
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg., 20 May 2022
Sec. Visceral Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.886478
This article is part of the Research TopicAdvances in Proctology and Colorectal SurgeryView all 45 articles
 Francesco Maione1*
Francesco Maione1* Michele Manigrasso2
Michele Manigrasso2 Alessia Chini1*
Alessia Chini1* Sara Vertaldi1Pietro Anoldo2Anna D’Amore1Alessandra Marello1Carmen Sorrentino1Grazia Cantore1
Sara Vertaldi1Pietro Anoldo2Anna D’Amore1Alessandra Marello1Carmen Sorrentino1Grazia Cantore1 Rosa Maione1
Rosa Maione1 Nicola Gennarelli1Salvatore D’Angelo1Nicola D’Alesio1Giuseppe De Simone1Giuseppe Servillo1
Nicola Gennarelli1Salvatore D’Angelo1Nicola D’Alesio1Giuseppe De Simone1Giuseppe Servillo1 Marco Milone1
Marco Milone1 Giovanni Domenico De Palma1
Giovanni Domenico De Palma1
Purposes: The aim of this study was to evaluate the importance of Indocyanine Green in control of anastomosis perfusion and on anastomotic leakage rates during laparoscopic and robotic colorectal procedures.
Methods: A retrospective review of patients who underwent elective minimally invasive surgery for colorectal cancer from 1 January 2018 to 31 December 2020 was performed. All patients underwent Near-Infrared Fluorescence-Indocyanine Green system in two moments: before performing the anastomosis and after completing the anastomotic procedure. Primary outcomes were the rate of intraoperative change in the surgical resection due to an inadequate vascularization and the rate of postoperative anastomotic leakage. Secondary outcomes were the postoperative complications, both medical and surgical (intra-abdominal bleeding, anastomotic leakage).
Results: Our analysis included 93 patients. Visible fluorescence was detected in 100% of the cases. In 7 patients (7.5%), the planned site of resection was changed due to inadequate perfusion. The mean extension of the surgical resection in these 7 patients was 2.2 ± 0.62. Anastomotic leakage occurred in 2 patients (2.1%). Other complications included 8 postoperative bleedings (8.6%) and 1 pulmonary thromboembolism.
Conclusions: The intraoperative use of Near-Infrared Fluorescence-Indocyanine Green in colorectal surgery is safe, feasible, and associated with a substantial reduction in postoperative anastomotic leakage rate.
Anastomotic leakage (AL) is defined as a dehiscence of the intestinal wall at the anastomotic site, that could require a surgical revision, and it represents one of the most common complications in colorectal surgery. The incidence of AL in ileocolic, colo-colic, and colorectal or coloanal anastomoses is 1–4%, 2–3%, and 5–19%, respectively (1, 2). In most cases, the development of AL depends on the state of perfusion, the surgical technique, and the anastomotic procedure. Data reported from the literature showed that there is no difference in the AL rate between open surgery and minimally invasive techniques; regarding the anastomotic technique, anastomosis with stapling devices is associated with a higher incidence of AL with respect to non-stapled anastomosis, as confirmed by a recent study conducted by Wurtz et al (3). Complications following surgery can be due to technical errors such as insufficient blood supply and increased tension to the anastomosis, technical failure of the stapler, and inadequate suturing. Advances in technology have introduced near-infrared (NIR) fluorescence imaging with indocyanine green (ICG) to evaluate the perfusion of colorectal anastomosis.
The aim of this study was to evaluate the role of ICG in control of perfusion to the anastomosis and on AL rates during minimally invasive colorectal surgery.
After the approval of the Institutional Review Board of the “Federico II” University of Naples, a retrospective chart review of the minimally invasive colorectal resection for cancer from 1 January 2018 to 31 December 2020 was performed.
All patients received an elective laparoscopic or robotic operation and they underwent previously a complete history and physical examination with blood tests, cross-sectional imaging (4), and colonoscopy. After the admission, the patients underwent bowel preparation with a combination of osmotic laxative, potassium and sodium salts if possible, preoperative antibiotics, and heparin prophylaxis according to the current literature (5–8).
All operations were performed by expert surgeons. In order to reduce the bias related to the different surgical techniques, only procedures performed according to the standardized criteria were included in the study.
All the patients were operated on under general anesthesia (9). In right colectomy, once identified the ileocolic pedicle, the peritoneum of the mesentery just inferior to the vessel should be opened with the creation of a mesenteric window. Thus, Toldt’s fascia was separated from Gerota’s plane, with identification and preservation of the right ureter, duodenum, and pancreatic head. After ligation of the ileocolic pedicles at their origin, the right colon was completely mobilized laterally from the right parietocolic gutter. The mesentery was dissected medially, with consequent ligation of the right colic vessels and the right branch of the middle colic vessels. After performing the right hemicolectomy with a linear stapler, the ileo-colic anastomosis was performed intracorporeally in a side-to-side isoperistaltic fashion. In the left colectomy, after the colo-epiploic detachment and the complete mobilization of the splenic flexure, the Inferior Mesenteric Vein (IMV) and the Inferior Mesenteric Artery (IMA) were isolated, clipped, and divided at their roots. After the detachment of the Toldt’s fascia from the Gerota’s plane, with the preservation of the retroperitoneal elements, left hemicolectomy was performed with a linear stapler and a colorectal end-to-end anastomosis was performed according to Knight–Griffen technique. In the case of anterior rectal resection, after the complete mobilization of the left colon as described, the intervention proceeded with a Partial or Total Mesorectal Excision (PME or TME). In segmental splenic flexure resection, after the mobilization of the descending and transverse colon, the left branches of the middle colic vessels and the left colic artery were isolated, clipped, and ligated at their origin. Finally, for transverse colon resection, both the colic flexures were completely mobilized and a wedge resection of the mesentery, including the branches of the middle colic artery, was performed. In the case of segmental resections, the colo-colic anastomosis was performed intracorporeally in a side-to-side isoperistaltic way.
All patients underwent NIR/ICG system according to a standardized technique at two different moments: before performing the anastomosis to control the adequate vascularization of the stumps and after completing the anastomosis to control its perfusion (Figure 1). In detail, before the colonic or rectal resection, the anesthesiologist administered a bolus of 0.2 mg/kg of ICG, and after a median time of 25 seconds, an adequate vascularization was visible (if present). The same procedure was repeated after performing the anastomosis.
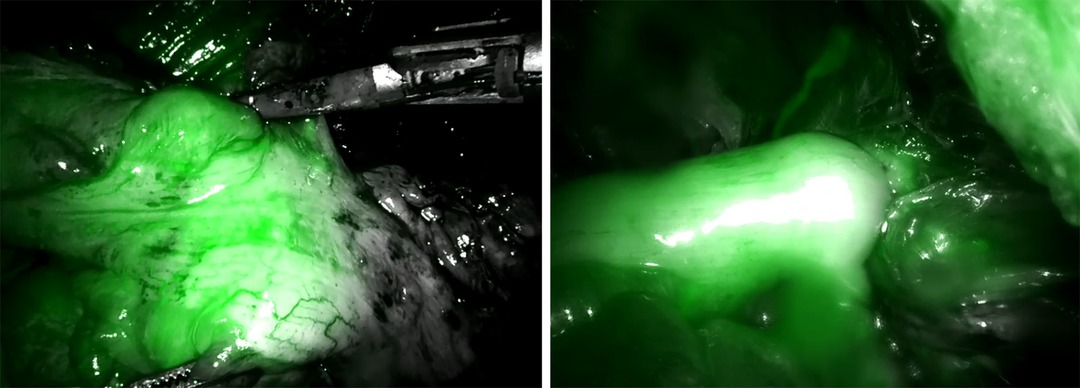
Figure 1. Pre- (A) and post-anastomotic (B) application of the Indocyanine Green technology.
Data were prospectively collected and included gender, age, Body Mass Index (BMI), American Society of Anesthesiologists (ASA) Score, conversion rate, and intraoperative complications.
Primary outcomes included the rate of intraoperative change in the surgical resection due to an inadequate vascularization at the NIR/ICG system and the rate of postoperative anastomotic leakage. In case of intraoperative changes due to an inadequate vascularization, the extension of the surgical resection was measured in centimeters and registered.
Secondary outcomes were the postoperative complications according to the Clavien–Dindo classification.
Anastomotic leakage was suspected based on fever, abdominal pain, fecal matter in abdominal drainage, abscess and gas around the anastomotic site at the computed tomography, and the presence of a communication between inside and outside the intestinal tract at the contrast enema. Anastomotic leakage was considered as a complication when a surgical re-intervention was necessary.
Statistical analysis was performed using the SPSS 26 system (SPSS Inc., Chicago, IL, USA). Continuous data were expressed as mean ± SD; categorical variables were expressed as %. Furthermore, a multivariate analysis was performed to assess if any patients’ or surgical characteristics (age, gender, BMI, ASA Score, the presence of diabetes or hypertension, the adoption of robotic or laparoscopic approach) could significantly impact on anastomotic leakage or bleeding rate. Results of the multivariate analysis were expressed by Odds Ratio (OR) and 95% Confidence interval (95% CI).
Our analysis included 93 patients; all patients underwent elective minimally invasive surgery (laparoscopic or robotic surgery) for malignant colorectal cancer. Of these, 40 were female and 53 were male (43% and 57%, respectively).
Demographic data are reported in Table 1. Mean age was 69.81 ± 12.06, mean BMI was 25.81 ± 4.29, and mean ASA Score was 2.54 ± 0.52. Of the included patients, 16 (17.2%) were smokers, 12 (12.9%) were obese, 20 (21.5%) were affected by diabetes, and 56 (60.2%) by hypertension. 24 patients (25.8%) underwent previous abdominal surgery.
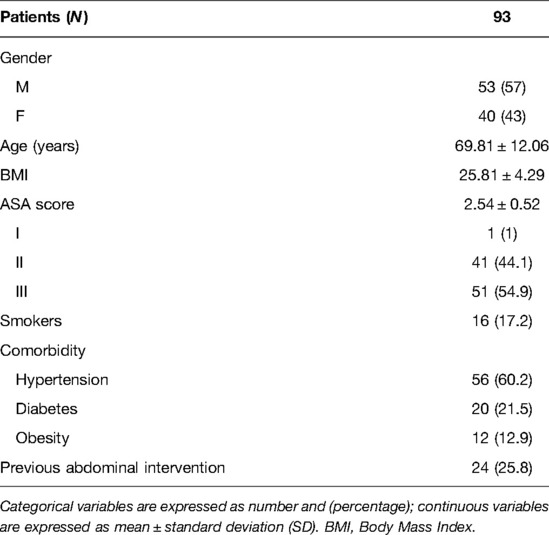
Table 1. Demographic data of the included patients.
Intraoperative data are reported in Table 2. Of the included procedures, 62 (66.6%) were laparoscopic and 31 (33.4%) robotic. 41 were right hemicolectomy (44.1%), 24 (25.8%) left hemicolectomy, 23 (24.7%) were rectal anterior resection (with or without protective loop ileostomy), 4 (4.3%) splenic flexure resection, and 1 (1.1%) was a segmental resection of the transverse colon. Intraoperative complications included 3 intraoperative bleeding, with no conversion needed. After the injection of the ICG, no adverse events were registered.
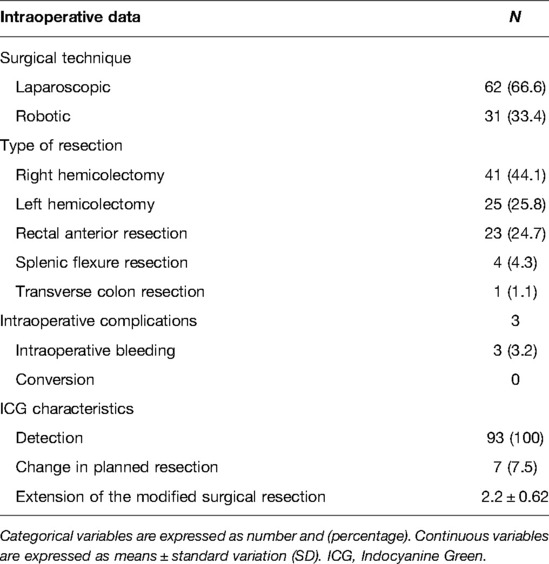
Table 2. Intraoperative data.
Visible fluorescence was detected in 100% of the cases and the meantime from ICG injection to visible fluorescence was 25 seconds. In 7 patients (7.5%), the planned site of resection was changed due to inadequate perfusion at NIR/ICG system. The mean extension of the surgical resection in these 7 patients was 2.2 ± 0.62.
After performing the anastomosis, the NIR/ICG system detected no cases of inadequate perfusion in the performed anastomoses.
Postoperative complications are summarized in Table 3. Anastomotic leakage occurred in 2 patients (2.1%), in which a protective loop ileostomy was performed. Other complications included 8 postoperative bleedings (8.6%), which required blood transfusion, and 1 pulmonary thromboembolism, which required implementation of anticoagulant therapy. Postoperative complications are defined according to the Clavien–Dindo classification, which consists of five severity grades. Grade 1 includes minor postoperative complications, not requiring therapy and none of the patients enrolled in the study is included in this group. Grade 2 complications require pharmacological treatment and eight patients with intra-abdominal bleeding are included in this group. Grade 3 complications, requiring surgical or radiological intervention, are recorded in 2 patients with anastomotic leakage, while Grade 4 complications, requiring an intensive care management for single or multiorgan disfunction, are recorded in 1 patient with pulmonary thromboembolism. Grade 5 indicates the death of the patient and it did not occur in any patients enrolled in the study (10).
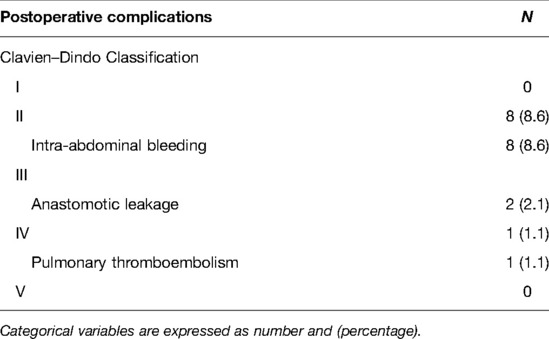
Table 3. Postoperative complications.
Table 4 reported results classifying patients according to precise categories: sex, age, obesity, defined as BMI > 30, presence of diabetes, hypertension, and previous abdominal intervention. For each category, the surgical technique, intraoperative complications, postoperative complications, and ICG detection were reported.
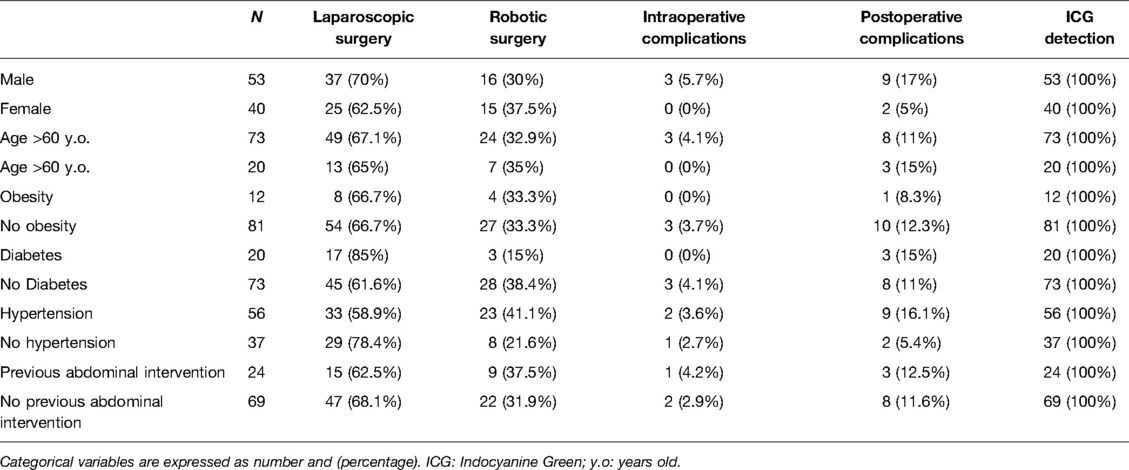
Table 4. Surgical technique, complications, and ICG detection according to patient categories.
Table 5 showed the results of the multivariate analysis. Specifically, none of the patients’ characteristics or the adoption of robotic or laparoscopic approaches significantly impacted on the rate of anastomotic leakage and bleeding.
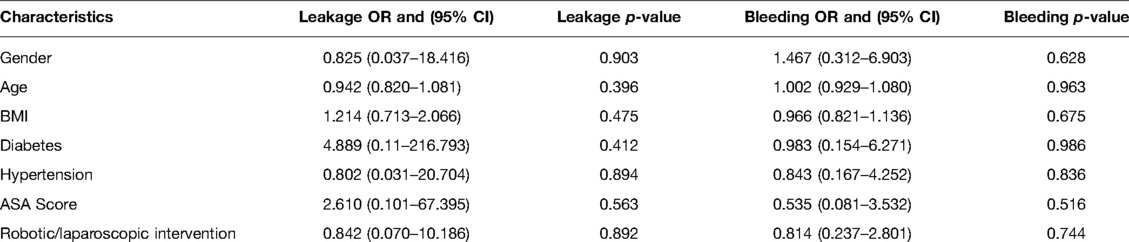
Table 5. Results of the multivariate analysis.
Although the benefits of the minimally invasive surgery in the treatment of the colorectal pathologies are well known (11–15), anastomotic leakage (AL) remains one of the most common complications in colorectal surgery. It increases morbidity and mortality, healthcare costs, and worsening long-term oncological outcomes. The risk factors for AL include: preoperative findings, such as tumor size and stage (16, 17), radiation, chemotherapy, male sex (18), nutrition (17), and comorbid condition such as obesity (19, 20), diabetes mellitus, cardiovascular disease; intraoperative factors, including the state of bowel perfusion, the level and the tension of anastomosis (21, 22), blood loss and operation time (16, 19, 23, 24); postoperative factors, such as the presence of diverting stoma (21), placement of abdominal drainage tube (16), and changes of intestinal microbes (25). Malignant involvement of local mesenteric lymph nodes could lead to mesenteric lymphadenopathy and increase the risk of complications, including AL, as reported also for several types of tumors (26).
The surgical technique and the state of perfusion are known to be important factors for the occurrence of AL. For years, anastomotic blood perfusion is assessed by the surgeons with visual evaluation of the resection margins, even if it has been reported to be a subjective analysis. In the last years, several studies have suggested that NIR has emerged as a promising method for a more accurate assessment of tissue perfusion during colorectal surgery, following intravenous infusion of indocyanine green (ICG).
ICG is a tricarbocyanine compound with a molecular mass of 776 Da, soluble in water. After its intravenous injection, ICG is quickly fixed to plasmatic proteins and, from the blood circulation, is carried to the liver, where ICG is extracted unchanged. In the case of extravenous injection, ICG is found in macrophages located in lymphatic vessels and lymph nodes.
ICG is captured by a system that activates its fluorescence with the light emitted by a led. Once excited, ICG sends fluorescent signals that have the ability to cross about 10 mm of the human soft tissue. From the intravenous injection, the spread of ICG to peripheral vessels is very rapid, in terms of few seconds. The reduction of the blood flow in a tissue leads to a decrease in ICG fluorescence emission. The evaluation of blood perfusion using ICG fluorescence imaging is applied not only to colorectal resection but also to breast reconstruction and coronary artery bypass grafting.
Several studies have reported the efficacy and the feasibility of the ICG injection in patients who underwent different surgical interventions under election for colorectal cancer (1, 27–33).
Impellizzeri et al. (1) showed that the intraoperative use of NIR/ICG for evaluation of anastomosis perfusion was safe for colorectal surgery and it significantly reduces the AL incidence. They conducted a retrospective study including 196 procedures of which 98 were without the use of ICG imaging and 98 were with the use of ICG imaging. In the first group, six patients developed AL, in the second no one. Similar encouraging results have been shown by other studies. Boni et al. (27) and Jafari et al. (28) conducted two case-control analyses, showing that the use of NIR/ICG for low anterior rectal resections, where the risk of AL is higher than in other large intestinal resection, demonstrated inadequate blood perfusion on the anastomosis site in 5%–19% of cases, thus the colonic transection point was changed, and it was associated with a reduction in AL rate (5%–12%), in comparison to the control group. The use of NIR/ICG in right and left hemicolectomy, segmental resection and anterior rectal resection reported a change of section line in 3.7%–7.9% of cases following NIR/ICG, with an AL incidence of 0.9%–1.4% (34, 35). Morales-Conde et al. (29), in their study, enrolled 192 patients who underwent different colorectal surgical procedures to evaluate in which one fluorescence angiography with indocyanine green (ICG-FA) was more effective in the anastomosis assessment, changing the section line level. The most significant value was observed in left hemicolectomy (25.9%), followed by anterior rectal resection (25.7%), segmental resection of the splenic flexure (11.1%), and right hemicolectomy (6%). Hasegawa et al. (2) conducted a retrospective study on 844 patients who underwent laparoscopic sphincter-sparing surgery: among them, 141 patients underwent ICG-FA to identify AL, and they were compared to 703 patients in whom ICG-FA was not performed. The incidence of AL was 2.8% in the first group and 12.4% in the second one. Also, Ishii et al. (31) evaluated the role of ICG-FA in their retrospective analysis, including 488 patients with colorectal cancer who underwent surgical intervention. ICG-FA was performed in 233 patients and they showed that the incidence of AL was no significantly different between the two groups in patients with colon cancer, while, in patients with rectal tumor, the incidence of AL was lower in the ICG group than in the no-ICG group (3.5% vs 10.5%). The retrospective case–control study by Brescia et al. (32) confirmed that the use of ICG-FA in patients managed with ERAS perioperative protocol was feasible, safe, and reduced the anastomotic leakage. They enrolled 182 patients who underwent laparoscopic colorectal surgery and divided them into two groups: a first group (A) including 107 patients managed with ERAS perioperative protocol and a second group (B) including 75 patients managed not only with ERAS pathway but also with the use of ICG-FA. 6 (5.6%) clinically relevant AL occurred in group A while there was none in group B. In a retrospective study, Kin et al. (33) evaluated the use of ICG-FA for the assessment of anastomosis perfusion in patients underwent colorectal surgery, but they did not find any advantage from the use of NIR/ICG, showing that the pelvic radiation therapy and the anastomosis proximity from anal verge were independent predictors of AL. However, they evaluated with NIR/ICG only the proximal point of transection. Thus, we believe that to reduce the AL rate, it is important to evaluate with NIR/ICG the perfusion of both the transection point and of the anastomosis once completed.
However, there is no unified system for the quantitative analysis of the fluorescence signal, thus it is not possible to reproduce and compare results from various studies. Moreover, there are some technical aspects of fluorescence imaging that we have to consider. Firstly, fluorescence intensity depends on the distance between the emission source and the target tissue. Moreover, ICG circulates dynamically in the tissues according to perfusion and this often leads to an underestimation of ischemic zones. Actually, few studies regarding the quantitative evaluation of perfusion in the colorectal anastomotic site are reported in literature. One of them is the study by Amagai et al. (36), where authors, in the evaluation of intestinal perfusion during colorectal surgery, considered four areas of interest: two proximal intestinal areas, one where the fluorescence was higher (proximal-high) and the other where it was lower (proximal-low), and two distal intestinal areas, one where the fluorescence was higher (distal-high) and the other where it was lower (distal-low). In each area, they considered the time from the intravenous injection of ICG to the maximum fluorescence (Tmax) and the time from the start of dyeing to the Tmax, which is defined as ΔT, and they found a correlation between Tmax e ΔT. Wada et al. (37) showed a correlation between the maximum fluorescence value (Fmax) and AL. On the contrary, Hayami et al. (38), analyzing Fmax data in their results, hypothesized a correlation with breath excursions, especially in minimally invasive surgery. For this reason, they considered Fmax as an unstable factor and it cannot be considered a feasible indicator of AL. Thus authors focused on the relationship between the period from the intravenous infusion of ICG to the beginning of fluorescent emission (T0) and AL and showed that patients with AL had longer T0 than those without AL. In another report, Son et al. (39) showed a correlation between time from first fluorescence increase to half of the maximum and AL and a correlation between the time ratio (time from first fluorescence increase to half of the maximum/ the time from the start of dyeing to the maximum fluorescence) and AL. D’Urso et al. (40) demonstrated that fluorescence-based enhanced reality (FLER) can be an accurate method to quantify fluorescence signal in augmented reality and to provide a feasible evaluation of intestinal perfusion.
During colorectal resections, ICG imaging also provides to facilitate vascular dissection when the vascular anatomy of tumor site is unclear and identifies the ureter to prevent iatrogenic injury. Santi et al. (41) prospectively enrolled 38 patients for a standard surgical treatment of laparoscopic colorectal resection, in six cases they used ICG imaging to identify vascular anatomy and to perform vascular dissection, in one case they used ICG imaging to identify the ureter which was tightly attached to the tumor.
In our study, we use indocyanine near-infrared fluorescence in two moments: before performing the anastomosis to control transection points and after completing the anastomotic procedure to control its perfusion. In 7.5% of the cases, the planned site of transection was changed because the demarcation line defined by NIR/ICG system was different from the point established by the surgeon’s visual inspection. AL developed only in 2.1% of the cases. In conclusion, the results of this retrospective analysis suggest that the intraoperative use of NIR/ICG in colorectal surgery is safe and feasible, both before performing the anastomosis to control the site of resection than after performing the anastomosis to evaluate the perfusion of the anastomotic site, regardless of patients’ characteristics and the surgical approach. Furthermore, the use of ICG did not result in allergic reactions and prolonged surgery time, and postoperative complications were not consequential to the additional technique. However, major limitations of this study have to be addressed. Being a retrospective cohort analysis, the bias related to the absence of randomization and of a control group clearly constituted a concern. For this reason, randomized prospective trials on intraoperative NIR/ICG use are necessary to confirm these data.
Therefore, despite there are several questions to be discussed and more high-quality large sample size randomized prospective trials are necessary to confirm the benefits of NIR/ICG in colorectal surgery, we believe that the assessment of an adequate vascularization by the use of NIR/ICG should be considered a key point to reduce the incidence of AL.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants, in accordance with the local legislation and institutional requirements.
MF: conception, design, interpretation of the data and drafting of the article; MM, CA, VS, AP, DA, MA, SC, CG, MR, DS, DN, GN, DSG, SG: acquisition, analysis, and interpretation of the data; MM and DPGD: interpretation of the data and critical revisions; MM and DPGD: critical revisions and final approval. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Impellizzeri HG, Pulvirenti A, Inama M, Bacchion M, Marrano E, Creciun M, et al. Near-infrared fluorescence angiography for colorectal surgery is associated with a reduction of anastomotic leak rate. Updates Surg. (2020) 72(4):991–8. doi: 10.1007/s13304-020-00758-x
2. Sciuto A, Merola G, De Palma GD, Sodo M, Pirozzi F, Bracale UM, et al. Predictive factors for anastomotic leakage after laparoscopic colorectal surgery. World J Gastroenterol. (2018) 24(21):2247–60. doi: 10.3748/wjg.v24.i21.2247
3. Würtz HJ, Bundgaard L, Rahr HB, Frostberg E. Anastomosis technique and leakage rates in minimally invasive surgery for right-sided colon cancer. A retrospective national cohort study. Int J Colorectal Dis. (2022) 37(3):701–8. doi: 10.1007/s00384-022-04107-9
4. Garfinkle R, Abou-Khalil J, Morin N, Ghitulescu G, Vasilevsky CA, Gordon P, et al. Is there a role for oral antibiotic preparation alone before colorectal surgery? ACS-NSQIP analysis by coarsened exact matching. Dis Colon Rectum. (2017) 60(7):729–37. doi: 10.1097/DCR.0000000000000851
5. Milone M, Di Minno MN, Musella M, Maietta P, Iaccarino V, Barone G, et al. Computed tomography findings of pneumatosis and portomesenteric venous gas in acute bowel ischemia. World J Gastroenterol. (2013) 19(39):6579–84. doi: 10.3748/wjg.v19.i39.6579
6. Yost MT, Jolissaint JS, Fields AC, Whang EE. Mechanical and oral antibiotic bowel preparation in the era of minimally invasive surgery and enhanced recovery. J Laparoendosc Adv Surg Tech A. (2018) 28(5):491–5. doi: 10.1089/lap.2018.0072
7. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. (2009) 250(2):187–96. doi: 10.1097/SLA.0b013e3181b13ca2
8. Di Minno MN, Milone M, Mastronardi P, Ambrosino P, Di Minno A, Parolari A, et al. Perioperative handling of antiplatelet drugs. A critical appraisal. Curr Drug Targets. (2013) 14(8):880–8. doi: 10.2174/1389450111314080008
9. Cirillo V, Zito Marinosci G, De Robertis E, Iacono C, Romano GM, Desantis O, et al. Navigator® and SmartPilot® View are helpful in guiding anesthesia and reducing anesthetic drug dosing. Minerva Anestesiol. (2015) 81(11):1163–9.
10. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. (2004) 240(2):205–13. doi: 10.1097/01.sla.0000133083.54934.ae
11. Ceccarelli G, Andolfi E, Biancafarina A, Rocca A, Amato M, Milone M, et al. Robot-assisted surgery in elderly and very elderly population: our experience in oncologic and general surgery with literature review. Aging Clin Exp Res. (2017) 29(Suppl 1):55–63. doi: 10.1007/s40520-016-0676-5
12. Milone M, Vignali A, Milone F, Pignata G, Elmore U, Musella M, et al. Colorectal resection in deep pelvic endometriosis: surgical technique and post-operative complications. World J Gastroenterol. (2015) 21(47):13345–51. doi: 10.3748/wjg.v21.i47.13345
13. Milone M, Elmore U, Vignali A, Mellano A, Gennarelli N, Manigrasso M, et al. Pulmonary complications after surgery for rectal cancer in elderly patients: evaluation of laparoscopic versus open approach from a multicenter study on 477 consecutive cases. Gastroenterol Res Pract. (2017) 2017:5893890. doi: 10.1155/2017/5893890
14. Milone M, Manigrasso M, Burati M, Velotti N, Milone F, De Palma GD. Surgical resection for rectal cancer. Is laparoscopic surgery as successful as open approach? A systematic review with meta-analysis. PLoS One. (2018) 13(10):e0204887. doi: 10.1371/journal.pone.0204887
15. Milone M, Elmore U, Vignali A, Gennarelli N, Manigrasso M, Burati M, et al. Recovery after intracorporeal anastomosis in laparoscopic right hemicolectomy: a systematic review and meta-analysis. Langenbecks Arch Surg. (2018) 403(1):1–10. doi: 10.1007/s00423-017-1645-y
16. Kawada K, Hasegawa S, Hida K, Hirai K, Okoshi K, Nomura A, et al. Risk factors for anastomotic leakage after laparoscopic low anterior resection with DST anastomosis. Surg Endosc. (2014) 28(10):2988–95. Erratum in: Surg Endosc. 2014 Oct;28(10):2996-7. doi: 10.1007/s00464-014-3564-0
17. Zhu QL, Feng B, Lu AG, Wang ML, Hu WG, Li JW, et al. Laparoscopic low anterior resection for rectal carcinoma: complications and management in 132 consecutive patients. World J Gastroenterol. (2010) 16(36):4605–10. doi: 10.3748/wjg.v16.i36.4605
18. Park JS, Choi GS, Kim SH, Kim HR, Kim NK, Lee KY, et al. Multicenter analysis of risk factors for anastomotic leakage after laparoscopic rectal cancer excision: the Korean laparoscopic colorectal surgery study group. Ann Surg. (2013) 257(4):665–71. doi: 10.1097/SLA.0b013e31827b8ed9
19. Silva-Velazco J, Stocchi L, Costedio M, Gorgun E, Kessler H, Remzi FH. Is there anything we can modify among factors associated with morbidity following elective laparoscopic sigmoidectomy for diverticulitis? Surg Endosc. (2016) 30(8):3541–51. doi: 10.1007/s00464-015-4651-6
20. Yamamoto S, Fujita S, Akasu T, Inada R, Moriya Y, Yamamoto S. Risk factors for anastomotic leakage after laparoscopic surgery for rectal cancer using a stapling technique. Surg Laparosc Endosc Percutan Tech. (2012) 22(3):239–43. doi: 10.1097/SLE.0b013e31824fbb56
21. Hamabe A, Ito M, Nishigori H, Nishizawa Y, Sasaki T. Preventive effect of diverting stoma on anastomotic leakage after laparoscopic low anterior resection with double stapling technique reconstruction applied based on risk stratification. Asian J Endosc Surg. (2018) 11(3):220–6. doi: 10.1111/ases.12439
22. Milone M, Elmore U, Allaix ME, Bianchi PP, Biondi A, Boni L, et al. Fashioning enterotomy closure after totally laparoscopic ileocolic anastomosis for right colon cancer: a multicenter experience. Surg Endosc. (2020) 34(2):557–63. doi: 10.1007/s00464-019-06796-w
23. Choi DH, Hwang JK, Ko YT, Jang HJ, Shin HK, Lee YC, et al. Risk factors for anastomotic leakage after laparoscopic rectal resection. J Korean Soc Coloproctol. (2010) 26(4):265–73. doi: 10.3393/jksc.2010.26.4.265
24. Huh JW, Kim HR, Kim YJ. Anastomotic leakage after laparoscopic resection of rectal cancer: the impact of fibrin glue. Am J Surg. (2010) 199(4):435–41. doi: 10.1016/j.amjsurg.2009.01.018
25. Shogan BD, Carlisle EM, Alverdy JC, Umanskiy K. Do we really know why colorectal anastomoses leak? J Gastrointest Surg. (2013) 17(9):1698–707. doi: 10.1007/s11605-013-2227-0
26. Gallotta V, Fanfani F, Fagotti A, Chiantera V, Legge F, Gueli Alletti S, et al. Mesenteric lymph node involvement in advanced ovarian cancer patients undergoing rectosigmoid resection: prognostic role and clinical considerations. Ann Surg Oncol. (2014) 21(7):2369–75. doi: 10.1245/s10434-014-3558-0
27. Boni L, Fingerhut A, Marzorati A, Rausei S, Dionigi G, Cassinotti E. Indocyanine green fluorescence angiography during laparoscopic low anterior resection: results of a case-matched study. Surg Endosc. (2017) 31(4):1836–40. doi: 10.1007/s00464-016-5181-6
28. Jafari MD, Lee KH, Halabi WJ, Mills SD, Carmichael JC, Stamos MJ, et al. The use of indocyanine green fluorescence to assess anastomotic perfusion during robotic assisted laparoscopic rectal surgery. Surg Endosc. (2013) 27(8):3003–8. doi: 10.1007/s00464-013-2832-8
29. Morales-Conde S, Alarcón I, Yang T, Licardie E, Camacho V, Aguilar Del Castillo F, et al. Fluorescence angiography with indocyanine green (ICG) to evaluate anastomosis in colorectal surgery: where does it have more value? Surg Endosc. (2020) 34(9):3897–907. doi: 10.1007/s00464-019-07159-1
30. Hasegawa H, Tsukada Y, Wakabayashi M, Nomura S, Sasaki T, Nishizawa Y, et al. Impact of intraoperative indocyanine green fluorescence angiography on anastomotic leakage after laparoscopic sphincter-sparing surgery for malignant rectal tumors. Int J Colorectal Dis. (2020) 35(3):471–80. doi: 10.1007/s00384-019-03490-0
31. Ishii M, Hamabe A, Okita K, Nishidate T, Okuya K, Usui A, et al. Efficacy of indocyanine green fluorescence angiography in preventing anastomotic leakage after laparoscopic colorectal cancer surgery. Int J Colorectal Dis. (2020) 35(2):269–75. doi: 10.1007/s00384-019-03482-0
32. Brescia A, Pezzatini M, Romeo G, Cinquepalmi M, Pindozzi F, Dall’Oglio A, et al. Indocyanine green fluorescence angiography: a new ERAS item. Updates Surg. (2018) 70(4):427–32. doi: 10.1007/s13304-018-0590-9
33. Kin C, Vo H, Welton L, Welton M. Equivocal effect of intraoperative fluorescence angiography on colorectal anastomotic leaks. Dis Colon Rectum. (2015) 58(6):582–7. doi: 10.1097/DCR.0000000000000320
34. Jafari MD, Wexner SD, Martz JE, McLemore EC, Margolin DA, Sherwinter DA, et al. Perfusion assessment in laparoscopic left-sided/anterior resection (PILLAR II): a multi-institutional study. J Am Coll Surg. (2015) 220(1):82–92.e1. doi: 10.1016/j.jamcollsurg.2014.09.015
35. Boni L, David G, Dionigi G, Rausei S, Cassinotti E, Fingerhut A. Indocyanine green-enhanced fluorescence to assess bowel perfusion during laparoscopic colorectal resection. Surg Endosc. (2016) 30(7):2736–42. doi: 10.1007/s00464-015-4540-z
36. Amagai H, Miyauchi H, Muto Y, Uesato M, Ohira G, Imanishi S, et al. Clinical utility of transanal indocyanine green near-infrared fluorescence imaging for evaluation of colorectal anastomotic perfusion. Surg Endosc. (2020) 34(12):5283–93. doi: 10.1007/s00464-019-07315-7
37. Wada T, Kawada K, Takahashi R, Yoshitomi M, Hida K, Hasegawa S, et al. ICG fluorescence imaging for quantitative evaluation of colonic perfusion in laparoscopic colorectal surgery. Surg Endosc. (2017) 31(10):4184–93. doi: 10.1007/s00464-017-5475-3
38. Hayami S, Matsuda K, Iwamoto H, Ueno M, Kawai M, Hirono S, et al. Visualization and quantification of anastomotic perfusion in colorectal surgery using near-infrared fluorescence. Tech Coloproctol. (2019) 23(10):973–80. doi: 10.1007/s10151-019-02089-5
39. Son GM, Kwon MS, Kim Y, Kim J, Kim SH, Lee JW. Quantitative analysis of colon perfusion pattern using indocyanine green (ICG) angiography in laparoscopic colorectal surgery. Surg Endosc. (2019) 33(5):1640–9. doi: 10.1007/s00464-018-6439-y
40. D’Urso A, Agnus V, Barberio M, Seeliger B, Marchegiani F, Charles AL, et al. Computer-assisted quantification and visualization of bowel perfusion using fluorescence-based enhanced reality in left-sided colonic resections. Surg Endosc. (2021) 35(8):4321–31. doi: 10.1007/s00464-020-07922-9
Keywords: indocyanine green, colorectal cancer, perfusion, minimally invasive surgery, nearinfrared fluorescence
Citation: Maione F, Manigrasso M, Chini A, Vertaldi S, Anoldo P, D’Amore A, Marello A, Sorrentino C, Cantore G, Maione R, Gennarelli N, D’Angelo S, D’Alesio N, De Simone G, Servillo G, Milone M and De Palma GD (2022) The Role of Indocyanine Near-Infrared Fluorescence in Colorectal Surgery. Front. Surg. 9:886478. doi: 10.3389/fsurg.2022.886478
Received: 28 February 2022; Accepted: 2 May 2022;
Published: 20 May 2022.
Edited by:
Alberto Realis Luc, Clinica Santa Rita, ItalyReviewed by:
Ludovico Carbone, University of Siena, ItalyCopyright © 2022 Maione, Manigrasso, Chini, Vertaldi, Anoldo, D'Amore, Marello, Sorrentino, Cantore, Maione, Gennarelli, D'Angelo, D'Alesio, De Simone, Servillo, Milone and De Palma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Maione ZnJhbmNlc2NvbWFpb25lNzlAZ21haWwuY29t; Alessia Chini ZHIuYWxlc3NpYWNoaW5pQGdtYWlsLmNvbQ==
Specialty section: This article was submitted to Visceral Surgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.