
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 24 August 2022
Sec. Obstetrics and Gynecological Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.976497
 Eva K. Egger1*
Eva K. Egger1* Freya Merker1
Freya Merker1 Damian J. Ralser1Milka Marinova2Tim O. Vilz3
Damian J. Ralser1Milka Marinova2Tim O. Vilz3 Hanno Matthaei3Tobias Hilbert4Alexander Mustea1
Hanno Matthaei3Tobias Hilbert4Alexander Mustea1
Aim: This study aims to evaluate the incidence of postoperative ileus (POI) following cytoreductive surgery in epithelial ovarian cancer (EOC) patients and its impact on anastomotic leakage occurrence and postoperative complications.
Methods: A total of 357 surgeries were performed on 346 ovarian cancer patients between 1/2010 and 12/2020 at our institution. The postoperative course regarding paralytic ileus, anastomotic leakage, and postoperative complications was analyzed by Fisher's exact test and through ordinal logistic regression.
Results: A total of 233 patients (65.3%) returned to normal gastrointestinal functions within 3 days after surgery. A total of 123 patients (34.5%) developed POI. There were 199 anastomoses in 165 patients and 24 leakages (12.1%). Postoperative antibiotics (p 0.001), stoma creation (p 0.0001), and early start of laxatives (p 0.0048) significantly decreased POI, while anastomoses in general (p 0.0465) and especially low anastomoses (p 0.0143) showed increased POI rates. Intraoperative positive fluid excess >5,000 cc was associated with a higher risk for POI (p 0.0063), anastomotic leakage (p 0.0254), and severe complications (p 0.0012).
Conclusion: Postoperative antibiotics, an early start with laxatives, and stoma creation were associated with reduced POI rates. Patients with anastomoses showed an increased risk for POI. Severe complications, anastomotic leakages, and POI were more common in the case of intraoperative fluid balance exceeding 5,000 cc.
Among gynecologic malignancies, epithelial ovarian cancer (EOC) is the most frequent cause of death in women (1). The most powerful therapeutic tool is optimal cytoreduction to no residual disease, usually requiring high surgical complexity and harboring the risk of increased morbidity (2–6). While enhanced recovery after surgery (ERAS) programs in colorectal and ovarian cancer surgery showed lower morbidity and mortality, no effect was seen on the frequency of postoperative paralytic ileus (POI) (7–10).
The POI relates to severe patient discomfort, including a lack of flatus, abdominal distension, nausea and vomiting, absence of normal bowel sounds, and a delay in the passage of stool, causing prolonged hospital stays, readmissions, reoperations, and possibly anastomotic leakages (11–13). POI represents the most frequent complication following gastrointestinal surgery affecting one out of eight patients (14). Its effect on the quality of life lasts even 3 and 6 months after surgery (15). Due to the lack of a standard POI definition, the I-FEED scoring system was developed by the American society for enhanced recovery after surgery. Here, the general postoperative ileus is split into three groups depending on the severity (measured by 0–2 points) of five different symptoms (oral intake, nauseated feeling, emesis, distension in examination, and duration of symptoms). Each symptom is attributed by 0–2 points according to the severity. A total score of 0–2 points is considered a normal postoperative state. In the case of 3 points or more, a patient is considered to experience POI. In the case of 3–5 points, the POI is milder and defined as gastrointestinal intolerance, and in the case of 6 points, the patients experience a severe form of POI considered as a gastrointestinal dysfunction (16, 17). The relevance of POI regarding the most feared complications as pancreatic fistulas and anastomotic leakages in ovarian cancer patients is unknown (18). Here, we aimed to evaluate the frequency of the postoperative paralytic ileus after cytoreduction in patients with epithelial ovarian cancer and its impact on anastomotic leakage and postoperative morbidity.
This study was conducted in accordance with the standards of the ethics committee of the Faculty of Medicine at the University of Bonn, Germany (No.: 14/22). The institutional record database was screened for ovarian cancer patients with cytoreductive surgery between January 2010 and December 2020. Pre-, intra-, and postoperative patient information was recorded from patient's charts, surgery reports, and pathologic findings. All data were evaluated regarding the following postoperative outcomes: postoperative paralytic ileus, anastomotic leakage, and general postoperative complications. In consideration of the I-FEED scoring system, POI was considered in case of an I-FEED score of equal or more than 3 points (17). The peritoneal carcinomatosis index (PCI) as the sum of carcinosis, quantified by size in 13 regions of the abdomen, was retrospectively calculated on the basis of surgery and pathology reports for the evaluation of the tumor load. Depending on the size of the largest tumor nodule in each region, patients received 0 points for no tumor, 1 point for nodules up to 5 mm, 2 points for tumor nodules up to 5 cm, and 3 points for nodules larger than 5 cm. All points were added up to the PCI score in the end (19). The age-adjusted comorbidity index was calculated based on patient's comorbidities that have been weighted analogously to the Charlson comorbidity index generated from patient's charts. Furthermore, one point was added for each decade above 40 years, as age has been identified as a comorbid factor as well (20). The surgical complexity score was evaluated for each patient according to the surgical report. All surgical procedures are attributed by 1–3 points depending on the complexity of the procedure, and the final sum is grouped into low surgical complexity (0–3 points), medium surgical complexity (3–7 points), and high surgical complexity (8–18 points) (21). Using the Memorial Sloan Kettering Cancer Center secondary surgical event score, we classified all postoperative complications from grades 1 to 5 (G1–G5). This score was created for the evaluation of complications within the first 30 days after surgery in cancer patients only. So far, more than 220 different secondary surgical events are included in this score. G1 and G2 complications are minor and treated by bedside care or oral medication and by intravenous medications or transfusions, respectively. G3 complications include anastomotic leakage and are treated by intervention, either radiologic, endoscopic, or operative. G4 complications lead to chronic disability or further organ resection, and G5 complications result in the death of the patient (22). The following aspects of enhanced recovery after surgery are standard of care in all our patients: Placement of a peridural catheter whenever possible, early mobilization on the first day after surgery, and guided mobilization by the nursing staff beginning on the first postoperative day. After mobilization, the urine catheter is removed. Early feeding and drinking should start after 6 h in the case of no anastomosis on the day of surgery, and in the case of an anastomosis, early drinking should start after 6 h on the day of surgery and fluid feeding on the first day after surgery in the morning. There should be immediate removal of the nasogastric tube at the end of surgery. The central venous catheter should be removed latest by the third postoperative day (16, 17).
All variables were analyzed by Fisher's exact test to identify significant correlations of pre-, intra-, and postoperative findings regarding the outcomes of POI, general morbidity, and anastomotic leakage. Differences were considered to be significant at a threshold of ≤0.05. Ordinal logistic regression was used to analyze morbidity in the context of comorbidity and surgical complexity. The test of all slopes equal to zero indicated that complications had a significant association with comorbidity and surgical complexity. The goodness of fit was tested by Pearson’s test and deviance test to verify that the model using link function logit was appropriate. All statistical analyses were performed using Minitab, version 18 (Minitab LLC., State College, PA, USA).
There were 357 surgeries in a total of 346 patients. Eleven patients received their primary surgery in our department, came back for recurrency, and received surgery again in our department. Fifteen patients received HIPEC (hyperthermic intraperitoneal chemotherapy) at the end of surgery. The median age was 61 years (range: 16–86 years). The physical status classification by the American Society of Anaesthesiologists (ASA) showed 1 ASA-4 patient and 104 ASA-3 patients. The rest of the patients scored ASA-1 and -2. The median PCI was 8 (range: 1–30). The median duration of surgery was 357 min (range: 24–695 min). The median amount of intraoperative kristalloid infusion was 7,500 ml (1,000 ml–21,500 ml). The median positive fluid excess was 6,580 ml (range: 0–19,100 ml). The median number of erythrocyte concentrates was 2 (range: 0–30). The median number of fresh frozen plasma was 0 (range: 0–19). The median highest intraoperative noradrenalin dosing during surgery was 5 µg/ml (range: 0–80 µg/ml). The median number of days in the intensive care unit was 1 day (range: 0–50 days). The median duration of postoperative ventilation was 4 h (range: 0–567 h). The median surgical complexity score was 6 (range: 0–15). Further general patient characteristics are presented in Table 1.
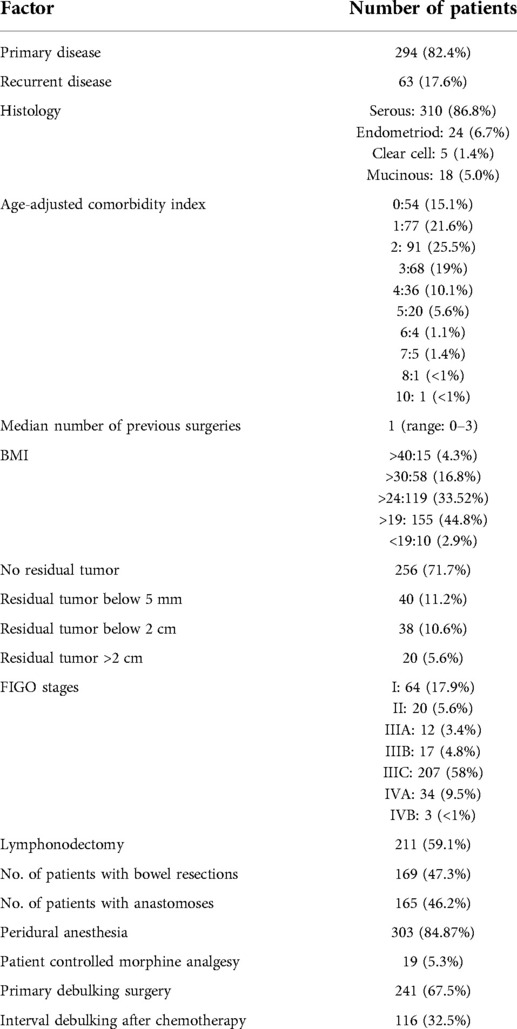
Table 1. General patients’ characteristics.
Table 2 presents all 199 anastomoses performed in 165 patients in detail. A total of 130 patients received one anastomosis, 32 patients had two anastomoses, and 3 patients had three anastomoses. A total of 175 involved the large colon and 24 involved only the small bowel. There were 24 leakages (12.06%). Table 2 presents the details.
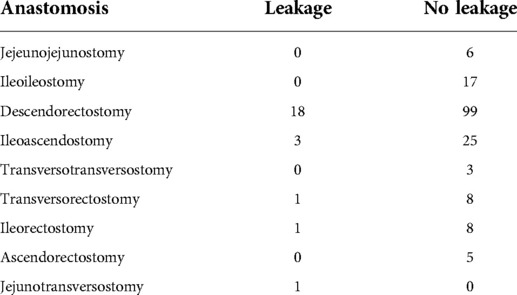
Table 2. 199 Anastomoses.
Of all patients, 233 (65.3%) returned to normal gastrointestinal functions within 3 days after surgery. A total of 123 patients (34.5%) were considered as experiencing POI due to a lack of flatus and defecation, nausea, and abdominal distension at least. Fifteen patients needed the placement of a nasogatric tube due to irresistible vomiting. Table 3 presents the day of first defecation after surgery in detail. Table 4 presents the factors associated with a decreased rate of POI and the factors associated with an increased rate of POI.
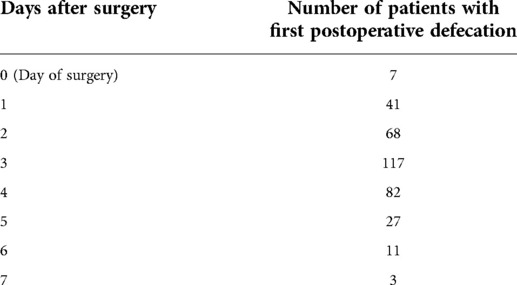
Table 3. First defecation after surgery.
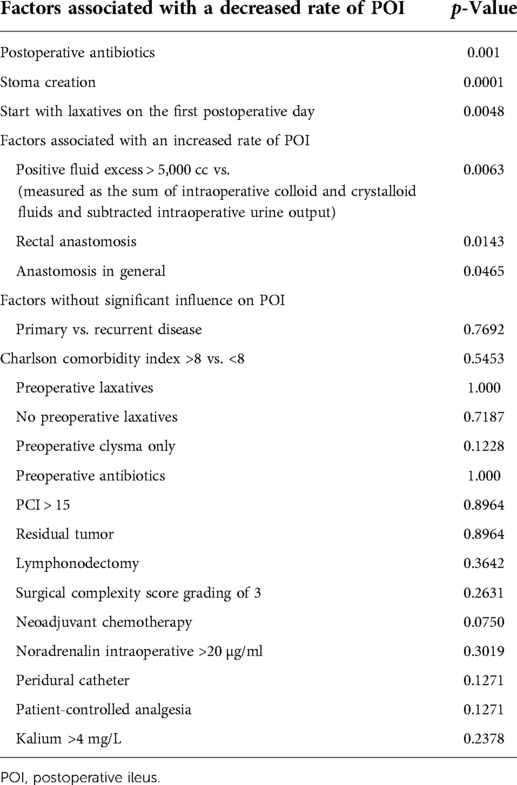
Table 4. Factors with increased and decreased POI rates.
There was no significant correlation between morbidity in general (G0 vs. G1–G5) and POI (p-value: 0.1634) and between severe postoperative morbidity (G4–G5) and POI (p-value: 0.4679). The comorbidity index did not correlate with increasing severe postoperative morbidity (G4–G5; p-value: 0.1680). A significant increase in severe postoperative morbidity was seen in the case of increasing surgical complexity (p-value: 0.0282).
A positive fluid excess of more than 5,000 ml showed a significant increase in severe complications (G3–G5) (p-value: 0.0012), anastomotic leakage (p-value: 0.0254), and POI (p-value: 0.0063). A significant prolongation of the hospital stay was seen in the case of anastomotic leckage (p-value: 0.000), severe postoperative complications (G3–G5) (p-value: 0.000), and anastomosis in general (p-value: 0.000) but not in the case of a prolonged POI only (>5 days without flatus/defecation, abdominal distension ± vomiting), as seen in Table 5.
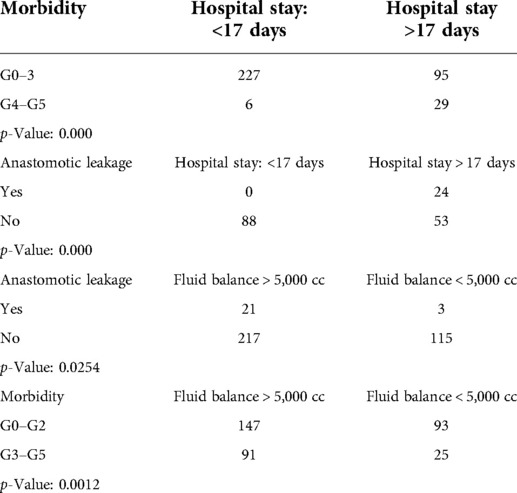
Table 5. Postoperative morbidity, hospital stay, fluid balance, and anastomotic leakage.
Considering surgical complexity, complications, and comorbidity index only, ordinal logistic regression showed significantly more severe postoperative complications (G4–G5) as comorbidity and surgical complexity increased (p-value: 0.037). The test of all slopes equal to zero indicated that severe complications had a significant association with comorbidity and surgical complexity. The goodness of fit was tested by Pearson’s test with a p-value of 0.249 and deviance test with a p-value of 0.243, indicating that the model using link function logit is appropriate. Odds ratios are seen in Table 6.
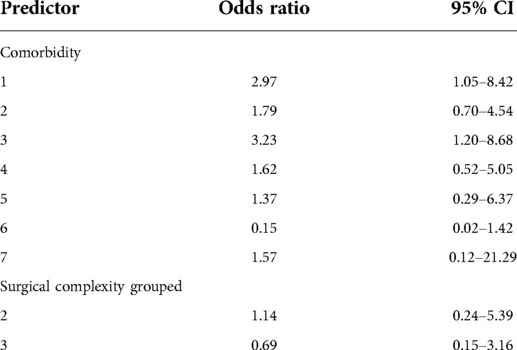
Table 6. Logistic regression table.
Anastomoses in general and especially low rectal anastomoses led to a significant increase in POI. No correlation was found between POI and anastomotic leakage or POI and small vs. large bowel anastomoses or POI in the case of anastomoses and increasing surgical complexity without stoma creation, as seen in Table 7.
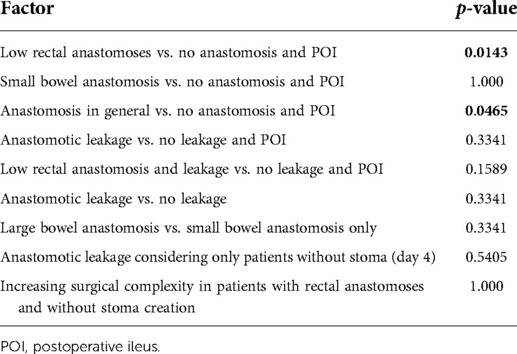
Table 7. POI and anastomoses.
There is a broad consensus that intestinal manipulation leads to intestinal inflammation causing impaired gastrointestinal motility (12, 23, 24). Advances in laparoscopic techniques have significantly reduced the immunological response and POI due to less tissue trauma and less stimulation of the bowel, vessels, and nervous system (25, 26). As ovarian cancer surgery remains an open surgical procedure, we could not show an association between POI and increasing surgical complexity. Like others, we saw increasing morbidity as surgical complexity increased (20). This matches well with data from colonic cancer, showing that the open approach in right-sided colonic resections only increased surgical complexity and significantly increased POI compared to the laparoscopic approach in colonic cancer (25, 26). In colorectal surgery, POI is considered a promoter of postoperative complications (15). In our cohort, we did not observe any association between POI and postoperative complications. Consistent with the recent literature in ovarian cancer surgery, a significant increase in severe complications apart from POI was found with increasing surgical complexity (21). While comorbidity only had no influence on POI or complication rate, the combination of increasing comorbidity and increasing surgical complexity showed a significant increase in severe postoperative complications.
Although there is strong evidence for the use of preoperative antibiotics in colorectal surgery to prevent POI, surgical site infections, and anastomotic leckage, there is little evidence for the same outcomes for the use of postoperative i.v. antibiotics (27, 28). Postoperative antibiotic use for 3–5 days resulted in a significant increase in the proportion of patients with defecation within the first 3 days in our cohort. Furthermore, we saw a significant decrease in POI in the case of laxative use starting on the first postoperative day. Here, metoclopramide and bisacodyl were used as a standard in our clinic for the first 3 days. Nevertheless, there is only weak evidence for using laxatives in colorectal surgery to prevent POI (29). Caffeine intake and coffee as a beverage, on the other hand, have shown promising results regarding prevention of POI and safety after colorectal surgery (30–32).
Fluid overload in colorectal surgery has been identified as a promoter of POI and increased complications such as anastomotic leakage. Especially crystalloid fluids are suspected of producing splanchnic edema and thus escalating abdominal pressure, which in turn reduces mesenteric blood flow and contributes to tissue hypoxemia and impaired anastomotic healing (33–36). Fluid management in ovarian cancer patients is often challenging due to intraoperative fluid shifts from the endovascular space to the intra-abdominal and interstitial space in part due to an increased expression of vascular leakage genes; this leads to increasing amounts of crystalloid infusion intraoperatively and slower bowel function recovery (37, 38). In our cohort, we saw a significant increase in POI, anastomotic leakage, and severe complications at a fluid excess of 5,000 cc and more. Compared to colorectal surgery, less data are available for ovarian cancer surgery regarding limited fluid administration, but it seems safe and decreases the time of gastrointestinal impairment and hospital stay (36). While postoperative ileus is not only a matter of gastrointestinal resections, we identified anastomoses, especially low anastomoses, which are the most common anastomoses in the case of ovarian cancer, as a significant additional risk factor for POI (39).
Diverting ileostomies may reduce the clinical severity of anastomotic leakage, but no reduction of leakages is seen in the case of rectal cancer, remaining a controversial topic (40). Especially high output diverting ileostomies are suspected to be at risk for POI, readmission, and subsequent ileus (40). In ovarian cancer, anastomoses are generally 3 cm–5 cm higher than in rectal cancer. Here, a preventive effect of diverting ileostomies on anastomotic leakage was seen (41). A recent study found more anastomotic leakage in the case of medium-low colorectal anastomosis <10 cm from the anal verge (42). Furthermore, in our actual study, we found a significant preventive effect for POI. Nevertheless, this may not be turned into a recommendation for stoma creation in the case of colorectal anastomoses as anastomotic leakage rates are generally low and POI will be overcome without stoma creation (43). Further improvements in surgical techniques such as total mesorectal resections with preservation of the superior rectal artery and improvements in the presurgical nutritional status may even lower the rate of colorectal anastomotic leakage (44, 45).
Most likely due to a different policy between the USA and Germany regarding the duration of in-hospital length of stay after major abdominal surgeries, we saw no significant association between POI and prolonged in-hospital length of stay (13).
Our study has some limitations. Due to the retrospective evaluation of POI, a clear distinction between gastrointestinal intolerance and gastrointestinal dysfunction was not possible, although it may be important, especially with regard to POI-associated morbidity. Therefore, over- and underestimation of the true postoperative gastrointestinal impairment may be possible.
Additionally, the fluid status depends on a number of factors such as the preoperative fluid status, preoperative bowel preparation, duration of surgery, blood loss, and patient fluid output by urine and intra-abdominally with respect to the amount of resected tumor. Therefore, more accurate measurements are needed in further studies to further define fluid overload in ovarian cancer patients.
The strength of our study is the homogenous patient population, of only patients undergoing cytoreduction for epithelial ovarian cancer. Furthermore, we are the first to show that increasing surgical complexity does relate to increased morbidity but does not affect POI.
The postoperative paralytic ileus may be reduced in the case of postoperative antibiotic use, early initiation of laxatives, and stoma creation. While antibiotics and laxatives are easy to implement, no recommendation for stoma creation can be drawn from our data due to the negative side effects of a stoma and POI will be overcome without a stoma. Optimal fluid management in ovarian cancer patients continues to be challenging as postoperative complications, postoperative paralytic ileus, and anastomotic leakage increase considerably with an increase in fluid excess. Duration of hospitalization is prolonged in the case of anastomotic leakage and severe morbidity but not in the case of a postoperative ileus.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of the Faculty of Medicine at the University of Bonn, Germany. The patients/participants provided their written informed consent to participate in this study.
EKE: conceived and designed the analysis; FM, MM, and HM: collected the data; TV and DJR: contributed data or analysis tools; EKE: performed the analysis; EKE: wrote the paper; AM, TH, and HM: edited the paper. All authors contributed to the article and approved the submitted version.
There was no funding for the above-mentioned study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. DuBois A, Reuss A, Pujade-Lauraine E, Harter P, Ray-Coquard I, Pfisterer J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: a combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: by the arbeitsgemeinschaft gynaekologische onkologie studiengruppe ovarialkarzinom (AGO-OVAR) and the groupe d’Investigateurs nationaux pour les etudes des cancers de l’Ovaire (GINECO). Cancer. (2009) 115:1234–44. doi: 10.1002/cncr.24149
3. Bristow RE, Tomacruz RS, Armstrong DK, Trimble EL, Montz FJ. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: a meta-analysis. J Clin Oncol. (2002) 20:1248–59. doi: 10.1200/JCO.20.5.1248
4. Chang SJ, Hodeib M, Chang J, Bristow RE. Survival impact of complete cytoreduction to no gross residual disease for advanced-stage ovarian cancer: a meta-analysis. Gynecol Oncol. (2013) 130:493–8. doi: 10.1016/j.ygyno.2013.05.040
5. Eisenhauer EL, Abu-Rustum NR, Sonoda Y, Aghajanian C, Barakat RR, Chi DS. The effect of maximal surgical cytoreduction on sensitivity to platinum-taxane chemotherapy and subsequent survival in patients with advanced ovarian cancer. Gynecol Oncol. (2008) 108:276–81. doi: 10.1016/j.ygyno.2007.10.022
6. Egger EK, Kohls N, Stope MB, Condic M, Keyver-Paik MD, Könsgen D, et al. Risk factors for severe complications in ovarian cancer surgery. In Vivo. (2020) 34:3361–5. doi: 10.21873/INVIVO.12174
7. Reuter S, Woelber L, Trepte CC, Daniel P, Zapf A, Cevirme S, et al. The impact of enhanced recovery after surgery (ERAS) pathways with regard to perioperative outcome in patients with ovarian cancer. Arch Gynecol Obstet. (2021) 306(1):199–207. doi: 10.1007/s00404-021-06339-6
8. Pędziwiatr M, Mavrikis J, Witowski J, Adamos A, Major P, Nowakowski M, et al. Current status of enhanced recovery after surgery (ERAS) protocol in gastrointestinal surgery. Med Oncol. (2018) 35:95. doi: 10.1007/s12032-018-1153-0
9. Gustafsson UO, Scott MJ, Hubner M, Nygren J, Demartines N, Francis N, et al. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS Ò) society recommendations: 2018. World J Surg. (2019) 43:659–95. doi: 10.1007/s00268-018-4844-y
10. Nazzani S, Bandini M, Preisser F, Mazzone E, Marchioni M, Tian Z, et al. Postoperative paralytic ileus after major oncological procedures in the enhanced recovery after surgery era: a population based analysis. Surg Oncol. (2019) 28:201–207S. doi: 10.1016/j.suronc.2019.01.011
11. Mazzotta E, Villalobos-Hernandez EC, Fiorda-Diaz J, Harzman A, Christofi FL. Postoperative ileus and postoperative gastrointestinal tract dysfunction: pathogenic mechanisms and novel treatment strategies beyond colorectal enhanced recovery after surgery protocols. Front Pharmacol. (2020) 11:1695. doi: 10.3389/FPHAR.2020.583422/BIBTEX.
12. Peters EG, Dekkers M, Van Leeuwen-Hilbers FW, Daams F, Hulsew KWE, De Jonge WJ. Relation between postoperative ileus and anastomotic leakage after colorectal resection: a post hoc analysis of a prospective randomized controlled trial. Colorectal Dis. (2017) 19:667–77. doi: 10.1111/codi.13582
13. Tevis SE, Carchman EH, Foley EF, Harms BA, Heise CP, Kennedy GD. Postoperative ileus-more than just prolonged length of stay? J Gastrointest Surg. (2015) 19:1684–90. doi: 10.1007/s11605-015-2877-1
14. Wolthuis AM, Bislenghi G, Fieuws S, de Buck van Overstraeten A, Boeckxstaens G, D’Hoore A. Incidence of prolonged postoperative ileus after colorectal surgery: a systematic review and meta-analysis. Colorectal Dis. (2016) 18:O1–9. doi: 10.1111/CODI.13210
15. Peters EG, Pattamatta M, Smeets BJ, Brinkman DJ, Evers AA, de Jonge SM, et al. The clinical and economical impact of postoperative ileus in patients undergoing colorectal surgery. Neurogastroenterol Motil. (2020) 32:13862. doi: 10.1111/nmo.13862
16. Lee MJ, Vaughan-Shaw P, Vimalachandran D. A systematic review and meta-analysis of baseline risk factors for the development of postoperative ileus in patients undergoing gastrointestinal surgery. Coll Surg Engl. (2020) 102:194–203. doi: 10.1308/rcsann.2019.0158
17. Hedrick TL, McEvoy MD, Mythen MG, Bergamaschi R, Gupta R, Holubar SD, et al. American society for enhanced recovery and perioperative quality initiative joint consensus statement on postoperative gastrointestinal dysfunction within an enhanced recovery pathway for elective colorectal surgery. Anesth Analg. (2018) 126:1896–907. doi: 10.1213/ANE.0000000000002742
18. Sozzi G, Petrillo M, Berretta R, Capozzi VA, Paci G, Musicò G, et al. Incidence, predictors and clinical outcome of pancreatic fistula in patients receiving splenectomy for advanced or recurrent ovarian cancer: a large multicentric experience. Arch Gynecol Obstet. (2020) 302:707–14. doi: 10.1007/s00404-020-05684-2
19. Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat Res. (1996) 82:359–74. doi: 10.1007/978-1-4613-1247-5_23
20. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. (1994) 47:1245–5147. doi: 10.1016/0895-4356(94)90129-5
21. Aletti GD, Santillan A, Eisenhauer EL, Hu J, Aletti G, Podratz KC, et al. A new frontier for quality of care in gynecologic oncology surgery: multi-institutional assessment of short-term outcomes for ovarian cancer using a risk-adjusted model. Gynecol Oncol. (2007) 107:99–106. doi: 10.1016/J.YGYNO.2007.05.032
22. Strong VE, Selby LV, Sovel M, Disa JJ, Hoskins W, Dematteo R, et al. Development and assessment of Memorial Sloan Kettering Cancer Center's Surgical secondary events grading system. Ann Surg Oncol. (2015) 22:1061–7. doi: 10.1245/s10434-014-4141-4
23. van Bree SHW, Cailotto C, Di Giovangiulio M, Jansen E, van der Vliet J, Costes L, et al. Systemic inflammation with enhanced brain activation contributes to more severe delay in postoperative ileus. Neurogastroenterol Motil. (2013) 25:540–925. doi: 10.1111/NMO.12157
24. The FO, Bennink RJ, Ankum WM, Buist MR, Busch ORC, Gouma DJ, et al. Intestinal handling-induced mast cell activation and inflammation in human postoperative ileus. Gut. (2008) 57:33–40. doi: 10.1136/gut.2007.120238
25. Wang H, Wang Y, Xing H, Zhou YA, Zhao JA, Jiang ADG, et al. Laparoscopic surgery within an enhanced recovery after surgery (ERAS) protocol reduced postoperative ileus by increasing postoperative treg levels in patients with right-Side colon carcinoma. Med Sci Monit. (2018) 24:7231–723. doi: 10.12659/MSM.910817
26. Wang G, Jiang Z, Zhao K, Li G, Liu F, Pan H, et al. Immunologic response after laparoscopic colon cancer operation within an enhanced recovery program. J Gastrointest Surg. (2012) 16:1379–88. doi: 10.1007/s11605-012-1880-z
27. Suzuki T, Sadahiro S, Tanaka A, Okada K, Saito G, Miyakita H, et al. Usefulness of preoperative mechanical bowel preparation in patients with colon cancer who undergo elective surgery: a prospective randomized trial using oral antibiotics. Dig Surg. (2020) 37(3):192–8. doi: 10.1159/000500020.31055568
28. Basany E, Solís-Peña E, Pellino A, Kreisler G, Fraccalvieri E, Muinelo-Lorenzo D, et al. Preoperative oral antibiotics and surgical-site infections in colon surgery (ORALEV): a multicentre, single-blind, pragmatic, randomised controlled trial. Lancet Gastroenterol Hepatol. (2020) 5:729–38. doi: 10.1016/S2468-1253(20)30075-3
29. Dudi-Venkata NN, Kroon HM, Bedrikovetski S, Moore JW, Sammour T. Systematic scoping review of enhanced recovery protocol recommendations targeting return of gastrointestinal function after colorectal surgery. ANZ J Surg. (2020) 90:41–7. doi: 10.1111/ANS.15319
30. Yang TW, Wang CC, Sung WW, Ting WC, Lin CC, Tsai MC. The effect of coffee/caffeine on postoperative ileus following elective colorectal surgery: a meta-analysis of randomized controlled trials. Int J Colorectal Dis. (2022) 37(3):623–30. doi: 10.1007/S00384-021-04086-3
31. Gkegkes ID, Minis EE, Iavazzo C. Effect of caffeine intake on postoperative ileus: a systematic review and meta-analysis. Dig Surg. (2020) 37:22–31. doi: 10.1159/000496431
32. Hasler-Gehrer S, Linecker M, Keerl A, Slieker J, Descloux A, Rosenberg R, et al. Does coffee intake reduce postoperative ileus after laparoscopic elective colorectal surgery? A prospective, randomized controlled study: the coffee study. Dis Colon Rectum. (2019) 62:997–1004. doi: 10.1097/DCR.0000000000001405
33. Namba Y, Hirata Y, Mukai S, Okimoto S, Fujisaki S, Takahashi M, et al. Clinical indicators for the incidence of postoperative ileus after elective surgery for colorectal cancer. BMC Surg. (2021) 21:1–6. doi: 10.1186/S12893-021-01093-7/FIGURES/2
34. VandeHei MS, Papageorge CM, Murphy MM, Kennedy GD. The effect of perioperative fluid management on postoperative ileus in rectal cancer patients. Surgery. (2017) 161:1628–32. doi: 10.1016/J.SURG.2016.11.015
35. Grass F, Lovely JK, Crippa J, Hübner M, Mathis KL, Larson DW. Potential association between perioperative fluid management and occurrence of postoperative ileus. Dis Colon Rectum. (2020) 63:68–74. doi: 10.1097/DCR.0000000000001522
36. Grass F, Pache B, Butti F, Solà J, Hahnloser D, Demartines N. Stringent fluid management might help to prevent postoperative ileus after loop ileostomy closure. Langenbecks Arch Surg. (2019) 404:39–43. doi: 10.1007/s00423-018-1744-4
37. Russo A, Aceto P, Grieco DL, Anzellotti GM, Perilli V, Costantini B, et al. Goal-directed hemodynamic management in patients undergoing primary debulking gynaecological surgery: a matched-controlled precision medicine study. Gynecol Oncol. (2018) 151:299–305. doi: 10.1016/J.YGYNO.2018.08.034
38. Kinnen A, Klaschik S, Neumann C, Egger EK, Mustea A, Soehle M, et al. Gene expression in the angiopoietin/TIE axis is altered in peripheral tissue of ovarian cancer patients: a prospective observational study. Life Sci. (2021) 1(274):119345. doi: 10.1016/J.LFS.2021.119345
39. Ahmed MR, Sayed Ahmed WA, Khamess RE, Youwakim MS, El-Nahas KM. Efficacy of three different regimens in recovery of bowel function following elective cesarean section: a randomized trial. J Perinat Med. (2018) 46:786–90. doi: 10.1515/jpm-2017-0389
40. Lee N, Young Lee S, Hyun Kim C, Deok Kwak H, Kyun Ju J, Rok Kim H. The relationship between high-output stomas, postoperative ileus, and readmission after rectal cancer surgery with diverting ileostomy. Ann Coloproctol. (2021) 37:44–50. doi: 10.3393/ac.2020.08.03
41. Koscielny A, Ko A, Egger EK, Kuhn W, Kalff JC, Keyver-Paik MD. Prevention of anastomotic leakage in ovarian cancer debulking surgery and its impact on overall survival. Anticancer Res. (2019) 39:5209–18. doi: 10.21873/ANTICANRES.13718
42. Costantini B, Vargiu V, Santullo F, Rosati A, Bruno M, Gallotta V, et al. Risk factors for anastomotic leakage in advanced ovarian cancer surgery: a large single-center experience. Ann Surg Oncol. (2022) 29:4791–802. doi: 10.1245/s10434-022-11686-y
43. Lago V, Fotopoulou C, Chiantera V, Minig L, Gil-Moreno A, Cascales-Campos PA, et al. Indications and practice of diverting ileostomy after colorectal resection and anastomosis in ovarian cancer cytoreduction. Gynecol Oncol. (2020) 158(3):603–7. doi: 10.1016/j.ygyno.2020.05.047
44. Rosati A, Vargiu V, Santullo F, Lodoli C, Attalla El Halabieh M, Scambia G, et al. Rectosigmoid mesorectal-sparing resection in advanced ovarian cancer surgery. Ann Surg Oncol. (2021) 28(11):6721–2. doi: 10.1245/s10434-021-09651-2
Keywords: paralytic ileus, ovarian cancer, surgical complexity, complications, anastomotic leakage
Citation: Egger EK, Merker F, Ralser DJ, Marinova M, Vilz TO, Matthaei H, Hilbert T and Mustea A (2022) Postoperative paralytic ileus following debulking surgery in ovarian cancer patients. Front. Surg. 9:976497. doi: 10.3389/fsurg.2022.976497
Received: 23 June 2022; Accepted: 8 August 2022;
Published: 24 August 2022.
Edited by:
Carlo Ronsini, Università degli Studi della Campania "Luigi Vanvitelli," ItalyReviewed by:
Stefano Restaino, Ospedale Santa Maria della Misericordia di Udine, Italy© 2022 Egger, Merker, Ralser, Marinova, Vilz, Matthaei, Hilbert and Mustea. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eva K. EggerZXZhLWthdGhhcmluYS5lZ2dlckB1a2Jvbm4uZGU=
Specialty Section: This article was submitted to Obstetrics and Gynecological Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.