
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 31 August 2022
Sec. Surgical Oncology
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.947218
This article is part of the Research TopicWomen in Surgical Oncology Vol II: 2022View all 7 articles
 Ailin Lan
Ailin Lan Yudi Jin
Yudi Jin Yu Wang
Yu Wang Nan Ding
Nan Ding Yihua Wang
Yihua Wang Yuran Dai
Yuran Dai Linshan JiangZhenrong Tang
Linshan JiangZhenrong Tang Yang Peng
Yang Peng Shengchun Liu*
Shengchun Liu*
Purpose: This study aimed to determine the effect of neoadjuvant chemotherapy (NAC) on circulating levels of reproductive hormones and evaluate the correlation of hormone changes after NAC with hormone receptors expression alterations and relapse-free survival (RFS) outcomes in breast cancer.
Methods: Information from 181 breast cancer patients who received NAC was retrospectively analyzed. For hormones parameters, the median and interquartile range (IQR) were provided at baseline and the end of NAC then was compared by Wilcoxon signed-rank test. Categorical variables were represented as numbers and percentages and were compared via two-sided chi-square and Fisher's tests. The RFS outcomes were compared between patients according to hormone changes using the log-rank test. Univariate and multivariate survival analyses with hazard ratios (HR) and 95% confidence intervals (95% CI) were carried out using Cox regression.
Results: Sex steroids including estradiol, progesterone, testosterone, and dehydroepiandrosterone sulfate (DHEAS) levels decreased significantly after NAC among both premenopausal and postmenopausal patients (all P < 0.05). Decreased estradiol levels were associated with reduced progesterone receptor (PR) expression (P = 0.030). In multivariate survival analysis, the non-decreased progesterone level was strongly associated with worse RFS (non-decreased vs. decreased, HR = 7.178, 95% CI 2.340–22.019, P = 0.001). Patients with decreased progesterone levels exhibited better 3-year RFS compared with those with non-decreased (87.6% vs. 58.3%, log-rank, P = 0.001).
Conclusion: Multiple reproductive hormone levels were influenced by NAC. The change in estradiol level had a positive connection with PR expression alteration. Furthermore, an inverse association between the change in progesterone level and RFS outcomes was found. These findings may provide a theoretical basis for pre-operative endocrine therapy combined with NAC in breast cancer patients.
Female breast cancer, as the leading cause of global cancer incidence in 2020, has been the fifth leading cause of cancer mortality worldwide, with an estimated 2.3 million new cases and 685,000 deaths (1). Neoadjuvant chemotherapy (NAC) as a standard of care for locally advanced breast cancer, is increasingly used for all breast cancer subtypes (2, 3), aiming to reduce tumor size before surgery. However, in young patients, chemotherapy-associated ovarian damage is a major limitation of NAC (4). Several mechanisms lead to chemotherapy-induced ovarian injury and reduction of the ovarian reserve (5, 6), directly affecting endogenous sex hormone concentrations such as estradiol, progesterone, follicle-stimulating hormone (FSH), and luteinizing hormone (LH) (7). Due to the benefit seen in some studies irrespective of the hormone receptors' status, a direct cytotoxic effect of chemotherapy on the ovary and an indirect endocrine effect have been postulated (8, 9).
It is well known that reproductive hormones play a critical role in breast carcinogenesis. Available evidence has demonstrated that endogenous reproductive hormones can sustain tumor growth and are associated with breast cancer risk (10). Our previous works (11) and other studies (12, 13) found an association between pre-treatment hormones and prognosis in patients who received NAC treatment. A recent study has described the association of chemotherapy-induced ovarian failure with the improved outcome regardless of hormone receptor status (14), highlighting the vital role of ovarian function suppression after neoadjuvant/adjuvant chemotherapy in inhibiting disease progression. Although this study reveals the potential role of reproductive hormones in cancer progression, it is not clear the exact effect of hormone changes after neoadjuvant/adjuvant chemotherapy on survival outcomes. To address this question, we evaluated serum reproductive hormone changes after NAC treatment in association with survival outcomes in breast cancer patients.
Most breast malignancies are hormone-dependent, and express hormone receptors such as estrogen receptor (ER) and progesterone receptor (PR). Many studies have suggested that the expression status of ER and PR may differ between the initial diagnostic core biopsies and excisional specimens after NAC (15, 16). The changes in these receptors reveal important clinical significance as clinicians need to make appropriate treatment adjustments according to the status of these biomarkers. However, the mechanisms mediating the changes in hormone receptor expression remain unknown. Although the effect of NAC on hormone receptor expression has been widely studied, the results were controversial.
In this context, we analyzed changes in estradiol, progesterone, testosterone, FSH, LH, dehydroepiandrosterone sulfate (DHEAS), sex hormone-binding globulin (SHBG) levels, and free androgen index (FAI) after NAC treatment in pre- and postmenopausal women diagnosed with invasive breast cancer. The correlation of hormone changes after NAC with hormone receptor expression alterations and relapse-free survival (RFS) outcomes have been investigated.
Details of the previous retrospective study on which this research is based have been posted (11). To investigate the relationship between changes in reproductive hormone levels after NAC treatment and survival outcomes, we included people with post-treatment hormone reports from previous study populations. This retrospective study included 181 female patients with breast cancer who were administered NAC between February 2013 and December 2019 at the First Affiliated Hospital of Chongqing Medical University (Chongqing, China). The inclusion criteria were as follows: (a) all enrolled breast cancer patients accepted NAC and subsequent surgery; (b) patients with serum reproductive hormones tests before NAC start and at the end of NAC; (c) patients received standard adjuvant therapy after surgery; (d) all included patients had complete clinical records. The exclusion criteria were as follows: (a) distant metastasis before NAC; (b) synchronous bilateral breast cancer; (c) administration of oral contraceptives or other hormones in the past 6 months; (d) pregnancy or lactation in the previous 6 months; (e) prior cancer diagnosis or serious organ disease; (f) endocrine therapy, radiotherapy or targeted therapy before NAC. Details related to the demographic and pathological characteristics were collected. Meanwhile, information on the serum reproductive hormones before initial NAC and after the last cycle of NAC, including estradiol, progesterone, testosterone, FSH, LH, DHEAS, FAI, and SHBG, was gathered. A total of 91 patients were enrolled in the follow-up group between February 2013 and December 2018, and each participant was followed from the baseline exam until death or February 1, 2021. The hospitalization information system was utilized to obtain the patients' in-hospital information, and outpatient information was obtained through the hospital outpatient system, face-to-face, or by telephone.
Samples were collected at baseline and the end of NAC. Concentrations of estradiol, progesterone, testosterone, FSH, LH, DHEAS, and SHBG were determined using an electrochemiluminescence method on an immunoassay analyzer (DxI 800 Immunoassay System; Beckman Coulter, Brea, CA, United States). FAI was calculated as FAI = (testosterone/SHBG) × 100.
All mammary gland malignant tumor specimens from core biopsies and surgical excisions were reviewed by two experienced pathologists. Immunohistochemistry (IHC) was utilized to measure ER, PR, the human epidermal growth factor receptor 2 (HER2) status, and the Ki67 index before and after NAC. The Ki67 was explained as the percentage of tumor cell nuclei between 400 and 500 cells.
Menopause was defined as no spontaneous menses over the past 1 year or no menses for <1 year with FSH and estradiol levels in the postmenopausal range or post bilateral oophorectomy. The ER and PR status were defined positive if >1% of cancer cells were stained, and the HER2 status was defined positive if >10% of the cancer cells showed a 3+ score by IHC or a >2.2-fold change compared to the expression of chromosome enumeration probe 17 (CEP17) in cancer cells via fluorescence in situ Hybridization (FISH) (17). The hormone receptors positive was explained as ER and/or PR positive. In accordance with the expression of hormone receptors and HER2 status, the included patients were classified according to the following four subtypes: luminal (ER+ and/or PR+, HER2−), luminal/HER2 (ER+ and/or PR+, HER2+), HER2 (ER− and PR−, HER2+), and triple-negative (ER− and PR−, HER2−). Pathological complete response (pCR) was defined as no remaining invasive tumor lesions in any excised breast tissue and lymph node (ypT0/Tis ypN0) (18). The RFS was explained as the time from the baseline exam to the time of the first event (invasive local recurrence, regional recurrence, distant recurrence, invasive contralateral breast cancer, secondary malignancy, or death for any reason).
The response of the tumor to NAC was evaluated by ultrasound and magnetic resonance imaging. Clinical response was assessed by making a comparison of the change of the primary site. The treatment response of NAC was assessed by imaging examinations based on the Response Evaluation Criteria in Solid Tumors (RECIST) guidelines version 1.1.
For the non-normally distributed continuous parameters, the median and interquartile range (IQR) were provided at baseline and the end of NAC, then were compared by Wilcoxon signed-rank test. Categorical variables were represented as numbers and percentages and were compared via two-sided chi-square and Fisher's tests. The RFS outcomes were compared between patients according to hormone changes using the log-rank test. Univariate and multivariate survival analyses with hazard ratios (HR) and 95% confidence intervals (95% CI) were carried out using Cox regression. In line with the widely used recommendations (19), variables with a P-value lower than 0.25 in univariate analysis were selected as independent variables and analyzed by multivariate Cox regression. Cases with missing values for any of the variables in the model were excluded from the analysis. The 95% CI was utilized to express ranges within which true parameter values were likely to lie. All statistical tests were 2-sided, and P values less than 0.05 were considered statistically significant. Data analyses were performed using SPSS (version 26.0) software (SPSS Inc., Chicago, IL, United States).
The clinicopathological characteristics of the study population at enrollment are summarized in Table 1. A total of 181 patients (premenopausal group: 101; postmenopausal group: 80) with invasive breast cancer were included in the study (Figure 1). The median age of the premenopausal and the postmenopausal patients was 44 years (Range, 21–57 years) and 56 years (Range, 45–69 years) respectively. Most the premenopausal patients with a BMI < 24 kg/m2 (71.2%), while most of postmenopausal with a BMI ≥ 24 kg/m2 (62.5%). Most of premenopausal and postmenopausal patients had cT2 (70.3% vs. 72.5%) or cN1/N2 (65.3% vs. 53.8%) disease. In the IHC or FISH of the excised specimens, most of premenopausal and postmenopausal patients were ER-positive (58.4% vs. 57.5%) and HER2-negative (56.4% vs. 61.3%) and had a Ki67 index >14% (81.2% vs. 80.0%). Most patients received 4 chemotherapy cycles (85.1% vs. 78.8% in the premenopausal and the postmenopausal groups respectively). The pCR rate of the premenopausal and the postmenopausal patients was 9.9% and 8.8% respectively.
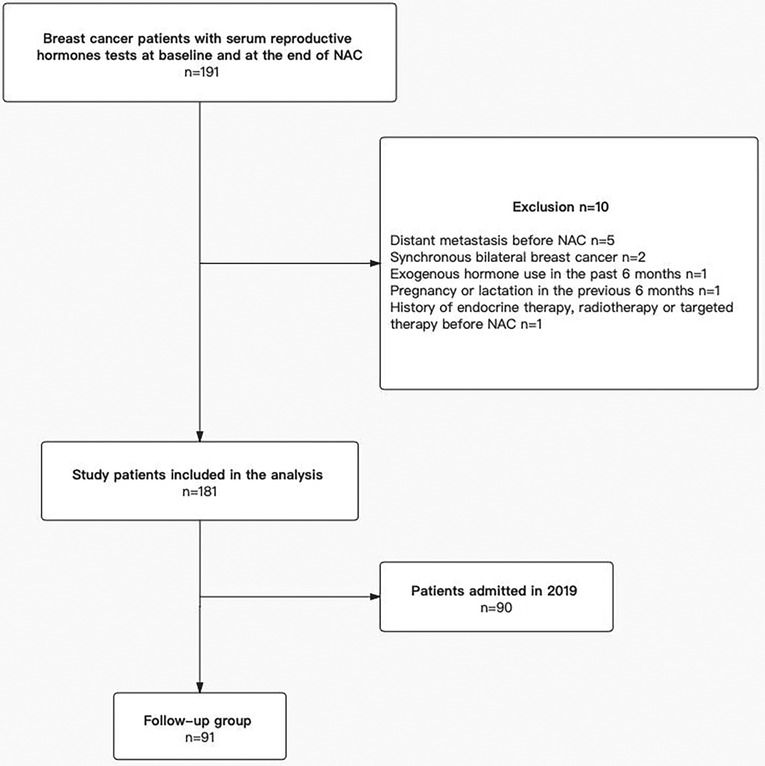
Figure 1. Flow chart of the patient selection. After exclusions, the final sample size was 181 patients, and a total of 91 patients were enrolled in the follow-up group. NAC, neoadjuvant chemotherapy.
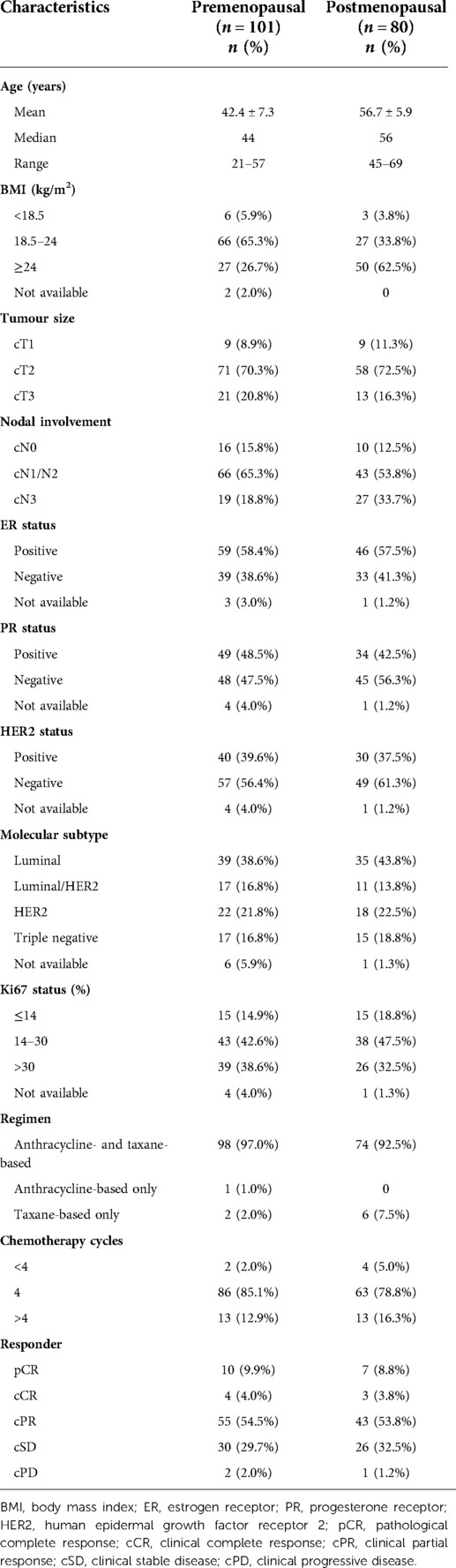
Table 1. Baseline clinicopathological characteristics of all patients.
Serum reproductive hormones changes after NAC in premenopausal and postmenopausal women with breast cancer as shown in Figure 2 and Table 2. In premenopausal women with breast cancer, a significant decrease in estradiol, progesterone, testosterone, DHEAS, and SHBG (all P < 0.001) levels was found. Meanwhile, we observed a significant increase in FSH and LH (both P < 0.001) levels. However, no significant changes were found in FAI (P > 0.05). In postmenopausal breast cancer patients, we found a significant reduction in progesterone, testosterone, DHEAS levels, and FAI (all P < 0.001). Concurrently, a slightly significant decrease in estradiol and FSH (both P < 0.05) levels was observed. No significant changes were found in LH and SHBG (both P > 0.05) levels.
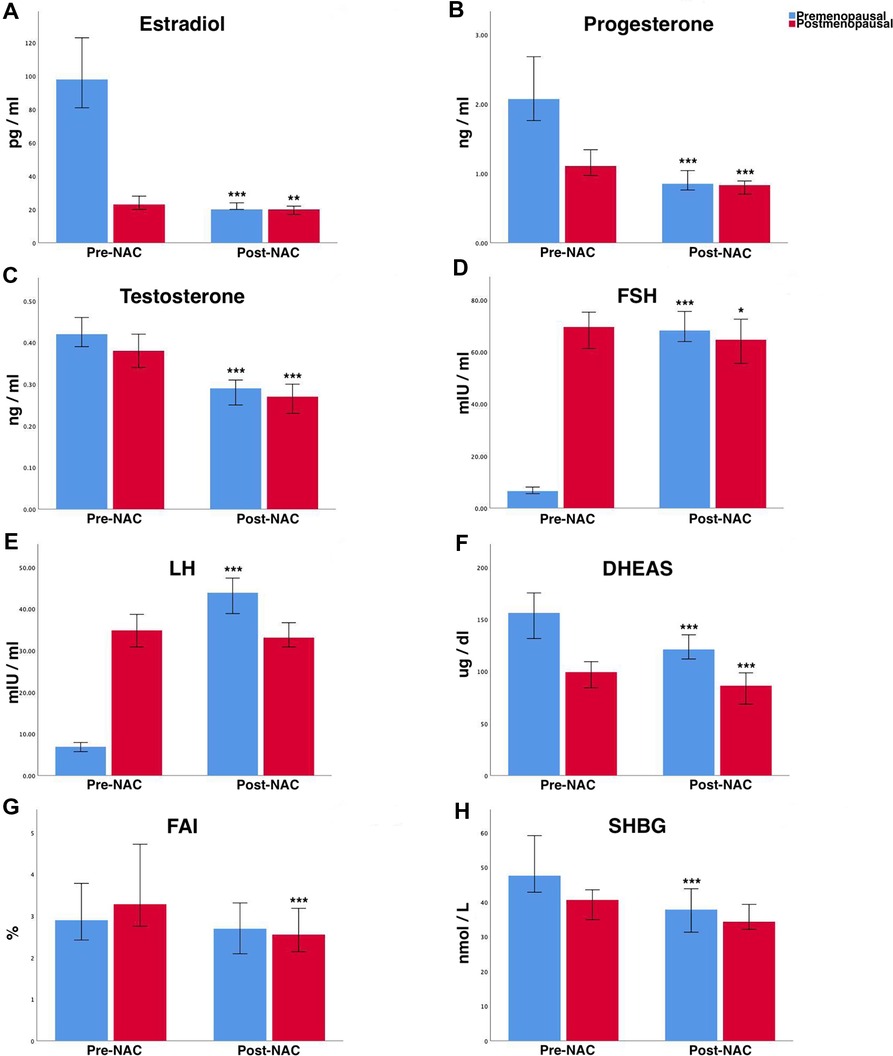
Figure 2. Changes of various serum reproductive hormones after NAC treatment in premenopausal and postmenopausal women with breast cancer. (A) Estradiol, (B) progesterone, (C) testosterone, (D) FSH, (E) LH, (F) DHEAS, (G) FAI, and (H) SHBG. Values are expressed as medians, and 95% CI are shown by whiskers. *P < 0.05; **P < 0.01; ***P < 0.001 (P-value by Wilcoxon signed-rank test). NAC, neoadjuvant chemotherapy; FSH, follicle stimulating hormone; LH, luteinizing hormone; DHEAS, dehydroepiandrosterone sulfate; FAI, free androgen index; SHBG, sex hormone-binding globulin; 95% CI, 95% confidence intervals.
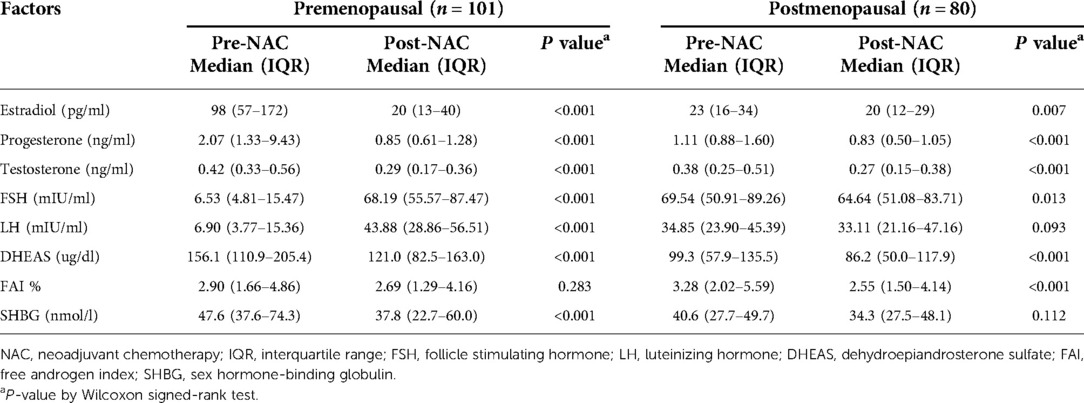
Table 2. Serum reproductive hormones changes after NAC treatment in premenopausal and postmenopausal women with breast cancer.
Table 3 summarized reproductive hormone changes with alterations in hormone receptors expression. Decreased estradiol levels associated with reduced PR expression were found (P = 0.030). Similar results were found among patients with hormone receptors positive (Table 4), decreased testosterone (P = 0.043), as well as estradiol (P = 0.042) levels, were associated with reduced PR expression. However, no significant connections between various reproductive hormone changes and alterations of ER expression were observed in all patients as well as patients with hormone receptors positive (all P > 0.05).
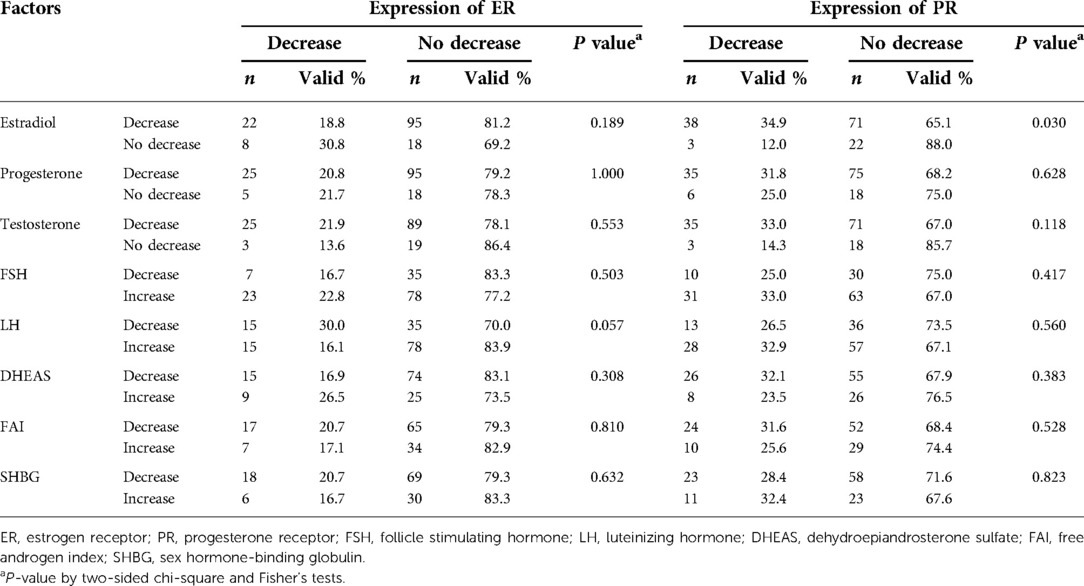
Table 3. Analysis of reproductive hormone changes associated with alterations of hormone receptors expression in all patients.
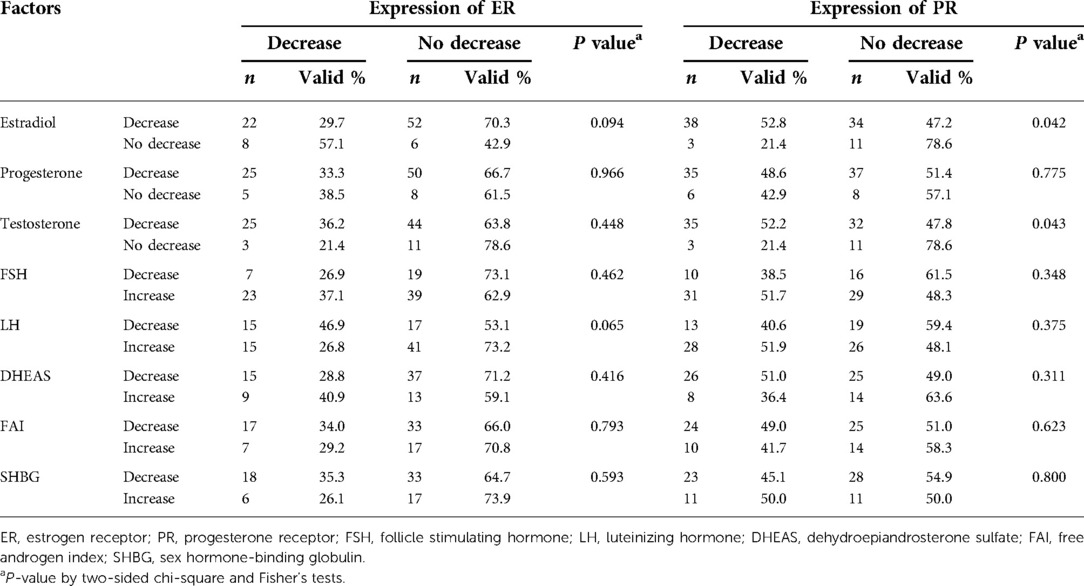
Table 4. Analysis of reproductive hormone changes associated with alterations of hormone receptors expression in patients with hormone receptors positive.
As of Feb. 1, 2021, we conducted follow-ups among a total of 91 patients (the loss rate of follow-up was 4.4%), and the clinicopathological characteristics of the study population at baseline were summarized in Table 5. The median follow-up time was 33 months (95%CI 31.3–34.7). Among the retrieved variations of reproductive hormone parameters of all patients in the follow-up subgroup, changes in estradiol (P = 0.022) and progesterone (P = 0.001) levels were associated with RFS outcomes (Table 6). These factors were then included in the Cox regression and the results were displayed in Table 7. On univariate analysis the following factors associated with worse RFS outcomes were found: younger age, premenopausal, lower BMI, larger clinical tumor size, hormone receptors negative, higher Ki67 index, decreased estradiol levels, and non-decreased progesterone levels (all P < 0.25). On multivariate analysis, the change of progesterone level (no decrease vs. decrease, HR = 7.178, 95% CI 2.340–22.019, P = 0.001) was an independent significant factor of RFS outcomes rather than the change of estradiol level. Comparison of the 3-year RFS between the decreased and the non-decreased progesterone levels groups were 87.6% and 58.3% respectively (log-rank, P = 0.001; Figure 3A). Similar trends were found among patients with hormone receptors positive, the survival analysis plotted as Figure 3B showed that patients with decreased progesterone levels exhibited better 3-year RFS compared with those with non-decreased (91.1% vs. 72.9%, log-rank, P = 0.015).
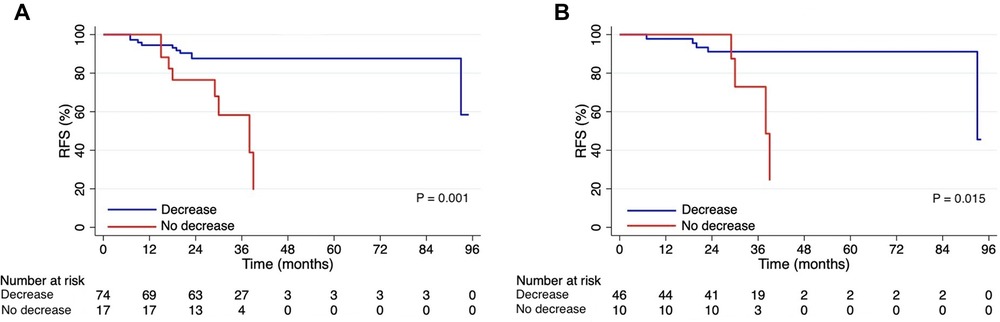
Figure 3. Kaplan-Meier curves display RFS by changes in progesterone levels. (A) Survival curves for the follow-up subgroup of 91 patients. (B) Survival curves for 56 patients with hormone receptors positive. RFS, relapse-free survival.
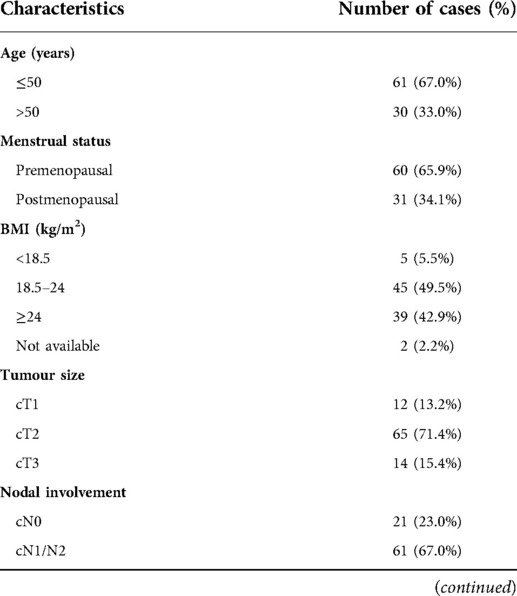
Table 5. Baseline clinicopathological characteristics of 91 patients in the follow-up subgroup.
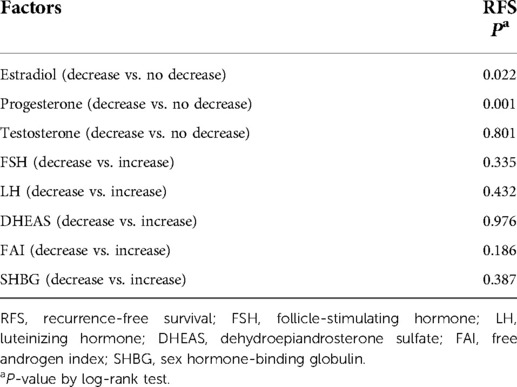
Table 6. Kaplan–meier analysis of RFS by reproductive hormones changes.
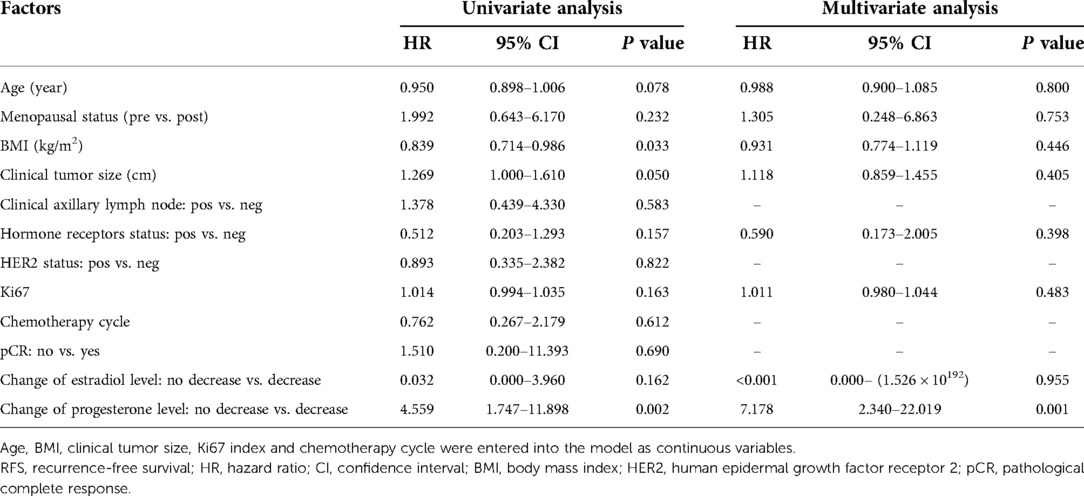
Table 7. Univariate and multivariate analysis for RFS in the follow-up subgroup of 91 patients.
The main finding of this study was that reproductive hormone levels were influenced by NAC treatment, having connections with hormone receptor expression alterations and RFS outcomes in women diagnosed with invasive breast cancer. To our knowledge, this is the first study to explore the correlation of serum reproductive hormone changes after NAC with hormone receptor expression alterations and survival outcomes in breast cancer. Though our previous study revealed that pre-treatment hormones have a predicted effect (11), the dynamics of reproductive hormones may be a better predictor of survival than pre-treatment hormones.
The changes in estradiol, FSH, and LH levels in premenopausal patients observed in our study are consistent with published studies reporting that the majority of young women receiving (neo)adjuvant chemotherapy rendered postmenopausal after chemotherapy (8, 14), although these studies focus on menstrual status or ovarian function rather than hormones. In postmenopausal patients, a slightly significant decrease in FSH levels and no significant changes in LH levels were observed in our study, as previously reported (7). In addition, we found that sex steroids including estradiol, progesterone, testosterone, and DHEAS levels decreased significantly after NAC among both premenopausal and postmenopausal patients. These changes in the hormonal profile of pre- and postmenopausal patients may be due to the ovarian and adrenal dysfunction produced by the chemotherapy treatment.
In our study, nearly all patients received anthracycline–taxane combination chemotherapy. The impact of chemotherapeutic agents on reproductive hormones is different due to the mechanism of action of anticancer drugs being diverse. The mechanism by which NAC, particularly alkylating agents, which show the highest level of gonadotoxicity, contributes to ovarian damage is unclear, but it could be related to apoptotic oocyte death in primordial follicles entering the differentiation stage, which is especially susceptible to chemotherapeutic drugs effects (20, 21). Thus, cyclophosphamide can cause ovarian function impairment and leads to a decrease in sex steroids. Doxorubicin can destroy the endothelium of blood vessels and lead to a reduction in ovarian blood flow. Taxane can disrupt normal polymerization/depolymerization, causing cell cycle arrest and apoptosis (22). The previous meta-analysis indicated that the incidence of chemotherapy-induced amenorrhea was lower in anthracycline-based compared to anthracycline–taxane combination chemotherapy (23), showing that the combination of anthracycline and taxane has a greater effect on hormones.
Even if there is no report that a cytotoxic chemotherapeutic agent induces adrenal dysfunction, the not rare incidence of adrenal insufficiency in advanced gastric cancer patients who received chemotherapy was reported in a prospective study (24).
The two major sites of de novo steroid hormone biosynthesis in a woman are the ovaries and adrenals, and both these organs produce active estrogens, progestogens, and androgens (25). The major sex steroids produced by the ovaries are estrogens and progestogens, while the adrenals are androgens. The loss of adrenal function in the presence of intact ovaries has been shown to result in a > 90% loss of androgen production (26), highlighting the vital role of adrenals in androgen synthesis. It is well known that the production of estrogen by the ovary decreases drastically after menopause. Although it was initially thought that estrogen production ceased completely, it is now clear that postmenopausal ovaries continue to produce estrogen, albeit at significantly reduced levels (27). Other sites of estrogen synthesis become increasingly important in the postmenopausal state. Extragonadal sites such as adrenals become the main source of sex steroids during menopause (25). Thus, chemotherapy-induced ovarian and adrenal dysfunction may result in a decrease in estrogens, progestogens, and androgens in both pre- and postmenopausal patients.
Alterations of hormone receptor status in breast cancer after NAC treatment have been described in published studies (15, 16). Whether these changes are due to NAC treatment, hormones, tumor heterogeneity, sampling or technical issues need to be further clarified. We observed that decreased estradiol levels were associated with reduced PR expression, which was supported by several studies that indicated that PR decrease was more obvious in premenopausal patients (28, 29). Furthermore, PR was also found to have the highest conversion rates in NAC and adjuvant chemotherapy (30, 31). Previous studies showed that pre-operative endocrine therapy, pre-operative chemoendocrine therapy, and NAC induced a significant decrease in the expression of PR in breast cancer patients with hormone receptors positive (32, 33), highlighting the potential role of sex hormones in PR expression, which is consistent with our finding that decreased estradiol and testosterone levels were associated with reduced PR expression in patients with hormone receptors positive. Possible mechanisms involve the survival mechanism of malignant cells by changing the specific molecular pathways following the changes in hormone levels resulting in resistance to a specific treatment (28).
PR plays an important role in normal breast development and has been linked to breast cancer. Moreover, PR has generally been considered solely as an indicator of ER functionality and responsiveness to endocrine therapy (34). The expression pattern of the hormone receptors such as ER and PR has been used clinically to guide therapy and predict survival outcomes. However, discordant results have been reported regarding whether a changed receptor status will affect the predictive or prognostic parameters. Although some studies suggested that PR loss may reflect a relatively poor response to chemotherapy and may be associated with a poor prognosis (35, 36), no consensus has been drawn on this topic.
Progesterone and its receptor are increasingly gaining attention for their emerging role as critical regulators of breast malignancies. Their complex and tightly regulated actions have been challenging to determine. The role of endogenous progesterone in breast malignancy pathogenesis remains largely unexplored to date, and the proliferative/antiproliferative effects of progestins continue to be debated. Inconsistent evidence showed that progesterone can facilitate, restrain, or have no action on the invasion and migration of breast cancer cells (25).
Epidemiologic studies evaluating circulating levels of progesterone remain limited. Previous clinical studies reporting increased breast cancer risk with the use of contraceptives or menopausal hormone therapy have primarily evaluated exogenous synthetic progestogen (progestin) use, rather than endogenous progesterone (37). The potential role of endogenous progesterone in breast cancer cannot be inferred from these studies.
In what appears to be the only prior study of progesterone and survival outcomes published to date, pre-operative progesterone treatment resulted in greater than 10% absolute improvement in 5-year disease-free survival among node-positive breast cancer patients independent of their PR status (38). In contrast to this study, patients with decreased progesterone levels exhibited better 3-year RFS compared with those with non-decreased in our study. The explanation could be that non-decreased progesterone concentrations after NAC may reflect a relatively poor response to chemotherapy or resistance to later endocrine therapy. These inconsistent results could be mainly attributable to different sources of progesterone, considering that the previous study evaluated progesterone in an exogenous state while our study evaluated the circulating endogenous progesterone levels in a neoadjuvant setting. In addition, relative concentrations of progesterone metabolites may be the potential factors contributing to these discordant results. With the proliferative/antiproliferative effects of different progesterone metabolites in breast cancer having been gradually explored, the importance of progesterone metabolites in breast cancer is highlighted. However, much of the difficulty lies in defining which progesterone and its metabolites exert their effects on different pathological types of breast cancer. Limited available in vivo evidence suggested the effects of progesterone metabolites on breast physiology and carcinogenesis (39). A previous study reported that the cancer-promoting effects of administered progesterone were in fact due to the locally produced progesterone metabolite, but not progesterone itself (40).
Progesterone also works in hormone receptor-negative breast malignancies. A recent study reported that progesterone accelerated cell growth in vitro and tumorigenesis in vivo in a triple-negative model (41), which supported our view.
The present study undoubtedly has limitations. A single blood sample may provide an inexact measure of long-term average hormone levels; however, a separate reproducibility study manifested moderate to high stability over 2 years in average intraclass correlation coefficients of all hormones measured (39). Serum reproductive hormone levels wave motion during the menstrual cycle in premenopausal women. In addition, data on postoperative adjuvant therapy was not available, but all treatment options are recommended in accordance with current guidelines. All included HER2-positive patients did not receive pre-operative anti-HER2 targeted therapy due to financial and medical insurance reasons, hence the pCR rates of this cohort were lower than those reported in other literature (2). The major limitation of the study is that it was a retrospective study in one single center, with a not large sample size and a shorter follow-up time (most patients were included between January 2017 and December 2019); thus, it was also partly limited by selection bias. Because of the above limitations, we only conducted a preliminary correlation study between RFS outcomes as well as alterations of hormone receptors expression and reproductive hormones changes after NAC. Therefore, it is necessary to perform long-term clinical application of a large sample to make a more objective analysis and support our results.
In conclusion, our results showed that sex steroids (including estradiol, progesterone, testosterone, and DHEAS) are affected by NAC and their levels are significantly reduced among both premenopausal and postmenopausal patients. Decreased estradiol levels were associated with reduced PR expression. More importantly, patients with decreased progesterone levels after NAC exhibited better 3-year RFS. Reproductive hormone levels should be part of the routine workup for patients with newly diagnosed breast cancer.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by The ethics committee of First Affiliated Hospital of Chongqing Medical University. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
SL and AL are the guarantors of integrity of the entire study; AL, YJ, YW and SL designed the study concepts/study design; AL, ND, YW, YHW, YJ, ZT, YP, YD, and LJ participated in the data acquisition or data analysis/interpretation; AL, YJ, YW and SL participated in the drafting or revising of manuscript for important intellectual content; all authors have approved the final version of submitted manuscript; AL and SL agreed to ensure any questions related to the work are appropriately resolved; AL and YW performed literature research; AL performed statistical analysis; AL participated in the manuscript editing. All authors contributed to the article and approved the submitted version.
This work was funded by the National Natural Science Foundation of China (No. 81772979 and 81472658). The funding source had no role in the study design, data collection, data analysis, data interpretation, or the writing of the report.
The authors thank Yinan Wu for her contribution to the data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: gLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71(3):209–49. doi: 10.3322/caac.21660
2. van Nes JG, Putter H, Julien JP, Tubiana-Hulin M, van de Vijver M, Bogaerts J, et al. Preoperative chemotherapy is safe in early breast cancer, even after 10 years of follow-up; clinical and translational results from the EORTC trial 10902. Breast Cancer Res Treat. (2009) 115(1):101–13. doi: 10.1007/s10549-008-0050-1
3. Chaudhary LN, Wilkinson KH, Kong A. Triple-Negative breast cancer: who should receive neoadjuvant chemotherapy? Surg Oncol Clin N Am. (2018) 27(1):141–53. doi: 10.1016/j.soc.2017.08.004
4. Lambertini M, Moore HCF, Leonard RCF, Loibl S, Munster P, Bruzzone M, et al. Gonadotropin-Releasing hormone agonists during chemotherapy for preservation of ovarian function and fertility in premenopausal patients with early breast cancer: a systematic review and meta-analysis of individual patient-level data. J Clin Oncol. (2018) 36(19):1981–90. doi: 10.1200/JCO.2018.78.0858
5. Rosendahl M, Andersen CY, la Cour Freiesleben N, Juul A, Løssl K, Andersen AN. Dynamics and mechanisms of chemotherapy-induced ovarian follicular depletion in women of fertile age. Fertil Steril. (2010) 94(1):156–66. doi: 10.1016/j.fertnstert.2009.02.043
6. Lambertini M, Peccatori FA, Demeestere I, Amant F, Wyns C, Stukenborg JB, et al. Fertility preservation and post-treatment pregnancies in post-pubertal cancer patients: eSMO clinical practice guidelines(†). Ann Oncol. (2020) 31(12):1664–78. doi: 10.1016/j.annonc.2020.09.006
7. Ramírez-Expósito MJ, Martínez-Martos JM, Dueñas-Rodríguez B, Navarro-Cecilia J, Carrera-González MP. Neoadjuvant chemotherapy modifies serum pyrrolidone carboxypeptidase specific activity in women with breast cancer and influences circulating levels of GnRH and gonadotropins. Breast Cancer Res Treat. (2020) 182(3):751–60. doi: 10.1007/s10549-020-05723-1
8. Walshe JM, Denduluri N, Swain SM. Amenorrhea in premenopausal women after adjuvant chemotherapy for breast cancer. J Clin Oncol. (2006) 24(36):5769–79. doi: 10.1200/JCO.2006.07.2793
9. Colleoni M, Gelber S, Goldhirsch A, Aebi S, Castiglione-Gertsch M, Price KN, et al. Tamoxifen after adjuvant chemotherapy for premenopausal women with lymph node-positive breast cancer: international breast cancer study group trial 13–93. J Clin Oncol. (2006) 24(9):1332–41. doi: 10.1200/JCO.2005.03.0783
10. Hankinson SE, Eliassen AH. Endogenous estrogen, testosterone and progesterone levels in relation to breast cancer risk. J Steroid Biochem Mol Biol. (2007) 106(1–5):24–30. doi: 10.1016/j.jsbmb.2007.05.012
11. Lan A, Jin Y, Wang Y, Wang Y, Ding N, Dai Y, et al. Pre-treatment circulating reproductive hormones levels predict pathological and survival outcomes in breast cancer submitted to neoadjuvant chemotherapy. Int J Clin Oncol. (2022) 27(5):899–910. doi: 10.1007/s10147-022-02141-9
12. Kensler KH, Eliassen AH, Rosner BA, Hankinson SE, Brown M, Tamimi RM. Pre-diagnostic sex hormone levels and survival among breast cancer patients. Breast Cancer Res Treat. (2019) 174(3):749–58. doi: 10.1007/s10549-018-05121-8
13. Duggan C, Stanczyk F, Campbell K, Neuhouser ML, Baumgartner RN, Baumgartner KB, et al. Associations of sex steroid hormones with mortality in women with breast cancer. Breast Cancer Res Treat. (2016) 155(3):559–67. doi: 10.1007/s10549-016-3704-4
14. Furlanetto J, Marmé F, Seiler S, Thode C, Untch M, Schmatloch S, et al. Chemotherapy-induced ovarian failure in young women with early breast cancer: prospective analysis of four randomised neoadjuvant/adjuvant breast cancer trials. Eur J Cancer. (2021) 152:193–203. doi: 10.1016/j.ejca.2021.04.038
15. Zhou X, Zhang J, Yun H, Shi R, Wang Y, Wang W, et al. Alterations of biomarker profiles after neoadjuvant chemotherapy in breast cancer: tumor heterogeneity should be taken into consideration. Oncotarget. (2015) 6(34):36894–902. doi: 10.18632/oncotarget.5050
16. Zhang N, Moran MS, Huo Q, Haffty BG, Yang Q. The hormonal receptor status in breast cancer can be altered by neoadjuvant chemotherapy: a meta-analysis. Cancer Invest. (2011) 29(9):594–8. doi: 10.3109/07357907.2011.621913
17. Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thürlimann B, Senn HJ. Strategies for subtypes--dealing with the diversity of breast cancer: highlights of the st. Gallen international expert consensus on the primary therapy of early breast cancer 2011. Ann Oncol. (2011) 22(8):1736–47. doi: 10.1093/annonc/mdr304
18. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. (2014) 384(9938):164–72. doi: 10.1016/S0140-6736(13)62422-8
19. Hosmer DW, Lemeshow S. Model-Building strategies and methods for logistic regression. In: Shewhart WA, Wilks SS, editors. Applied logistic regression, 2nd ed. New York: John Wiley & Sons (2000). p. 91–142.
20. Blumenfeld Z. Fertility preservation by endocrine suppression of ovarian function using gonadotropin-releasing hormone agonists: the End of the controversy? J Clin Oncol. (2018) 36(19):1895–7. doi: 10.1200/JCO.2018.78.9347
21. Blumenfeld Z. Investigational and experimental GnRH analogs and associated neurotransmitters. Expert Opin Investig Drugs. (2017) 26(6):661–7. doi: 10.1080/13543784.2017.1323869
22. Ben-Aharon I, Shalgi R. What lies behind chemotherapy-induced ovarian toxicity? Reproduction. (2012) 144(2):153–63. doi: 10.1530/REP-12-0121
23. Zhao J, Liu J, Chen K, Li S, Wang Y, Yang Y, et al. What lies behind chemotherapy-induced amenorrhea for breast cancer patients: a meta-analysis. Breast Cancer Res Treat. (2014) 145(1):113–28. doi: 10.1007/s10549-014-2914-x
24. Kim HR, Kim JH, Rhee Y, Lee H, Song SE, Kim C, et al. Assessment of adrenal function and health-related quality of life in advanced gastric cancer patients who received first-line chemotherapy. Oncology. (2016) 90(5):248–54. doi: 10.1159/000445010
25. Africander D, Storbeck KH. Steroid metabolism in breast cancer: where are we and what are we missing? Mol Cell Endocrinol. (2018) 466:86–97. doi: 10.1016/j.mce.2017.05.016
26. Arlt W, Callies F, van Vlijmen JC, Koehler I, Reincke M, Bidlingmaier M, et al. Dehydroepiandrosterone replacement in women with adrenal insufficiency. N Engl J Med. (1999) 341(14):1013–20. doi: 10.1056/NEJM199909303411401
27. Fogle RH, Stanczyk FZ, Zhang X, Paulson RJ. Ovarian androgen production in postmenopausal women. J Clin Endocrinol Metab. (2007) 92(8):3040–3. doi: 10.1210/jc.2007-0581
28. Xie L, Li X, Wang Q, Zhou J, Shen J, Luo L, et al. Effects of core needle biopsy and subsequent neoadjuvant chemotherapy on molecular alterations and outcome in breast cancer. Onco Targets Ther. (2018) 11:677–85. doi: 10.2147/OTT.S145715
29. Enomoto Y, Morimoto T, Nishimukai A, Higuchi T, Yanai A, Miyagawa Y, et al. Impact of biomarker changes during neoadjuvant chemotherapy for clinical response in patients with residual breast cancers. Int J Clin Oncol. (2016) 21(2):254–61. doi: 10.1007/s10147-015-0897-1
30. Zhao W, Sun L, Dong G, Wang X, Jia Y, Tong Z. Receptor conversion impacts outcomes of different molecular subtypes of primary breast cancer. Ther Adv Med Oncol. (2021) 13:17588359211012982. doi: 10.1177/17588359211012982.
31. Mohan S, Walcott-Sapp S, Lee M, Srour M, Kim S, Amersi F, et al. Alterations in breast cancer biomarkers following neoadjuvant therapy. Ann Surg Oncol. (2021) 28(11):5907–17. doi: 10.1245/s10434-021-09814-1
32. Shimizu D, Ishikawa T, Tanabe M, Sasaki T, Ichikawa Y, Chishima T, et al. Preoperative endocrine therapy with goserelin acetate and tamoxifen in hormone receptor-positive premenopausal breast cancer patients. Breast Cancer. (2014) 21(5):557–62. doi: 10.1007/s12282-012-0429-z
33. Torrisi R, Bagnardi V, Rotmensz N, Scarano E, Iorfida M, Veronesi P, et al. Letrozole plus GnRH analogue as preoperative and adjuvant therapy in premenopausal women with ER positive locally advanced breast cancer. Breast Cancer Res Treat. (2011) 126(2):431–41. doi: 10.1007/s10549-010-1340-y
34. Carroll JS, Hickey TE, Tarulli GA, Williams M, Tilley WD. Deciphering the divergent roles of progestogens in breast cancer. Nat Rev Cancer. (2017) 17(1):54–64. doi: 10.1038/nrc.2016.116
35. Cancello G, Maisonneuve P, Rotmensz N, Viale G, Mastropasqua MG, Pruneri G, et al. Progesterone receptor loss identifies luminal B breast cancer subgroups at higher risk of relapse. Ann Oncol. (2013) 24(3):661–8. doi: 10.1093/annonc/mds430
36. Chen S, Huang L, Chen CM, Shao ZM. Progesterone receptor loss identifies luminal-type local advanced breast cancer with poor survival in patients who fail to achieve a pathological complete response to neoadjuvant chemotherapy. Oncotarget. (2015) 6(20):18174–82. doi: 10.18632/oncotarget.4225
37. Trabert B, Sherman ME, Kannan N, Stanczyk FZ. Progesterone and breast cancer. Endocr Rev. (2020) 41(2):320–44. doi: 10.1210/endrev/bnz001
38. Badwe R, Hawaldar R, Parmar V, Nadkarni M, Shet T, Desai S, et al. Single-injection depot progesterone before surgery and survival in women with operable breast cancer: a randomized controlled trial. J Clin Oncol. (2011) 29(21):2845–51. doi: 10.1200/JCO.2010.33.0738
39. Trabert B, Bauer DC, Buist DSM, Cauley JA, Falk RT, Geczik AM, et al. Association of circulating progesterone with breast cancer risk among postmenopausal women. JAMA Netw Open. (2020) 3(4):e203645. doi: 10.1001/jamanetworkopen.2020.3645
40. Wiebe JP, Pawlak KJ, Kwok A. Mechanism of action of the breast cancer-promoter hormone, 5α-dihydroprogesterone (5αP), involves plasma membrane-associated receptors and MAPK activation. J Steroid Biochem Mol Biol. (2016) 155(Pt A):166–76. doi: 10.1016/j.jsbmb.2015.10.021
Keywords: breast cancer, reproductive hormones, neoadjuvant therapy, sex steroids, hormone receptors, progesterone
Citation: Lan A, Jin Y, Wang Y, Ding N, Wang Y, Dai Y, Jiang L, Tang Z, Peng Y and Liu S (2022) Association of serum reproductive hormones changes after neoadjuvant chemotherapy with hormone receptors expression alterations and survival outcomes in breast cancer. Front. Surg. 9:947218. doi: 10.3389/fsurg.2022.947218
Received: 18 May 2022; Accepted: 15 August 2022;
Published: 31 August 2022.
Edited by:
Alba Di Leone, Agostino Gemelli University Polyclinic (IRCCS), ItalyReviewed by:
Xiaowei Qi, Army Medical University, China© 2022 Lan, Jin, Wang, Ding, Wang, Dai, Jiang, Tang, Peng and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shengchun Liu bGl1c2hlbmdjaHVuMTk2OEAxNjMuY29t
Specialty Section: This article was submitted to Surgical Oncology, a section of the journal Frontiers in Surgery
Abbreviations NAC, neoadjuvant chemotherapy; RFS, relapse-free survival; IQR, interquartile range; HR, hazard ratios; CI, confidence interval; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; FSH, follicle-stimulating hormone; LH, luteinizing hormone; DHEAS, dehydroepiandrosterone sulfate; SHBG, sex hormone-binding globulin; FAI, free androgen index; IHC, immunohistochemistry; CEP17, chromosome enumeration probe 17; FISH, fluorescence
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.