
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Surg., 18 July 2022
Sec. Thoracic Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.943829
This article is part of the Research TopicNear-Infrared Fluorescence Guided Surgery: State of the evidence from a health technology assessment perspectiveView all 10 articles
 Riccardo Tajè1,†
Riccardo Tajè1,† Filippo Tommaso Gallina1*†
Filippo Tommaso Gallina1*† Daniele Forcella1Giulio Eugenio Vallati2Federico Cappelli2Federico Pierconti3Paolo Visca4Enrico Melis1Francesco Facciolo1
Daniele Forcella1Giulio Eugenio Vallati2Federico Cappelli2Federico Pierconti3Paolo Visca4Enrico Melis1Francesco Facciolo1
In the last few years, minimally invasive surgery has become the standard routine practice to manage lung nodules. Particularly in the case of robotic thoracic surgery, the identification of the lung nodules that do not surface on the visceral pleura could be challenging. Therefore, together with the evolution of surgical instruments to provide the best option in terms of invasiveness, lung nodule localization techniques should be improved to achieve the best outcomes in terms of safety and sensibility. In this review, we aim to overview all principal techniques used to detect the lung nodules that do not present the visceral pleura retraction. We investigate the accuracy of fluorescence guided thoracic surgery in nodule detection and the differences among the most common tracers used.
Along with the diffusion of lung cancer screening, an increasing number of ground glass opacities (GGO) and sub-centimetric pulmonary nodules are detected. Although both GGO and sub-centimetric nodules are non-specific radiological features, a consistent rate of these findings may be revealed as early-stage lung cancer requiring surgical resection (1, 2).
Minimally invasive thoracic surgery is now the new paradigm in the treatment of Non-Small Cells Lung Cancer (NSCLC) (3, 4). Video-thoracoscopic and robotic approaches have demonstrated better perioperative outcomes compared with the open approach. Although controversies still remain with regard to intraoperative lymph node assessment, the long-term oncological outcomes seem to be similar to those of thoracotomy (5). Nonetheless, irrespective of whether surgical techniques are in tune with the rapid technological advancements of the last few decades, nodule detection is still restricted to a visual inspection of indirect signs, such as visceral pleura retraction, and manual palpation (6). However, sub-centimetric nodules or GGO lesions, especially if deeply located in the parenchyma, may let the visceral pleura unaltered, and video-thoracoscopic access or insensitive robotic instruments may hinder a manual inspection of the lung. Nodule localization failure leads to conversion to thoracotomy in up to 63% of the procedures. Nonetheless, a vague nodule localization can result in an insufficient margin, especially in sub-lobar resections (7–9). Thus, several strategies such as hook wire positioning and intraoperative fluoroscopy have been used to pre-operatively localize pulmonary nodules and ensure adequate margin, but some complications have been recorded (10–12).
Fluorescence and near-infrared (NIR) fluorescence guided surgery have been recently implemented in surgical oncology to localize hard-to-detect nodules and to ameliorate surgical radicality (6, 13). This technique takes advantage from direct injection inside or near the targeted nodule of a fluorescent tracer. The tracer can be injected by percutaneous fine needle puncturing under CT guidance or through endobronchial navigation. In the latter, a 3-dimensional virtual reconstruction of the patient lung is obtained based on CT imaging. The airway proximal to the nodule is then identified and the tracer is injected through a bronchoscopic catheter (14).
The primary endpoint of this review is to establish the localization effectiveness of fluorescence-guided thoracic surgery in nodule detection. The secondary endpoints of this study are to evaluate the differences among the most common tracers used for nodule detection, in order to establish the most used tracer dosage, evaluate the radiological characteristics of the detected nodules, nodule diameter, and distance between the nodule and the visceral pleura, establish the best time interval between nodule marking and surgery, and discern the characteristics of the failure of the marking procedure.
The literature search has been done on PubMed. Only English language studies published before March 2022 have been included.
References of the studies found with the PubMed search terms and of previously published literature reviews on the topic have been reviewed as a supplement by two independent reviewers. The study selection process and the terms used in the search are provided in the Supplementary Material in accordance with PRISMA guidelines. For the search strategy, no filters or limits have been applied.
All studies involving fluorescence-guided adult human thoracic surgery have been included. Furthermore, only studies involving more than 10 marking procedures were included. Case reports, reviews, the category how-to-do-it, and technical studies have been excluded. Clinical heterogeneity has been assessed by two independent reviewers. Enrolled studies included consecutive or random samples of patients with pulmonary nodules. Case-control studies have been excluded, unless data on the results of the fluorescence-guided subgroup could be undoubtedly retrieved.
As one of the features analyzed in this study is to assess the NIR dye-administered dosage and pharmacodynamics characteristics of the dye, studies involving patients with age below 18 years old have been excluded. Finally, studies in which data on the used fluorescent dye results are lacking have been excluded.
From each study, two independent reviewers collected and analyzed in an excel sheet the following data: the demographic characteristics of the patients; the number, dimension, distance from the visceral pleura, and radiological features of the labelled nodules; the type, dosage, administration modality, duration, marking procedure-related complications, and dye tracer-related toxicities of the adopted fluorescent tracer; the time interval between dye tracer administration and surgery; the type and duration of surgical resection.
Of the 892 studies identified from PubMed search, 55 studies have been considered eligible for this review (15–69).
The results are summarized in Table 1. A total of 3399 patients presenting with 3741 pulmonary nodules were enrolled in this systematic review. Particularly, the average nodule dimension was under 10 mm in 29 studies ranging from 2 to 46 mm. The radiological feature of the nodule revealed a solid morphology in 699 nodules, while 602 nodules were subsolid and 1625 were GGO. Finally, the remaining 12 nodules were cavitary. In 1129 nodules, the radiological appearance of the nodule was not reported. The distance from the nodule to the visceral pleura ranged from 0 to 60 mm. The outcomes of the principal techniques analyzed in this review are summarized in Figure 1.

Figure 1. Localization effectiveness of the main techniques according to the depth from the nodule to the visceral pleura.
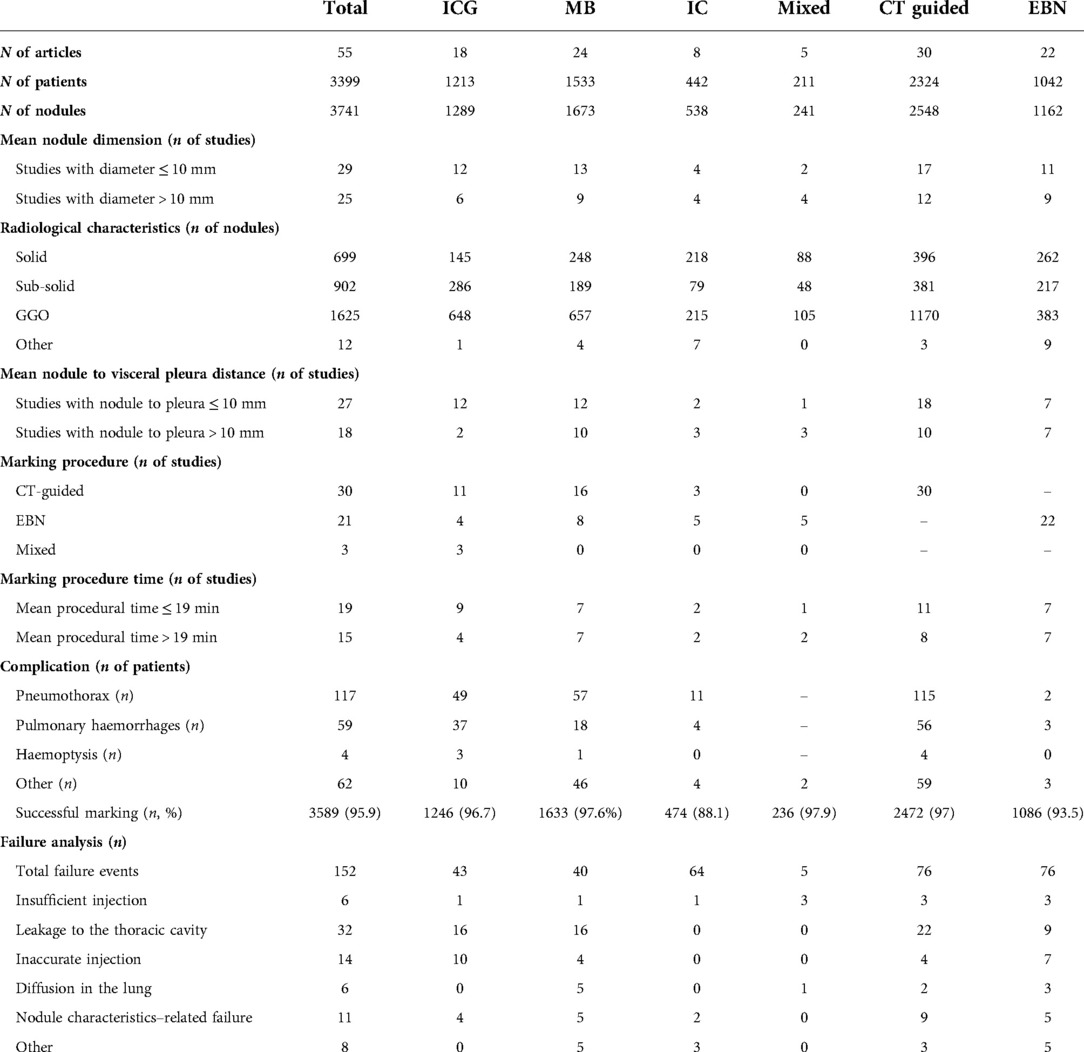
Table 1. Patients and techniques characteristics.
Methylene blue (MB) has been used as the only fluorescent tracer in 1533 patients with 1673 nodules.
MB is a blue-colored thiazine dye. It can be administered orally, topically, or intravenously. MB has an excitation peak of approximately 670 nm and an emission peak at 690 nm. This range of fluorescence can interfere with the background autofluorescence emanated by haemoglobin and cytochromes. MB has a renal metabolism and is excreted through urine; thus, it should be avoided for renal insufficiency. Transient desaturation, cardiac arrhythmias, coronary vasoconstriction, reduced cardiac output, and decreased renal and mesenteric blood flow after intravenous administration have been recorded (13, 70, 71)
Percutaneous CT-guided dye injection was used in two-thirds of the studies. The mean marking procedure time was reported in 14 papers. Luo et al. (24) reported the maximal marking procedure duration of 120 min.
The mean dosage of administered MB was 1.22 ml ranging from 0.04 to 7 ml. MB was administered in combination with autologous blood in two reports (19, 28), as a medical glue in two reports (33, 34), non-ionic contrast agent in two reports (15, 17), collagen in one report (31), and in a mixture of MB, fibrinogen, and thrombin in one report (24). No MB-related side effects were demonstrated in the different studies.
In most of the papers, the administration was performed the same day of the surgical procedure. In a report by Sun et al. (35), MB diffused on the pleural surface in a patient undergoing an 8-hour delay in surgery. Similarly, Zhang et al. (32) reported a localization failure in a patient undergoing resection 24 hours after the marking procedure. Vandoni et al. (17) found a significant correlation between the time interval between labelling and resection-affected MB density of coloration, resulting in three nodules undergoing localization failures at 190, 260, and 270 min. As shown in Figure 1, in most of the papers, MB was used for nodules ranging from 12 to 16 mm from the pleural surface, and the maximal depth was 60 mm (33).
In the different studies, localization effectiveness ranged from 78.9 to 100%. In 8 of the 24 studies, all nodules were correctly resected after the MB marking procedure. Among the 1673 nodules, MB-guided surgery correctly localized and resected 1633 nodules (97.6% 95%CI [93.3%,98%]).
Marking procedure failures were recorded in detail in 14 reports. Leakage of the tracer to the pleural cavity due to pleural perforation or unprecise nodule puncturing was recorded in 16 marking procedures included in 10 different reports (17, 18, 21, 26, 28, 29, 33, 35, 36, 38). In three reports, including five localization failure events, MB diffused in the pulmonary parenchyma, resulting in a wide-labelled area including the nodule (19, 30, 38). Finally, four marking procedures failed due to misplaced trajectory during tracer injection (18, 36). Particularly, marking procedure–related failures were associated with excessive dilution of the tracer (28). In this paper, mixing MB with autologous blood helped to reduce color vanishing. Nodule characteristics–related failures were reported in seven reports (15, 17, 18, 26, 32, 36, 38). Particularly, extensive anthracosis, inadequate pulmonary exclusion during surgery, and subpleural nodules resulted in incorrect labelling procedures. Munoz et al. reported a marking failure in a 4 -mm nodule located 40 mm deep in the parenchyma (26). Finally, as previously stated, the interval time between the marking procedure and surgical resection significantly affected the labelling process (17, 32).
ICG was used as the only fluorescent tracer in 1213 patients with 1289 nodules. In two-third of the studies, the mean nodule diameter was below 10 mm, and 50% of the nodules were GGO.
ICG is a hydro-soluble, anionic, and amphiphilic tricarbocyanine dye. It can be administered intravenously or topically. The excitation peak is at 780 nm and the emission peak is at 820 nm. This range of fluorescence prevents any interference with the background tissue autofluorescence. NIR fluorescence can vary in depths ranging from 0.5 to 1 cm. The safety spectrum is well established, with a low risk of adverse effects. ICG also allows multiple repeated uses due to its short half-life of 150 to 180 s and is cleared exclusively by the liver (6, 13).
Percutaneous CT-guided dye injection was used in most of the studies. The mean marking procedure time was reported in 13 papers and ranged from 9 to 35 min. The marking procedure was accomplished in less than one hour.
Administered ICG solution concentration ranged from 0.125 mg/ml to 2.5 mg/ml. The total dosage of administered ICG ranged from 0.0125 mg to 1.25 mg of the dye. No ICG-related side effects were demonstrated in the different studies.
In most of the papers, the administration was performed the same day of the surgical procedure. Nonetheless, in 14 studies, the nodule marking procedure was accomplished preoperatively. In the report of Kim et al. (48), nodule marking was performed on an average 5 h before the procedure and up to 31 h before the procedure. The procedure still yielded successful intraoperative localization and resection of all the marked nodules with adequate oncological margins larger than the nodule diameter or larger than 20 millimeters, with the exception of one patient. In this case, margin infiltration was unrelated to nodule marking. In most of the papers, ICG was used for nodules ranging from 5 to 8 mm from the pleural surface, and maximal depth was 42 mm (48) (Figure 1).
In the different studies, localization effectiveness ranged from 86 to 100%. In 8 of the 18 studies, all the nodules were correctly resected under ICG guidance. Among the 1289 nodules, ICG-guided surgery correctly localized and resected 1246 nodules (96.7% 95%CI [93.9%,98.4%]). Marking procedure failures were recorded in detail in seven reports. Particularly, marking procedure–related failures were associated with insufficient administration of ICG injection in 1 patient (44), and leakage of the tracer to the pleural cavity due to pleural perforation in 16 nodules was included in 5 different reports (44, 43, 49, 55, 46). Finally, inaccurate injection and failure of the bronchoscopic navigational system were reported by Geraci et al. (46) in seven and three cases, respectively. Nodule characteristics–related failures were reported in four studies (44, 39, 42, 55). Particularly, no pleural marks were developed in a nodule located at a 20 mm depth in the pulmonary parenchyma at a ICG dosage of 0,3ml of a 2,5 mg/ml ICG concentration (55). Anayama et al. (42), reported two failures for nodules located at 28 and 30 mm from the visceral pleura after endobronchial administration of ICG-iopamidol. Ujiie et al. (39) demonstrated no pleural marking of a centimetric nodule located at 48 mm from the visceral pleura. In another patient, the lung could not be properly deflated leading to fluorescent localization failure. Finally, Zhang et al. (44) failed to localize a 6 mm nodule located 1.1 mm from the pleura.
Surgical margins were histologically negative because of neoplastic invasion in all nodules but two (41, 48). Surgical radicality was considered according to the guideline only in one study (48). In the other studies, surgical margins were considered adequate by the authors, but there is still no definition of surgical margin adequacy.
Indigo Carmine has been used as the only dye fluorescent tracer in 442 patients with 583 nodules.
Endobronchial dye injection was used in five out of eight enrolled reports. The mean marking procedure time ranged from 6 to 35 min (57, 58).
The administered IC dosage ranged from 0.5 to 2 ml, more frequently, 1 ml of dye tracer was injected. Dosages below 0.5 ml of IC are at high risk of localization failure (62). IC administration was performed up to 3 days before the surgical procedure (58). In a report by Hasegawa et al. (62), an interval time between marking and surgical procedure longer than 24 h significantly affected resection. In this report, a mixture of IC and a non-ionic contrast agent allowed intraoperative fluoroscopy, resulting in a complete resection of the nodules up to three days after the marking procedure. In most of the papers, IC was used for nodules from 5 to 17 mm from the pleural surface. Results: In the different studies, localization effectiveness ranged from 83.3 to 100%. In four of the eight studies, all the nodules were correctly resected after the IC marking procedure. Among the 538 nodules, IC-guided surgery correctly localized and resected 474 nodules (88.1% 95%CI [85.8%,99.3%]).
Marking procedure failures were recorded in detail in three reports (59, 57, 62).
Particularly, marking procedure–related failures were associated with an IC dosage below 0.5 ml and a three-day delay between labelling procedure and surgery (62). Nodule-related failures were associated with extensive anthracosis (57, 62) and parietal pleura to nodule distance >10 mm (59). Finally, Sato et al. demonstrated a 10% increase in failure risk in nodules requiring resection depth greater than 30 mm (59).
Surgical margins were histologically negative because of neoplastic invasion in all the reports, with the exception of Sato et al. (59).
In this review, the efficacy of pulmonary nodule labelling for fluorescence-guided surgical resection of three different fluorescent dyes have been investigated. Methylene blue demonstrated the highest effectiveness in preoperative nodule labelling. Nonetheless, MB demonstrated a significant tendency to diffuse in the adjacent parenchyma. This result is consistent with previous findings (72). In order to avoid MB diffusion or dilution, surgery should be scheduled preferably the same day of nodule MB labelling due to the decrease of color intensity and the higher risk of targeting failure following the first 24 h from the targeting procedure (17, 32). Mixing MB with collagen or blood enhanced MB color intensity duration (19, 28, 31). ICG demonstrated similar results in terms of localization effectiveness. Nonetheless, the viscosity characterizing ICG and its ability to bind autologous collagen resulted in better results in terms of nodule definition and marking duration. Nonetheless, in Wen et al., the exceeding tracer could be removed by cleansing it with a surgical drape, following which the exact marking location was revealed (41). Kim et al. (48) demonstrated that ICG was still vividly detectable at surgery 3 days after the marking procedure. In a case report, ICG label could be detected up to 6 days after the marking procedure (73). IC showed the worst results in terms of nodule identification. This testifies to the limited number of reports on IC. Nonetheless, failure explanations were reported only in three of these papers for 5 failed procedures out of 64. Further studies are needed to evaluate IC in clinical practice, eventually building strategies to improve these results. In one of the reports (69), an endobronchial virtual-assisted-lung-mapping compared ICG and IC, demonstrating better results in the ICG group. The nodule depth from the pleural surface has a major impact on nodule localization effectiveness. As depicted in Figure 1, ICG demonstrated better results for subpleural nodules, while MB achieved better results in deeper nodules. IC was the tracer with a wider range of nodule-from-the-pleura deepness, but the overall number of studies are still limited.
Among the 55 reports included in this review, the fluorescent dye was injected through a CT-guided percutaneous administration in 30 of the enrolled studies, while endobronchial labelling of the nodules was used in 22 reports. From an analysis of data retrieved from 54 of the 55 papers, 2,324 patients underwent CT-guided labelling of 2548 nodules, while 1042 patients underwent bronchoscopic labelling of 1162 nodules. The rate of complications was higher in the CT-guided group, and pneumothorax was the most frequent complication experienced in this group. This is consistent with the finding of previous reports (42, 51). Thus, endobronchial localization can be particularly indicated for the emphysematous lung or for patients requiring labelling of multiple or bilateral nodules. The reasons underling localization failures in the reports included in the groups have been compared. The procedures failed due to leakage of the fluorescent dye to the thoracic cavity twice in the CT-guided group when compared with that in the endobronchial group, while inaccurate administration of injection was more frequent in the endobronchial group. As depicted in Figure 1, CT-guided labelling demonstrated better results for nodules up to 12 mm, while EBN labelling demonstrated better results in deeper nodules.
With improvements in minimally invasive and robotic approaches, nodule localization strategies are gaining great importance. Therefore, future research studies are needed to address several unsolved issues. Particularly, comparative studies to evaluate the best fluorescence-based-tracer and to compare the best administration strategies are lacking in the different settings. Nonetheless, fluorescent tracers that can be absorbed by the tumors preserving fluorescence can lead future research.
In this review, we analyzed the principal fluorescence-guided techniques used to visualize the lung nodule. Despite the accurate selection criteria, the heterogeneous nature of the studies could represent a limitation to identify the best technique. However, we can conclude that fluorescence-guided surgical resection of pulmonary nodules is safe and feasible. A preoperative marking procedure can facilitate surgical resection of hard-to-localize nodules. The choice between the tracer and the marking technique should be balanced by considering the nodule depth in the pulmonary parenchyma, tracer characteristics, and the time interval between marking procedure and surgery.
Conceptualization was done by FTG and FF.; methodology was devised by FTG and RT.; software was provided by DF, RT, and FC; validation was done by FF and FP; formal analysis was done by FTG, RT, and GV; investigation was done by FC, VC, and PV; resources were provided by FF and GV; data curation was done by FTG and RT; writing—original draft preparation was done by FTG, RT, EM, and FF; writing, review, and editing were done by EM, FF, FC, and DF; visualization was performed by DF and FP; supervision was done by FF and EM; project administration was managed by GV and FF; funding acquisition was provided by FC and FF. All authors contributed to the article and approved the submitted version.
This work was supported by Funds “Ricerca Corrente 2022” from the Italian Ministry of Health.
The authors extend our deepest gratitude to those who have contributed to our project over the last few years. The authors wish to thank the Scientific Direction of the IRCCS “Regina Elena” National Cancer Institute for the support provided to the study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2022.943829/full#supplementary-material.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Lin M-W, Chen J-S. Image-guided techniques for localizing pulmonary nodules in thoracoscopic surgery. J Thorac Dis. (2016) 8(Suppl 9):S749–S755. doi: 10.21037/jtd.2016.09.71
2. Callister ME, Baldwin DR, Akram AR, Barnard S, Cane P, Draffan J, et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules. Thorax. (2015) 70(Suppl 2):ii1–ii54. doi: 10.1136/thoraxjnl-2015-207168
3. Gallina FT, Tajè R, Forcella D, Corzani F, Cerasoli V, Visca P, et al. Oncological outcomes of robotic lobectomy and radical lymphadenectomy for early-stage non-small cell lung cancer. J Clin Med. (2022) 11:2173. doi: 10.3390/jcm11082173
4. Swanson SJ, Herndon JE 2nd, D'Amico TA, Demmy TL, McKenna RJ Jr, Green MR, et al. Video-assisted thoracic surgery lobectomy: report of CALGB 39802–a prospective, multi-institution feasibility study. J Clin Oncol. (2007 Nov 1) 25(31):4993–7. doi: 10.1200/JCO.2007.12.6649
5. Gallina FT, Melis E, Forcella D, Mercadante E, Marinelli D, Ceddia S, et al. Nodal upstaging evaluation after robotic-assisted lobectomy for early-stage non-small cell lung cancer compared to video-assisted thoracic surgery and thoracotomy: a retrospective single center analysis. Front Surg. (2021) 8:666158. doi: 10.3389/fsurg.2021.666158
6. Nagaya T, Nakamura YA, Choyke PL, Kobayashi H. Fluorescence-guided surgery. Front Oncol. (2017) 7:314. doi: 10.3389/fonc.2017.00314
7. Suzuki K, Nagai K, Yoshida J, Ohmatsu H, Takahashi K, Nishimura M, et al. Video-assisted thoracoscopic surgery for small indeterminate pulmonary nodules: indications for preoperative marking. Chest. (1999) 115:563–8. doi: 10.1378/chest.115.2.563
8. Cardillo G, Regal M, Sera F, Di Martino M, Carbone L, Facciolo F, et al. Videothoracoscopic management of the solitary pulmonary nodule: a single-institution study on 429 cases. Ann Thorac Surg. (2003) 75:1607–11. doi: 10.1016/S0003-4975(02)04827-0
9. Powell TI, Jangra D, Clifton JC, Lara-Guerra H, Church N, English J, et al. Peripheral lung nodules. Ann Surg. (2004) 240:481–9. doi: 10.1097/01.sla.0000137132.01881.57
10. Zhou J, Yang F, Jiang G, Wang J. Applications of indocyanine green based near-infrared fluorescence imaging in thoracic surgery. J Thorac Dis. (2016 Oct) 8(Suppl 9):S738–S743. doi: 10.21037/jtd.2016.09.49
11. Park CH, Han K, Hur J, Lee SM, Lee JW, Hwang SH, et al. Comparative effectiveness and safety of preoperative lung localization for pulmonary nodules: a systematic review and meta-analysis. Chest. (2017) 151:316–28. doi: 10.1016/j.chest.2016.09.017
12. Farkas EA, Stoeckel DA, Nassif AS, Lim MJ, Naunheim KS. Intracoronary fiducial embolization after percutaneous placement for stereotactic radiosurgery. Ann Thorac Surg. (2012) 93:1715–17. doi: 10.1016/j.athoracsur.2011.08.057
13. Thammineedi SR, Saksena AR, Nusrath S, Iyer RR, Shukla S, Patnaik SC, et al. Fluorescence-guided cancer surgery-a new paradigm. J Surg Oncol. (2021 May) 123(8):1679–98. doi: 10.1002/jso.26469
14. Cornella KN, Repper DC, Palafox BA, Razavi MK, Loh CT, Markle KM, et al. A surgeon’s fuide for various lung nodule localization techniques and the newest technologies. Innovations. (2021 Jan–Feb) 16(1):26–33. doi: 10.1177/1556984520966999
15. Wicky S, Mayor B, Cuttat JF, Schnyder P. CT-guided localizations of pulmonary nodules with methylene blue injections for thoracoscopic resections. Chest. (1994 Nov) 106(5):1326–8. doi: 10.1378/chest.106.5.1326
16. Lenglinger FX, Schwarz CD, Artmann W. Localization of pulmonary nodules before thoracoscopic surgery: value of percutaneous staining with methylene blue. AJR Am J Roentgenol. (1994 Aug) 163(2):297–300. doi: 10.2214/ajr.163.2.7518642
17. Vandoni RE, Cuttat JF, Wicky S, Suter M. CT-guided methylene-blue labelling before thoracoscopic resection of pulmonary nodules. Eur J Cardiothorac Surg. (1998 Sep) 14(3):265–70. doi: 10.1016/s1010-7940(98)00160-2
18. Shentu Y, Zhang L, Gu H, Mao F, Cai M, Ding Z, et al. A new technique combining virtual simulation and methylene blue staining for the localization of small peripheral pulmonary lesions. BMC Cancer. (2014 Feb 11) 14:79. doi: 10.1186/1471-2407-14-79
19. Stephenson JA, Mahfouz A, Rathinam S, Nakas A, Bajaj A. A simple and safe technique for CT guided lung nodule marking prior to video assisted thoracoscopic surgical resection revisited. Lung Cancer Int. (2015) 2015:235720. doi: 10.1155/2015/235720
20. Kleedehn M, Kim DH, Lee FT, Lubner MG, Robbins JB, Ziemlewicz TJ, et al. Preoperative pulmonary nodule localization: a comparison of methylene blue and Hookwire techniques. AJR Am J Roentgenol. (2016 Dec) 207(6):1334–39. doi: 10.2214/AJR.16.16272
21. Marino KA, Sullivan JL, Weksler B. Electromagnetic navigation bronchoscopy for identifying lung nodules for thoracoscopic resection. Ann Thorac Surg. (2016 Aug) 102(2):454–7. doi: 10.1016/j.athoracsur.2016.03.010
22. Liu Z, Yang R, Shao F, Pan Y. Localization of small peripheral pulmonary lesion by methylene blue injection with radial endobronchial ultrasonography in sublobar resection. Ann Thorac Surg. (2016 Feb) 101(2):e57–9. doi: 10.1016/j.athoracsur.2015.09.091
23. Findik G, Demiröz SM, Apaydın SMK, Ertürk H, Biri S, Incekara F, et al. Computed tomography-guided methylene blue labeling prior to thoracoscopic resection of small deeply placed pulmonary nodules. Do we really need palpation? Thorac Cardiovasc Surg. (2017 Aug) 65(5):387–91. doi: 10.1055/s-0036-1598019
24. Luo K, Lin Y, Lin X, Yu X, Wen J, Xi K, et al. Localization of peripheral pulmonary lesions to aid surgical resection: a novel approach for electromagnetic navigation bronchoscopic dye marking. Eur J Cardiothorac Surg. (2017 Sep 1) 52(3):516–21. doi: 10.1093/ejcts/ezx114
25. Pupovac SS, Chaudhry A, Singh VA. Benefits of electromagnetic navigational bronchoscopy for identifying pulmonary nodules for robotic resections. Innovations. (2017 Nov/Dec) 12(6):418–20. doi: 10.1097/IMI.0000000000000440
26. Muñoz-Largacha JA, Ebright MI, Litle VR, Fernando HC. Electromagnetic navigational bronchoscopy with dye marking for identification of small peripheral lung nodules during minimally invasive surgical resection. J Thorac Dis. (2017 Mar) 9(3):802–808. doi: 10.21037/jtd.2017.03.18
27. Lachkar S, Baste JM, Thiberville L, Peillon C, Rinieri P, Piton N, et al. Pleural dye marking using radial endobronchial ultrasound and virtual bronchoscopy before sublobar pulmonary resection for small peripheral nodules. Respiration. (2018) 95(5):354–61. doi: 10.1159/000486205
28. Long J, Petrov R, Haithcock B, Chambers D, Belanger A, Burks AC, et al. Electromagnetic transthoracic nodule localization for minimally invasive pulmonary resection. Ann Thorac Surg. (2019 Nov) 108(5):1528–34. doi: 10.1016/j.athoracsur.2019.04.107
29. Zhang WH, Bai YY, Guo W, Li M, Chang GX, Liu W, et al. Application of intrapulmonary wire combined with intrapleural fibrin glue in preoperative localization of small pulmonary nodules. Medicine. (2019 Jan) 98(4):e14029. doi: 10.1097/MD.0000000000014029
30. Qian K, Deng Y, Shen C, Feng YG, Deng B, Tan QY. Combination of electromagnetic navigation bronchoscopy-guided biopsy with a novel staining for peripheral pulmonary lesions. World J Surg Oncol. (2019 Sep 10) 17(1):158. doi: 10.1186/s12957-019-1704-7
31. Aoun HD, Littrup PJ, Heath KE, Adam B, Prus M, Beydoun R, et al. Methylene blue/collagen mixture for CT-guided presurgical lung nodule marking: high efficacy and safety. J Vasc Interv Radiol. (2020 Oct) 31(10):1682.e1–1682.e7. doi: 10.1016/j.jvir.2020.04.028
32. Zhang ZD, Wang HL, Liu XY, Xia FF, Fu YF. Methylene blue versus coil-based computed tomography-guided localization of lung nodules. Thorac Cardiovasc Surg. (2020 Sep) 68(6):540–4. doi: 10.1055/s-0040-1708836
33. Jiang T, Lin M, Zhao M, Zhan C, Li M, Feng M, et al. Preoperative computed tomography-guided localization for pulmonary nodules with glue and dye. Thorac Cardiovasc Surg. (2020 Sep) 68(6):525–32. doi: 10.1055/s-0039-3400999
34. Wang J, Gao LB, Zhang H, Wang J, Liu L, Shi WY. Preresection stained glue injection to localize pulmonary small nodules and ground-glass opacities. J Thorac Imaging. (2020 Jul) 35(4):260–64. doi: 10.1097/RTI.0000000000000479
35. Sun S, Liu K, Gao X, Ren B, Sun L, Xu L. Application of modified tailed microcoil in preoperative localization of small pulmonary nodules: a retrospective study. Thorac Cardiovasc Surg. (2020 Sep) 68(6):533–9. doi: 10.1055/s-0040-1708471
36. Lin CY, Chang CC, Huang LT, Chung TJ, Liu YS, Yen YT, et al. Computed tomography-guided methylene blue localization: single vs. multiple lung nodules. Front Med. (2021 Apr 14) 8:661956. doi: 10.3389/fmed.2021.661956
37. Sun SH, Gao J, Zeng XM, Zhang YF. Computed tomography-guided localization for lung nodules: methylene-blue versus coil localization. Minim Invasive Ther Allied Technol. (2021 Aug) 30(4):215–20. doi: 10.1080/13645706.2020.1725579
38. Mariolo AV, Vieira T, Stern JB, Perrot L, Caliandro R, Escande R, et al. Electromagnetic navigation bronchoscopy localization of lung nodules for thoracoscopic resection. J Thorac Dis. (2021 Jul) 13(7):4371–7. doi: 10.21037/jtd-21-223
39. Ujiie H, Kato T, Hu HP, Patel P, Wada H, Fujino K, et al. A novel minimally invasive near-infrared thoracoscopic localization technique of small pulmonary nodules: a phase I feasibility trial. J Thorac Cardiovasc Surg. (2017 Aug) 154(2):702–11. doi: 10.1016/j.jtcvs.2017.03.140
40. Hachey KJ, Digesu CS, Armstrong KW, Gilmore DM, Khullar OV, Whang B, et al. A novel technique for tumor localization and targeted lymphatic mapping in early-stage lung cancer. J Thorac Cardiovasc Surg. (2017 Sep) 154(3):1110–18. doi: 10.1016/j.jtcvs.2016.12.058
41. Wen CT, Liu YY, Fang HY, Hsieh MJ, Chao YK. Image-guided video-assisted thoracoscopic small lung tumor resection using near-infrared marking. Surg Endosc. (2018 Nov) 32(11):4673–80. doi: 10.1007/s00464-018-6252-7
42. Anayama T, Hirohashi K, Miyazaki R, Okada H, Kawamoto N, Yamamoto M, et al. Near-infrared dye marking for thoracoscopic resection of small-sized pulmonary nodules: comparison of percutaneous and bronchoscopic injection techniques. J Cardiothorac Surg. (2018 Jan 12) 13(1):5. doi: 10.1186/s13019-018-0697-6
43. Nagai K, Kuriyama K, Inoue A, Yoshida Y, Takami K. Computed tomography-guided preoperative localization of small lung nodules with indocyanine green. Acta Radiol. (2018 Jul) 59(7):830–5. doi: 10.1177/0284185117733507
44. Zhang C, Lin H, Fu R, Zhang T, Nie Q, Dong S, et al. Application of indocyanine green fluorescence for precision sublobar resection. Thorac Cancer. (2019 Apr) 10(4):624–30. doi: 10.1111/1759-7714.12972
45. Zhong L, Hu W, Li S, Wei Z, Zhu Z, Jin G, et al. Clinical study of video-assisted thoracoscopic surgery wedge resection in early-stage lung cancer by tumor mapping with indocyanine green. Wideochir Inne Tech Maloinwazyjne. (2019 Dec) 14(4):545–50. doi: 10.5114/wiitm.2019.89986
46. Geraci TC, Ferrari-Light D, Kent A, Michaud G, Zervos M, Pass HI, et al. Technique, outcomes with navigational bronchoscopy using indocyanine green for robotic segmentectomy. Ann Thorac Surg. (2019 Aug) 108(2):363–9. doi: 10.1016/j.athoracsur.2019.03.032
47. Chao YK, Leow OQY, Wen CT, Fang HY. Image-guided thoracoscopic lung resection using a dual-marker localization technique in a hybrid operating room. Surg Endosc. (2019 Nov) 33(11):3858–63. doi: 10.1007/s00464-019-06883-y
48. Kim Y, Rho J, Quan YH, Choi BH, Han KN, Kim HK, et al. Simultaneous visualization of pulmonary nodules and intersegmental planes on fluorescent images in pulmonary segmentectomy. Eur J Cardiothorac Surg. (2020 Aug 1) 58(Suppl_1):i77–i84. doi: 10.1093/ejcts/ezaa064
49. Li A, Chan S, Thung KH. Pre-operative CT localization for patients with subsolid opacities expecting video-assisted thoracoscopic surgery-single center experience of fluorescent iodized emulsion and hook-wire localization technique. Br J Radiol. (2020 May 1) 93(1109):20190938. doi: 10.1259/bjr.20190938
50. Hsu PK, Lee YY, Chuang LC, Ting CK, Tsou MY. Nonintubated versus intubated “one-stage” preoperative localization and thoracoscopic lung resection. JTCVS Tech. (2021 Sep 21) 10:517–25. doi: 10.1016/j.xjtc.2021.09.032
51. Yang YL, Li ZZ, Huang WC, Zhuang J, Lin DY, Zhong WZ, et al. Electromagnetic navigation bronchoscopic localization versus percutaneous CT-guided localization for thoracoscopic resection of small pulmonary nodules. Thorac Cancer. (2021 Feb) 12(4):468–74. doi: 10.1111/1759-7714.13775
52. Sekine Y, Koh E, Hoshino H. The efficacy of transbronchial indocyanine green instillation for fluorescent-guided wedge resection. Interact Cardiovasc Thorac Surg. (2021 Jun 28) 33(1):51–59. doi: 10.1093/icvts/ivab054
53. Zhang J, He J, Chen J, Zhong Y, He J, Li S. Application of indocyanine green injection guided by electromagnetic navigation bronchoscopy in localization of pulmonary nodules. Transl Lung Cancer Res. (2021 Dec) 10(12):4414–22. doi: 10.21037/tlcr-21-699
54. Li X, Xu K, Cen R, Deng J, Hao Z, Liu J, et al. Preoperative computer tomography-guided indocyanine green injection is associated with successful localization of small pulmonary nodules. Transl Lung Cancer Res. (2021 May) 10(5):2229–36. doi: 10.21037/tlcr-21-425
55. Wu Z, Zhang L, Zhao XT, Zhou D, Yang XY. Localization of subcentimeter pulmonary nodules using an indocyanine green near-infrared imaging system during uniportal video-assisted thoracoscopic surgery. J Cardiothorac Surg. (2021 Aug 6) 16(1):224. doi: 10.1186/s13019-021-01603-x
56. Ding N, Wang K, Cao J, Hu G, Wang Z, Jin Z. Targeted near-infrared fluorescence imaging with iodized indocyanine green in preoperative pulmonary localization: comparative efficacy, safety, patient perception with hook-wire localization. Front Oncol. (2021 Oct 27) 11:707425. doi: 10.3389/fonc.2021.707425
57. Choi BG, Kim HH, Kim BS, Kim KT, Shinn KS, Moon SW. Pulmonary nodules: CT-guided contrast material localization for thoracoscopic resection. Radiology. (1998 Aug) 208(2):399–401. doi: 10.1148/radiology.208.2.9680566
58. Endo M, Kotani Y, Satouchi M, Takada Y, Sakamoto T, Tsubota N, et al. CT fluoroscopy-guided bronchoscopic dye marking for resection of small peripheral pulmonary nodules. Chest. (2004 May) 125(5):1747–52. doi: 10.1378/chest.125.5.1747
59. Sato M, Omasa M, Chen F, Sato T, Sonobe M, Bando T, et al. Use of virtual assisted lung mapping (VAL-MAP), a bronchoscopic multispot dye-marking technique using virtual images, for precise navigation of thoracoscopic sublobar lung resection. J Thorac Cardiovasc Surg. (2014 Jun) 147(6):1813–9. doi: 10.1016/j.jtcvs.2013.11.046
60. Sato M, Kobayashi M, Kojima F, Tanaka F, Yanagiya M, Kosaka S, et al. Effect of virtual-assisted lung mapping in acquisition of surgical margins in sublobar lung resection. J Thorac Cardiovasc Surg. (2018 Oct) 156(4):1691–1701.e5. doi: 10.1016/j.jtcvs.2018.05.122
61. Shimamura Y, Sasaki S, Shimohira M, Ogino H, Yuki D, Nakamae K, et al. New technique of percutaneous CT fluoroscopy-guided marking before video-assisted thoracoscopic surgery for small lung lesions: feasibility of using a 25-gauge needle without local anaesthesia. Br J Radiol. (2018 Feb) 91(1083):20170692. doi: 10.1259/bjr.20170692
62. Hasegawa T, Kuroda H, Sato Y, Matsuo K, Sakata S, Yashiro H, et al. The utility of indigo carmine and lipiodol mixture for preoperative pulmonary nodule localization before video-assisted thoracic surgery. J Vasc Interv Radiol. (2019 Mar) 30(3):446–52. doi: 10.1016/j.jvir.2018.08.024
63. Piao Z, Han SJ, Cho HJ, Kang MW. Feasibility of electromagnetic navigation bronchoscopy-guided lung resection for pulmonary ground-glass opacity nodules. J Thorac Dis. (2020 May) 12(5):2467–73. doi: 10.21037/jtd.2020.03.71
64. Jeong JH, Park H, Choi CM, Oh JH, Lee GD, Kim DK, et al. Preoperative electromagnetic navigation bronchoscopy-guided one-stage multiple-dye localization for resection of subsolid nodules: A single-center pilot study. Thorac Cancer. (2022 Feb) 13(3):466–73. doi: 10.1111/1759-7714.14283
65. Krimsky WS, Minnich DJ, Cattaneo SM, Sarkar SA, Harley DP, Finley DJ, et al. Thoracoscopic detection of occult indeterminate pulmonary nodules using bronchoscopic pleural dye marking. J Community Hosp Intern Med Perspect. (2014) 4:23084. doi: 10.3402/jchimp.v4.23084
66. Abbas A, Kadakia S, Ambur V, Muro K, Kaiser L. Intraoperative electromagnetic navigational bronchoscopic localization of small, deep, or subsolid pulmonary nodules. J Thorac Cardiovasc Surg. (2017 Jun) 153(6):1581–90. doi: 10.1016/j.jtcvs.2016.12.044
67. Yang SM, Yu KL, Lin KH, Liu YL, Sun SE, Meng LH, et al. Real-time augmented fluoroscopy-guided lung marking for thoracoscopic resection of small pulmonary nodules. Surg Endosc. (2020 Jan) 34(1):477–84. doi: 10.1007/s00464-019-06972-y
68. Wang LL, He BF, Cui JH, Gao XL, Chen PP, Zhong WZ, et al. Electromagnetic navigational bronchoscopy-directed dye marking for locating pulmonary nodules. Postgrad Med J. (2020 Nov) 96(1141):674–9. doi: 10.1136/postgradmedj-2019-137083
69. Tokuno J, Chen-Yoshikawa TF, Nakajima D, Aoyama A, Motoyama H, Sato M, et al. Improved visualization of virtual-assisted lung mapping by indocyanine green. JTCVS Tech. (2021 Aug 8) 10:542–9. doi: 10.1016/j.xjtc.2021.07.019
70. Van Manen L, Handgraaf HJM, Diana M, Dijkstra J, Ishizawa T, Vahrmeijer AL, et al. A practical guide for the use of indocyanine green and methylene blue in fluorescence-guided abdominal surgery. J Surg Oncol. (2018) 118(2):283–300. doi: 10.1002/jso.25105
71. Cwalinski T, Polom W, Marano L, Roviello G, D'Angelo A, Cwalina N, et al. Methylene blue—current knowledge, fluorescent properties, and its future use. J Clin Med. (2020) 29(11):3538. doi: 10.3390/jcm9113538
72. Nomori H, Horio H. Colored collagen is a long-lasting point marker for small pulmonary nodules in thoracoscopic operations. Ann Thorac Surg. (1996 Apr) 61(4):1070–3. doi: 10.1016/0003-4975(96)00024-0
Keywords: NSCLC, NIR-guided surgery, minimally invasive thoracic surgery, RATS, VATS, lung cancer
Citation: Tajè R, Gallina FT, Forcella D, Vallati GE, Cappelli F, Pierconti F, Visca P, Melis E and Facciolo F (2022) Fluorescence-guided lung nodule identification during minimally invasive lung resections. Front. Surg. 9:943829. doi: 10.3389/fsurg.2022.943829
Received: 14 May 2022; Accepted: 24 June 2022;
Published: 18 July 2022.
Edited by:
Mong-Wei Lin, National Taiwan University Hospital, TaiwanReviewed by:
Savvas Lampridis, Guy's and St Thomas’ NHS Foundation Trust, United Kingdom© 2022 Tajè, Gallina, Forcella, Vallati, Cappelli, Pierconti, Visca, Melis and Facciolo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Filippo Tommaso Gallina ZmlsaXBwb2dhbGxpbmE5MkBnbWFpbC5jb20=
†These authors have contributed equally to this work.
Specialty Section: This article was submitted to Thoracic Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.