 Shujun Yu1
Shujun Yu1 Song Wang
Song Wang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 13 September 2022
Sec. Orthopedic Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.924585
This article is part of the Research TopicInsights in Orthopedic Surgery: 2021View all 10 articles
Purpose: The purpose of this study was to identify which of the risk factors would contribute to the contralateral fracture in very elderly patients after intramedullary nail fixation.
Methods: Clinical data of 227 intertrochanteric fracture patients aged 80 years or older were retrospectively reviewed. Intramedullary nails (IMNs) were used on all of the patients. Potential risk factors for contralateral hip refractures were determined using univariate and logistic regression analyses.
Results: Contralateral hip refractures occurred in 11 patients (4.84%). Univariate analysis revealed that age, gender, body mass index, fracture classification, hematocrit, D-dimer, and CRP level were not associated with contralateral fractures (P > 0.05). However, neurological diseases, cardiovascular disease, and visual impairments were significantly associated with contralateral fractures (P < 0.05). Multivariate analysis further revealed that neurological diseases (OR 4.25, P = 0.044) and visual impairments (OR 5.42, P = 0.015) were independent risk factors associated with contralateral refractures.
Conclusion: To prevent contralateral refractures, more attention should be paid to elderly intertrochanteric fracture patients with underlying neurological disease and visual impairments.
Hip fractures remain a worldwide epidemic and costly injury in the elderly, and the number of patients will increase significantly in the future (1, 2). Some investigational data have shown that between 1.2% and 9% of patients who have a hip fracture will suffer a contralateral refracture within 1 year (3, 4) and up to 20% in the course of their lives (5–7). Second contralateral fractures are related to significantly higher complication rates, socioeconomic cost, and mortality than the first fractures (8–11).
Associations between several risk factors and contralateral fractures have been reported, including gender, osteoporosis, body mass index (BMI), dementia, diabetes, and heart disease (12, 13). In general, patients aged over 80 years are more susceptible to medical comorbidities and possibly at high risk of contralateral fracture (14, 15). Another characteristic of elderly patients is that advanced age is more strongly associated with the risk of intertrochanteric fractures than femoral neck fractures, and intramedullary nails (IMNs) are recommended for fixation (16–18). Some studies, for example, on femoral neck fractures, have revealed that specific fixation methods are associated with a different risk of second hip fracture (19–22). One possible explanation is that surgical fixation may alter an individual’s gait and subsequently increase the fall risk by changing muscle moment and bone structure at the fracture site (23). Similarly, for intertrochanteric fractures, intramedullary nailing has been shown to alter the strength of hip muscles and the walking gait (24, 25). However, no research has been able to determine the IMN relative risk for contralateral refractures, especially in patients of advanced age. We hypothesized that the incidence and risk factors of these patients might differ from those of the general population. The aim is to explore potential contralateral fracture risk factors for intertrochanteric fracture patients who aged over 80 years and were treated with intramedullary nails.
Medical records of 227 eligible patients who had been treated for intertrochanteric fracture in our institution from January 2019 to January 2021 were retrospectively reviewed. In the study, intertrochanteric fractures were classified using AO/OTA criteria (26, 27). The inclusion criteria are as follows: (1) ≥80 years old; (2) intertrochanteric fractures; and (3) stabilized with proximal femur nail antirotation (PFNA). Patients with the following conditions were excluded: (1) hip fractures caused by high-energy trauma; (2) open fractures; (3) pathological fractures caused by bone tumors; and (4) incomplete clinical information. The involvers were monitored until a contralateral hip fracture occurred until February 2022. The study was reviewed and approved by the Ethics Committee of our institution.
Various parameters were analyzed to identify potential risk factors for contralateral refractures. The following clinical information is carefully extracted from their clinical data: age, gender, body height/weight, BMI, living circumstances, fracture site, and classification. Comorbidities are categorized as follows: hypertension, cardiovascular disease, diabetes mellitus, respiratory disease, neurological diseases, and visual impairments. The category of cardiovascular disease included coronary atherosclerotic heart disease, cardiomyopathy, heart failure, and arrhythmia. Respiratory diseases included bronchiectasis, pulmonary tuberculosis, chronic obstructive obstructive pulmonary disease (COPD), chronic bronchitis, and bronchial asthma. The category of neurological diseases included dementia, Parkinson’s disease, intracerebral hemorrhage, and stroke. Cataract, diabetic retinopathy, retinal neurodegeneration, and glaucoma are all examples of visual impairments. Surgical information included time from fracture to surgery, operation time, and intraoperative blood loss (ml). Peripheral blood samples were collected for laboratory tests including hematocrit (HCT), hemoglobin levels, D-dimer, and C-reactive protein (CRP).
Continuous data were presented as mean ± standard; categorical data were expressed as frequencies. Statistical analyses were performed using Student’s t-test or χ2 test relatively. Multivariate analysis was performed using logistic regression analysis to determine the risk factors, and results were presented as the odds ratios (OR) by 95% confidence interval (CI). P < 0.05 was considered statistically significant.
The general clinical features of the two groups are presented in Table 1. A total of 234 patients were enrolled in the study; 7 patients were excluded due to a lack of data on whether a contralateral hip fracture occurred. A total of 227 individuals were finally included, including 75 males and 152 females. Contralateral hip refractures occurred in 11 patients (4.84%) within 1 year after the surgery, including 1 male patient and 10 female patients. Each of the 11 patients had a history of falling and sustaining an injury.
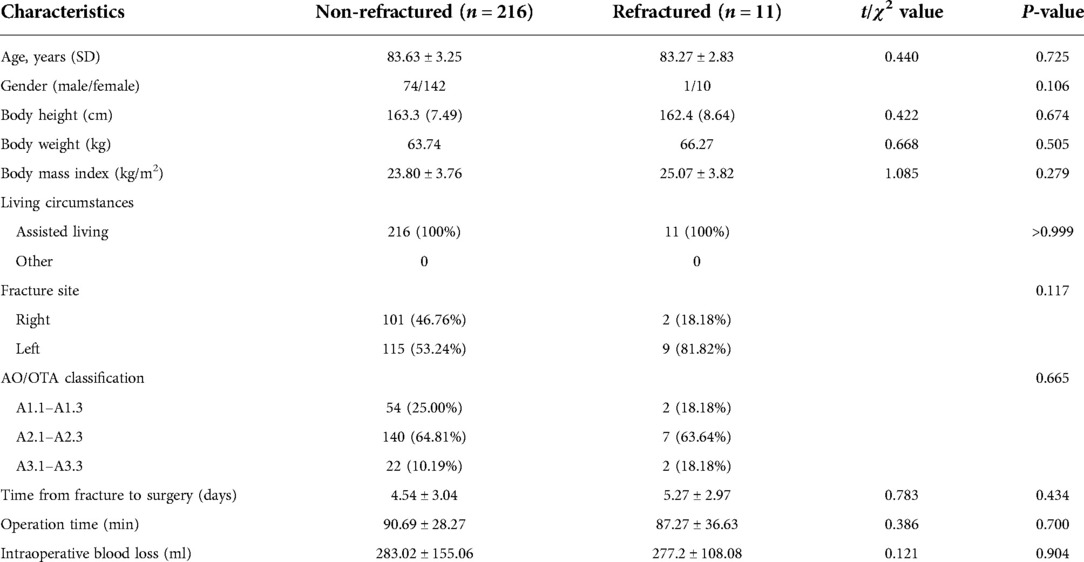
Table 1. Comparison of baseline data between the two groups.
The baseline data from the two groups were compared. No significant differences were found in age, gender, BMI, fracture site, AO/OTA classification, time from fracture to surgery, operation time, and intraoperative blood loss between the contralateral fracture and nonfractured patients (P > 0.05).
There was no significant statistical difference between the 11 patients and the 216 controls when preoperative and postoperative laboratory tests of hematocrit, D-dimer level, and C-reactive protein level were examined (P > 0.05; Table 2). In addition, no statistical difference was founded in hemoglobin levels between the contralateral fracture and nonfractured patients (P > 0.05).
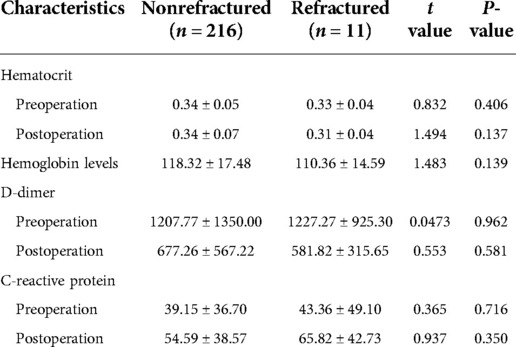
Table 2. Comparison of laboratory tests between the two groups.
For comorbid medical diseases, contralateral fracture patients had higher rates of hypertension, cardiovascular disease, neurological diseases, respiratory disease, and visual impairments than the control group (Table 3). However, only visual impairments and neurological and cardiovascular diseases were seen as significantly different between the two groups (P < 0.05).
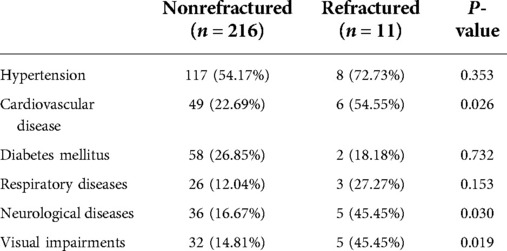
Table 3. Comparison of comorbidity between the two groups.
Univariate analysis revealed that demographic characteristics, fracture features, and laboratory tests were not associated with contralateral fractures. However, neurological diseases, cardiovascular disease, and visual impairments were significantly associated with contralateral fractures. Multivariate analysis further revealed that visual impairments (OR 5.42, P = 0.015) and neurological diseases (OR 4.25, P = 0.044) were independent risk factors for contralateral hip refractures (Table 4).
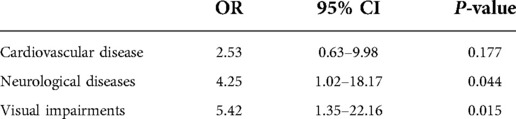
Table 4. Univariate and multivariate analyses of factors.
Contralateral hip refractures are associated with major clinical and social cost implications (4, 11, 28, 29). How to develop effective preventive strategies for hip fracture patients is still under controversy (13). Recently, reports have raised the question of whether specific surgical fixation of the initial hip fracture is associated with a different risk of subsequent contralateral fracture. Souder et al. (22) found an increased risk of hip refractures in patients who underwent closed reduction and percutaneous puncture compared to those who underwent arthroplasty. Changes in individual’s gait and subsequent fall risk due to different fixation methods may be one of the important reasons (23, 24). To our knowledge, no research has determined the IMN relative risk of contralateral hip refractures, especially in patients of advanced age.
Our results showed that 11 in 227 patients (4.84%) suffered a contralateral hip refracture during the data collection period. The incidence correlated with the risk of 3%–10% for second hip refractures (3, 20, 30, 31). In general, elderly patients are prone to contralateral fractures due to osteoporosis and susceptible to medical comorbidities (15). However, only a few studies have reported the age-specific incidence and risk factors for contralateral fractures. Yamanashi et al. (32) reported that the incidence was 3.8% within the first year in patients aged ≥65 years. Similarly, Lönnroos et al. (33) noted an incidence of 5.08% for patients aged ≥60 years within the first year, and the rate increased further to 8.11% at 2 years following the initial fracture. For very elderly patients, Vochteloo et al. (34) found that the incidence of patients aged over 85 years was not different from other age categories. Lawrence et al. (35) also found female patients over the age of 84 years have a similar risk to the general population. Similarly, our results showed that the incidence of patients aged over 80 years was not significantly increased compared to previous hip refracture data. One theoretical explanation is that the increasing age of patients is not exclusively related to bone strength loss. Indeed, Gnudi et al. (36) suggested that bone loss will gradually slow down after the age of 65 years. Moreover, we noted that none of the enrolled patients lived alone and had a reduced range of physical activity, which may have reduced the risk of falls, which are a major cause of hip fractures.
To further identify risk factors, we evaluated the difference between the patients who suffered a contralateral hip fracture and those in the control group. Univariate analysis revealed that gender distribution, BMI, fracture classification, operation time, and intraoperative blood loss were not associated with contralateral fractures. Although some authors have emphasized the relationship between gender and second hip fractures (7, 31), our study did not support this suggestion. Similar to our results, no significant gender difference was also seen in previous studies (15, 33, 34, 37, 38).
At present, few publications have emphasized the value of laboratory-based indicators for contralateral fracture risk. Preoperative CRP was found to be a primary risk factor for postoperative death in elderly patients with hip fractures in a recent study (39). Chen et al. (37) reported that the serum CRP/Alb ratio is a risk factor in elderly hip fracture patients treated by total hip arthroplasty. In our study, there was no difference between the patient’s preoperative and postoperative laboratory tests of hematocrit, D-dimer level, and CRP level between the two groups. Traumatic stress and perioperative drugs all affect the level of expression of these inflammatory and nutritional indicators in the perioperative period (40); therefore, their significance in contralateral fracture needs to be further evaluated.
An increased risk of contralateral hip refractures has been found to be associated with several comorbid diseases (12, 13, 38, 41–43), including hypertension, diabetes mellitus, cardiovascular disease, neurological diseases, respiratory diseases, and visual impairments. In our study, neurological diseases and visual impairments were found to be significantly associated with contralateral hip refractures. Although contralateral fracture patients had higher rates of hypertension, cardiovascular disease, and respiratory diseases than the control group, differences were only seen in neurological diseases, cardiovascular disease, and visual impairments using univariate analysis. Multivariate analysis revealed that neurological diseases and visual impairments were independent risk factors for contralateral hip refractures. Risk factors determined in our study can aid in identifying high-risk populations among very elderly intertrochanteric fracture patients. However, our research also has some limitations. Some clinical information was collected retrospectively, and a relatively small population was the study's main limitation. This may have led to a bias in the analysis of the incidence of contralateral fractures. In addition, some potentially meaningful items, such as the clinical data on vitamin D levels and the use of bone health medications (vitamin D, bisphosphonates, trospium) were not available for all patients, so this was not analyzed in the study.
In summary, neurological diseases and underlying visual impairments are risk factors for contralateral hip refractures in intertrochanteric fracture patients aged over 80 years and who were treated with intramedullary nails. More attention should be given to the patients with these underlying comorbidities.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Ethics Committee of Tianjin Hospital. The patients/participants provided their written informed consent to participate in this study.
SY and SW designed the study. CL, YZ, and JZ collected clinical data and performed statistical analysis. ZZ and SW wrote the manuscript. SY and YZ revised the manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the Beijing Medical and Health Foundation (B20664FN).
The authors would like to thank all the participants and researchers who participated in this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rapp K, Büchele G, Dreinhöfer K, Bücking B, Becker C, Benzinger P. Epidemiology of hip fractures. Z Gerontol Geriat. (2019) 52:10–6. doi: 10.1007/s00391-018-1382-z
2. van Leendert JAA, Linkens AEMJH, Poeze M, Pijpers E, Magdelijns F, Ten Broeke RHM, et al. Mortality in hip fracture patients after implementation of a nurse practitioner-led orthogeriatric care program: results of a 1-year follow-up. Age Ageing. (2021) 50:1744–50. doi: 10.1093/ageing/afab031
3. Chang J-D, Yoo J-H, Reddy P, Lee S-S, Hwang J-H, Kim T-Y. Risk factors for contra-lateral hip fracture in elderly patients with previous hip fracture. Injury. (2013) 44:1930–3. doi: 10.1016/j.injury.2013.03.034
4. Ho AWH, Wong SH. Second hip fracture in Hong Kong - incidence, demographics, and mortality. Osteoporos Sarcopenia. (2020) 6:71–4. doi: 10.1016/j.afos.2020.05.004
5. Berry SD, Samelson EJ, Hannan MT, McLean RR, Lu M, Cupples LA, et al. Second hip fracture in older men and women: the framingham study. Arch Intern Med. (2007) 167:1971–6. doi: 10.1001/archinte.167.18.1971
6. Chapurlat RD, Bauer DC, Nevitt M, Stone K, Cummings SR. Incidence and risk factors for a second hip fracture in elderly women. The study of osteoporotic fractures. Osteoporos Int. (2003) 14:130–6. doi: 10.1007/s00198-002-1327-6
7. Lau JCF, Ho KW, Sadiq S. Patient characteristics and risk of subsequent contralateral hip fracture after surgical management of first fracture. Injury. (2014) 45:1620–3. doi: 10.1016/j.injury.2014.05.030
8. Müller F, Galler M, Zellner M, Bäuml C, Roll C, Füchtmeier B. Comparative analysis of non-simultaneous bilateral fractures of the proximal femur. Eur J Trauma Emerg Surg. (2019) 45:1053–7. doi: 10.1007/s00068-018-0981-0
9. Sawalha S, Parker MJ. Characteristics and outcome in patients sustaining a second contralateral fracture of the hip. J Bone Joint Surg Br. (2012) 94:102–6. doi: 10.1302/0301-620X.94B1.27983
10. Sobolev B, Sheehan KJ, Kuramoto L, Guy P. Excess mortality associated with second hip fracture. Osteoporos Int. (2015) 26:1903–10. doi: 10.1007/s00198-015-3104-3
11. van der Steenhoven TJ, Staffhorst B, Van de Velde SK, Nelissen RGHH, Verhofstad MHJ. Complications and institutionalization are almost doubled after second hip fracture surgery in the elderly patient. J Orthop Trauma. (2015) 29:e103–8. doi: 10.1097/BOT.0000000000000233
12. Zhu Y, Chen W, Sun T, Zhang Q, Cheng J, Zhang Y. Meta-analysis of risk factors for the second hip fracture (SHF) in elderly patients. Arch Gerontol Geriatr. (2014) 59:1–6. doi: 10.1016/j.archger.2014.02.012
13. Liu S, Zhu Y, Chen W, Sun T, Cheng J, Zhang Y. Risk factors for the second contralateral hip fracture in elderly patients: a systematic review and meta-analysis. Clin Rehabil. (2015) 29:285–94. doi: 10.1177/0269215514542358
14. Maruhashi T, Kajikawa M, Kishimoto S, Hashimoto H, Takaeko Y, Yamaji T, et al. Vascular function is further impaired in subjects aged 80 years or older. Hypertens Res. (2020) 43:914–21. doi: 10.1038/s41440-020-0435-z
15. Angthong C, Suntharapa T, Harnroongroj T. Major risk factors for the second contralateral hip fracture in the elderly. Acta Orthop Traumatol Turc. (2009) 43:193–8. doi: 10.3944/AOTT.2009.193
16. Karagas MR, Lu-Yao GL, Barrett JA, Beach ML, Baron JA. Heterogeneity of hip fracture: age, race, sex, and geographic patterns of femoral neck and trochanteric fractures among the US elderly. Am J Epidemiol. (1996) 143:677–82. doi: 10.1093/oxfordjournals.aje.a008800
17. Baudoin C, Fardellone P, Sebert JL. Effect of sex and age on the ratio of cervical to trochanteric hip fracture. A meta-analysis of 16 reports on 36,451 cases. Acta Orthop Scand. (1993) 64:647–53. doi: 10.3109/17453679308994590
18. Niu E, Yang A, Harris AHS, Bishop J. Which fixation device is preferred for surgical treatment of intertrochanteric hip fractures in the United States? A survey of orthopaedic surgeons. Clin Orthop Relat Res. (2015) 473:3647–55. doi: 10.1007/s11999-015-4469-5
19. Shabat S, Gepstein R, Mann G, Kish B, Fredman B, Nyska M. The second hip fracture–an analysis of 84 elderly patients. J Orthop Trauma. (2003) 17:613–7. doi: 10.1097/00005131-200310000-00003
20. Dretakis KE, Dretakis EK, Papakitsou EF, Psarakis S, Steriopoulos K. Possible predisposing factors for the second hip fracture. Calcif Tissue Int. (1998) 62:366–9. doi: 10.1007/s002239900446
21. Yoshii I, Kitaoka K, Hashimoto K. Clinical characteristics of osteoporotic second hip fracture: from the data of clinical pathway with regional alliance in rural region in Japan. J Orthop Sci. (2019) 24:836–41. doi: 10.1016/j.jos.2018.12.029
22. Souder CD, Brennan ML, Brennan KL, Song J, Williams J, Chaput C. The rate of contralateral proximal femoral fracture following closed reduction and percutaneous pinning compared with arthroplasty for the treatment of femoral neck fractures. J Bone Joint Surg Am. (2012) 94:418–25. doi: 10.2106/JBJS.J.01134
23. Zlowodzki M, Ayeni O, Ayieni O, Petrisor BA, Bhandari M. Femoral neck shortening after fracture fixation with multiple cancellous screws: incidence and effect on function. J Trauma. (2008) 64:163–9. doi: 10.1097/01.ta.0000241143.71274.63
24. Güven M, Kocadal O, Akman B, Poyanlı OS, Kemah B, Atay EF. Proximal femoral nail shows better concordance of gait analysis between operated and uninjured limbs compared to hemiarthroplasty in intertrochanteric femoral fractures. Injury. (2016) 47:1325–31. doi: 10.1016/j.injury.2016.03.009
25. Noda M, Saegusa Y, Takahashi M, Takada Y, Fujita M, Shinohara I. Decreased postoperative gluteus medius muscle cross-sectional area measured by computed tomography scan in patients with intertrochanteric fractures nailing. J Orthop Surg. (2017) 25:2309499017727943. doi: 10.1177/2309499017727943
26. Orthopaedic Trauma Association Committee for Coding and Classification. Fracture and dislocation compendium. J Orthop Trauma. (1996) v–ix(10 Suppl 1):1–154. PMID: 8814583
27. Marsh JL, Slongo TF, Agel J, Scott Broderick J, Creevey W, DeCoste TA, et al. Fracture and dislocation classification compendium 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. (2007) 21:S1–S6. doi: 10.1097/00005131-200711101-00001
28. Hagino H. Current and future burden of hip and vertebral fractures in Asia. Yonago Acta Med. (2021) 64:147–54. doi: 10.33160/yam.2021.05.001
29. Mazzucchelli R, Pérez-Fernández E, Crespí N, García-Vadillo A, Rodriguez Caravaca G, Gil de Miguel A, et al. Second hip fracture: incidence, trends, and predictors. Calcif Tissue Int. (2018) 102:619–26. doi: 10.1007/s00223-017-0364-2
30. Kaper BP, Mayor MB. Incidence of bilateral proximal femoral fractures in a tertiary care center. Orthopedics. (2001) 24:571–4. doi: 10.3928/0147-7447-20010601-14
31. Gaumetou E, Zilber S, Hernigou P. Non-simultaneous bilateral hip fracture: epidemiologic study of 241 hip fractures. Orthop Traumatol Surg Res. (2011) 97:22–7. doi: 10.1016/j.otsr.2010.07.011
32. Yamanashi A, Yamazaki K, Kanamori M, Mochizuki K, Okamoto S, Koide Y, et al. Assessment of risk factors for second hip fractures in Japanese elderly. Osteoporos Int. (2005) 16:1239–46. doi: 10.1007/s00198-005-1835-2
33. Lönnroos E, Kautiainen H, Karppi P, Hartikainen S, Kiviranta I, Sulkava R. Incidence of second hip fractures. A population-based study. Osteoporos Int. (2007) 18:1279–85. doi: 10.1007/s00198-007-0375-3
34. Vochteloo AJH, Borger van der Burg BLS, Röling MA, van Leeuwen DH, van den Berg P, Niggebrugge AHP, et al. Contralateral hip fractures and other osteoporosis-related fractures in hip fracture patients: incidence and risk factors. An observational cohort study of 1,229 patients. Arch Orthop Trauma Surg. (2012) 132:1191–7. doi: 10.1007/s00402-012-1520-9
35. Lawrence TM, Wenn R, Boulton CT, Moran CG. Age-specific incidence of first and second fractures of the hip. J Bone Joint Surg Br. (2010) 92:258–61. doi: 10.1302/0301-620X.92B2.23108
36. Gnudi S, Sitta E, Fiumi N. Bone density and geometry in assessing hip fracture risk in post-menopausal women. Br J Radiol. (2007) 80:893–7. doi: 10.1259/bjr/37401526
37. Chen L, Zhang J, Zhang W, Deng C. Correlation between C-reactive protein/albumin and contralateral hip refracture after total hip arthroplasty in elderly patients with hip fractures. Ann Palliat Med. (2020) 9:1055–61. doi: 10.21037/apm-20-855
38. Juhász K, Boncz I, Patczai B, Mintál T, Sebestyén A. Risk factors for contralateral hip fractures following femoral neck fractures in elderly: analysis of the Hungarian nationwide health insurance database. Eklem Hastalik Cerrahisi. (2016) 27:146–52. doi: 10.5606/ehc.2016.30
39. Kim B-G, Lee Y-K, Park H-P, Sohn H-M, Oh A-Y, Jeon Y-T, et al. C-reactive protein is an independent predictor for 1-year mortality in elderly patients undergoing hip fracture surgery: a retrospective analysis. Medicine. (2016) 95:e5152. doi: 10.1097/MD.0000000000005152
40. Eriksson AL, Movérare-Skrtic S, Ljunggren Ö, Karlsson M, Mellström D, Ohlsson C. High-sensitivity CRP is an independent risk factor for all fractures and vertebral fractures in elderly men: the MrOS Sweden study. J Bone Miner Res. (2014) 29:418–23. doi: 10.1002/jbmr.2037
41. Fukushima T, Sudo A, Uchida A. Bilateral hip fractures. J Orthop Sci. (2006) 11:435–8. doi: 10.1007/s00776-006-1056-3
42. Lee Y-K, Ha Y-C, Yoon B-H, Koo K-H. Incidence of second hip fracture and compliant use of bisphosphonate. Osteoporos Int. (2013) 24:2099–104. doi: 10.1007/s00198-012-2250-0
Keywords: contralateral hip refracture, intertrochanteric fracture, intramedullary nails, elderly patients, refractures
Citation: Yu S, Li C, Zhong Y, Zang J, Zhou Z, Wang S and Zhang Y (2022) Risk factors for contralateral hip refractures in patients aged over 80 years with intertrochanteric femoral fractures. Front. Surg. 9:924585. doi: 10.3389/fsurg.2022.924585
Received: 20 April 2022; Accepted: 22 August 2022;
Published: 13 September 2022.
Edited by:
Chenchen Yan, Huazhong University of Science and Technology, ChinaReviewed by:
Ashley Levack, Loyola University Chicago, United States© 2022 Yu, Li, Zhong, Zang, Zhou, Wang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Song Wang bXJ3YW5nc25nQDE2My5jb20= Yinguang Zhang MTM4MjA3NzA3NjhAMTYzLmNvbQ==
Specialty Section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.