 Qiao Zhong
Qiao Zhong Mei-Jie Yang
Mei-Jie Yang Yan Hu1
Yan Hu1 Li Jiang
Li Jiang Jing-Wen Yu
Jing-Wen Yu Jin-Yun Chen
Jin-Yun Chen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 12 October 2022
Sec. Obstetrics and Gynecological Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.941368
This article is part of the Research Topic Women in Obstetrics and Gynecology View all 32 articles
Objective: To explore the influencing factors of decision-making in patients with adenomyosis, who are receiving high-intensity focused ultrasound (HIFU) treatment.
Methods: A total of 776 patients with adenomyosis were enrolled into HIFU group (241 cases) and hysterectomy group (535 cases) according to the treatment methods. The general data, clinical symptoms, marital and childbearing history, and economic status were compared between the two groups, and factors with P < 0.05 were introduced into multivariate logistic regression analysis to determine the determinants of patients choosing HIFU.
Results: The average age of the patients in the HIFU group was 39.1 ± 5.2 years, which was lower than that in the hysterectomy group, which was 45.1 ± 3.9 years (P < 0.05). The basic medical insurance for urban workers in the HIFU group was more than the hysterectomy group (P < 0.05). 95.9% of the hysterectomy group had no desire to have children, compared to 60.6% of the HIFU group, the difference was significant (P < 0.05). The treatment costs of HIFU group were significantly lower than that of hysterectomy group (P < 0.05). The main symptoms of the two groups were dysmenorrhea, menorrhagia, and secondary anemia. The results of multivariate logistic regression analysis showed that 31–40 years old, fertility desire, dysmenorrhea, menorrhagia, anemia and dizziness and fatigue were the influencing factors for the decision-making of HIFU for patients with adenomyosis.
Conclusion: 31–40 years old, fertility desire, dysmenorrhea, menorrhagia, anemia and dizziness and fatigue were the influencing factors for patients to choose HIFU treatment. HIFU therapy has emerged as a new option for patients with adenomyosis as an alternative to hysterectomy.
Adenomyosis (AM) is a common benign gynecological disease, defined as the presence of endometrial glands and stroma deep within the myometrium, causing myometrial hypertrophy and hyperplasia (1, 2). The true prevalence of adenomyosis is difficult to determine; for decades, the diagnosis of adenomyosis has been made mainly by pathology after hysterectomy, with a prevalence of about 5% to 70% (3). Over the past decade, adenomyosis can also be diagnosed without surgical intervention. Advances in imaging technology have created the possibility of non-invasive diagnosis of adenomyosis, such as magnetic resonance imaging (MRI) and transvaginal ultrasonography (TVUS). This allows the diagnosis to be made in young women, with or without clinical symptoms (4–7). Clinically, adenomyosis can result in abnormal bleeding, pelvic pain, and infertility, although approximately 30% of patients are asymptomatic (8–10). There are two types of adenomyosis: diffuse and focal (when a definite nodule is found, it can be called an adenomyoma). In addition, adenomyosis is often combined with other gynecological diseases, such as endometriosis (11, 12) and leiomyoma (13).
Adenomyosis treatment includes drug therapy, conservative surgery, interventional therapy, and hysterectomy. Hysterectomy is currently considered to be the last resort for adenomyosis (14), but it is a difficult choice for patients who want to preserve their uterus or maintain fertility. Unfortunately, approximately 50% of patients will experience relapse after conservative surgery (15). Drug therapy can effectively relieve clinical symptoms such as dysmenorrhea and menorrhagia (16).
High-intensity focused ultrasound (HIFU) is a new technology developed in recent years for non-invasive local hyperthermia treatment of tumors. It is widely used in gynecological diseases and has a good curative effect on uterine fibroids and adenomyosis (17, 18). The therapeutic mechanism of HIFU therapy is to focus the ultrasound beam generated by an external transducer on the target lesion in the body. The mechanical effect of ultrasound is transformed into thermal effect and cavitation effect. The purpose of HIFU in the treatment of adenomyosis is to selectively ablate adenomyosis lesions to relieve the symptoms. It relies on highly focused ultrasound energy to precisely destroy uterine adenomyosis in a non-invasive, bloodless manner (19). Patients treated with HIFU had significantly fewer symptoms of adenomyosis and recovered at a relatively high pregnancy rate after the treatment (20, 21). However, due to the unclear boundary of adenomyosis, some patients' symptom relief only lasts for a certain period, Liu et al. showed that 26% of patients relapsed after HIFU treatment, and the median time to relapse was 12 months (22). It should be noted that HIFU treatment is mainly suitable for symptomatic patients with lesions larger than 3 cm (23, 24).
Currently, there is no guideline for the management of adenomyosis, especially the uterine-sparing treatment of these adenomyosis presents formidable challenges to the gynecologist. Therefore, this study aimed to explore the factors influencing a patient's decision to undergo HIFU by extracting raw medical records, which can provide a basis for exploring optimized treatment strategies and clinical management options for patients with adenomyosis.
This cross-sectional retrospective study was conducted at the First Hospital of Chongqing Medical University. We reviewed all patients with adenomyosis (ICD-10: n80.001) who were admitted to hospital and received treatment from January 2013 to December 2020. Inclusion criteria were as follows: (1) premenopausal women; (2) typical symptoms: dysmenorrhea, menorrhagia; (3) diagnosis of adenomyosis by clinical evaluation, vaginal ultrasound and/or MRI (Figure 1).
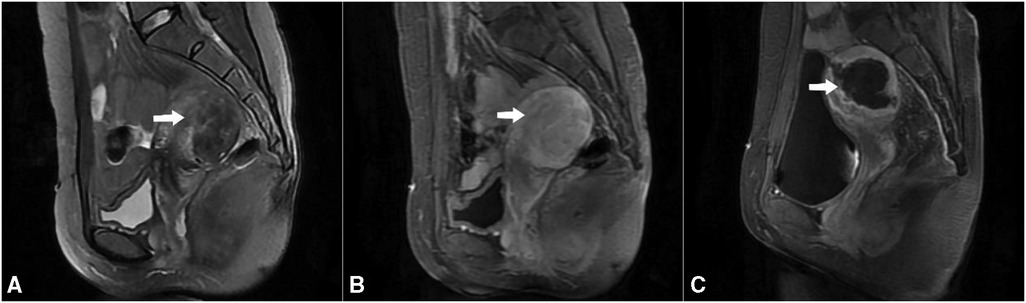
Figure 1. Mr images obtained from a patient with adenomyosis. (A) T2WI shows a well-defined adenomyosis lesion, which is a poorly defined low-signal lesion with scattered punctate and patchy high-signal foci located in the posterior uterine wall (arrow); (B) Contrast-enhanced MRI showed perfusion of the adenomyotic lesion (arrow); (C) Post-treatment T1-weighted contrast-enhanced image shows that the non-perfused volume ratio was 83.5% (arrow).
The exclusion criteria were: (1) no intervention on the day of admission and discharge; (2) incomplete electronic medical record description information; (3) postmenopausal women with abnormal uterine bleeding or/and lower abdominal pain; (4) patients who received treatments other than hysterectomy and HIFU; (5) patients with suspected or confirmed uterine malignancy; (6) patients with acute pelvic inflammatory disease.
After deliberation by the ethics committee of Chongqing Medical University (Ethics Approval Number, 2021–006), it is unnecessary to sign the informed consent form. However, it shall be implemented in strict accordance with the general provisions of the Declaration of Helsinki. Besides, all patient information is strictly confidential.
The age of each patient was calculated from the date of birth recorded in the case record to the date of hospitalization. At the same time, the clinical data of all patients were collected through a medical history system. These data included the patients' age, reproductive desire, work status, symptoms, marital status, abortion, deliver, cesarean section, medical insurance, and medical expenses.
SPSS 22.0 statistical software (IBM SPSS, USA) was used for the data analysis. Quantitative data are presented as mean ± SD, while count data are presented as [n (%)]. The χ2 test was used to compare differences between groups and P < 0.05 was considered statistically significant. In addition, multivariate logistic regression analysis was used to determine the influencing factors of patients' choice of HIFU.
There was a total of 973 patients diagnosed with adenomyosis on admission, excluding 127 patients who received drug treatment, 42 patients who received lesion resection, and 29 patients with abnormal uterine bleeding or lower abdominal pain in postmenopausal women. The remaining 776 patients, including 535 (57.5%) patients who underwent hysterectomy and 241 (42.5%) who underwent HIFU treatment, were included in this study.
Among the 776 patients, 626 (80.7%) complained of dysmenorrhea, 497 (64%) menorrhagia, 427 (55%) secondary anemia and 230 (29.6%) lower abdominal pain (Figure 2).
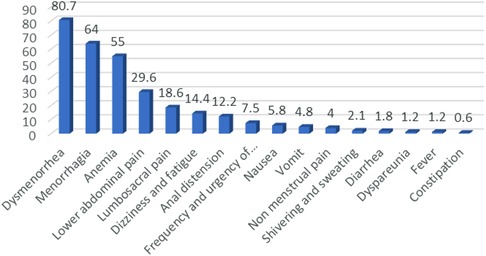
Figure 2. Symptoms of patients with adenomyosis (%).
The patients were enrolled into two groups according to the treatment method. The mean age of patients in the hysterectomy group was 45.1 ± 3.9 years (range = 31–52 years), and the HIFU group was 39.1 ± 5.2 years (range = 25–52 years), the difference was significant (t = 17.704 P < 0.001).60.6% of the HIFU group were younger than 40 years old, and only 11.6% were in the hysterectomy group. There was a statistically significant difference in age distribution between the two groups (χ2 = 211.722, P < 0.001). Meanwhile, the HIFU group had a desire to have children in 60.6%, which was significantly higher than the hysterectomy group (4.1%) (χ2 = 312.346, P < 0.001).In addition, patients with jobs in the HIFU group accounted for 74.4%, which was significantly higher than that in the hysterectomy group (50.3%); while 23.7% of the patients in the HIFU group had temporary job, which was significantly lower than that in the hysterectomy group (41.1%) (χ2 = 42.656, P < 0.001) (Table 1).
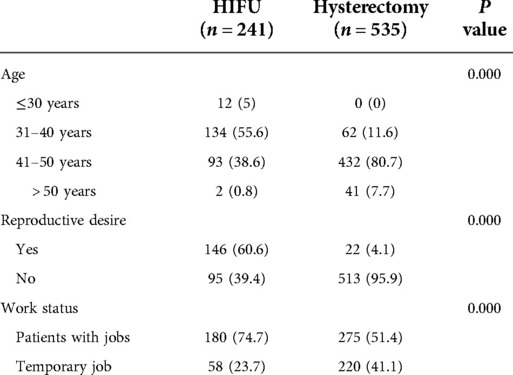
Table 1. Comparison of basic conditions of patients with adenomyosis [n(%)].
The main clinical manifestations of hospitalized patients were dysmenorrhea, menorrhagia, secondary anemia, and lower abdominal pain. Compared with the two treatment decisions, dysmenorrhea accounted for 90.1% in the HIFU group, which was significantly higher than that in the hysterectomy group (75.9%) (χ2 = 21.470, P < 0.001); Menorrhagia in the HIFU group were 52.1%, which was significantly lower than that in the hysterectomy group (69.3%) (χ2 = 21.009, P < 0.001);The secondary anemia covered 38.8% in the HIFU group, which was significantly lower than that in the hysterectomy group (61.9%) (χ2 = 38.161, P < 0.001).At the same time, other symptoms included dizziness and fatigue, urinary frequency and urgency, nausea, vomiting, diarrhea and dyspareunia, and the difference between the two groups was statistically significant (all P < 0.05) (Table 2).
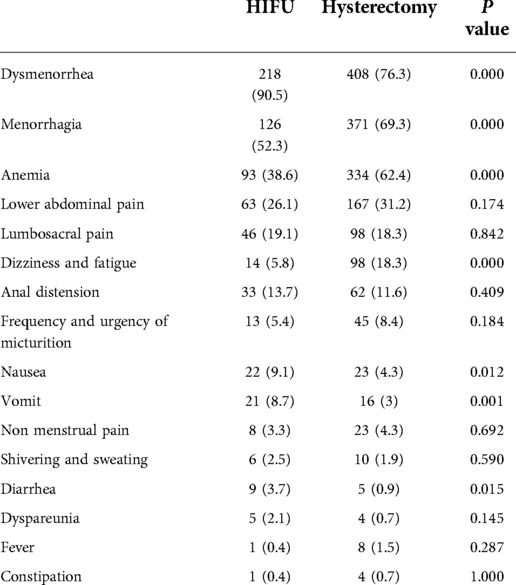
Table 2. Comparison of related symptoms in patients with adenomyosis [n(%)].
The patients who have childbirth history of the HIFU group was 79.3%, which was lower than that of the hysterectomy group (92.3%), and the difference was statistically significant (χ2 = 27.475, P < 0.001). There was no significant difference in marital status, history of abortion, and childbirth between the two groups (P > 0.05) (Table 3).
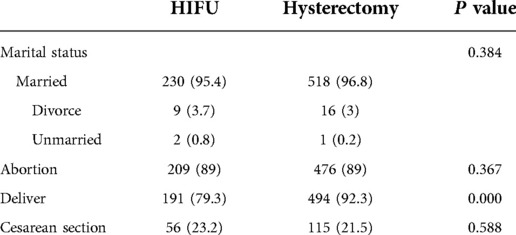
Table 3. Comparison of marital and reproductive status of patients with adenomyosis. [n(%)].
The basic medical insurance for urban workers in the HIFU group (71.4%) was higher than that in the hysterectomy group (53.6%), while the basic medical insurance for urban residents in the HIFU group (24.5%) was lower than that in the hysterectomy group (40.7%). (χ2 = 25.793, P < 0.001). The proportion of HIFU treatment costs less than ¥25,000 was 62.2%, while that in the hysterectomy group was 19.4%. There was a statistically significant difference in the distribution of treatment costs between the two groups, and the hysterectomy group was higher (χ2 = 230.024, P < 0.001) (Table 4).
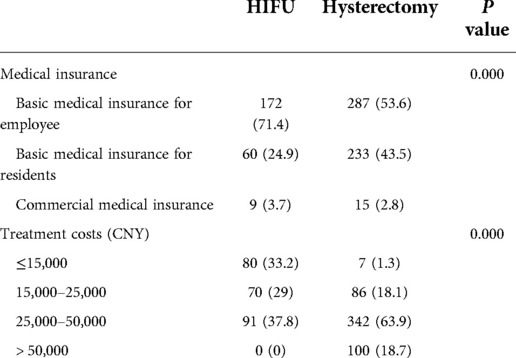
Table 4. Comparison of economic situation of patients with adenomyosis [n(%)].
Univariate analysis was performed on the influence of patients' general information, clinical symptoms, marriage and childbearing history, economic status, etc. on treatment decisions, and statistically significant indicators were included in multivariate analysis, including age, medical insurance category, work status, reproductive requirements, and birth history., dysmenorrhea, menorrhagia, anemia, nausea, vomiting, diarrhea, dizziness and fatigue, P < 0.05 was used to screen the patients with adenomyosis Influencing factors for choosing HIFU.
The results showed that between 31 and 40 years old (OR = 0.188, P = 0.039), fertility requirements (OR = 0.051, P < 0.001), dysmenorrhea (OR = 0.525, P = 0.035), menorrhagia (OR = 1.605, P = 0.048), secondary anemia (OR = 1.799, P = 0.013), and dizziness and fatigue (OR = 2.453, P = 0.023) were the influencing factors for HIFU decision-making in patients with adenomyosis (Table 5).
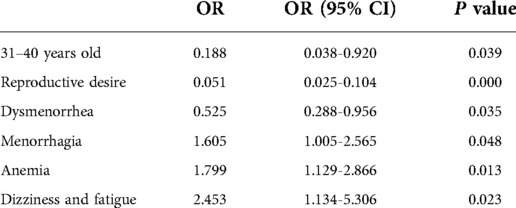
Table 5. Factors influencing decision-making for HIFU treatment [n(%)].
Adenomyosis is a common chronic gynecological disease. Treating adenomyosis remains a global challenge, and most women want to protect their uterus while effectively relieving symptoms and improving their quality of life. The problem that this study attempts to solve is to find out the characteristics of the population who choose HIFU treatment and hysterectomy treatment, and the factors influencing the decision-making of patients choosing HIFU treatment. The results show that patients under the age of 40, who have jobs, have basic medical insurance for urban workers, and have fertility requirements are more inclined to choose HIFU; However, patients who are older than 40 years old, have no fixed jobs, have basic medical insurance for urban residents, and have no desire to have children tend to choose hysterectomy. In addition, the HIFU group had fewer treatment costs compared to hysterectomy.
In clinical practice, we found that many factors may affect patients' choice for HIFU treatment. In this study, patients treated with HIFU were significantly younger than the hysterectomy group (P < 0.001), with a range of age 31–40 years (55.6%), meanwhile there was also a statistical difference in fertility requirements between patients treated with HIFU and the hysterectomy group (P < 0.001), with 60.6% of patients treated with HIFU having fertility requirements. More and more young women were diagnosed, mainly because the diagnosis now was based on imaging diagnoses such as TVUS and MRI (9, 20). At the same time, with the change in women's concept of fertility, more and more women choose to give birth after the age of 30 and retain the uterus, and symptom relief are their primary concerns when seeking treatment options. Therefore, as a non-invasive treatment, HIFU has become the preferred treatment method for women of childbearing age between 31 and 40 years old. There are multiple clinical case reports of improved fertility after HIFU treatment (25, 26). The benefit of HIFU treatment for patients with adenomyosis deserves further study.
Severe dysmenorrhea and menorrhagia are considered as the most important symptoms affecting patients' quality of life. The main purpose of adenomyosis treatment is to relieve symptoms and improve the quality of life of patients. HIFU has been used to treat adenomyosis for many years. Recently, more and more gynecologists in China consider HIFU as a routine treatment for patients with adenomyosis. The results of 3–12 months' follow-up of patients with adenomyosis treated with HIFU showed that the clinical effective rate of improving dysmenorrhea or menorrhea was about 80% (18, 27). And combined treatment regimen with GnRHa and LNG-IUS after HIFU can significantly improve long-term outcomes (28). Although hysterectomy can also solve the patient's symptom problems, it brings many serious side effects, such as loss of reproductive function, impaired pelvic anatomical integrity, impaired neural network systems, and the gonadal endocrine axis (29, 30). Therefore, hysterectomy is mainly suitable for older patients, who have no fertility requirements, severe symptoms, and poor drug treatment effects or drug contraindications. HIFU may be a better choice for patients who have fertility requirements and want to relieve symptoms. However, HIFU technology as a way to treat adenomyosis, its comprehensive management plan which needs further study, to improve its long-term efficacy and reduce recurrence.
Another important finding of this study was that work status and medical insurance category were significantly associated with the choice of HIFU treatment in patients. 74.7% of the patients who received HIFU treatment were working and had a high level of basic medical insurance for urban workers. The main reason may be that the Patients with jobs have less time controllability than who with temporary job. Considering the postoperative recovery time, HIFU has more advantages than hysterectomy. Another aspect is that the proportion of anyone at work who have received higher education is relatively high, they have a deeper understanding of health awareness and medical knowledge and are more inclined to new technologies with fewer side effects (23). In addition, adenomyosis is still at risk of recurrence after HIFU treatment and the possibility of getting secondary interventions is high. Therefore, financial freedom and independent decision-making ability have become important factors affecting treatment decisions. Patients with jobs are more inclined to choose less traumatic and repeatable treatments.
The main concern of patients when they visit the clinic, besides the cure rate of the disease, is the actual cost of medical care. This study found that the medical cost of HIFU treatment was significantly lower than that of hysterectomy (P < 0.001), and 62.2% of patients spent less than 25,000 CNY. Therefore, HIFU is inexpensive than hysterectomy. Evaluating the cost of care not only helps healthcare providers and healthcare systems utilize limited healthcare resources, it also provides a way to maximize benefits to patients and healthcare systems.
This study is a retrospective study, there is no unified path design for patient selection, and it is difficult to avoid the influence of physicians' own technical knowledge on patients' treatment choices. Due to the possibility of skin and subcutaneous tissue burns during HIFU treatment, the limitation of large abdominal scarring in the path of the ultrasound beam remains (31). Although research has shown that scar patches are safe and effective in relieving abdominal scarring in patients with uterine and adenomyosis treated with MRgHIFU (32). But this study did not consider the effect of this factor on treatment decisions in patients with adenomyosis, which is one of the study's limitations.
The results of this study show that HIFU is safe and effective in the treatment of adenomyosis, and the cost is lower than that of hysterectomy. Age 31–40, fertility desire, dysmenorrhea, menorrhagia, anemia, and dizziness and fatigue were the factors influencing patients' treatment decision to choose HIFU. In conclusion, HIFU treatment can keep the uterus while relieving symptoms. It has become one of the new choices for patients with adenomyosis, and younger (31–40 years old) working patients who are willing to choose HIFU treatment. Meanwhile, prospective studies on patient self-report scales are needed in the future to optimize patient treatment decisions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Haifu Hospital of Chongqing Medical University. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
ZQ, CJY, and CWZ contributed to conception and design of the study. ZQ organized the database. ZQ, YMJ performed the statistical analysis. ZQ, wrote the first draft of the manuscript. ZQ, YMJ, HY, JL, and YJW wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
We thank The First Affiliated Hospital of Chongqing Medical University, Chongqing, China for providing related clinical data.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Donnez J, Donnez O, Dolmans MM. Introduction: uterine adenomyosis, another enigmatic disease of our time. Fertil Steril. (2018) 109(3):369–70. doi: 10.1016/j.fertnstert.2018.01.035
2. Senturk LM, Imamoglu M. Adenomyosis: what is new? Women's Health. (2015) 11(5):717–24. doi: 10.2217/whe.15.60
3. Protopapas A, Grimbizis G, Athanasiou S, Loutradis D. Adenomyosis: disease, uterine aging process leading to symptoms, or both? Facts, Views Vision in ObGyn. (2020) 12(2):91–104.
4. Kishi Y, Suginami H, Kuramori R, Yabuta M, Suginami R, Taniguchi F. Four subtypes of adenomyosis assessed by magnetic resonance imaging and their specification. Am J Obstet Gynecol. (2012) 207(2):114.e1–7. doi: 10.1016/j.ajog.2012.06.027
5. Van den Bosch T, Van Schoubroeck D. Ultrasound diagnosis of endometriosis and adenomyosis: state of the art. Best Pract Res Clin Obstet Gynaecol. (2018) 51:16–24. doi: 10.1016/j.bpobgyn.2018.01.013
6. Loring M, Chen TY, Isaacson KB. A systematic review of adenomyosis: it is time to reassess what we thought we knew about the disease. J Minim Invasive Gynecol. (2021) 28(3):644–55. doi: 10.1016/j.jmig.2020.10.012
7. Chapron C, Vannuccini S, Santulli P, Abrão MS, Carmona F, Fraser IS, et al. Diagnosing adenomyosis: an integrated clinical and imaging approach. Hum Reprod Update. (2020) 26(3):392–411. doi: 10.1093/humupd/dmz049
8. Abbott JA. Adenomyosis and abnormal uterine bleeding (Aub-a)-pathogenesis, diagnosis, and management. Best Prac Res Clin Obstet Gynaecol. (2017) 40:68–81. doi: 10.1016/j.bpobgyn.2016.09.006
9. Pinzauti S, Lazzeri L, Tosti C, Centini G, Orlandini C, Luisi S, et al. Transvaginal sonographic features of diffuse adenomyosis in 18–30-year-old nulligravid women without endometriosis: association with symptoms. Ultrasound Obstet Gynecol. (2015) 46(6):730–6. doi: 10.1002/uog.14834
10. Bourdon M, Santulli P, Marcellin L, Maignien C, Maitrot-Mantelet L, Bordonne C, et al. Adenomyosis: an update regarding its diagnosis and clinical features. J Gynecol Obstet Hum Reprod. (2021) 50(10):102228. doi: 10.1016/j.jogoh.2021.102228
11. Di Donato N, Montanari G, Benfenati A, Leonardi D, Bertoldo V, Monti G, et al. Prevalence of adenomyosis in women undergoing surgery for endometriosis. Eur J Obstet Gynecol Reprod Biol. (2014) 181:289–93. doi: 10.1016/j.ejogrb.2014.08.016
12. Eisenberg VH, Arbib N, Schiff E, Goldenberg M, Seidman DS, Soriano D. Sonographic signs of adenomyosis are prevalent in women undergoing surgery for endometriosis and may suggest a higher risk of infertility. Biomed Res Int. (2017) 2017:8967803. doi: 10.1155/2017/8967803
13. Brucker SY, Huebner M, Wallwiener M, Stewart EA, Ebersoll S, Schoenfisch B, et al. Clinical characteristics indicating adenomyosis coexisting with leiomyomas: a retrospective, questionnaire-based study. Fertil Steril. (2014) 101(1):237–41. doi: 10.1016/j.fertnstert.2013.09.038
14. Li X, Liu X, Guo SW. Clinical profiles of 710 premenopausal women with adenomyosis who underwent hysterectomy. J Obstet Gynaecol Res. (2014) 40(2):485–94. doi: 10.1111/jog.12211
15. Younes G, Tulandi T. Conservative surgery for adenomyosis and results: a systematic review. J Minim Invasive Gynecol. (2018) 25(2):265–76. doi: 10.1016/j.jmig.2017.07.014
16. Farquhar C, Brosens I. Medical and surgical management of adenomyosis. Best Pract Res Clin Obstet Gynaecol. (2006) 20(4):603–16. doi: 10.1016/j.bpobgyn.2006.01.012
17. Fan HJ, Zhang C, Lei HT, Cun JP, Zhao W, Huang JQ, et al. Ultrasound-Guided high-intensity focused ultrasound in the treatment of uterine fibroids. Medicine (Baltimore). (2019) 98(10):e14566. doi: 10.1097/md.0000000000014566
18. Zhang X, Li K, Xie B, He M, He J, Zhang L. Effective ablation therapy of adenomyosis with ultrasound-guided high-intensity focused ultrasound. Int J Gynaecol Obstet. (2014) 124(3):207–11. doi: 10.1016/j.ijgo.2013.08.022
19. Stewart EA, Gedroyc WM, Tempany CM, Quade BJ, Inbar Y, Ehrenstein T, et al. Focused ultrasound treatment of uterine fibroid tumors: safety and feasibility of a noninvasive thermoablative technique. Am J Obstet Gynecol. (2003) 189(1):48–54. doi: 10.1067/mob.2003.345
20. Guo Q, Xu F, Ding Z, Li P, Wang X, Gao B. High intensity focused ultrasound treatment of adenomyosis: a comparative study. Int J Hyperthermia. (2018) 35(1):505–9. doi: 10.1080/02656736.2018.1509238
21. Parazzini F, Mais V, Cipriani S, Busacca M, Venturini P. Determinants of adenomyosis in women who underwent hysterectomy for benign gynecological conditions: results from a prospective multicentric study in Italy. Eur J Obstet Gynecol Reprod Biol. (2009) 143(2):103–6. doi: 10.1016/j.ejogrb.2008.12.010
22. Liu X, Wang W, Wang Y, Wang Y, Li Q, Tang J. Clinical predictors of long-term success in ultrasound-guided high-intensity focused ultrasound ablation treatment for adenomyosis: a retrospective study. Medicine (Baltimore). (2016) 95(3):e2443. doi: 10.1097/md.0000000000002443
23. Zhang L, Rao F, Setzen R. High intensity focused ultrasound for the treatment of adenomyosis: selection criteria, efficacy, safety and fertility. Acta Obstet Gynecol Scand. (2017) 96(6):707–14. doi: 10.1111/aogs.13159
24. Keserci B, Duc NM, Nadarajan C, Huy HQ, Saizan A, Wan Ahmed WA, et al. Volumetric mri-guided, high-intensity focused ultrasound ablation of uterine leiomyomas: asean preliminary experience. Diagnostic Intervent Radiol. (2020) 26(3):207–15. doi: 10.5152/dir.2019.19157
25. Huang YF, Deng J, Wei XL, Sun X, Xue M, Zhu XG, et al. A comparison of reproductive outcomes of patients with adenomyosis and infertility treated with high-intensity focused ultrasound and laparoscopic excision. Int J Hyperthermia. (2020) 37(1):301–7. doi: 10.1080/02656736.2020.1742390
26. Zhou CY, Xu XJ, He J. Pregnancy outcomes and symptom improvement of patients with adenomyosis treated with high intensity focused ultrasound ablation. Zhonghua fu Chan ke za zhi. (2016) 51(11):845–9. doi: 10.3760/cma.j.issn.0529-567X.2016.11.009
27. Haiyan S, Lin W, Shuhua H, Wang W. High-Intensity focused ultrasound (hifu) combined with gonadotropin-releasing hormone analogs (gnrha) and levonorgestrel-releasing intrauterine system (lng-ius) for adenomyosis: a case series with long-term follow up. Int J Hyperthermia. (2019) 36(1):1179–85. doi: 10.1080/02656736.2019.1679892
28. Li X, Zhu X, He S, Jiang Z, Li H, Tian X, et al. High-intensity focused ultrasound in the management of adenomyosis: long-term results from a single center. Int J Hyperthermia. (2021) 38(1):241–7. doi: 10.1080/02656736.2021.1886347
29. Ryann Louie A, Armstrong JA, Findeiss LK, Goodwin SC. Comparison of sexual dysfunction using the female sexual function Index following surgical treatments for uterine fibroids. Case Rep Obstet Gynecol. (2012) 2012:368136. doi: 10.1155/2012/368136
30. Barber EL, Harris B, Gehrig PA. Trainee participation and perioperative complications in benign hysterectomy: the effect of route of surgery. Am J Obstet Gynecol. (2016) 215(2):215.e1–7. doi: 10.1016/j.ajog.2016.02.022
31. Hindley J, Gedroyc WM, Regan L, Stewart E, Tempany C, Hynyen K, et al. Mri guidance of focused ultrasound therapy of uterine fibroids: early results. AJR Am J Roentgenol. (2004) 183(6):1713–9. doi: 10.2214/ajr.183.6.01831713
Keywords: adenomyosis, HIFU, dysmenorrhea, menorrhagia, decision-making
Citation: Zhong Q, Yang M-J, Hu Y, Jiang L, Yu J-W, Chen J-Y and Chen W-Z (2022) Factors influencing treatment decisions in HIFU treatment of adenomyosis: A retrospective study. Front. Surg. 9:941368. doi: 10.3389/fsurg.2022.941368
Received: 11 May 2022; Accepted: 26 September 2022;
Published: 12 October 2022.
Edited by:
Grigoris F Grimbizis, Aristotle University of Thessaloniki, GreeceReviewed by:
Andrea Giannini, University of Pisa, Italy© 2022 Zhong, Yang, Hu, Jiang, Yu, Chen and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jin-Yun Chen Y2hlbmp5QGNxbXUuZWR1LmNu
Specialty Section: This article was submitted to Obstetrics and Gynecological Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.