
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg., 28 January 2019
Sec. Visceral Surgery
Volume 6 - 2019 | https://doi.org/10.3389/fsurg.2019.00001
 Wolfgang Reinpold1†
Wolfgang Reinpold1† Ferdinand Köckerling2*†Reinhard Bittner3Joachim Conze4
Ferdinand Köckerling2*†Reinhard Bittner3Joachim Conze4 René Fortelny5
René Fortelny5 Andreas Koch6Jan Kukleta7Andreas Kuthe8
Andreas Koch6Jan Kukleta7Andreas Kuthe8 Ralph Lorenz9
Ralph Lorenz9 Bernd Stechemesser10
Bernd Stechemesser10Introduction: Recently, the promising results of new procedures for the treatment of rectus diastasis with concomitant hernias using extraperitoneal mesh placement and anatomical restoration of the linea alba were published. To date, there is no recognized classification of rectus diastasis (RD) with concomitant hernias. This is urgently needed for comparative assessment of new surgical techniques. A working group of the German Hernia Society (DHG) and the International Endohernia Society (IEHS) set itself the task of devising such a classification.
Materials and Methods: A systematic search of the available literature was performed up to October 2018 using Medline, PubMed, Scopus, Embase, Springer Link, and the Cochrane Library. A meeting of the working group was held in May 2018 in Hamburg. For the present analysis 30 publications were identified as relevant.
Results: In addition to the usual patient- and technique-related influencing factors on the outcome of hernia surgery, a typical means of rectus diastasis classification and diagnosis should be devised. Here the length of the rectus diastasis should be classified in terms of the respective subxiphoidal, epigastric, umbilical, infraumbilical, and suprapubic sectors affected as well as by the width in centimeters, whereby W1 < 3 cm, W2 = 3− ≤ 5 cm, and W3 > 5 cm. Furthermore, gender, the concomitant hernias, previous abdominal surgery, number of pregnancies and multiple births, spontaneous birth or caesarian section, skin condition, diagnostic procedures and preoperative pain rate and localization of pain should be recorded.
Conclusion: Such a unique classification is needed for assessment of the treatment results in patients with RD.
The rectus muscles are normally fused at the midline with no more than 1 to 2 cm separating them (1). Rectus diastasis (RD) (diastasis recti, divarication of the rectus muscles) is an acquired condition in which the rectus muscles are separated by an abnormal distance along their length, but with no fascial defect (1). A separation of >2 cm is considered to be a rectus diastasis (1). It is most commonly found in middle-aged and older men with central obesity, or in women who have carried a large fetus or twins to term (1). RD is characterized by a protruding midline following an increase in intra-abdominal pressure (2). The condition is characterized by a gradual thinning and widening of the linea alba, combined with a general laxity of the ventral abdominal wall muscles (2). The musculofascial continuity of the midline and subsequent absence of a true hernia sac is what sets RD apart from a ventral hernia (2). But thinning and stretching of the linea alba is an important risk factor for actual development of midline hernias (umbilical, epigastric, trocar, incisional hernia) due to the deterioration of the connective tissue and the pulling of the abdominal muscles (3). In a series of even small umbilical and epigastric hernias (<2 cm) concomitant rectus diastasis was diagnosed in 45% of patients (3). If RD is associated with midline hernias, the surgical procedure most recommended could be corrective surgery of both pathologies at the same time (4).
In systematic reviews the published literature on surgical treatment of RD is assessed to be of low scientific and methodological quality (2, 5). There is currently no consensus as to the definition and classification of RD (4). Based on the current literature, no clear distinction can be made in the recurrence rate, postoperative complications, or patient reported outcomes (2). This applies, in particular, to the numerous innovative minimally invasive techniques recently reported in the literature for treatment of RD with concomitant ventral hernias (4, 6–19). The promising results of new procedures with extraperitoneal mesh placement and anatomical restoration of the linea alba, such as the endoscopic-assisted or endoscopic mini open sublay repair (MILOS, EMILOS), endoscopic-assisted linea alba reconstruction (ELAR), laparoscopic linea alba stapler repair, enhanced total extraperitoneal ventral hernia repair (eTEP), laparoscopic intracorporeal rectus aponeuroplasty (LIRA), preaponeurotic endoscopic repair (REPA) and totally endoscopic sublay (TES), have to be confirmed in future trials (4, 6–19). For enhanced comparability of the treatment results of hernia surgery a recognized classification system is indispensable (20). Moreover, all patient characteristics influencing the treatment results should be analyzed (21).
Therefore, on the basis of the existing literature, a working group of the German Hernia Society (DHG) and the International Endohernia Society (IEHS) set about defining the patient- and technique-related factors in order to propose a classification of RD.
The members of the working group were requested, on the basis of a literature search, to identify potential classification features for rectus diastasis. The results of that literature search were presented by the members to the group at a meeting in May 2018 in Hamburg. Then a consensus was reached by the group (Figure 1). The consensus-building results are now presented below. Consensus building was based on 30 relevant literature sources identified in searches of PubMed, Medline, Google scholar, and the Cochrane Library. The following search terms were used: “Rectus diastasis,” “Diastasis recti,” “Rectus divarication,” “Rectus abdominis diastasis,” “Sublay repair,” “Sublay technique,” “Retromuscular mesh placement,” “Ventral hernia,” “Ventral hernia repair,” “Abdominal wall reconstruction.”
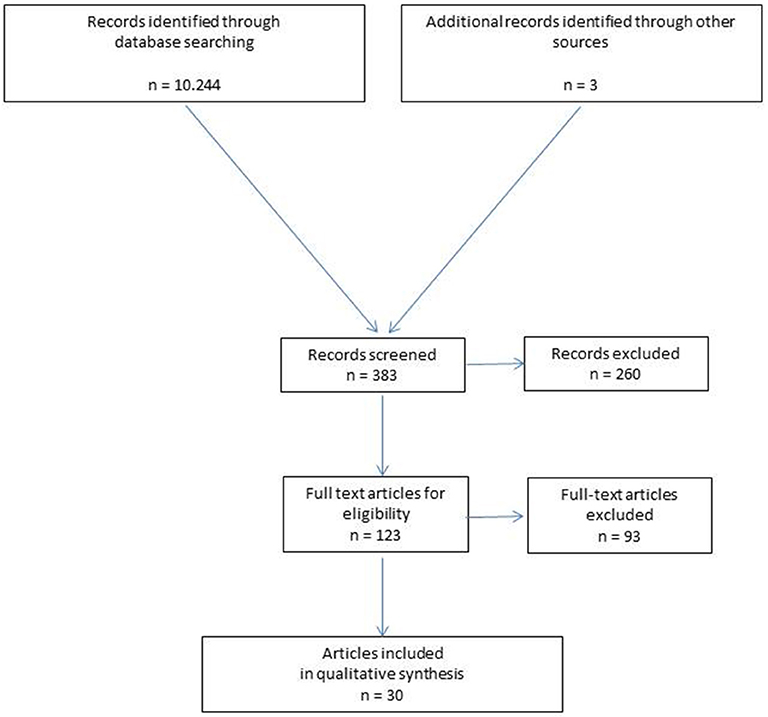
Figure 1. Flowchart of study inclusion.
The existence of the linea alba implies a physiological distance between the two rectus muscles. Beer et al. (22) examined 150 nulliparous women between 20 and 45 years of age and with a body mass index <30 kg/m2 by ultrasound at three reference points: the origin at the xiphoid, 3 cm above and 2 cm below the umbilicus. The mean width was 7 ± 5 mm at the xiphoid, 13 ± 7 mm above and 8 ± 6 mm below the umbilicus. For the definition of the normal width of the linea alba, the 10 and 90th percentiles were taken. The authors concluded that in nulliparous women the linea alba can be considered “normal” up to a width of 15 mm at the xiphoid, up to 22 mm at 3 cm above the umbilicus and up to 16 mm at the reference point 2 cm below the umbilicus.
In a recent ultrasound trial of 84 primiparous women, Mota et al. (23) measured the linea alba during and after pregnancy. The normal width of the linea alba was defined by the 20 and 80th percentiles. During pregnancy, the 20th and the 80th percentile corresponded to 49–79 mm at 2 cm below the umbilicus, 54–86 mm at 2 cm above the umbilicus and 44–79 mm at 5 cm above the umbilicus. At 6 months postpartum, the 20th and the 80th percentile corresponded to 9–21 mm, 17–28 mm, and 12–24 mm at 2 cm below, 2 cm above and 5 cm above the umbilicus, respectively.
In an anatomical study by Rath et al. (24), RD in patients below 45 years of age was considered as a separation of the two rectus muscles exceeding 10 mm above the umbilicus, 27 mm at the umbilical ring and 9 mm below the umbilicus. Above 45 years of age, the corresponding values were 15, 27, and 14 mm, respectively.
Hence, the anatomical measurements and ultrasound examinations produce similar findings. A separation of the rectus muscles of up to 2 cm can thus be considered normal. A separation of both medial edges of the rectus muscles of >2 cm must therefore be considered pathologic.
Ranney (25) proposed a classification of RD based on the width of the defect (Table 1): An observed separation of <3 cm between the rectus muscles has been labeled mild diastasis, 3–5 cm separation moderate diastasis and more than 5 cm severe diastasis.

Table 1. Width of RD according to Ranney (25).
For the length of the RD the European Hernia Society classification of midline incisional hernias can be used (20), separating the distance between the xiphoid and pubic bone into the subxiphoidal, epigastric, umbilical, infraumbilical, and suprapubic sectors (Figure 2). In addition to classification of the width and length (Figure 2 and Table 1), the maximum width and length of the RD should also be given in centimeters.
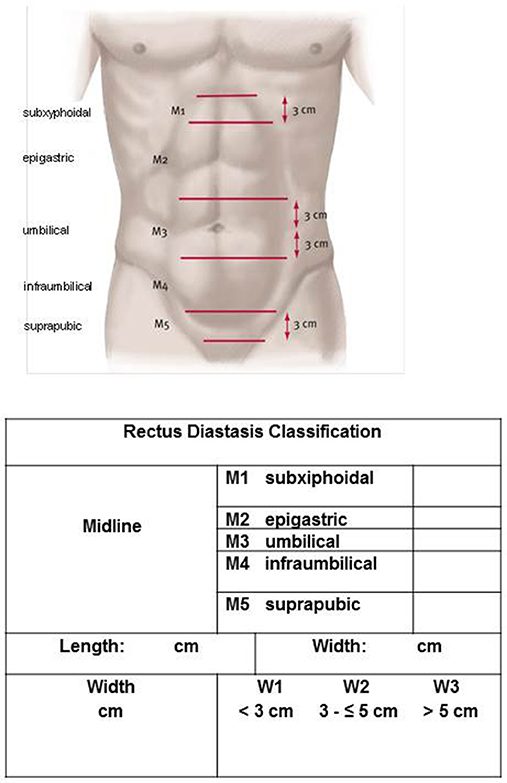
Figure 2. Length of RD according to the EHS incisional hernia classification.
Since concomitant hernias are the real indication for surgical treatment of RD (4), these should also be recorded. Often, several hernias are observed in association with RD (Table 2).
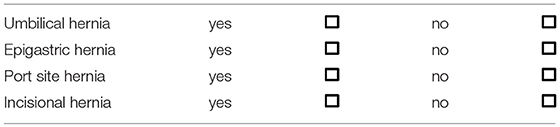
Table 2. Type of concomitant hernias in patients with RD.
It is also important to document all previous laparoscopic or open surgical procedures in cases of rectus diastasis (Table 3). Here a distinction should be made between previous primary ventral hernia repairs (umbilical or epigastric hernia) and laparoscopic and open abdominal surgical procedures as well as gynecology operations (Table 3) (26).
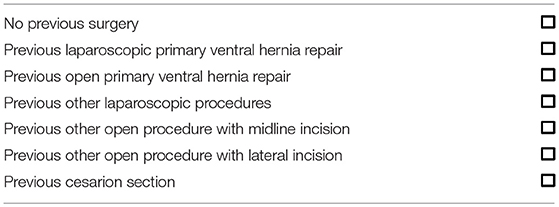
Table 3. Previous abdominal surgery within the width and length of the RD.
It is believed that women with RD have a greater number of pregnancies and deliveries. However, the results of other studies showed that RD above the umbilicus has similar prevalence in primiparae and multiparae (27). In order to obtain better data on this in the future, the number of pregnancies and multiple births should be precisely documented (Table 4). Older age at the first pregnancy and caesarian section lead more often to post-partum functional deficits of the lower trunk.
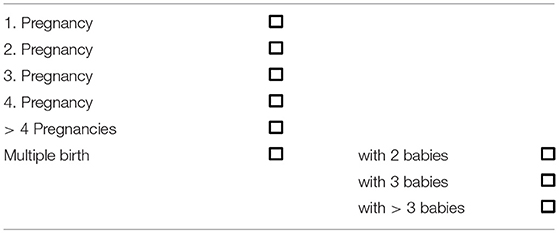
Table 4. Number of pregnancies and multiple birth.
Following childbirth women often experience not just RD but are also left with considerable excess skin, with upright skin folds. These patients will not benefit from corrective RD surgery alone but will also need to undergo abdominoplasty (28). Without appropriate abdominoplasty there will be even more excess skin and more pronounced skin folds following corrective RD surgery alone, with an unaesthetic cosmetic result and corresponding patient dissatisfaction. Therefore, due attention should be paid to the skin condition in therapy decision-making (Table 5) (28).

Table 5. Skin condition.
In a systematic review the available information supports the belief that ultrasound and calipers are adequate methods to asses RD (29). For other methods limited measurement information of low to moderate quality is available and further evaluation of these measurement properties is required (Table 6) (29).
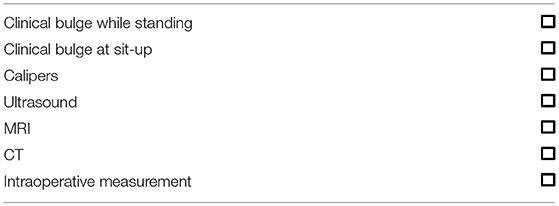
Table 6. Diagnostics of RD.
Patients with ventral hernias who already experience preoperative pain are also at higher risk of postoperative chronic pain (21). Patients with RD also experience more low back pain due to the instability of the abdominal wall (30). RD width may be associated with severity of low back pain (30). Therefore, the preoperative pain severity and localization should be carefully documented (Tables 7, 8).
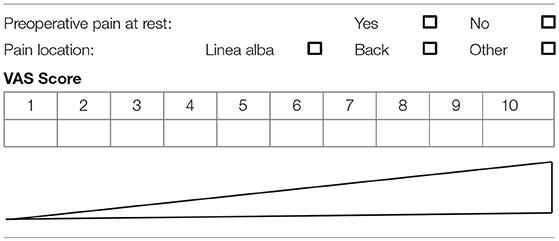
Table 7. Preoperative pain at rest.
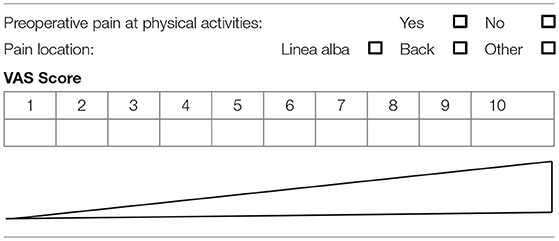
Table 8. Preoperative pain at physical activities.
In addition to the aforementioned, specific characteristics of rectus diastasis that could potentially affect the outcome, all other patient- and technique-related factors known to impact the outcome should of course also be documented (Tables 9, 10) (21).
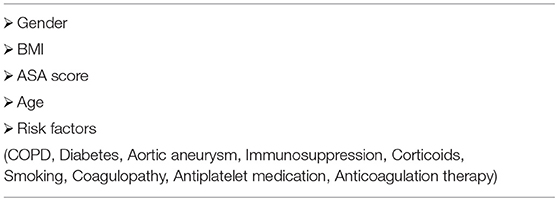
Table 9. Patient-related influencing factors on the outcome in hernia surgery.
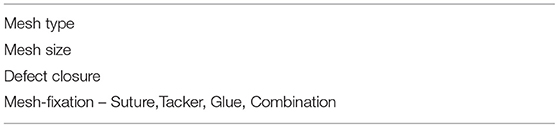
Table 10. Technic-related influencing factors on the outcome in hernia surgery.
In systematic reviews of the surgical treatment of RD, the published studies are assessed to be of low scientific and methodological quality (2, 5). The main reason for the poor quality of these studies on surgical treatment of RD is thought to be the lack of a uniform definition and classification of RD. This hampers comparability of the study findings on RD. Recently, numerous innovative techniques, with case series reports, have been introduced for surgical treatment of RD (4, 6–19). Classification of RD is needed in order to be able to evaluate the significance of all these different techniques and to properly characterize the respective patient collective in comparative studies. Only on the basis of comparative RD patient collectives can an acceptable method comparison be made.
Therefore, a working group of the DHG and the IEHS has compiled the classification presented here. In doing so, it has closely followed the European Hernia Society classification of primary and incisional abdominal wall hernias (20) and has added specific aspects of RD. In addition to the assignment of the RD longitudinal extension to midline sectors (subxiphoidal, epigastric, umbilical, infraumbilical, and subrapubic), the extension in centimeters is also recorded, as is the width of the rectus diastasis. Besides, the width of the rectus diastasis should be classified according to Ranney (25). An observed separation of <3 cm between the rectus muscles is labeled mild diastasis, 3–5 cm separation of the rectus muscles moderate diastasis and more than 5 cm severe diastasis (25). The concomitant hernias should be documented as well as any previous surgery. In particular in the case of women, the skin condition should be described since this has implications for treatment, generally involving a combination of corrective rectus diastasis surgery and abdominoplasty (28). The number of pregnancies and multiple births should also be documented. Since preoperative pain constitutes a risk factor for chronic postoperative pain, preoperative pain severity, and pain localization should also be noted (21). The diagnostic procedures used should also be specified in order to ascertain the basis on which the aforementioned parameters were defined.
In addition to these RD-specific factors, all patient-related factors known to impact the outcome of hernia surgery should of course also be documented (age, gender, ASA score, BMI, risk factors, COPD, diabetes, aortic aneurysm, immunosuppression, corticoids, smoking, coagulopathy, antiplatelet medication, and anticoagulation therapy) (21).
Likewise, the technical details of the operation, such as the mesh type, mesh size, defect closure and the fixation technique, should be documented (21). Only in that way will it be possible in multivariable analyses to identify all influencing factors on the outcome of a specific operation technique. Precise characterization of the patient collective is also needed for comparative analysis of operation techniques (21). Armed with that information it will be possible in the future to make a quality-oriented decision on the many new surgical techniques for treatment of RD.
In summary, in addition to the patient- and technique-related factors, RD-specific classification is needed for qualitative assessment of the numerous innovative surgical techniques for treatment of RD. The proposal presented here by a working group of the DHG and the IEHS classifies RD on the basis of the diastasis length (subxiphoidal, epigastric, umbilical, infraumbilical, and suprapubic), diastasis width (W1 < 3 cm, W2 = 3 – ≤ 5 cm, and W3 > 5 cm) concomitant hernias (umbilical, epigastric, port-site, and incisional hernia), previous operations, number of pregnancies and multiple births, skin condition and severity and localization of preoperative pain.
WR and FK: publication concept and draft. All authors: literature search, literature analysis, and critical review of the publication draft.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
2. Mommers EHH, Ponten JEH, Al Omar AK, de Vries Reilingh TS, Bouvy ND, Nienhuijs SW. The general surgeon's perspective of rectus diastasis. A systematic review of treatment options. Surg Endosc. (2017) 31:4934–49. doi: 10.1007/s00464-017-5607-9
3. Köhler G, Kuketina RR, Emmanuel K. Sutured repair of primary small umbilical and epigastric hernias: concomitant rectus diastasis is a significant risk factor for recurrence. World J Surg. (2015) 39:121–6. doi: 10.1007/s00268-014-2765-y
4. Bellido Luque J, Bellido Luque A, Valdivia J, Suarez Grau JM, Gomez Menchero J, Garcia Moreno J, et al. Totally endoscopic surgery on diastasis recti associated with midline hernias. The advantages of a minimally invasive approach. Prospective cohort study. Hernia (2014) 19:493–501. doi: 10.1007/s10029-014-1300-2
5. Hickey F, Finch JG, Khanna A. A systematic review on the outcomes of correction of diastasis of the recti. Hernia (2011) 15:607–14. doi: 10.1007/s10029-011-0839-4
6. Reinpold W, Schröder M, Berger C, Nehls J, Schröder A, Hukauf M, et al. Mini- or Less-open Sublay Operation (MILOS): a new minimally invasive technique for the extraperitoneal mesh repair of incisional hernias. Ann Surg. (2018). doi: 10.1097/SLA.0000000000002661
7. Schwarz J, Reinpold W, Bittner R. Endoscopic mini/less open sublay technique (EMILOS) – a new technique for ventral hernia repair. Langenbecks Arch Surg. (2017) 402:173–8. doi: 10.1007/s00423-016-1522-0
8. Reinpold W, Schröder M, Schröder A, Berger C, Nehls J, Stoltenberg W, et al. Minimally invasive sublay mesh repair of incisional and primary abdominal wall hernias using the MILOS technique. Eur Surg. (2017) 49:59–64. doi: 10.1007/s10353-017-0475-z
9. Bittner R, Schwarz J. Endoscopic mini/less open sublay operation for treatment of primary and secondary ventral hernias of the abdominal wall. Eur Surg. (2017) 49:65–70. doi: 10.1007/s10353-017-0472-2
10. Köckerling F, Botsinis MD, Rohde C, Reinpold W, Schug-Pass C. Endoscopic-assisted linea alba reconstruction new technique for treatment of symptomatic umbilical, trocar, and/or epigastric hernias with concomitant rectus abdominis diastasis. Eur Surg. (2017) 49:71–5. doi: 10.1007/s10353-017-0473-1
11. Köckerling F, Botsinis MD, Rohde C, Reinpold W. Endoscopic-assisted linea alba reconstruction plus mesh augmentation for treatment of umbilical and/or epigastric hernias and rectus abdominis diastasis – early results. Front Surg. (2016) 3:27. doi: 10.3389/fsurg.2016.00027
12. Belyansky I, Daes J, Radu VG, Balasubramanian R, Zahiri HR, Weltz AS, et al. A novel approach using the enhanced-view totally extraperitoneal (eTEP) technique for laparoscopic retromuscular hernia repair. Surg Endosc. (2018) 32:1525–32. doi: 10.1007/s00464-017-5840-2
13. Köhler G, Fischer I, Kaltenböck R, Schrittwieser R. Minimal invasive linea alba reconstruction for the treatment of umbilical and epigastric hernias with coexisting rectus abdominis diastasis. J Laparoendosc Adv Surg Tech A (2018) 28:1223–8. doi: 10.1089/lap.2018.0018
14. Goez-Menchero J, Guadalajara Jurado JF, Suarez Grau JM, Bellido Luque JA, Garcia Moreno JL, Alarcon del Agua I, et al. Laparoscopic intracorporeal rectus aponeuroplasty a step forward in minimally invasive abdominal wall reconstruction for ventral hernia repair (LVHR). Surg Endosc. (2018) 32:3502–8. doi: 10.1007/s00464-018-6070-y
15. Costa TN, Abdalla RZ, Santo MA, Tavares RRFM, Abdalla BMZ, Cecconello I. Transabdominal midline reconstruction by minimally invasive surgery: technique and results. Hernia (2016) 20:257–65. doi: 10.1007/s10029-016-1457-y
16. Moore AM, Gefen D, Anderson LN, Chen DC. Laparoscopic stapled sublay repair with self-grippen mesh: a simplified technique for minimally invasive etraperitoneal ventral hernia repair. Surg Technol Int. (2016) 29:131–9.
17. Nguyen DK, Chen DC. Laparoscopic stapled rives stoppa sublay technique for extraperitoneal ventral hernia repair. Eur Surg. (2017) 49:175–9. doi: 10.1007/s10353-017-0483-z
18. Juarez Muas DM. Preaponeurotic endoscopic repair (REPA) of diastasis recti associated or not to midline hernias. Surg Endosc. (2018). doi: 10.1007/s00464-018-6450-3. [Epub ahead of print].
19. Li B, Quin C, Bittner R. Totally endoscopic sublay (TES) repair for midline ventral hernia_ surgical technique and preliminary results. Surg. Endosc. (2018). doi: 10.1007/s00464-018-6568-3
20. Muysoms FE, Miserez M, Berrevoet F, Campanelli G, Champault GG, Chelala E, et al. Classification of primary and incisional abdominal wall hernias. Hernia (2009) 13:407–14. doi: 10.1007/s10029-009-0518-x
21. Köckerling F, Simon T, Hukauf M, Hellinger A, Fortelny R, Reinpold W, et al. The importance of registries in the postmarketing surveillance of surgical meshes. Ann Surgery (2017) 268:1097–1104. doi: 10.1097/SLA.0000000000002326
22. Beer GM, Schuster A, Seifert B, Manestar M, Mihic-Probst D, Weber SA. The normal width of the linea alba in nulliparous women. Clin Anat. (2009) 22:706–11. doi: 10.1002/ca.20836
23. Mota P, Pascoal AG, Carita AI, Bo K. Normal width of the inter-recti distance in pregnant and postpartum primiparous women. Musculoskelet Sci Pract. (2018) 35:34–7. doi: 10.1016/j.msksp.2018.02.004
24. Rath AM, Attali P, Dumal JL, Goldlust D, Zhang J, Chevrel JP. The abdominal linea alba: an anatomo-radiologic and biomechanical study. Surg Radiol Anat. (1996) 18:281–8. doi: 10.1007/BF01627606
25. Ranney B. Diastasis recti and umbilical hernia causes, recognition and repair. SDJ Med. (1990) 43:5–8.
26. Tadiparthi S, Shokrollahi K, Doyle GS, Fahmy FS. Rectus sheath plication in abdominoplasty: assessment of its longevity and a review of the literature. JPRAS (2012) 65:328–32. doi: 10.1016/j.bjps.2011.09.024
27. Rett MT, Braga MD, Bernardes NO, Andrade SC. Prevalence of diastasis of the rectus abdominis muscles immediately postpartum: comparison between primaparae and multiparae. Brazil J Phys Ther. (2009) 13:275–80. doi: 10.1590/S1413-35552009005000037
28. Nahas FX. An aesthetic classification of the abdomen based on the myoaponeurotic layer Plast. Reconstr Surg. (2001) 108:1787–95. doi: 10.1097/00006534-200111000-00058
29. Van de Water ATM, Benjamin DR. Measurement methods to assess diastasis of the rectus abdominis muscle (DRAM): as systematic review of their measurement properties and meta-analytic reliability generalization. Man Ther. (2016) 21:41–53. doi: 10.1016/j.math.2015.09.013
Keywords: rectus diastasis, classification, concomitant hernia, pregnancy, defect width
Citation: Reinpold W, Köckerling F, Bittner R, Conze J, Fortelny R, Koch A, Kukleta J, Kuthe A, Lorenz R and Stechemesser B (2019) Classification of Rectus Diastasis—A Proposal by the German Hernia Society (DHG) and the International Endohernia Society (IEHS). Front. Surg. 6:1. doi: 10.3389/fsurg.2019.00001
Received: 20 November 2018; Accepted: 09 January 2019;
Published: 28 January 2019.
Edited by:
Hakan Kulacoglu, Recep Tayyip Erdogan University, TurkeyReviewed by:
Andrew Gumbs, Summit Medical Group, United StatesCopyright © 2019 Reinpold, Köckerling, Bittner, Conze, Fortelny, Koch, Kukleta, Kuthe, Lorenz and Stechemesser. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ferdinand Köckerling, ZmVyZGluYW5kLmtvZWNrZXJsaW5nQHZpdmFudGVzLmRl
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.