
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 02 November 2022
Sec. Neurosurgery
Volume 9 - 2022 | https://doi.org/10.3389/fsurg.2022.1026926
This article is part of the Research Topic Craniopharyngioma- A Multimodal Approach in the Management Dilemma View all 4 articles
 Luxwell Jokonya1*
Luxwell Jokonya1* Tariro Lavender Mduluza-Jokonya2Ignatius Esene3Garikai Mwale1
Tariro Lavender Mduluza-Jokonya2Ignatius Esene3Garikai Mwale1 Nqobile Sindiswa Thango4Takafira Mduluza1Thajasvarie Naicker2
Nqobile Sindiswa Thango4Takafira Mduluza1Thajasvarie Naicker2
Introduction: Craniopharyngioma is a rare brain tumour. Despite being histologically benign, it behaves aggressively and is often difficult to manage. Descriptive epidemiological data on the tumour is lacking in sub-Saharan Africa, and there is none for Zimbabwe. The tumour usually has a cystic component that has been raising interest in the past decade. Few studies have looked at the biochemical composition thereof. This study aims to give a landscape view of craniopharyngiomas (CPs) in Zimbabwe and then profile the biochemical properties of the cystic component of paediatric adamantinomatous craniopharyngioma.
Methodology: A prospective cohort study was done in Zimbabwe over a 2-year period to study the epidemiological distribution of craniopharyngioma and examine the biochemical composition of adamantinomatous craniopharyngioma cystic fluid in the paediatric population. Fifteen patients were recruited who had craniopharyngiomas, and of those, nine paediatric adamantinomatous craniopharyngiomas had fluid analysed for biochemical components. SPSS statistical package was used to analyse the data. Descriptive statistics were used for epidemiological data.
Results: The incidence of CP was calculated to be 0.53 per million person-years. Incidence among the paediatric population 0–14 years was 1.2 per 100,000 person-years. Several biological components were found to be elevated significantly compared to serum and cerebral spinal fluid (CSF). These are sodium, potassium, urea, alkaline phosphatase, phosphate, magnesium, albumin, gamma-glutamyl transferase, calcium, low-density lipids, and glucose.
Conclusion: The incidence of CP in Zimbabwe is similar to the rest of the world. Some biochemical components have been noted to be markedly elevated in the cystic fluid and were mirroring serum rather than CSF in concentration.
Craniopharyngioma (CP) is a benign, brain tumour that commonly occurs in the suprasellar region of the brain. It has a worldwide incidence of 0.5–2 cases per million persons per year. This represents 1%–4% of tumours in the paediatric population. In the United States alone, around 338 cases occur per annum. There have been no ethnicity or gender differences noted. Epidemiological data for this tumour are difficult, not only because the tumour is rare but also because most cancer registries compute data on malignant tumours omit CP although it is borderline malignant. Furthermore, in the international classification for the disease of oncology, CP is classified under one code even though we now know that it represents dual pathologies. Adamantinomatous craniopharyngioma occurs predominantly in the paediatric population with a peak age of 5–14 years and is of embryonal aetiology (1–5).
In contrast, papillary craniopharyngioma occurs almost exclusively in the adult population with a peak incidence at 50–74 years and is thought to originate from metaplasia of remnants of Rathke’s pouch (6). Adamantinomatous CP exhibits a dysregulation of the Wnt signalling pathway while papillary is associated in 95% of cases with BRAF V600E mutations [valine (V) is substituted by glutamic acid (E) at amino acid 600]. These two are distinct, but because of the rarity of the tumour, most epidemiological studies tend to group them two together (7).
Of all the brain tumours, CP is perhaps the only one that has undergone radical changes in clinical management because of its associated profound challenges. Preferred management has shifted from radical to conservative resection, with an acceptance that this is a chronic disease, and the goal of therapy is to provide a good quality of life rather than a cure. The majority of options favour partial debulking of the tumour, intra-cystic therapies, and radiotherapy (8–13). Raised awareness of the cystic component for Ommaya reservoirs and intra-cystic drug therapies has resulted in several studies that explore the nature and contents of this cyst. We recently reported on the possible antimicrobial properties of the cystic craniopharyngioma fluid (14, 15). This study aimed to assess the biochemical components of the CP fluid to elucidate any antimicrobial properties.
A prospective cohort study was carried out to study the epidemiology of craniopharyngiomas and the biochemical composition of adamantinomatous craniopharyngioma cystic fluid over 2 years extending from July 2019 to August 2021. The catchment area for participants encompassed the entire country of Zimbabwe, a sub-Saharan country (Figure 1). Investigators had access to all government and private patients over the study period. At the time of the study, all neurosurgical government patients were being referred to the three quaternary hospitals as shown in Figure 1. All patients included in the study had a final diagnosis of craniopharyngioma. At the time of the study, the Zimbabwean population between the ages of 0–14 years was 42,000 and the total population was 14 million. The STROBE checklist was used in the write-up of the paper.
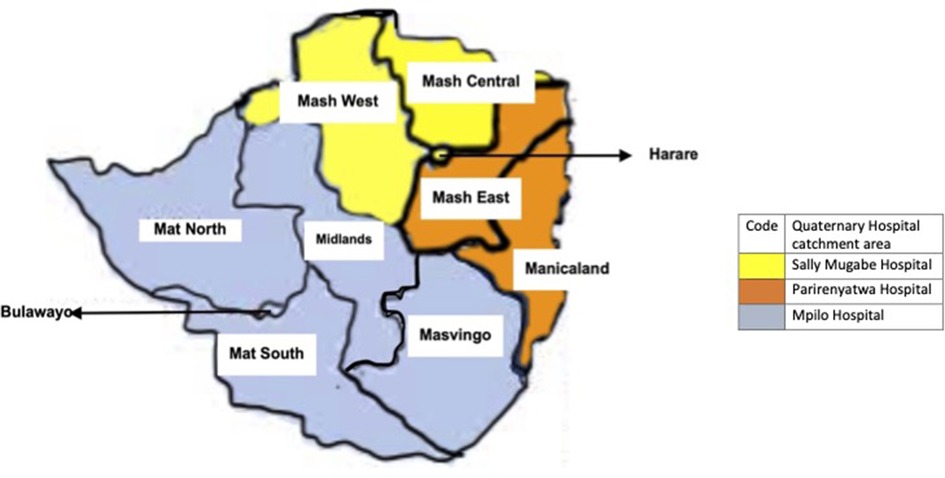
Figure 1. Map showing hospital catchment areas for neurosurgical patients in Zimbabwe.
Diagnosis of craniopharyngioma was based on histological confirmation. In a few cases where biopsy for histology was unavailable, the diagnosis was made by a consensus of two of any combination of either a senior neurosurgeon and/or a senior radiologist based on typical radiological findings (including spectrometry), and if there was any doubt, then the diagnosis was not made. Otherwise, a histological result was the gold standard.
The study did not influence or affect the standard management of craniopharyngioma which included resection, debulking, and Ommaya shunt insertion depending on the decision of the managing surgeon and the particular patient.
All patients presenting to the three main teaching hospitals in the country (only state institutions offering neurosurgery services at the time of the study) with a diagnosis of craniopharyngioma were considered for study. Liaison with all neurosurgeons in the country (eight at that time) facilitate access to those patients from the private institutions (no CP patients were seen in the private sector during the period of study). Hence, all patients seen in the country with craniopharyngiomas could be captured.
Ethical approval was obtained from the Medical Research Council of Zimbabwe (MRCZ/A/1854). Informed consent was obtained from the participants or their guardians; assent was obtained for all children above the age of 7 years.
The patients (or caregivers) were interviewed. Past hospital documentation that included imaging and histology was reviewed. Demographic, history, examinations, investigations findings, and management information were captured. Patients with missing data would be excluded.
Plasma and sera were obtained from blood collected in well-labelled ethylenediamine tetraacetic acid and coagulant-free blood collection tubes, respectively. Serum was tested for biochemical components.
CSF was collected during the insertion of a ventriculoperitoneal shunt when this was indicated for the treatment of the patient. After normal shunt insertion during the confirmation of the shunt working, some CSF fluid is allowed to drop out of the peritoneal end of the shunt.
Cystic fluid was collected, from the Ommaya reservoir, during scheduled drainage of the fluid or it was collected during surgical resection of the tumour.
The specimens were sent to a clinical pathology laboratory for biochemical analysis: urea and electrolytes, calcium, magnesium, phosphate, and liver function tests. All lipid measurements were performed in the same central laboratory. Serum concentrations of total cholesterol, high-density lipoprotein, low-density lipoprotein (LDL), cholesterol, and triglycerides were also measured.
The clinical management of the patients’ ailments was per hospital protocol, and the study did not interfere with their standard management.
Data were then captured into a software package SPSS (SPSS, Chicago) for analysis. Descriptive statistics were used to summarise the patients’ demographical and clinical data. To determine statistical significance for parametrically distributed data, a t-test or one-way ANOVA with Bonferroni multiple comparison tests were used. For non-parametric data, a Mann–Whitney or Kruskal–Wallis test along with a Dunn’s multiple comparison test was used. Comparisons of proportions were performed using the Fisher exact and Chi-square tests. Significance was accepted with p values of <0.05. Data were expressed as median (90% confidence limits) as appropriate. Incidence was calculated using the formula: .
Of a total of 15 patients with craniopharyngioma, 9 patients were diagnosed with paediatric adamantinomatous craniopharyngioma and were recruited for fluid analysis in the study (Figure 2). The number of males was 6 (66.7%) and females were 3. The mean age is 9 ± SD was ±3.07 years and varied from 4 to 14 years (Table 1).
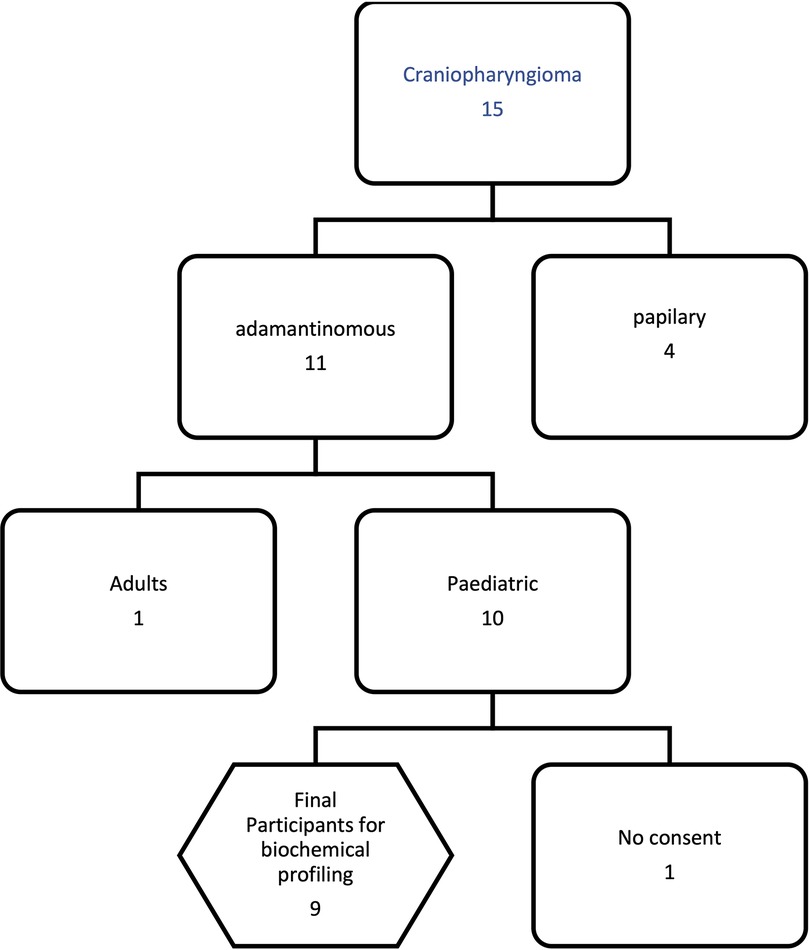
Figure 2. Study profile.
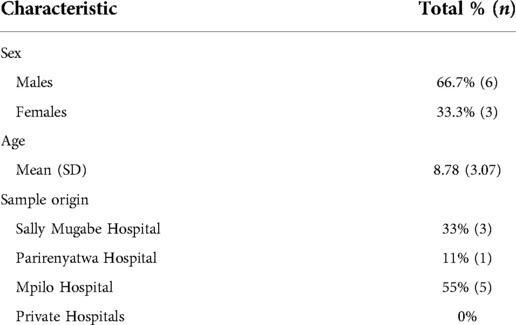
Table 1. Participant’s characteristics.
Over the 2-year study period, a total of 15 patients were diagnosed. The Zimbabwe population was estimated at 14 million; hence, the incidence of craniopharyngioma was calculated to be 0.53 per million person-years. Incidence among the paediatric population 0–14 years was 1.2 per 100,000 person-years, which translates to five children in the 0–14 years age group are expected to present for the first time with craniopharyngioma annually in Zimbabwe.
The following biochemical components were elevated in CP cystic fluid in comparison to the serum normal values: sodium, potassium, urea, alkaline phosphatase, phosphate, magnesium, albumin, gamma-glutamyl transferase (GGT), calcium, low-density lipoproteins, and glucose (Table 2). In addition, the cystic fluid also contained chloride, bilirubin, AST, ALT, creatinine, cholesterol, and amylase. The following biochemical components were present in all the fluids (serum, CSF, and the cystic fluid); sodium, potassium, chloride, urea, alkaline phosphatase, ALT, AST, albumin, GGT, calcium, creatinine cholesterol, LDL, amylase, and glucose (Table 3). Bilirubin and β-hCG were present in serum and the cystic fluid. The cystic fluid mirrored the serum as opposed to CSF (Figure 3, Table 2).
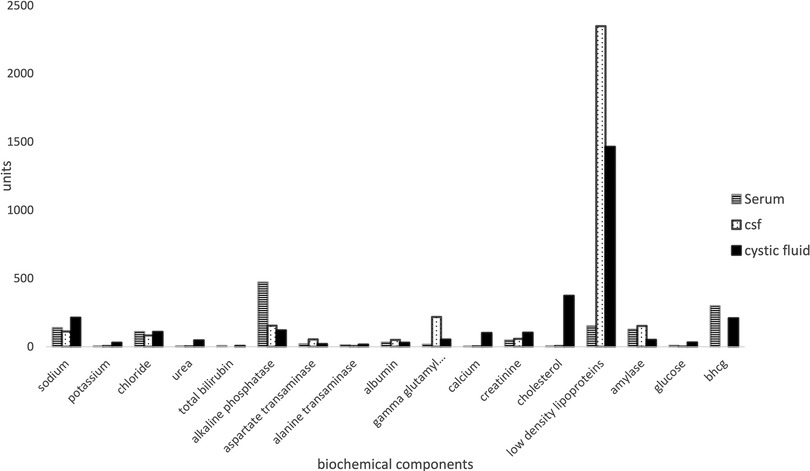
Figure 3. Relative concentrations between cystic fluid, serum, and CSF.
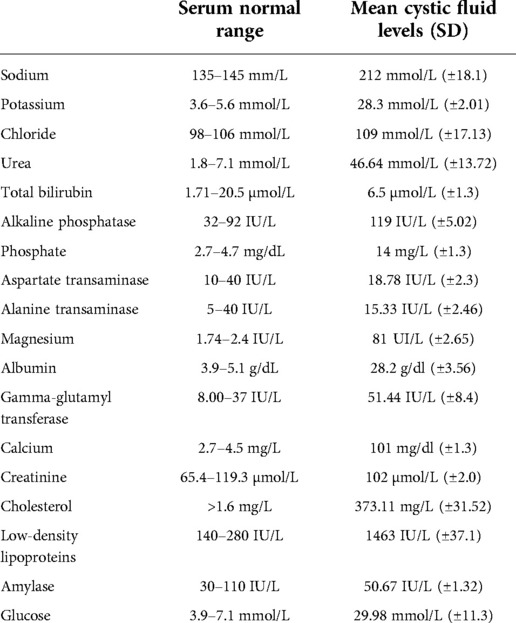
Table 2. Cystic fluid biochemical component means relative to normal serum ranges.
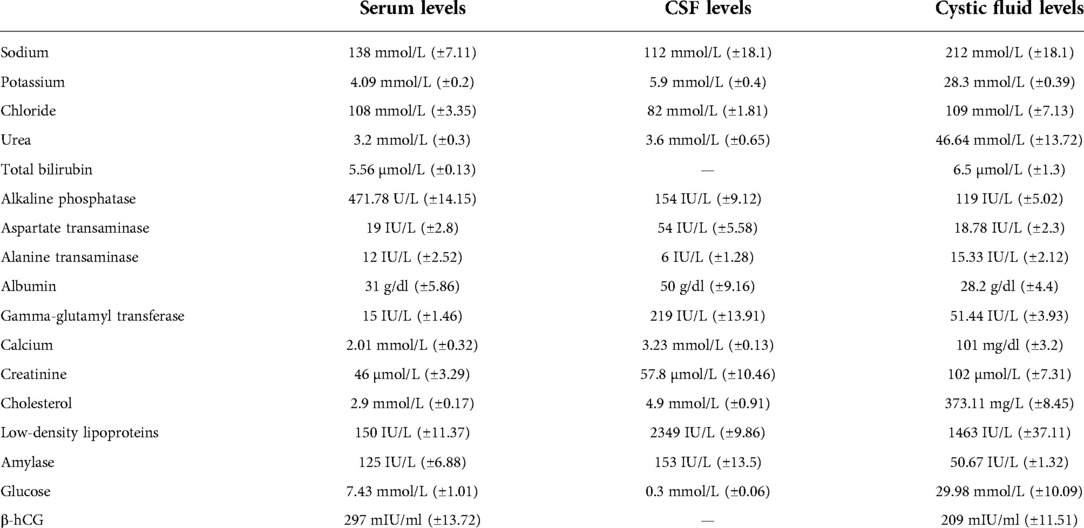
Table 3. Cystic biochemical components in relation to patient CSF and serum.
This paper presents for the first time the incidence of craniopharyngiomas in the paediatric population in a sub-Saharan country, Zimbabwe. It was calculated to be 0.53 per million person-years and in accordance with global estimates. However, the incidence among the 0–14-year age group is twofold higher than in other countries, with five children expected to present with CP every year. This is very worrisome given that Zimbabwe is a low-income country with relatively low health services. It is plausible that this elevation may be that the actual incidence of CP tumours in sub-Saharan Africa is high and also have high mortality (preventing them from getting into adulthood). A follow-up study to determine 5- and 10-year survival of these patients is urgently required to confirm these data.
Our study showed a male preponderance of 2:1. While American and Finland data showed no gender preference, a large hospital-based study in the United Kingdom reported a male preponderance with a ratio of 1.3–1.6 in the paediatric population (1, 11). We noted a slightly higher number of cases from the southern part of the country (Mpilo hospital) albeit this difference was statistically non-significant.
We report that CP cystic fluid had elements found in both CSF and serum, though the quantity was significantly elevated in the cystic fluid. This finding is significant as it is evident that the fluid is actively secreted by tumour components as opposed to past studies which suggested that the fluid was transudate. We report elevated urea and electrolytes compared to the serum values of the same participants. The level of sodium was reported to be twice as high as in the serum of CP patients. Sodium is reported to have antimicrobial properties, particularly in lactic acid-producing bacteria such as Staphylococcus aureus and Salmonella (16–20). Additionally, potassium was elevated fourfold that of serum levels. Moreover, chlorine a halogen that is widely used for inactivating microorganisms was similar in CP cystic fluid compared to that in serum. Also, urea concentration in the CP cystic fluid was found to be elevated 15-fold than that of serum levels. Creatinine was twofold elevated in CP cystic fluid in comparison to its value in the serum of CP patients. Calcium, phosphorus, and magnesium account for 98% of the body’s mineral content by weight. We report that magnesium was 40 times elevated in CP fluid compared to the serum. Phosphate was threefold higher in CP fluid compared to serum. This study aimed to elucidate the biochemical components of adamantinomatous CP cystic fluid with the view of possible antimicrobial components as a follow-up to a previous study that had shown significant antimicrobial activity in the fluid (11–13). All these biochemical components have different antimicrobial properties among other things (21–31).
The CP cystic fluid is also termed machinery oil fluid particularly because of its elevated oil levels. Low-density lipoproteins (LDL) were 100 times elevated in CP cystic fluid compared to serum. In our study, cholesterol was 100 times elevated in the CP compared to serum. This finding can be potentially useful in spectrometry to diagnose CP in the absence of histology (34, 35). In the same vein, β-hCG can potentially be used to aid in diagnosis as well. In addition, glucose was four times elevated in CP cystic fluid, in contrast to amylase which is lower in CP fluid than serum. Biochemical profiling of the cystic fluid composition can potentially assist in the development of targeted intra-cystic therapeutics.
To the best of our knowledge, amylase is being reported for the first time in craniopharyngioma cystic fluid in this study. Studies on the biochemical composition of the cystic fluid are scanty, and there have been reports of lipids, proteins, glucose, urea, creatinine, sodium, calcium, magnesium, phosphorous, chlorine, ALT, AST, and GGT, but none on amylase (7, 8, 14, 34, 35). The significance of this important finding remains to be elucidated.
The study strength is that the catchment area encompassed the entire country and we managed to confirm most of the diagnoses histologically. Some of the limitations of the study are that some patients, particularly those who seek help in traditional medicine or foreign countries, could have been missed. More specimens would increase the strength of the study; however, craniopharyngioma is classified as a rare disease, hence the small participant size (1, 2).
Our study demonstrates for the first time the prevalence of CP in a sub-Saharan country, Zimbabwe, to be 0.53 per million person-years. This study demonstrates higher concentrations of sodium, potassium, urea, bilirubin, creatinine, cholesterol, and low-density lipoproteins in CP fluid compared to serum; this better understanding of the cystic fluid composition has a bearing on the further development of targeted diagnostics and therapeutics in this difficult to manage tumour.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Medical Research Council of Zimbabwe. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
LJ, TLM-J, TM, and TN conceived and designed the study. TLM-J, LJ, NST, IE, and TM performed the clinical examination or biochemical tests and the data analysis. LJ wrote the first draft and all authors read, edited, and approved the final manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bunin GR, Surawicz TS, Witman PA, Preston-Martin S, Davis F, Bruner JM. The descriptive epidemiology of craniopharyngioma. J Neurosurg. (1998) 89(4):547–51. doi: 10.3171/jns.1998.89.4.0547
2. Feng S, Zhang Y, Yu X, Chen X, Zhou T, Bu B, et al. Microsurgical treatment of craniopharyngioma: experiences on 183 consecutive patients. Medicine (Baltimore). (2018) 97(34):e11746. doi: 10.1097/MD.0000000000011746
3. Olsson DS, Andersson E, Bryngelsson IL, Nilsson AG, Johannsson G. Excess mortality and morbidity in patients with craniopharyngioma, especially in patients with childhood-onset: a population-based study in Sweden. J Clin Endocrinol Metab. (2015) 100(2):467–74. doi: 10.1210/jc.2014-3525
4. Borrill R, Cheesman E, Stivaros S, Kamaly-Asl ID, Gnanalingham K, Kilday JP. Papillary craniopharyngioma in a 4-year-old girl with BRAF V600E mutation: a case report and review of the literature. Child’s Nerv Syst. (2019) 35(1):169–73. doi: 10.1007/s00381-018-3925-4
5. Dzinotizei M. Inter-censal demographic survey, ZIMSTAT. ICDS_2017 (2017). Available at: https://www.zimstat.co.zw/wp-content/uploads/publications/Population/population/ICDS_2017.pdf
7. Crotty TB, Scheithauer BW, Young WF Jr., Davis DH, Shaw EG, Miller GM, et al. Papillary craniopharyngioma: a clinicopathological study of 48 cases. J Neurosurg. (1995) 83(2):206–14. doi: 10.3171/jns.1995.83.2.0206
8. Whelan R, Hengartner A, Folzenlogen Z, Prince E, Hankinson TC. Adamantinomatous craniopharyngioma in the molecular age and the potential of targeted therapies: a review. Childs Nerv Syst. (2020) 36(8):1635–42. doi: 10.1007/s00381-020-04677-5
9. Reddy GD, Hansen D, Patel A, Lin Y, Jea A, Lam S. Treatment options for pediatric craniopharyngioma. Surg Neurol Int. (2016) 7:174–8. doi: 10.4103/2152-7806.178570
10. Broogi G. Therapeutic role of intracavitary bleomycin administration in cystic craniopharyngioma. Springer-Verlag Italia. (1995) 11:11–2. doi: 10.1007/978-88-470-2291-1_11
11. Moussa AH, Kerasha AA, Mahmoud ME. Surprising outcome of Ommaya reservoir in treating cystic craniopharyngioma: a retrospective study. Br J Neurosurg. (2013) 27(3):370–3. doi: 10.3109/02688697.2012.741732
12. Kumar PP, Good RR, Skultety FM, Jones EO, Chu WK. Retreatment of recurrent cystic craniopharyngioma with chromic phosphorus p 32. J Natl Med Assoc. (1986) 78(6):542–9. http://www.ncbi.nlm.nih.gov/pmc/articles/pmc2571306/3735454
13. Cohen M, Bartels U, Branson H, Kulkarni AV, Hamilton J. Trends in treatment and outcomes of pediatric craniopharyngioma, 1975–2011. Neuro-Oncology. (2013) 15(6):767–74. doi: 10.1093/neuonc/not026
14. Jokonya L, Reid T, Kasambala M, Mduluza-Jokonya TL, Fieggen G, Mduluza T, et al. Antimicrobial effects of craniopharyngioma cystic fluid. Childs Nerv Syst. (2020) 36(11):2641–6. doi: 10.1007/s00381-020-04825-x
15. Jokonya L, Musara A, Mduluza-Jokonya T, Esene I. Are Ommaya shunt infection rates low in craniopharyngioma patients? PAMJ Clin Med. (2020) 4(61). doi: 10.11604/pamj-cm.2020.4.61.22497
16. Cabezas-Pizarro J, Redondo-Solano M, Umaña-Gamboa C, Arias-Echandi ML. Antimicrobial activity of different sodium and potassium salts of carboxylic acid against some common foodborne pathogens and spoilage-associated bacteria. Rev Argent Microbiol. (2018) 50(1):56–61. doi: 10.1016/j.ram.2016.11.011
17. Bidlas E, Lambert RJW. Comparing the antimicrobial effectiveness of NaCl and KCl with a view to salt/sodium replacement. Int J Food Microbiol. (2008) 124(1):98–102. doi: 10.1016/j.ijfoodmicro.2008.02.031
18. Dawson KA, Boling JA. Effects of potassium ion concentrations on the antimicrobial activities of ionophores against ruminal anaerobes. Appl Environ Microbiol. (1987) 53(10):2363–7. doi: 10.1128/aem.53.10.2363-2367.1987
19. Jin M, Liu L, Wang D, Yang D, Liu W, Yin J, et al. Chlorine disinfection promotes the exchange of antibiotic resistance genes across bacterial genera by natural transformation. ISME J. (2020) 14(7):1847–56. doi: 10.1038/s41396-020-0656-9
20. Huang C, Chen Y, Sun G, Yan K. Disinfectant performance of a chlorine regenerable antibacterial microfiber fabric as a reusable wiper. Materials (Basel). (2019) 12(1). doi: 10.3390/ma12010127
21. Gottardi W, Nagl M. Chlorine covers on living bacteria: the initial step in antimicrobial action of active chlorine compounds. J Antimicrob Chemother. (2005) 55(4):475–82. doi: 10.1093/jac/dki054
22. Kumar R, Vadehra DV. Antibacterial activity of human urine. Indian J Exp Biol. (1979) 17(8):808–10. doi: 10.1172/jci105921
23. Wang N, Xu Q, Liu Y, Jin Y, Harlina PW, Ma M. Highly efficient extraction and purification of low-density lipoprotein from hen egg yolk. Poult Sci. (2018) 97(6):2230–8. doi: 10.3382/ps/pey059
24. Patil M, Noonikara-Poyil A, Joshi SD, Patil SA, Patil SA, Bugarin A. New urea derivatives as potential antimicrobial agents: synthesis, biological evaluation, and molecular docking studies. Antibiotics. (2019) 8(4). doi: 10.3390/antibiotics8040178
25. Narendra babu K, Nagarjuna U, Reddy GD, Padmaja A, Padmavathi V. Synthesis and antimicrobial activity of benzazolyl azolyl urea derivatives. J Mol Struct. (2019) 1198:126871. doi: 10.1016/j.molstruc.2019.126871
26. McDonald T, Drescher KM, Weber A, Tracy S. Creatinine inhibits bacterial replication. J Antibiot. (2012) 65(3):153–6. doi: 10.1038/ja.2011.131
27. Delanaye P, Mariat C, Cavalier E, Maillard N, Krzesinski JM, White CA. Trimethoprim, creatinine and creatinine-based equations. Nephron Clin Pract. (2011) 119(3):187–94. doi: 10.1159/000328911
28. Zagorski BM, Trick WE, Schwartz DN, Wisniewski MF, Hershow RC, Fridkin SK, et al. The effect of renal dysfunction on antimicrobial use measurements. Clin Infect Dis. (2002) 35(12):1491–7. doi: 10.1086/344753
29. Li Y, Liu G, Zhai Z, Liu L, Li H, Yang K, et al. Antibacterial properties of magnesium in vitro and in an in vivo model of implant-associated methicillin-resistant Staphylococcus aureus infection. Antimicrob Agents Chemother. (2014) 58(12):7586–91. doi: 10.1128/AAC.03936-14
30. Lee R. Antibacterial mechanism of phosphates in Staphylococcus aureus. [dissertation/master’s thesis]. Iowa State University (1993). Retrospective Theses and Dissertations.
31. Ji HS, Li H, Mo EJ, Kim UH, Kim YH, Park HY, Jeong TS. Low-density lipoprotein-antioxidant flavonoids and a phenolic ester from Plectranthus hadiensis var. tomentosus. Appl Biol Chem. (2019) 62(1):1–12.
32. Grin PM, Dwivedi DJ, Chathely KM, Trigatti BL, Prat A, Seidah NG, et al. Low-density lipoprotein (LDL)-dependent uptake of Gram-positive lipoteichoic acid and Gram-negative lipopolysaccharide occurs through LDL receptor. Sci Rep. (2018) 8(1):1–11. doi: 10.1038/s41598-018-28777-0
33. Blake GJ, Otvos JD, Rifai N, Ridker PM. Low-density lipoprotein particle concentration and size as determined by nuclear magnetic resonance spectroscopy as predictors of cardiovascular disease in women. Circulation. (2002) 106(15):1930–7. doi: 10.1161/01.CIR.0000033222.75187.B9
34. Arefyeva IA, Semenova JB, Zubairaev MS, Kondrasheva EA, Moshkin AV. Analysis of fluid in craniopharyngioma-related cysts in children: proteins, lactate and pH. Acta Neurochir (Wien). (2002) 144(6):551–4. discussion 554. doi: 10.1007/s007010200077
Keywords: craniopharyngioma, craniopharyngioma cystic fluid, Africa Zimbabwe brain tumours, antimicrobials, sub-Saharan brain tumours
Citation: Jokonya L, Mduluza-Jokonya TL, Esene I, Mwale G, Thango NS, Mduluza T and Naicker T (2022) Biochemical profile of paediatric adamantinomatous craniopharyngiomas: A prospective cohort study. Front. Surg. 9:1026926. doi: 10.3389/fsurg.2022.1026926
Received: 24 August 2022; Accepted: 5 October 2022;
Published: 2 November 2022.
Edited by:
Claire Karekezi, Rwanda Military Hospital, RwandaReviewed by:
Tsegazeab Laeke, Addis Ababa University, Ethiopia© 2022 Jokonya, Mduluza-Jokonya, Esene, Mwale, Thango, Mduluza and Naicker. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luxwell Jokonya ZG9jbHV4QGdtYWlsLmNvbQ==
Specialty Section: This article was submitted to Neurosurgery, a section of the journal Frontiers in Surgery
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.