 Ana Cristina Veiga Silva1,2*
Ana Cristina Veiga Silva1,2* Camila Mendonça Lins3
Camila Mendonça Lins3 Renan Furtado de Almeida Mendes4Marcelo Henrique Simões Silva5Joaquim Fechine de Alencar Neto6Caio César Maia Lopes3Gabriela Lisboa de Souza Ferraz3Diego Felipe Rodrigues de Sousa7Luiz Severo Bem Junior2Marcelo Moraes Valença2Hildo Rocha Cirne de Azevedo-Filho1,2
Renan Furtado de Almeida Mendes4Marcelo Henrique Simões Silva5Joaquim Fechine de Alencar Neto6Caio César Maia Lopes3Gabriela Lisboa de Souza Ferraz3Diego Felipe Rodrigues de Sousa7Luiz Severo Bem Junior2Marcelo Moraes Valença2Hildo Rocha Cirne de Azevedo-Filho1,2
- 1Department of Neurosurgery, Hospital da Restauração, Recife, Brazil
- 2Neuroscience Post-Graduate Program, Federal University of Pernambuco, Recife-PE, Brazil
- 3Faculty of Medical Sciences, University of Pernambuco, Recife, Brazil
- 4Center for Medical Sciences, Federal University of Paraíba, João Pessoa, Brazil
- 5Department of Pathology of the Medicine Faculty, University of Paulo, São Paulo, Brazil
- 6Faculty of Medical Sciences, Unifacisa university center, Campina Grande, Brazil
- 7Department of Radiology, Hospital da Restauração, Recife, Brazil
Pott’s Puffy tumor, also called Pott’s edematous tumor (PET), is a subperiosteal abscess of the frontal bone, associated with osteomyelitis of the frontal bone. In this paper, we report the case of a 16-year-old patient who presented with headache associated with progressive forehead swelling and fever. Clinical and imaging exams pointed to the hypothesis of PET associated with brain abscess. Patient was submitted to surgical excision of the abscess and treatment of osteomyelitis, with intraoperative findings corroborating the condition. There was a good clinical-radiological recovery associated with prolonged antibiotic therapy and satisfactory follow-up after hospital. PET, which often results from an underdiagnosed or partially treated frontal sinusitis, is a condition that must be promptly recognized and directed to an adequate therapeutic approach due to the risk of serious complications that it entails.
Introduction
PET is usually an extracranial complication of frontal sinusitis and is characterized as subperiosteal abscess of the anterior wall of the frontal sinus, associated with osteomyelitis of the frontal bone. It was first described by Sir Percival Pott, as a consequence of head trauma (1), however, it is known that currently the main causes are rhinosinusitis, acute or chronic, underdiagnosed or inadequately treated (2–4). PET may still be associated with other conditions such as drug use, infections and frontal surgeries (2).
Due to the modern age of antibiotics, it is a rare entity and occurs more frequently in adolescents, probably due to vascularization and abundant flow in the diploic veins in this age group, facilitating the spread of infection (3). Its most common clinical manifestation is localized frontal swelling accompanied by fever and headache (2).
Early diagnosis plays a decisive role in patients with PET, as it allows the execution of precise treatment before the onset of complications, such as epidural, cerebral abscesses, subdural empyema, meningitis, and cerebral venous thrombosis. The clinical history added to the radiological findings of computed tomography (CT) directs the diagnosis. In cases of suspected intracranial injury, magnetic resonance (MRI) is indicated (4).
We describe the case of an adolescent patient, complaining of headache and presenting with fever, vomiting and forehead swelling. The patient, without known comorbidities, developed an intracranial complication of an infrequent sinus infection. The findings reported were related to relevant data from the literature, emphasizing the management and the need for early diagnosis.
Methods
This article is a case report with a literature review. Patient data and images were collected by the researchers who participated in the patient’s care. The consent form was signed, and the patient and guardians are aware of the possibility of writing and publishing the data and images present in the manuscript. The literature was reviewed by one of the researchers based on the search for articles in the PubMed database. For the research, the following keywords were inserted: “Pott puffy” and “tumor”, “Pott’s edematous tumor”. The “Boolean Operator” “AND” was used to maximize the amount of articles published. Inclusion criteria reached articles published in the last five years, case reports and patients aged up to 18 years. Thus, 49 articles were found based on the ones, of which 22 met the defined analysis criteria.
Case Description
Female patient, 16-year-old, single, brown, student, born in rural area of Pernambuco/Brazil, referred to the neurology and neurosurgery service of the Hospital da Restauração with a history of frontal, pulsing and progressive headache, worsening over weeks, associated with emetic episodes and fever. The condition evolved with progressive growth of a painful, adhered and fibroelastic consistency mass in the central region of the forehead of the skull, eight days before admission. Report of fever stopped two days after admission, with no signs of meningism, rhinorrhea or any focal neurological deficit. No traumatic event, past or recurrence of sinusopathy or other comorbidity that was related. Patient also referred no use of antibiotics. Laboratory tests also did not present alterations of hematimetric indices or inflammatory tests.
Blood culture was not performed. CT scan of the skull was performed, which showed an expansive hypodense lesion in the frontal region with intracranial extension associated with perilesional edema (Figure 1), and then transferred to the neurosurgery department with suspicion that the identified expansive formation would have neoplastic origin.
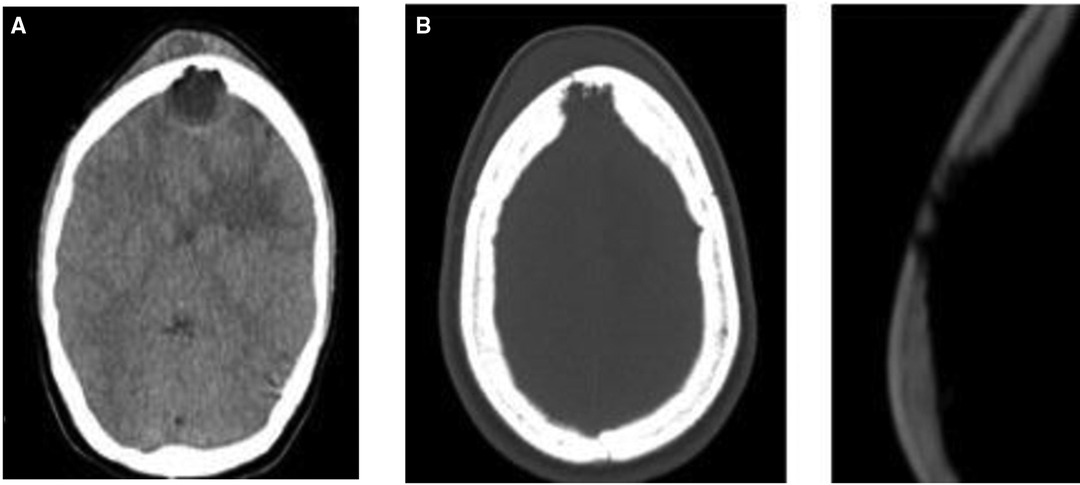
Figure 1. (A) Cranial CT, without contrast, axial cut, evidencing subgaleal hypoattenuating formation in the frontal region, noting in the same plane, but in intracranial and extra-axial situation, hypoattenuating lesion with expansive character associated with irregularities in the contours of the inner table of the adjacent frontal bone. (B) bone window, in the same plane of subgaleal and extra-axial lesions, evidencing in the frontal bone, especially in the internal table lytic destruction with bone discontinuity.
The patient underwent brain MRI, which revealed an expansive lesion in the frontal subcutaneous tissue, extending through a bone defect in the frontal sinus that communicated with an extra-axial nodular formation with intra-axial component and circumcision edema with important compressive effect, suggesting a complicated PET with concomitant cerebral abscess (Figure 2). Empirical intravenous antibiotic therapy with ceftriaxone (2 g administrated 12 h/12 h) and metronidazole (7,5 mg/kg administrated each 8 h) was initiated, for eight days before the surgery. Intranasal corticosteroid therapy was not prescribed for our patient.
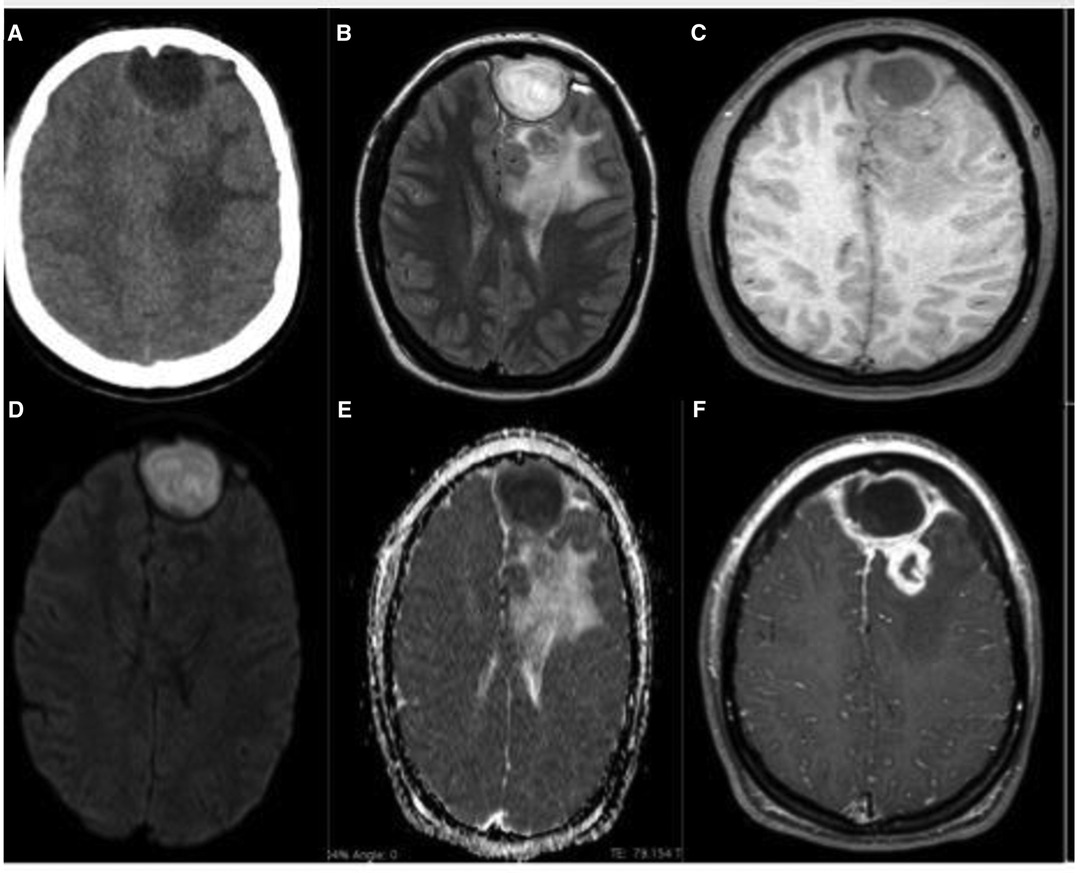
Figure 2. (A) Skull CT, without contrast, axial section, evidencing frontal extra-axial lesion, in left paramedian situation and hypoattenuation in the white matter of the left frontal lobe; (B) brain MRI, T2/FLAIR, axial, shows better the extra-axial expansive formation, located in the left anterior frontal pole, rounded, with apparent capsule, promoting compressive effect on the adjacent parenchyma, besides evidencing in adjacent frontal lobe small intraparenchymal lesion surrounded by important edema; (C) MRI of the brain, T1 after axial contrast, with important peripheral enhancement of both the extra-axial lesion (including with important enhancement of the locoregional meningeal plane) and intra-axial; (D) (DWI, axial section) evidences important central restriction of the extra-axial lesion with corresponding signal loss on the ADC Map (E) being compatible with empyema/abscess.
The patient was submitted to neurosurgical approach by bicoronal incision and, as cutaneous flap was rebalanced, granulation tissue, bone erosion with dural adhesion and spontaneous extravasation of purulent secretion was identified. Drainage of the abscess by puncture initially. Performed 5 × 5 cm frontal craniotomy resecting the entire osteomyelitis area. Resected the residual abscess and capsule, a fistulous hole (Figure 3B) was verified communicating purulent contents of the frontal sinus with brain abscess. After cranialization of the frontal sinus, evacuation of the subdural empyema and subgaleal abscess, exhaustive cavity washing was performed with 1,500 mL of saline plus gentamicin. Cranial reconstruction performed with autologous bone part, after curettage and drill of the internal eroded plate of the frontal bone flap and resected material (pus, granulation tissue and frontal sinus mucosa) sent for microbiological analysis and culture, but it was not identified any organism’s growth. This sterile culture result was probably due to empirical use of preoperative antibiotics, but anaerobic causative agents, destroyed after contact with oxygen, are also a possibility. Similarly, access to histological examination of the frontal sinus mucosa and the granulation tissue collected was not obtained. This type of intervention - surgical approach, associated with antibiotic therapy, was determined based on characteristics such as continuous abscess growth, intracranial mass effect, risk of complications, and neurological deficits.

Figure 3. (A) Positioning for surgical approach and marking of the bicoronal incision, evidencing the protuberance of the forehead by progressive swelling. (B) Intraoperative image after craniotomy with emphasis on fistulous hole of communication with frontal sinus, enhanced.
The patient followed a prolonged course of intravenous antibiotic therapy, ceftriaxone, and metronidazole (7 weeks). A new MRI was performed, 28 days after surgery, and showed the surgical a marked reduction of the frontal extra-axial collection. Meningeal thickening and residual frontal abscess surround by perilesional edema were observed, as shown in the pre and postoperative comparative images in Figure 4.
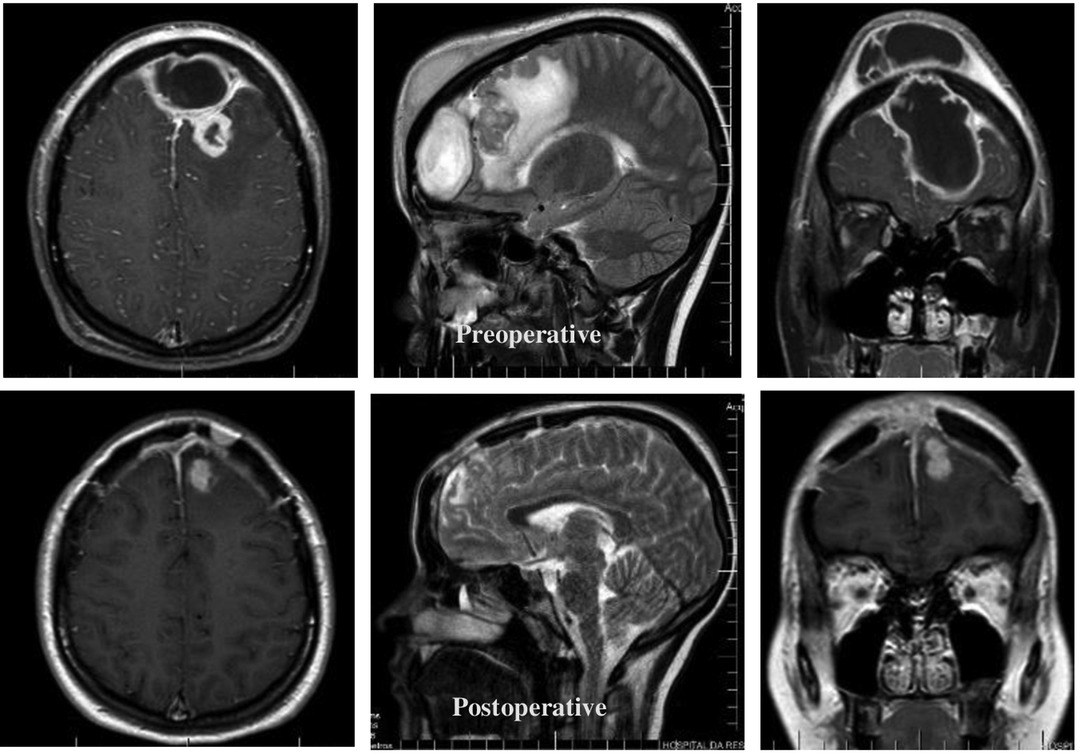
Figure 4. Comparative study between MRI in axial, sagittal and coronal sections before and after the surgical approach.
Due to the significant improvement of our patient condition, she was discharged after 43 days of post-surgical follow-up, with complementary oral antibiotic therapy with ciprofloxacin. It was chosen due to their broad spectrum, low cost, affordability and recommendation by the Hospital Infection Control Committee. The patient was subsequent outpatient follow-up at the service during the first 9 months, in three consultations, with satisfactory clinical, functional, and radiological control. Diagnosis and hospital therapy did not involve an otolaryngologist, but the patient was referred to a professional in the area.
Discussion
PET is a subperiosteal abscess of the frontal bone as a result of osteomyelitis of the frontal sinus walls (1). Episodes of cranial osteomyelitis are considered rare and are most commonly seen in countries with reduced health capacity, although an increase in the number of cases reported from the second millennium has been observed, most likely due to the improvement in the diagnostic capacity of radiological examinations (5).
Many papers details case reports of PET, and the number of children affected, and the similarity of the associated signs and symptoms are quite relevant, especially in correspondence with the affected locations and the consequent surgical intervention, as described in Table 1. Although this condition can affect both sexes and any age group, reviewing 24 case reports on Pott’s Puffy tumor in patients up to 18 years of age published in the last 5 years, we found reports of patients between 5 and 17 years of age (22 males and 2 females), and observed that there is a higher prevalence among adolescents, in an average age group of 11 years, and in males, as could be noted in Table 1, corresponding to 70% of cases (4). This occurs by the pneumatization process, venous drainage and the peak blood circulation in diploic veins, which occurs around 15 years of age (28). In addition, brain abscess is a complication found in only 12% of patients with PET, and is therefore a relevant fact in the case discussed (4).
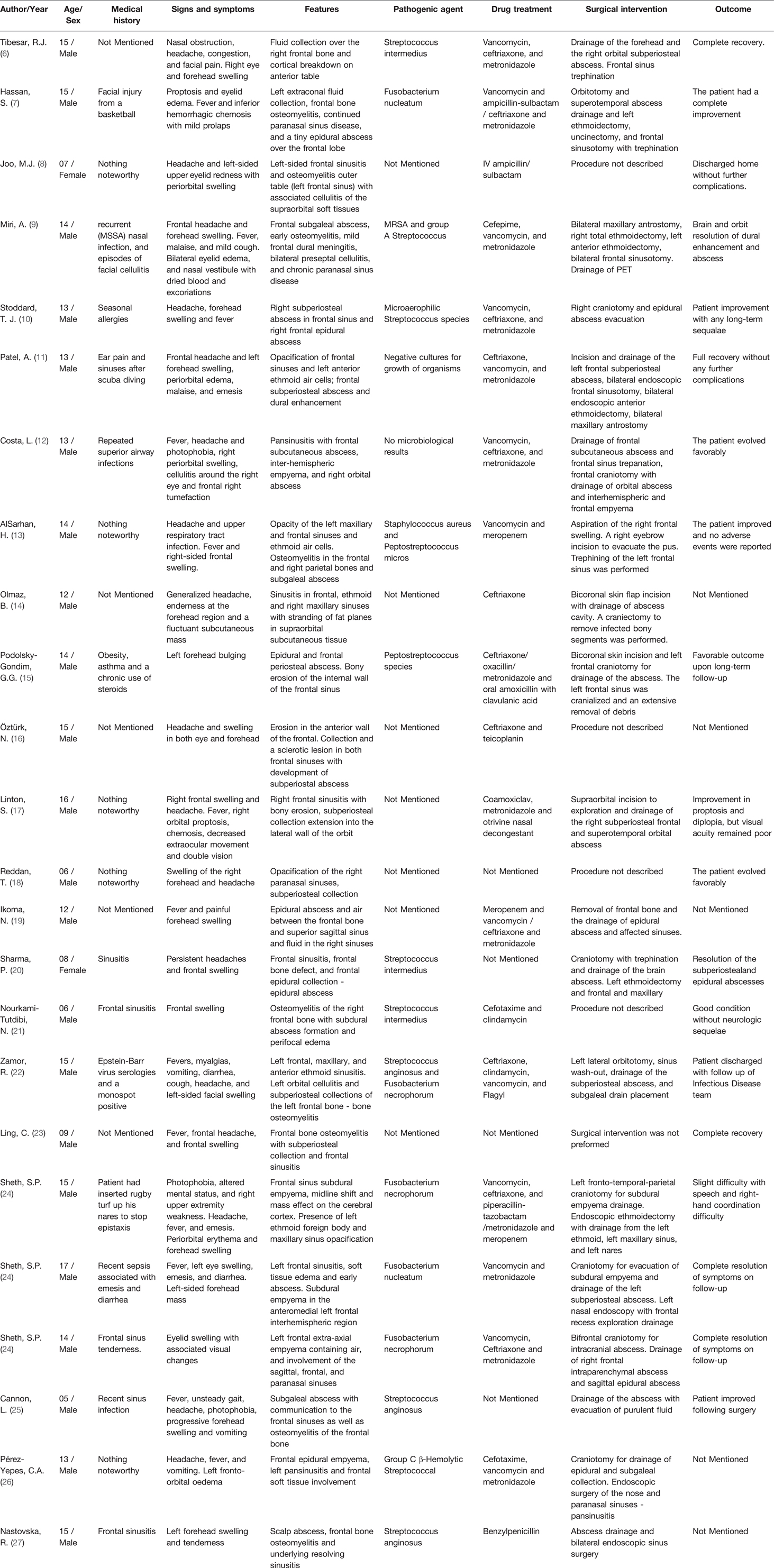
Table 1. Review of case reports about Pott’s Puffy tumor in patients up to 18 years old.
The most commonly cause of PET reported in the literature is acute or chronic sinusitis, which, when treated inappropriately, can culminate in a bone erosion caused by direct contact of the infected material with the walls of the skull cap (28). In addition to this more obvious route of dissemination, there is still the possibility of hematogenous infection through the diploic veins, which, due to the absence of valves, allow a retrograde septic thrombophlebitis more easily, which would explain parenchymal intracranial lesions and subdural collections without epidural involvement (29). Although less frequent, another important cause of PET is craniofacial trauma with a history of fracture. In adults, cocaine or methamphetamine abuse is also reported (2). In our review of case reports, we found that patients had recent or recurrent sinusitis or upper airway infection as the most frequent antecedent (reported in 6 cases), while we found a report of trauma in only one patient.
In addition to the characteristic association with traumatic brain injury and medical history of sinusitis, the presence of more prevalent infectious agents is also well-described for PET. Bacteria’s of rhinogenic pathologies, such as community-acquired sinusitis, are the most common, being Streptococcus and Staphylococcus the most recurrent agents, such as Staphylococcus aureus, Streptococcus spp, and anaerobic (30), although fungal infections can also be found. This prevalence can be analyzed on Table 1, which, despite the small amount of data collected, presents 11 (73.3%) cases of Streptococcus, among those that reported the causative microbiological agent.
In our review, the most frequently reported symptom is forehead swelling (present in 21 reports), followed by headache (present in 17 reports), fever (present in 13 reports) and symptoms associated with orbital and/or periorbital involvement (present in in 12 reports). As shown in Table 1, it’s notorious that the classic manifestation of this conditions is frontal swelling, usually accompanied by headache and fever. Furthermore, periorbital swelling and pain may suggest cellulitis, being important signs for PET due to possible involvement of the orbital cavity, in addition to purulent or not rhinorrhea (2–4, 28, 29). Symptoms such as nausea, vomiting, changes in the level of consciousness and convulsions may alert to intracranial involvements, such as epidural abscesses, subdural, cerebral, meningitis and thrombosis of the upper sagittal sinus (4). The recommended imaging test to confirm the diagnosis is cranial CT, as it allows a detailed visualization of bone involvement to assess the degree of osteomyelitis. For suspected intracranial lesions, MRI has a greater ability to reveal information, with greater accuracy for soft tissues, it is possible to better quantify the extent of frontal abscesses, for example (2).
In view of the signs and symptoms characteristic of this condition include above all swelling of the frontal region, fever, periorbital swelling, and headache, among the differential diagnoses are those that have mass effect, as well as PET. Thus, the analysis of the presence of soft tissue or skin infection without the presence of osteomyelitis, hematomas and other types of tumor formations should be investigated and ruled out in suspected PET, since they are the main conditions of differential diagnosis (31).
The approach should be based on a combined early intervention of antibiotic therapy and surgical procedure. Initially, the use of broad-spectrum antibiotics is recommended due to the variety of pathogens related with this condition. After the culture result, more specific coverage should be adopted, with the prescribing time ranging from 6 to 8 weeks after surgery (4). The procedure performed can be done from traditional craniotomies, as well as through endoscopic alternatives (32). However, in cases of important lesions, such as brain abscesses, it is mandatory to choose craniectomies with removal of the affected bone, since a high recurrence rate was observed in cases of bone replacement (28, 29). In most of the case reports reviewed, the treatment involved a surgical approach associated with antibiotic therapy, and the majority of patients evolved with a good outcome after treatment, with a description of recovery without sequelae in 14 reports (Table 1).
Conclusion
Although rare, PET is still present in the pediatric, adolescent and less frequent adult population. The need to rapid recognize and prevent, this sometimes, fatal complication of an apparently benign infection such as bacterial sinusitis, is necessary and mandatory for optimal outcome.
Parents, general clinicians, and pediatricians should be aware of patients presenting recurrent sinusitis, fever, forehead swelling and headache to seek specialist evaluation. Early diagnosis allows for a less invasive approach but in complicated cases, with bone and parenchymal involvement, surgical intervention is crucial to effective treatment, recurrence prevention, and deformity correction. The best management is showed to be a combination of surgical intervention and prolonged intravenous antibiotics.
Suspected by the physician in the context of known risk factors and underlying causes, both clinical and psychosocial, should be searched. In addition, it is a condition that should be readily recognized by the risk of suspected psychosocial clinical complications. An integrated approach is crucial for efficient care.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Written informed consent was obtained from the individual(s), and minor(s)’ legal guardian/next of kin, for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Conceptualization: AS, HA, Methodology: AS, LJ, Research: AS, GF, JN, Supervision: HA, MV, Project management: AS, CL, RM, Acquisition of funding: AS, Resources: AS, CL, JN, Data curation: AS, RM, MV, DS, JN, Software: AS, RM, CL, DS, Visualization: CL, GF, MS, DS, JN, Writing: AS, CL, RM, MS, JN, Review and Editing: LJ, AS. All authors contributed to the article and approved the submitted version.
Funding
The authors declare that the research was conducted in the absence of any commercial or financial support.
Acknowledgments
To the Professors of Hospital da Restauração who provided insight and expertise that greatly assisted the research and actively stimulated the search for answers.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Pott P. The Chirurgical Works of Percivall Pott, Vol. 1. London, UK: Woods and Innes (1808). https://openlibrary.org/books/OL24611442M/The_chirurgical_works_of_Percivall_Pott
2. Sandoval JI, De Jesus O. Pott Puffy Tumor. StatPearls. Treasure Island (FL): StatPearls Publishing (2021). Available from: http://www.ncbi.nlm.nih.gov/pubmed/32809624 (Accessed March 11, 2021).
3. Hasan I, Smith SF, Hammond-Kenny A. Potts puffy tumour: a rare but important diagnosis. J Surg Case Rep. (2019) 2019(4):1–2. doi: 10.1093/jscr/rjz099
4. Koltsidopoulos P, Papageorgiou E, Skoulakis C. Pott’s Puffy tumor in children: a review of the literature. Laryngoscope. (2020) 130(1):225–31. doi: 10.1002/lary.27757
5. Akhaddar A. Cranial osteomyelitis: Diagnosis and treatment. Cranial Osteomyelitis Diagn Treat. (2016) 286–92. doi: 10.1007/978-3-319-30268-3
6. Tibesar RJ, Azhdam AM, Borrelli M. Pott’s Puffy Tumor. Ear Nose Throat J. (2021) 100(6_suppl):870S–2S. doi: 10.1177/01455613211039031
7. Hassan S, Rahmani B, Rastatter JC, Jaju AI, Kurup SP. Trauma-associated Pott’s puffy tumor: an ophthalmologic perspective. Orbit. (2020) 39(1):38–40. doi: 10.1080/01676830.2019.1573909
8. Joo MJ, Schapira KE. Pott’s puffy tumor: a potentially deadly complication of sinusitis. Cureus. (2019) 11(12):e6351. doi: 10.7759/cureus.6351
9. Miri A, Sato AI, Sewell RK, Huang-Pacheco A. Pott’s puffy tumor in an inflammatory bowel disease patient on anti-TNF therapy. Am J Case Rep. (2021) 22:e929892. doi: 10.12659/AJCR.929892
10. Stoddard TJ, Tung P, Kelly MN. Pott’s puffy tumor: a case report. J Pediatr Health Care. (2019) 33(5):585–8. doi: 10.1016/j.pedhc.2019.05.005
11. Patel A, Vuppula S, Hayward H, Lakhani A, Lighter J. A case of Pott’s puffy tumor associated with barosinusitis from scuba diving. Pediatr Emerg Care. (2021) 37(1):e51–4. doi: 10.1097/PEC.0000000000001657
12. Costa L, Mendes Leal L, Vales F, Santos M. Pott’s puffy tumor: rare complication of sinusitis. Braz J Otorhinolaryngol. (2020) 86(6):812–4. doi: 10.1016/j.bjorl.2016.08.005
13. AlSarhan H, Jwery AK, Mohammed AA. Pott’s puffy tumour of the frontal and Parietal bones with subgaleal abscess as a complication of acute sinusitis - a case report. J Pak Med Assoc. (2021) 71(Suppl 8 12):S170–3. https://jpma.org.pk/PdfDownloadsupplements/69435130243
14. Olmaz B, Cingoz M, Akdogan E, Kandemirli SG. Correlation of imaging and intraoperative findings in Pott’s puffy tumour. Scott Med J. (2019) 64(1):25–9. doi: 10.1177/0036933018803787
15. Pololsky G, Santos M, Carneiro V, Pires L, Pacheco R, Santos R. Neurosurgical management of Pott’s puffy tumor in an obese adolescent with asthma: case report with a brief review of the literature. Cureus. (2018) 10(6):e2836. doi: 10.7759/cureus.2836
16. Öztürk N, Atay K, Çekin İE, Erkul BE, Karademir F. A rare case in childhood: Pott’s puffy tumor developing secondary to frontal sinus osteoma. Turk Pediatri Ars. (2020) 55(4):445–8. doi: 10.14744/TurkPediatriArs.2020.28863
17. Linton S, Pearman A, Joganathan V, Karagama Y. Orbital abscess as a complication of Pott’s puffy tumour in an adolescent male. BMJ Case Rep. (2019) 12(7):e229664. doi: 10.1136/bcr-2019-229664
18. Reddan T, Connor P. Not just a bump on the head: ultrasound as first-line imaging in a boy with Pott’s puffy tumour. J Med Radiat Sci. (2018) 65(1):71–3. doi: 10.1002/jmrs.251
19. Ikoma N, Aizawa Y, Sasaki T, Oishi M, Saito N, Yoshida H, et al. Pott’s puffy tumour: a rare and life-threatening disease. Lancet Infect Dis. (2020) 20(12):1482. doi: 10.1016/S1473-3099(20)30684-8
20. Sharma P, Sharma S, Gupta N, Kochar P, Kumar Y. Pott puffy tumor. Proc (Bayl Univ Med Cent). (2017) 30(2):179–81. doi: 10.1080/08998280.2017.11929575
21. Nourkami-Tutdibi N, Linsler S, Yilmaz U, Pfeifer J, Derouet C, Becker SL, et al. A 6-year-old boy with a frontal mass: Pott puffy tumor. J Pediatr. (2020) 217:211. doi: 10.1016/j.jpeds.2019.09.047
22. Zamor R, Edmunds K, Orscheln E, Duma E. Severe complications from infectious mononucleosis after prolonged steroid therapy. Pediatr Emerg Care. (2021) 37(12):e1741–4. doi: 10.1097/PEC.0000000000001940
23. Ling C, Ng DCE, A/P Bag Amiya Kumar T. More than a bump on the head. J Pediatr. (2021) 238:331. doi: 10.1016/j.jpeds.2021.06.052
24. Sheth SP, Ilkanich P, Congeni B. Complicated fusobacterium sinusitis: a case report. Pediatr Infect Dis J. (2018) 37(9):e246–8. doi: 10.1097/INF.0000000000001927
25. Cannon L, Zwemer E, Stephens JR. Puff laddy: a 5-year-old-boy with forehead swelling. BMJ Case Rep. (2017) 2017:bcr2017223340. doi: 10.1136/bcr-2017-223340
26. Pérez-Yepes CA, Avilés-Robles M. Fronto-orbital headache and oedema of sudden onset in an adolescent. Enferm Infecc Microbiol Clin. (2017) 35(6):386–387. English, Spanish. doi: 10.1016/j.eimc.2015.07.014.
27. Nastovska R, Lim LL. Sinusitis complicated by frontal bone osteomyelitis in a young patient. Med J Aust. (2017) 207(9):376. doi: 10.5694/mja16.01434
28. Salomão JF, Cervante TP, Bellas AR, Boechat MCB, Pone SM, Pone MVS, et al. Neurosurgical implications of Pott’s puffy tumor in children and adolescents. Childs Nerv Syst. (2014) 30(9):1527–34. doi: 10.1007/s00381-014-2480-x
29. Bambakidis NC, Cohen AR. Intracranial complications of frontal sinusitis in children: Pott’s puffy tumor revisited. Pediatr Neurosurg. (2001) 35(2):82–9. doi: 10.1159/000050395
30. Kühn JP, Linsler S, Nourkami-Tutdibi N, Meyer S, Becker SL, Yilmaz U, et al. Pott’s puffy tumor: a need for interdisciplinary diagnosis and treatment. HNO. (2022) 70(Suppl 1):8–13. doi: 10.1007/s00106-021-01134-w
31. Ketenci I, Unlü Y, Tucer B, Vural A. The Pott’s puffy tumor: a dangerous sign for intracranial complications. Eur Arch Otorhinolaryngol. (2011) 268(12):1755–63. doi: 10.1007/s00405-011-1660-5
Keywords: Pott’s Puffy tumor, Pott’s edematous tumor, osteomyelitis, sinusistis, forehead swelling
Citation: Silva ACV, Lins CM, Mendes Renan Furtado de Almeida, Silva MHS, de Alencar Neto JF, Lopes C, Ferraz Gabriela Lisboa de Souza, de Sousa D, Bem Junior LS, Valença MM and Azevedo-Filho Hildo Rocha Cirne de (2022) Case Report: Pott's Edematous Tumor: Complicated Frontal Sinusitis - An Unremembered Diagnosis. Front. Surg. 9:889463. doi: 10.3389/fsurg.2022.889463
Received: 4 March 2022; Accepted: 30 May 2022;
Published: 27 June 2022.
Edited by:
Lynne Lourdes Navarrete Lucena, Bicol University, PhilippinesReviewed by:
Aleksandar Peric, Military Medical Academy, SerbiaYener Aydin, Atatürk University, Turkey
Gönül Tanır, Dr Sami Ulus Child Health and Diseases Training and Research Hospital, Turkey
Copyright © 2022 Silva, Lins, Mendes, Silva, de Alencar Neto, Lopes, Ferraz, de Sousa, Bem Junior, Valença and Azevedo-Filho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Cristina Veiga Silva Y3Jpc3RpbmEudmVpZ2FAdWZwZS5icg==
Specialty section: This article was submitted to Neurosurgery, a section of the journal Frontiers in Surgery