 Li Zhang1
Li Zhang1 Luyuan Tao
Luyuan Tao Youyou Zhang
Youyou Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 07 June 2022
Sec. Visceral Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.891047
This article is part of the Research Topic Co-use of medicines in surgery View all 114 articles
Purpose: To explore the risk factors of ischemia reperfusion injury (IRI) after percutaneous coronary intervention (PCI) in patients with acute ST-segment elevation myocardial infarction (STEMI) and its influence on prognosis.
Methods: The clinical data of 80 patients with STMEI undergoing PCI in our hospital from June 2020 to June 2021 were collected. According to whether IRI occurred after PCI, STMEI patients were divided into IRI group and non-IRI group. The basic information, clinical characteristics, examination parameters and other data of all patients were collected, and the prognosis of the two groups was observed. Risk factors were analyzed by fitting binary Logistic regression model. The survival prognosis was analyzed by Kaplan-Meier survival curve.
Results: Logistic regression analysis showed that type 2 diabetes mellitus (T2DM), pre-hospital delay time (PHD) and door-to-balloon expansion time (DTB) were the influencing factors of IRI in patients with STMEI (p < 0.05). MACE occurred in 11 cases (32.35%) in the IRI group and 13 cases (28.26%) in the non-IRI group. Log-rank test showed p = 0.503, indicating no statistically significant difference.
Conclusion: T2DM, PHD and DTB were the influencing factors of IRI in patients with STMEI, and IRI will not reduce the prognosis of patients.
ST-segment elevation myocardial infarction (STEMI) is mainly caused by unstable plaque detachment in coronary artery to form thrombus, which leads to acute myocardial ischemia and necrosis. The main clinical symptoms are persistent ischemic chest pain, elevated serum myocardial injury markers and elevation of ST segment of electrocardiogram (1). STEMI has an acute onset and rapid onset. Patients may suffer from myocardial injury and necrosis in a short period of time, even death in severe cases, which poses a serious threat to the life and health of patients (2). With the continuous development of medical technology, the early mortality of STEMI in clinic has dropped significantly, from 13% in 1986 to <4% in 2000, which is mainly due to the application of early opening of infarction-related vascular technology (3). Percutaneous coronary intervention (PCI) is the most common method for the treatment of STEMI. It can recanalize infarct-related arteries, restore myocardial perfusion and restore blood supply, and has been widely carried out in China (4). However, with the deepening of relevant research, scholars have found that effective reperfusion therapy may not only restore the forward blood flow of infarct-related arteries, but also lead to the further aggravation of myocardial ischemic injury, that is, ischemia reperfusion injury (IRI) (5). IRI can be manifested as severe slow arrhythmia, malignant ventricular arrhythmia, cardiac insufficiency and sudden drop of blood pressure after vascular opening, resulting in acute and chronic organ failure, even sudden death, which affects postoperative recovery, so it has been widely valued by doctors in recent years (6). Therefore, it is particularly important to identify the risk factors of IRI in STEMI patients as early as possible clinically. We aim to observe the influencing factors of IRI in STEMI patients after PCI, and whether the occurrence of IRI affects the prognosis of patients.
The clinical data of 80 patients with STMEI undergoing PCI in our hospital from June 2020 to June 2021 were collected. According to whether IRI occurred after PCI, STMEI patients were divided into two groups: 34 cases in IRI group and 46 cases in non-IRI group. Inclusion criteria: Patients meet the diagnostic criteria of STMEI (7); The duration of onset of chest pain ≥30 min; The patient can accurately tell the doctor the specific time of onset; Complete clinical data. Exclusion criteria: those who failed to receive PCI treatment within 12 h of onset due to various reasons; Coronary angiography confirmed incomplete occlusion of criminals’ blood vessels; Patients who died during PCI or 24 h after PCI; Patients with active visceral hemorrhage, cardiogenic shock; Liver and renal insufficiency; Combined with malignant tumor.
The diagnostic criteria of IRI were as follows: ① Severe bradycardia, hypotension and frequent premature ventricular contractions within minutes after opening coronary artery vessels during interventional therapy; ② Serious ventricular arrhythmias still occur after drug therapy and/or electrocardioversion and electrodefibrillation; ③ coronary angiography detected coronary angiography TIMI ≤ grade 2, combined with thrombus, dissection or spasm.
All patients received comprehensive treatment measures before operation such as oxygen inhalation, sedation, analgesia, ECG monitoring. The patients were treated with nitrates, β-blockers, heparin and angiotensin converting enzyme inhibitors. Within 12 h of onset, PCI was completed under the guidance of angiography system. Routine percutaneous puncture of the radial artery or femoral artery, coronary angiography was performed, and after the coronary artery disease was identified, the location of the infarction-related artery disease was determined, stent placement was performed, and PCI treatment was completed immediately. PCI was performed by experienced physicians. All patients were treated with double antiplatelet aggregation therapy after operation. If there were no contraindications, nitrates, β -blockers and other drugs were added.
The clinical data of all patients were collected, including: ① age, sex, hypertension, type 2 diabetes mellitus (T2DM), hyperlipidemia, smoking history (>20 cigarettes/day) and alcoholism history (>150 mg/day); ② Admission systolic blood pressure, admission diastolic blood pressure, admission heart rate, pre-hospital delay time (PHD) and door-to-balloon expansion time (DTB); ③ White blood cell count (WBC), platelet count (PLT), total cholesterol (TC) and low density lipoprotein cholesterol (LDL-C) at admission.
Telephone and outpatient follow-up were conducted 6 months after operation to record the prognosis of patients, including major adverse cardiovascular events (MACE) such as readmission, recurrent myocardial infarction, revascularization, fatal arrhythmia, heart failure, stroke, bleeding of vital organs and cardiogenic death. Patients who died or lost follow-up during the follow-up period were excluded.
Used SPSS 22.0 software to process. The measurement data was expressed by mean ± standard deviation, and the comparison was made by t test. The count data are expressed by ratio, and the comparison is made by χ2 test. Risk factors were analyzed by fitting binary Logistic regression model. The survival prognosis was analyzed by Kaplan-Meier survival curve, and the comparison was made by Log-rank test. Inspection level α = 0.05.
There were significant differences in hypertension and T2DM between IRI group and non-IRI group (p < 0.05) (Table 1).
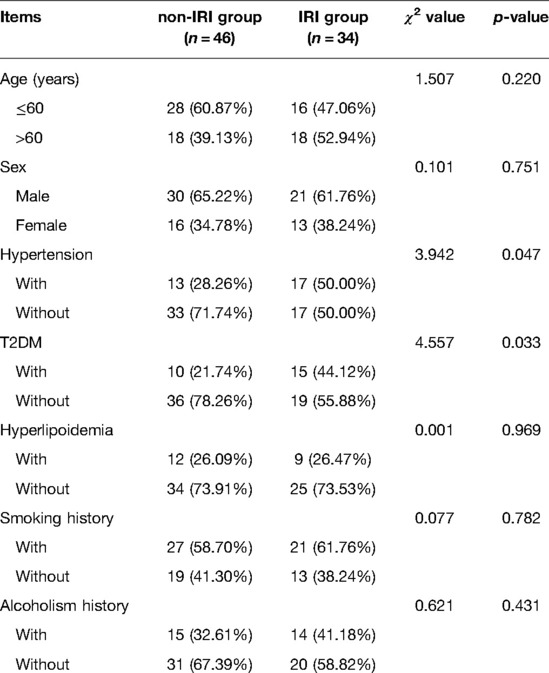
Table 1. Basic information of patients (n,%).
There were significant differences in PHD and DTB between IRI group and non-IRI group (p < 0.05) (Table 2).

Table 2. Clinical characteristics of patients (n, , %).
There was no significant difference in WBC, PLT, TC and LDL-C between IRI group and non-IRI group (p > 0.05) (Table 3).
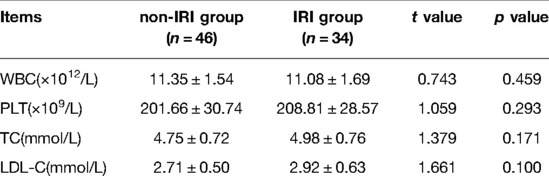
Table 3. Examination parameters of patients (n, ).
Logistic regression analysis showed that T2DM, PHD and DTB were the influencing factors of IRI in patients with STMEI (p < 0.05) (Tables 4, 5).
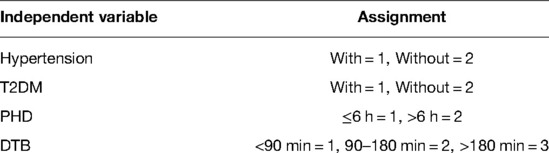
Table 4. Multi-factor assignment.
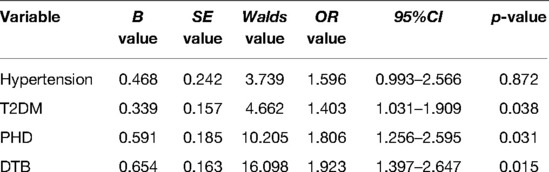
Table 5. Multivariate analysis of IRI in patients with STMEI.
As of January 2022, all patients were followed up. MACE occurred in 11 cases (32.35%) in the IRI group and 13 cases (28.26%) in the non-IRI group. Log-rank test showed p = 0.503, indicating no statistically significant difference (Figure 1).
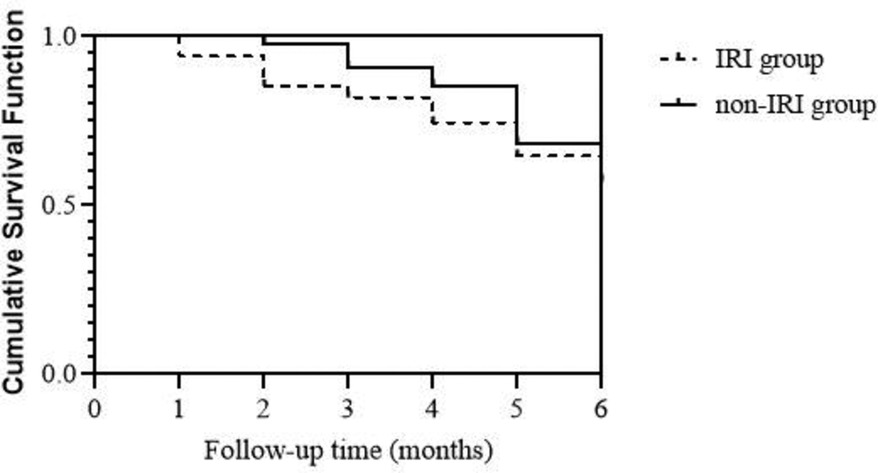
Figure 1. Follow-up of patients.
STEMI can cause arrhythmia, myocardial injury and other symptoms, and severe conditions can endanger the patient’s life. PCI can open infarct-related vessels and restore distal myocardial perfusion, which is an efficient and safe treatment for STEMI (8). PCI for STEMI patients can restore the effective blood supply of coronary artery as soon as possible. However, reperfusion therapy after ischemia may further cause myocardial injury, which can seriously affect the surgical efficacy and prognosis. The main mechanisms of IRI are oxidative stress, intracellular calcium overload, destruction of microvascular structure and function, and opening of mitochondrial membrane permeability transformation pores (9, 10). Therefore, exploring the related factors of IRI has becomes an important issue to prevent the occurrence of IRI in STEMI patients after PCI.
This study found that T2DM is the influencing factor of IRI in patients with STMEI. Literature reports at home and abroad show that there are inconsistent research results on the issue of DM on IRI. Dia’s team research showed that patients without DM often fail to establish a good collateral circulation before acute occlusion due to their previous health and lack of long-term chronic myocardial ischemia preconditioning before acute occlusion of criminals’ blood vessels. Therefore, compared with STEMI patients with DM, patients without DM have stronger reaction to acute ischemic injury and are more prone to IRI (11). Muráriková’ s team believed that because the heart of DM patients may adapt to the changes caused by DM and increase tolerance to ischemic injury, the recovery of DM patients after IRI is better than that of patients without DM, with fewer cardiovascular events (12). However, there are also different research results on the relationship between DM and IRI in clinic. Badalzadeh’s team found that STEMI patients with DM have a higher risk of IRI, which may be due to the combined effects of changes of glucose and lipid energy metabolism based on insulin resistance, enhanced oxidative stress and systemic inflammatory responses and ion channel dysfunction (13). Some scholars also believe that long-term chronic hyperglycemia can affect the function and structure of platelets, damage vascular endothelial cells, cause microvascular lesions, and weaken the repair ability of vascular endothelial cells, leading to coronary circulation disorder. DM is one of the main causes of IRI (14). In addition, it has been reported that T2DM has a series of metabolic syndromes caused by insulin resistance, while T1DM does not have insulin resistance in the early stage, and with the prolongation of the disease course, T1DM also gradually develops insulin resistance. Clinically, DM patients with STEMI undergoing PCI often have a long course of disease, and almost all of them have insulin resistance, so the IRI is seriously damaged (15, 16).
In this study, under the condition of PHD ≤ 6 h and DTB < 90 min, the probability of IRI in patients with STMEI is small, while when PHD exceeds 6 h and DTB exceeds 180 min, the probability of IRI is significantly increased. Guidelines have shown that opening occluded blood vessels within 12 h of onset of STMEI patients can have beneficial effects on the patient (17). There is a time window from acute coronary artery occlusion to transmural myocardial necrosis, which is about 6 h. Recanalization of coronary arteries within this time window can save ischemic myocardium on the verge of necrosis, promote the body to recover the forward blood flow and occlude blood vessels as soon as possible, and improve the myocardial microcirculation perfusion level (18, 19). The delay in the visit of patients with STMEI can seriously affect the follow-up cardiac function, and early seeing a doctor can provide patients with the opportunity to obtain a good prognosis. In addition, the earlier the treatment of the first balloon dilatation is performed, the greater the benefit of patients. Bruce’s team conducted a long-term follow-up of patients with acute myocardial infarction who underwent PCI. The results found that prolongation of DTB could increase the risk of in-hospital death and late death, and DTB > 2 h was an independent risk factor of death (20). De Luca’s team showed that with the delay of DTB, the one-year mortality rate of patients with STMEI increased, and the relative risk of death was 1.08 for every 30 min increase in DTB (21, 22). Scholars at home and abroad believe that DTB < 90 min is the best time for the first balloon dilatation, and the shortest DTB can greatly reduce the incidence of short-term and long-term adverse cardiac events after PCI (23, 24). Prehospital delays mainly include patient delays and transport delays. The patient delay is due to the patient’s lack of awareness of the visit to the clinic, which leads to the extension of PHD. Transport delay is due to the large number of patients in the hospital, which leads to a delay in the time of transfer and treatment. In clinical practice, out-of-hospital ECG can greatly shorten PHD and DTB, which is beneficial to quickly determine whether IRI occurs in STMEI patients, so as to make correct treatment decisions. At the same time, an in-hospital emergency service system composed of well-trained ambulance teams is also crucial. The development of the in-hospital emergency service system can avoid the transition of wards or coronary heart disease care units, thereby shortening the time for transferring patients in the hospital and further reducing DTB. In addition, medical staff need to strengthen the people’s awareness of STEMI, and identify and treat IRI in patients with STMEI as soon as possible.
In addition, we also found that the occurrence of IRI has no significant influence on whether there is MACE in patients with STMEI. The results suggest that although IRI may have some adverse effects on patients with STMEI, it is a pathophysiological change in a short time during myocardial reperfusion, and IRI in STMEI patients after PCI will not reduce the prognosis of patients. Medical staff need to improve the ability to identify the risk of IRI, and to carry out risk prevention and effective treatment for high-risk factors, without changing the treatment strategy due to IRI.
To sum up, T2DM, PHD and DTB were the influencing factors of IRI in patients with STMEI, and IRI will not reduce the prognosis of patients. This study is a single-center, small-sample study, and there is a lack of longer follow-up for patients. We need to improve the research scheme in the future.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by This study was approved by the ethics committee of our hospital. The patients/participants provided their written informed consent to participate in this study.
LZ and LW are the mainly responsible for the writing of the article. LT is mainly responsible for research design. CC is mainly responsible for data analysis. LZ and SR are responsible for the guidance of the entire research. The corresponding author is YZ and she is responsible for ensuring that the descriptions are accurate and agreed by all authors. All authors contributed to the article and approved the submitted version.
This study was supported by the Taizhou Social Development Science and Technology Plan Project (No: 21ywb46).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Govea A, Lipinksi J, Patel MP. Prehospital evaluation, ED management, transfers, and management of inpatient STEMI. Interv Cardiol Clin. (2021) 10:293–306. doi: 10.1016/j.iccl.2021.03.002
2. Aoun J, Kleiman NS, Goel SS. Diagnosis and management of late-presentation ST-elevation myocardial infarction and complications. Interv Cardiol Clin. (2021) 10:369–80. doi: 10.1016/j.iccl.2021.03.008
3. Hausenloy DJ, Yellon DM. Myocardial ischemia-reperfusion injury: a neglected therapeutic target. J Clin Invest. (2013) 123:92–100. doi: 10.1172/JCI62874
4. Giannini F, Candilio L, Mitomo S, Ruparelia N, Chieffo A, Baldetti L, et al. A Practical approach to the management of complications during percutaneous coronary intervention. JACC Cardiovasc Interv. (2018) 11:1797–810. doi: 10.1016/j.jcin.2018.05.052
5. Toldo S, Mauro AG, Cutter Z, Abbate A. Inflammasome, pyroptosis, and cytokines in myocardial ischemia-reperfusion injury. Am J Physiol Heart Circ Physiol. (2018) 315:H1553–68. doi: 10.1152/ajpheart.00158.2018
6. Konijnenberg LSF, Damman P, Duncker DJ, Kloner RA, Nijveldt R, van Geuns RM, et al. Pathophysiology and diagnosis of coronary microvascular dysfunction in ST-elevation myocardial infarction. Cardiovasc Res. (2020) 116:787–805. doi: 10.1093/cvr/cvz301
7. Thiele H, Desch S, de Waha S. Akuter myokardinfarkt bei patienten mit ST-strecken-hebungs-infarkt : ESC-leitlinien 2017 [acute myocardial infarction in patients with ST- segment elevation myocardial infarction: ESC guidelines 2017]. Herz. (2017) 42:728–38. doi: 10.1007/s00059-017-4641-7
8. Baralis G, Rossini R, Musumeci G. Antiplatelet therapy in STEMI undergoing primary PCI: when, which one and how long. Minerva Cardioangiol. (2018) 66:422–8. doi: 10.23736/S0026-4725.18.04640-6
9. Song YJ, Zhong CB, Wang XB. Heat shock protein 70: a promising therapeutic target for myocardial ischemia-reperfusion injury. J Cell Physiol. (2019) 234:1190–207. doi: 10.1002/jcp.27110
10. Al-Salam S, Hashmi S. Myocardial ischemia reperfusion injury: apoptotic, inflammatory and oxidative stress role of galectin-3. Cell Physiol Biochem. (2018) 50:1123–39. doi: 10.1159/000494539
11. Dia M, Paccalet A, Pillot B, Leon C, Ovize M, Crola Da Silva C, et al. Myocardial ischemia-reperfusion and diabetes: lessons learned from bedside to bench. Front Cardiovasc Med. (2021) 8:660698. doi: 10.3389/fcvm.2021.660698
12. Muráriková M, Ferko M, Waczulíková I, Jašová M, Kancirová I, Murínová J, et al. Changes in mitochondrial properties may contribute to enhanced resistance to ischemia-reperfusion injury in the diabetic rat heart. Can J Physiol Pharmacol. (2017) 95:969–76. doi: 10.1139/cjpp-2017-0211
13. Badalzadeh R, Azimi A, Alihemmati A, Yousefi B. Chronic type-I diabetes could not impede the anti-inflammatory and anti-apoptotic effects of combined postconditioning with ischemia and cy closporine A in myocardial reperfusion injury. J Physiol Biochem. (2017) 73:111–20. doi: 10.1007/s13105-016-0530-4
14. Cai L, Keller BB. Cardiac regeneration and diabetes. Regen Med Res. (2014) 2:1. doi: 10.1186/2050-490X-2-1
15. Russo I, Penna C, Musso T, Popara J, Alloatti G, Cavalot F, et al. Platelets, diabetes and myocardial ischemia/reperfusion injury. Cardiovasc Diabetol. (2017) 16:71. doi: 10.1186/s12933-017-0550-6
16. Kristiansen SB, Pælestik KB, Johnsen J, Jespersen NR, Pryds K, Hjortbak MV, et al. Impact of hyperglycemia on myocardial ischemia-reperfusion susceptibility and ischemic preconditioning in hearts from rats with type 2 diabetes. Cardiovasc Diabetol. (2019) 18:66. doi: 10.1186/s12933-019-0872-7
17. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018) 39:119–77. doi: 10.1093/eurheartj/ehx393
18. Park K, Park JS, Cho YR, Park TH, Kim MH, Yang TH, et al. Community-based pre-hospital electrocardiogram transmission program for reducing systemic time delay in acute ST-segment elevation myocardial infarction. Korean Circ J. (2020) 50:709–19. doi: 10.4070/kcj.2019.0337
19. Chowdhury IZ, Amin MN, Chowdhury MZ, Rahman SM, Ahmed M, Cader FA. Pre hospital delay and its associated factors in acute myocardial infarction in a developing country. PLoS One. (2021) 16:e0259979. doi: 10.1371/journal.pone.0259979
20. Brodie BR, Hansen C, Stuckey TD, Richter S, Versteeg DS, Gupta N, et al. Door-to-balloon time with primary percutaneous coronary intervention for acute myocardial infarction impacts late cardiac mortality in hi gh-risk patients and patients presenting early after the onset of symptoms. J Am Coll Cardiol. (2006) 47:289–95. doi: 10.1016/j.jacc.2005.08.065
21. De Luca G, Cassetti E, Marino P. Percutaneous coronary intervention-related time delay, patient's risk profile, and survival benefits of primary angioplasty vs lytic therapy in ST-segment elevation myocardial infarction. Am J Emerg Med. (2009) 27:712–9. doi: 10.1016/j.ajem.2008.04.026
22. De Luca G, Suryapranata H, Zijlstra F, van ‘t Hof AW, Hoorntje JC, Gosselink AT, et al. Symptom-onset-to-balloon time and mortality in patients with acute myocardial infarction treated by primary angioplasty. J Am Coll Cardiol. (2003) 42:991–7. doi: 10.1016/s0735-1097(03)00919-7
23. Ferlini M, De Ferrari GM, Moroni G, Roversi P, Potenza A, Leonardi S, et al. Strategies for reducing door to balloon time in patients with acute myocardial infarction undergoing primary angioplasty: the Pavia experience. G Ital Cardiol (Rome). (2016) 17:51–7. doi: 10.1714/2140.23192
Keywords: ST-segment elevation myocardial infarction, percutaneous coronary intervention, ischemia reperfusion injury, risk factors, prognosis
Citation: Zhang L, Wang L, Tao L, Chen C, Ren S and Zhang Y (2022) Risk Factors of Ischemia Reperfusion Injury After PCI in Patients with Acute ST-Segment Elevation Myocardial Infarction and its Influence on Prognosis. Front. Surg. 9:891047. doi: 10.3389/fsurg.2022.891047
Received: 7 March 2022; Accepted: 5 May 2022;
Published: 7 June 2022.
Edited by:
Songwen Tan, Central South University, ChinaReviewed by:
Wenjun Gu, The Ninth People’s Hospital, Shanghai Jiaotong University School of Medicine, ChinaCopyright © 2022 Zhang, Wang, Tao, Chen, Ren and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Youyou Zhang enFxMTE0NzEyMjFAMTYzLmNvbQ==
Specialty section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.