 Fei Zhang
Fei Zhang Li Wang
Li Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 19 August 2022
Sec. Genitourinary Surgery and Interventions
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.938911
Purpose: We present our experience with retroperitoneoscopic pyeloplasty with simultaneous pyelolithotomy using a flexible cystoscope in patients with ureteropelvic junction obstruction(UPJO) complicated with kidney stones.
Materials and Methods: The records of 37 patients who underwent retroperitoneoscopic pyeloplasty with simultaneous pyelolithotomy using a flexible cystoscope to manage UPJO complicated with kidney stones from July 2015 to December 2020 were retrospectively reviewed. All patients underwent one-stage retroperitoneoscopic pyeloplasty combined with flexible cystoscopic pyelolithotomy. The operative time, blood volume, stone clearance rate, length of hospital stay, complications and follow-up events were recorded.
Results: The operation went smoothly in all 37 patients. The mean operative time was 148.4 ± 24.2 min. The mean intraoperative blood loss volume was 54.3 ± 20.5 ml. The mean hospitalization time was 10.6 ± 3.7 days. The stone clearance rate was 81.08%. The mean follow-up period was 23.5 months (range 12–53 months). Hydronephrosis was significantly decreased in 33 of the 37 cases. The success rate of the operation was 89.19%. Stones recurred in 9 patients during follow-up, for a recurrence rate of 24.32%.
Conclusion: Retroperitoneoscopic pyeloplasty with simultaneous pyelolithotomy using a flexible cystoscope in patients with UPJO complicated with kidney stones is safe, effective and worthy of promotion.
Ureteropelvic junction obstruction is a common anatomic lesion in urology. Its congenital incidence is approximately 0.1% (1). UPJO is complicated with kidney stones in up to 20% of cases due to obstruction and hydronephrosis (2, 3). UPJO complicated with kidney stones is difficult to treat surgically. Surgical methods for treating UPJO complicated by kidney stones include open surgery, percutaneous nephrolithotomy (PNL) with endopyelotomy, retroperitoneoscopic or laparoscopic robot-assisted pyeloplasty with flexible or rigid scopes, and simultaneous or staged surgery (4, 5). In the past, PNL with endopyelotomy was the preferred treatment, but its long-term efficacy is unsatisfactory (6). Staged surgery adds time and financial cost to patients. For most hospitals and patients in China, the Da Vinci surgical robotic system (DVSS) is too expensive (7). In recent years, with the rapid development of laparoscopic and endoscopic surgery, combined laparoscopic and endoscopic technology in the management of UPJO complicated with kidney stones has achieved desirable results (8–10).
From July 2015 to December 2020, a retroperitoneoscopic method combined with the use of a flexible cystoscope was used for pyelolithotomy in 37 cases in our hospital, and it achieved favourable efficacy. The present study aimed to introduce our experience with combined retroperitoneoscopy and flexible cystoscopic pyelolithotomy for patients with UPJO complicated with kidney stones.
The study was approved by the ethics committee of our hospital. Written informed consent was obtained from all patients. All patients underwent intravenous pyelography (IVP) and CT examinations routinely. If IVP imaging was not clear, retrograde pyelography was performed. Inclusion criteria were a diagnosis of UPJO complicated with kidney stones and treatment with retroperitoneoscopic pyeloplasty with simultaneous pyelolithotomy using a flexible cystoscope. Patients who were complicated with a nonfunctional kidney were excluded from our analysis. From July 2015 to May 2020, 37 patients with symptomatic ureteropelvic obstruction and kidney stones underwent retroperitoneoscopic pyeloplasty with concomitant pyelolithotomy. The age range of the participants was 27–67 years, and the mean age was 43.8 ± 11.1 years. The clinical manifestations included back pain in 29 patients, gross haematuria in 11 patients, and recurrent pyelonephritis in 10 patients. Mild hydronephrosis, moderate hydronephrosis and severe hydronephrosis were diagnosed in 3 cases, 25 cases and 9 cases, respectively. Seven patients had a single kidney stone, and 30 patients had multiple kidney stones, with a maximum diameter of 23 mm. Eight patients received other treatments prior to admission, such as high-pressure balloon catheter dilation or ureteral stent placement. Enhanced urinary computed tomography was performed preoperatively for all patients, and retrograde renal pyelography was employed for 9 patients to clarify the diagnosis. Other clinical data were shown in Table 1.
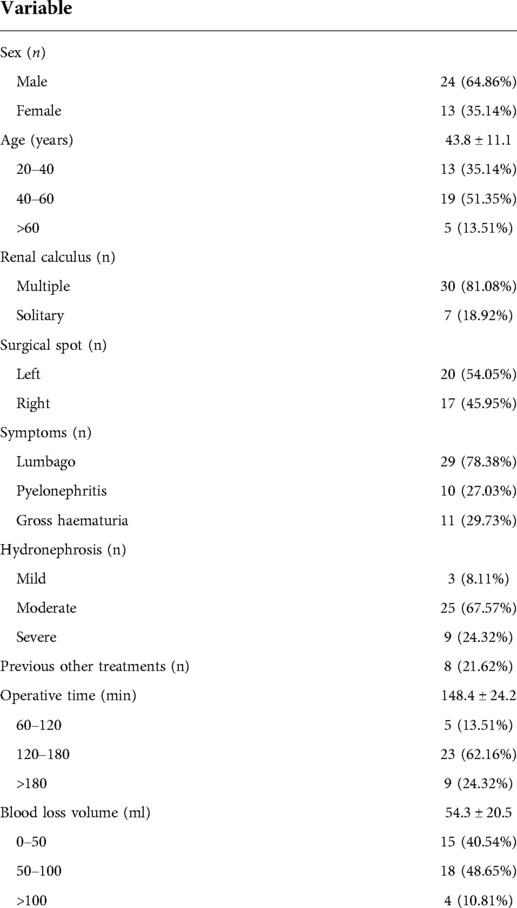
Table 1. Demographic characteristics and surgical statistics.
Two sets of endoscopic monitoring equipment were placed at the head of the patient. After general anaesthesia was induced, an indwelling catheter was placed. Then, the patient was placed in the flank position, depending upon the side to be operated on.
The primary port, a 12 mm incision, was made 1 cm below the 12th rib margin of the posterior axillary line. Balloon dilation through this port was done to create the retroperitoneal space. Once balloon dilation was completed, the second port, a 12 mm incision, was placed 1 cm below the 12th rib margin of the anterior axillary line. The third port, a 12 mm incision, was made at the midaxillary line approximately two finger breadths cephalad to the anterior superior iliac spine. The third port was used to hold the laparoscope. Antibiotics were administered during anaesthesia induction. The perirenal fascia was longitudinally opened. The inferior pole of the kidney was dissociated. The renal pelvis and upper ureter were exposed. A 15 mm incision was made in the pelvis. The flexible cystoscope was placed into the retroperitoneal space through a 12 mm trocar and then inserted into the pelvis to detect the stone with the aid of the assistant (Figure 1B). The stone was removed using a stone basket catheter through the working channel of the flexible cystoscope (Figure 1C). The stone was ablated using a holmium laser if it was too large to be removed. Whether the stone had been completely removed was verified by referring to the preoperative computed tomography scan. The ureteropelvic junction obstruction was managed on the basis of the Anderson-Hynes procedure. At the end of the operation, an F6 double-J stent was placed into the ureter. Urological computed tomography examination was performed on the third day after the operation, and the ureteral stent was removed two months after the operation. CT urography was carried out three months after the surgery. Successful operation was defined as a CT reexamination showing a significant reduction in hydronephrosis after the removal of the double J tubes. Urological ultrasonography examination was performed every 3 months.

Figure 1. (A) Two monitors were placed at the head of the patient. The surgeon stood behind the patient, and the assistant stood in front of the patient. (B) The flexible cystoscope was placed in the retroperitoneal space through a 12 mm trocar and was then inserted into the pelvis to detect the stone with the aid of the assistant. (C) The fragments were extracted using a Nitinol stone basket.
The operation went smoothly in all 37 patients. The mean operative time was 148.4 ± 24.2 min (range, 97–182). The mean intraoperative blood loss volume was 54.3 ± 20.5 ml (range, 25–150). The mean hospitalization time was 10.6 ± 3.7 days (range 7–11). Six patients suffered from complications (Clavien I and IIIa). Three patients had postoperative fever, which was treated medically. Three patients suffered urine leakage from the double-J stent bending; the perirenal effusion was absorbed two weeks later after repositioning of the double-J stent. At two months, 7 patients had residual calculi, for a stone clearance rate of 81.08%. Consequently, these patients underwent further stone management, including ureteroscopy and shock wave lithotripsy. The mean follow-up period was 23.5 months (range 12–53 months). Frequent haematuria occurred in 8 patients before removal of ureteral stents, and 11 patients presented with mild back pain. Hydronephrosis was significantly decreased in 33 of the 37 patients, for a success rate of the UPJO operation of 89.19%. Stones recurred in 9 patients during follow-up, a recurrence rate of 24.32% (Table 2).
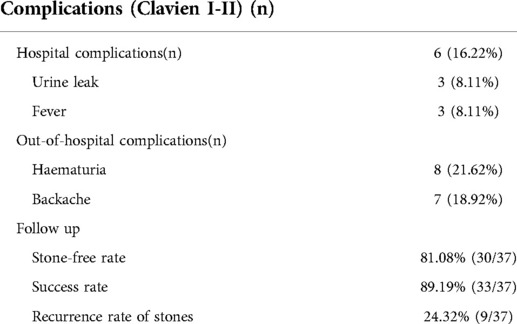
Table 2. Complications and follow-up.
UPJO is a common anatomic lesion in urology. Its congenital incidence is approximately 0.1%. Up to 20% of UPJOs are complicated with kidney stones due to obstruction and hydronephrosis. In the past 20 years, with the development of laparoscopy, laparoscopic pyeloplasty has become the main treatment for UPJO. The laparoscopic technique is superior to open surgery due to its low trauma, favourable field of exposure and ease of suturing (11).
In patients diagnosed with UPJO complicated with kidney stones, the stones tend to be located in the lower calyx of the kidney. The treatment of UPJO complicated with kidney stones with a laparoscopic method alone is frequently not desirable. When percutaneous lithotripsy has been performed to treat both UPJO and kidney stones, the postoperative follow-up indicated poor outcomes (4–6). A two-stage procedure for patients with UPJO complicated with kidney stones, including a first-stage laparoscopic pyeloplasty for UPJO and second-stage percutaneous nephroscopy for kidney stones, is effective, but this increases the medical costs to the patient significantly.
The angle of the renal pelvis and lower calyx make it very difficult to deal with kidney stones. The treatment of UPJO combined with kidney stones using a laparoscopic or endoscopic method alone is difficult and unsatisfactory. In recent years, some scholars have reported that the combination of laparoscopic or robotic laparoscopic surgery and flexible cystoscopy in the treatment of UPJO complicated with kidney stones leads to excellent outcomes in terms of both the stone clearance rate and protecting renal function. Peng et al. introduced a flexible guiding tube as a simple modification of laparoscopic pyeloplasty combined with a flexible cystoscope for the treatment of UPJO complicated with renal calculi (12). An et al. introduced laparoscopic pyeloplasty combined with a 19.5-F rigid nephroscope for the treatment of UPJO complicated with kidney stones (13). Lambertini et al. reported on 43 cases of UPJO with urolithiasis that were treated with robotic-assisted pyeloplasty with endoscopic removal of stones, and the effects were satisfactory (14). Hüttenbrink et al. reported a stone clearance rate of 100% with no complications from a combination of robotic pyeloplasty and percutaneous renal surgery for the treatment of UPJO and calyx stones (15).
Since July 2015, we have used retroperitoneoscopic pyeloplasty combined with antegrade flexible cystoscopic pyelolithotomy in one stage to treat 37 cases of UPJO complicated with kidney stones, with a stone clearance rate of 81.08% and a UPJO operation success rate of 89.19%. The advantages of our procedure include the following: (1) When UPJO is complicated with kidney stones, most of the stones are located in the lower renal calyx, and the angle of the renal pelvis and lower calyx makes it very difficult to deal with kidney stones there. However, in anterograde flexible cystoscopic pyelolithotomy, the stone clearance rate is almost unaffected by the angle. (2) The body of the flexible cystoscope used for pyelolithotomy is thick and short, making it more manipulable through anterograde procedures than a flexible ureteroscope. However, for patients with a narrow calyceal neck, an antegrade flexible ureteroscope can be used to remove the stone. Of the 37 cases here, 6 needed the flexible ureteroscope due to a narrow calyx neck, while the remaining procedures were completed by flexible cystoscopic pyelolithotomy. (3) A 15 mm incision in the renal pelvis is a good size. A smaller incision causes difficulty removing stones, and larger incisions cause difficulties in filling the renal pelvis with perfusion fluid, leading to renal pelvis collapse and no room for the operation. During flexible cystoscopic pyelolithotomy, perfusion fluid in the renal pelvis is removed through a suction apparatus by an assistant to help keep the surgical field clear. (4) Patience and carefulness are indispensable for performing antegrade flexible cystoscopic pyelolithotomy due to changes in operating habits. Larger kidney stones can be broken into pieces with a holmium laser, followed by removal with a stone basket. (5) The retroperitoneal approach is as effective as the intraperitoneal approach, with little interference by abdominal organs and rapid postoperative recovery. Sometimes, operation through the intraperitoneal approach may cause abdominal infection and intestinal adhesion. (6) Two procedures, retroperitoneoscopic pyeloplasty and flexible cystoscopic pyelolithotomy, can complement each other to combine their advantages and avoid their disadvantages and clear stones to the greatest extent. (7) Retroperitoneoscopic pyeloplasty and flexible cystoscopic pyelolithotomy can be used to manage UPJO complicated with kidney stones in one stage, thus avoiding a second surgery and reducing medical costs.
Retroperitoneoscopic pyeloplasty combined with antegrade flexible cystoscopic pyelolithotomy for UPJO complicated with kidney stones is advantageous in terms of minimal trauma, rapid recovery and a high stone clearance rate. Retroperitoneoscopic pyeloplasty and antegrade flexible cystoscopic pyelolithotomy can complement each other. This technology can avoid a second operation, reduce the medical costs to patients, and efficiently treat UPJO complicated with kidney stones. Of course, there are some limitations to our work. Due to the lack of a DVSS here, we were unable to compare the pros and cons of DVSS and retroperitoneoscopy in the management of UPJO complicated with kidney stones, which may be a more interesting question. Though it is the most sensitive indicator of renal function, we rarely do kidney scans for a variety of reasons, and this might affect the quality of our conclusions. We look forward to conducting a larger, prospective, multicentre, well-equipped clinical trial to further investigate the treatment of UPJO complicated with kidney stones.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Human Research Ethics Committee of Hwa Mei Hospital, Univeisity of Chinese Academy of Sciences. The patients/participants provided their written informed consent to participate in this study.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
FZ and LW have contributed equally to this work and LW should be considered as co-first author. FZ and LW drafted the manuscript and helped with the statistical analysis. HMY participated in the design of the study and revised the manuscript. ZBG participated in data collection. All authors contributed to the article and approved the submitted version.
This work was supported by Taizhou Science and Technology Projects: 20ywb64.
The authors genuinely thank the reviewers for their helpful comments on this paper.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Skolarikos A, Dellis A, Knoll T. Ureteropelvic obstruction and renal stones: etiology and treatment. Urolithiasis. (2015) 43(1):5–12. doi: 10.1007/s00240-014-0736-2
2. Stasinou T, Bourdoumis A, Masood J. Forming a stone in pelviureteric junction obstruction: cause or effect?. Int Braz J Urol. (2017) 43:13–9. doi: 10.1590/s1677-5538.ibju.2015.0515
3. Krajewski W, Wojciechowska J, Dembowski J, Zdrojowy R, Szydelko T. Hydronephrosis in the course of ureteropelvic junction obstruction: an underestimated problem? Current opinions on the pathogenesis, diagnosis and treatment. Adv Clin Exp Med. (2017) 26(5):857–64. doi: 10.17219/acem/59509
4. Mantica G, Balzarini F, Chierigo F, Keller EX, Talso M, Emiliani E, et al. The fight between PCNL, laparoscopic and robotic pyelolithotomy: do we have a winner? A systematic review and meta-analysis. Minerva Urol Nephrol. (2022) 74(2):169–77. doi: 10.23736/S2724-6051.21.04587-0
5. Kartal I, Tuygun C, Karakoyunlu AN, Sandikci F, Baylan B, Ersoy H. Retrograde intrarenal surgery following laser endopyelotomy; sequential procedures for ureteropelvic junction obstruction and nephrolithiasis. Urol J. (2019) 16(6):541–6. doi: 10.22037/uj.v0i0.5205
6. Wei C, Wang T, Chen S, Ren XB, Chen XD. Concomitant management of renal calculi and recurrent ureteropelvic junction obstruction with percutaneous nephrolithotomy and antegrade balloon dilation. J Int Med Res. (2020) 48(5):030006052091125. doi: 10.1177/0300060520911252
7. Yang C, Zhou J, Lu ZX, Hao ZY, Wang JZ, Zhang L, et al. Simultaneous treatment of ureteropelvic junction obstruction complicated by renal calculi with robotic laparoscopic surgery and flexible cystoscope. World J Urol. (2019) 37(10):2217–23. doi: 10.1007/s00345-018-2608-9
8. Yin Z, Wei YB, Liang BL, Zhou KQ, Gao YL, Yan B, et al. Initial experiences with laparoscopy and flexible ureteroscopy combination pyeloplasty in management of ectopic pelvic kidney with stone and ureter–pelvic junction obstruction. Urolithiasis. (2015) 43(3):255–60. doi: 10.1007/s00240-015-0753-9
9. Ballesteros N, Snow ZA, Moscardi PRM, Ransford GA, Gomez P, Castellan M. Robotic management of urolithiasis in the pediatric population. Front Pediatr. (2019) 7:351. doi: 10.3389/fped.2019.00351
10. Sforza S, Muto G, Lambertini L, Maida FD, Grosso AA, Salvi M, et al. Robotic surgery for ureteropelvic junction obstruction and urolithiasis. Minerva Urol Nephrol. (2022) 74(3):384–6. doi: 10.23736/S2724-6051.21.04617-6
11. Rivas JG, y Gregorio SA, Sánchez LC, Portella PF, Barthel JJP. Evolution in the treatment of the ureteropelvic junction obstruction syndrome. Laparoscopic versus open pyeloplasty. Cent European J Urol. (2015) 68(3):384–8. doi: 10.1016/j.eururo.2015.05.004
12. Hong P, Li Z, Zhu D, Zhuang L, Yang K, Hao H, et al. A simple modification for the usage of flexible cystoscope in modified laparoscopic pyeloplasty for ureteropelvic junction obstruction with renal calculi: a flexible guiding tube. Urol Int. (2019) 102(3):262–8. doi: 10.1159/000495569
13. An L, Xiong L, Chen L, Ye XJ, Huang XB. Concomitant treatment of ureteropelvic junction obstruction complicated by renal calculi with laparoscopic pyeloplasty and pyelolithotomy via 19.5 F rigid nephroscope: a report of 12 cases. J Invest Surg. (2022) 35(1):77–82. doi: 10.1080/08941939.2020.1824248
14. Lambertini L, Sforza S, Tuccio A, Crisci A, Masieri L. Ureteropelvic Junction Obstruction with urolithiasis: experience from a single tertiary referral center of robotic assisted pyeloplasty with endoscopic removal of stones. Eur Urol Open Sci. (2020) 20:S72–3. doi: 10.1016/S2666-1683(20)35416-1
Keywords: ureteropelvic junction obstruction, flexible cystoscope, kidney stone, retroperitoneoscopy, pyeloplasty
Citation: Zhang F, Wang L, Gao Z and Yang H (2022) Retroperitoneoscopic pyeloplasty with simultaneous pyelolithotomy using a flexible cystoscope: Our initial experience at a single centre. Front. Surg. 9:938911. doi: 10.3389/fsurg.2022.938911
Received: 8 May 2022; Accepted: 11 July 2022;
Published: 19 August 2022.
Edited by:
Richard Naspro, San Matteo Hospital Foundation (IRCCS), ItalyReviewed by:
Lorenzo Masieri, Meyer Children's Hospital, Italy© 2022 Zhang, Wang, Gao and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: HouMeng Yang eWhtNjMyODgwQDE2My5jb20=
Specialty Section: This article was submitted to Genitourinary Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.