
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 30 August 2022
Sec. Orthopedic Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.944481
This article is part of the Research Topic Surgical Innovation and Advancement in Orthopedics View all 57 articles
 Sheng Li1,2
Sheng Li1,2 Liang A1,2*
Liang A1,2*
Background: With respect to knee arthroscopy, assessing the amount of hidden blood loss is of great importance to avoid potential complications such as fever, anemia, difficulty in wound healing and wound infection. The current study aims to investigate the hidden blood loss and its factors in patients who underwent minimally invasive knee arthroscopy.
Methods: Consecutive patients with knee joint injury, who underwent arthroscopic minimally invasive treatment, were enrolled from January 2019 to November 2020 and were retrospectively studied. Demographic information on these patients, such as medical history and biochemical parameters, was collected. The hidden blood loss was calculated. Multivariate linear regression analysis was used to confirm independent factors associated with hidden blood loss.
Results: Finally, a total of 100 patients aged 44.78 ± 13.67 (range 17–66) years were reviewed, and it was found that a substantial amount of [387.02 ± 252.56 (range 18.89–1130.06) ml] hidden blood loss occurred after minimally invasive knee arthroscopy. Univariate analysis showed that this hidden blood loss was negatively correlated with age, gender, postoperative hemoglobin, and postoperative hematocrit (all P < 0.05), while it was positively correlated with body mass index (BMI), length of hospital stay, preoperative red blood cells, preoperative hemoglobin, preoperative hematocrit, blood volume, and the presence of medical conditions (all P < 0.05). Further multivariate linear regression indicated that preoperative hematocrit, blood volume, and postoperative hematocrit were independent factors associated with actual blood loss, and preoperative hematocrit, blood volume, postoperative hematocrit, and gender were independent factors associated with hidden blood loss, respectively (all P < 0.05).
Conclusion: Preoperative hematocrit, preoperative blood volume, postoperative hematocrit, and gender are the influencing factors of hidden blood loss in patients undergoing minimally invasive treatment under knee arthroscopy. More attention should be paid to hidden blood loss and its factors during the perioperative period.
Arthroscopy provides a technical guarantee for the minimally invasive treatment of orthopedic knee joint injury. Compared with traditional open surgery, it has the advantages of minimized surgical trauma, less bleeding, and accelerated postoperative rehabilitation (1). At present, it is being widely used in medical surgery for sports orthopedics and is achieving good clinical results (2). However, the relevant complications after arthroscopy are also becoming a matter of wide concern, and a few examples of these are fever, anemia, difficulty in wound healing, and wound infection. In response to these complications, clinicians have found many causes, of which hidden blood loss after knee arthroscopy is being paid increasing attention by everyone, following which it has become a non-negligible factor (3). Hidden blood loss is not usually mentioned during general assessment because of its invisibility, while an association has been found between increased blood loss and perioperative complications (4). Concerning minimally invasive knee arthroscopy, evaluating hidden blood loss is of great importance to prevent the aforementioned potential complications.
Since researchers proposed the concept of hidden blood loss in 2000 (5), a series of studies on various treatments for this blood loss in the field of orthopedic surgery has been reported successively, such as minimally invasive treatment of tibial fractures (6), minimally invasive treatment of fractures, knee replacement, hip replacement, and spinal surgery (7). To the best of our knowledge, there was no report in the literature on the factors causing hidden blood loss from minimally invasive treatment with knee arthroscopy. Herein, the current study retrospectively reviewed the medical data of patients who underwent minimally invasive knee arthroscopy to evaluate hidden blood loss and identify its associated factors.
The study protocol was approved by the Institutional Review Committee (IRB) of the Central Hospital Affiliated with Shenyang Medical College and followed the tenets of the Declaration of Helsinki. The IRB confirmed that informed consent was waived due to the retrospective nature of the study design and data were analyzed anonymously. From January 2019 to November 2020, 100 consecutive patients who underwent arthroscopically minimally invasive treatment for knee injuries in our hospital met our inclusion criteria and were enrolled in our study. The inclusion criteria were as follows: (1) fresh knee joint injury in one limb, no other serious trauma; (2) minimally invasive arthroscopic knee treatment; (3) blood parameters before surgery and within 3 days after surgery; (4) no hematological diseases (hemophilia or vitamin K deficiency, etc.); and (5) no history of anticoagulant drugs. The exclusion criteria were as follows: patients (1) younger than 16 years; (2) those with previous knee surgery; (3) knee surgery combined with serious blood-related diseases; and (4) oral anticoagulants before 3 months. Demographic information such as age, gender, medical history, diagnosis, and laboratory investigations as well as pre-, intra-, and postoperative data were collected via the electronic medical record system.
An incision of approximately 0.5 cm in the anterolateral and medial sides of the knee was performed, the arthroscopy was located to check the joint cavity, and then the planer was cleaned to determine the injury of the cruciate ligament and meniscus. The hamstring tendon was taken out as the transplanted tendon. The edge of the irregular meniscus was removed and the torn meniscus was sutured. The process of making the cruciate ligament bone tunnel included (1) locating with a femoral and tibial guide; (2) drilling into the Kirschner wire; (3) drilling through the bone cortex with a hollow drill; (4) measuring the bone tunnel; and (5) selecting an appropriate hollow drill to drill an appropriate depth according to the tendon thickness.
Hidden blood loss (ml) = actual total blood loss − overt blood loss + transfusion volume;
Actual total blood loss (ml) = blood volume × (preoperative hematocrit − postoperative hematocrit)/mean hematocrit (Gross equation)
The estimated blood volume (EBV) of each patient was calculated by using the Nadler formula (8). EBV (L) = k1 × height (m)3 + k2 × weight (kg) + k3, where k1 = 0.3669, k2 = 0.03219, and k3 = 0.6041 for males and k1 = 0.3561, k2 = 0.03308, and k3 = 0.1833 for females.
SPSS v20.0 for Windows (IBM Corp., Armonk, NY, USA) was used for data analysis. The Shapiro–Wilk test was used to assess the normality of data distribution. Continuous data were described as either mean ± standard deviation (SD) or median and range based on their distribution. A comparison among different categories was assessed by using the Student's t-test. Pearson's correlation analysis and Spearman's correlation analysis were performed according to the normality of data distribution. Multiple linear regression was conducted for evaluated associated factors on blood loss. A P-value of less than 0.05 was considered statistically significant.
All demographic and baseline characteristics of the included participants are summarized in Table 1. Among 100 patients, there were 58 (58%) males and 42 (42%) females, aged 17–66 years, with a mean of 44.78 ± 13.67 years. Their mean BMI was 18.59–36.98 kg/m2. The mean total actual blood loss was 512.32 ± 317.29 ml, and the mean hidden blood loss was 387.02 ± 252.56 ml.
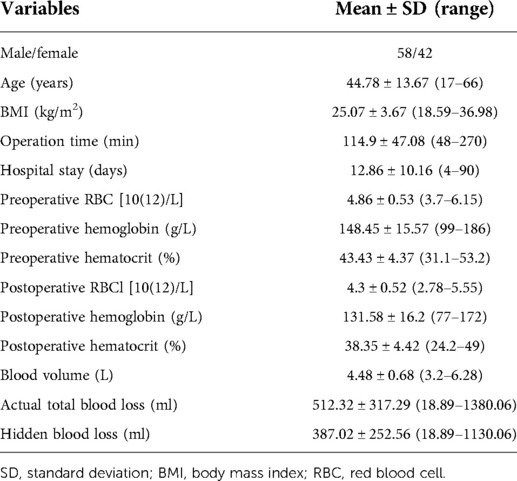
Table 1. Overall characteristics of the study population.
In terms of total actual blood loss, male patients (P = 0.001) without previous medical disease (P < 0.001) had a higher total actual blood loss postoperatively. Similar results were found in hidden blood loss assessments (Table 2).
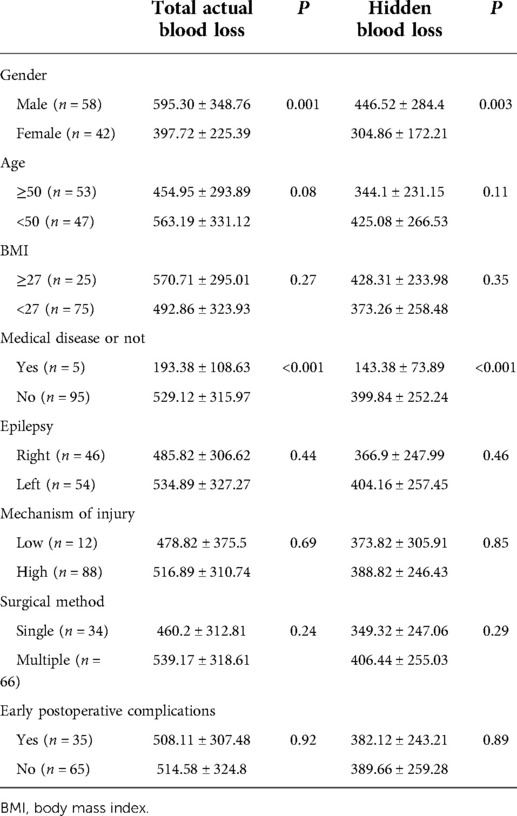
Table 2. Characteristics of included patients.
In correlation analysis, age, gender, postoperative hemoglobin, postoperative hematocrit, BMI, length of hospital stay, preoperative red blood cells, preoperative hemoglobin, preoperative hematocrit, blood volume, and the presence of medical conditions were correlated with actual blood loss and hidden blood loss, respectively (all P < 0.05, Table 3).
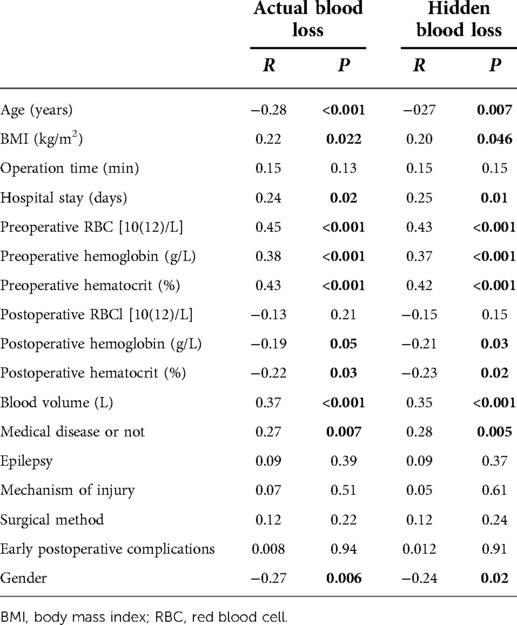
Table 3. Correlation between various indicators and actual blood loss and hidden blood loss.
Multivariate linear regression analysis demonstrated that preoperative hematocrit (β = 100.407, P < 0.001), blood volume (β = 134.497, P < 0.001), and postoperative hematocrit (β = −90.944, P < 0.001) were independently associated with actual blood loss (Table 4). Furthermore, preoperative hematocrit (β = 78.613, P < 0.001), blood volume (β = 119.371, P < 0.001), postoperative hematocrit (β = −72.719, P < 0.001), and gender (β = 52.280, P = 0.011) were independent factors for hidden blood loss (Table 5).
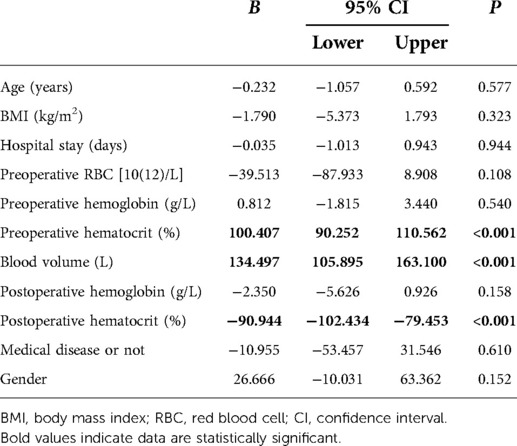
Table 4. Multiple regression analysis related to actual blood loss.
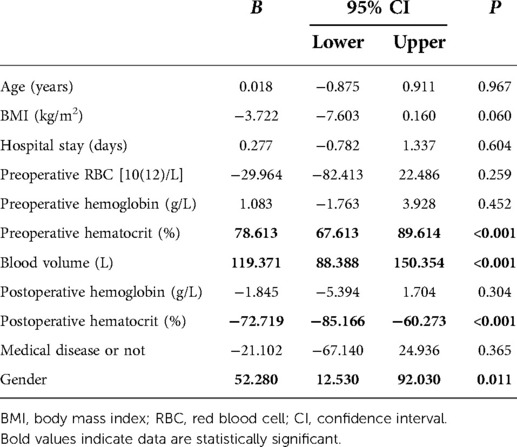
Table 5. Multiple regression analysis associated with hidden blood loss.
To date, the most common complications occurring after arthroscopic surgery may be related to hidden blood loss, which is to rule out significant blood loss during surgery and postoperative drainage volume, as the part of the body’s hidden loss of blood volume. Hidden blood loss is generally associated with hematocele in the joint space, interstitial hematocele, hemolysis, and stress gastrointestinal bleeding leading to hemoglobin loss (9). However, there are few reports on the factors behind hidden blood loss after knee arthroscopic surgery. To address this research gap, our study demonstrated that preoperative hematocrit, blood volume, and postoperative hematocrit were independent factors associated with actual blood loss, and preoperative hematocrit, blood volume, postoperative hematocrit, and gender were independent factors associated with hidden blood loss, respectively.
Numerous studies have shown that hidden blood loss is also an important factor in other surgeries that also belong to the minimally invasive category in clinical practice. Femoral fractures are common in the elderly, with more than 10% of European fracture patients dying within 30 days and more than 25% within 1 year (10). Anemia is one of the important factors associated with mortality, which increases the incidence of lung and brain diseases and disrupts the balance of oxygen supply. At present, the intramedullary nailing fracture technique used in clinical practice is a relatively minimally invasive surgery, which reduces the surgical incision of patients and also the intraoperative visible blood loss on the surface. However, patients still show symptoms of anemia in the perioperative period, which is inseparable from hidden blood loss. Hidden blood loss accounts for a high proportion of total perioperative blood loss in patients with femoral fractures. If its influence is not considered, it often leads to anemia or hypovolemia, which will affect the postoperative recovery of patients (11). If the perioperative blood loss of elderly patients with intertrochanteric fractures is 863.8 ± 429.9 ml, then the hidden blood loss will be 772.3 ± 424.7 ml (12), and so it can be seen that the hidden blood loss is predominant. This is consistent with the results obtained by researchers (4), who observed that the total blood loss of more than 500 patients with fractures was approximately 6 times the operative blood loss. Intramedullary nailing is also used by surgeons in minimally invasive surgery for tibial fractures because of its wide indications, minimal trauma, reliable fixation, and antirotation. Also, due to less intraoperative blood loss, total blood loss in the perioperative period of patients is rarely noticed. However, when reaming intramedullary nails are used to fix tibial fractures, intramedullary nails damage the medulla and significantly increase hidden blood loss (13). Endoscopic lumbar discectomy has been standardized as a typical minimally invasive surgical technique for lumbar disc herniation (14), and studies have shown that this minimally invasive surgery also presents with a large amount of hidden blood loss (15).
The mechanism of hidden blood loss can be summarized as blood stasis in the joint cavity and interstitial space, hemolysis, and gastrointestinal bleeding. Even if wound drainage is done after surgery, bleeding in the patient’s surgical area cannot be completely discharged, and some bleeding remains in the joint cavity and tissue space and is gradually absorbed, organized, and exuded. These hemorrhages are large and do not participate in the systemic circulation, inducing the loss of hemoglobin. This may be related to the abnormal coagulation mechanism of patients suffering from rheumatoid arthritis (16) and blood system bleeding diseases. Perioperative use of anticoagulant drugs will also increase the risk of bleeding. Vascular anatomy (17) shows that the branches of the middle knee artery are distributed in the posterior condylar recess, the posterior half of the medial and lateral ventricles of the knee joint, and the posterior horn of the medial meniscus, forming a vascular plexus extending into the intercondylar fossa and supplying the anterior and posterior cruciate ligaments. The arterioles of the medial and lateral knee arteries form a periteniscal capillary plexus and annular vascular network in the synovium and joint capsule, and the meniscus; the lateral knee artery surrounds the lateral tibial condyle anteriorly and anteriorly from outside, immediately adjacent to the edge of the lateral meniscus body; the inferior transverse branch of the peripatellar artery network runs in the infrapatellar fat pad. These vessels, which supply the anterior and posterior cruciate ligaments, menisci, synovium, joint capsule, and fat pad, carry a high risk of injury during arthroscopic knee surgery, opening the possibility of hidden blood loss. In addition, the use of a tourniquet in patients also destroys the soft tissue at the extrusion site and leads to an increase of a certain amount of interstitial hematocele. Hemolysis, as another factor in the mechanism of action of hidden blood loss, is often easily overlooked. The use of a tourniquet effectively reduces significant blood loss seen intraoperatively, but excessive tourniquet time and reperfusion of limb blood loss after loosening can present additional injuries. Reactive hyperemia of the limbs can lead to a release of the tissue plasminogen activator from the vascular endothelium, which increases the fibrinolytic activity and accelerates the hemolytic reaction, resulting in hidden blood loss after surgery. After prolonged ischemia of tissues, there is a compensatory increase of anaerobic metabolism, activating a large number of oxygen-free radicals, and the body is in a state of oxidative stress (18), which can lead to red blood cell injury and induce hemolysis in the body (19). Hemolysis can further activate oxidative stress (20), resulting in hidden blood loss (21).
Prolonged surgery and blood transfusion also induce hemolysis, which is associated with the use of cardiopulmonary bypass (22) and also with oxidative cell damage (23). Transfused patients experience elevated bilirubin and decreased hemoglobin increment (24), which indicates that hemolysis is also present after transfusion, and it can also lead to hidden blood loss. In addition, gastrointestinal bleeding due to stress ulcers is also responsible for the increase in occult bleeding volume. Patient studied in the literature (25) was hospitalized several times for severe anemia of unknown origin (Hb 40-50 g/l) due to hidden blood loss from the jejunum, which was effectively controlled after treatment with gastrointestinal hemostasis. Perioperative patients are at risk of developing stress ulcers, which may lead to clinically important bleeding, and stress ulcer prevention should be taken seriously in patients in intensive care units and general wards (26).
There are many factors affecting hidden blood loss in the minimally invasive treatment of the knee joint. We hereby study to find out the related factors and guide clinical practice according to the mechanism affecting hidden blood loss. We selected 100 patients with knee joint injury who received arthroscopic minimally invasive treatment. According to the inclusion criteria, there were 58 males and 42 females, aged 17–66 years, with a mean of (44.78 ± 13.67) years; mean BMI (25.07 ± 3.67) kg/m2; mean total actual blood loss in the study population (512.32 ± 317.29) ml; and mean hidden blood loss (387.02 ± 252.56) ml. It can be seen from the characteristics of the study population that a major part of the population is middle-aged, mainly male, with hidden blood loss accounting for approximately 76% of the actual blood loss. It can be seen that hidden blood loss is predominant in a majority of the population, which is consistent with the findings of other minimally invasive surgeries (12). Gender differences associated with hidden blood loss were found in orthognathic surgery studies, with equal gender-related percentages of blood loss (27), which is consistent with our findings. However, in another study of perioperative hidden blood loss in patients undergoing posterior lumbar fusion, gender was not associated with hidden blood loss (28). Interestingly, among patients treated with anterior cervical discectomy and fusion, male patients were an independent risk factor for hidden blood loss (29). Hidden blood loss in females was found more in univariate analysis, which was consistent with the meta-analysis exploring that the risk factors of perioperative hidden blood loss in Chinese patients with femoral fracture were female patients (30), which may be related to the unique physiological structure of women. These discrepancies may be due to different study designs, surgery methods, and perioperative management. In laparoscopic cholecystectomy, hypertension is a contributing factor to hidden blood loss (31). There is a high hidden blood loss during spinal perioperative surgery, and studies have shown that hypertension, diabetes, and heart disease are all risk factors for hidden blood loss (32). Patients with medical diseases often undergo changes in hemodynamics and blood composition, and such patients have coagulation disorders, abnormal cardiopulmonary compensation, poor vascular elasticity, and lower tolerance to anemia, which all lead to more hidden blood loss (33). Most of the patients in this study with a long hospital stay were young patients with high-energy injuries and multiple knee injuries, which potentially increase the risk of occult bleeding.
Moreover, our study demonstrated that preoperative hematocrit, blood volume, and postoperative hematocrit were independent factors associated with actual blood loss, while preoperative hematocrit, blood volume, postoperative hematocrit, and gender were independent factors associated with hidden blood loss. Through a multifactor comprehensive analysis, considering that the muscle and bone content of male patients was significantly higher than that of female patients, these results determined that the male patients had higher preoperative blood volume and preoperative hematocrit. When knee joint injury and minimally invasive surgery occurred, it was accompanied by more muscle and soft tissue injury, especially when the bone tunnel was made, and it was accompanied by more bone loss and bone injury, resulting in more severe hidden blood loss, as demonstrated by lower postoperative hematocrit. According to the present study results, we recommend that in minimally invasive knee surgery, stable normal blood pressure be maintained to prevent more hidden blood loss induced by blood pressure fluctuations, and the tourniquet use time be controlled to prevent local soft tissue injury caused by tourniquet and ischemia-reperfusion to induce more hidden blood loss. Also, the following is recommended: radiofrequency ablation knife hemostasis after loosening the tourniquet to reduce hidden blood loss (34); appropriate perioperative administration of drugs to protect the gastric mucosa to prevent the occurrence of stress ulcers; appropriate use of antioxidants, such as vitamin E and carotene, to prevent hemolysis. It is suggested to use tranexamic acid to reduce blood loss in arthroscopic surgery (35). Studies have shown that (36) tranexamic acid, combined with systemic and local application, has important clinical significance in reducing perioperative blood loss and blood cell loss in patients with femoral fracture, with good safety; it is recommended to cold-compress the incision and surrounding tissues, as low temperatures can constrict capillaries and reduce local oxygen consumption, thereby reducing hidden blood loss (37).
There were some limitations in the current study. First, the sample size was relatively small. Second, this was a retrospective study and there was no control group. In addition, some variables such as the timing of drain removal and liquid balance, which may influence the outcome of hidden blood loss, were not included, and thus, these warrant further investigation. Last but not least, this was a single-center study, so the findings need to be subjected to further validation.
Preoperative hematocrit, blood volume, postoperative hematocrit, and gender are independent factors for hidden blood loss in patients undergoing minimally invasive treatment of the knee joint. More attention to, and adequate management of, these factors will help reduce postoperative hidden blood loss.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Institutional Review Committee (IRB) of the Central Hospital Affiliated to Shenyang Medical College. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
All authors contributed to data analysis, drafting, or revising the article, agreed on the journal to which the article will be submitted, gave final approval for the version to be published, and agreed to be accountable for all aspects of the work. All authors contributed to the article and approved the submitted version.
The present study was supported by the Effect of Ligament Stump Treatment on Bone Tendon Healing in Anterior Cruciate Ligament Injury (Doctoral Research Start-Up Fund of Shenyang Medical College 2020, no. 20205040, SL).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Liu S. Early reconstruction treatment of shot putters’ acute complete anterior cruciate ligament injury under knee arthroscopy. Biomed Res. (2017) 28(20):8818–21.
2. Huang HF, Tian JL, Sun L, Yang XT, Shen YK, Li SS, et al. The effect of anticoagulants on venous thrombosis prevention after knee arthroscopy: a systematic review. Int Orthop. (2019) 43(10):2303–8. doi: 10.1007/s00264-018-4212-4
3. Panagiotis K. Hidden blood loss in spine surgery for A1–A3 thoracolumbar fractures. Comparison between three approaches. J Invest Surg. (2019) 32(8):761–2. doi: 10.1080/08941939.2018.1462418
4. Foss NB, Kehlet H. Hidden blood loss after surgery for hip fracture. J Bone Joint Surg Br. (2006) 88(8):1053–9. doi: 10.1302/0301-620X.88B8.17534
5. Sehat KR, Evans R, Newman JH. How much blood is really lost in total knee arthroplasty? Correct blood loss management should take hidden loss into account. Knee. (2000) 7:151–5. doi: 10.1016/S0968-0160(00)00047-8
6. Wang JQ, Huang XJ, Guo WJ, Zhao YM, Luo P. Hidden blood loss and the influential factors after intramedullary nail fixation of extra-articular tibial fractures - a retrospective cohort study. Injury. (2020) 51(6):1382–6. doi: 10.1016/j.injury.2020.04.025
7. Mima Y, Yagi M, Suzuki S, Tsuji O, Nagoshi N, Okada E, et al. Hidden blood loss in extreme lateral interbody fusion for adult spinal deformity. J Orthop Sci. (2022):S0949-2658(22)00014-8. doi: 10.1016/j.jos.2022.01.003
8. Nadler SB, Hidalgo JU, Bloch T. Prediction of blood volume in normal human adults. Surgery. (1962) 57:224–32.
9. Hu M, Zhang Y, Zhao WJ, Liu X, Shi PZ, Wang JW, et al. Perioperative hidden blood loss in lumbar disk herniation patients with percutaneous endoscopic transforaminal discectomy and influencing factors. Clin Spine Surg. (2022) 35(5):E438–E43. doi: 10.1097/BSD.0000000000001282
10. Tian S, Shen Z, Liu Y, Zhang Y, Peng A. The effect of tranexamic acid on hidden bleeding in older intertrochanteric fracture patients treated with PFNA. Injury. (2018) 49(3):680–4. doi: 10.1016/j.injury.2018.01.026
11. Cui H, Chen K, Lv S, Yuan C, Wang Y. An analysis of perioperative hidden blood loss in femoral intertrochanteric fractures: bone density is an important influencing factor. BMC Musculoskelet Disord. (2021) 22(1):6. doi: 10.1186/s12891-020-03922-x
12. Li B, Li J, Wang S, Liu L. Clinical analysis of peri-operative hidden blood loss of elderly patients with intertrochanteric fractures treated by unreamed proximal femoral nail anti-rotation. Sci Rep. (2018) 8:3225. doi: 10.1038/s41598-018-21703-4
13. Wang JQ, Chen ZX, Guo WJ, Zhao YM. Comparison of plate and intramedullary nail fixation of extra-articular tibial fractures: a retrospective study exploring hidden blood loss. Injury. (2019) 50(2):546–50. doi: 10.1016/j.injury.2018.12.016
14. Chen F, Xin J, Su C, Liu X, Cui X. Pain variability of tissues under endoscope in percutaneous endoscopic lumbar discectomy and its significance: a retrospective study. Pain Phys. (2021) 24(6):E877–82. doi: 10.36076/ppj.2021.24.E877
15. Ao S, Zheng W, Wu J, Tang Y, Zhang C, Zhou Y, et al. Comparison of preliminary clinical outcomes between percutaneous endoscopic and minimally invasive transforaminal lumbar interbody fusion for lumbar degenerative diseases in a tertiary hospital: is percutaneous endoscopic procedure superior to MIS-TLIF? A prospective cohort study. Int J Surg. (2020) 76:136–43. doi: 10.1016/j.ijsu.2020.02.043
16. Xu S, Liang Y, Wang J, Yu G, Guo C, Zhu ZQ, et al. Blood loss of posterior lumbar interbody fusion on lumbar stenosis in patients with rheumatoid arthritis: a case-control study. Spine. (2019) 44(17):E1045–52. doi: 10.1097/BRS.0000000000003037
17. Jia JX, Yan XS, Song W. Modern Clinical Applied Anatomy. Harbin: Heilongjiang Science and Technology Press (2018). 165–7 p.
18. Chen H, Wei JQ, Wang YW, Zhou KP, He Y, Liu H, et al. Protective effects of rocuronium bromide on ischemia-reperfusion injury in skeletal muscle induced by tourniquet in patients undergoing elective unilateral total knee arthroplasty: a prospective, double blind, randomized, controlled study. Drug Des Devel Ther. (2020) 14:3373–84. doi: 10.2147/DDDT.S252546
19. Delvasto NL, Roem D, Bakhtiari K, Van MG, Meijers JCM, Jongerius I, et al. Iron-driven alterations on red blood cell-derived microvesicles amplify coagulation during hemolysis via the intrinsic tenase complex. Thromb Haemostasis. (2022) 122(1):80–91. doi: 10.1055/a-1497-9573
20. Maksimovich E, Pronko T, Yanushko ZV, Gulay I, Snezhitsky V. Assessment of oxidative stress during coronary artery bypass grafting in persons with different degrees of intraoperative hemolysis (article). Kardiol v Belarusi. (2019) 11(3):418–29.
21. Yuan T, Cong Y, Meng J, Qian H, Ye W, Sun WS, et al. Arachidonic acid causes hidden blood loss-like red blood cell damage through oxidative stress reactions. J Surg Res. (2017) 211(1):14–20. doi: 10.1016/j.jss.2016.11.060
22. Spina S, Lei C, Pinciroli R, Berra L. Hemolysis and kidney injury in cardiac surgery: the protective role of nitric oxide therapy. Semin Nephrol. (2019) 39(5):484–95. doi: 10.1016/j.semnephrol.2019.06.008
23. Sovira N, Lubis M, Wahidiyat PA, Suyatna FD, Gatot D, Bardosono S. Effects of α-tocopherol on hemolysis and oxidative stress markers on red blood cells in β-thalassemia major. Clin Exp Pediatr. (2020) 63(8):314–20. doi: 10.3345/cep.2019.00542
24. Roubinian NH, Reese SE, Qiao H, Plimier C, Fang F, Page GP, et al. Donor genetic and nongenetic factors affecting red blood cell transfusion effectiveness. JCI Insight. (2022) 7(1):e152598. doi: 10.1172/jci.insight.152598
25. Kumskova MA, Zozulya N, Dvyrnik VN, Likhachyova E, Yakovleva E, Savchenko VG. Comparison of different phenotypes of Bernard–Soulier syndrome. Blood. (2017) 130(1):4856. doi: 10.1182/blood.V130.Suppl_1.4856.4856
26. Xing XX, Zhu C, Chu YQ, Bai XR, Wang K, Zhang ST, et al. Physicians’ knowledge, attitude, and prescribing behavior regarding stress ulcer prophylaxis in China: a multi-center study. BMC Gastroenterol. (2021) 21(1):402. doi: 10.1186/s12876-021-01979-z
27. Michael S, Jürgen W, Sarah-Jayne E, Irene M, Jasmin R, Thomas G, et al. Is there a hidden blood loss in orthognathic surgery and should it be considered? Results of a prospective cohort study. J Craniomaxillofac Surg. (2021) 49(7):545–55. doi: 10.1016/j.jcms.2020.07.015
28. Fei L, Zhongyang L, Wen H, Xinggui T, Lipeng Z, Jianping K, et al. Hidden blood loss and the risk factors after posterior lumbar fusion surgery: a retrospective study. Medicine (Baltimore). (2020) 99(19):e20103. doi: 10.1097/MD.0000000000020103
29. Tongchuan C, Dong C, Shuguang W, Pengzhi S, Junwu W, Pingchuan W, et al. Perioperative hidden blood loss in elderly cervical spondylosis patients with anterior cervical discectomy fusion and influencing factors. Geriatr Orthop Surg Rehabil. (2021) 12:1–6. doi: 10.1177/21514593211002164
30. Tao W, Junfei G, Zhiyong H. Risk factors for perioperative hidden blood loss after intertrochanteric fracture surgery in Chinese patients: a meta-analysis. Geriatr Orthop Surg Rehabil. (2022) 13:1–10. doi: 10.1177/21514593221083816
31. Ren-Rui W, Yong-Li W, Xiao-Chang W, Hai Q, Zhen-Hua T, Ren-Yi X, et al. Hidden blood loss and the influencing factors after laparoscopic cholecystectomy. ANZ J Surg. (2020) 90(1–2):103–8. doi: 10.1111/ans.15502
32. Zhixiang G, Cong X, Hongtao Y, Xiangyu M. Statistical decision tree model analysis on hidden blood loss in the perioperative period of thoracolumbar burst fracture accompanied with neurological deficiency. Chin J Tissue Eng Res. (2021) 21(15):2364–9. doi: 10.3969/j.issn.2095-4344.3817
33. Yuanxing Z, Xin F, Yang M, Ke S, Wang B, Zhonghai L. Hidden blood loss and its possible risk factors in minimally invasive transforaminal lumbar interbody fusion. J Orthop Surg Res. (2020) 15(1):445. doi: 10.1186/s13018-020-01971-5
34. Hui-liang S, Zheng L, Ming-li F, Guang-le C. Analysis on hidden blood loss of total knee arthroplasty in treating knee osteoarthritis. Chin Med J. (2011) 124(11):1653–6. doi: 10.3760/cma.j.issn.0366-6999.2011.11.009
35. Akti S, Zeybek H, Bilekli AB, Çelebi NÖ, Erdem Y, Çankaya D. The effect of tranexamic acid on hidden blood loss in total hip arthroplasty. Jt Dis Relat Surg. (2022) 33(1):102–8. doi: 10.52312/jdrs.2022.446
36. Jun-An L, Hai-Dong C, Ye H, Shu-Jun L. Application of tranexamic acid in the treatment of intertrochanteric fracture of femur. Chin J Orthop Traumatol. (2021) 34(7):601–4. doi: 10.12200/j.issn.1003-0034.2021.07.003
37. Han M, Wu C. Effects of circulatory compression cold therapy combined with nursing intervention of behavior change theory on perioperative period hidden blood loss volume and coping style of patients with intertrochanteric fracture. Curr Med Res Pract. (2021) 6(8):153–5. doi: 10.19347/j.cnki.2096-1413.202108051
Keywords: arthroscopy, minimally invasive, knee, hidden blood loss, risk factors
Citation: Li S and A L (2022) The hidden blood loss and its factors in patients undergoing minimally invasive knee arthroscopy. Front. Surg. 9:944481. doi: 10.3389/fsurg.2022.944481
Received: 15 May 2022; Accepted: 22 July 2022;
Published: 30 August 2022.
Edited by:
Paphon Sa-ngasoongsong, Mahidol University, ThailandReviewed by:
Lei Liu, Guangdong Provincial People's Hospital, China© 2022 Li and A. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Liang A YWxpYW5ndnZpcEAxNjMuY29t
Specialty Section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.