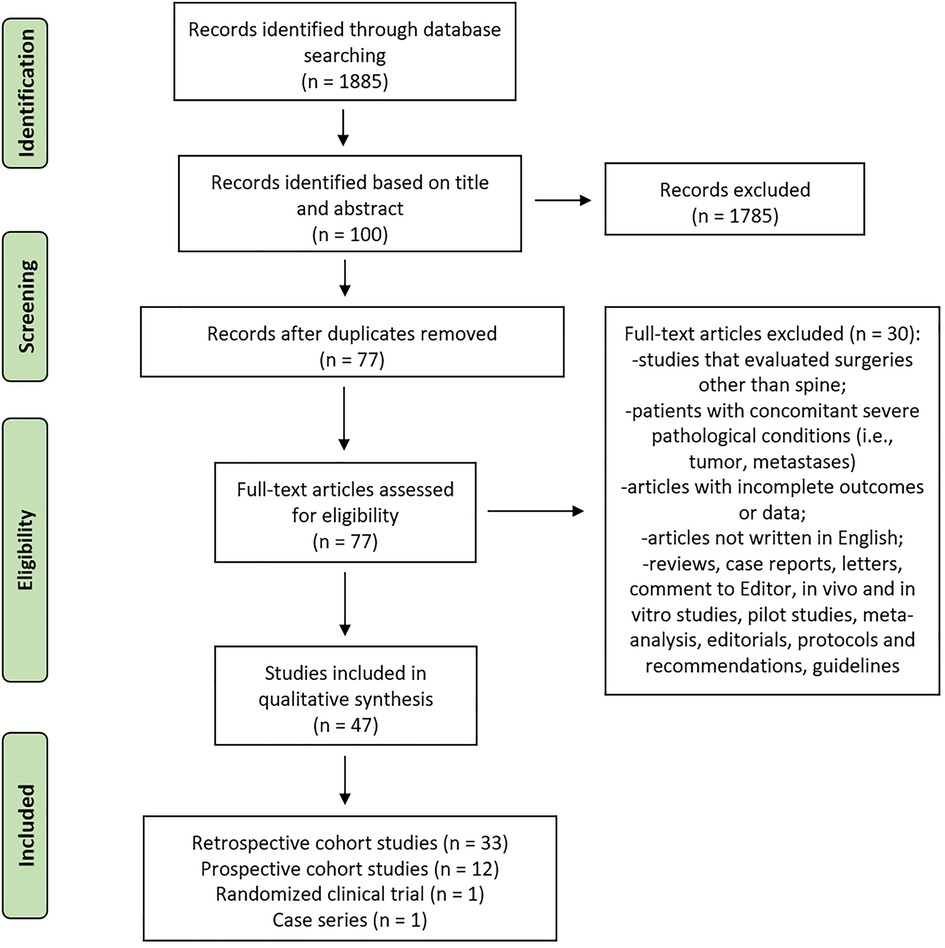
Figure 1. Systematic review flow diagram. The PRISMA flow diagram for the systematic review detailing the database searches, the number of abstracts screened, and the full texts retrieved.
Assessment of methodological quality
In our quality assessment, the randomized trial is judged to raise some concerns, but not to be at high risk of bias for any domain. The risk of bias was mainly about the randomization process and measurement of the outcome. The 70% of the nonrandomized studies were rated at low risk of bias for all domains, 21% were rated at moderate risk of bias, and 9% were rated at critical risk of bias. Methodological weaknesses that led to moderate or weak quality scores often included bias due to confounding, missing data, deviations from intended interventions, and bias in the measurement of the outcome. Risks of bias assessments for each randomized and nonrandomized study were reported in Supplementary Tables S2 and S3.
Studies general information, objectives, and cohort characteristics
Descriptive characteristics of each study are presented in Tables 1 and 2. The included studies involved a total of 1,158,555 patients. The overall percentages of female and male patients were 51.31% and 48.69%, respectively. Apart from five studies evaluating adolescent patients, the others consider patients operated at a mean age of 55.55 ± 7.38 years. Most studies (n = 23) examined the association between sex/gender and clinical outcomes in relation to a general clinical assessment and/or to specific scores. Eighteen studies also evaluated the association between sex/gender and postoperative complications, such as intensive care unit (ICU) admission, superficial and deep SSI, postoperative fractures, cardiac events, heterotopic ossifications, instrumentation failure and reoperation rate, length of stay (LOS), or specific risk factors (opioid use, smoking, obesity). Furthermore, one study examined sex/gender differences in relation to recombinant human bone morphogenetic protein-2 (rhBMP2) use during spinal fusion surgery.
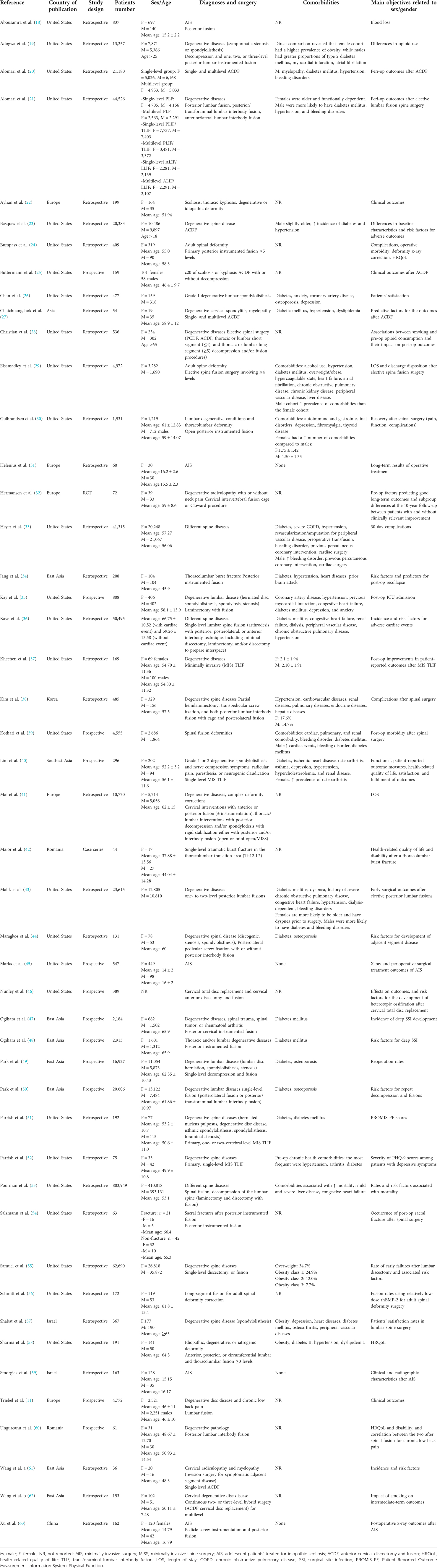
Table 1. Studies general information.

Table 2. Clinical assessment and outcomes.
Examining sex/gender differences was the primary objective in 25 (52.1%) studies while the remaining evaluated the influence of several predictors and risk factors (age, smoking history, number, and location of fusion segments, plate-to-disc distances, excessive disc space distraction, kyphotic malalignment), also including sex/gender as a secondary aim.
Comorbidities were assessed in 63.8% of the studies (n = 30). In two of these studies, no comorbidities were present. In the remaining 28 studies, different comorbidities were present that include diabetes (in 50% of included studies), cardiac diseases (25%) and/or hypertension (17.8%), blending disorders (14.2%), pulmonary diseases (10.7%), obesity and overweight (10.7%), osteoporosis (7.1%), dyslipidemia (7.1%), renal diseases (7.1%), osteoarthritis (7.1%), depression (7.1%), and others less common comorbidity, i.e., liver diseases, brain attack, vascular diseases, asthma, and anxiety. In 12/27 studies where comorbidities were present and described gender-related differences in comorbidities distribution were also reported. The major comorbidity reported in females was obesity while in males were diabetes, cardiovascular morbidities (prevalently atrial fibrillation and hypertension), and bleeding disorders.
Qualitative and quantitative measures used for patient assessment were detailed in Table 1. The Visual Analogue Scale (VAS) score for back or leg pain was used, alone or in association with other measurements, by 21.2% of the studies, the Oswestry Disability Index (ODI) by 25.5% of studies, x-ray, to evaluate pre-and postoperative sized main curves, sagittal Cobb angle, kyphosis, by 27.6% and specific patient-reported outcomes measures and standardized measure of health-related quality of life (HRQoL) by 42.5% of studies. Other less common measures used include the numeric rating scale (NRS) scores for low back pain (NRS-BP), leg pain (NRS-LP), Japanese Orthopedic Association (JOA) scale, magnetic resonance imaging (MRI), computed tomography (CT), and laboratory values. Except for one study that evaluated sex/gender differences at discharge, all other studies performed clinical assessments from 30-day of follow-up up to 10 years.
Types of spine surgery and pathological conditions
Patients were diagnosed with different spine diseases, mainly degenerative pathological conditions such as disc herniation, stenosis, spondylolysis, radiculopathy, spondylolisthesis, myelopathy (55.3%), spinal deformities as adult scoliosis or kyphosis (12.7%), adolescent idiopathic scoliosis (10.6%), degenerative and deformity conditions together (14.8%), and traumatic pathologies such as fractures (6.3%). In detail, 235,140 patients (26 studies) were treated for degenerative diseases using anterior or posterior approaches (Table 1). Of these, 17 studies were retrospective and analyzed 188,278 patients, 8 were prospective and included 46,862 patients, and 1 study was an RCT with 72 patients. A total of five studies (four retrospective and one prospective) analyzed 1,769 adolescent patients' treated for idiopathic scoliosis (AIS) using a posterior approach. Concerning adult deformities, a total of 4,714 patients were evaluated in two prospective studies and 5,752 patients in four retrospective studies, using anterior or posterior approaches. Studies that analyzed degenerative and deformity conditions together (six retrospective studies and one prospective) evaluated 910,835 patients. Finally, 315 patients (three studies) were treated for traumatic sacral or thoracolumbar fractures after posterior instrumented fusion. Of these, two studies were retrospective with 271 patients, and one study was a case series with 44 patients.
Procedures associated with spinal fusion surgery included minor, major, and complex surgeries, such as posterior lumbar interbody fusion (PLIF), hemilaminectomy, decompression, anterior cervical discectomy and fusion (ACDF), transforaminal lumbar interbody fusion (TLIF), discectomy, anterior lumbar interbody fusion (ALIF) and laminectomy (Table 1). Because the types of spine fusion surgery were not standardized across the 47 studies, it was difficult to quantify the prevalence of any single type of procedure among the studies. However, most interventions were implemented for lumbar spine procedures, through techniques such as PLIF and TLIF, followed by cervical procedures such as ACDF.
Sex/gender differences in outcomes after spinal fusion surgery
In this review, 76.6% (n = 36) of studies reported sex/gender-related differences in postoperative clinical outcomes and/or complications, while the remaining studies described comparable results between males and females (Table 2). Of these 36 studies where sex/gender differences were present, n = 21 (58.3%) were on degenerative diseases, prevalently of the lumbar spine, 13.9% were on spine deformities (1 on AIS and 4 on adult deformities), 8.4% on spine fractures, and 19.4% considered degenerative conditions and deformities together (Table 1).
Degenerative spine diseases
More than half of studies on degenerative spine diseases on the lumbar spine reported worse female experiences after spinal fusion surgery (63.8%). Kay et al. showed that the female gender was associated with an increased risk of postoperative ICU admission in patients undergoing lumbar spine surgery (35). Furthermore, Maragkos et al. also reported that female patients were 2.55 times more likely than male ones to develop adjacent segment disease requiring reoperation (44). In detail, within 30 days of follow-up female gender resulted in an independent risk factor significantly associated with a LOS longer than 3 days, occurrence of complications, including wound complications, urinary tract infection (UTI), and nonhome discharge; while the adverse outcomes associated with males were renal complication and myocardial infarction (20, 43). At the same follow-up female gender also resulted in an increased risk of readmission for pain or neurological symptoms (55). At a longer follow-up, 1 year, it was analyzed the influence that gender plays on HRQoL, disability, and the correlation between these two in patients undergoing spinal fusion for chronic low back pain (60). Results showed that male patients had higher disability scores at the preoperative evaluation but improved more than females in all domains of disability postoperatively. HRQoL improved similarly in both genders. The ODI score showed a strong or moderate correlation with six of the domains of the Short Form Health Survey 36 (SF-36) in males, but with only three domains in females (60). At the same follow-up, it was also shown that gender differences influence the satisfaction rate of lumbar spinal stenosis surgery in elderly patients (≥65 years) with female patients that had less satisfactory results than male ones (57). After 2 years of follow-up, it was shown that the female gender was also associated with prolonged opioid use (19). Several studies reported different results. Parrish et al. reported that females experienced significantly more improvement in postoperative Patient-Reported Outcome Measurement Information System-Physical Function (PROMIS-PF) score than males at the 3-month time point (51). Chan et al. reported that at 1 year of follow-up, the female gender resulted also associated with more satisfaction than males (58.4% vs. 38.5%) (26). These results were further confirmed by Triebel et al. where it was shown that females had a high rate of improvement from baseline to follow-up (2 years) in leg pain, back pain, HRQoL, and disability, in comparison to males, but it was also reported that females improve more slowly in leg pain, back pain, and disability (11). At longer follow-up (up to 4.5 years), Park et al. showed that the male gender was a risk factor for reoperation (49, 50).
In cervical degenerative diseases at 1 year of follow-up a higher percentage of improvement was detected in male patients than in females (27). This result was also confirmed at 10 years of follow-up, where it was demonstrated a higher neck- and arm-related pain intensity, more disability, and worse psychosocial status in females than in males (32). Specifically, the male gender was a predictor of clinically relevant improvement in neck-specific disability (32). Differently, Nunley et al. (46) showed that males were ∼3 times more likely to develop heterotopic ossification than females as well as they were at greater risk of any adverse event (23). Alomari et al. (21) described an increased risk for UTI in females and myocardial infarction in males. Two studies also evaluated the correlation between gender, spinal fusion surgery, and smoking. A higher proportion of male smokers who underwent posterior cervical decompression and fusion (PCDF) compared to female smokers (9.93% vs. 5.98%) was detected (28). In addition, a significant difference in the early fusion process among current smokers, former smokers, and nonsmokers was detected for male patients, but no significant differences were founded at 1-year of follow-up. For female patients, statistical differences were found in both the early fusion process and the 1-year fusion rate (62).
The only study on sex/gender differences considering thoracic spine surgery was by Ogihara et al. using a multivariate analysis that showed that male gender was significantly correlated with a higher incidence of deep SSI, although it was not a significant factor in univariate analysis (48).
Spine deformities
Of the 36 studies where sex/gender differences were evaluated, n = 4 were on adult spinal deformities. Two studies reported that female sex/gender was associated with increased postoperative morbidity compared to males; after 30 days from spinal surgery, it was observed an increased postoperative transfusion rate and complications, in particular, UTI and LOS longer than 5 days, in female patients (29, 39). Conversely, one study reported that male patients were at a greater risk for bleeding compared to females (24). Differently, from the above-mentioned studies, Schmitt et al. evaluated at 2 years of follow-up the fusion rates using relatively low-dose rhBMP-2 for the treatment of adult spinal deformity surgery, showing that gender was associated with fusion status, with 79.8% of females with a good spinal fusion compared to 60.4% of males (56).
Only one study on AIS detected gender-related differences, showing that male patients, with severe thoracic lordosis, were at a higher risk of bleeding than females (18).
Degenerative conditions and deformities
Seven studies reported sex/gender-related differences considering patients treated for degenerative conditions and deformities together. In detail, at 30 days of follow-up, Heyer et al. (33) reported postoperative differences in complications between males and females. Females were at increased risk for superficial SSI, UTI, transfusions, and longer LOS while males were at increased risk of pneumonia and reintubation (33, 41). At the same experimental time, it was also shown that the male gender was associated with an increased risk of cardiac events (36). At a longer experimental time, 1-year follow-up, it was shown that the male gender represented a risk factor for deep SSI (47).
In a study on the mortality rates after spinal fusion surgery and on factors associated with its occurrence over a 10-year follow-up, it was shown that the male gender was a risk factor significantly associated with increased mortality rates (53). In addition to complications and risk factors related to gender, Gulbrandsen et al. (30) indicated that females reported slightly more pain and worse function than males at the time of surgery. Finally, Sharma et al. also showed that in spine surgeries gender interacted with obesity at 1 year of follow-up: obese males with at higher odds of improvement when compared to nonobese males; among females, obesity did not affect the odds of improvement (58).
Spine fractures
Of the 35 studies where sex/gender differences were present, n = 3 were on spine fractures after spinal fusion surgery. One study was on sacral fractures (54), and two studies were on thoracolumbar burst fractures (34, 42). Salzmann et al. observed, at a 6-month follow-up, that female gender (76.2%), advanced age (mean, 66.4 years), and obesity were risk factors for post-op sacral fractures (54). Differently, Jang et al. showed that the male gender was a risk factor for recollapse of thoracolumbar burst fractures (34). At 1-year follow-up, Maior et al. reported that male patients have better outcomes than females after thoracolumbar burst fractures; an increased score in each item of the SF-36 in male than female patients was also observed (42).
Discussion
From an epidemiological perspective, it would be critical to understand how sex/gender differences can affect clinical outcomes after spinal fusion surgery. This aspect becomes more critical from a surgical point of view since the identification of specific sex/gender differences would offer personalized approaches for patients undergoing spinal fusion procedures. Thus, the focus of this review was to analyze clinical studies aimed at evaluating sex/gender differences following spinal fusion surgery.
Our review showed that most of the analyzed studies (76.6%) report sex/gender-related differences in postoperative clinical status, outcomes, and/or complications, while the remaining described equivalent results. Furthermore, in 38.3% of the studies where comorbidities were described gender-related differences in their distribution were reported. In the female sex, obesity was the most prevalent comorbidity while in the male sex the prevalently dominant comorbidities were diabetes, cardiovascular morbidities (prevalently atrial fibrillation and hypertension), and bleeding disorders. These differences are of critical importance and could represent potential risk factors related to gender differences (both pre-op and post-op) to be analyzed in future studies, in which it will be mandatory to analyze a larger homogeneous cohort of patients, considering specific and individual spine diseases and surgical approaches. In fact, it is important to highlight that there is significant heterogeneity across the analyzed studies in terms of pathological spine diseases (degenerative, deformity, fracture), type of the spinal level treated (cervical, thoracic, lumbar, sacral), number of levels treated, and surgical approaches. In addition, it is important to underline that none of the analyzed studies evaluated specific physiological changes related to postmenopausal status in female patients submitted to spinal fusion procedures. It is known that the direct negative effects of estrogen-deficiency on bone as well as the indirect effects of altered immune status in postmenopausal women contribute to low bone mass and bone microarchitecture destruction. These bone alterations may represent a negative prognostic factor for the success of spinal fusion surgery.
In this review, most of the studies where sex/gender-related differences were present were on the patient treated for lumbar degenerative diseases (disc degeneration, disc herniation, and spondylolisthesis). Of those more than half reported a worse postoperative outcome in terms of pain, disability, HRQoL, and complications in female patients, while the remaining reported worse outcomes in terms of HRQoL and satisfaction in male patients. In studies examining pain, disability, and HRQoL differences between females and males, the complexity of evaluating these parameters which include many clinical signs and subjective outcomes must be considered. Undoubtedly, females treated for lumbar degenerative disease reported the worst postoperative scenario, but the perception and measurements of pain and disability have been debated and investigated: some studies concluded that females had lower perception thresholds and pain thresholds than males (64). This worst postoperative state in female patients is probably the reason for the prolonged postoperative opioid consumption associated with this gender (19). However, epidemiological studies have indicated that analgesic use may vary between males and females, suggesting that opioid use was higher in the female gender in general adult populations (65, 66). This systematic review found that females were also at increased risk of complications (UTI, readmission for pain or neurological symptoms, adjacent segment disease), and consequent longer LOS, following spinal fusion surgery for lumbar degenerative disease (20, 43, 44, 55). These postoperative complications may also have a link to the long-term opioid use detected in female patients. While for degenerative lumbar spine diseases a potential link between gender and clinical outcomes resulted more evident, for degenerative diseases of the cervical and thoracic spine this link is not so clear. This is probably due to the heterogenicity of the analyzed studies but also to the small number of studies found in this review. However, at 10-year to 13-year of follow-up, a prospective randomized study indicated that predictive factors of good outcome after ACDF included initial high neck-related pain intensity, nonsmoking status at the time of surgery, and male gender (32). On the contrary, other clinical studies indicated that males were more likely to develop clinically relevant heterotopic ossification than females as well as a greater risk of any adverse event, also severe (23). Similar contradictory results were also found after spinal deformity surgery, when degenerative diseases and deformities were considered and analyzed together and following spine fractures (sacral fractures and thoracolumbar burst fractures). Also, in these cases, the limited number of studies and the heterogeneity between studies remained critical factors that limit the interpretation of the results. For adult spinal deformities, a gender difference was founded by using relatively low-dose rhBMP-2 with the female gender demonstrating a better spinal fusion compared to of male one (56). In this study, there were substantial differences between the patient's series and those in the comparison groups. When degenerative diseases and deformities were considered and analyzed together it was also shown that gender interacted with obesity at 1 year of follow-up; obese males showed a higher odd of improvement when compared to nonobese males while among females, obesity did not affect the odds of improvement (58). Nevertheless, it should be noted that numerous studies present in the literature did not investigate and analyze spinal fusion outcomes dichotomizing by gender, thus it is difficult to establish a real conclusion and draw definitive results. As such, a true systematic review was not feasible. Furthermore, some limitations of this review warrant discussion. Most eligible studies in this review were retrospective and only one RCT on 47 analyzed studies was found and included. Additionally, many included studies had a small sample size and may be underpowered to identify significant clinical responses. Numerous studies, accounting for most patients, were prevalently published by groups in the United States; cultural discrepancies in patient-reported clinical assessment scores may differ geographically. The clinical assessment tools used to determine the postoperative outcomes are, prevalently, subjective patient-reported measures. Results were also difficult to interpret due to specific differences in spine diseases in the retrieved studies; for example, insufficient heterogenic data were retrieved for cervical and sacral degenerative diseases, spinal deformities, and traumatic spinal fractures. Furthermore, also searching for “spinal fusion” and “sex” or “gender” on the www.clinicaltrialg.gov website (accessed on 22 May 2022) no clinical trials had, as a primary or secondary outcome, the analysis of sex/gender differences.
Conclusions
The review highlighted those female patients treated for lumbar degenerative spine diseases probably require more clinical awareness during postoperative care. The understanding of how sex/gender differences can really affect clinical outcomes after spinal fusion surgeries have the potential to enhance clinical decision-making and care practices and may be crucially important in the context of providing patient personalized care, a critical field of contemporary medical practice.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
FS, DC, and MF contributed to the conceptualization of the study and to the writing—original draft preparation. FS, DC, MT, VB, and CG contributed to the methodology and data curation. FS, DC, AG, and MF contributed to the writing—review, and editing. AG and MF contributed to the supervision. MF contributed to the funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by grants from IRCCS Istituto Ortopedico Rizzoli (Ricerca Corrente), by 5X1000 2019 project entitled “Medicina rigenerativa e riparativa personalizzata per le patologie dei tessuti muscolo-scheletrici e la chirurgia ricostruttiva ortopedica” (PRWEB: 2021/730567).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2022.983931/full#supplementary-material.
References
1. Legato MJ, Johnson PA, Manson JE. Consideration of sex differences in medicine to improve health care and patient outcomes. JAMA. (2016) 316(18):1865–6. doi: 10.1001/jama.2016.13995
2. NIH policy on sex as a biological variable. Available at: https://orwh.od.nih.gov/sex-gender/nih-policy-sex-biological-variable (Accessed May 22, 2022).
3. MacDonald SJ, Charron KD, Bourne RB, Naudie DD, McCalden RW, Rorabeck CH. The John Insall Award: gender-specific total knee replacement: prospectively collected clinical outcomes. Clin Orthop Relat Res. (2008) 466(11):2612–6. doi: 10.1007/s11999-008-0430-1
4. Schoenfeld AJ, Nelson JH, Burks R, Belmont PJ Jr. Incidence and risk factors for lumbar degenerative disc disease in the United States military 1999–2008. Mil Med. (2011) 176(11):1320–4. doi: 10.7205/milmed-d-11-00061
5. Schoenfeld AJ, Laughlin M, Bader JO, Bono CM. Characterization of the incidence and risk factors for the development of lumbar radiculopathy. J Spinal Disord Tech. (2012) 25(3):163–7. doi: 10.1097/BSD.0b013e3182146e55
6. Schoenfeld AJ, Bader JO. Cauda equina syndrome: an analysis of incidence rates and risk factors among a closed North American military population. Clin Neurol Neurosurg. (2012) 114(7):947–50. doi: 10.1016/j.clineuro.2012.02.012
7. Taylor BA, Casas-Ganem J, Vaccaro AR, Hilibrand AS, Hanscom BS, Albert TJ. Differences in the work-up and treatment of conditions associated with low back pain by patient gender and ethnic background. Spine (Phila Pa 1976). (2005) 30(3):359–64. doi: 10.1097/01.brs.0000152115.79236.6e
8. Gehrchen PM, Dahl B, Katonis P, Blyme P, Tøndevold E, Kiaer T. No difference in clinical outcome after posterolateral lumbar fusion between patients with isthmic spondylolisthesis and those with degenerative disc disease using pedicle screw instrumentation: a comparative study of 112 patients with 4 years of follow-up. Eur Spine J. (2002) 11(5):423–7. doi: 10.1007/s00586-002-0401-2
9. Ekman P, Möller H, Shalabi A, Yu YX, Hedlund R. A prospective randomised study on the long-term effect of lumbar fusion on adjacent disc degeneration. Eur Spine J. (2009) 18(8):1175–86. doi: 10.1007/s00586-009-0947-3
10. Ekman P, Möller H, Hedlund R. Predictive factors for the outcome of fusion in adult isthmic spondylolisthesis. Spine (Phila Pa 1976). (2009) 34(11):1204–10. doi: 10.1097/BRS.0b013e3181a19e66
11. Triebel J, Snellman G, Sandén B, Strömqvist F, Robinson Y. Women do not fare worse than men after lumbar fusion surgery: two-year follow-up results from 4,780 prospectively collected patients in the Swedish National Spine Register with lumbar degenerative disc disease and chronic low back pain. Spine J. (2017) 17(5):656–62. doi: 10.1016/j.spinee.2016.11.001
12. Cahill KS, Chi JH, Day A, Claus EB. Prevalence, complications, and hospital charges associated with use of bone-morphogenetic proteins in spinal fusion procedures. JAMA. (2009) 302(1):58–66. doi: 10.1001/jama.2009.956
13. Schoenfeld AJ, Ochoa LM, Bader JO, Belmont PJ Jr. Risk factors for immediate postoperative complications and mortality following spine surgery: a study of 3475 patients from the National Surgical Quality Improvement Program. J Bone Joint Surg Am. (2011) 93(17):1577–82. doi: 10.2106/JBJS.J.01048
14. Shen Y, Silverstein JC, Roth S. In-hospital complications and mortality after elective spinal fusion surgery in the United States: a study of the nationwide inpatient sample from 2001 to 2005. J Neurosurg Anesthesiol. (2009) 21(1):21–30. doi: 10.1097/ANA.0b013e31818b47e9
15. Schoenfeld AJ, Reamer EN, Wynkoop EI, Choi H, Bono CM. Does patient sex affect the rate of mortality and complications after spine surgery? A systematic review. Clin Orthop Relat Res. (2015) 473(8):2479–86. doi: 10.1007/s11999-014-4102-z
16. Tugwell P, Tovey D. PRISMA 2020. J Clin Epidemiol. (2021) 134:A5–6. doi: 10.1016/j.jclinepi.2021.04.008
17. Cochrane training. Available at: https://training.cochrane.org/handbook/current (Accessed September 4, 2022).
18. Abousamra O, Sponseller PD, Lonner BS, Shah SA, Marks MC, Cahill PJ, et al. Thoracic lordosis, especially in males, increases blood loss in adolescent idiopathic scoliosis. J Pediatr Orthop. (2019) 39(3):e201–4. doi: 10.1097/BPO.0000000000001264
19. Adogwa O, Davison MA, Vuong V, Desai SA, Lilly DT, Moreno J, et al. Sex differences in opioid use in patients with symptomatic lumbar stenosis or spondylolisthesis undergoing lumbar decompression and fusion. Spine (Phila Pa 1976). (2019) 44(13):E800–7. doi: 10.1097/BRS.0000000000002965
20. Alomari S, Liu A, Westbroek E, Witham T, Bydon A, Lo SFL. Effect of patient’s sex on early perioperative outcomes following anterior cervical discectomy and fusion. J Clin Neurosci. (2021) 93:247–52. doi: 10.1016/j.jocn.2021.09.015
21. Alomari S, Liu A, Westbroek E, Witham T, Bydon A, Lo SFL. Influence of sex on early outcomes of elective lumbar fusions: an updated propensity-matched and subgroup analysis. World Neurosurg. (2021) 150:e388–99. doi: 10.1016/j.wneu.2021.03.025
22. Ayhan S, Yuksel S, Nabiyev V, Adhikari P, Villa-Casademunt A, Pellise F, et al. The influence of diagnosis, age, and gender on surgical outcomes in patients with adult spinal deformity. Global Spine J. (2018) 8(8):803–9. doi: 10.1177/2192568218772568
23. Basques BA, Hijji FY, Khechen B, Haws BE, Mayo BC, Massel DH, et al. Sex differences for anterior cervical fusion: complications and length of stay. Spine (Phila Pa 1976). (2018) 43(15):1025–30. doi: 10.1097/BRS.0000000000002512
24. Bumpass DB, Lenke LG, Gum JL, Shaffrey CI, Smith JS, Ames CP, et al. Male sex may not be associated with worse outcomes in primary all-posterior adult spinal deformity surgery: a multicenter analysis. Neurosurg Focus. (2017) 43(6):E9. doi: 10.3171/2017.9.FOCUS17475
25. Buttermann GR. Anterior cervical discectomy and fusion outcomes over 10 years: a prospective study. Spine (Phila Pa 1976). (2018) 43(3):207–14. doi: 10.1097/BRS.0000000000002273
26. Chan AK, Bisson EF, Bydon M, Glassman SD, Foley KT, Potts EA, et al. Women fare best following surgery for degenerative lumbar spondylolisthesis: a comparison of the most and least satisfied patients utilizing data from the Quality Outcomes Database. Neurosurg Focus. (2018) 44(1):E3. doi: 10.3171/2017.10.FOCUS17553
27. Chaichuangchok C, Nitising A, Phonwijit L, Jetjumnong C. Factors predicting outcomes of anterior cervical discectomy and fusion in cervical spondylotic myelopathy: a prospective study. J Med Assoc Thai. (2017) 100(4):96.
28. Christian ZK, Youssef CA, Aoun SG, Afuwape O, Barrie U, Johnson ZD, et al. Smoking has a dose-dependent effect on the incidence of preoperative opioid consumption in female geriatric patients with spine disease. J Clin Neurosci. (2020) 81:173–7. doi: 10.1016/j.jocn.2020.09.066
29. Elsamadicy AA, Freedman IG, Koo AB, David WB, Lee M, Kundishora AJ, et al. Influence of gender on discharge disposition after spinal fusion for adult spine deformity correction. Clin Neurol Neurosurg. (2020) 194:105875. doi: 10.1016/j.clineuro.2020.105875
30. Gulbrandsen MT, Lara N, Beauchamp JA, Chung A, Chang M, Crandall D. Early gender differences in pain and functional recovery following thoracolumbar spinal arthrodesis. J Clin Med. (2021) 10(16):3654. doi: 10.3390/jcm10163654
31. Helenius I, Remes V, Yrjönen T, Ylikoski M, Schlenzka D, Helenius M, et al. Does gender affect outcome of surgery in adolescent idiopathic scoliosis? Spine (Phila Pa 1976). (2005) 30(4):462–7. doi: 10.1097/01.brs.0000153347.11559.de
32. Hermansen A, Hedlund R, Vavruch L, Peolsson A. Positive predictive factors and subgroup analysis of clinically relevant improvement after anterior cervical decompression and fusion for cervical disc disease: a 10- to 13-year follow-up of a prospective randomized study: clinical article. J Neurosurg Spine. (2013) 19(4):403–11. doi: 10.3171/2013.7.SPINE12843
33. Heyer JH, Cao NA, Amdur RL, Rao RR. Postoperative complications following orthopedic spine surgery: is there a difference between men and women? Int J Spine Surg. (2019) 13(2):125–31. doi: 10.14444/6017
34. Jang HD, Bang C, Lee JC, Soh JW, Choi SW, Cho HK, et al. Risk factor analysis for predicting vertebral body recollapse after posterior instrumented fusion in thoracolumbar burst fracture. Spine J. (2018) 18(2):285–93. doi: 10.1016/j.spinee.2017.07.168
35. Kay HF, Chotai S, Wick JB, Stonko DP, McGirt MJ, Devin CJ. Preoperative and surgical factors associated with postoperative intensive care unit admission following operative treatment for degenerative lumbar spine disease. Eur Spine J. (2016) 25(3):843–9. doi: 10.1007/s00586-015-4175-8
36. Kaye ID, Wagner SC, Butler JS, Sebastian A, Morrissey PB, Kepler C. Risk factors for adverse cardiac events after lumbar spine fusion. Int J Spine Surg. (2018) 12(5):638–43. doi: 10.14444/5079
37. Khechen B, Haws BE, Patel DV, Cardinal KL, Guntin JA, Singh K. Does gender influence postoperative outcomes in minimally invasive transforaminal lumbar interbody fusion? Clin Spine Surg. (2019) 32(2):E107–11. doi: 10.1097/BSD.0000000000000735
38. Kim IC, Hur JW, Kwon KY, Lee JJ, Lee JW, Lee HK. The efficacy and perioperative complications associated with lumbar spinal fusion surgery, focusing on geriatric patients in the Republic of Korea. J Korean Neurosurg Soc. (2013) 54(4):323–8. doi: 10.3340/jkns.2013.54.4.323
39. Kothari P, Lee NJ, Leven DM, Lakomkin N, Shin JI, Skovrlj B, et al. Impact of gender on 30-day complications after adult spinal deformity surgery. Spine (Phila Pa 1976). (2016) 41(14):1133–8. doi: 10.1097/BRS.0000000000001499
40. Lim WSR, Liow MHL, Goh GS, Yeo W, Ling ZM, Yue WM, et al. Women do not have poorer outcomes after minimally invasive lumbar fusion surgery: a five-year follow-up study. Int J Spine Surg. (2020) 14(5):756–61. doi: 10.14444/7108
41. Mai D, Brand C, Haschtmann D, Pirvu T, Fekete TF, Mannion AF. Non-medical factors significantly influence the length of hospital stay after surgery for degenerative spine disorders. Eur Spine J. (2020) 29(2):203–12. doi: 10.1007/s00586-019-06209-5
42. Maior T, Ungureanu G, Kakucs C, Berce C, Petrushev B, Florian IS. Influence of gender on health-related quality of life and disability at 1 year after surgery for thoracolumbar burst fractures. Global Spine J. (2018) 8(3):237–43. doi: 10.1177/2192568217710854
43. Malik AT, Jain N, Yu E, Kim J, Khan SN. Is there a “sex effect” in 30-day outcomes after elective posterior lumbar fusions? World Neurosurg. (2018) 120:e428–33. doi: 10.1016/j.wneu.2018.08.097
44. Maragkos GA, Atesok K, Papavassiliou E. Prognostic factors for adjacent segment disease after L4-L5 lumbar fusion. Neurosurgery. (2020) 86(6):835–42. doi: 10.1093/neuros/nyz241
45. Marks M, Petcharaporn M, Betz RR, Clements D, Lenke L, Newton PO. Outcomes of surgical treatment in male versus female adolescent idiopathic scoliosis patients. Spine (Phila Pa 1976). (2007) 32(5):544–9. doi: 10.1097/01.brs.0000256908.51822.6e
46. Nunley PD, Cavanaugh DA, Kerr EJ 3rd, Utter PA, Campbell PG, Frank KA, et al. Heterotopic ossification after cervical total disc replacement at 7 years—prevalence, progression, clinical implications, and risk factors. Int J Spine Surg. (2018) 12(3):352–61. doi: 10.14444/5041
47. Ogihara S, Yamazaki T, Shiibashi M, Chikuda H, Maruyama T, Miyoshi K, et al. Risk factors for deep surgical site infection after posterior cervical spine surgery in adults: a multicentre observational cohort study. Sci Rep. (2021) 11(1):7519. doi: 10.1038/s41598-021-87110-4
48. Ogihara S, Yamazaki T, Shiibashi M, Chikuda H, Maruyama T, Miyoshi K, et al. Risk factors for deep surgical site infection following posterior instrumented fusion for degenerative diseases in the thoracic and/or lumbar spine: a multicenter, observational cohort study of 2913 consecutive cases. Eur Spine J. (2021) 30(6):1756–64. doi: 10.1007/s00586-020-06609-y
49. Park MS, Ju YS, Moon SH, Kim TH, Oh JK, Sung PS, et al. Reoperation rates after posterior lumbar spinal fusion surgery according to preoperative diagnoses: a national population-based cohort study. Clin Neurol Neurosurg. (2019) 184:105408. doi: 10.1016/j.clineuro.2019.105408
50. Park MS, Ju YS, Moon SH, Kim TH, Oh JK, Lim JK, et al. Repeat decompression and fusions following posterolateral fusion versus posterior/transforaminal lumbar interbody fusion for lumbar spondylosis: a national database study. Sci Rep. (2019) 9(1):4926. doi: 10.1038/s41598-019-41366-z
51. Parrish JM, Jenkins NW, Hrynewycz NM, Brundage TS, Singh K. The influence of gender on postoperative PROMIS physical function outcomes following minimally invasive transforaminal lumbar interbody fusion. J Clin Orthop Trauma. (2020) 11(5):910–5. doi: 10.1016/j.jcot.2020.04.007
52. Parrish JM, Jenkins NW, Massel DH, Rush AJ 3rd, Parrish MS, Hrynewycz NM, et al. The perioperative symptom severity of higher patient health questionnaire-9 scores between genders in single-level lumbar fusion. Int J Spine Surg. (2021) 15(1):62–73. doi: 10.14444/8007
53. Poorman GW, Moon JY, Wang C, Horn SR, Beaubrun BM, Bono OJ, et al. Rates of mortality in lumbar spine surgery and factors associated with its occurrence over a 10-year period: a study of 803,949 patients in the nationwide inpatient sample. Int J Spine Surg. (2018) 12(5):617–23. doi: 10.14444/5076
54. Salzmann SN, Miller CO, Carrino JA, Yang J, Shue J, Sama AA, et al. BMI and gender increase risk of sacral fractures after multilevel instrumented spinal fusion compared with bone mineral density and pelvic parameters. Spine J. (2019) 19(2):238–45. doi: 10.1016/j.spinee.2018.05.021
55. Samuel AM, Morse K, Lovecchio F, Maza N, Vaishnav AS, Katsuura Y, et al. Early failures after lumbar discectomy surgery: an analysis of 62 690 patients. Global Spine J. (2021) 11(7):1025–31. doi: 10.1177/2192568220935404
56. Schmitt PJ, Kelleher JP, Ailon T, Heller JE, Kasliwal MK, Shaffrey CI, et al. Long-segment fusion for adult spinal deformity correction using low-dose recombinant human bone morphogenetic protein-2: a retrospective review of fusion rates. Neurosurgery. (2016) 79(2):212–21. doi: 10.1227/NEU.0000000000001194
57. Shabat S, Folman Y, Arinzon Z, Adunsky A, Catz A, Gepstein R. Gender differences as an influence on patients’ satisfaction rates in spinal surgery of elderly patients. Eur Spine J. (2005) 14(10):1027–32. doi: 10.1007/s00586-004-0808-z
58. Sharma A, Tanenbaum JE, Hogue O, Mehdi S, Vallabh S, Hu E, et al. Predicting clinical outcomes following surgical correction of adult spinal deformity. Neurosurgery. (2019) 84(3):733–40. doi: 10.1093/neuros/nyy190
59. Smorgick Y, Nassar M, Tamir E, Tal S, Mirovsky Y, Anekstein Y. Clinical and radiographical characteristics in male and female adolescent idiopathic scoliosis surgical candidates. Isr Med Assoc J. (2019) 21(3):213–6.
60. Ungureanu G, Chitu A, Iancu I, Kakucs C, Maior T, Florian IS. Gender differences in the self-assessment of quality of life and disability after spinal fusion for chronic low back pain at a neurosurgical center in Eastern Europe. Neurospine. (2018) 15(3):261–8. doi: 10.14245/ns.1836076.038
61. Wang F, Hou HT, Wang P, Zhang JT, Shen Y. Symptomatic adjacent segment disease after single-lever anterior cervical discectomy and fusion: incidence and risk factors. Medicine (Baltimore). (2017) 96(47):e8663. doi: 10.1097/MD.0000000000008663
62. Wang H, Meng Y, Liu H, Wang X, Hong Y. The impact of smoking on outcomes following anterior cervical fusion-nonfusion hybrid surgery: a retrospective single-center cohort study. BMC Musculoskelet Disord. (2021) 22(1):612. doi: 10.1186/s12891-021-04501-4
63. Xu X, Wang F, Zhou X, Cheng Y, Wei X, Bai Y, et al. Comparison of radiographic postoperative outcomes between males and females with AIS. Medicine (Baltimore). (2015) 94(41):e1616. doi: 10.1097/MD.0000000000001616
64. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. (2013) 111(1):52–8. doi: 10.1093/bja/aet127
65. Riley JL 3rd, Robinson ME, Wise EA, Myers CD, Fillingim RB. Sex differences in the perception of noxious experimental stimuli: a meta-analysis. Pain. (1998) 74(2–3):181–7. doi: 10.1016/s0304-3959(97)00199-1
Keywords: spinal fusion surgery, clinical data, systematic review, sex, gender differences
Citation: Salamanna F, Contartese D, Tschon M, Borsari V, Griffoni C, Gasbarrini A and Fini M (2022) Sex and gender determinants following spinal fusion surgery: A systematic review of clinical data. Front. Surg. 9:983931. doi: 10.3389/fsurg.2022.983931
Received: 1 July 2022; Accepted: 16 September 2022;
Published: 17 October 2022.
Edited by:
Ziya Levent Gokaslan, Brown University, United StatesReviewed by:
Luca Ambrosio, Campus Bio-Medico University, ItalyJohn Charles Rotondo, University of Ferrara, Italy
© 2022 Salamanna, Contartese, Tschon, Borsari, Griffoni, Gasbarrini and Fini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Deyanira Contartese ZGV5YW5pcmEuY29udGFydGVzZUBpb3IuaXQ=
Specialty Section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery