
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg. , 23 August 2022
Sec. Obstetrics and Gynecological Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.973034
This article is part of the Research Topic Management of Borderline Ovarian Tumor: The best treatment is a real challenge in the era of precision medicine View all 6 articles
 Luigi Della Corte1
Luigi Della Corte1 Antonio Mercorio1*
Antonio Mercorio1* Paolo Serafino1Francesco Viciglione1Mario Palumbo1Maria Chiara De Angelis2
Paolo Serafino1Francesco Viciglione1Mario Palumbo1Maria Chiara De Angelis2 Maria Borgo2Cira Buonfantino2Marina Tesorone3Giuseppe Bifulco1
Maria Borgo2Cira Buonfantino2Marina Tesorone3Giuseppe Bifulco1 Pierluigi Giampaolino2
Pierluigi Giampaolino2
Borderline ovarian tumors (BOTs) account for approximately 15% of all epithelial ovarian cancers. In 80% of cases the diagnosis of BOTs is done at stage I and more than a third of BOTs occurs in women younger than 40 years of age wishing to preserve their childbearing potential; the issue of conservative surgical management (fertility-sparing treatment) is thus becoming of paramount importance. At early stages, the modalities of conservative treatment could range from mono-lateral cystectomy to bilateral salpingo-oophorectomy. Although cystectomy is the preferred method to promote fertility it can lead to an elevated risk of recurrence; therefore, an appropriate counseling about the risk of relapse is mandatory before opting for this treatment. Nevertheless, relapses are often benign and can be treated by repeated conservative surgery. Besides the stage of the disease, histological subtype is another essential factor when considering the proper procedure: as most mucinous BOTs (mBOTs) are more commonly unilateral, the risk of an invasive recurrence seems to be higher, compared to serous histotype, therefore unilateral salpingo-oophorectomy is recommended. In the appraisal of current literature, this review aims to gain better insight on the current recommendations to identify the right balance between an accurate staging and an optimal fertility outcome.
Borderline ovarian tumors (BOTs) are a heterogeneous group of neoplasms with recognized potential malignancy, histologically defined by epithelial proliferation and nuclear atypia without recognizable destructive stromal invasion. Similar to carcinoma they can spread to the peritoneum and eventually to lymph nodes and in some patients can recur (1).
Peritoneal spread is present in 10% of BOTs and is divided into non-invasive (nearly 85% of implants) or invasive (2); the mortality rate for patients with non-invasive and invasive implants is 4.7% and 34% respectively (3).
BOTs are staged according to the FIGO staging system used for ovarian carcinoma (4). Most of the BOTs have a low potential for malignancy and are confined to the ovaries at presentation: unlike ovarian carcinoma in nearly 80% of cases the diagnosis is done at stage I with <1% of women diagnosed at stage IV (5).
Borderline ovarian tumors survival is 95% at 5 years, 90% at 10 years for women with FIGO stage I-III and nearly 77% at stage IV (6).
The vast majority of BOTs have serous or mucinous histotypes; about two-thirds are serous BOT (Table 1). Other rare types (<5%) are clear cell, endometrioid and Brenner tumors. A description of the natural behavior of the different histotypes is essential for the selection of the most appropriate surgical strategy.
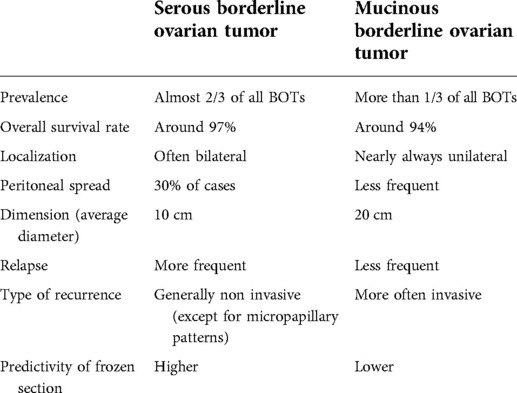
Table 1. Main characteristics of the two most common BOTs histotypes.
Serous borderline ovarian tumors (sBOTs) are bilateral in 15%–25% of cases and noninvasive peritoneal spread is present in 15%/40% of cases (7) (Figure 1). The risk of invasive peritoneal spread is very low in early-stage serous tumors; only in a small percentage of cases do the implants infiltrate the underlying subperitoneal tissue and should thus be considered, according to the 2014 WHO (World Health Organization), as low-grade serous carcinoma (8).

Figure 1. Ovarian serous borderline tumor.
The micropapillary/cribriform pattern is a variant of the common sBOT.
This lesion is defined by distinct morphological criteria and is more likely associated with a higher rate of bilateral ovarian involvement, recurrence, and invasive peritoneal implants compared with serous lesions without micropapillary patterns (9).
Mucinous borderline ovarian tumors (mBOTs) represent the second most common histologic subtype accounting for 30%–50% of all borderline ovarian tumors. Mucinous borderline tumors are nearly always unilateral and tend to be larger than sBOTs (average diameter of 20 cm) (Table 1) (10). Patients with mBOTs relapse less frequently than patients with serous disease, but when an extraovarian relapse occurs, the risk of an invasive recurrence and possible death seems to be higher (11).
An electronic database search (Pubmed, Medline and Embase) was performed up to April 2022.
A search algorithm was developed incorporating the following medical terms “borderline ovarian tumors”, “low malignant potential”, “conservative surgery”, “fertility-sparing surgery”, “laparoscopy”, “invasive implants”, “micropapillary patterns”, “recurrence”.
All pertinent articles evaluating the diagnostic and therapeutic approaches centered on fertility-sparing treatment of borderline ovarian tumors have been included in this review.
All original studies, meta-analyses, systematic reviews and case reports published in English were considered. The reference lists were systematically reviewed to identify other studies for potential inclusion in this narrative review.
Fertility sparing surgery (FSS) has been defined as the preservation of the uterus and ovarian tissue in one or both adnexa (12). More than a third of BOTs affect women of reproductive age who wish to preserve their fertility potential.
In the management of early-stage BOTs, FSS is the mainstay of treatment, as an alternative to radical surgery (13).
In the advanced stages of the disease, the oncological safety of conservative treatment has still to be clarified (14). As a rule, patients with advanced-stage BOT should be considered not amenable to conservative surgical therapy in the presence of invasive implants or noninvasive implants not completely resectable (15–17).
Great attention has been recently focused on uterine preservation in the management of patients where preservation of healthy ovarian tissue is not feasible (18).
Indeed, ovarian tissue cryopreservation at the time of surgery, oocyte freezing, oocyte donation or a transfer of frozen embryos obtained before the surgical procedure are proposed to permit fertility (12, 19, 20).
FSS does not seem to affect the overall survival (21) however conservative treatment has been found to increase the relapse rate and therefore it is necessary to give full information to the patients about this risk.
Although the definitive diagnosis requires pathological evaluation after surgical excision, however preoperative knowledge of the specific ultrasonographic and macroscopic MRI features to differentiate BOTs subtypes can be extremely helpful to promote optimal patient management (22, 23).
The Frozen section (FS) plays an additional important role in determining the appropriate surgical management however, the surgeon should be aware of the well-known limitations of FS. The diagnostic accuracy rate for FS remains high for benign and malignant ovarian tumors but is relatively low for BOTs.
Frozen samples tend to under diagnose BOT as benign tumors in 25%–30% of cases, and improperly identify BOTs as carcinoma in 20%–30% of cases (24, 25). More caution in the use of FS in BOTs is needed, especially in cases of bulky tumors, where the intraoperative histology may lead to misdiagnosis of some features (e.g., microinvasion, papillary variant,intraepithelial carcinoma, stromal microinvasion) (26–28).
Although surgical staging does not have a significant impact on survival rate (29), nevertheless an initial complete staging appears to significantly reduce recurrence among BOTs patients (30). A complete exploration of the abdominal-pelvic peritoneal cavity, peritoneal washing, multiple peritoneal biopsies, infracolic omentectomy and complete resection of the implants for staging purposes are recommended (31).
A primary task for the surgeon is the complete removal of all peritoneal implants for both staging and therapeutic purposes with wide resection of surrounding tissue to allow the pathologist to discriminate non-invasive from invasive implants (32).
For the aforementioned reasons, surgical restaging should be considered in patients at higher risk of malignancy (mBOT, micropapillary variant, etc.) who underwent incomplete visual exploration of the abdominal pelvic peritoneum at the first surgery (33).
Lymph nodes involvement has a low prognostic value (34). In a retrospective analysis by Matsuo et al., no difference was found in survival rates in patients undergoing lymphadenectomy (35).
Lymphadenectomy is usually suggested only for cases with enlarged lymph nodes or invasive tumors detected on frozen examination (36, 37).
Obtaining a biopsy for the histopathologic evaluation from a normal appearing contra-lateral ovary is not helpful to reduce the risk of recurrence; an accurate preoperative ultrasonographic examination and a careful intraoperative macroscopic inspection is considered adequate for this purpose (38).
The use of minimally invasive or traditional open surgery has been evaluated in the literature: whatever the approach used, rupture of an intact tumor during its dissection/removal could alter the FIGO staging and affect the risk of recurrence (36).
In the last years, the use of minimally invasive procedure has increased dramatically, because of their reduced postoperative complications, blood loss, shorter postoperative recovery and cosmetic results. However, the decision on the surgical approach for BOT patients should be based on preoperative diagnostic features, epidemiological aspect and the surgeon's skill.
Published data report an increased intraoperative tumor rupture during laparoscopy cystectomies and identifies tumor volume as the main predictor factor.
Indeed, in a retrospective study of 105 patients, the tumor rupture was significantly more frequent during laparoscopy compared to laparotomy (29.5% vs. 13.1%, p = 0.038) (39). The conversion laparotomy rates is reporting of approximately 30% for BOT patients (40).
In another retrospective analysis, adnexa larger than 10 cm in maximum diameter were associated with a 4-fold risk of surgical spillage with laparoscopic approach (54.5% vs. 12.1%) compared to open surgery (37).
The laparoscopy compared to laparotomy has not shown a negative impact in terms of the recurrence rate, the survival and the feasibility of surgical management of BOTs (41). If surgery without risk of tumor rupture is possible, then the laparoscopic approach could be considered feasible, safe and recommended over laparotomy (40).
Robotic surgery is a feasible alternative in managing ovarian cancer as long as there is careful consideration given to patient selection (42). Robotic surgery is considered an option for the treatment borderline ovarian tumors, however the haptic feedback allowing to measure tissue traction and avoid cyst rupture is present only in some robotic platforms (43). Prospective randomized studies are needed to determine the relevance of robotic surgery in this context.
Another ultra minimally invasive approaches is the mini-laparoscopy that represents a great challenge for adnexal disease. Gueli Alletti et al. (44) have described a successful case of conservative staging surgery through the use of 2.4 mm needleoscopic instruments concluding that this could prove a beneficial tool in borderline disease.
There is a lack of clear international guidelines on the optimal FSS procedure. FSS in stage I include unilateral/bilateral cystectomy, unilateral salpingo-oophorectomy and unilateral salpingo-oophorectomy plus contra-lateral cystectomy.
The impact of the histological subtype and the presence of factors associated with poor prognosis (microinvasion, micropapillary pattern, peritoneal implants) on FSS approach is relevant (45). As most mBOTs are at high risk of invasive recurrence and co-existence with invasive cancer areas is possible, unilateral salpingo-oophorectomy is considered the preferred surgical treatment in these cases (46); cystectomy is admissible only in presence of bilateral mBOT or when controlateral cystectomy is the only method to preserve fertility in patients with previous salpingo-oophorectomy (47).
Concerning sBOTs, often bilateral and characterized by a relatively benign behavior compared to mBOTs, the theoretically reproductive advantage of cystectomy as opposed to unilateral salpingo-oophorectomy is still waiting for a definitive conclusion.
The reproductive outcome seems not different between unilateral oophorectomy and cystectomy (48) on the other hand, but the available literature has raised concerns about a higher recurrence rate after cystectomy (49).
In a French multicenter study, including 313 patients with stage I BOTs, the recurrence rates after cystectomy, unilateral salpingo-oophorectomy or bilateral salpingo-oophorectomy have been found as 30.3%, 11% and 1.7%, respectively (50).
These results have been confirmed in a recent systematic review reporting the rate of recurrence correlated with the type of conservative surgery with a higher rate after cystectomy (41).
As opposite, Palomba et al. report that the use of bilateral cystectomy compared with a unilateral salpingo-oophorectomy and a contralateral cystectomy (in patients with bilateral BOTs, mainly in serous subtype) increases the fertility rate without increasing the recurrence rate (51). Vasconcelos et al. confirmed these results in a meta-analysis showing that, in case of bilateral serous BOT, unilateral salpingo-oophorectomy + contra-lateral cystectomy did not obtain any advantage compared to bilateral cystectomy in terms of recurrence (26.1% vs. 25.6%) (52). Standing this unresolved dispute, it is wise to concludethat whenever cystectomy is the selected procedure then appropriate counseling is recommended about a possible higher risk of local and peritoneal recurrence compared with salpingo-oophorectomy.
Obviously, cystectomy or unilateral salpingectomy + contra-lateral cystectomy remains the only fertility-sparing option in case of bilateral sBOT and in rare cases of previous surgical salpingo-oophorectomy (53).
Conservative management has a significant impact on the development of BOTs recurrence if compared with radical surgery (5%–34% vs. 3.2%–7%) (52, 53).
The overall risk of recurrence varies between 2% and 24% and the risk of invasive recurrence ranges from 0.5% to 3.8%. Recurrences are seen in the remnant ovary after cystectomy, or in contralateral ovary or as extraovarian peritoneal and omental implants (54).
Complete surgical eradication of ovarian tumors and peritoneal implants even if not visible macroscopically is the prerequisite in minimizing the risk of disease relapse; pre- and intra-operative ultrasounds are of invaluable help to accomplish this goal (55).
Twenty-five percent of recurrences are diagnosed after 5 years (56); however, the recurrence rate is time-dependent and relapses may occur 15 years after surgery.
During the first two post-operative years, recurrences seem to be more frequent; a close follow-up is needed for this period through a systematic clinical examination including transvaginal ultrasonography and serum markers (57); unfortunately, only 40% of women with stage I BOTs have elevated levels of Ca125 and can benefit of this diagnostic measure (58, 59).
Most of sBOTs recurrences are in greater part borderline tumors, easily treated by repeated conservative surgery in patients desiring to preserve fertility (60).
Concerning mBOTs, if the risk of relapse is significantly lower compared with sBOTs, on the other side the risk of an invasive recurrence is higher (61).
Along with the histotype, some further clinico-pathological factors, although not unanimously, are considered helpful to identify patients more prone to invasive recurrence (60, 62).
Early-stage according to FIGO classification is a well-known independent risk factor for recurrence (63, 64); indeed, the rate of extraovarian recurrence has been demonstrated higher in stage IC3 and grade 3 tumors and consequently such aspects should be recognized as limits of conservative management for oncology safety (65).
Other factors such as micropapillary pattern and stromal microinvasion are histological aspects featuring a high-risk group likely to develop an invasive recurrence (57, 66).
Serous borderline ovarian tumors with micropapillary patterns seem to be more commonly associated with advanced stage, bilateral ovarian involvement, and invasive recurrence than the typical sBOTs (67, 68).
Notably, serous BOT displaying a micropapillary pattern without implants (stage I) or with non-invasive implants (stage II and III) could have the same prognosis as serous BOT without a micropapillary pattern (69).
On this basis, in case of micropapillary serous BOT without invasive implants it could be reasonable to propose a conservative approach only if combined with a careful and long follow-up (70); radical surgery to avoid any recurrence should be considered in those patients who completed their reproductive plans after conservative surgery or in cases without follow-up opportunities (71).
Data from literature identifies, stromal microinvasion, defined as a lesion that invades the stroma to a depth of 5 mm or less as a predictor of relapses: In a case series evaluating follow up data of 171 borderline mucinous tumors,microinvasive pattern was associated with an higher reuccrence rate (p = 0.013). In particular, in the group without microinvasion the rate of recurrence was 1.7% (2 of 116 cases), whereas in the group with microinvasion 14.3% (4 of 28 cases). No significant association was reported between clinicopathologic variables of these tumor and recurrence (72).
Higher rate of recurrence were also reported in a a retrospective study conducted on 902 patients with BOTs. Patients with microinvasive BOT had a significantly higher rate of recurrence than patients without microinvasive BOT (17.4 vs. 7.8%, OR 3.55, 95% CI 1.091–11.59, p = 0.03) . In particular stromal microinvasion was found as a prognostic factor for significantly shorter disease free survival (26.7 vs. 11.9 months, p = 0.031) (73).
In addition, data from 209 patients confirm that microinvasive BOTs recurred earlier with respect to noninvasive BOTs, with the median time to recurrence of 10.5 months for the first one and 17 months for the latter .For these patients unilateral salpingo-oophorectomy instead of cystectomy seems to not prevent relapses in microinvasive BOTs, that were recorded in 27% of the patients (74). However, in the studies, the overall survival seems to not differ significantly from BOTs without microinvasion.
Regrettably, microinvasion is associated with high frequency with the micropapillary variant in the serous BOTs and this is a potential confounding factor to identify its exact role in the genesis of recurrence (75–77). Due to these uncertainties, also for these patients, fertility-sparing surgery may be a reasonable option in young patients with BOTs, only if an accurate and strict follow-up is possible (78). Frequency and types of exams to perform in the follow-up surveillance are not established (79).
Studies provide inconclusive findings about the impact of fertility-sparing treatments for BOTs on ovarian function (80) and an unanswered question remain whether pregnancy outcome is determined by the type of conservative approach (unilateral salpingo-oophorectomy/ovarian cystectomy). It is clear that ovarian surgery, especially after a second attempt, may reduce healthy ovarian parenchyma, increasing the risk of infertility. Moreover, the occurrence of postoperative adhesions might interfere with fallopian tube function (80–83).
However, after fertility-sparing surgery, pregnancy outcomes are encouraging and most pregnancies are achieved spontaneously as early as 3 months after surgery (84).
To avoid pregnancies complicated by recurrent disease, many physicians recommend delaying pregnancy until a sufficient follow-up period after initial surgical treatment (85, 86).
Little is known about the incidence and management of BOTs during pregnancy; however, expectant management could be a safe option in case of recurrences in pregnancy (87).
There is no specific data on the management of infertility following conservative treatment of BOTs and it is unclear if there is a potential impact of the use of fertility drugs on the recurrence rate of the disease (88).
Further data are needed on this topic considering that induction of ovulation and in vitro fertilization may be required in order to enhance the chance of conceiving.
Little is known about incidence and management of BOTs during pregnancy. In reported literature, Borderline tumors diagnosed in pregnancy contain features concerning for aggressive behavior if compared to those diagnosed in non pregnant patients. A higher incidence of advanced stage at presentation as well as an higher higher percentage of mucinous BOT with intraepithelial carcinoma and microinvasion, and serous BOT with micropapillary component have been reported (89).
Unfortunately, concerning the management of BOT during pregnancy,only limited data, based mostly on case reports, are present in the literature.
As such, the standardization of the management strategy during pregnancy is difficult and, at the moment, it is based on the gold standard treatment of non-pregnant women.
An attitude of close surveillance should be adopted to exclude sign of malignant transformation (rapid enlargement of tumor, abnormal vascularization, presence of solid tissue) (90).
It is advisable that pregnancy and delivery are carried out in a tertiary center specialized in gynecology oncology. Technical difficulties of performing a complete staging for these patients at the initial surgery could necessitate a post partum completion staging or a debulking procedure and eventually an adjuvant chemotherapy (91).
Fertility-sparing surgery is a well-established strategy available for patients with BOTs who desire to preserve fertility. This procedure is characterized by an excellent reproductive outcome and long-term survival.
Invasive recurrences remain one of the most important parameters of the safety of FSS. Unfortunately, the paucity of available data does not permit a definite identification of the prognostic factors of recurrence and makes the extent of conservative surgery as well as the modalities of a careful and effective post-operative follow-up still matter of debate.
Additional well-designed prospective studies, with larger samples, are needed to clarify these unresolved issues.
AM, LDC, PS undertook the searches. PG, MB, CB contributed to data extraction and drafted the manuscript. AM, MP, FV, MCDA, MT participated in data analysis and interpretation, preparation of the manuscript and critically revising the paper, conceived the idea of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Fischerova D, Zikan M, Dundr P, Cibula D. Diagnosis, treatment, and follow-up of borderline ovarian tumors. Oncologist. (2012) 17(12):1515–33. doi: 10.1634/theoncologist.2012-0139
2. Colombo N, Sessa C, du Bois A, Ledermann J, McCluggage WG, McNeish I, et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Ann Oncol. (2019) 30(5):672–705. doi: 10.1093/annonc/mdz062
3. Kempson RL, Hendrickson MR. Ovarian serous borderline tumors: the citadel defended. Hum Pathol. (2000) 31(5):525–6. doi: 10.1053/hp.2000.8046
4. Pereira A, Pérez-Medina T, Magrina JF, Magtibay PM, Rodríguez-Tapia A, Peregrin I, et al. International Federation of gynecology and obstetrics staging classification for cancer of the ovary, fallopian tube, and peritoneum: estimation of survival in patients with node-positive epithelial ovarian cancer. Int J Gynecol Cancer. (2015) 25:49–54. doi: 10.1097/IGC.0000000000000316
5. Trillsch F, Mahner S, Ruetzel J, Harter P, Ewald-Riegler N, Jaenicke F, et al. Clinical management of borderline ovarian tumors. Expert Rev Anticancer Ther. (2010) 10:1115–24. doi: 10.1586/era.10.90
6. Huchon C, Bourdel N, Abdel Wahab C, Azaïs H, Bendifallah S, Bolze PA, et al. Borderline ovarian tumors: French guidelines from the CNGOF. Part 1. Epidemiology, biopathology, imaging and biomarkers. J Gynecol Obstet Hum Reprod. (2021) 50(1):101965. doi: 10.1016/j.jogoh.2020.101965
7. Vancraeynest E, Moerman P, Leunen K, Amant F, Neven P, Vergote I. Fertility preservation is safe for serous borderline ovarian tumors. Int J Gynecol Cancer. (2016) 26(8):1399–406. doi: 10.1097/IGC.0000000000000782
8. Kurman RJ, Carcangiu ML, Herrington CS. WHO classification of tumours of female reproductive organs. Lyon: IARC Press (2014). 264–98 pp.
9. Chang SJ, Ryu HS, Chang KH, Yoo SC, Yoon JH. Prognostic significance of the micropapillary pattern in patients with serous borderline ovarian tumors. Acta Obstet Gynecol Scand. (2008) 87(4):476–81. doi: 10.1080/00016340801995640
10. Hart WR. Mucinous tumors of the ovary: a review. Int J Gynecol Pathol. (2005) 24:4–25. PMID: 15626914
11. Barnhill DR, Kurman RJ, Brady MF, Omura GA, Yordan E, Given FT, et al. Preliminary analysis of the behavior of stage I ovarian serous tumors of low malignant potential: a gynecologic oncology group study. J Clin Oncol. (1995) 13(11):2752–6. doi: 10.1200/JCO.1995.13.11.2752
12. Darai E, Fauvet R, Uzan C, Gouy S, Duvillard P, Morice P. Fertility and borderline ovarian tumor: a systematic review of conservative management, risk of recurrence and alternative option. Hum Reprod Update. (2013) 19:151–66. doi: 10.1093/humupd/dms047
13. Maramai M, Barra F, Menada MV, Stigliani S, Moioli M, Costantini S, et al. Borderline ovarian tumours: management in the era of fertility-sparing surgery. Ecancermedicalscience. (2020) 14:1031. doi: 10.3332/ecancer.2020.103
14. Kasaven LS, Chawla M, Jones BP, Al-Memar M, Galazis N, Ahmed-Salim Y, et al. Fertility sparing surgery and borderline ovarian tumours. Cancers (Basel). (2022) 14(6):1485. doi: 10.3390/cancers14061485
15. Kane A, Uzan C, Rey A, Gouy S, Camatte S, Pautier P, et al. Prognostic factors in patients with ovarian serous low malignant potential (borderline) tumors with peritoneal implants. Oncologist. (2009) 14(6):591–600. doi: 10.1634/theoncologist.2008-0263
16. Longacre TA, McKenney JK, Tazelaar HD, Kempson RL, Hendrickson MR. Ovarian serous tumors of low malignant potential (borderline tumors): outcome-based study of 276 patients with long-term (> or =5-year) follow-up. Am J Surg Pathol. (2005) 29(6):707–23. doi: 10.1097/01.pas.0000164030.82810.db
17. Uzan C, Kane A, Rey A, Gouy S, Duvillard P, Morice P. Outcomes after conservative treatment of advanced-stage serous borderline tumors of the ovary. Ann Oncol. (2010) 21(1):55–60. doi: 10.1093/annonc/mdp267
18. Mangili G, Somigliana E, Giorgione V, Martinelli F, Filippi F, Petrella MC, et al. Fertility preservation in women with borderline ovarian tumours. Cancer Treat Rev. (2016) 49:13–24. doi: 10.1016/j.ctrv.2016.06.010
19. Fain-Kahn V, Poirot C, Uzan C, Prades M, Gouy S, Genestie C, et al. Feasibility of ovarian cryopreservation in borderline ovarian tumours. Hum Reprod. (2009) 24(4):850–5. doi: 10.1093/humrep/den459
20. Huang JYJ, Buckett WM, Gilbert L, Tan SL, Chian R-C. Retrieval of immature oocytes followed by in vitro maturation and vitrification: a case report on a new strategy of fertility preservation in women with borderline ovarian malignancy. Gynecol Oncol. (2007) 105(2):542–4. doi: 10.1016/j.ygyno.2007.01.036
21. Mandelbaum RS, Blake EA, Machida H, Grubbs BH, Roman LD, Matsuo K. Utero-ovarian preservation and overall survival of young women with early-stage borderline ovarian tumors. Arch Gynecol Obstet. (2019) 299(6):1651–8. doi: 10.1007/s00404-019-05121-z
22. Wahab C A, Rousset P, Bolze PA, Thomassin-Naggara I. Tumeurs frontières de l’ovaire. Recommandations pour la pratique clinique du CNGOF – imagerie [borderline ovarian tumours: CNGOF guidelines for clinical practice - imaging]. Gynecol Obstet Fertil Senol. (2020) 48(3):260–76. doi: 10.1016/j.gofs.2020.01.014
23. Marko J, Marko KI, Pachigolla SL, Crothers BA, Mattu R, Wolfman DJ. Mucinous neoplasms of the ovary: radiologic-pathologic correlation. Radiographics. (2019) 39(4):982–97. doi: 10.1148/rg.2019180221
24. Ureyen I, Turan T, Cirik DA, Tasci T, Boran N, Bulbul D, et al. Frozen section in borderline ovarian tumors: is it reliable? Eur J Obstet Gynecol Reprod Biol. (2014) 181:115–8. doi: 10.1016/j.ejogrb.2014.07.039
25. Ratnavelu ND, Brown AP, Mallett S, Scholten RJ, Patel A, Founta C, et al. Intraoperative frozen section analysis for the diagnosis of early stage ovarian cancer in suspicious pelvic masses. Cochrane Database Syst Rev. (2016) 3(3):CD010360. doi: 10.1002/14651858.CD010360.pub2
26. De Decker K, Jaroch KH, Edens MA, Bart J, Kooreman LFS, Kruitwagen RFPM, et al. Frozen section diagnosis of borderline ovarian tumors with suspicious features of invasive cancer is a devil's dilemma for the surgeon: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. (2021) 100(8):1369–76. doi: 10.1111/aogs.14105
27. Gungorduk K, Asicioglu O, Braicu EI, Almuheimid J, Gokulu SG, Cetinkaya N, et al. The impact of surgical staging on the prognosis of mucinous borderline tumors of the ovaries: a multicenter study. Anticancer Res. (2017) 37(10):5609–16. doi: 10.21873/anticanres.11995
28. Shim SH, Kim SN, Jung PS, Dong M, Kim JE, Lee SJ. Impact of surgical staging on prognosis in patients with borderline ovarian tumours: a meta-analysis. Eur J Cancer. (2016) 54:84–95. doi: 10.1016/j.ejca.2015.11.005
29. Cadron I, Leunen K, Van Gorp T, Amant F, Neven P, Vergote I. Management of borderline ovarian neoplasms. J Clin Oncol. (2007) 25(20):2928–37. doi: 10.1200/JCO.2007.10.8076
30. Zanetta G, Rota S, Chiari S, Bonazzi C, Bratina G, Mangioni C. Behavior of borderline tumors with particular interest to persistence, recurrence, and progression to invasive carcinoma: a prospective study. J Clin Oncol. (2001) 19(10):2658–64. doi: 10.1200/JCO.2001.19.10.2658
31. Chevrot A, Héquet D, Fauconnier A, Huchon C. Impact of surgical restaging on recurrence in patients with borderline ovarian tumors: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. (2020) 248:227–32. doi: 10.1016/j.ejogrb.2020.03.023
32. Seidman JD, Kurman RJ. Ovarian serous borderline tumors: a critical review of the literature with emphasis on prognostic indicators. Hum Pathol. (2000) 31(5):539–57. doi: 10.1053/hp.2000.8048
33. Matsuo K, Machida H, Takiuchi T, Grubbs BH, Roman LD, Sood AK. Role of hysterectomy and lymphadenectomy in the management of early-stage borderline ovarian tumors. Gynecol Oncol. (2017) 144(3):496–502. doi: 10.1016/j.ygyno.2017.01.019
34. Seracchioli R, Venturoli S, Colombo FM, Govoni F, Missiroli S, Bagnoli A. Fertility and tumor recurrence rate after conservative laparoscopic management of young women with early-stage borderline ovarian tumors. Fertil Steril. (2001) 76:999–1004. doi: 10.1016/s0015-0282(01)02842-4
35. Qian XQ, Hua XP, Wu JH, Shen YM, Cheng XD, Wan XY. Clinical predictors of recurrence and prognostic value of lymph node involvement in the serous borderline ovarian tumor. Int J Gynecol Cancer. (2018) 28(2):279–84. doi: 10.1097/IGC.0000000000001154
36. Vergote I, De Brabanter J, Fyles A, Bertelsen K, Einhorn N, Sevelda P, et al. Prognostic importance of degree of differentiation and cyst rupture in stage I invasive epithelial ovarian carcinoma. Lancet. (2001) 357(9251):176–82. doi: 10.1016/S0140-6736(00)03590-X
37. Casarin J, Laganà AS, Uccella S, Cromi A, Pinelli C, Gisone B, et al. Surgical treatment of large adnexal masses: a retrospective analysis of 330 consecutive cases. Minim Invasive Ther Allied Technol. (2020) 29(6):366–74. doi: 10.1080/13645706.2019.1649700
38. Salcedo-Hernández RA, Cantú-de-León DF, Pérez-Montiel D, García-Pérez L, Lino-Silva LS, Zepeda-Najar C, et al. The usefulness of intraoperative consultation for the diagnosis of borderline ovarian tumors. Ann Transl Med. (2021) 9(3):261. doi: 10.21037/atm-20-3932
39. Trillsch F, Ruetzel JD, Herwig U, Doerste U, Woelber L, Grimm D, et al. Surgical management and perioperative morbidity of patients with primary borderline ovarian tumor (BOT). J Ovarian Res. (2013) 6(1):48. doi: 10.1186/1757-2215-6-48
40. Fauvet R, Boccara J, Dufournet C, Poncelet C, Darai E. Laparoscopic management of borderline ovarian tumors: results of a French multicenter study. Ann Oncol. (2005) 16:403–10. doi: 10.1093/annonc/mdi083
41. du Bois A, Ewald-Riegler N, de Gregorio N, Reuss A, Mahner S, Fotopoulou C, et al. Borderline tumours of the ovary: a cohort study of the arbeitsgmeinschaft gynakologische onkologie (AGO) study group. Eur J Cancer. (2013) 49:1905–14. doi: 10.1016/j.ejca.2013.01.035
42. Iglesias DA, Ramirez PT. Role of minimally invasive surgery in staging of ovarian cancer. Curr Treat Options Oncol. (2011) 12:217. doi: 10.1007/s11864-011-0155
43. Cianci S, Rossitto C, Perrone E, Alletti SG. Senhance robotic platform for ovarian borderline tumor treatment: minimally invasive robotic approach for conservative adnexal surgery. Gynecol Pelvic Med. (2020) 3:27. doi: 10.21037/gpm-20-27
44. Gueli Alletti S, Rossitto C, Perrone E, Cianci S, De Blasis I, Fagotti A, et al. Needleoscopic conservative staging of borderline ovarian tumor. J Minim Invasive Gynecol. (2017) 24(4):529–30. doi: 10.1016/j.jmig.2016.10.009
45. Uzan C, Nikpayam M, Ribassin-Majed L, Gouy S, Bendifallah S, Cortez A, et al. Influence of histological subtypes on the risk of an invasive recurrence in a large series of stage I borderline ovarian tumor including 191 conservative treatments. Ann Oncol. (2014) 25(7):1312–9. doi: 10.1093/annonc/mdu139
46. Nomura K, Aizawa S, Hano H. Ovarian mucinous borderline tumors of intestinal type without intraepithelial carcinoma: are they still tumors of low malignant potential? Pathol Int. (2004) 54:420–24. doi: 10.1111/j.1440-1827.2004.01645.x
47. Salomon LJ, Lhommé C, Pautier P, Duvillard P, Morice P. Safety of simple cystectomy in patients with unilateral mucinous borderline tumors. Fertil Steril. (2006) 85(5):1510.e1-4. doi: 10.1016/j.fertnstert.2005.10.065
48. Johansen G, Dahm-Kähler P, Staf C, Flöter Rådestad A, Rodriguez-Wallberg KA. Reproductive and obstetrical outcomes with the overall survival of fertile-age women treated with fertility-sparing surgery for borderline ovarian tumors in Sweden: a prospective nationwide population-based study. Fertil Steril. (2021) 115(1):157–63. doi: 10.1016/j.fertnstert.2020.07.043
49. Abascal-Saiz A, Sotillo-Mallo L, de Santiago J, Zapardiel I. Management of borderline ovarian tumours: a comprehensive review of the literature. Ecancermedicalscience. (2014) 8:403. doi: 10.3332/ecancer.2014.403
50. Poncelet C, Fauvet R, Boccara J, Daraï E. Recurrence after cystectomy for borderline ovarian tumors: results of a French multicenter study. Ann Surg Oncol. (2006) 13(4):565–71. doi: 10.1245/ASO.2006.12.024
51. Palomba S, Falbo A, Del Negro S, Rocca M, Russo T, Cariati F, et al. Ultra-conservative fertility-sparing strategy for bilateral borderline ovarian tumours: an 11-year follow-up. Hum Reprod. (2010) 25(8):1966–72. doi: 10.1093/humrep/deq159
52. Vasconcelos I, de Sousa Mendes M. Conservative surgery in ovarian borderline tumours: a meta-analysis with emphasis on recurrence risk. Eur J Cancer. (2015) 51(5):620–31. doi: 10.1016/j.ejca.2015.01.004
53. Tropé CG, Kaern J, Davidson B. Borderline ovarian tumours. Best Pract Res Clin Obstet Gynaecol. (2012) 26(3):325–36. doi: 10.1016/j.bpobgyn.2011.12.006
54. Daraï E, Fauvet R, Uzan C, Gouy S, Duvillard P, Morice P. Fertility and borderline ovarian tumor: a systematic review of conservative management, risk of recurrence and alternative options. Hum Reprod Update. (2013) 19(2):151–66. doi: 10.1093/humupd/dms047
55. Qi Y, Wang M, Yang Y, Zeng Z, Zhou Y. Analysis of factors influencing relapse and pregnancy in patients with borderline ovarian tumors. J Cancer. (2021) 12(17):5275–85. doi: 10.7150/jca.56387
56. du Bois A, Trillsch F, Mahner S, Heitz F, Harter P. Management of borderline ovarian tumors. Ann Oncol. (2016) 27(Suppl 1):i20–2. doi: 10.1093/annonc/mdw090
57. Bentivegna E, Fruscio R, Roussin S, Ceppi L, Satoh T, Kajiyama H, et al. Long-term follow-up of patients with an isolated ovarian recurrence after conservative treatment of epithelial ovarian cancer: review of the results of an international multicenter study comprising 545 patients. Fertil Steril. (2015) 104(5):1319–24. doi: 10.1016/j.fertnstert.2015.06.008
58. Romeo M, Pons F, Barretina P, Radua J. Incomplete staging surgery as a major predictor of relapse of borderline ovarian tumor. World J Surg Oncol. (2013) 11:13. doi: 10.1186/1477-7819-11-13
59. Poncelet C, Fauvet R, Yazbeck C, Coutant C, Darai E. Impact of serum tumor marker determination on the management of women with borderline ovarian tumors: multivariate analysis of a French multicentre study. Eur J Surg Oncol. (2010) 36(11):1066–72. doi: 10.1016/j.ejso.2010.07.004
60. Morice P, Uzan C, Fauvet R, Gouy S, Duvillard P, Darai E. Borderline ovarian tumour: pathological diagnostic dilemma and risk factors for invasive or lethal recurrence. Lancet Oncol. (2012) 13(3):e103–15. doi: 10.1016/S1470-2045(11)70288-1
61. Nyangoh-Timoh K, Bendifallah S, Dion L, Ouldamer L, Levêque J. Tumeurs frontières de l’ovaire. Recommandations pour la pratique clinique du CNGOF – pertinence des marqueurs tumoraux [borderline ovarian tumours: CNGOF guidelines for clinical practice - value of tumor markers]. Gynecol Obstet Fertil Senol. (2020) 48(3):277–86. doi: 10.1016/j.gofs.2020.01.015
62. Buonomo B, Peccatori FA. Fertility preservation strategies in borderline ovarian tumor recurrences: different sides of the same coin. J Assist Reprod Genet. (2020) 37(5):1217–9. doi: 10.1007/s10815-020-01738-1
63. Birge O, Bakır MS, Karadag C, Dinc C, Dogan S, Tuncer HA, et al. Risk factors that increase recurrence in borderline ovarian cancers. Am J Transl Res. (2021) 13(7):8438–49. PMID: 34377341
64. He Y, Zhong J, Yang H, Shan N, Cheng A. Clinical characteristics predict recurrence in borderline ovarian tumor patients with fertility-preserving surgery. Int J Gen Med. (2022) 15:2197–206. doi: 10.2147/IJGM.S349451
65. Ditto A, Leone Roberti Maggiore U, Bogani G, Martinelli F, Chiappa V, Evangelista MT, et al. Predictive factors of recurrence in patients with early-stage epithelial ovarian cancer. Int J Gynaecol Obstet. (2019) 145(1):28–33. doi: 10.1002/ijgo.12769
66. Childress KJ, Patil NM, Muscal JA, Dietrich JE, Venkatramani R. Borderline ovarian tumor in the pediatric and adolescent population: a case series and literature review. J Pediatr Adolesc Gynecol. (2018) 31(1):48–54. doi: 10.1016/j.jpag.2017.09.001
67. Benito V, Lubrano A, Arencibia O, Medina N, Álvarez Eva E, Andújar M, et al. Serous and mucinous borderline ovarian tumors: are there real differences between these two entities? Eur J Obstet Gynecol Reprod Biol. (2010) 153(2):188–92. doi: 10.1016/j.ejogrb.2010.07.024
68. Prat J. Serous tumors of the ovary (borderline tumors and carcinomas) with and without micropapillary features. Int J Gynecol Pathol. (2003) 22(1):25–8. doi: 10.1097/00004347-200301000-00007
69. Park SB, Kim MJ, Lee KH, Ko Y. Ovarian serous surface papillary borderline tumor: characteristic imaging features with clinicopathological correlation. Br J Radiol. (2018) 91(1088):20170689. doi: 10.1259/bjr.20170689
70. Malpica A, Longacre TA. Prognostic indicators in ovarian serous borderline tumours. Pathology. (2018) 50(2):205–13. doi: 10.1016/j.pathol.2017.12.001
71. Sozen H, Vatansever D, Topuz S, Iyibozkurt C, Kandemir H, Yalçin I, et al. Clinicopathological analysis of borderline ovarian tumours and risk factors related to recurrence: experience of single institution. J Obstet Gynaecol. (2019) 39(2):253–8. doi: 10.1080/01443615.2018.1499076
72. Khunamornpong S, Settakorn J, Sukpan K, Suprasert P, Siriaunkgul S. Mucinous tumor of low malignant potential (“borderline” or “atypical proliferative” tumor) of the ovary: a study of 171 cases with the assessment of intraepithelial carcinoma and microinvasion. Int J Gynecol Pathol. (2011) 30(3):218–30. doi: 10.1097/PGP.0b013e3181fcf01a
73. Boyraz G, Salman MC, Gultekin M, Ozkan NT, Uckan HH, Gungorduk K, et al. What is the impact of stromal microinvasion on oncologic outcomes in borderline ovarian tumors? A multicenter case-control study. Arch Gynecol Obstet. (2017) 296(5):979–87. doi: 10.1007/s00404-017-4496-4
74. Ferrero A, Strada I, Di Marcoberardino B, Maccarini LR, Pozzati F, Rossi M, et al. Clinical significance of microinvasion in borderline ovarian tumors and its impact on surgical management. Int J Gynecol Cancer. (2012) 22(7):1158–62. doi: 10.1097/IGC.0b013e31825e5254
75. Seong SJ, Kim DH, Kim MK, Song T. Controversies in borderline ovarian tumors. J Gynecol Oncol. (2015) 26(4):343–9. doi: 10.3802/jgo.2015.26.4.343
76. Prat J, De Nictolis M. Serous borderline tumors of the ovary: a long-term follow-up study of 137 cases, including 18 with a micropapillary pattern and 20 with microinvasion. Am J Surg Pathol. (2002) 26(9):1111–28. doi: 10.1097/00000478-200209000-00002
77. Ren J, Peng Z, Yang K. A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors. Gynecol Oncol. (2008) 110(2):162–7. doi: 10.1016/j.ygyno.2008.03.019
78. Laurent I, Uzan C, Gouy S, Pautier P, Duvillard P, Morice P. Results after conservative treatment of serous borderline tumours of the ovary with stromal microinvasion but without micropapillary pattern. BJOG. (2009) 116(6):860–2. doi: 10.1111/j.1471-0528.2009.02118.x
79. Candotti G, Peiretti M, Mangili G, Bergamini A, Candiani M, Cioffi R, et al. What women want: fertility sparing surgery in borderline ovarian tumours patients and pregnancy outcome. Eur J Surg Oncol. (2020) 46(5):888–92. doi: 10.1016/j.ejso.2019.11.001
80. Benedet JL, Bender H, Jones H, Ngan HY, Pecorelli S. FIGO Staging classifications and clinical practice guidelines in the management of gynecologic cancers. FIGO committee on gynecologic oncology. Int J Gynaecol Obstet. (2000) 70(2):209–62. doi: 10.1016/S0020-7292(00)00300-3
81. Somigliana E, Ragni G, Infantino M, Benedetti F, Arnoldi M, Crosignani PG. Does laparoscopic removal of nonendometriotic benign ovarian cysts affect ovarian reserve? Acta Obstet Gynecol Scand. (2006) 85(1):74–7. doi: 10.1080/00016340500334802
82. Bolnick A, Bolnick J, Diamond MP. Postoperative adhesions as a consequence of pelvic surgery. J Minim Invasive Gynecol. (2015) 22(4):549–63. doi: 10.1016/j.jmig.2014.12.009
83. Jones BP, Saso S, Farren J, El-Bahrawy M, Ghaem-Maghami S, Smith JR, et al. Ultrasound-guided laparoscopic ovarian wedge resection in recurrent serous borderline ovarian tumours. Int J Gynecol Cancer. (2017) 27(9):1813–8. doi: 10.1097/IGC.0000000000001096
84. Marchette M D, Ceppi L, Andreano A, Bonazzi CM, Buda A, Grassi T, et al. Oncologic and fertility impact of surgical approach for borderline ovarian tumours treated with fertility sparing surgery. Eur J Cancer. (2019) 111:61–8. doi: 10.1016/j.ejca.2019.01.021
85. Fauvet R, Poncelet C, Boccara J, Descamps P, Fondrinier E, Daraï E. Fertility after conservative treatment for borderline ovarian tumors: a French multicenter study. Fertil Steril. (2005) 83(2):284–90; quiz 525–6. doi: 10.1016/j.fertnstert.2004.10.009
86. Morris RT, Gershenson DM, Silva EG, Follen M, Morris M, Wharton JT. Outcome and reproductive function after conservative surgery for borderline ovarian tumors. Obstet Gynecol. (2000) 95(4):541–7. doi: 10.1016/s0029-7844(99)00619-5
87. Urbinati AM V, Iacobone AD, Di Pace RC, Pino I, Pittelli MR, Guerrieri ME, et al. Borderline ovarian tumor in pregnancy: can surgery wait? A case series. Arch Gynecol Obstet. (2021) 304(6):1561–8. doi: 10.1007/s00404-021-06080-0
88. Spaan M, van den Belt-Dusebout AW, Lambalk CB, van Boven HH, Schats R, Kortman M, et al. Long-term risk of ovarian cancer and borderline tumors after assisted reproductive technology. J Natl Cancer Inst. (2021) 113(6):699–709. doi: 10.1093/jnci/djaa163
89. Fauvet R, Brzakowski M, Morice P, Resch B, Marret H, Graesslin O, et al. Borderline ovarian tumors diagnosed during pregnancy exhibit a high incidence of aggressive features: results of a French multicenter study. Ann Oncol. (2012) 23(6):1481–7. doi: 10.1093/annonc/mdr452
90. Cosentino F, Turco LC, Cianci S, Fanfani F, Fagotti A, Alletti SG, et al. Management, prognosis and reproductive outcomes of borderline ovarian tumor relapse during pregnancy: from diagnosis to potential treatment options. J Prenat Med. (2016) 10(1–2):8–14. doi: 10.11138/jpm/2016.10.1.008
Keywords: bordeline ovarian tumor, conservative surgery, ovary, fertility, recurrence, survival
Citation: Della Corte L, Mercorio A, Serafino P, Viciglione F, Palumbo M, De Angelis MC, Borgo M, Buonfantino C, Tesorone M, Bifulco G and Giampaolino P (2022) The challenging management of borderline ovarian tumors (BOTs) in women of childbearing age. Front. Surg. 9:973034. doi: 10.3389/fsurg.2022.973034
Received: 19 June 2022; Accepted: 9 August 2022;
Published: 23 August 2022.
Edited by:
Ursula Catena, Agostino Gemelli University Polyclinic (IRCCS), ItalyReviewed by:
Luigi Turco, Mater Olbia Hospital, Italy© 2022 Della Corte, Mercorio, Serafino, Viciglione, Palumbo, De Angelis, Borgo, Buonfantino, Tesorone, Bifulco and Giampaolino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Mercorio YW50b25pb21lcmNvcmlvQGdtYWlsLmNvbQ==
Specialty Section: This article was submitted to Obstetrics and Gynecological Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.