 Xiaodong Bai
Xiaodong Bai Zhenyu Liu
Zhenyu Liu Wentao Chen
Wentao Chen Baojun Wang
Baojun Wang- Department of Orthopedics, Beijing Friendship Hospital, Capital Medical University, Beijing, China
Objective: Both bone forearm fractures are common in children and rare in adults. The main surgical treatment is open reduction and internal fixation (ORIF) with plate, while the hybrid fixation of elastic-stable intramedullary nailing (ESIN) and the plate has been rarely reported before.
Case report: We report a case of a 29-year-old male patient with both bone forearm fractures. Temporarily closed reduction and plaster external fixation were performed in the emergency room, and the patient was admitted to the orthopedic trauma ward for surgery. The patient underwent open reduction and plate fixation of the ulna and closed reduction and ESIN fixation of the radius. The fractures healing was satisfactory and the internal fixation was removed 12 months postoperatively.
Conclusion: The hybrid fixation of ESIN and plate is an effective option for both bone forearm fractures in adults.
Introduction
Both bone forearm fractures are technically challenging for orthopedic surgeons (1). The peak incidence rate is mainly for children and adolescents (2, 3), while the incidence rate of adults is low. At present, elastic-stable intramedullary nailing (ESIN) is the main treatment option for both bone forearm fractures in children and adolescents with the advantages of minimal invasion and less damage to fracture blood supply (3). However, ESIN is not stable fixation and patients need to be assisted with plaster external fixation after the operation, resulting in low postoperative comfort and inability to exercise early (4). The main treatment for both bone forearm fractures in adults is open reduction and internal plate fixation (5). There are some problems associated with internal plate fixation, such as soft tissue injury, fracture nonunion, secondary fracture after plate removal and so on. Therefore, we used hybrid fixation in the treatment of both bone forearm fractures in an adult in our hospital. We report a 29-year-old patient who presented with both bone forearm fractures and underwent open reduction and internal plate fixation of the ulna and closed reduction and internal ESIN fixation of the radius.
Case presentation
A 29-year-old male patient fell and suffered trauma to his left forearm while riding a bicycle. He was unable to move his left arm immediately because of extreme pain and was sent to the emergency department. The patient had no family history of osteoporosis or pathological fractures. He had no history of consuming alcohol, smoking, or using drugs. He was 182 cm in height and 95 kg in weight (the body mass index was 28.7 kg/m2). Swelling and deformity of the left forearm were found, and the range of motion was restricted. Considering the possibility of both bone forearm fractures, the emergency doctor suggested the patient to take x-ray examinations (Figures 1A,B). X-ray examinations showed both bone forearm fractures on the left forearm. According to AO-OTA classification, the fracture classification of this patient was 2R2A2 and 2U2A2. Indications for surgery were clear and temporary plaster external fixation was performed in emergency. The characteristics of both bone forearm fractures were assessed by three-dimensional reconstructive CT scans (Figures 2A–D). We checked the nerves and artery vessels of the patient at different time points, including when the patient went to the emergency department, after admission, and before surgery, to confirm that the patient had no clear artery injury and clinical manifestations of nerve injury. The patient underwent open reduction and internal plate fixation of ulna and closed reduction and internal ESIN fixation of radius (Figures 3A,B), with no plaster fixation after the operation. The fracture healed 4 months later (Figures 3C,D). The internal fixation was removed 12 months postoperatively (Figures 3E,F). Disability of arm shoulder and hand (DASH) score was assessed at three-time points after surgery. According to the DASH score, 25 points in the 1st month, 13.7 points in the 4th month, and 6.7 points in the 12th-month. During the 12th month follow-up period, the range of supination and pronation was 88° and 85°, which was 92% and 90% of the contralateral rotation, respectively. (Figures 4A–D).
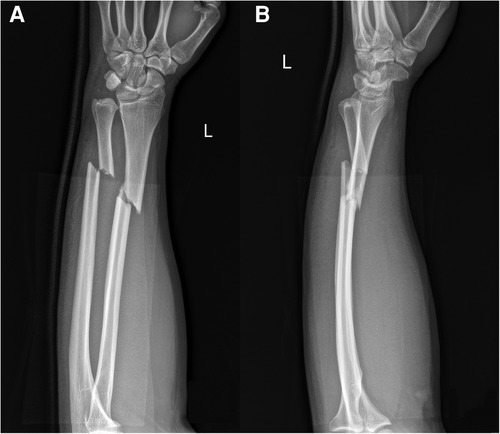
Figure 1. X-ray images (A,B) of the left forearm showed both bone forearm fractures with marrow edema.
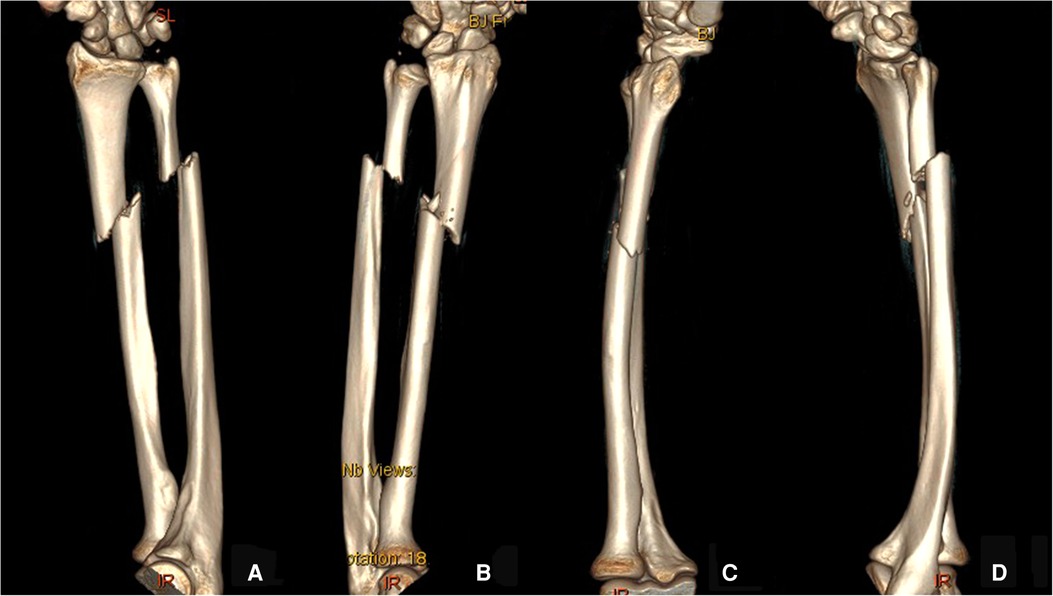
Figure 2. Preoperative three-dimensional reconstructive CT images (A–D) of the left forearm.
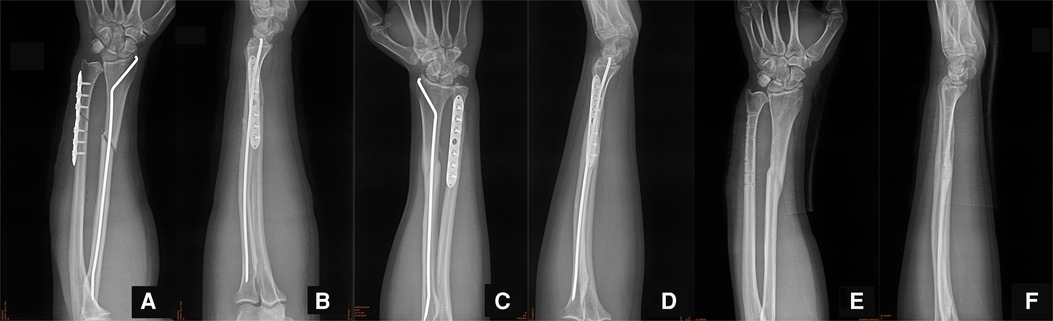
Figure 3. (A,B) Postoperative x-ray films of the left forearm. (C,D) X-ray films of the patient at 1 month after surgery. (E,F) X-ray films of the patient after removal of the internal fixation at 12 months after surgery.
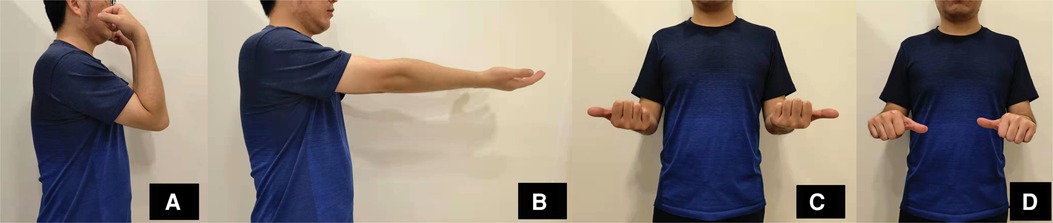
Figure 4. Follow-up after 12 months of surgery of the patient. (A) The flexion and (B) extension functions of the elbow joint. (C) The supination and (D) pronation of the forearm.
Discussion
The peak incidence rate of both bone forearm fractures is found in children and adolescents (6). The incidence rate of both bone forearm fractures in adults is relatively low. The low incidence rate of adult fractures leads to few epidemiological studies. The treatment of both bone forearm fractures in children is mainly conservative (7, 8). For cases with obvious fracture displacement, surgical treatment is usually used. Minimally invasive ESIN is the main surgical treatment, while open reduction and internal fixation (ORIF) is rarely used (9). Both bone forearm fractures in adult are usually caused by high energy trauma, and are usually displaced significantly, which often require surgical treatment. At present, the main surgical treatment is open reduction and internal plate fixation, and a few patients were treated with intramedullary nail fixation (10). Hybrid fixation of ESIN and plate has been attempted in the treatment of both bone forearm fractures in children and adolescents, and satisfactory results have been obtained (11, 12). For both bone forearm fractures in adults, hybrid fixation has been rarely reported before. In our case, we tried to apply the hybrid fixation of ESIN and plate to the surgical treatment of both bone forearm fractures in an adult and achieved satisfactory results.
The common mechanism of this fracture pertains to the axial load on the extended hand or the direct impact on the forearm (13). In addition, poor bone quality, caused by osteoporosis, is an important inducement (14). Patients with both bone forearm fractures often show obvious deformities in the appearance of their forearms. Special attention should be paid to whether there is a risk of an open fracture or potential open fracture during physical examination (15). At the same time, we should focus on the potential forearm nerve injury and evaluate the motor and sensory defects of the anterior interosseous nerve, posterior interosseous nerve, and ulnar nerve (16, 17). Meanwhile, an evaluation of blood supply should include the palpation of the radial artery and ulnar artery pulsation and an evaluation of the capillary filling of the fingers, and this should be evaluated several times at different time points. The consequences of the compartment syndrome of the forearm can be disastrous, so we should always be vigilant, even if its incidence is not high (18). In children and adolescents, both bone forearm fractures are often treated non-surgically, which usually helps to achieve good clinical results. However, there are a few successful cases or studies of conservative treatment of both bone forearm fractures in adults (19). The reduction and fixation should be carried out as soon as possible in the emergency department to create conditions for the surgery that follows. Thorough flushing and debridement should also be carried out, and antibiotics should be used to prevent infection in patients with severe open fractures. The wrist joint and elbow joint should be included in plaster fixation to effectively prevent the rotation of the forearm, and the forearm should remain in a neutral or mild supination position, subject to the patient's tolerance levels of pain and comfort levels.
The surgical treatment of both bone forearm fractures in adults includes open reduction and internal plate fixation and intramedullary nail. Open reduction and internal plate fixation are considered to be the gold standard of treatment. For oblique or transverse fractures, the compression plate can achieve the compression at the fracture site and promote primary fracture healing. In long oblique or spiral fractures, the inter block screw compression technology can achieve the satisfactory clinical curative effect through the neutralization plate. Some studies have shown that the combination of radial plate fixation and ulnar intramedullary nail fixation proved to be a better method, which had good rotation stability and restored the radial arch effectively, and achieved satisfactory clinical results (20). Intramedullary nail fixation can shorten operation time and reduce surgical scar (21). However, it should be noted that the intramedullary nails used in abovementioned studies were straight interlocking intramedullary nails, which could not restore the radial arch or the rotation function of the forearm when fixing the radius. The ESIN used in this case was with the prebending design of the radial arch. The radial arch could be effectively restored by three-point contact fixation, so as to recover the rotation stability of the forearm. During the operation, the placement of the radial ESIN could be completed through a surgical incision just about 2 cm in length. The reduction process completed by manual close reduction or percutaneous poking reduction with Kirschner wires was minimally invasive, compared with traditional open reduction. The forearm rotation axis practically intersected the center of the radial head and the base of the ulnar styloid process, at the center of the ulnar head cylinder (22). During forearm rotation, there was a statistically significant difference in ulnar variance between the pronation and neutral views and between the pronation and supination views; nonetheless, rotating the forearm from neutral to supination did not significantly change the measurement of ulnar variance (23). Anterior forearm rotation could be restored only when the axis was effectively stabilized, and ESIN fixation of the radius allowed local micro motion, which could promote callus growth and fracture healing. In addition, this hybrid fixation method could effectively reduce the risk of secondary fracture after internal fixation removal.
Conclusion
The hybrid fixation method may be an effective option for treating both bone forearm fractures in adults. For the surgical treatment of these fractures, orthopedic surgeons should follow the principle of minimally invasive and individualized treatment to achieve satisfactory clinical results.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
XB and BW performed the surgery, WC and ZL were involved in the collection of information on the patient, XB and WC reviewed the literature and contributed to manuscript drafting, and WC and BW were responsible for the revision of the manuscript. All authors have read and approved the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Morrison MJ, Speirs JN, Chicorelli AM, Garner M, Flynn JJM, Herman MJ. Intramedullary fixation of both bone forearm fractures in children and adolescents: healing correlates with development of the olecranon apophysis. J Pediatr Orthop. (2020) 40(3):e198–202. doi: 10.1097/BPO.0000000000001419
2. Ploegmakers J, Groen W, Haverlag R, Bulstra S. Predictors for losing reduction after reposition in conservatively treated both bone forearm fractures in 38 children. J Clin Orthop Trauma. (2020) 11(2):269–74. doi: 10.1016/j.jcot.2019.04.022
3. Upasani VV, Li Y. Elastic intramedullary nailing of pediatric both bone forearm fractures. JBJS Essent Surg Tech. (2020) 10(4):1–2. doi: 10.2106/JBJS.ST.19.00055
4. Poutoglidou F, Metaxiotis D, Kazas C, Alvanos D, Mpeletsiotis A. Flexible intramedullary nailing in the treatment of forearm fractures in children and adolescents: a systematic review. J Orthop. (2020) 20:125–30. doi: 10.1016/j.jor.2020.01.002
5. Lee SK, Kim YH, Kim SM, Choy WS. A comparative study of three different surgical methods for both-forearm-bone fractures in adults. Acta Orthop Belg. (2019) 85(3):305–16. PMID: 3167762631677626
6. Orgel M, Zimmer G, Graulich T, Gräff P, Macke C, Krettek C, et al. The impact of lifestyle on forearm fractures in children: a retrospective cohort analysis. Bone. (2021) 153:116149. doi: 10.1016/j.bone.2021.116149
7. Greig D, Silva M. Management of distal radius fractures in adolescent patients. J Pediatr Orthop. (2021) 41(Suppl 1):S1–5. doi: 10.1097/BPO.0000000000001778
8. Babazadeh S, Mason TG, Petterwood J, Taylor SW, Chapman N, Fettke GR. Extension casting for both bone forearm fractures in children. Acta Orthop Belg. (2017) 83(3):445–8. PMID: 3042364730423647
9. Liu Y, Zhang FY, Zhen YF, Zhu LQ, Guo ZX, Wang XD. Treatment choice of complete distal forearm fractures in 8 to 14 years old children. J Pediatr Orthop. (2021) 41(9):e763–7. doi: 10.1097/BPO.0000000000001934
10. Liu L, Zeng XT, Zhao JG. Regarding “minimally invasive plating versus either open reduction and plate fixation or intramedullary nailing of humeral shaft fractures: a systematic review and meta-analysis of randomized controlled trials”. J Shoulder Elbow Surg. (2017) 26(3):e78. doi: 10.1016/j.jse.2016.11.013
11. Cai L, Wang J, Du S, Zhu S, Wang T, Lu D, et al. Comparison of hybrid fixation to dual plating for both bone forearm fractures in older children. Am J Ther. (2016) 23(6):e1391–6. doi: 10.1097/MJT.0000000000000227
12. Zhu S, Yang D, Gong C, Chen C, Chen L. A novel hybrid fixation versus dual plating for both bone forearm fractures in older children: a prospective comparative study. Int J Surg. (2019) 70:19–24. doi: 10.1016/j.ijsu.2019.08.002
13. Schulte LM, Meals CG, Neviaser RJ. Management of adult diaphyseal both bone forearm fractures. J Am Acad Orthop Surg. (2014) 22(7):437–46. doi: 10.5435/JAAOS-22-07-437
14. Chalitsios CV, McKeever TM, Shaw DE. Incidence of osteoporosis and fragility fractures in asthma: a UK population-based matched cohort study. Eur Respir J. (2021) 57(1):1–10. doi: 10.1183/13993003.01251-2020
15. McHale C. CORR insights(R): union rates and reported range of motion are acceptable after open forearm fractures in military combatants. Clin Orthop Relat Res. (2019) 477(10):2329–31. doi: 10.1097/CORR.0000000000000750
16. Federer AE, Murphy JS, Calandruccio JH, Devito DP, Kozin SH, Slappey GS, et al. Ulnar nerve injury in pediatric midshaft forearm fractures: a case series. J Orthop Trauma. (2018) 32(9):e359–65. doi: 10.1097/BOT.0000000000001238
17. Schwartsmann CR, Ruschel PH, Huyer RG. Ulnar nerve paralysis after forearm bone fracture. Rev Bras Ortop. (2016) 51(4):475–7. doi: 10.1016/j.rbo.2015.09.011
18. Auld TS, Hwang JS, Stekas N, Gibson PD, Sirkin MS, Reilly MC, et al. The correlation between the OTA/AO classification system and compartment syndrome in both bone forearm fractures. J Orthop Trauma. (2017) 31(11):606–9. doi: 10.1097/BOT.0000000000001020
19. Hong DY, Berube ER, Strauch RJ. Non-operative management of adult both bone forearm fractures – a case report and literature review. J Orthop Case Rep. (2020) 10(7):53–6. doi: 10.13107/jocr.2020.v10.i07.1916
20. Zhang XF, Huang JW, Mao HX, Chen WB, Luo Y. Adult diaphyseal both bone forearm fractures: a clinical and biomechanical comparison of four different fixations. Orthop Traumatol Surg Res. (2016) 102(3):319–25. doi: 10.1016/j.otsr.2015.11.019
21. Blazevic D, Bencic I, Cuti T, Bakota B, Dobric I, Sabalic S, et al. Intramedullary nailing of adult forearm fractures: results and complications. Injury. (2021) 52(5):S44–8. doi: 10.1016/j.injury.2020.11.012
22. Soubeyrand M, Assabah B, Begin M, Laemmel E, Dos Santos A, Creze M. Pronation and supination of the hand: anatomy and biomechanics. Hand Surg Rehabil. (2017) 36(1):2–11. doi: 10.1016/j.hansur.2016.09.012
Keywords: forearm fractures, open reduction and internal fixation, elastic-stable intramedullary nailing, case report, hybrid fixation
Citation: Bai X, Liu Z, Chen W and Wang B (2022) Hybrid fixation with ESIN for both bone forearm fractures in adults: A case report and literature review. Front. Surg. 9:949727. doi: 10.3389/fsurg.2022.949727
Received: 21 May 2022; Accepted: 29 June 2022;
Published: 26 July 2022.
Edited by:
Qiling Yuan, Xi’an Jiaotong University, China© 2022 Bai, Liu, Chen and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wentao Chen Y2hlbndlbnRhb0BjY211LmVkdS5jbg== Baojun Wang ZG9jYmp3YW5nQDEyNi5jb20=
Specialty Section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery
Abbreviations DASH, disability of arm shoulder and hand; ESIN, elastic-stable intramedullary nailing; ORIF, open reduction and internal fixation.