 Shangren Wang1,‡
Shangren Wang1,‡ Shiqiao Huang2,‡
Shiqiao Huang2,‡ Yang Pan1Yong Ma2
Yang Pan1Yong Ma2 Jiaqi Kang1Li Liu1Xiaoqiang Liu1*†https://orcid.org/0000-0003-3524-6783
Jiaqi Kang1Li Liu1Xiaoqiang Liu1*†https://orcid.org/0000-0003-3524-6783
- 1Department of Urology, Tianjin Medical University General Hospital, Tianjin, China
- 2Department of Urology, Shanxian Central Hospital (Affiliated Huxi Hospital of Jining Medical University), Heze, China
Purpose: It is rare to find a large leiomyoma in the prostate, especially in that of a young man. This case report and systematic review provides additional information on the diagnosis, distinguishing features of imaging examinations, and treatment options.
Patients and Methods: We report on the case of a thirty-year-old man with a large leiomyoma of the prostate. MRI of the prostate revealed a round mass in the posterior lobe, 8.0 × 8.0 × 5.5 cm in size. With the assistance of laparoscopy, we resected the prostate mass completely and spared this organ. A systematic review was conducted utilizing the Preferred Reporting Items for Systematic Reviews (PRISMA) including English language published reports, from 1970 to December 2021.
Results: Urinary and erectile functioning was preserved postoperatively. After a year of follow-up, no evidence of recurrence emerged. A total of 21 studies were included for analysis.
Conclusions: A medical history of no, or few, lower urinary tract symptoms; the characteristics of a benign tumor in imaging examinations; and negative tumor markers should be included in any differential diagnosis of leiomyoma of the prostrate. A prostate biopsy should be performed before the preparative radical prostatectomy and choose nonsurgical treatment to confirm the diagnosis. Nowadays, minimally invasive surgery is the preferred effective option for this disease. It is a rare recurrence after its removal by means of surgery.
Introduction
Leiomymia, most commonly located in the uterus, is a benign tumor composed of smooth muscle fibers (1). A leiomyoma in the prostate is rare, especially a large leiomymia in the prostrate of a young man (2). Leiomyoma of the prostrate may be misdiagnosed as prostate cancer. Treatments for leiomyoma of the prostate have changed in the past decades, and newer treatment options have been applied such as minimally invasive surgery and embolization. Our case and systematic review provides additional information on diagnosis, distinguishing features of imaging examinations, and treatment options.
Case report
A thirty-year-old man presented at our urology department for a mass in the prostate which had been identified during a routine physical examination. He reported no urinary tract symptoms and no other medical history. On digital rectal examination (DRE), we found a large, solid prostate mass.
Laboratory tests showed a prostate-specific antigen (PSA) level of 1.28 ng/ml (normal 0.00–4.00), a free PSA (f-PSA) level of 0.63 ng/ml (normal 0.00–0.93), a carcinoembryonic antigen (CEA) level of 0.5 ng/ml (normal 0.0–5.0), a carbohydrate antigen 199 (CA199) level of 2.3 U/ml (normal 0.0–37.0), a carbohydrate antigen 50 (CA50) level of 3.5 U/ml (normal 0.0–25.0), an α-fetoprotein (AFP) level of 4.9 ng/ml (normal 0.0–15.0), and a neuron-specific enolase (NSE) level of 6.7 ng/ml (normal 0.0–12.5). The patient had normal renal function, normal liver function and negative urinalysis results.
Magnetic resonance imaging (MRI) of the prostate revealed a round mass in the posterior lobe, 8.0 × 8.0 × 5.5 cm in size (Figure 1). With no mass invasion, prostatic glandular tissue and seminal vesicles were compressed anteriorly, and the rectum was compressed posteriorly. A well-circumscribed capsule was observed around the tumor between the normal prostate, seminal vesicles, rectum and other organizational structures (Figure 1). The capsule was clearly visible on MRI axial fat-suppressed T2-weighted images. This capsule was not the tumor's intrinsic capsule; therefore, we referred to it as the surgical capsule (Figure 1C arrow; Figure 1D light blue and arrow).
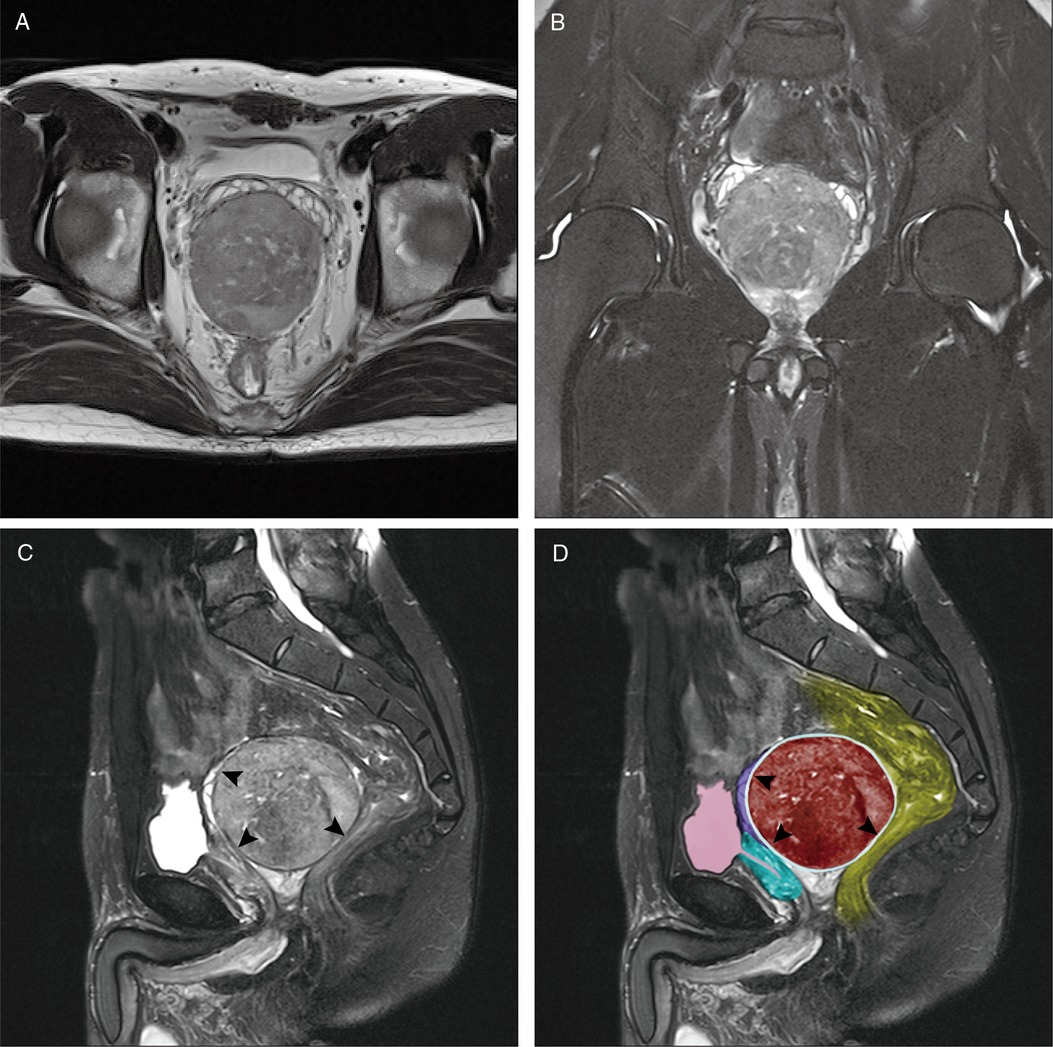
Figure 1. MRI of the leiomyoma of the prostate. MRI T2-weighted axial image (A) and fat-suppressed coronal image (B) shows a round mass in the prostate posterior lobe; fat-suppressed sagittal image (C,D) shows the clear surgical capsule of the tumor (arrow) and shows that normal prostatic glandular tissue and seminal vesicles were compressed anteriorly. The rectum was compressed posteriorly (red: leiomyoma of the prostate; green: prostate; pink: bladder and urethra; yellow: rectum; purple: seminal vesicles; light blue and arrow: surgical capsule of the tumour).
Based on the patient's medical history, PSA and other tumor markers were negative, and MRI revealed a spherically shaped tumor with a surgical capsule. The preoperative diagnosis was a benign prostate tumour. With the assistance of laparoscopy, we resected the prostate mass completely and were able to spare it. We placed three working ports in the abdomen: a 10-mm umbilical port, and 12-mm and 5-mm trocars located at the right and left of the lateral border of the rectus abdominis, respectively. Cavity insufflation of carbon dioxide and abdominal pressure was maintained at 12–14 mmHg. A fifteen degree head-down tilt operating table was used. We found an 8.0 × 8.0 cm solid round mass protruding in the center of the pelvis and outside the peritoneum. The bladder was lifted forward and the peritoneum of the bladder rectal lacuna was opened. The tumor was located between the seminal vesicles and the rectum. The tumor capsule was complete and a clear space (surgical capsular) was not adherent to surrounding organs. The vas deferens, seminal vesicles, and rectum were dissected and protected. Within the surgical capsular space and the external intrinsic capsule of the mass, the tumor was carefully isolated from the prostate tissue with an ultrasound knife, as hemostasis was maintained (Figure 2A). Eventually, the tumor was completely removed (Figure 2B), and the prostate and surrounding structures were spared. A pelvic drainage tube was placed. The amount of intraoperative bleeding was approximately 50 ml and no blood transfusion was required. The surgical procedure was smooth with a duration of 2 h.
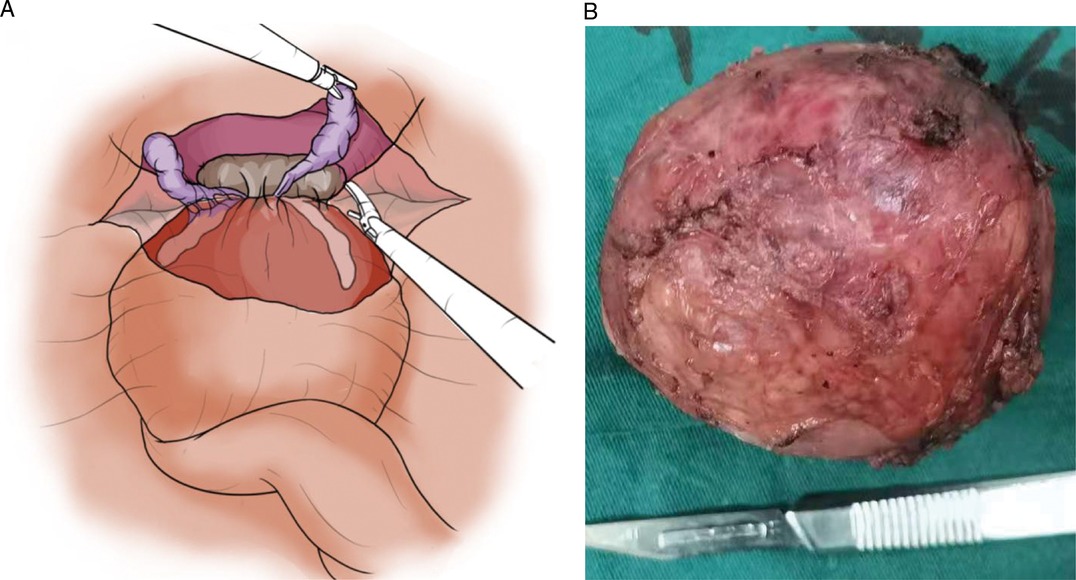
Figure 2. We were able to spare the prostate with the assistance of laparoscopy (A) and the prostate mass was completely resected (B).
Histopathological examination exhibited a bland spindle cell proliferation (Figure 3A). Immunohistochemical staining was positive for smooth muscle actin (SMA) (Figure 3B) and desmin (Figure 3C), and CD34 (vascular endothelium +, proliferating cells -) was negative for S-100, CD117, Dog-1, CK, and ALK. The Ki-67 proliferation index was low (3%-5%), and the pathological diagnosis was leiomyoma of the prostate.
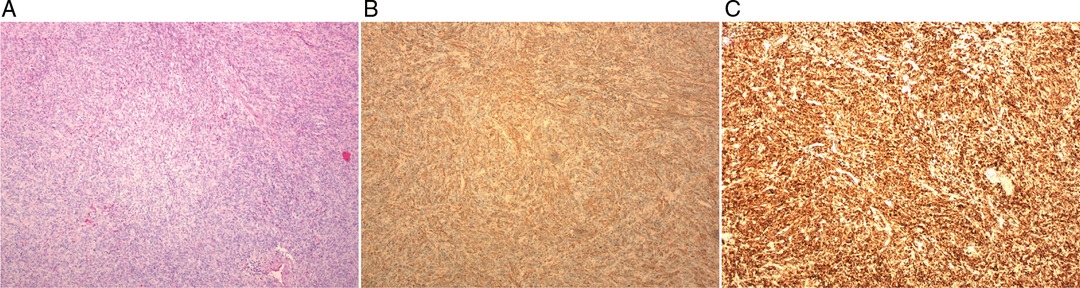
Figure 3. The pathology of leiomyoma of the prostate. (A): Histopathological examination showed bland spindle cell proliferation (200×). (B,C): Immunohistochemical staining was positive for smooth muscle actin (SMA) (B) and Desmin (C).
The patient did not develop any urinary dysfunction after 10 days of surgery and was discharged. During follow-up sessions for a year, the patient's score of International Index of Erectile Function (IIEF 5) (before 23 vs. after 22), International Prostate Symptom Score (IPSS) (before 5 vs. after 2), and Quality of Life (QOL) (before 2 vs. after 2) had no significant difference before and after surgery. Therefore, the patient's urinary function, sexual function and quality of life did not change as compared to before the surgery. And no evidence of recurrence was evident.
Systematic review
Methods
A systematic review was conducted utilizing the Preferred Reporting Items for Systematic Reviews (PRISMA) (3). We searched in PubMed, Web of Science databases, Embase, and Medline in the English language from 1970 to December 2021. The keywords used were “Leiomyoma” and “prostate”. All the case reports and series studies were included in this research. All non-English, review articles, for which we could not obtain a full text, were excluded. We extracted the following details of each article: first author, date of publication, country, numbers of patients, age, symptoms, PSA, DRE, the size of the tumor, position, biopsy or not, imaging examinations, initial diagnosis, treatment, follow-up and malignancy.
Results
After the selection procedure according to PRISMA (Figure 4), a total of 21 studies were included in our systematic review (1, 2, 4, 6–23). There were 35 cases of leiomyoma of the prostate included for analysis and characteristics of the cases are shown in Table 1.
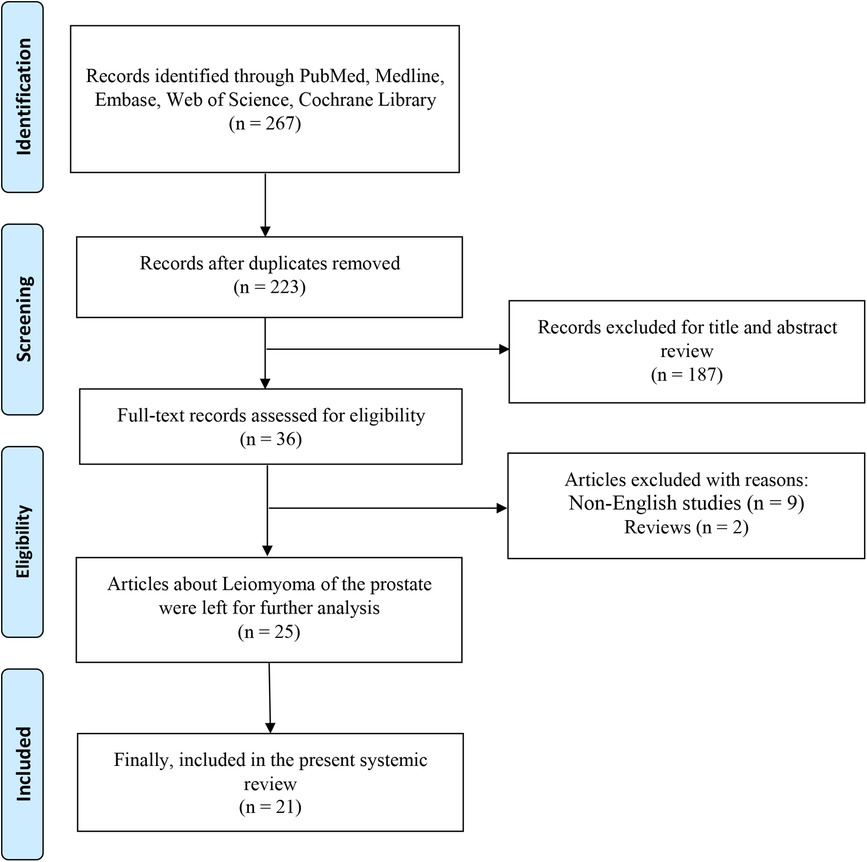
Figure 4. PRISMA flowchart of literature selection process.
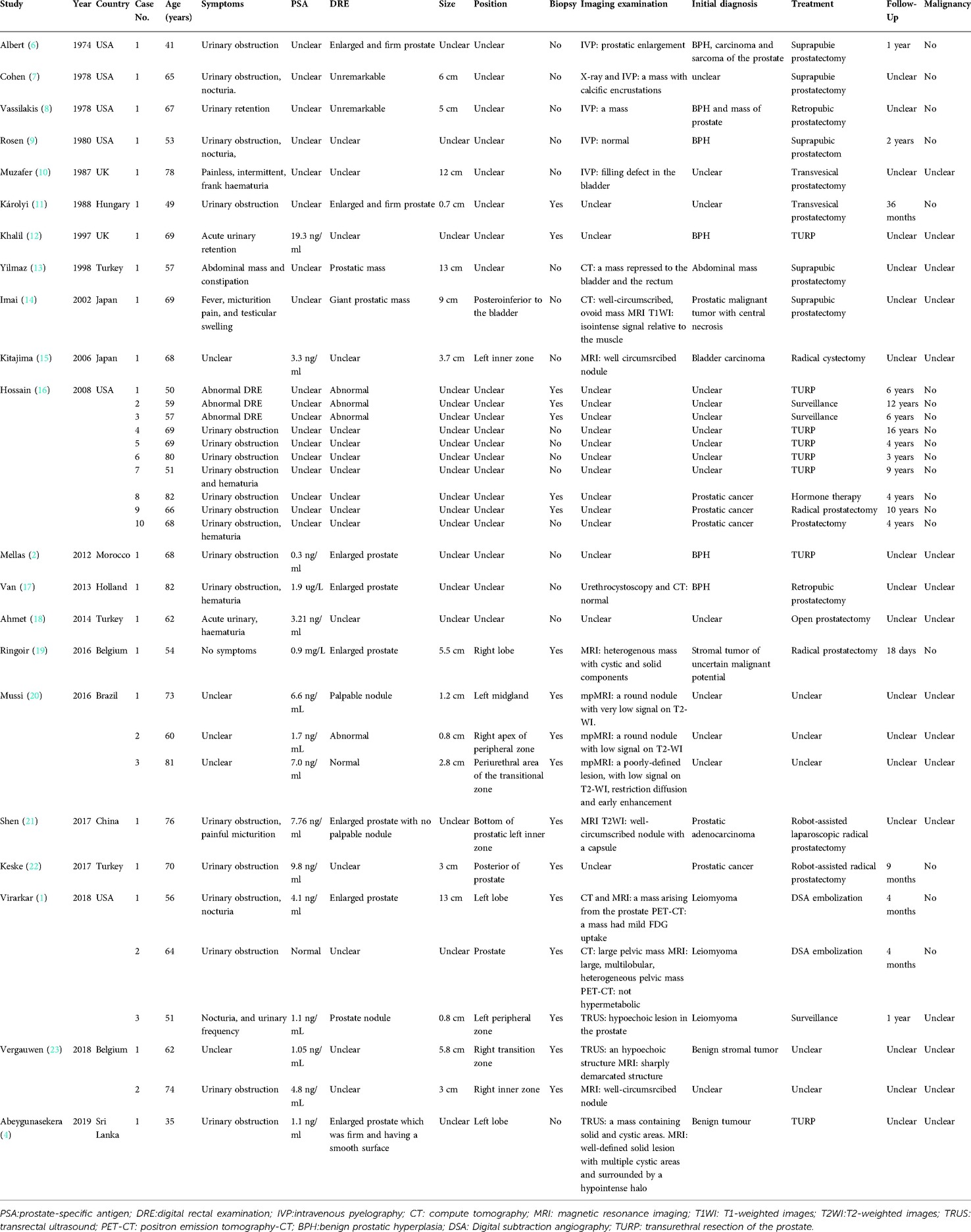
Table 1. Characteristics of cases with leiomyoma of the prostate.
The average age of the patients was 63.86 ± 1.94 years old. The average size (diameter) of the tumors was 5.73 ± 1.03 cm. Leiomyoma of the prostate appeared more frequently in 50–60 year old men (26%) and 60–70 year old men (41%). It rarely occurred in young men <40 years (3%) (Figure 5A). With regard to diagnosis, a biopsy was performed in about 51% cases to obtain a preoperative diagnosis or to distinguish the mass from a malignant prostate tumor (Figure 5B). About 17% cases of leiomyoma of the prostate combined with other malignant tumors, such as prostate cancer or bladder cancer (Figure 5C). For treatment, the majority of cases were subjected to surgical treatment (74%), and only 11% cases were selected for active surveillance (Figure 5D). In the past approximately 50 years, the surgical method of choice for leiomyoma of the prostate has gradually changed from open surgery to minimally invasive surgery (Figure 6). Meanwhile, imaging examinations for leiomyoma of the prostate have changed from X-rays or intravenous pyelograms to computed tomography (CT), MRI, and positron emission tomography-CT (PET-CT) (Figure 6).
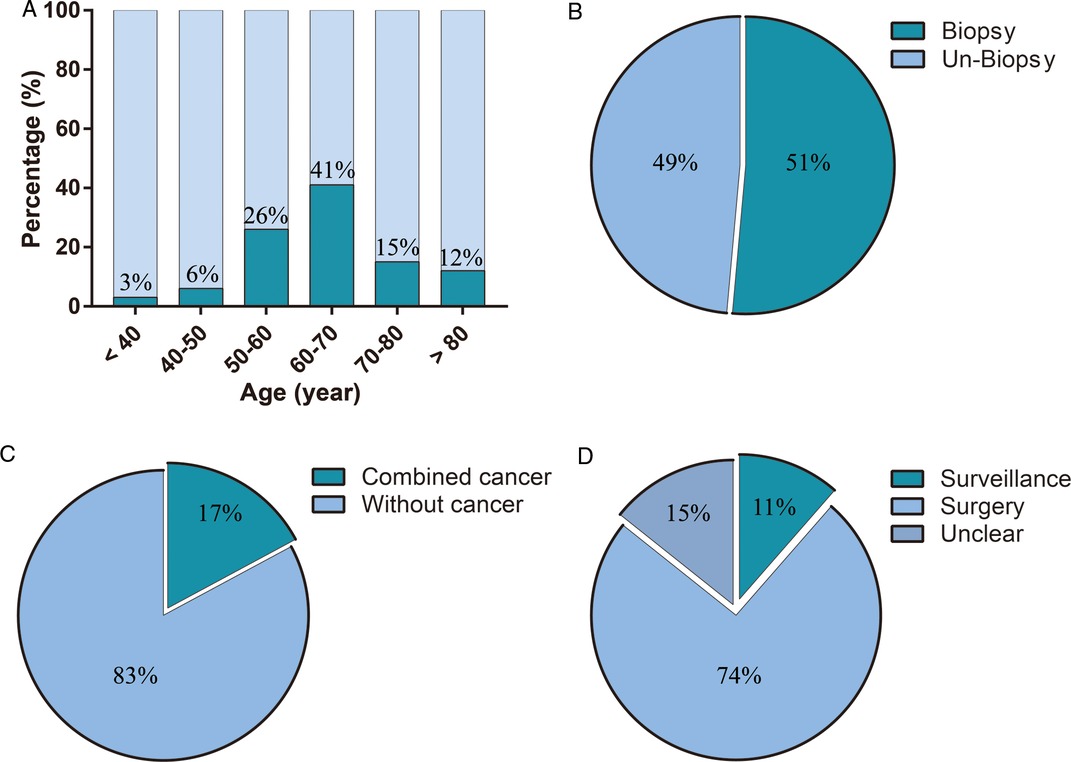
Figure 5. The features of leiomyoma of the prostate, and the experience of diagnosis and treatment. (A) age of patients, (B) features of biopsy, (C) features of combined diseases, (D) features of treatment.
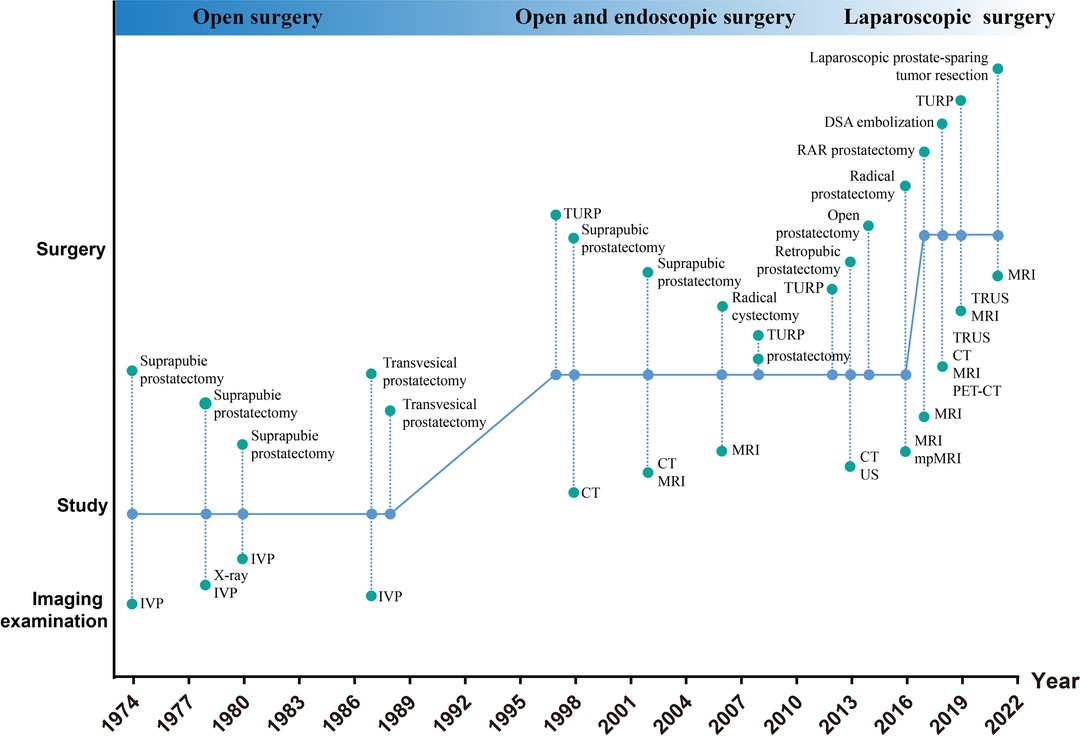
Figure 6. Shifts in the past 50 years of methods of treatment and imaging examination for leiomyoma of the prostate. IVP:intravenous pyelography; CT: compute tomography; MRI: magnetic resonance imaging; PET-CT: positron emission tomography-CT; TRUS: transrectal ultrasound; DSA: Digital subtraction angiography; TURP: transurethral resection of the prostate.
Discussion
Leiomyomas are rarely found in the prostate. Kaufman et al. reviewed the relevant literature and first defined the leiomyoma of the prostate as “a circumscribed and encapsulated mass of smooth muscle, 1 cm or more in diameter, containing varying amounts of fibrous tissue but devoid of glandular elements and which is either obviously prostatic or juxta prostatic in origin and position” (5). The exact pathogenesis is still unclear. Inflammatory, infectious and embryological Müllerian duct remnants are the possible mechanisms of pathogenesis (24).
In past decades, some case report studies of leiomyoma of the prostate have been published (1). However, there are still no available guidelines. Imaging diagnoses, preoperative diagnoses, treatment methods and surgical techniques have been insufficiently explored.
We have presented a case of a thirty years old man, who, to our knowledge, is the youngest man suffering from a huge leiomyoma of the prostate in a reported case. In this study, we analyzed the typical imaging features of leiomyoma of the prostate on MRI, and explored prostate-sparing and simple tumor surgical removal techniques. Meanwhile, we performed a systematic review of the English language literature from 1970 to 2021, a period spanning about 50 years, focusing on the features of leiomyoma of the prostate, and the descriptions of diagnosis, imaging examinations and surgical treatments.
Demographics
Leiomyoma of the prostate occurs more frequently in middle-aged or older men (17). Previous reports have shown that the average age of patients is 63.86 ± 1.94 years old (ranging from 35 to 82 years old). Leiomyoma of the prostate occurs more frequently in 50–60 year old men (26%) and 60–70 year old men (41%). It occurs rarely in young men. In our review, only one case was thirty-five years old (4). In our case report, the patient is a thirty-year-old man. To our knowledge, our case presents the youngest male who has suffered from a leiomyoma of the prostate.
Diagnosis
Leiomyoma of the prostate has non-specific symptoms. On digital rectal examination, we found a solid prostate mass. Previous reports have shown that lower urinary tract symptoms are common. These include dysuria, urinary frequency, significant nocturia, urgency, painful micturition and acute urinary retention (1, 4, 19). Gross haematuria is a rare symptom, and in our systematic review, only 3 cases reported gross haematuria (10, 17, 18). A large leiomyoma in the prostate posterior lobe would place pressure on the rectum leading to constipation (13).
Leiomyoma of the prostate is sometimes difficult to distinguish from benign prostatic hyperplasia or prostate cancer. In older men, leiomyomas are usually combined with benign prostatic hyperplasia and other malignant tumors, such as prostate cancer or bladder cancer (15, 16). Some leiomyomas of the prostate have been identified in surgical specimens of benign prostatic hyperplasia, prostate cancer and bladder cancer (12, 15).
Few reports have described the features of imaging examinations (14, 15). A hypoechoic or hyperechoic lesion in the prostate may be evident in transrectal ultrasonography (1, 12). A mass of the prostate in the pelvis can be seen in CT imaging (14). These masses are usually well-circumscribed nodules or masses and no lymphadenopathy or distant metastasis may be detected. PET-CT would exhibit no hypermetabolic mass of the prostate (1).
MRI features of leiomyoma of the prostate reveal a well-circumscribed round mass, with isointense and homogeneous signals relative to the muscle on T1WI. A slightly hyperintense or hypointense well-circumscribed mass with a capsule around the tumor between the normal prostate, seminal vesicles, rectum and other organizational structures are exhibited in a T2WI image (23). The capsule is clearly visible in MRI axial fat-suppressed T2-weighted images. It is a feature of a benign tumor. Other traditional and new imaging methods may provide us with more other useful information to make a correct diagnosis, such as TURS, CT, PET-CT.
In our case, the clear surgical capsule around the tumor could be seen in MRI imaging and helped us to make a differential diagnosis from prostate cancer. This capsule was not the tumor's intrinsic capsule. During surgery, along with the capsular space and the external intrinsic capsule of the tumor, we resected the prostate mass completely and were able to spare the prostate. Thus, we referred to it as the surgical capsule.
In general, the PSA of a prostate leiomyoma or leiomyo sarcoma is at a normal level. Abdollahi's study found that PSA has little clinical utility in the diagnosis of leiomyoma (24). When prostate leiomyoma is combined with BPH or prostate cancer, the PSA level becomes raised (12, 20). Biopsy is then useful in assisting with a correct diagnosis. In previous reports, biopsies were performed on about 51% cases before surgery. A preoperative biopsy of the prostate in a small prostate leiomyoma or a prostate leiomyoma of irregular shape is necessary as it is difficult to distinguish between prostate malignant tumors, such as leiomyoma sarcomas, adenocarcinomas and retrovesical ectopic prostatic adenomas (25). We recommend that a prostate biopsy should be performed before the preparative radical prostatectomy to confirm the diagnosis and avoid excessive diagnosis and therapy. And prostate biopsy is necessary for patients who choose nonsurgical treatment to avoid the risk of cancer.
In our case, the PSA was at a normal level, the age of the man was young and on MRI the characteristics of a benign tumor were exhibited. This information did not appear to support a diagnosis of cancer. Nevertheless, we recommend that patients undergo prostate biopsies preoperatively. Moreover, the behavior of the patient was an important factor in our choice of treatment. After communicating with him, he refused to undergo a biopsy as he feared that he would have to wait too long for surgery after the biopsy.
When there is a medical history of no, or few, lower urinary tract symptoms, evident characteristics of a benign tumor in imaging examinations, and negative tumor markers, leiomyoma of the prostate should be included in the differential diagnosis.
The final diagnosis may be reached by histopathological and immunohistochemical analysis (12, 20). The mass of leiomyoma of the prostate is usually well circumscribed, with a smooth surface. It is a homogeneous solid mass with gross features similar to that of a uterine leiomyomas. The mass is composed of bland spindle proliferating cells on microscopic evaluation. No atypical mitosis, pleomorphism or glandular component is identified. In immunohistochemical analysis, the spindle cells are positive for smooth muscle actin (SMA) and desmin. CD34 is negative, in contrast to stromal tumors of unknown malignant potential.
Treatment
Methods of treatment for leiomyoma of the prostate have changed in the past decades. Prostatectomy was considered the standard surgical approach for leiomyomas of the prostate before the 1990s (10). For aging men, leiomyoma of the prostate frequently combines with benign prostatic hyperplasia. With the development of endoscopic surgery, the transurethral resection of the prostate (TURP) has been gradually applied to the treatment of leiomyoma of the prostate. However, it is important in the case of young men to protect their sexual functioning. At present, with the development of laparoscopy technology, prostate-sparing and simple tumor surgical removal is achievable for pelvic or retroperitoneum tumors (26). However, use of this surgical technique has been rarely reported in studies of leiomyoma of the prostate. In our case, with the assistance of laparoscopy, we resected the prostate mass completely, and the prostate was spared. Furthermore, the urinary and sexual functioning of the patient was preserved after surgery. The key to success in prostate sparing is accurately identifying the surgical capsular space.
Prostate artery embolization is a treatment option for men who are not suited to surgical treatment (1, 23). Active surveillance of asymptomatic patients with a low risk of prostate cancer is necessary. The key to successful nonsurgical treatment lies with the selection of appropriate candidates.
Prognosis
Leiomyoma of the prostate is a benign tumor. No reports have indicated recurrence of prostatic leiomyomas after surgical removal. In our case, one year after follow-up, there was no evidence of recurrence.
Conclusion
Leiomyoma of the prostate is a benign tumor. No, or few, lower urinary tract symptoms in the medical history, negative PSA and other tumor markers, and a spherically shaped tumor with a surgical capsule on MRI are indicative of leiomyoma of the prostate, and should be included in relevant differential diagnoses. Other imaging methods may help us with diagnosis, such as TURS, CT and PET-CT. A prostate biopsy should be performed before the preparative radical prostatectomy and choose nonsurgical treatment to confirm the diagnosis. At present, minimally invasive surgery is the preferred effective option for leiomyoma of the prostate as it is important that young men preserve their urinary and sexual functioning. Furthermore, it is a rare recurrence after being completely removed by means of surgery.
Data availability statement
Data available on request from the authors.
Author contributions
SRW and SQH cared for the patient. XQL and YM developed the surgical protocol and performed the surgery. SRW, YP, JQK and XQL conducted the systematic review. All authors wrote the manuscript and approved the final manuscript. Written consent for publication was obtained from the patient.
Funding
National Natural Science Funds of China (82171594); Zhao Yi-Cheng Medical Science Foundation (ZYYFY2018031).
Acknowledgments
Thanks to Li Song, Hou Zhaoli and Wang Beicheng for the help of picture editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Virarkar M, de Castro FS, Patnana M, Zhang M, Sagebiel T. Leiomyoma of the prostate: case report and review of the literature. Clin Genitourin Cancer. (2018) 16(4):e771–6. doi: 10.1016/j.clgc.2018.01.012
2. Mellas S, Bouchikhi AA, Tazi M, Khallouk A, Elammari J, El Fassi M, et al. Prostatic leiomyoma: a case report. Case Rep Urol. (2012) 2012:1–2. doi: 10.1155/2012/702762
3. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
4. Abeygunasekera AM, Kumara MSGR, Ambegoda AMLC, Ranasingha DD, Sosai CP. Prostatic leiomyoma in a young man. Ceylon Med J. (2019) 64(2):76–7. doi: 10.4038/cmj.v64i2.8893
5. Kaufman JJ, Berneike RR. Leiomyoma of the prostate. J Urol. (1951) 65(2):297–310. doi: 10.1016/s0022-5347(17)68484-2
6. Albert PS, Sinatra T, Nagamatsu GR. Retroperitoneal leiomyoma presenting as prostatic mass. Urology (Ridgewood, N.J.). (1974) 3(5):607. doi: 10.1016/S0090-4295(74)80257-8
7. Cohen MS, Mcdonald DF, Smith JH. Solitary leiomyoma of the prostate presenting as an encrusted intravesical mass. J Urol. (1978) 120(5):641–2. doi: 10.1016/s0022-5347(17)57309-7
8. Vassilakis GB. Pure leiomyoma of prostate. Urology. (1978) 11(1):93–4. doi: 10.1016/0090-4295(78)90214-5
9. Rosen Y, Ambiavagar PC, Vuletin JC, Macchia RJ. Atypical leiomyoma of prostate. Urology (Ridgewood, N.J.). (1980) 15(2):183. doi: 10.1016/0090-4295(80)90417-3
10. Muzafer MH. Large leiomyoma of prostate. Br J Urol. (1987) 59(2):192–3. doi: 10.1111/j.1464-410x.1987.tb04820.x
11. Károlyi P, Endes P, Krasznai G, Tönköl I. Bizarre leiomyoma of the prostate. Virchows Arch A Pathol Anat Histopathol. (1988) 412(4):383–6. doi: 10.1007/BF00750266
12. Khalil KH, Rix GH, McBrien MP, Al-Rufaie HK. Bizarre leiomyoma of the prostate. Br J Urol. (1997) 79(4):660. doi: 10.1046/j.1464-410x.1997.00169.x
13. Yilmaz F, Sahin H, Hakverdi S, Arslan A, Bircan MK, Kilic N. Huge leiomyoma of the prostate. Scand J Urol Nephrol. (1998) 32(3):223–4. doi: 10.1080/003655998750015638
14. Imai S, Ayabe Y, Iiyama T, Muramatsu H, Matsuo Y, Kudo S. Leiomyoma of the prostate: cT and MR findings. Abdom imaging. (2002) 27(6):674–6. doi: 10.1007/s00261-001-0150-4
15. Kitajima K, Kaji Y, Imanaka K, Hayashi M, Kuwata Y, Sugimura K. MR Imaging findings of pure prostatic leiomyoma: a report of two cases. J Comput Assist Tomo. (2006) 30(6):910–2. doi: 10.1097/01.rct.0000220808.58350.39
16. Hossain D, Meiers I, Qian J, MacLennan GT, Bostwick DG. Prostatic leiomyoma with atypia: follow-up study of 10 cases. Ann Diagn Pathol. (2008) 12(5):328–32. doi: 10.1016/j.anndiagpath.2008.02.009
17. van Ulden-Bleumink WM, Dom PGB, Ramakers BPM, van Adrichem NPH. A rare prostatic diagnosis of an old man: a pure prostatic leiomyoma. Case Rep Urol. (2013) 2013:1–3. doi: 10.1155/2013/741235
18. Ahmet A, Altinay S. Leiomyoma of the prostate, A rare mesenchymal tumour. West Indian Med J. (2014) 63(1):116–7. doi: 10.7727/wimj.2013.173
19. Ringoir A, Rappe B, Dhaene K, Schallier D. Prostatic leiomyoma: a case Report. Urol Case Rep. (2016) 9:45–7. doi: 10.1016/j.eucr.2016.08.014
20. Mussi TC, Costa YB, Obara MT, Queiroz MRGD, Garcia RG, Longo JADC, et al. Multiparametric magnetic resonance imaging findings of prostatic pure leiomyomas. Einstein (São Paulo). (2016) 14(3):374–7. doi: 10.1590/S1679-45082016AO3715
21. Shen Y, Zhong Y, Wang H, Ma L, Wang Y, Pan J, et al. Ultra-high b-value diffusion-weighted imaging features of the prostatic leiomyoma-case report. Bmc Med Imaging. (2017) 17(1):63. doi: 10.1186/s12880-017-0234-4
22. Keske M, Canda AE, Atmaca AF, Bedir F, Gecit I, Ardicoglu A, et al. A large posteriorly located prostatic mass lesion challenging the robotic surgeon: prostate leiomyoma. Journal of Endourology Case Reports. (2017) 3(1):61–3. doi: 10.1089/cren.2017.0033
23. Vergauwen O, Vereecke E, Villeirs G. Prostatic leiomyoma – multiparametric prostate MRI features. J Belg Soc Radiol. (2018) 102(1):39. doi: 10.5334/jbsr.1543
24. Abdollahi A. Is prostate-specific antigen a reliable marker for uterine leiomyoma detection? Ann Afr Med. (2015) 14(1):57–61. doi: 10.4103/1596-3519.148743
25. Pepe P, Pepe L, Pennisi M, Fraggetta F. Giant retrovesical ectopic prostatic adenoma. Case report and revision of the literature. Urol Case Rep. (2020) 33:101383. doi: 10.1016/j.eucr.2020.101383
Keywords: prostate, leiomyoma, surgery, case report, systematic review
Citation: Wang S, Huang S, Pan Y, Ma Y, Kang J, Liu L and Liu X (2022) Leiomyoma of the prostate: A case report and systematic review. Front. Surg. 9:878411. doi: 10.3389/fsurg.2022.878411
Received: 18 February 2022; Accepted: 27 June 2022;
Published: 19 July 2022.
Edited by:
Paolo Capogrosso, University of Insubria, ItalyReviewed by:
Pietro Pepe, Cannizzaro Hospital, ItalySoufiane Mellas, Centre Hospitalier Universitaire Hassan II, Morocco
© 2022 Wang, Huang, Pan, Ma, Kang, Liu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoqiang Liu eGlhb3FpYW5nbGl1MUAxNjMuY29t
†ORCID Xiaoqiang Liu orcid.org/0000-0003-3524-6783
‡These authors have contributed equally to this work and share first authorship.
Specialty Section: This article was submitted to Genitourinary Surgery, a section of the journal Frontiers in Surgery