
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 20 September 2022
Sec. Neurosurgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.942755
This article is part of the Research TopicPeripheral Nerve Surgery: Neurosurgery beyond technologyView all 10 articles
 Lukas Rasulić1,2*
Lukas Rasulić1,2* Slavko Đjurašković3
Slavko Đjurašković3 Novak Lakićević3
Novak Lakićević3 Milan Lepić4
Milan Lepić4 Andrija Savić1,2
Andrija Savić1,2 Jovan Grujić1,2
Jovan Grujić1,2 Aleksa Mićić1Stefan Radojević1María Elena Córdoba-Mosqueda5
Aleksa Mićić1Stefan Radojević1María Elena Córdoba-Mosqueda5 Jacopo Visani6Vladimir Puzović7Vojin Kovačević8,9Filip Vitošević10Stefan Mandić-Rajčević11Saša Knezevic12
Jacopo Visani6Vladimir Puzović7Vojin Kovačević8,9Filip Vitošević10Stefan Mandić-Rajčević11Saša Knezevic12
Introduction: Radial nerve lesions present a clinical entity that may lead to disability, psychological distress, and job loss, and thus requires great attention. Knowledge of the etiology and exact mechanism of the nerve impairment is of great importance for appropriate management of these patients, and there are only a few papers that focused on these features in patients with surgically treated radial nerve lesions. The lack of studies presenting the etiology and injury mechanisms of surgically treated radial nerve lesions may be due to a relatively small number of specialized referral centers, dispersion to low-flow centers, and a greater focus on the surgical treatment outcomes.
Aim: The aim of this study was to describe the etiological and epidemiological characteristics of patients with surgically treated radial nerve lesions of various origins.
Methods: This retrospective study evaluated 147 consecutive patients with radial nerve lesion, treated in the department during the last 20 years, from January 1, 2001, until December 31, 2020.
Results: The majority of patients belonged to the working population, and 70.1% of them were male. Most commonly, the etiology of nerve lesion was trauma (63.3%) or iatrogenic injury (28.6%), while the less common origin was idiopathic (4.1%) or neoplastic (4.1%). The most frequent location of the lesion was in the upper arm, followed by the elbow and forearm. Fracture-related contusion was the most common mechanism (29.9%), followed by postoperative fibrosis (17.7%), lacerations (17.7%), and compression (15.6%).
Conclusion: Based on the fact that traumatic or iatrogenic injuries constitute the majority of cases, with their relevant mechanisms and upper arm predomination, it is crucial to raise awareness and understanding of the radial nerve injuries among orthopedic surgeons to decrease the numbers of these patients and properly preserve or treat them within the initial surgery.
Radial nerve lesions present a clinical entity that may lead to functional loss (1), disability (2), psychological distress (3), and job loss (4) and should be, therefore, recognized as a significant socioeconomic problem (5, 6). Knowledge of the etiology and exact mechanism of the nerve impairment is of great importance for appropriate management of these patients (7), and there are only a few papers that focused on these features in patients with surgically treated radial nerve lesions (8, 9).
While many of the posture or compression-related radial nerve palsies may recover spontaneously, as do some of the contusion lesions associated with bone fractures (10, 11), radial nerve lesions demanding surgery are most commonly caused by trauma (8, 12), unlike lesions of the median and ulnar nerve, whose origin is most often idiopathic entrapment (13). While the frequency of iatrogenic radial nerve lesions referred for surgery is similar to that of other major nerves of the arm (14), neoplastic lesions are rare and account only for a small portion of all peripheral nerve tumors (15).
The radial is the deep seated nerve, adjacent to the bones and frequently subjected to fracture-related contusion (8, 16) or laceration (16–18), by the rule a consequence of humeral shaft fracture in the upper arm (8, 19), while the lesions of the trunk or its main branches in the distal parts of the arm are mostly associated with the elbow, radius, and ulna fractures (8). Less frequently, the nerve may be compressed, contused, lacerated, or cut without an associated bone fracture (8, 9, 20–23).
Because of its frequent association with humeral shaft fracture (24), the majority of studies concerning radial nerve lesions have focused on patients with this associated fracture (10, 16–18, 20, 25). The lack of studies presenting the etiology and injury mechanisms of surgically treated radial nerve lesions may also be due to a relatively small number of specialized referral centers, dispersion to low-flow centers, and a greater focus on the surgical treatment (26).
The aim of this study was to describe the etiological and epidemiological characteristics of patients with surgically treated radial nerve lesions of various origins in a single-center during a 20-year period.
This is a retrospective study that included 147 consecutive patients with radial nerve lesion treated at the Department for Peripheral Nerve Surgery, Functional Neurosurgery and Pain Management Surgery, Clinic for Neurosurgery, University Clinical Center of Serbia, in Belgrade, Serbia, in a 20-year period from January 1, 2001, to December 31, 2020.
The patients with radial nerve lesions were included in the study according to the following criteria:
• Patients with ultrasonography and electromyoneurography verified radial nerve lesion referred for surgery and treated during the study period.
• Radial nerve lesion located in the upper arm, elbow, or forearm region.
• Lesion of the radial nerve main branches (deep-motor and superficial-sensitive).
• Posterior interosseous nerve (PIN) lesion.
• Superficial sensory radial nerve (SSRN) lesion.
• Patients with radial nerve lesion undergoing conservative treatment.
• Radial nerve lesion in the infraclavicular region, as the part of brachial plexus injury.
All data in the study were obtained by reviewing patients’ hospital records and follow-up examinations. We collected data on age (<25, 26–50, 51–75), gender (male/female), whether belonging to the working-age population (27), area of residence (urban/rural), tobacco smoking (yes/no), associated diseases, etiology of nerve lesion (traumatic/iatrogenic/neoplastic/idiopathic), and mechanism of nerve injury. In addition, for patients with traumatic injuries, we noted the energy of the trauma (high-energy/low-energy), associated injuries, and nerve continuity (preserved/disrupted).
All statistical procedures were performed with SPSS v26.0 software package (IBM Corporation, Armonk, NY, USA). For descriptions of the parameters of interest, we used the methods of descriptive statistics: mean, median, range, absolute (N), and relative (%) frequencies. The normality of data was assessed using the Shapiro–Wilk test. The association between patients’ groups was analyzed using the Chi-square test with a 95% confidence interval, and statistical significance set at p < 0.05.
Out of all studied patients, 104 (70.7%) were male and 43 (29.3%) were female. The patients' age ranged from 12 to 75 years, and the mean age of the population was 38.2 ± 15.3. Two-thirds of the male patients −69 (66.3%) were younger than 40 years (mean age = 35.4), while female patients had more even distribution, counting 24 (55.8%) older than 40 (mean age = 45.1). All patients aged under 18 years were males (12, 14, and 16 years old). The youngest female patient was aged 18, while the oldest male and female patients were aged 72 and 75, respectively.
The majority of studied patients—137 (93.20%)—belonged to the working-age population, and there was a statistically significant difference in the male to female ratio regarding the analyzed age groups: the majority of male patients belonged to the group aged 0–25 years (87.1%), while the most of the women were aged 26–50 years (75.6%). Slightly more than a half of the patients—79 (53.7%)—lived in urban places, while 68 (46.3%) lived in rural places. Comorbidities were present in 43 (29.2%), and 61 (41.5%) patients were tobacco smokers before and at the time of surgery (Table 1).
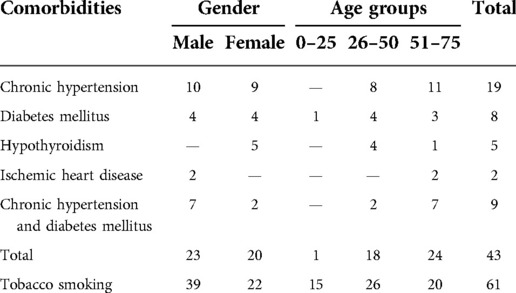
Table 1. Patient distribution with reference to comorbidities and tobacco smoking within gender and age groups.
The most common location of the nerve lesion was in the upper arm −110 (74.8%), followed by the elbow −24 (16.3%) and forearm −13 (8.8%). Almost all elbow injuries—21 (87.5%)—involved the radial nerve trunk, while only 2 involved both radial nerve main branches. The majority of forearm nerve lesions—11 (84.6%)—involved PIN, while only 2 (15.4%) involved SSRN. The mechanisms of nerve injury at different locations in the upper extremity are presented in Figure 1.
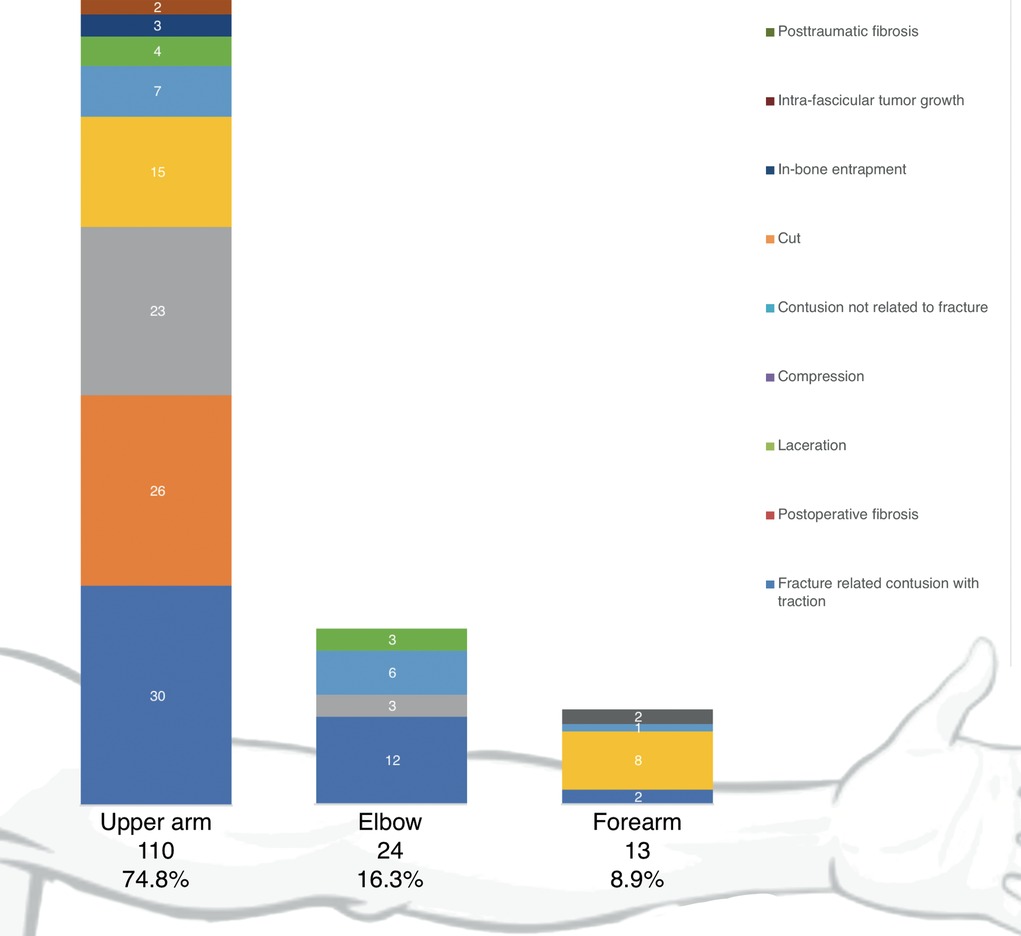
Figure 1. Distribution of the patients with reference to location and mechanism of nerve injury.
Out of all studied patients, 100 (68.0%) had preserved, while 47 (32.0%) had disrupted nerve continuity (complete vs. partial disruption = 46:1).
Out of the total 147 patients, the majority (129) were trauma patients. Nerve injury in these occurred due to the trauma in 93 (72.1%) patients, while 36 (24.5%) developed iatrogenic nerve injury. The remaining six iatrogenic injuries occurred in nontraumatized patients. Neoplastic and idiopathic nerve lesions involved six patients each (Table 2).
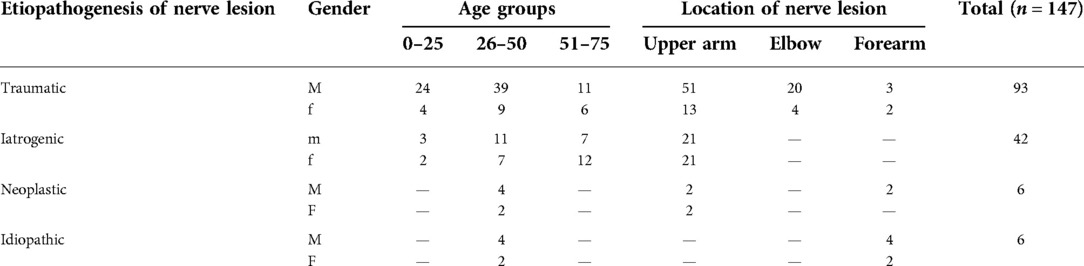
Table 2. Distribution of the patients with reference to etiology, among gender, age groups, and location of the nerve lesion.
Most of the studied patients—129 (87.7%)—developed nerve lesion due to trauma (high-energy vs. low-energy trauma = 71:58). Males were more commonly injured during road traffic accidents [31 (77.5%)], occupational accidents [27 (87.1%)], and physical confrontation [8 (100%)], while more than a half of the females [20 (54.0%)] were injured during fall from the standing position. Table 3 presents further details on the cause of trauma.

Table 3. Cause of trauma, age, and gender distribution in 129 traumatized patients.
Excluding the radial nerve injury, most of the traumatized patients [110 (85.3%)] had other associated injuries (Table 4), the majority of which [79 (71.9%)] had a humeral shaft fracture.

Table 4. Location of nerve lesion and other associated injuries.
Table 5 reviews the causes and mechanisms of traumatic nerve injuries. The most common cause were road traffic accidents −27 (29.0%), occupational accidents −26 (28.0%) and falls from the standing position −20 (21.5%). The most common mechanisms of nerve injury were fracture related contusion −44 (47.3%) and laceration −18 (19.3%). The majority of fracture related contusions −30 (68.2%) were a consequence of humeral shaft fracture, as well as 13 (72.2%) lacerations, and 2 (28.6%) cuts. The elbow fractures resulted in 7 (15.9%) contusions and 1 laceration, while radius and/or ulna fractures resulted in 7 (15.9%) contusions and 2 lacerations. The 14 contusions, 5 cuts, and 2 lacerations, without an associated fracture, were a consequence blunt trauma or injury by a sharp object. Two injuries by a sharp object resulted in posttraumatic fibrosis, while all compression injuries occurred due to bad posture during sleep (Saturday night palsy).
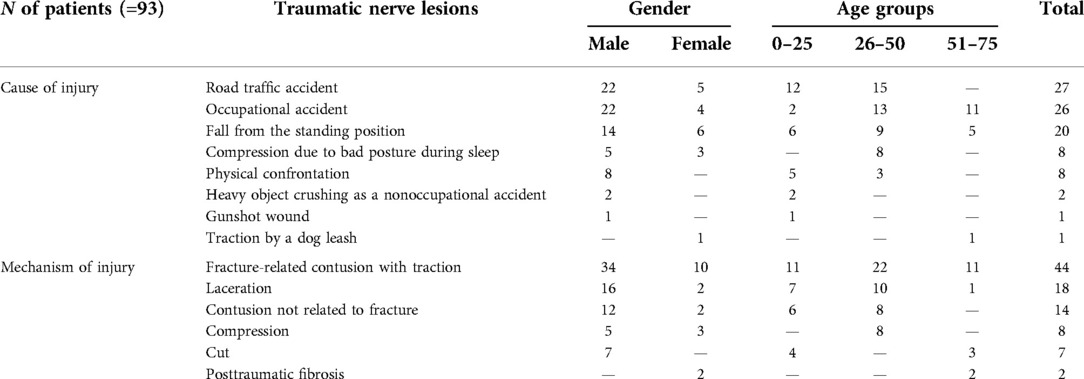
Table 5. Causes and mechanisms of traumatic radial nerve injuries.
Table 6 reviews the causes and mechanisms of iatrogenic nerve injuries. The most common cause was open reduction and internal fixation (ORIF) of the humeral shaft [29 (69.0%)]. The most common mechanism of nerve injury associated with ORIF was postoperative fibrosis [20 (69.0%)], while the less common were nerve entrapment between the bone fragments [3 (10.3%)], nerve compression by a plate [3 (10.3%)], and nerve laceration [3 (10.3%)]. The osteosynthesis material removal led to nerve laceration in five patients. All cases of tumor resection (six) resulted in postoperative fibrosis. In two cases, repositioning under general anesthesia led to the compression injury.
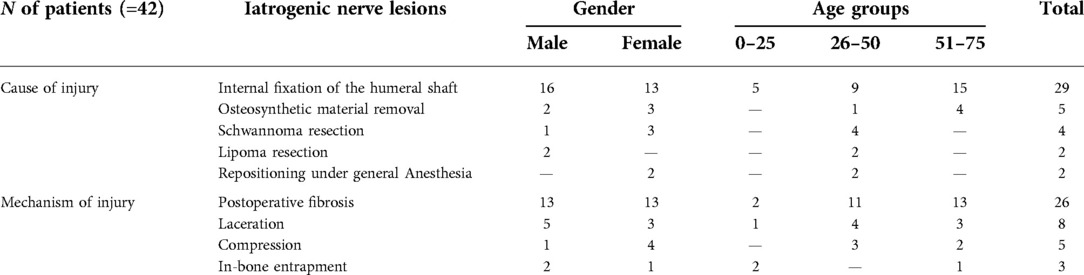
Table 6. Causes and mechanisms of iatrogenic radial nerve injuries.
All patients with neoplastic etiology of the nerve lesion (male vs. female = 4:2) had benign peripheral nerve sheath tumor (PNST), out of whom three had schwannoma (arising from the sensory fibers), two had neurofibroma (arising from the motor fibers), and one had a hybrid tumor with neurofibroma capsule and schwannoma tissue (arising from the sensory fibers). All but two schwannomas in the forearm region originating from the SSRN were located in the upper arm region.
All patients with idiopathic etiology of the nerve lesion (male vs. female −4:2) had PIN entrapment syndrome due to the nerve compression at the supinator muscle arch—the arcade of Frohse.
For more than 40 years, our department is dedicated to the surgery of peripheral nerves. In the last 20 years, we surgically treated 147 patients with radial nerve lesion, which is a remarkable number of cases. The Department for Peripheral Nerve Surgery, Functional Neurosurgery, and Pain Management Surgery at the Clinic for Neurosurgery, Clinical Center of Serbia in Belgrade, Serbia, is a referral center for peripheral nerve injuries and diseases, serving the approximate population of 7 million people of Serbia (28), where every patient in the need for nerve surgery should be automatically referred, as well as the complex patients from the former Yugoslavia region. The present study is the largest in Europe and one of the largest published series on the surgical treatment of radial nerve lesions worldwide (8, 19).
Based on our experience, surgical treatment of radial nerve lesions demands the surgeon to meticulously analyze all aspects of the injury and be aware of the relevant surgical treatment options (17, 29, 30). Detailed insight into etiological and epidemiological characteristics (age, working-age, gender, mechanism, location, extent of an injury, etc.) lead to the clear and more accurate prognosis and recovery expectations. This allows us to achieve best possible outcomes and also to avoid additional surgeries, which may compromise the recovery or even lead to severe consequences.
According to the published literature (26, 31–37), the patients referred for peripheral nerve surgery usually belong to the working population, and majority of them are male. This has also been shown in a study of surgically treated radial nerve lesions in general (38) as well as a study of surgically treated radial nerve lesions associated with humeral shaft fractures (17). The results of our study are in accordance with the results of aforementioned studies.
Regarding some studies (39–49), gender of the patients may be associated with the cause of trauma, which is in line with the results of our study. Most of our patients injured during road traffic accidents, occupational accidents, and fights were males, while most of those who fell were females. These results may be explained by a greater chance for male population to participate in traffic (41–44), fights (48, 49), or work with heavy machines and objects (45, 46), unlike the females, which make them prone to these accidents. On the other hand, the lower body strength of females, in general, may be the reason why they suffer severe injuries in low/energy trauma (50).
Most of the patients in our study were traumatized, and the most common etiology of the nerve lesion was traumatic. These results are in accordance with the results of studies concerning surgically treated radial nerve lesions in general (8, 9), as well as radial nerve lesions associated with humeral shaft fracture (17).
The distribution of mechanisms of traumatic nerve injuries referred for surgery mostly depend on the affected nerve and at what location in the extremity the damage occurred (8, 13, 37). The median and ulnar nerve are more superficial (51), and therefore more exposed to laceration and cutting (13, 37), while the radial nerve, which lays close to the bones, is usually subjected to fracture-related contusion (8, 16). The results of our study may be compared with that of the study by Kim et al. (8). A lower occurrence of our patients with gunshot wounds may be explained by the different firearms available in these two countries (52, 53), as well as the different global peace index (GPI) (54) and different shooting frequency during the study periods (55, 56).
The higher occurrence of iatrogenic nerve lesions in our study, comparing to the study of Kim et al. (8), may be due to different referral of patients in our country. Overall, patients with iatrogenic radial nerve lesions are commonly managed by the surgeons who performed the primary surgery (57). In our country, majority of iatrogenic nerve lesions referred for surgery are managed at our department (14).
Most of the iatrogenic nerve lesions in our study were a consequence of ORIF of the humeral shaft, which is in accordance with the published literature (14, 16, 58). The fact that iatrogenic nerve injuries are a common consequence of the extremity surgery (59) may explain why some of our patients acquired radial nerve lesion during resection of the tumor in the upper arm. The reported cases of iatrogenic radial nerve lesions due to repositioning under general anesthesia are described in the literature (60), and this happened in two of our patients during an emergency surgery. No injection injuries (8) and injuries due to blood pressure cap compression (7) were noted, probably due to the increased awareness of these injuries in the last few decades.
Idiopathic radial nerve lesions may occur due to the nerve entrapment at multiple sites in the upper extremity (7, 61, 62), out of which the most commonly described is at the supinator muscle arch, the arcade of Frohse, which is in accordance with our results. A lower occurrence of patients with radial nerve entrapment in our study, compared to the study of Kim et al., may be due to the low familiarity of treating physicians with this particular entity and a considerable part remaining underdiagnosed.
The most common PNST in the published literature are schwannoma and neurofibroma, usually occurring between the third and fifth decades of life, as solitary lesions, or within neurocutaneous syndromes (15). The schwannomas rarely involve intrafascicular growth of the tumor, unlike neurofibroma, which usually involves several fascicles (63). The results of our study concerning the age, frequency, and presence of infiltration are in accordance with the published literature.
The results of this study suggest that the etiology of radial nerve lesions demanding surgery is most often accidental, rather than health related, and the resources should be directed toward the prevention of such accidents (both traumatic and iatrogenic). Future studies should focus on all aspects of the lesion to better guide the management and potentially predict outcomes of surgical treatment.
The major limitations of this study are its retrospective nature and the involvement of only surgically treated patients. The former may also be the reason for somewhat later referral, as these patients initially seek help from their local medical care providers and get referred only after the definitive failure of conservative treatment. A decent amount of patients received surgical treatment in local centers, especially the iatrogenic cases; therefore, we lack some data that prevent us to analyze the whole patient population.
The etiology of radial nerve lesion is most often traumatic, and almost all patients belong to the male working-age population. Iatrogenic nerve injuries were frequent and most often a consequence of open reduction and internal fixation of the humeral shaft. The nerve lesions of neoplastic and idiopathic entrapment origin are less frequent in our population.
Based on the fact that traumatic or iatrogenic injuries constitute the majority of cases, with their relevant mechanisms and upper arm predomination, it is crucial to raise awareness and understanding of the radial nerve injuries among orthopedic surgeons to decrease the numbers of these patients and properly preserve or treat them within the initial surgery.
When occurred, the radial nerve lesions may be associated with significant functional and socioeconomic consequences and should be managed by experienced specialists.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of the Faculty of Medicine in Belgrade. The patients/participants provided their written informed consent to participate in this study.
All authors have significantly contributed to the manuscript, in design of the study, data gathering, statistical analysis, interpretation of results, and deriving conclusions. The final manuscript was revised by the two senior authors LR and NL, before submission. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ljungquist KL, Martineau P, Allan C. Radial nerve injuries. J Hand Surg Am. (2015) 40(1):166–72. doi: 10.1016/j.jhsa.2014.05.010
2. Novak CB, Anastakis DJ, Beaton DE, Mackinnon SE, Katz J. Biomedical and psychosocial factors associated with disability after peripheral nerve injury. J Bone Jt Surg. (2011) 93(10):929–36. doi: 10.2106/JBJS.J.00110
3. Miller C, Peek AL, Power D, Heneghan NR. Psychological consequences of traumatic upper limb peripheral nerve injury: a systematic review. Hand Ther. (2017) 22(1):35–45. doi: 10.1177/1758998316679387
4. Jaquet JB, Luijsterburg AJ, Kalmijn S, Kuypers PD, Hofman A, Hovius SE. Median, ulnar, and combined median-ulnar nerve injuries: functional outcome and return to productivity. J Trauma (2001) 51(4):687–92. doi: 10.1097/00005373-200110000-0001111586160
5. Rosberg HE, Carlsson KS, Dahlin LB. Prospective study of patients with injuries to the hand and forearm: costs, function, and general health. Scand J Plast Reconstr Surg Hand Surg. (2005) 39(6):360–9. doi: 10.1080/02844310500340046
6. Dias JJ, Garcia-Elias M. Hand injury costs. Injury. (2006) 37(11):1071–7. doi: 10.1016/j.injury.2006.07.023
7. Latef TJ, Bilal M, Vetter M, Iwanaga J, Oskouian RJ, Tubbs RS. Injury of the radial nerve in the arm: a review. Cureus. (2018) 10(2):e2199. doi: 10.7759/cureus.2199
8. Kim DH, Kam AC, Chandika P, Tiel RL, Kline DG. Surgical management and outcome in patients with radial nerve lesions. J Neurosurg. (2001) 95(4):573–83. doi: 10.3171/jns.2001.95.4.0573
9. Kallio PK, Vastamäki M, Solonen KA. The results of secondary microsurgical repair of radial nerve in 33 patients. J Hand Surg Eur Vol. (1993) 18(3):320–2. doi: 10.1016/0266-7681(93)90052-H
10. Belayneh R, Lott A, Haglin J, Konda S, Leucht P, Egol K. Final outcomes of radial nerve palsy associated with humeral shaft fracture and nonunion. J Orthop Traumatol. (2019) 20(1):18. doi: 10.1186/s10195-019-0526-2
11. Ekholm R, Ponzer S, Törnkvist H, Adami J, Tidermark J. Primary radial nerve palsy in patients with acute humeral shaft fractures. J Orthop Trauma. (2008) 22(6):408–14. doi: 10.1097/BOT.0b013e318177eb06
12. Bartels RHMA. History of the surgical treatment of ulnar nerve compression at the elbow. Neurosurgery. (2001) 49(2):391–9. doi: 10.1097/00006123-200108000-00023
13. Kim DH, Han K, Tiel RL, Murovic JA, Kline DG. Surgical outcomes of 654 ulnar nerve lesions. J Neurosurg. (2003) 98(5):993–1004. doi: 10.3171/jns.2003.98.5.0993
14. Rasulić L, Savić A, Vitošević F, Samardžić M, Živković B, Mićović M, et al. Iatrogenic peripheral nerve injuries—surgical treatment and outcome: 10 years’ experience. World Neurosurg. (2017) 103:841–51.e6. doi: 10.1016/j.wneu.2017.04.099
15. Reinhard F, Caroline D. Peripheral nerve sheath tumors of the upper extremity and hand in patients with neurofibromatosis type 1: topography of tumors and evaluation of surgical treatment in 62 patients. (2017) 6:Doc15. doi: 10.3205/iprs000117
16. Rasulić L, Samardzić M, Bascarević V, Jovanović M, Malis M, Nikolić V, et al. Current trends in surgical treatment of radial nerve injuries associated with injuries of the humerus. Acta Chir Iugosl. (2010) 57(1):77–80. doi: 10.2298/ACI1001077R
17. Rasulić L, Djurašković S, Lakićević N, Lepić M, Savić A, Grujić J, et al. Surgical treatment of radial nerve injuries associated with humeral shaft fracture—a single center experience. Front Surg. (2021) 8:774411. doi: 10.3389/fsurg.2021.774411
18. Samardžić M, Grujičić D, Milinković ZB. Radial nerve lesions associated with fractures of the humeral shaft. Injury. (1990) 21(4):220–2. doi: 10.1016/0020-1383(90)90006-G
19. Pan CH, Chuang DCC, Rodriguez-Lorenzo A. Outcomes of nerve reconstruction for radial nerve injuries based on the level of injury in 244 operative cases. J Hand Surg Eur Vol. (2010) 35(5):385–91. doi: 10.1177/1753193409360283
20. Nachef N, Bariatinsky V, Sulimovic S, Fontaine C, Chantelot C. Predictors of radial nerve palsy recovery in humeral shaft fractures: a retrospective review of 17 patients. Orthop Traumatol Surg Res. (2017) 103(2):177–82. doi: 10.1016/j.otsr.2016.10.023
21. Guo Y, Chiou-Tan FY. Radial nerve injuries from gunshot wounds and other trauma: comparison of electrodiagnostic findings. Am J Phys Med Rehabil. (2002) 81(3):207–11. doi: 10.1097/00002060-200203000-00009
22. Roganovic Z, Petkovic S, Carlstedt T, Mehta VS. Missile severances of the radial nerve. Results of 131 repairs. Acta Neurochir (Wien). (2004) 146(11):1185–92. doi: 10.1007/s00701-004-0361-x
23. Provencher MT, Allen LR, Gladden MJ, Shin AY. The underestimation of a glass injury to the hand. Am J Orthop (Belle Mead NJ). (2006) 35(2):91–4.16584084
24. Burnett MG, Zager EL. Pathophysiology of peripheral nerve injury: a brief review. Neurosurg Focus. (2004) 16(5):1–7. doi: 10.3171/foc.2004.16.5.2
25. Bishop J, Ring D. Management of radial nerve palsy associated with humeral shaft fracture: a decision analysis model. J Hand Surg Am. (2009) 34(6):991–6.e1. doi: 10.1016/j.jhsa.2008.12.029
26. Rasulić LG, Puzović V, Rotim K, Jovanović M, Samardžić M, Živković B, et al. The epidemiology of forearm nerve injuries—a retrospective study. Acta Clin Croat. (2015) 54(1):19–24.
27. Schmitt N, Schmitt J. Definition of public health. In: Kirch W. editor. Encyclopedia of Public Health. Springer: Dordrecht (2008).
28. Vukmirović D. Comparative Overview of the Number of Households 1948–2011 and Dwellings 1971–2011 (2014). Available from: https://publikacije.stat.gov.rs/G2014/PdfE/G201418096.pdf
29. Bertelli JA, Nehete S, Winkelmann Duarte EC, Ghizoni MF. Transfer of the distal anterior interosseous nerve for thumb motion reconstruction in radial nerve paralysis. J Hand Surg Am. (2020) 45(9):877.e1–e10. doi: 10.1016/j.jhsa.2020.02.011
30. Samardžić M, Rasulić L, Stanković L. Motor nerve transfers for restoration of upper arm function in adult brachial plexus injuries—basics, advantages, problems and strategies. Neurohirurgija Serbian J Neurosurg. (2021) 1(1):9–16. doi: 10.55005/sjns.v1i1.6
31. Kouyoumdjian JA. Peripheral nerve injuries: a retrospective survey of 456 cases. Muscle Nerve. (2006) 34(6):785–8. doi: 10.1002/mus.20624
32. Saadat S, Eslami V, Rahimi-Movaghar V. The incidence of peripheral nerve injury in trauma patients in Iran. Ulus Travma ve Acil Cerrahi Derg. (2011) 17(6):539–44. doi: 10.5505/tjtes.2011.75735
33. Kouyoumdjian JA, Graça CR, Ferreira VFM. Peripheral nerve injuries: a retrospective survey of 1124 cases. Neurol India. (2017) 65:551–5. doi: 10.4103/neuroindia.NI_987_16
34. Rasulić L, Savić A, Lepić M, Puzović V, Karaleić S, Kovačević V, et al. Epidemiological characteristics of surgically treated civilian traumatic brachial plexus injuries in Serbia. Acta Neurochir (Wien). (2018) 160(9):1837–45. doi: 10.1007/s00701-018-3640-7
35. Jain DKA, Bhardwaj P, Venkataramani H, Sabapathy SR, et al. An epidemiological study of traumatic brachial plexus injury patients treated at an Indian centre. Indian J Plast Surg. (2012) 45:498–503. doi: 10.4103/0970-0358.105960
36. Faglioni W, Siqueira MG, Martins RS, Heise CO, Foroni L. The epidemiology of adult traumatic brachial plexus lesions in a large metropolis. Acta Neurochir (Wien). (2014) 156(5):1025–8. doi: 10.1007/s00701-013-1948-x
37. Puzović V, Samardžić M, Jovanović M, Živković B, Savić A, Rasulić LG. Etiology and mechanisms of ulnar and median forearm nerve injuries. Vojnosanit Pregl. (2015) 72(11):961–7. doi: 10.2298/VSP140818106P
38. Terzis JK, Konofaos P. Radial nerve injuries and outcomes: our experience. Plast Reconstr Surg. (2011) 127(2):739–51. doi: 10.1097/PRS.0b013e3181fed7de
39. Boniface R, Museru L, Kiloloma O, Munthali V. Factors associated with road traffic injuries in Tanzania. Pan Afr Med J. (2016) 23:1–8. doi: 10.11604/pamj.2016.23.46.7487
40. Khan MH, Ahmed INZ. Road traffic accidents; study of risk factors. Prof Med J. (2007) 14(2):323–7.
41. Pešić D, Antić B, Smailović E, Marković N. Driving under the influence of alcohol and the effects of alcohol prohibition—case study in Serbia. Traffic Inj Prev. (2019) 20(5):467–71. doi: 10.1080/15389588.2019.1612058
42. Vranes AJ, Mikanovic VB, Lazovic JM, Kosanovic V. Road traffic safety as a public health problem: evidence from Serbia. J Transp Heal. (2018) 8:55–62. doi: 10.1016/j.jth.2017.12.005
43. Sârbescu P, Stanojević P, Jovanović D. A cross-cultural analysis of aggressive driving: evidence from Serbia and Romania. Transp Res Part F Traffic Psychol Behav. (2014) 24:210–7. doi: 10.1016/j.trf.2014.04.002
44. Santamariña-Rubio E, Pérez K, Olabarria M, Novoa AM. Gender differences in road traffic injury rate using time travelled as a measure of exposure. Accid Anal Prev. (2014) 65:1–7. doi: 10.1016/j.aap.2013.11.015
45. Islam SS, Velilla AM, Doyle EJ, Ducatman AM. Gender differences in work-related injury/illness: analysis of workers compensation claims. Am J Ind Med. (2001) 39(1):84–91. doi: 10.1002/1097-0274(200101)39:1%3C84::AID-AJIM8%3E3.0.CO;2-T
46. Åkerstedt T, Fredlund P, Gillberg M, Jansson B. A prospective study of fatal occupational accidents—relationship to sleeping difficulties and occupational factors. J Sleep Res. (2002) 11(1):69–71. doi: 10.1046/j.1365-2869.2002.00287.x
47. Samuel JC, Akinkuotu A, Villaveces A, Charles AG, Lee CN, Hoffman IF, et al. Epidemiology of injuries at a tertiary care center in Malawi. World J Surg. (2009) 33(9):1836–41. doi: 10.1007/s00268-009-0113-4
48. Golding P, Fitzgerald HE. The early biopsychosocial development of boys and the origins of violence in males. Infant Ment Health J. (2019) 40(1):5–22. doi: 10.1002/imhj.21753
49. Sousa S, Correia T, Ramos E, Fraga S, Barros H. Violence in adolescents: social and behavioural factors. Gac Sanit. (2010) 24(1):47–52. doi: 10.1016/j.gaceta.2009.08.002
50. Stevens JA, Sogolow ED. Gender differences for non-fatal unintentional fall related injuries among older adults. Inj Prev. (2005) 11(2):115–9. doi: 10.1136/ip.2004.005835
51. Jabaley ME, Wallace WH, Heckler FR. Internal topography of major nerves of the forearm and hand: a current view. J Hand Surg Am. (1980) 5(1):1–18. doi: 10.1016/S0363-5023(80)80035-9
52. Hemenway D, Miller M. Firearm availability and homicide rates across 26 high-income countries. J Trauma Inj Infect Crit Care. (2000) 49(6):985–8. doi: 10.1097/00005373-200012000-00001
53. Miller M, Azrael D, Hemenway D. Rates of household firearm ownership and homicide across US regions and states, 1988–1997. Am J Public Health. (2002) 92(12):1988–93. doi: 10.2105/AJPH.92.12.1988
54. Schippa C. The global peace index. In: International Place Branding Yearbook 2011. London: Palgrave Macmillan (2011), p. 112–29. doi: 10.1057/9780230343320_10
55. Airgun-related mortality and morbidity in the United States. Sydney School of Public Health. (2015). Available from: https://www.gunpolicy.org/firearms/region/united-states
56. Alpers P, Picard M, Mourlevat C. Guns in Serbia: Rate of All Gun Deaths per 100,000 People. Sydney School of Public Health, The University of Sydney (2021). Available from: https://www.gunpolicy.org/firearms/compareyears/159/rate_of_all_gun_deaths_per_100_000_people
57. Reichert P, Wnukiewicz W, Witkowski J, Bocheńska A, Mizia S, Gosk J, et al. Causes of secondary radial nerve palsy and results of treatment. Med Sci Monit. (2016) 22:554–62. doi: 10.12659/MSM.897170
58. Zhao JG, Wang J, Meng XH, Zeng XT, Kan SL. Surgical interventions to treat humerus shaft fractures: a network meta-analysis of randomized controlled trials. PLoS One. (2017) 12(3):1–12. doi: doi: 10.1371/journal.pone.0173634
59. Bumbasirevic M, Palibrk T, Lesic A, Atkinson HDE. Radial nerve palsy. EFORT Open Rev. (2016) 1(8):286–94. doi: 10.1302/2058-5241.1.000028
60. Tuncali BE, Tuncali B, Kuvaki B, Cinar O, Doǧan A, Elar Z. Radial nerve injury after general anaesthesia in the lateral decubitus position. Anaesthesia. (2005) 60(6):602–4. doi: 10.1111/j.1365-2044.2005.04177.x
61. Xiao TG, Cartwright MS. Ultrasound in the evaluation of radial neuropathies at the elbow. Front Neurol. (2019) 10:1–7. doi: doi: 10.3389/fneur.2019.00216
Keywords: radial nerve, etiology, epidemiology, mechanism of injury, surgery
Citation: Rasulić L, Đjurašković S, Lakićević N, Lepić M, Savić A, Grujić J, Mićić A, Radojević S, Córdoba-Mosqueda ME, Visani J, Puzović V, Kovačević V, Vitošević F, Mandić-Rajčević S and Knezevic S (2022) Etiological and epidemiological characteristics of surgically treated radial nerve lesions: A 20-year single-center experience. Front. Surg. 9:942755. doi: 10.3389/fsurg.2022.942755
Received: 12 May 2022; Accepted: 30 August 2022;
Published: 20 September 2022.
Edited by:
Ziya Levent Gokaslan, Brown University, United StatesReviewed by:
Karim Sarhane, Vanderbilt University, United States© 2022 Rasulić, Djuraskovic, Lakićević, Lepić, Savić, Grujić, Mićić, Radojevic, Cordoba Mosqueda, Visani, Puzovic, Kovačević, Vitošević, Mandic-Rajcevic and Knezevic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lukas Rasulić bHVrYXMucmFzdWxpY0BnbWFpbC5jb20=
Specialty Section: This article was submitted to Neurosurgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.