 Junfeng He
Junfeng He Qing Ling2
Qing Ling2 Yuhong Chen
Yuhong Chen
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 18 November 2021
Sec. Cardiovascular Surgery
Volume 8 - 2021 | https://doi.org/10.3389/fsurg.2021.772675
Background: Postoperative delirium (POD), an alteration in a patient's consciousness pattern, can affect the treatment and prognosis of a disease.
Objective: To construct a prediction model for delirium in patients with type A aortic dissection after surgery and to validate its effectiveness.
Methods: A retrospective cohort design was used to study 438 patients undergoing surgical treatment for type A aortic dissection from April 2019 to June 2020 in tertiary care hospitals. POD (n = 78) and non-delirium groups (n = 360) were compared and analyzed for each index in the perioperative period. A prediction model was established using multifactorial logistic regression, and 30 patients' perioperative data were collected for model validation.
Results: Eight predictors were included in this study: smoking, diabetes, previous cardiovascular surgery, ejection fraction (EF), time to aortic block, acute kidney injury, low cardiac output syndrome, and pulmonary complications. The area under the receiver operating characteristic (ROC) curve of the constructed prediction model was 0.98 ± 0.005, and the Youden index was 0.91. The validation results showed 97% sensitivity, 100% specificity, and 93% accuracy. The expression of the model was Z = Smoking assignment* – 2.807 – 6.009*Diabetes assignment – 2.994*Previous cardiovascular surgery assignment – 0.129*Ejection fraction assignment + 0.071*Brain perfusion time assignment – 2.583*Acute kidney injury assignment – 2.916*Low cardiac output syndrome assignment – 3.461*Pulmonary related complications assignment + 20.576.
Conclusion: The construction of an effective prediction model for the risk of delirium in patients after type A aortic stratification can help identify patients at high risk of POD early. It also provides a reference for healthcare professionals in the prevention and care of these patients.
Aortic dissection (AD) is caused by the tearing of the intimal layer of the aorta or bleeding within the aortic wall, where blood flows between the layers of the aortic wall, separating the layers of the same (entrapment) (1). It is a common condition associated with high mortality (2). Type A aortic dissection involves the ascending aorta and is the most severe type; related studies (3) have shown that the morbidity and mortality rates of patients with type A aortic dissection increase by 1% per hour for 2 days after the onset of the disease. In addition, the morbidity and mortality rate of patients treated non-operatively is up to 74% within 2 weeks, and surgery remains the main treatment for type A aortic dissection (4). However, there are many potential complications after surgery (5), including delirium, which is known to be common after cardiac surgery, with an incidence of 11–46% (6).
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (7) or the International Statistical Classification of Diseases and Related Health Problems, Tenth Edition (ICD 10) (8), delirium is an acute fluctuating change in mental status with reduced consciousness. POD is an acute fluctuating change in the mental state with impaired consciousness and attention. POD is characterized by inattention and fluctuations in consciousness that occur within 30 days after surgery (9, 10) and is associated with high morbidity and mortality, with a prevalence of up to 72% (11). Its incidence depends on risk factors associated with the perioperative period (12). The occurrence of POD prolongs the total length of hospital stay, increases intensive care unit (ICU) morbidity and mortality two to fourfold (13), and significantly increases the level of care dependency in patients who develop POD after discharge (14). This limits their activities for up to 12 months (15) and imposes a huge burden on the individual and society. Here, we investigated the risk factors for POD in patients with aortic dissection and constructed a prediction model to predict such risks.
This was a retrospective cohort study with convenience sampling and a randomized controlled trial. Patients who met the inclusion and exclusion criteria in several hospitals in Jiangsu Province from June 2019 to April 2020 were selected. Inclusion criteria: (1) age ≥ 18 years, (2) type A aortic dissection treated with open-heart surgery, (3) no psychiatric or family history, and (4) no previous history of cognitive impairment or stroke. Exclusion criteria: (1) patients with delirium before admission, (2) patients who were in a coma or deep sedation (RASS score ≤ −3) continuously after surgery, (3) patients who were lost to follow-up, patients with incomplete data, and patients with definite cerebrovascular accidents on postoperative computed tomography (CT), (4) patients who stopped treatment unplanned, patients who died, and patients who stopped participation in the study during treatment, and (5) patients who had a second open-heart surgery because of entrapment. This study was approved by the Ethics Committee.
Delirium was assessed during the ICU treatment phase using the Confusion Assessment Method for the ICU (CAM-ICU), which is recommended by the Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the ICU (16). This method is highly sensitive and specific. Patients were transferred to the ward treatment phase using the 3-min CAM (3D-CAM). The CAM included four aspects: (1) acute alterations and fluctuations in consciousness, (2) inattention, (3) disorganized thinking, and (4) altered clarity of consciousness. Delirium in a patient was determined by the presence of (1) and (2), plus one of (3) or (4) (15).
Sedation levels were assessed using the rating sedation scale (RASS), which allows health professionals to assess the level of bedside sedation or agitation after sedation infusion is stopped (17). Patients were defined as unconscious if they responded to pain/physical stimuli but did not open their eyes (RASS score of −4). A RASS score of −5 indicated that the patient did not respond to physical or verbal stimuli. If the patient had a negative score (> −3 to +4), he or she could be screened for delirium using the CAM-ICU diagnostic tool (18).
The risk factors involved in this study were collected by the investigator on the first day immediately after surgery, and the patients were excluded using the RASS score to identify their coma status. The assessment was stopped if the patient developed POD and continued if the patient did not develop POD until discharge.
R 3.6.3 and SPSS 25.0 were used for the statistical analysis of the data. Count data were expressed as frequencies and percentages, and a χ2 test was used for comparison between groups. Measurement data obeying normal distribution were expressed as x ± s, and a t-test was used for comparison between groups. Non-normally distributed measurement data were described using medians and quartiles; a rank-sum test was used. The least absolute shrinkage and selection operator (LASSO) regression was used to screen and compress the predictors, and logistic stepwise regression was applied to determine the predictors of POD. The alpha level of the entry model was taken to be 0.05 and that of the exit model was 0.1. The odds ratio (OR) values and 95% confidence intervals (CIs) were used to express the independent predictive ability of the predictors. The area under the receiver operating characteristic (ROC) curve was used to judge the discriminatory ability of the model and to evaluate the ability of the risk factors to predict the occurrence of POD. p < 0.05 was considered a statistically significant difference.
From June 2019 to April 2020, 469 patients met the inclusion criterion of the surgical treatment of type A aortic dissection; however, 31 patients were excluded. These comprised 14 deaths, 14 discharges against medical advice, and 3 cases with missing data. A total of 438 cases were statistically analyzed: 315 (71.92%) were men and 123 (28.08%) were women. All were within the age range of 18–86 (57.89 ± 12.41). Delirium occurred in 78 cases, with an incidence rate of 17.8%.
The LASSO regression was used to screen the independent variables to reduce the dimensionality of the data, with 68 starting variables and 17 final variables. Patients in the delirium group were analyzed for risk factors associated with the non-delirium group, and the results showed statistically significant differences (p < 0.05) in smoking, diabetes, previous cardiovascular surgery, ejection fraction (EF), EuroScore II, circulatory arrest time, cardio-pulmonary bypass (CPB) time, cross-clamp time, postoperative/cryoprecipitation, acute kidney injury, low cardiac output syndrome, and pulmonary complications (Table 1).
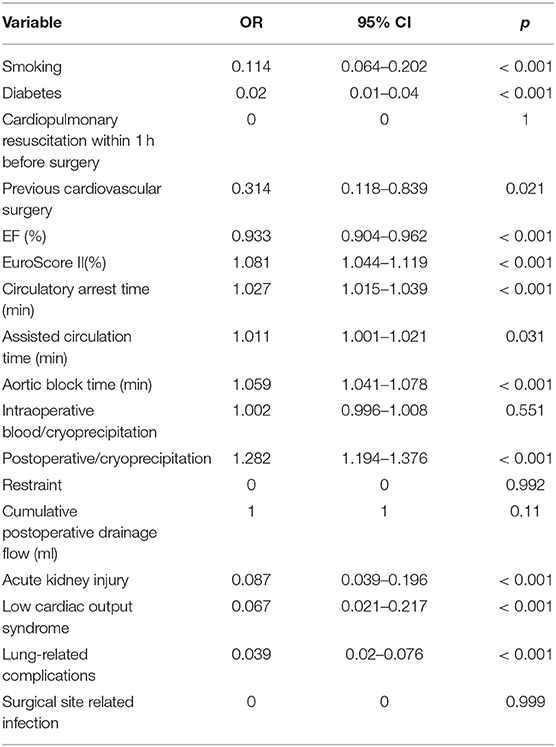
Table 1. Univariate analysis of patients with type A aortic dissection (n = 438).
The statistically significant variables in the univariate analysis were included in the multivariate analysis, and the results showed that smoking, diabetes, previous cardiovascular surgery, EF, aortic block time, acute kidney injury, low cardiac output syndrome, and pulmonary complications independently influenced POD (p < 0.05) (Table 2). The final expression of the formula model was Z = smoking assignment* −2.807 – 6.009*diabetes assignment – 2.994*previous cardiovascular surgery assignment – 0.129*ejection fraction assignment + 0.071*aortic block time assignment – 2.583*acute kidney injury assignment – 2.916*low cardiac output syndrome assignment – 3.461*lung-related complications assignment + 20.576 (Tables 3, 4).
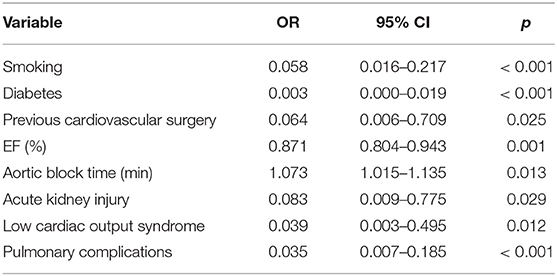
Table 2. Multifactorial analysis of patients with type A aortic dissection (n = 438).
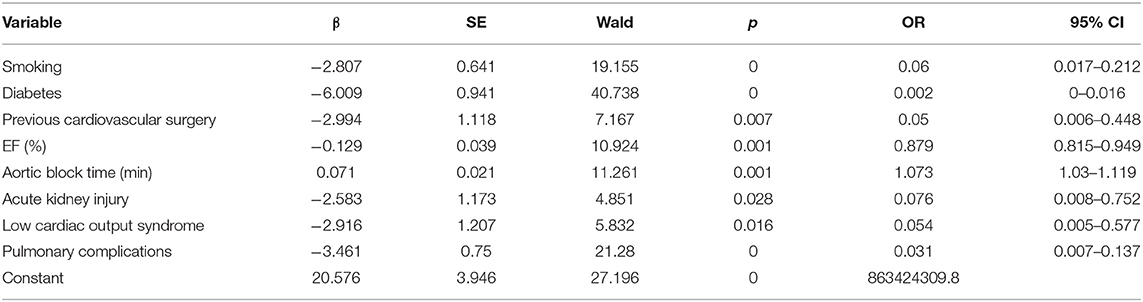
Table 3. Logistic regression modeling (n = 438).
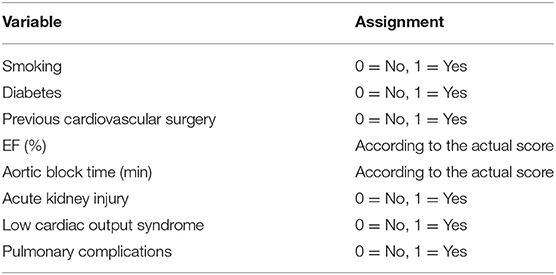
Table 4. Assignment of factors influencing POD.
Logistic regression models containing the aforementioned eight independent variables were developed using logit (P/1–P) as the dependent variable. A patient's score was calculated using the formula of the prediction model, and the ROC curve was used to test the fitting effect between the patient's model score and the occurrence of delirium in the patient (Figure 1). The maximum value of the Youden index was used as the best critical value of the prediction model. The final measured area under the ROC curve was 0.98 ± 0.005, with a 95% CI of 0.973–0.996. The Youden index of the ROC curve was 0.91; the model sensitivity was 0.97, and the specificity was 0.93 (Figure 1).
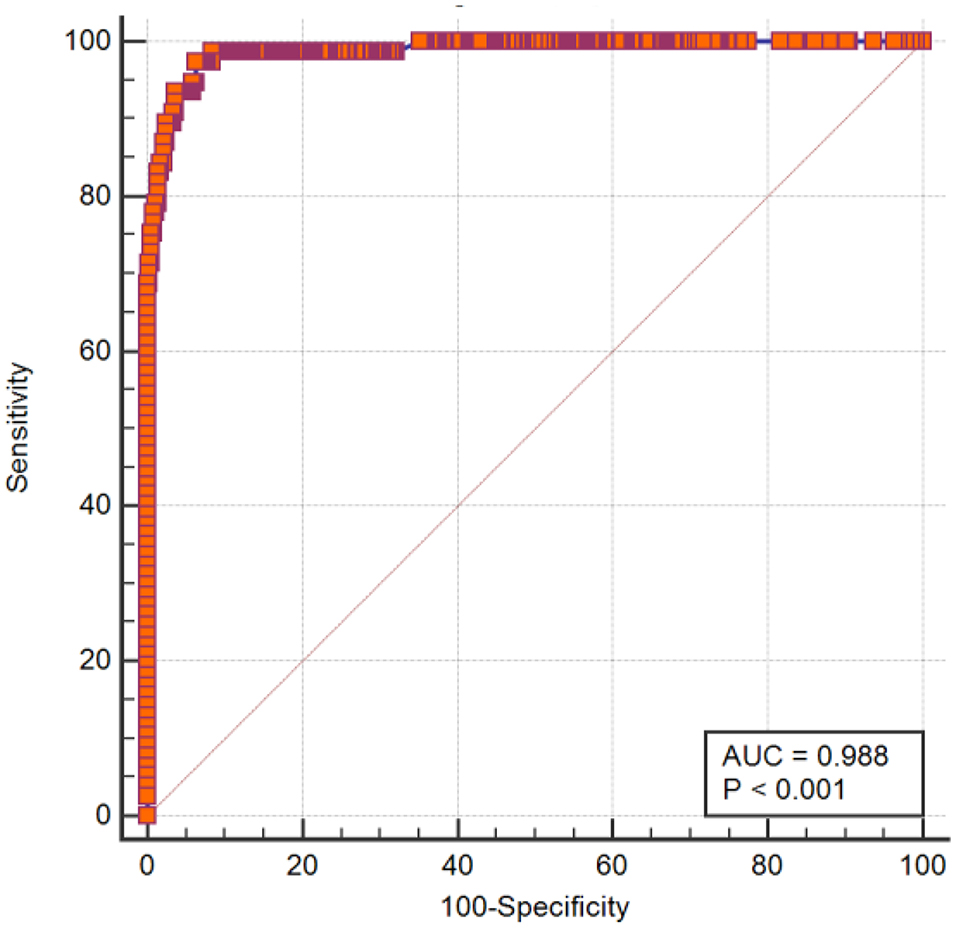
Figure 1. ROC curve of the postoperative delirium prediction model for type A aortic dissection.
The data of 30 patients undergoing surgical treatment for type A aortic dissection in a tertiary care hospital from May 2020 to June 2020 were selected for model validation. There were 17 men and 13 women, within the age range of 33–85 (60.43 ± 12.89). According to the formula of this prediction model, patients were considered to develop delirium when Z ≥ 0.91. The model predicted that delirium would occur in 3 patients and would not occur in 27 patients. The actual results showed that delirium occurred in 5 patients and did not occur in 25 patients. The sensitivity of the model was 97%, the specificity was 100%, and the accuracy was 93% when the predicted results were compared with the actual results.
Owing to the specificity of the pathogenesis of type A aortic dissection, aggressiveness of the disease, and complexity of the treatment modality (19), delirium is a common and serious neurological complication in patients after surgery (20). Related studies have shown that the incidence of POD after type A aortic dissection ranges from 31.1 to 41.6% (21, 22). POD affects patient prognosis (23), and a model that comprises independent influencing factors with good predictive ability can identify and screen high-risk patients. For the inclusion of variables in this study, recent studies on risk factors for POD were comprehensively analyzed (24, 25), and the final variables included were available in the medical and nursing cases of patients with the characteristics of the study population.
Smoking and smoking cessation are potentially modifiable risk factors for POD. Certain studies (26, 27) have shown that smokers exhibit severe agitation, sleep disturbances, mood swings, and manifestations associated with delirium. In addition, it was observed that the onset of delirium is associated with a disruption in specific neurotransmitter activity. Patients experience withdrawal symptoms after admission as treatment is initiated and smoking is discontinued. It was proposed that changes in dopamine can explain the different symptoms of delirium and that different levels of dopamine in the body cause different subtypes of delirium (28, 29). During nicotine withdrawal, there is a decrease in voxel dopamine activity. However, an increase in the dopamine release from the prefrontal cortex, which may play an important role in the regulation of anxiety in patients, can elucidate the high prevalence of delirium in patients with nicotine withdrawal, considering the role of the prefrontal cortex in delirium manifestation (30). Recent studies suggest that nicotine withdrawal and delirium share common pathophysiological mechanisms that are mediated by changes in various neurotransmitter systems, including dopamine, opioids, and cholinergic systems. It was also suggested that early identification and management of withdrawal symptoms in patients can improve sleep-wake disturbances and emotional instability, thereby preventing delirium (31–34). Therefore, caregivers should have detailed knowledge of the patient's smoking history, cessation, and possible symptoms and reactions to nicotine withdrawal for timely assessment and prevention.
Studies have shown a correlation between diabetes and a 1.84-fold increase in the incidence of POD (35–37). Patients with diabetes typically exhibit greater cerebral and hippocampal atrophy (38), cerebral microvascular damage (39), and macrovascular damage (40), compared to those without diabetes. In addition, impaired glucose metabolism exerts important effects on the brain and is a predisposing factor to cognitive impairment (41). Recent studies on epidemiology do not reveal a definite causal relationship; however, evidence suggests (42) the neurotoxic effects of sustained hyperglycemia, which ultimately damages neurons and leads to loss of function. Therefore, nursing staff should understand the patient's history, pay close attention to the patient's blood glucose fluctuations, and cooperate with the physician to promptly improve the patient's blood glucose abnormalities.
Patients with a previous history of cardiovascular surgery are susceptible to POD because of a combination of cardiovascular surgery modalities and previous perioperative risk factors.
Reduced EF causes a reduction in the blood supply to body tissues and organs, which in turn triggers edema and pulmonary stasis due to nutritional deficiencies (43), leading to heart failure. Iwata et al. (44) showed that the degree of delirium correlates with the severity of heart failure, and the development of delirium during hospitalization was associated with short-term and long-term mortality in patients, although this can be predicted by the degree of heart failure.
Cerebral perfusion is dependent on cardiac output, arterial pulsation intensity, cerebral artery patency, cerebral autoregulation, cerebellar vascular patency, and venous patency. If these parameters change, cognition can be affected. Thus, cardiac pathology affecting cerebral hemodynamics may affect cellular function before irreversible structural alterations (45). Decreased cardiac function, which affects the connection between the heart and brain, may lead to acute cognitive impairment, and consequently, POD.
Therefore, nursing staff should closely monitor important reference indicators of cardiac function. In addition, the vital signs of patients with low preoperative EF and poor cardiac function should be closely monitored to obtain relevant examination results. These patients should follow correct medical advice and undergo psychological care and active monitoring to prevent POD.
Extended operative and aortic block times were shown to be predisposing factors for POD (46–48). The aortic block time is an independent risk factor for POD after cardiac surgery. The correlation between the aortic block time and POD has been demonstrated in related studies (49). Andrejaitiene and Sirvinskas (50) reported that the incidence of POD increased eightfold for each minute of an extended aortic block time. This is because long aortic block times induce a risk of inadequate cerebral perfusion in patients, which aggravates brain cell ischemia and hypoxia, causing impaired nerve cell function and affecting the patient's postoperative cognitive function, leading to POD. Nursing staff should understand patients' intraoperative-related passages, identify relevant risk factors, and raise awareness early.
Acute kidney injury (AKI) is commonly observed in patients undergoing cardiac surgery and in the perioperative period of critically ill patients. It can increase morbidity and mortality by affecting distal organ function (51). Improving Global Outcomes (KDIGO) criteria for AKI staging (52), definition of AKI: an increase in serum creatinine by ≥0.3 mg/dl (≥26.5 μmol/l) within 48 h, an increase in serum creatinine to ≥1.5–1.9 times baseline levels, which is known or presumed to have occurred within the prior 7 days and urine volume <0.5 ml/kg/h for 6 h. Numerous studies have shown that acute kidney injury significantly affects the function of extrarenal organs, including the brain (53). Siew et al. (54) reported that acute kidney injury was an independent risk factor for the development of delirium or the diagnosis of coma during critical illnesses. Grigoriieyev et al. (53) confirmed the effects of acute kidney injury on distal organs, verifying that such injuries may lead to a strong inflammatory response with different effects in the brain and lungs. During acute kidney injuries, both organs may interact through multiple mechanisms, such as the amplification of cytokine-induced damage, leukocyte extravasation, sodium and potassium dysregulation, oxidative stress, and use of water channels (55). The occurrence of acute kidney injury in postoperative cardiac patients, regardless of their stage, is associated with an increased incidence of POD (56). Nursing staff should closely monitor the patient's intake and output, pay attention to the patient's laboratory test results, and correctly cooperate with continuous renal replacement therapy (CRRT) and other related treatments.
Certain patients suffer from perioperative low cardiac output syndrome; however, the brain depends on a continuous and adequate blood supply, and disruption of cerebral blood flow can lead to cerebral dysfunction and death (57). Cardiogenic dementia (58) was proposed early in the 1970s, and the concept of cardiocerebral codependency was formed. Ample evidence suggests that adequate cerebral perfusion is a prerequisite for maintaining normal cognitive function (59). It is common for patients to experience a decline in cardiac function, cognitive impairment, and consequently, delirium (60). Nursing staff should closely monitor patients for signs, such as heart rate, blood pressure, and peripheral circulation, with timely feedback and dynamic follow-ups.
The definition of postoperative pulmonary complication (PPC) varies widely, leading to large variation in reported frequency, and is usually dependent upon a set of criteria which may include signs such as chest X-ray findings, pyrexia and positive sputum microbiology. The Melbourne Group Scale (MGS) (61) was used in this study to assess the occurrence of PPC in patients: Temperature>38°C, White cell count >11.2 or respiratory, antibiotics, Physician diagnosis of pneumonia or chest infection, Chest X-ray report of atelectasis/consolidation, Production of purulent (yellow/green), sputum differing from preoperative Positive signs on sputum microbiology, SpO2 < 90% on room air and Re-admission to or prolonged stay (over 36 h) on the intensive care unit/high dependency unit for respiratory problems PPC = four or more positive variables. Studies have shown multiple correlations between pulmonary complications and POD, which are mutually causal (62). Patients with pulmonary complications after aortic dissection surgery are prone to hypoxemia, which causes cerebral hypoperfusion and leads to neuroinflammation, as a cause of POD (63). Certain studies have shown that the risk factors and consequences associated with hypoxemia are closely related to delirium; therefore, delirium and hypoxemia are related (63). Considering the severity of pulmonary complications and complex treatment protocols, patients who develop pulmonary complications usually have long hospital stays and are prone to ICU delirium (64). In a study of acute respiratory distress syndrome (ARDS) survivors, the degree of cognitive impairment in these survivors correlated with the severity of hypoxemia. They were observed to have deficits in memory, attention, concentration, and recollection (65). Patients who develop pulmonary complications are at greater risk of POD, resulting from a combination of hypoxemia and inflammation, drug exposure, and prolonged ICU and hospital stay (66).
Delirium is a common complication in postoperative patients with type A aortic dissection, and its occurrence is influenced by multiple factors, with nurses playing a crucial role in the prevention phase. Here, a risk prediction model with eight factors was developed to help nurses identify patients at high risk of POD early and execute targeted interventions to reduce the incidence of POD and improve patient prognoses.
Combined with the characteristics of the treatment of type A aortic dissection, patients mostly undergo emergency surgery; therefore, this model performs risk assessment after the surgery. This assessment can be completed based on the patient's surgery records, relevant examination results, and course of the disease records. When the patient's score was greater than or equal to 0.91, it was considered that the patient would probably develop POD and should receive attention from nursing staff in the form of interventions in cooperation with doctors. When the patient's risk assessment was close to the critical value, it was considered that the patient had a certain risk for POD and close attention should be paid to such a patient to prevent POD. When the patient's condition changed during treatment, it was evaluated using a dynamic assessment to minimize the risk of POD.
Compared with previous studies, this study did not stop at the first treatment stage for patients but attempted to include data for the whole perioperative period of patients before, during, and after surgery (including ICU and ward) to avoid missing relevant factors. An evidence-based analysis of relevant risk factors was used; it elucidated gaps in certain studies related to the model for POD in type A aortic dissection. The model involved patient-related assessment data that were simple and easy to obtain, providing a reference for the prevention and treatment of clinical delirium. A limitation of this study is that although the data sources were obtained from multiple hospitals, the sample sizes used in the analysis and that of the model validation were small, and the relevant conclusions require further validation.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Committee of Nanjing First Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
JFH conceived, designed, and implemented the study, collected and analyzed the data, and wrote the article. QL critically reviewed the content of articles and assisted with data collection. YHC was the grantee of the grant program, provided research funding, also gave administrative support and critically reviewed the content of articles. All authors contributed to the article and approved the submitted version.
This study was funded by Government of Jiangsu Province, award number: ZKX1803 (grant recipient: YC).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Mussa FF, Horton JD, Moridzadeh R, Nicholson J, Trimarchi S, Eagle KA. Acute aortic dissection and intramural hematoma: a systematic review. JAMA. (2016) 316:754–63. doi: 10.1001/jama.2016.10026
2. Anagnostopoulos CE, Prabhakar MJ, Kittle CF. Aortic dissections and dissecting aneurysms. Am J Cardiol. (1972) 30:263–73. doi: 10.1016/0002-9149(72)90070-7
3. Sun L, Li J. Progress and challenge of Stanford type A aortic dissection in China. Chin J Surg. (2017) 55:241–4. doi: 10.3760/cma.j.issn.0529-5815.2017.04.001
4. Nienaber CA, Clough RE. Management of acute aortic dissection. Lancet. (2015) 385:800–11. doi: 10.1016/S0140-6736(14)61005-9
5. Rubino AS, Onorati F, Caroleo S, Galato E, Nucera S, Amantea B, et al. Impact of clonidine administration on delirium and related respiratory weaning after surgical correction of acute type-A aortic dissection: results of a pilot study. Interact Cardiovasc Thorac Surg. (2010) 10:58–62. doi: 10.1510/icvts.2009.217562
6. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. (2014) 383:911–22. doi: 10.1016/S0140-6736(13)60688-1
7. Wilson JE, Mart MF, Cunningham C, Shehabi Y, Girard TD, MacLullich AMJ, et al. Delirium. Erratum in: Nat Rev Dis Primers. (2020) 6(1):94. Nat Rev Dis Primers. (2020) 6:90. doi: 10.1038/s41572-020-00223-4
8. World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision. (2015). Available online at: http://apps.who.int/classifications/icd10/browse/2016/en (accessed December 9, 2015).
9. Pallaria TJ, Panebianco C, Kamienski MC. Perioperative delirium protocol for the older patient. J Perianesth Nurs. (2018) 33:275–80. doi: 10.1016/j.jopan.2016.08.015
10. Hollinger A, Siegemund M, Goettel N, Steiner LA. Postoperative delirium in cardiac surgery: an unavoidable menace? J Cardiothorac Vasc Anesth. (2015) 29:1677–87. doi: 10.1053/j.jvca.2014.08.021
11. Stachon P, Kaier K, Zirlik A, Reinöhl J, Heidt T, Bothe W, et al. Risk factors and outcome of postoperative delirium after transcatheter aortic valve replacement. Clin Res Cardiol. (2018) 107:756–62. doi: 10.1007/s00392-018-1241-3
12. Smulter N, Lingehall HC, Gustafson Y, Olofsson B, Engström KG. Delirium after cardiac surgery: incidence and risk factors. Interact Cardiovasc Thorac Surg. (2013) 17:790–6. doi: 10.1093/icvts/ivt323
13. Francis J, Martin D, Kapoor WN. A prospective study of delirium in hospitalized elderly. JAMA. (1990) 263:1097–101. doi: 10.1001/jama.1990.03440080075027
14. Chuan A, Zhao L, Tillekeratne N, Alani S, Middleton PM, Harris IA, et al. The effect of a multidisciplinary care bundle on the incidence of delirium after hip fracture surgery: a quality improvement study. Anaesthesia. (2020) 75:63–71. doi: 10.1111/anae.14840
15. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. (1990) 113:941–8. doi: 10.7326/0003-4819-113-12-941
16. Devlin JW, Skrobik Y, Gélinas C, Needham DM, Slooter AJC, Pandharipande PP, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. (2018) 46:e825–73. doi: 10.1097/CCM.0000000000003299
17. Hughes CG, Boncyk CS, Culley DJ, Fleisher LA, Leung JM, McDonagh DL, et al. Perioperative quality initiative (POQI) 6 workgroup. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Postoperative Delirium Prevention. Anesth Analg. (2020) 130:1572–90. doi: 10.1213/ANE.0000000000004641
18. Martin BJ, Buth KJ, Arora RC, Baskett RJ. Delirium: a cause for concern beyond the immediate postoperative period. Ann Thorac Surg. (2012) 93:1114–20. doi: 10.1016/j.athoracsur.2011.09.011
19. Maldonado JR. Acute brain failure: pathophysiology, diagnosis, management, and sequelae of delirium. Crit Care Clin. (2017) 33:461–519. doi: 10.1016/j.ccc.2017.03.013
20. Visser L, Prent A, van der Laan MJ, van Leeuwen BL, Izaks GJ, Zeebregts CJ, et al. Predicting postoperative delirium after vascular surgical procedures. J Vasc Surg. (2015) 62:183–9. doi: 10.1016/j.jvs.2015.01.041
21. Song X, Meng L, Yuan X, Fu W, Cao Y, Li J, et al. Establishment of perioperative risk assessment system for type A aortic dissection. Chin J Thoracic Cardiovasc Surg. (2018) 34:350–5.
22. Zhou C, Yang J, Wen J, Jiang N, Zhang Z, Liu X, et al. Chen X. Analysis of risk factors for postoperative delirium in patients with acute type A aortic dissection. Chin. J. Arterioscl. (2016) 24:1253–7.
23. Gómez Tovar LO, Henao Castaño AM. Analysis of delirium from the dynamic symptoms model: a literature review. Crit Care Nurs Q. (2020) 43:312–36. doi: 10.1097/CNQ.0000000000000316
24. Raats JW, Steunenberg SL, de Lange DC, van der Laan L. Risk factors of post-operative delirium after elective vascular surgery in the elderly: a systematic review. Int J Surg. (2016) 35:1–6. doi: 10.1016/j.ijsu.2016.09.001
25. Zhao J, Wu Y. Research progress in nursing care for postoperative delirium in patients with aortic dissection. Chin J Mod Nurs. (2018) 24:2993–7.
26. Ross CA, Peyser CE, Shapiro I, Folstein MF. Delirium: phenomenologic and etiologic subtypes. Int Psychogeriatr. (1991) 3:135–47. doi: 10.1017/s1041610291000613
27. Trzepacz PT. Anticholinergic model for delirium. Semin Clin Neuropsychiatry. (1996) 1:294–303. doi: 10.1053/SCNP00100294
28. Hshieh TT, Fong TG, Marcantonio ER, Inouye SK. Cholinergic deficiency hypothesis in delirium: a synthesis of current evidence. J Gerontol A Biol Sci Med Sci. (2008) 63:764–72. doi: 10.1093/gerona/63.7.764
29. Smith HA, Brink E, Fuchs DC, Ely EW, Pandharipande PP. Pediatric delirium: monitoring and management in the pediatric intensive care unit. Pediatr Clin North Am. (2013) 60:741–60. doi: 10.1016/j.pcl.2013.02.010
30. Stagno D, Gibson C, Breitbart W. The delirium subtypes: a review of prevalence, phenomenology, pathophysiology, and treatment response. Palliat Support Care. (2004) 2:171–9. doi: 10.1017/s1478951504040234
31. Joseph AM, Norman SM, Ferry LH, Prochazka AV, Westman EC, Steele BG, et al. The safety of transdermal nicotine as an aid to smoking cessation in patients with cardiac disease. Erratum in: N Engl J Med. (2007) 14;356(24):2554. Antonnucio, DO [corrected to Antonuccio, DO]. N Engl J Med. (1996) 335:1792–8. doi: 10.1056/NEJM199612123352402
32. Hartmann-Boyce J, Chepkin SC, Ye W, Bullen C, Lancaster T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst Rev. (2018) 5:CD000146. doi: 10.1002/14651858.CD000146.pub5
33. Gourlay SG, Stead LF, Benowitz NL. Clonidine for smoking cessation. Cochrane Database Syst Rev. (2004) 2004:CD000058. doi: 10.1002/14651858.CD000058.pub2
34. Reade MC, O'Sullivan K, Bates S, Goldsmith D, Ainslie WR, Bellomo R. Dexmedetomidine vs. haloperidol in delirious, agitated, intubated patients: a randomised open-label trial. Crit Care. (2009) 13:R75. doi: 10.1186/cc7890
35. Feinkohl I, Winterer G, Pischon T. Obesity and post-operative cognitive dysfunction: a systematic review and meta-analysis. Diabetes Metab Res Rev. (2016) 32:643–51. doi: 10.1002/dmrr.2786
36. Feinkohl I, Winterer G, Pischon T. Diabetes is associated with risk of postoperative cognitive dysfunction: a meta-analysis. Diabetes Metab Res Rev. (2017) 33:2884. doi: 10.1002/dmrr.2884
37. Feinkohl I, Winterer G, Pischon T. Hypertension and risk of post-operative cognitive dysfunction (POCD): a systematic review and meta-analysis. Clin Pract Epidemiol Ment Health. (2017) 13:27–42. doi: 10.2174/1745017901713010027
38. Hayashi K, Kurioka S, Yamaguchi T, Morita M, Kanazawa I, Takase H, et al. Association of cognitive dysfunction with hippocampal atrophy in elderly Japanese people with type 2 diabetes. Diabetes Res Clin Pract. (2011) 94:180–5. doi: 10.1016/j.diabres.2011.07.002
39. Fülesdi B, Limburg M, Bereczki D, Káplár M, Molnár C, Kappelmayer J, et al. Cerebrovascular reactivity and reserve capacity in type II diabetes mellitus. J Diabetes Complications. (1999) 13:191–9. doi: 10.1016/s1056-8727(99)00044-6
40. Sanjari Moghaddam H, Ghazi Sherbaf F, Aarabi MH. Brain microstructural abnormalities in type 2 diabetes mellitus: a systematic review of diffusion tensor imaging studies. Front Neuroendocrinol. (2019) 55:100782. doi: 10.1016/j.yfrne.2019.100782
41. Chatterjee S, Peters SA, Woodward M, Mejia Arango S, Batty GD, Beckett N, et al. Type 2 diabetes as a risk factor for dementia in women compared with men: a pooled analysis of 2.3 million people comprising more than 100,000 cases of dementia diabetes care. (2016) 39:300–7. doi: 10.2337/dc15-1588
42. Tomlinson DR, Gardiner NJ. Glucose neurotoxicity. Nat Rev Neurosci. (2008) 9:36–45. doi: 10.1038/nrn2294
43. Zhao L, Dai S, Yang J, Zhong H. Value of electrocardiogram combined with echocardiography in diagnosis of different degrees of coronary heart disease patient with heart failure. Clin Misdiagn Mistherapy. (2017) 30: 55–9.
44. IIwata E, Kondo T, Kato T, Okumura T, Nishiyama I, Kazama S, et al. Prognostic value of delirium in patients with acute heart failure in the intensive care unit. Can J Cardiol. (2020) 36:1649–57. doi: 10.1016/j.cjca.2020.01.006
45. van Buchem MA, Biessels GJ, Brunner la Rocca HP, de Craen AJ, van der Flier WM, Ikram MA, et al. The heart-brain connection: a multidisciplinary approach targeting a missing link in the pathophysiology of vascular cognitive impairment. J Alzheimers Dis. (2014) 42 Suppl 4:S443–51. doi: 10.3233/JAD-141542
46. Zhang WY, Wu WL, Gu JJ, Sun Y, Ye XF, Qiu WJ, et al. Risk factors for postoperative delirium in patients after coronary artery bypass grafting: a prospective cohort study. J Crit Care. (2015) 30:606–12. doi: 10.1016/j.jcrc.2015.02.003
47. Kazmierski J, Kowman M, Banach M, Fendler W, Okonski P, Banys A, et al. IPDACS Study. Incidence and predictors of delirium after cardiac surgery: results from The IPDACS Study. J Psychosom Res. (2010) 69:179–85. doi: 10.1016/j.jpsychores.2010.02.009
48. Afonso A, Scurlock C, Reich D, Raikhelkar J, Hossain S, Bodian C, et al. Predictive model for postoperative delirium in cardiac surgical patients. Semin Cardiothorac Vasc Anesth. (2010) 14:212–7. doi: 10.1177/1089253210374650
49. Tully PJ, Baker RA, Winefield HR, Turnbull DA. Depression, anxiety disorders and Type D personality as risk factors for delirium after cardiac surgery. Aust N Z J Psychiatry. (2010) 44:1005–11. doi: 10.3109/00048674.2010.495053
50. Andrejaitiene J, Sirvinskas E. Early post-cardiac surgery delirium risk factors. Perfusion. (2012) 27:105–12. doi: 10.1177/0267659111425621
51. Wan R, McKenzie CA, Taylor D, Camporota L, Ostermann M. Acute kidney injury as a risk factor of hyperactive delirium: a case control study. J Crit Care. (2020) 55:194–7. doi: 10.1016/j.jcrc.2019.10.013
52. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. (2012) 120:c179–84. doi: 10.1159/000339789
53. Grigoryev DN, Liu M, Hassoun HT, Cheadle C, Barnes KC, Rabb H. The local and systemic inflammatory transcriptome after acute kidney injury. J Am Soc Nephrol. (2008) 19:547–58. doi: 10.1681/ASN.2007040469
54. Siew ED, Fissell WH, Tripp CM, Blume JD, Wilson MD, Clark AJ, et al. Acute kidney injury as a risk factor for delirium and coma during critical illness. Am J Respir Crit Care Med. (2017) 195:1597–607. doi: 10.1164/rccm.201603-0476OC
55. Liu M, Liang Y, Chigurupati S, Lathia JD, Pletnikov M, Sun Z, et al. Acute kidney injury leads to inflammation and functional changes in the brain. J Am Soc Nephrol. (2008) 19:1360–70. doi: 10.1681/ASN.2007080901
56. Kotfis K, Slozowska J, Listewnik M, Szylińska A, Rotter I. The impact of acute kidney injury in the perioperative period on the incidence of postoperative delirium in patients undergoing coronary artery bypass grafting-observational cohort study. Int J Environ Res Public Health. (2020) 17:1440. doi: 10.3390/ijerph17041440
57. Moskowitz MA, Lo EH, Iadecola C. The science of stroke: mechanisms in search of treatments. Erratum in: Neuron. 2010 Oct 6;68(1):161. Neuron. (2010) 67:181–98. doi: 10.1016/j.neuron.2010.07.002
58. Cannon JA, McMurray JJ, Quinn TJ. 'Hearts and minds': association, causation and implication of cognitive impairment in heart failure. Alzheimers Res Ther. (2015) 7:22. doi: 10.1186/s13195-015-0106-5
59. Gorelick PB, Scuteri A, Black SE, Decarli C, Greenberg SM, Iadecola C, et al. American Heart Association Stroke Council, Council on Epidemiology and Prevention, Council on Cardiovascular Nursing, Council on Cardiovascular Radiology and Intervention, and Council on Cardiovascular Surgery and Anesthesia. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the american heart association/American stroke association. Stroke. (2011) 42:2672–713. doi: 10.1161/STR.0b013e3182299496
60. Cai S, Latour JM, Lin Y, Pan W, Zheng J, Xue Y, et al. Preoperative cardiac function parameters as valuable predictors for nurses to recognise delirium after cardiac surgery: a prospective cohort study. Eur J Cardiovasc Nurs. (2020) 19:310–9. doi: 10.1177/1474515119886155
61. Agostini P, Naidu B, Cieslik H, Rathinam S, Bishay E, Kalkat MS, et al. Comparison of recognition tools for postoperative pulmonary complications following thoracotomy. Physiotherapy. (2011) 97:278–83. doi: 10.1016/j.physio.2010.11.007
62. Sugimura Y, Sipahi NF, Mehdiani A, Petrov G, Awe M, Minol JP, et al. Risk and consequences of postoperative delirium in cardiac surgery. Thorac Cardiovasc Surg. (2020) 68:417–24. doi: 10.1055/s-0040-1708046
63. Hsieh SJ, Soto GJ, Hope AA, Ponea A, Gong MN. The association between acute respiratory distress syndrome, delirium, and in-hospital mortality in intensive care unit patients. Am J Respir Crit Care Med. (2015) 191:71–8. doi: 10.1164/rccm.201409-1690OC
64. Wilcox ME, Brummel NE, Archer K, Ely EW, Jackson JC, Hopkins RO. Cognitive dysfunction in ICU patients: risk factors, predictors, and rehabilitation interventions. Crit Care Med. (2013) 41(9 Suppl 1):S81–98. doi: 10.1097/CCM.0b013e3182a16946
65. Hopkins RO, Weaver LK, Pope D, Orme JF, Bigler ED, Larson-LOHR V. Neuropsychological sequelae and impaired health status in survivors of severe acute respiratory distress syndrome. Am J Respir Crit Care Med. (1999) 160:50–6. doi: 10.1164/ajrccm.160.1.9708059
Keywords: type A aortic dissection, postoperative delirium, predictive model, nursing, factor
Citation: He JF, Ling Q and Chen YH (2021) Construction and Application of a Model for Predicting the Risk of Delirium in Postoperative Patients With Type a Aortic Dissection. Front. Surg. 8:772675. doi: 10.3389/fsurg.2021.772675
Received: 08 September 2021; Accepted: 11 October 2021;
Published: 18 November 2021.
Edited by:
Mohamad Bashir, SRM University, IndiaReviewed by:
Bleri Celmeta, Istituto Clinico Sant'Ambrogio, ItalyCopyright © 2021 He, Ling and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuhong Chen, MTg5NTE2NzA5NTVAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.