 Aiyuan Guo
Aiyuan Guo Jie Gu
Jie Gu Jiayi Yang3,4*
Jiayi Yang3,4*

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 04 November 2022
Sec. Genitourinary Surgery and Interventions
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.959573
Background: This study aims to systematically evaluate predictive factors for lung metastasis (LM) in patients with testicular cancer (TC) and to investigate cancer-specific survival (CSS) and overall survival (OS) of LM in TC patients based on a large population-cohort.
Methods: A total of 10,414 patients diagnosed with TC during 2010–2015 were adopted from the Surveillance, Epidemiology, and End Results (SEER). After propensity score matching (PSM), 493 patients with LM were included for subsequent analysis. Univariate and multivariate logistic regression analyses were employed to identify risk factors, a nomogram was developed, and the receiver operating characteristic (ROC) curve was utilized to confirm the validation of the nomogram. Prognostic factors for OS and CSS among TC patients with LM were estimated via Cox proportional hazards models.
Results: Postmatching indicated that 11 parameters were successfully balanced between both groups (P > 0.05). After PSM, TC patients with LM presented an undesirable prognosis in both CSS and OS than those without LM (P < 0.001). The logistic regression model showed that tumor size; T stage; N stage; liver, brain, and bone metastases; and histology were positively associated with LM (P < 0.05). A nomogram was developed to predict diagnostic possibilities based on the independent risk variables, and the ROC curve verified the predictive capacity of the logistic regression model [area under the curve (AUC) = 0.910].
Conclusion: The selected variates in the nomogram can be predictive criteria for TC patients with LM. Brain metastasis, liver metastasis, and larger tumor size were prognostic factors for CCS and OS among TC patients with LM.
Testicular cancer (TC) is the most common malignancy among young men, gradually increasing over recent decades (1). Nonseminomatous germ cell tumor (NSGCT) is one of the major pathological types of TC, in which about half of the patients present with metastatic disease (2). For metastatic TC, the combination treatment is closely related to improved survival. However, TC is the only tumor with a mean age of survivors younger than 65 years, and its 5-year survival decreases sharply from 99% (without metastases) to 74% (metastases) (3, 4). In this regard, characterizing metastatic TC risk factors based on variant clinical outcomes is indispensable.
The most common metastatic site in TC patients is the lungs (5, 6). The incidence of TC metastasizing to the lungs has been increasing in recent years (3), possibly due to the improved diagnostic tools and appliance of developed multidisciplinary management on metastatic lung lesions such as surgical removal, radiation, salvage treatments, and systemic chemotherapy, which may contribute to the increased survival time and incidence of lung metastasis (LM) in TC patients (7–10). Furthermore, the treatments of metastatic TC have a profound impact on the quality of life of patients, such as sexual function, reproductive capacity, and psychological situation (11, 12). Unfortunately, risk factors and population-level estimates for prognosis related to the development of LM among TC patients, which removed confounding factors, have not been extensively studied.
Therefore, we employed propensity score matching (PSM) for the first time to balance the confounding biases between testicular patients with and without LM. What's more, we developed a nomogram to predict the probability of LM in TC patients.
This study is based on the Surveillance, Epidemiology, and End Results (SEER) database to identify predictive factors for LM in TC patients. Due to the poor prognosis of LM in TC patients and because its etiology remains unclear, prognosis factors such as clinical and sociodemographic predictors of poor survival in these patients were also investigated to assess the overall and cancer-specific survival (CSS) of TC patients with LM.
TC patients were identified from the SEER database (13). Since the details of LM were not available before 2010, primary TC patients initially diagnosed between 2010 and 2015 were collected (the latest data is on December 31, 2015). Patients diagnosed with TC from January 1, 2010 to December 31, 2015, were adopted to analyze risk factors.
Patients' demographic and clinical characteristics are presented as follows: age (<50 and ≥50 years), race (White, Black, others), marital status (married or unmarried), tumor grade (I = well-differentiated, II = moderately differentiated, III = poorly differentiated, IV = undifferentiated and anaplastic, unknown), primary tumor stage (T stage: T1, T2, T3, and T4), regional lymph node stage (N stage: N0, N1, N2, and N3), primary site (testis, descended testis, and undescended testis), histology (seminoma, nonseminoma, nongerminal neoplasm, and mixed tumor), laterality [left, right, bilateral, only one side (unspecified), and paired site], the presence of bone metastasis, liver metastasis, brain metastasis, tumor size (<67 mm and ≥67 mm), lymph nodes (regional, distant, none, and unknown), and lymph nodes size (≤2 cm, >2 cm and ≤5 cm, >5 cm, none). The differences in the LM incidence between the categorical variables were analyzed by Pearson's χ2 test or the rank-sum test.
PSM analysis (nearest-neighbor matching) was then utilized to adjust for differences between LM and non-LM TC patients (14). Propensity scores were analyzed using R (version 3.5.1). The covariates used in generating the propensity score included age, race, marital status, grade, primary site, histology, laterality, bone metastasis, liver metastasis, brain metastasis, T stage, N stage, tumor size, lymph nodes, and lymph node size. After PSM, 493 patients with LM were matched with patients without LM at a 1 : 1 ratio to assess the difference in survival probability (OS and CSS).
The risk factors for TC patients with de novo LM were determined by univariate and multivariate logistic regression analyses. The logistic regression model, which adopted the bidirectional elimination method and was optimized by the Akaike information criterion (AIC) protocol, was used to screen the risk factors. Then, a nomogram was developed by using the RMS package in R version 3.5.1 (http://www.r-project.org/). Harrell's C index and receiver operating characteristic (ROC) curve were used to evaluate the validation of the nomogram, which could assess the consistency between the actual and predicted results. The calibration curve described the average predictive estimate against actual observation and evaluated the nomogram performance visually, and the calibration plot was used for internal validation.
Prognostic factors for OS and CSS among TC patients with LM were estimated using univariate and multivariate analyses with Cox proportional hazards models. All statistical analyses were performed using R version 3.5.1; P-value < 0.05 was considered statistically significant.
A total of 10,414 patients diagnosed with TC during 2010–2015 met the inclusion criteria. The mean age of the patients at diagnosis was approximately 34.31 years, most of whom were White (91.16%). Among these patients, 493 patients were diagnosed with TC with LM during 2010–2015. The demographic and clinical characteristics of the included patients are presented in Table 1.
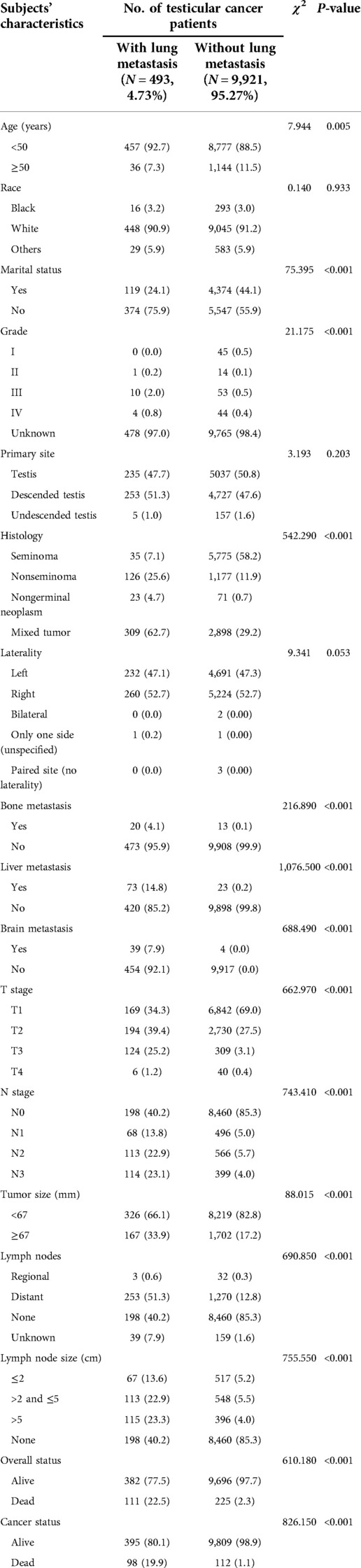
Table 1. Baseline of the demographic and clinical characteristics for patients diagnosed with testicular cancer.
A total of 493 patients with TC were diagnosed with LM (4.73%) among 10,414 patients, and the incidences of LM in the testis, descended testis, and undescended testis were 47.7%, 51.3%, and 1.0%, respectively, without a significant difference (P = 0.203) (Table 1). Subgroup analysis also showed that younger patients (<50 years) presented a significantly higher incidence of LM than those older patients (≥50 years) (χ2 = 7.944, P = 0.005). Moreover, patients with negative marital status (including single, unmarried, divorced, separated, and widowed patients) (χ2 = 75.395, P < 0.001), mixed tumor histology (χ2 = 542.290, P < 0.001), bone metastasis (χ2 = 216.890, P < 0.001), liver metastasis (χ2 = 1076.500, P < 0.001), brain metastasis (χ2 = 688.490, P < 0.001), higher T stage (χ2 = 662.970, P < 0.001), higher N stage (χ2 = 743.410, P < 0.001), lymph nodes metastasis (χ2 = 690.850, P < 0.001), lymph node size (χ2 = 755.550, P < 0.001), with alive cancer status (χ2 = 826.150, P < 0.001) and alive overall status (χ2 = 610.180, P < 0.001) presented higher LM incidence than their counterparts (Table 1).
To account for confounding bias inherent to TC patients with LM, PSM was used to adjust for differences in all variates (including age, race, marital status, grade, primary site, grade, histology, laterality, bone metastasis, brain metastasis, liver metastasis, T stage, N stage, tumor size, lymph nodes metastases, and lymph node size) (Table 2). Of the 493 available cases with LM, 493 cases without LM were able to be matched, and the matching ratio was 1 : 1. All 15 variables were involved in PSM. However, postmatching P-value indicated that 11 variables were successfully balanced between both groups while the other 4 variables (laterality, bone metastasis, brain metastasis, and liver metastasis) failed to be balanced, among which the P-value for laterality was NA and the P-values for the other three were >0.05.
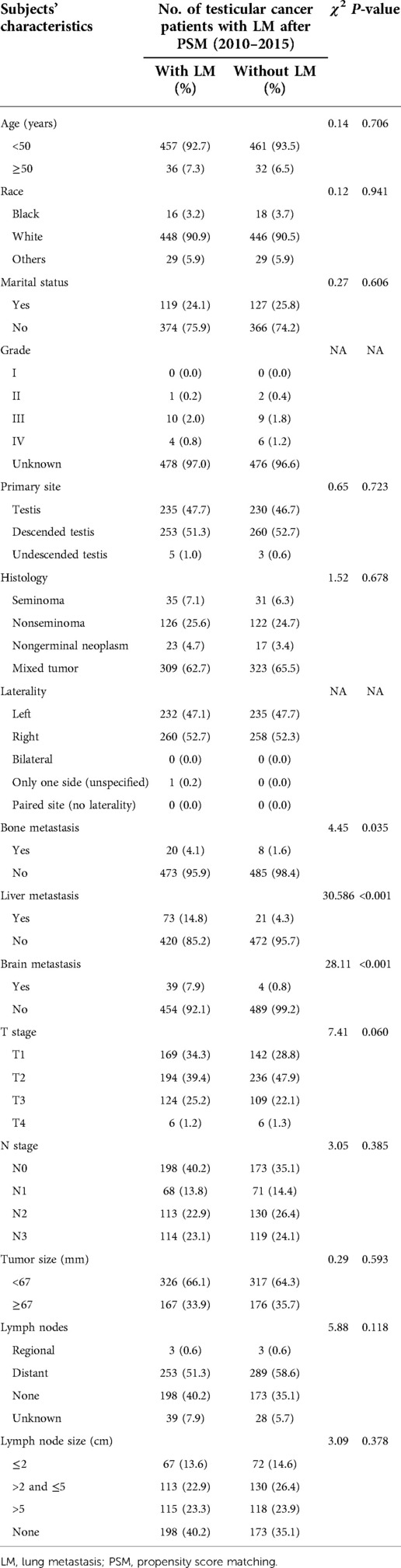
Table 2. Clinical characteristics of testicular cancer patients with lung metastasis after propensity score matching (n = 493).
Figures 1A,B describe the overall survival (OS) and CSS for 493 cases with LM after PSM, and the curves substantiated that the survival probability of TC patients with LM was significantly lower than those of TC patients without LM in both OS and CSS.
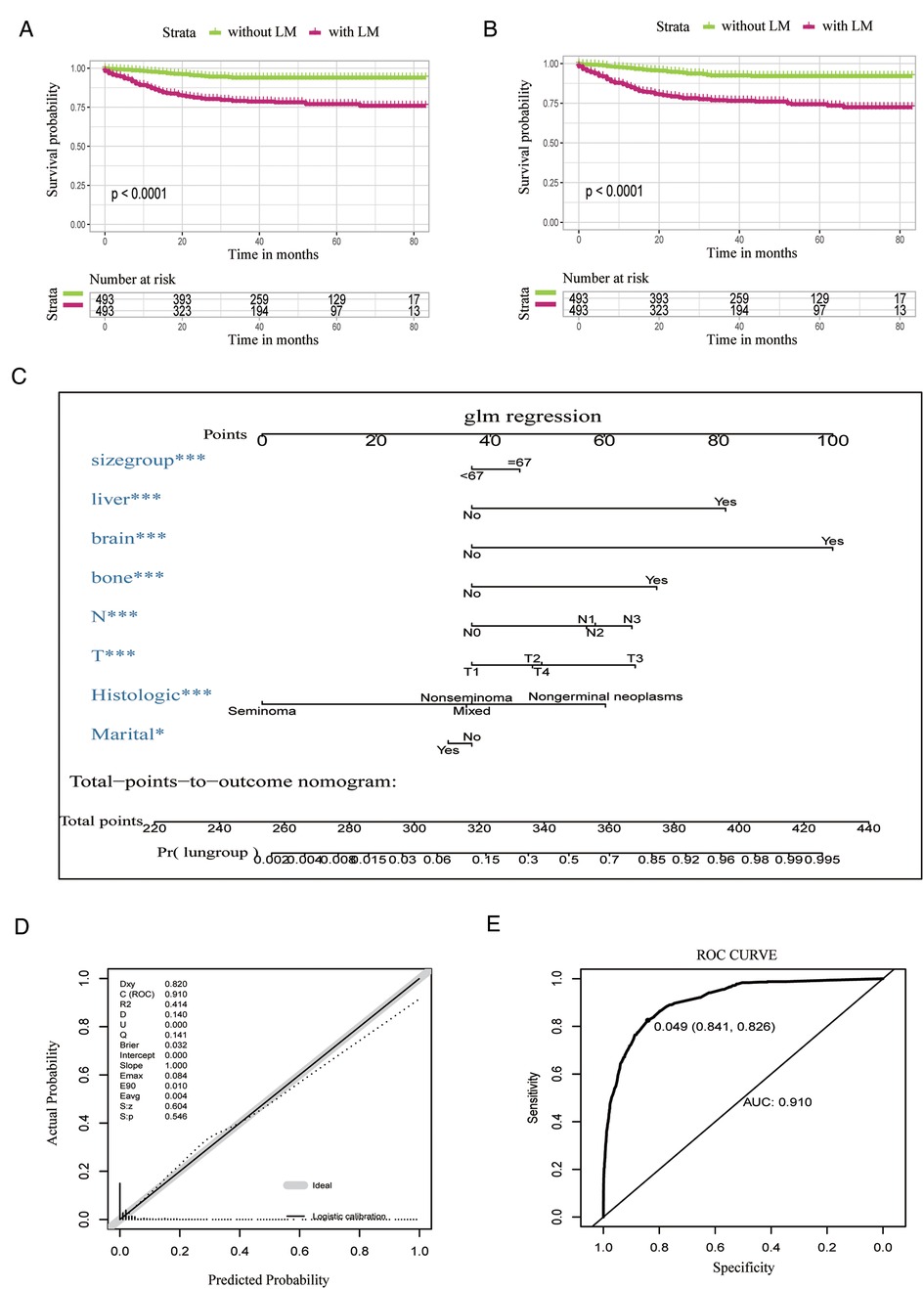
Figure 1. Survival analyses after PSM and the nomogram, the calibration curve for the nomogram, and summarized risks and prognostic factors for TC patients diagnosed with LM. (A) OS analysis after PSM. (B) CSS analysis after PSM. (C) Nomogram predicting the diagnostic possibility for lung metastasis based on the selected variables. (D) Logistic calibration curve of the nomogram. (E) ROC curve of logistic regression analysis. PSM, propensity score matching; TC, testicular cancer; LM, lung metastasis; OS, overall survival; CSS, cancer-specific survival; ROC, receiver operating characteristic.
Univariate logistic regression analysis showed that age [odds ratio (OR) = 0.60, 95% confidence interval (CI): 0.42–0.84, P = 0.004], marital status (OR = 0.40, 95% CI: 0.33–0.50, P < 0.001), and seminoma (OR = 0.06, 95% CI: 0.04–0.08, P < 0.001) were all negatively associated with LM incidence, while tumor grade III (OR = 3.85, 95% CI: 1.84–7.29, P < 0.001), nongerminal neoplasm (OR = 3.04, 95% CI: 1.83–4.86, P < 0.001), unspecified one-side laterality (OR = 2.02 × 100, 95% CI: 0.80–5.12 × 102, P < 0.034), bone metastasis (OR = 32.23, 95% CI: 16.10–66.78, P < 0.001), liver metastasis (OR = 74.80, 95% CI: 47.10–123.25, P < 0.001), brain metastasis (OR = 212.98, 95% CI: 85.29–712.33, P < 0.001), higher T stage (T2/T1: OR = 2.88, 95% CI: 2.33–3.55, P < 0.001; T3/T1: OR = 16.25, 95% CI: 12.54–21.02, P < 0.001; T4/T1: OR = 6.07, 95% CI: 2.29–13.48, P < 0.001), higher N stage (N1/N0: OR = 5.86, 95% CI: 4.36–7.79, P < 0.001; N2/N0: OR = 8.53, 95% CI: 6.65–10.89, P < 0.001; N3/N0: OR = 12.21, 95% CI: 9.48–15.67, P < 0.001), larger tumor size (≥67 mm) (OR = 2.47, 95% CI: 2.03–3.00, P < 0.001), and lymph nodes (regional: OR = 3.41, 95% CI: 0.82–9.61, P = 0.043; distant: OR = 7.24, 95% CI: 6.01–8.73, P < 0.001) were all significantly associated with high risk of LM individually (Table 3).
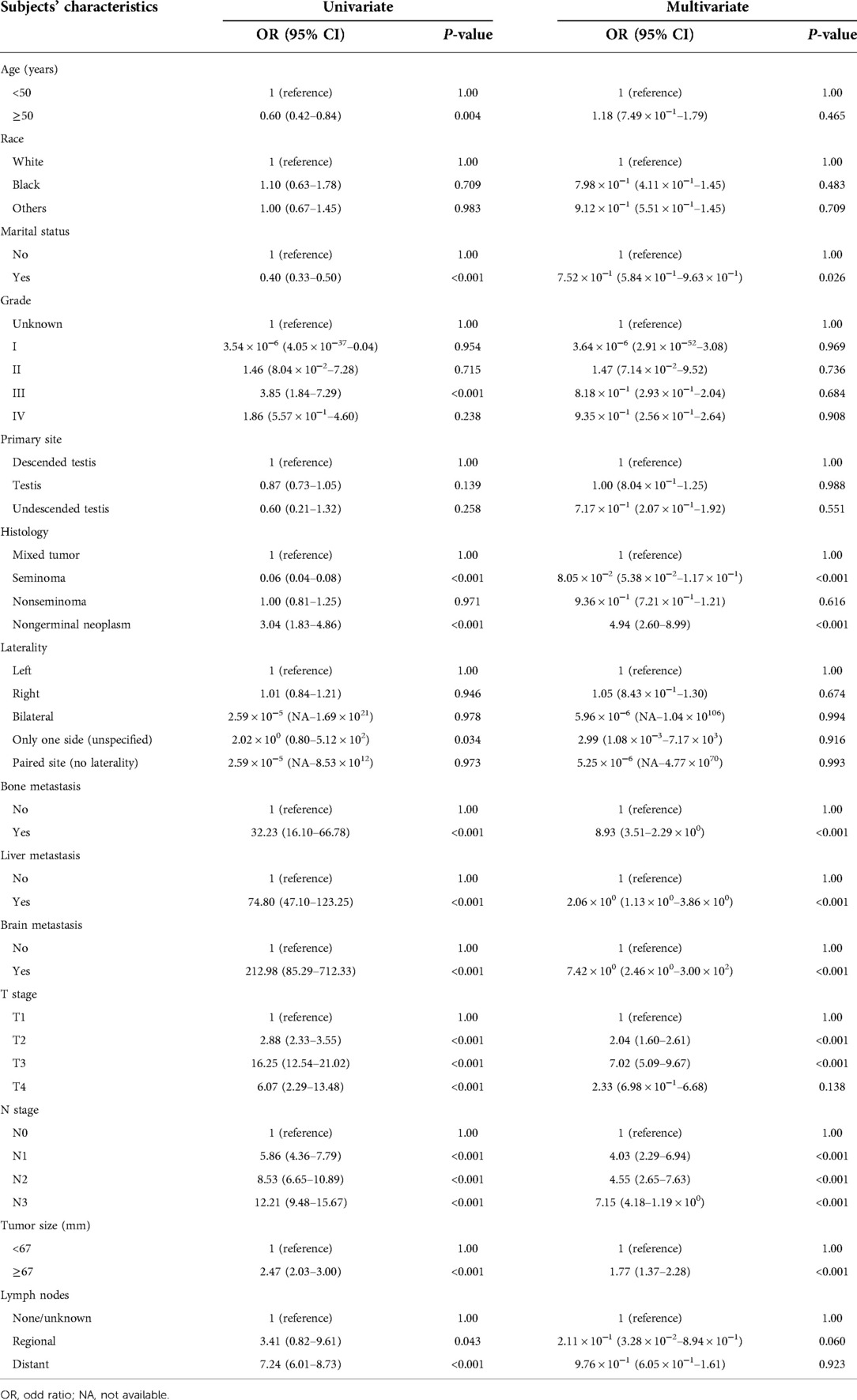
Table 3. Univariate and multivariate logistic regression for analyzing the associated factors for developing lung metastasis in testicular cancer patients.
Multivariable logistic regression analysis illustrated that marital status (OR = 7.52 × 10−1, 95% CI: 5.84 × 10−1–9.63 × 10−1, P = 0.026) is negatively associated with LM. In comparison, nongerminal neoplasm (OR = 4.94, 95% CI: 2.60–8.99, P < 0.001), bone metastases (OR = 8.93, 95% CI: 3.51–2.29 × 100, P < 0.001), liver metastases (OR = 2.06 × 100, 95% CI: 1.13 × 100–3.86 × 100, P < 0.001), brain metastasis (OR = 7.42 × 100, 95% CI: 2.46 × 100–3.00 × 102, P < 0.001), higher T stage (T2/T1: OR = 2.04, 95% CI: 1.60–2.61, P < 0.001; T3/T1: OR = 7.02, 95% CI: 5.09–9.67, P < 0.001), higher N stage (N1/N0: OR = 4.03, 95% CI: 2.29–6.94, P < 0.001; N2/N0: OR = 4.55, 95% CI: 2.65–7.63, P < 0.001; N3/N0: OR = 7.15, 95% CI: 4.18–1.19 × 100, P < 0.001), and larger tumor size (≥67 mm) (OR = 1.77, 95% CI: 1.37–2.28, P < 0.001) were all positively associated with LM (Table 3).
Figure 1C (nomogram) illustrates the diagnostic possibility based on the independent risk factors (marital status, tumor size, T stage, N stage, liver, brain and bone metastases, and histologic type). The patient's diagnostic possibility can be calculated by summing the scores for each selected variable, and the total scores projected on the bottom scale represents the diagnostic possibility for LM.
The logistic calibration showed the predicted probability of the nomogram was in line with ideal expectations (Figure 1D). Subsequently, the ROC curve was employed to analyze the validation of the logistic regression model (Figure 1E). The ROC curve showed that the area under the curve (AUC) is 91.0%.
Univariate Cox regression analysis for patients showed that older age (≥50 years) [hazard ratio (HR) = 1.91, 95% CI: 1.02–3.57, P = 0.044], tumor grade III (HR = 3.01, 95% CI: 1.22–7.40, P = 0.017), bone metastasis (HR = 2.25, 95% CI: 1.09–4.64, P = 0.028), brain metastasis (HR = 2.61, 95% CI: 1.50–4.52, P = 0.001), liver metastasis (HR = 2.87, 95% CI: 1.84–4.47, P = 3.33 × 10−6), and larger tumor size (≥67 mm) (HR = 1.53, 95% CI: 1.03–2.29, P = 0.037) contributed to the poor prognosis of patients' CSS, while not a single variable was negatively associated with CSS (Table 4).
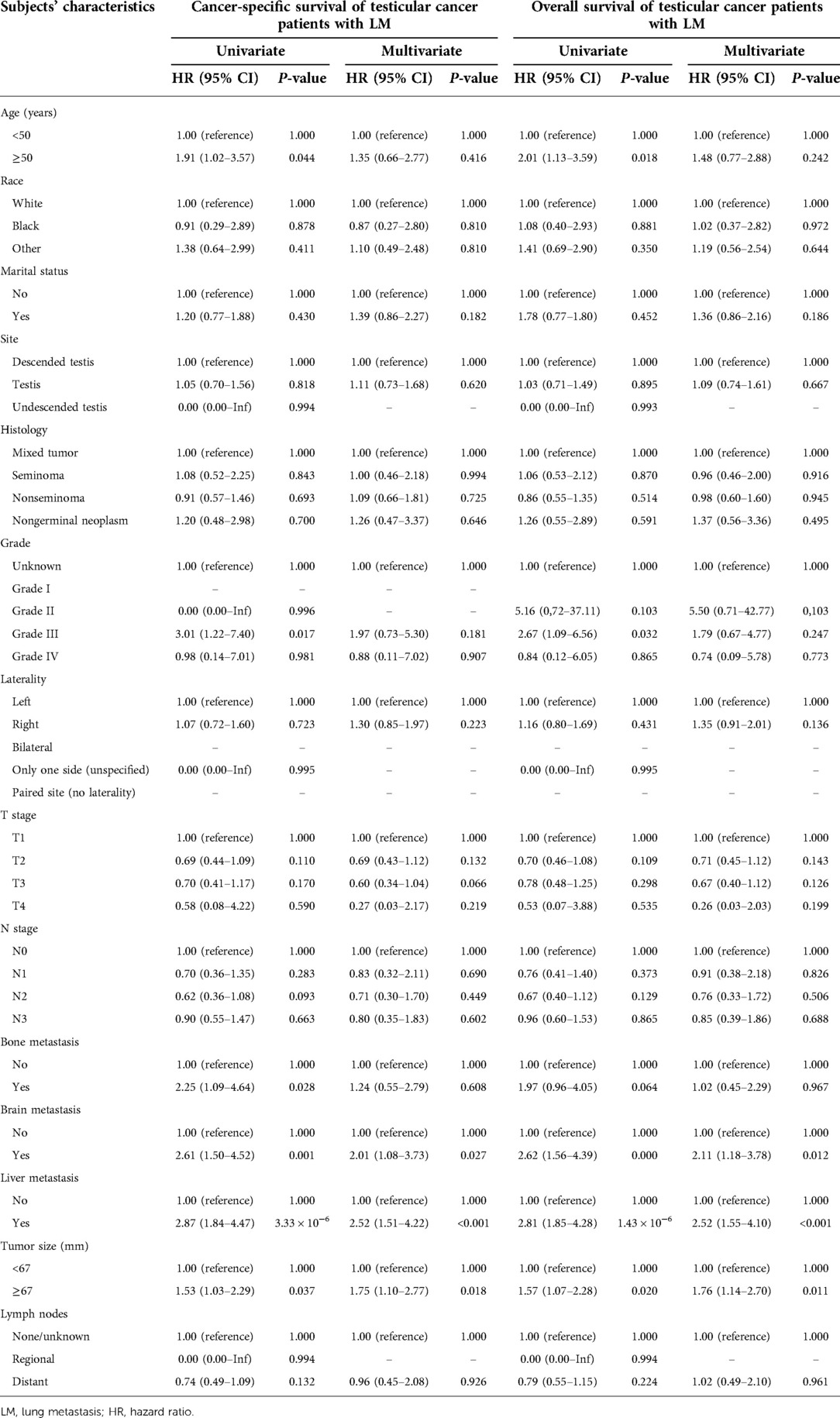
Table 4. Cox regression of univariate and multivariate analyses associated with cancer-specific survival and overall survival of testicular cancer patients with lung metastasis.
However, multivariate Cox regression analysis illustrated that brain metastasis (HR = 2.01, 95% CI: 1.56–4.39, P < 0.001), liver metastasis (HR = 2.81, 95% CI: 1.85–4.28, P = 1.43 × 10−6), and larger tumor size (≥67 mm) (HR = 1.57, 95% CI: 1.07–2.28, P = 0.020) were all positively associated with the risk of patients' CSS (Table 4).
Univariate Cox regression analysis for patients' OS indicated that older age (≥50) (HR = 2.01, 95% CI: 1.13–3.59, P = 0.018), tumor grade III (HR = 2.67, 95% CI: 1.09–6.56, P = 0.032), brain metastasis (HR = 2.62, 95% CI: 1.56–4.39, P < 0.001), liver metastasis (HR = 2.81, 95% CI: 1.85–4.28, P = 1.43 × 10−6), and larger tumor size (≥67 mm) (HR = 1.57, 95% CI: 1.07–2.28, P = 0.020) all positively contributed to patients' OS (Table 4).
However, multivariate Cox regression analysis represented that brain metastasis (HR = 2.11, 95% CI: 1.18–3.78, P = 0.012), liver metastasis (HR = 2.52, 95% CI: 1.55–4.10, P < 0.001), and larger tumor size (≥67 mm) (HR = 1.76, 95% CI: 1.14–2.70, P = 0.011) all were positively associated with the risk of patients' OS (Table 4).
In recent decades, TC has become the most prevalent solid cancer in men aged 14–44 years, and the international trends of incidence have been increasing (1, 15). Poor outcomes in TC are driven primarily by metastatic involvement (clinical stage III disease). Among patients with tumor metastasis (lung, lymph node, liver, and central nervous system), predictors of survival are multifactorial (6, 16). Given the development of multimodal strategies to manage lung metastatic TC, patients tend to exhibit improved clinical outcomes. However, the relative risk factors that removed confounding parameters on survival among TC patients with LM have not been systematically evaluated. Herein, we systematically assess the impact of the LM on survival using a large, nationally population-based cancer cohort. Clarifying the specific influence of organotropism on survival outcomes might improve current prognostic models for lung metastatic TC and provide insight into the heterogeneity of TC.
For lung metastasis TC, platinum-based chemotherapy is typically utilized as an adjuvant treatment after radical orchiectomy combined with multimodality treatments. Adjuvant chemotherapy with platinum/etoposide/bleomycin (BEP) is the commonly used chemotherapy regimen, which dramatically improves the outcome for patients with metastatic TC (17). However, chemotherapy for metastatic TC remains incurable and the poor prognosis now exceeds 20% (18). Therefore, radiotherapy or surgical management is developed for adjunctive therapy to chemotherapy. Studies revealed a promising improvement in OS of thoracic metastasectomy/pulmonary resection (19, 20). To achieve an optimal curative effect, postchemotherapy surgery retroperitoneal lymph node dissection is a critical procedure of metastatic TC management (21). PSM is a prevalent analytic method that may remove the effects of confounding biases due to measured baseline covariates when estimating the outcomes using observational data (14). PSM was employed in the analysis for CSS and OS to abbreviate the confounding biases of several variates and evaluate whether LM is an independent risk factor for survival probability in TC patients. After PSM, OS, and CSS between 493 groups were analyzed, and a higher survival probability was observed among patients without LM compared to those with LM. The application of the PSM method definitely increases the reliability and accuracy of our model.
For the first time, we utilized the largest real-world SEER database (2010–2015) to determine the related risk factors for TC patients with LM. Our research based on the logistic regression model revealed that nongerminal neoplasm, bone metastasis, liver metastasis, brain metastasis, higher T stage, higher N stage, and larger tumor size are independent risk factors positively related to LM development; marital status is a protective factor in TC patients with LM. Therefore, we suggest that the LM risk of TC patients should be carefully revalued in the contemporary cohort according to these risk factors. In this study, we also found that a higher T stage and higher N stage were associated with a greater possibility of LM, which commonly illustrates more aggressive biological behavior of cancer and worse physical status. In addition, previous studies demonstrated the importance of racial disparities in developing TC in young-onset patients (22, 23). However, race is not a risk factor for developing TC with LM in our study (P-value = 0.933).
A nomogram was constructed using our logistic regression model to demonstrate the diagnostic possibility based on the independent risk variates (marital status; tumor size; T stage; N stage; liver, brain, and bone metastases; and histologic type). The diagnostic possibility can be estimated by adding the score of each selected variate, and the total scores projected on the bottom scales presents the diagnostic possibility for LM. Nomograms allow medical practitioners to assess the patients' physical situation more accurately and intuitively to evaluate the personalized prediction for cancer prognosis. Subsequently, we applied the ROC curves to verify the predictive capacity of the prognostic model; the AUCs of the ROC were 0.910, indicating a favorable predictive performance. Mao et al. and Wu et al. reported nomograms for predicting survival in germ cell TC, which showed a moderate diagnostic value (0.7–0.9) (23).
The Cox regression model was utilized to determine the predictive factors for CSS and OS among TC patients with LM based on the SEER database. Brain and liver metastases and larger tumor size (≥67 mm) were observed to be positively associated with the risk of patients' CSS and OS in multivariate analysis. Notably, our study is the first to address the role of tumor size in lung metastatic TC patients' survival using a contemporary large-sample cohort. Interestingly, a previous study revealed that testicular tumor size is associated with relapse (24). Furthermore, our study is consistent with previous studies (5, 6) that patients with involvement of liver or brain metastatic sites presented worse outcomes than those with bone metastasis. The tendency of a tumor to metastasize to particular organ sites might reflect an interplay between the underlying biology of the tumor cells and a permissive host organ microenvironment (25–27).
At last, despite the advantages of our study, there exist some limitations. First, potential biases among children, adolescents, and young adults exist in our study, which may affect our results to some extent. Second, detailed information for diagnosing LM is unavailable in this SEER database, thus adding much uncertainty to the current amount of TC patients with LM. In addition, the lack of external validation due to the low number of cases in other cohorts is a limitation of our study. Given the retrospective nature, there are clinical parameters associated with the treatments that were not included or missed. Finally, subanalyses could be performed between young and older TC patients with LM to get a comprehensive pattern of TC.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding author/s.
The study was performed in accordance with the Declaration of Helsinki and the requirement for informed consent was exempted because of the retrospective nature of this study. The authors signed authorization forms and received permission from SEER to access and use the dataset.
JY and JG: Project development and data analysis. AG and JG: Data management, data analysis, and manuscript writing. All authors contributed to the article and approved the submitted version.
This work was supported by the National Science Foundation of Hunan Province (Grant No. 2020JJ5850 and Grant No. 2021JJ70149).
Jie Gu is supported by a scholarship from the China Scholarship Council Program (Grant No. 201906370030).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
NSGCT, nonseminomatous germ cell tumors; PSM, propensity score matching; TC, testicular cancer; LM, lung metastasis; CSS, cancer-specific survival; OS, overall survival; SEER, Surveillance, Epidemiology and End Results; ROC, receiver operating characteristic; BEP, platinum/etoposide/bleomycin.
1. Fode M, Jensen CF, Azawi N, Østergren PB. Perspectives on a global change in testicular cancer incidence. Eur Urol. (2019) 76(5):624–5. doi: 10.1016/j.eururo.2019.07.038
2. Gillessen S, Sauvé N, Collette L, Daugaard G, de Wit R, Albany C, et al. Predicting outcomes in men with metastatic nonseminomatous germ cell tumors (NSGCT): results from the IGCCCG update consortium. J Clin Oncol. (2021) 39(14):1563–74. doi: 10.1200/JCO.20.03296
3. Miller KD, Nogueira L, Mariotto AB, Rowland JH, Yabroff KR, Alfano CM, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. (2019) 69(5):363–85. doi: 10.3322/caac.21565
4. Rothermundt C, Thurneysen C, Cathomas R, Müller B, Mingrone W, Hirschi-Blickenstorfer A, et al. Baseline characteristics and patterns of care in testicular cancer patients: first data from the Swiss Austrian German Testicular Cancer Cohort Study (SAG TCCS). Swiss Med Wkly. (2018) 148:w14640. doi: 10.4414/smw.2018.14640
5. Xu P, Wang J, Abudurexiti M, Jin S, Wu J, Shen Y, et al. Prognosis of patients with testicular carcinoma is dependent on metastatic site. Front Oncol. (2020) 9:1495. doi: 10.3389/fonc.2019.01495
6. Patel HD, Singla N, Ghandour RA, Freifeld Y, Cheaib JG, Woldu SL, et al. Site of extranodal metastasis impacts survival in patients with testicular germ cell tumors. Cancer. (2019) 125(22):3947–52. doi: 10.1002/cncr.32427
7. Fankhauser CD, Sander S, Roth L, Beyer J, Hermanns T. Improved survival in metastatic germ-cell cancer. Ann Oncol. (2018) 29(2):347–51. doi: 10.1093/annonc/mdx741
8. Gilligan T, Lin DW, Aggarwal R, Chism D, Cost N, Derweesh IH, et al. Testicular cancer, version 2.2020. J Natl Compr Cancer Netw. (2019) 17(12):1529–54. doi: 10.6004/jnccn.2019.0058
9. Kier MG, Lauritsen J, Mortensen MS, Bandak M, Andersen KK, Hansen MK, et al. Prognostic factors and treatment results after bleomycin, etoposide, and cisplatin in germ cell cancer: a population-based study. Eur Urol. (2017) 71(2):290–8. doi: 10.1016/j.eururo.2016.09.015
10. Honecker F, Aparicio J, Berney D, Beyer J, Bokemeyer C, Cathomas R, et al. ESMO consensus conference on testicular germ cell cancer: diagnosis, treatment and follow-up. Ann Oncol. (2018) 29(8):1658–86. doi: 10.1093/annonc/mdy217
11. Bandak M, Lauritsen J, Johansen C, Kreiberg M, Skøtt JW, Agerbaek M, et al. Sexual function in a nationwide cohort of 2,260 survivors of testicular cancer after 17 years of followup. J Urol. (2018) 200(4):794–800. doi: 10.1016/j.juro.2018.04.077
12. Ljungman L, Eriksson LE, Flynn KE, Gorman JR, Ståhl O, Weinfurt K, et al. Sexual dysfunction and reproductive concerns in young men diagnosed with testicular cancer: an observational study. J Sex Med. (2019) 16(7):1049–59. doi: 10.1016/j.jsxm.2019.05.005
13. Pan Y, Lu L, Chen J, Zhong Y, Dai Z. Analysis of prognostic factors for survival in patients with primary spinal chordoma using the SEER registry from 1973 to 2014. J Orthop Surg Res. (2018) 13(1):76. doi: 10.1186/s13018-018-0784-3
14. Austin PC, Fine JP. Propensity-score matching with competing risks in survival analysis. Stat Med. (2019) 38(5):751–77. doi: 10.1002/sim.8008
15. Gurney JK, Florio AA, Znaor A, Ferlay J, Laversanne M, Sarfati D, et al. International trends in the incidence of testicular cancer: lessons from 35 years and 41 countries. Eur Urol. (2019) 76(5):615–23. doi: 10.1016/j.eururo.2019.07.002
16. Hassan O, Epstein JI. The clinical significance of a small component of choriocarcinoma in testicular mixed germ cell tumor (MGCT). Am J Surg Pathol. (2018) 42(8):1113–20. doi: 10.1097/PAS.0000000000001088
17. Hanna NH, Einhorn LH. Testicular cancer—discoveries and updates. N Engl J Med. (2014) 371(21):2005–16. doi: 10.1056/nejmra1407550
18. IGCCCG. International germ cell consensus classification: a prognostic factor-based staging system for metastatic germ cell cancers. International germ cell cancer collaborative group. J Clin Oncol. (1997) 15(2):594–603. doi: 10.1200/JCO.1997.15.2.594
19. Caso R, Jones GD, Tan KS, Bosl GJ, Funt SA, Sheinfeld J, et al. Thoracic metastasectomy in germ cell tumor patients treated with first-line versus salvage therapy. Anna Thorac Surg. (2021) 111(4):1141–9. doi: 10.1016/j.athoracsur.2020.06.072
20. Besse B, Grunenwald D, Fléchon A, Caty A, Chevreau C, Culine S, et al. Nonseminomatous germ cell tumors: assessing the need for postchemotherapy contralateral pulmonary resection in patients with ipsilateral complete necrosis. J Thorac Cardiovasc Surg. (2009) 137(2):448–52. doi: 10.1016/j.jtcvs.2008.09.032
21. Fléchon A, Bompas E, Biron P, Droz JP. Management of post-chemotherapy residual masses in advanced seminoma. J Urol. (2002) 168(5):1975–9. doi: 10.1097/01.ju.0000034401.89295.67
22. Wu J, Ye J, Wu W, Fang D, Wang K, Yang L, et al. Racial disparities in young-onset patients with colorectal, breast and testicular cancer. J Cancer. (2019) 10(22):5388–96. doi: 10.7150/jca.32435
23. Mao W, Wu J, Kong Q, Li J, Xu B, Chen M. Development and validation of prognostic nomogram for germ cell testicular cancer patients. Aging. (2020) 12(21):22095–111. doi: 10.18632/aging.104063
24. von der Maase H, Specht L, Jacobsen GK, Jakobsen A, Madsen EL, Pedersen M, et al. Surveillance following orchidectomy for stage I seminoma of the testis. Eur J Cancer. (1993) 29A(14):1931–4. doi: 10.1016/0959-8049(93)90446-M
25. Fidler IJ. The pathogenesis of cancer metastasis: the “seed and soil” hypothesis revisited. Nat Rev Cancer. (2003) 3(6):453–8. doi: 10.1038/nrc1098
26. Obenauf AC, Massagué J. Surviving at a distance: organ-specific metastasis. Trends Cancer. (2015) 1(1):76–91. doi: 10.1016/j.trecan.2015.07.009
Keywords: testicular cancer, lung metastasis, propensity score matching, nomogram, risk factors, survival analysis
Citation: Guo A, Gu J and Yang J (2022) Characteristics of lung metastasis in testicular cancer: A large-scale population analysis based on propensity score matching. Front. Surg. 9:959573. doi: 10.3389/fsurg.2022.959573
Received: 1 June 2022; Accepted: 30 September 2022;
Published: 4 November 2022.
Edited by:
Petros Sountoulides, Aristotle University of Thessaloniki, GreeceReviewed by:
Mierxiati Abudurexiti, Fudan University, China© 2022 Guo, Gu and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jie Gu amllZ3U5MjkyQDE2My5jb20= Jiayi Yang amlheWkyMzU1QGNzdS5lZHUuY24=
Specialty Section: This article was submitted to Genitourinary Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.