 Riccardo Campi1,2*
Riccardo Campi1,2* Francesco Sessa1
Francesco Sessa1 Fabrizio Di Maida1Isabella Greco1Andrea Mari1,2
Fabrizio Di Maida1Isabella Greco1Andrea Mari1,2 Tána Takáčová3Andrea Cocci1Riccardo Fantechi1Alberto Lapini1Sergio Serni1,2Marco Carini1,2Andrea Minervini1,2
Tána Takáčová3Andrea Cocci1Riccardo Fantechi1Alberto Lapini1Sergio Serni1,2Marco Carini1,2Andrea Minervini1,2- 1Department of Urology, Careggi Hospital, University of Florence, Florence, Italy
- 2Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy
- 3Department of Internal Medicine IV, Rheumatology, Clinical Immunology, Nephrology, HELIOS Dr. Horst-Schmidt-Kliniken Wiesbaden, Wiesbaden, Germany
Background: The role of lymph node dissection (LND) for renal cell carcinoma (RCC) is controversial. Notably, the conflicting evidence on the benefits and harms of LND is inherently linked to the lack of consensus on both anatomic templates and extent of lymphadenectomy. Herein, we provide a detailed overview of the most commonly dissected templates of LND for RCC, focusing on key anatomic landmarks and patterns of lymphatic drainage.
Methods: A systematic review of the English-language literature was performed without time filters in July 2018 in accordance to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement recommendations. The primary endpoint was to summarize the most commonly dissected templates of LND according to the side of RCC.
Results: Overall, 25 studies were selected for qualitative analysis. Of these, most were retrospective. The LND template was heterogeneous across studies. Indications and extent of LND were either not reported or not standardized in most series. The most commonly dissected template for right-sided tumors included hilar, paracaval, and precaval nodes, with few authors extending the dissection to the inter-aortocaval, retrocaval, common iliac or pre/paraaortic nodes. Similarly, the most commonly dissected template for left-sided tumors encompassed the renal hilar, preaortic and paraaortic nodes, with few authors reporting a systematic dissection of inter-aortocaval, retro-aortic, common iliac, or para-caval nodes.
Conclusions: In light of the unpredictable renal lymphatic anatomy and the evidence from available prospective mapping studies, the extent of the most commonly dissected templates might be insufficient to catch the overall anatomic pattern of lymphatic drainage from RCC.
Introduction
The role of lymph node dissection (LND) for renal cell carcinoma (RCC) is controversial (1–6). Indeed, while the latest Guidelines of the European Association of Urology (EAU) recommend considering an extended LND in patients with adverse clinical features and in the presence of clinically positive lymph nodes (LN) (5), the American Urological Association (AUA) and National Comprehensive Cancer Network (NCCN) Guidelines stressed that LND should be performed primarily for staging and prognostic purposes, and recommended not to perform routine LND in patients with clinically negative nodes (4, 7).
The lack of consensus on indications and value of LND stems from conflicting evidence on its ultimate impact on oncologic outcomes in both non-metastatic and metastatic patients with RCC (8–11). Yet, several factors may play a role in determining the outcomes of this procedure, such as surgical techniques, anatomic dissection templates and patient selection. In addition, there is lack of definitive knowledge on the anatomy of lymphatic drainage from RCC, which is unpredictable due to a wide heterogeneity of lymphatic vessels anatomy (12–14), the potential early hematogenous dissemination without LN infiltration (11, 12, 15) and the effects of local tumor progression (1).
Notably, as in other urological malignancies (16), the evidence on the anatomic templates of LND at the time of conservative or radical surgery for RCC is sparse and fragmentary (1, 2), making the interpretation of its benefits and harms challenging.
Therefore, we aimed to provide a detailed overview of the most commonly dissected templates of LND for RCC, focusing on key anatomic landmarks and patterns of lymphatic drainage.
Methods
Search Strategy
A systematic review of the English-language literature was performed without time filters using the MEDLINE (via PubMed), Cochrane Central Register of Controlled Trials and Web of Science (WoS) databases in July 2018 using the keywords ‘lymph node dissection’ or ‘lymphadenectomy’ or ‘lymph nodes’ or ‘lymphatic drainage’ or ‘sentinel node’ or ‘mapping’ combined with ‘renal cancer’ or ‘renal cell carcinoma’ and ‘template’ or ‘landmark’ or ‘extent’. The review process was performed in accordance to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement recommendations (17). A specific search strategy was designed using both free text and Mesh Terms. Hand-search of bibliographies of included studies and previous reviews on the topic was also performed to include additional relevant studies. Two reviewers (RC and FS) carried out the literature search independently.
Inclusion Criteria
A specific population (P), intervention (I), comparator (C), outcome (O), and study design (S) (PICOS) framework was specified to define study eligibility, as recommended (17). In particular, the following criteria were outlined:
- Population (P): patients with non-metastatic or metastatic RCC;
- Intervention (I): conservative (partial nephrectomy) or radical (radical nephrectomy) surgery with LND;
- Comparison (C): patients undergoing surgery without LND (this criterion was not mandatory for inclusion of the studies in this review);
- Outcomes (O): anatomic extent of LND with detailed reporting of side-specific templates, including upper/lower boundaries of dissection, as well as of the number of patients undergoing LND;
- Study design (S): randomized-controlled or prospective/retrospective cohort studies with or without comparison of different LND templates.
Studies with insufficient reporting of the PICOS criteria were excluded. The primary endpoint of this review was to summarize the most commonly dissected templates of LND according to the side of RCC.
Systematic Review Process
Mendeley reference software (Mendeley Ltd, London, UK) was used to identify and remove duplicates among records identified. Overall, 4,205 articles were preliminarily identified by the literature search. After exclusion of duplicates and articles not related to the topic of this review (n = 2,671), two independent reviewers (RC, FS.) screened titles and abstracts of 1,534 records. An a priori developed screening form was created to guide study selection. Disagreement was solved by a third party (AM), who supervised the systematic review process. After exclusion of case reports, book chapters, editorials, conference abstracts, animal studies, pre-clinical studies, previous reviews, and articles not related to the primary endpoint of this review, 103 articles were assessed for eligibility. Finally, 25 studies fullfilling all inclusion criteria were selected for qualitative analysis. The flow-chart depicting the overall review process according to PRISMA is shown in Supplementary Figure 1.
Data Extraction
Data were extracted independently by two authors (IG, TT) in a-priori developed data extraction form. This included all relevant information on the anatomic landmarks of LND and on all elements of the PICOS framework, including study design, patient population, RCC characteristics and pathologic stage, indication for LND, extent of LND, LND metrics (number of LNs removed and of positive LNs, if provided) and specific description of LND templates according to tumor side (Table 1). A narrative form was used for qualitative data synthesis.
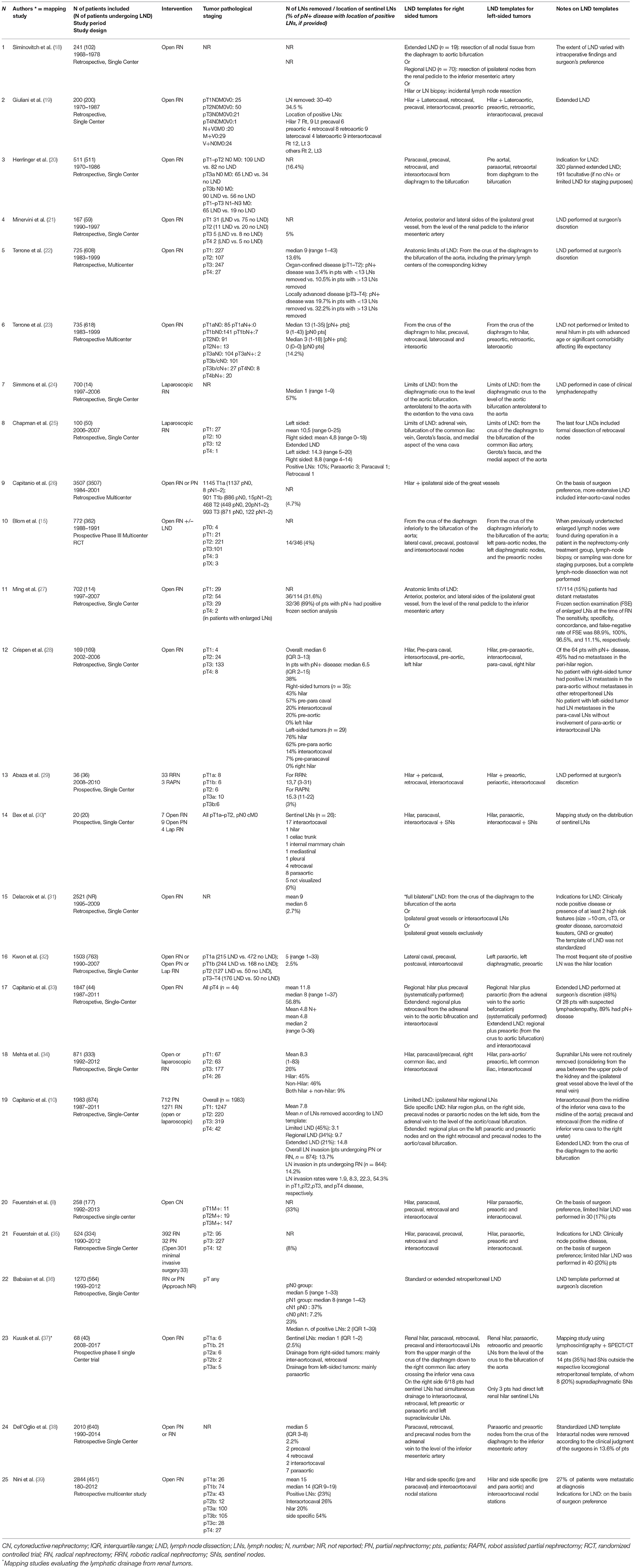
Table 1. Characteristics of studies included in the review with focus on study design, intervention, tumor stage, and anatomical templates of lymph node dissection in patients with renal cell carcinoma (RCC).
Results
Characteristics of Included Study and Quality of Reporting LND Templates
The key characteristics and findings of the studies included in the review are shown in Table 1. Of the 25 studies included in final qualitative analysis, 21 were retrospective, either single- (n = 17) or multicenter (n = 4), while 3 were prospective single-center. One multicenter randomized-controlled trial (RCT) was included (15). Only two studies were specifically designed to evaluate the pattern of lymphatic drainage from RCC by using sequential lymphoscintigraphy and sentinel node (SN) biopsy (30, 37). No study compared LN yield, cancer control and surgical complications of extended vs. limited LND. Risk of bias assessment for the studies included in the review is depicted in Supplementary Table 1. Overall, the quality of evidence according to Grading of Recommendations Assessment, Development, and Evaluation (GRADE) is low.
Overall, the proportion of patients undergoing LND was heterogeneous across included studies and indications for LND were not standardized in most series, being based on surgeon's preference and/or according to intraoperative suspicion of LN metastases (Table 1). Most studies described an open surgical approach for both nephrectomy and LND. A minimally invasive approach was used in selected series, using either a laparoscopic (n = 7) (8, 10, 24, 25, 30, 34, 35) or robotic approach (n = 1) (29). Pathologic tumor stage was heterogeneous across included studies, although most series considered locally advanced tumors (pT stage 3–4) (15, 22, 23, 28, 34, 35, 39). One study examined the role of LND at the time of cytoreductive nephrectomy (8).
The overall number of LNs removed at the time of surgery (10, 19, 22–25, 28–34, 36–39), as well as the proportion of positive LNs, were reported by the majority of included studies, despite the latter was highly variable across the included studies (range 0–56,8%) (Table 1). Of note, only a minority of reports described the specific anatomic location (and number) of positive nodes (19, 25, 28, 30, 34, 37–39). All included studies reported a side-specific anatomical template of LND, with description of the anatomical boundaries and upper/lower limits of dissection; yet, indications and extent (i.e., standard vs. extended) of LND were either not reported or not standardized in most series. Furthermore, only few authors reported the lateral landmarks of dissection for the paracaval/paraaortic templates [i.e., the right and left ureter, respectively (10)].
The overview of the most commonly dissected templates of LND for RCC according to tumor side is shown in Figure 1, while a detailed analysis of the specific templates considered in each study included in the review in Table 1. Of note, it was not possible to define a putative pattern of lymphatic spread from RCC due to lack of information on the location of positive LNs within the anatomical sites of the template in most series.
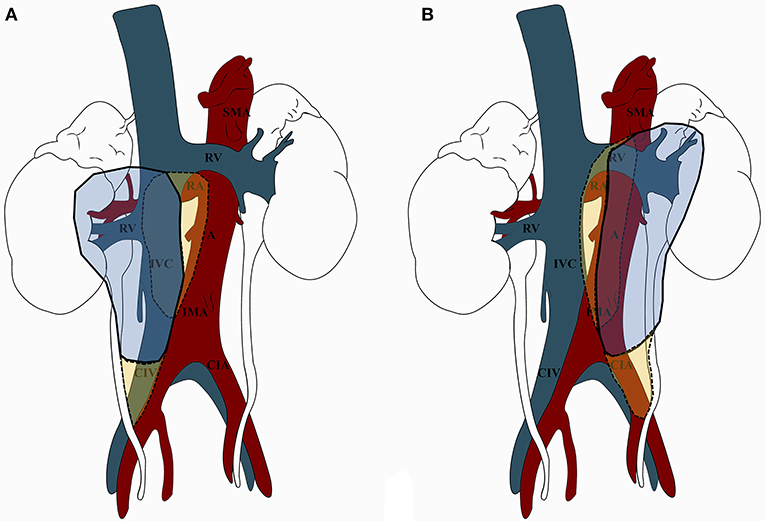
Figure 1. Overview of the most commonly dissected templates of lymph node dissection (LND) for renal cell carcinoma (RCC) according to tumor side (A. Right-sided tumors; B. Left-sided tumors). (A) For right-sided tumors, LND included in most cases (continuous line) the renal hilar, paracaval, and precaval nodes, from the crus of the diaphragm to the aortic bifurcation (in blue). Extended LND (dotted line) also included the inter-aortocaval/retrocaval nodes and the right common iliac nodes (in yellow). (B). For left-sided tumors, LND included in most cases (continuous line) the renal hilar, preaortic, and paraaortic nodes, from the crus of the diaphragm to the aortic bifurcation (in blue). Extended LND (dotted line) also included the inter-aortocaval/retroaortic nodes and the left common iliac nodes (in yellow). A, aorta; CIA, common iliac artery; CIV, common iliac vein; IMA, inferior mesenteric artery; IVC, inferior vena cava; RA, renal artery; RV, renal vein; SMA, superior mesenteric artery.
Templates of Lymph Node Dissection for Right-Sided RCC
For right-sided tumors, the LND template included in most cases the hilar, paracaval (on the lateral side of the vena cava), and precaval (i.e., on the anterior side of the vena cava) nodes, from the crus of the diaphragm to the aortic bifurcation (Table 1). Some authors reported the dissection of a more extended template including the inter-aortocaval (8, 15, 19, 20, 25, 28–30, 32–35, 37, 39), retrocaval (8, 15, 19–21, 23, 27, 29, 32, 35, 37, 38), common iliac (25) nodes or even pre/paraaortic nodes (19). In their retrospective study on the outcomes of laparoscopic radical nephrectomy with or without LND, Chapman et al. included the removal of inter-aortocaval and retrocaval nodes only in the last group of patients included in the series (25). Notably, Abaza et al. showed the feasibility of performing LND for right-sided tumors including paracaval, retrocaval, and inter-aortocaval nodes using a robotic approach (29).
The study by Nini et al. evaluated the pattern of nodal metastatic dissemination from RCC in a cohort of patients undergoing extended LND including removal of hilar, pre/paracaval and inter-aortocaval nodes (39). The authors found that, in case of right-sided tumors, the positive LNs were located in the paracaval, interaortocaval, and renal hilar regions in 44, 40, and 16% of cases, respectively. When two nodal areas were involved, they included the paracaval + interaortocaval regions in 87% of cases. It is important to highlight that in their retrospective cohort study, Crispen et al. reported that, despite the location of LN metastases was related to the tumor side, 45% of patients with pN+ disease had no metastases in the perihilar nodes and no patient with a right-sided tumor had involvement of the para-aortic LNs without metastases in other retroperitoneal lymph nodes (28).
Templates of Lymph Node Dissection for Left-Sided RCC
For left-sided tumors, the most commonly dissected anatomical templates were the renal hilar, pre/para aortic (i.e., on the anterior and lateral side of the aorta) from the crus of the diaphragm to the aortic bifurcation (Table 1). Of note, only few authors reported a systematic dissection of a more extended template including inter-aortocaval (8, 19, 25, 28–30, 34, 35, 39), retro-aortic (19–21, 23, 27, 28, 37), common iliac (25), or even para-caval (28) nodes. A LND template including periaortic and interaortocaval nodes was also described by Abaza et al. in their study including patients undergoing robotic LND (29). In their study on extended LND, Nini et al. reported that positive LNs from left-sided tumors were located in the pre/paraaortic, interaortocaval, and renal hilar regions in 67, 9, and 24% of cases (39). When two nodal areas were involved, they included the pre/paraaortic + renal hilar regions in 91% of cases. Of note, in the retrospective study by Crispen et al. (28), no patient with a left-sided tumor had positive paracaval LNs without involvement of para-aortic or interaortocaval nodes.
Mapping Studies Using the Sentinel Node Technique Assessing the Pattern of Lymphatic Drainage From RCC
Two studies included in the review were specifically designed to evaluate the pattern of lymphatic drainage from RCC using sequential lymphoscintigraphy and sentinel node biopsy (30, 37). In the largest prospective phase II single-arm study evaluating the distribution of sentinel LNs and the lymphatic drainage pattern of renal tumors in vivo with SPECT, Kuusk et al. found that drainage from right-sided tumors was predominantly into inter-aortocaval and retrocaval sentinel nodes (37). Moreover, 6/18 (33%) patients with right-sided tumors had simultaneous drainage to interaortocaval, retrocaval, left preaortic or para-aortic, and left supraclavicular lymph nodes. Only three patients had sentinel LNs in the right paracaval and renal hilar and no patient to precaval LNs. The distribution of sentinel LNs from left-sided tumors revealed that the lymphatic drainage was mainly into para-aortic LNs and that very few patients had direct left hilar sentinel LNs (37). Moreover, 9/22 (41%) had simultaneous renal hilar, mediastinal, left supraclavicular, retrocrural, left common iliac, renal fossa, and interaortocaval sentinel LNs.
Discussion
Lymph node dissection has staging, prognostic and potentially therapeutic roles in several urologic malignancies, including prostate (40), bladder (41), testis (42), and upper tract urothelial (16) tumors. Of note, its role in the management of RCC is still debated (3–5, 7). Accordingly, a recent large European multi-institutional study reported a trend toward lower rates of LND over time for patients undergoing radical or partial nephrectomy for RCC (43). The most recent systematic review on this topic (3) concluded that, although LND yields independent prognostic information, the existing literature does not support a therapeutic benefit in either non-metastatic or metastatic RCC. Nonetheless, LND may have a role in selected high-risk non-metastatic patients, for whom further prospective studies are warranted (3). Indeed, the extent of LND has been shown to affect cancer-specific survival and metastatic progression in specific sub-categories of patients with RCC (10).
This conflicting evidence on the benefits and harms of LND for RCC (1, 9, 11, 44), which directly impacts the strengths of Guidelines recommendations (4, 5, 7), is inherently linked to the lack of consensus on both anatomic templates and extent of lymphadenectomy (4). In this regard, some authors advocate routine extended LND (if indicated) (6); yet, the potential oncologic benefits should be balanced with the increased risk of surgical complications, which may be not negligible in this setting (45). Beyond the lack of standardized reporting of surgical templates of LND in the literature (including the only RCT available to date (1, 2, 14, 15), the complex anatomy of lymphatic drainage from RCC undermines a thorough understanding of the anatomic sites of lymphatic involvement.
Therefore, in this review we provided a detailed assessment of the most commonly dissected templates of LND for RCC, focusing on the key anatomic landmarks and on the putative patterns of lymphatic drainage, as suggested by available mapping studies.
The available autopsy studies underscore the unpredictable variability of drainage patterns and the heterogeneity of lymphatic metastases from RCC; as such, they provided only limited evidence for defining effective LND templates to date (1, 12, 13, 46–48). Overall, four critical issues should be considered when evaluating potential anatomic templates of LND for RCC. First, the presence of anterior, intravascular, and posterior bundles of efferent lymphatic vessels from both the right and left kidney, whose drainage pattern is still not completely understood (12). These efferent lymphatics drain into paracaval, precaval, retrocaval, and interaortocaval nodes, for right-sided tumors, and into paraaortic, preaortic, and retroaortic nodes, for left-sided tumors (13, 46). Second, the existence of peripheral lymphovenous communication sites located in the inferior vena cava at the level of the renal veins or through the thoracic duct (12); these communications may imply LN station skipping and explain how distant metastases can occur without concurrent retroperitoneal LN involvement (14, 46). Third, the effects of local tumor growth may be responsible for further unpredictability (2). Finally, renal hilar regions have been shown to be rarely affected by LN metastases (49, 50).
The anatomy of lymphatic drainage from RCC has been also investigated in vivo taking advantage of sentinel LN biopsy (12, 30, 37, 51). Although this technique may be theoretically challenged by tumor lymphangiogenesis and lymphatic remodeling, the largest mapping study available to date showed that drainage from right-sided tumors was predominantly into inter-aortocaval and retrocaval sentinel nodes while drainage from left-sided tumors mainly into para-aortic LNs (37). Moreover, only a negligible proportion of patients had sentinel LNs in the ipsilateral renal hilar regions.
Our review provides relevant information to better contextualize the current evidence on anatomic templates of LND for RCC.
A key finding is that the surgical template for LND was heterogenous across the included studies and only a minority of reports described the specific anatomic location (and number) of positive nodes within the template (Table 1). Moreover, indications and extent of LND were either not reported or not standardized in most series and relied mainly on surgeon's judgement. An additional finding is that the most commonly dissected template for right-sided tumors included hilar, paracaval, and precaval nodes, with few authors extending the dissection to the inter-aortocaval, retrocaval, common iliac, or pre/paraaortic nodes (Table 1). As such, considering the findings of the available mapping studies using the SN technique (30, 37) as well as those of studies reporting an extended LND in high-risk patients (28, 39), the extent of the most commonly dissected templates for right-sided tumors (especially if advanced in stage) might be insufficient to catch the comprehensive pattern of lymphatic drainage, which frequently involves the retro-caval and inter-aorto-caval sites. Similarly, the most commonly dissected template for left-sided tumors encompassed the renal hilar, pre/para aortic nodes, with few authors reporting a systematic dissection of inter-aortocaval, retro-aortic, common iliac, or para-caval nodes (Figure 1). In conclusion, in light of the above discussed anatomic considerations, the templates of LND most commonly dissected for both right- and left-sided tumors might be unable to capture the complexity of the LN drainage from RCC. This concept is reflected in the relatively low number of LNs removed in most of the included studies (Table 1).
The findings from our review should be interpreted in light of several limitations at both a review- and study-level. Our review was not designed to assess the association of LND templates with positive LNs and key oncologic outcomes after surgery for RCC. As such, we were unable to evaluate the potential impact of extent of LND and cancer-specific or overall survival after surgery. Second, the review strategy might not have been able to identify all relevant studies on the topic of interest. In particular, a limitation of our review is that studies that did not fulfill the pre-specified eligibility criteria (including detailed reporting of anatomical LND templates) were excluded from the qualitative synthesis. Therefore, studies that attempted to address the role of extended vs. limited LND which did not adequately report the anatomic sites of LND were not included in our review. Third, most studies included in qualitative analysis were retrospective, subject to selection bias. Moreover, patient populations, surgical approaches, techniques for LND and quality of reporting LND results were highly heterogeneous across included studies, reducing the generalizability of findings. In this regard, due to the low number of series reporting LND during robotic or laparoscopic surgery, the above mentioned LND templates may not be entirely applicable to minimally-invasive surgery. Finally, it was not possible to evaluate the potential association between number of LNs removed (which has been associated with rate of LN metastases and cancer-specific survival (10, 11, 22) and anatomic extent of LND template, due to the lack of this information in most series.
Our review affords opportunities for significant further research in this field. In particular, future RCTs should evaluate the benefits and harms of extended LND using standardized anatomic templates in patients with high-risk RCC, where LND may significantly impact on the disease course (45). Such studies should aim to build an evidence-based consensus on the surgical management of retroperitoneal nodes in patients with RCC, overcoming the complexity of renal lymphatic anatomy. To this aim, an effective study design should compare extended vs. no LND to avoid risk of misclassification of pN status due to the confounding effect of a limited LND arm (52). Future mapping studies should improve in vivo evaluation of lymphatic drainage from RCC, taking advantage of sentinel node (37) and frozen section analysis (27), novel technologies (including indocyanine green fluorescent lymphography) and advanced multimodality imaging (12). Finally, further research should explore the role of LND during minimally-invasive surgery to assess the feasibility and outcomes of extended surgical templates.
Conclusions
The conflicting evidence on the benefits and harms of LND for RCC is inherently linked to the lack of consensus on anatomic templates and extent of lymphadenectomy. In this review, we provided an overview of the most commonly dissected templates of LND, focusing on key anatomic landmarks and patterns of lymphatic drainage. The surgical template for LND was heterogenous across included studies, and indications and extent of LND were either not reported or not standardized in most series.
For right-sided tumors, the most commonly dissected templates were the hilar, paracaval, and precaval nodes, while for left-sided tumors, the renal hilar, pre/para aortic nodes, both from the crus of the diaphragm to the aortic bifurcation.
In light of the unpredictable renal lymphatic anatomy and considering the evidence from available prospective mapping studies, which suggest that lymphatic drainage from renal tumors may be directed predominantly to inter-aortocaval and retrocaval nodes—on the right side—and para-aortic and inter-aortocaval nodes—on the left side, the extent of the most commonly dissected templates might be insufficient to catch the overall anatomic pattern of lymphatic drainage from RCC, especially for higher stage and right-sided tumors.
Author Contributions
RC and AMi contributed conception and design of the study. RC and FS performed the literature review (study screening and study selection). IG and TT performed the data extraction from the studies included in the review. RC, FS, AMa, AL, SS, MC, and AMi analyzed and interpreted the data extracted from the studies included in the review. RC and FS wrote the first draft of the manuscript. All authors contributed to manuscript revision, read and approved the submitted version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling Editor declared past co-authorships with several of the authors RC, FS, AMa, TT, SS, MC, and AMi.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2018.00076/full#supplementary-material
Supplementary Figure 1. Flow-chart showing the literature search and systematic review process according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement recommendations.
Supplementary Table 1. Risk of bias assessment among studies included in the review according to the Newcastle-Ottawa-Scale (NOS) for non-randomized studies and to the Cochrane risk of bias assessment tool for randomized trials. / = not applicable; Un = unclear. The overall quality of evidence was assessed according to Grading of Recommendations Assessment, Development, and Evaluation (GRADE) recommendations (53).
References
1. Capitanio U, Becker F, Blute ML, Mulders P, Patard JJ, Russo P, et al. Lymph node dissection in renal cell carcinoma. Eur Urol. (2011) 60:1212–20. doi: 10.1016/j.eururo.2011.09.003
2. Capitanio U, Leibovich BC. The rationale and the role of lymph node dissection in renal cell carcinoma. World J Urol. (2017) 35:497–506. doi: 10.1007/s00345-016-1886-3
3. Bhindi B, Wallis CJD, Boorjian SA, Thompson RH, Farrell A, Kim SP, et al. The role of lymph node dissection in the management of renal cell carcinoma: a systematic review and meta-analysis. BJU Int. (2018) 121:684–98. doi: 10.1111/bju.14127
4. Campbell S, Uzzo RG, Allaf ME, Bass EB, Cadeddu JA, Chang A, et al. Renal mass and localized renal cancer: AUA guideline. J Urol. (2017) 198:520–9. doi: 10.1016/j.juro.2017.04.100
5. Lyunberg B, Albiges L, Bensalah K, Bex A, Giles RH, Hora M, et al. European Association of Urology Guidelines on Renal Cell Carcinoma. Edn. Presented at the EAU Annual Congress. Copenhagen (2018). Available online at: https://uroweb.org/guideline/renal-cell-carcinoma/
6. Montgomery JS, Leibovich BC. Lymph node excision for renal cancer. J Urol. (2013) 189:419–21. doi: 10.1016/j.juro.2012.11.086
7. Motzer RJ, Jonasch E, Agarwal N, Bhayani S, Bro WP, Chang SS, et al. Kidney cancer, version 2.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2017) 15:804–34. doi: 10.6004/jnccn.2017.0100
8. Feuerstein MA, Kent M, Bernstein M, Russo P. Lymph node dissection during cytoreductive nephrectomy: a retrospective analysis. Int J Urol. (2014) 21:874–9. doi: 10.1111/iju.12457
9. Gershman B, Thompson RH, Moreira DM, Boorjian SA, Tollefson MK, Lohse CM, et al. Radical nephrectomy with or without lymph node dissection for nonmetastatic renal cell carcinoma: a propensity score-based analysis. Eur Urol. (2017) 71:560–7. doi: 10.1016/j.eururo.2016.09.019
10. Capitanio U, Suardi N, Matloob R, Roscigno M, Abdollah F, Di Trapani E, et al. Extent of lymph node dissection at nephrectomy affects cancer-specific survival and metastatic progression in specific sub-categories of patients with renal cell carcinoma (RCC). BJU Int. (2014) 114:210–5. doi: 10.1111/bju.12508
11. Whitson JM, Harris CR, Reese AC, Meng MV. Lymphadenectomy improves survival of patients with renal cell carcinoma and nodal metastases. J Urol. (2011) 185:1615–20. doi: 10.1016/j.juro.2010.12.053
12. Karmali RJ, Suami H, Wood CG, Karam JA. Lymphatic drainage in renal cell carcinoma: back to the basics. BJU Int. (2014) 114:806–17. doi: 10.1111/bju.12814
13. Parker A. Studies on the main posterior lymph channels of the abdomen and their connections with the lymphatics of the genitourinary system. Am J Anat. (1935) 56:409–43. doi: 10.1002/aja.1000560305
14. Moschini M, Dell'Oglio P, Larcher A, Capitanio U. Lymph node dissection for renal carcinoma: what are we missing? Curr Opin Urol. (2016) 26:424–31. doi: 10.1097/MOU.0000000000000312
15. Blom JH, van Poppel H, Maréchal JM, Jacqmin D, Schröder FH, de Prijck L, et al. EORTC genitourinary tract cancer group. radical nephrectomy with and without lymph-node dissection: final results of European Organization for Research and Treatment of Cancer (EORTC) randomized phase 3 trial 30881. Eur Urol. (2009) 55:28–34. doi: 10.1016/j.eururo.2008.09.052
16. Campi R, Minervini A, Mari A, Hatzichristodoulou G, Sessa F, Lapini A, et al. Anatomical templates of lymph node dissection for upper tract urothelial carcinoma: a systematic review of the literature. Expert Rev Anticancer Ther. (2017) 17:235–46. doi: 10.1080/14737140.2017.1285232
17. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. (2009) 62:1006–12. doi: 10.1016/j.jclinepi.2009.06.005
18. Siminovitch JP, Montie JE, Straffon RA. Lymphadenectomy in renal adenocarcinoma. J Urol. (1982) 127:1090–91. doi: 10.1016/S0022-5347(17)54242-1
19. Giuliani L, Giberti C, Martorana G, Rovida S. Radical extensive surgery for renal cell carcinoma: long-term results and prognostic factors. J Urol. (1990) 143:468–73. doi: 10.1016/S0022-5347(17)39992-5
20. Herrlinger A, Schrott KM, Schott G, Sigel A. What are the benefits of extended dissection of the regional renal lymph nodes in the therapy of renal cell carcinoma. J Urol. (1991) 146:1224–7. doi: 10.1016/S0022-5347(17)38052-7
21. Minervini A, Lilas L, Morelli G, Traversi C, Battaglia S, Cristofani R, et al. Regional lymph node dissection in the treatment of renal cell carcinoma: is it useful in patients with no suspected adenopathy before or during surgery? BJU Int. (2001) 88:169–72. doi: 10.1046/j.1464-410x.2001.02315.x
22. Terrone C, Guercio S, De Luca S, Poggio M, Castelli E, Scoffone C, et al. The number of lymph nodes examined and staging accuracy in renal cell carcinoma. BJU Int. (2003) 91:37–40. doi: 10.1046/j.1464-410X.2003.04017.x
23. Terrone C, Cracco C, Porpiglia F, Bollito E, Scoffone C, Poggio M, et al. Reassessing the current TNM lymph node staging for renal cell carcinoma. Eur Urol. (2006) 49:324–31. doi: 10.1016/j.eururo.2005.11.014
24. Simmons MN, Kaouk J, Gill IS, Fergany A. Laparoscopic radical nephrectomy with hilar lymph node dissection in patients with advanced renal cell carcinoma. Urology (2007) 70:43–6. doi: 10.1016/j.urology.2007.03.048
25. Chapman TN, Sharma S, Zhang S, Wong MK, Kim HL. Laparoscopic lymph node dissection in clinically node-negative patients undergoing laparoscopic nephrectomy for renal carcinoma. Urology (2008) 71:287–91. doi: 10.1016/j.urology.2007.08.057
26. Capitanio U, Jeldres C, Patard JJ, Perrotte P, Zini L, de La Taille A, et al. Stage-specific effect of nodal metastases on survival in patients with non-metastatic renal cell carcinoma. BJU Int. (2009) 103:33–7. doi: 10.1111/j.1464-410X.2008.08014.x
27. Ming X, Ningshu L, Hanzhong L, Zhongming H, Tonghua L. Value of frozen section analysis of enlarged lymph nodes during radical nephrectomy for renal cell carcinoma. Urology (2009) 74:364–8. doi: 10.1016/j.urology.2008.12.075
28. Crispen PL, Breau RH, Allmer C, Lohse CM, Cheville JC, Leibovich BC, et al. Lymph node dissection at the time of radical nephrectomy for high-risk clear cell renal cell carcinoma: indications and recommendations for surgical templates. Eur Urol. (2011) 59:18–23. doi: 10.1016/j.eururo.2010.08.042
29. Abaza R, Lowe G. Feasibility and adequacy of robot-assisted lymphadenectomy for renal-cell carcinoma. J Endourol. (2011) 25:1155–9. doi: 10.1089/end.2010.0742
30. Bex A, Vermeeren L, Meinhardt W, Prevoo W, Horenblas S, Valdés Olmos RA. Intraoperative sentinel node identification and sampling in clinically node-negative renal cell carcinoma: initial experience in 20 patients. World J Urol. (2011) 29:793–9. doi: 10.1007/s00345-010-0615-6
31. Delacroix SE Jr, Chapin BF, Chen JJ, Nogueras-Gonzalez GM, Tamboli P, Matin SF, et al. Can a durable disease-free survival be achieved with surgical resection in patients with pathological node positive renal cell carcinoma? J Urol. (2011) 186:1236–41. doi: 10.1016/j.juro.2011.05.051
32. Kwon T, Song C, Hong JH, Kim CS, Ahn H. Reassessment of renal cell carcinoma lymph node staging: analysis of patterns of progression. Urology (2011) 77:373–8. doi: 10.1016/j.urology.2010.06.015
33. Capitanio U, Matloob R, Suardi N, Abdollah F, Castiglione F, Di Trapani D, et al. The extent of lymphadenectomy does affect cancer specific survival in pathologically confirmed T4 renal cell carcinoma. Urologia (2012) 79:109–15. doi: 10.5301/RU.2012.9255
34. Mehta V, Mudaliar K, Ghai R, Quek ML, Milner J, Flanigan RC, et al. Renal lymph nodes for tumor staging: appraisal of 871 nephrectomies with examination of hilar fat. Arch Pathol Lab Med. (2013) 137:1584–90. doi: 10.5858/arpa.2012-0485-OA
35. Feuerstein MA, Kent M, Bazzi WM, Bernstein M, Russo P. Analysis of lymph node dissection in patients with ≥7-cm renal tumors. World J Urol. (2014) 32:1531–6. doi: 10.1007/s00345-013-1233-x
36. Babaian KN, Kim DY, Kenney PA, Wood CG, Jr, Wong J, Sanchez C, et al. Preoperative predictors of pathological lymph node metastasis in patients with renal cell carcinoma undergoing retroperitoneal lymph node dissection. J Urol. (2015) 193:1101–7. doi: 10.1016/j.juro.2014.10.096
37. Kuusk T, De Bruijn R, Brouwer OR, De Jong J, Donswijk M, Grivas N, et al. Lymphatic drainage from renal tumors in vivo: a prospective sentinel node study using SPECT/CT imaging. J Urol. (2018) 199:1426–32. doi: 10.1016/j.juro.2017.11.112
38. Dell'Oglio P, Larcher A, Muttin F, Di Trapani E, Trevisani F, Ripa F, et al. Lymph node dissection should not be dismissed in case of localized renal cell carcinoma in the presence of larger diseases. Urol Oncol. (2017) 35:662.e9–662.e15. doi: 10.1016/j.urolonc.2017.07.010
39. Nini A, Larcher A, Cianflone F, Trevisani F, Terrone C, Volpe A, et al. The effect of anatomical location of lymph node metastases on cancer specific survival in patients with clear cell renal cell carcinoma. Front Surg. (2018) 5:26. doi: 10.3389/fsurg.2018.00026
40. Fossati N, Willemse PM, Van den Broeck T, van den Bergh RCN, Yuan CY, Briers E, et al. The benefits and harms of different extents of lymph node dissection during radical prostatectomy for prostate cancer: a systematic review. Eur Urol. (2017) 72:84–109. doi: 10.1016/j.eururo.2016.12.003
41. Cattaneo F, Motterle G, Zattoni F, Morlacco A, Dal Moro F. The role of lymph node dissection in the treatment of bladder cancer. Front Surg. (2018) 5:62. doi: 10.3389/fsurg.2018.00062
42. Hu B, Djaladat H. Lymphadenectomy for testicular, penile, upper tract urothelial and urethral cancers. Curr Opin Urol. (2015) 25:129–35. doi: 10.1097/MOU.0000000000000151
43. Capitanio U, Stewart GD, Larcher A, Ouzaid I, Akdogan B, Roscigno M, et al. Kidney Cancer Working Group of the Young Academic Urologists (YAU) Working Party of the European Association of Urology (EAU). European temporal trends in the use of lymph node dissection in patients with renal cancer. Eur J Surg Oncol. (2017) 43:2184–92. doi: 10.1016/j.ejso.2017.07.016
44. Gershman B, Thompson RH, Boorjian SA, Larcher A, Capitanio U, Montorsi F, et al. Radical nephrectomy with or without lymph node dissection for high risk nonmetastatic renal cell carcinoma: a multi-institutional analysis. J Urol. (2018) 199:1143–8. doi: 10.1016/j.juro.2017.11.114
45. Porter JR. The role of lymphadenectomy for renal cell carcinoma: are we any closer to an answer? Eur Urol. (2017) 71:568–9. doi: 10.1016/j.eururo.2016.10.028
46. Assouad J, Riquet M, Berna P, Danel C. Intrapulmonary lymph node metastasis and renal cell carcinoma. Eur J Cardiothorac Surg. (2007) 31:132–4. doi: 10.1016/j.ejcts.2006.10.025
47. Hadley DA, Stephenson RA, Samlowski WE, Dechet CB. Patterns of enlarged lymph nodes in patients with metastatic renal cell carcinoma. Urol Oncol. (2011) 29:751–5. doi: 10.1016/j.urolonc.2009.10.013
48. Saitoh H, Nakayama M, Nakamura K, Satoh T. Distant metastasis of renal adenocarcinoma in nephrectomized cases. J Urol. (1982) 127:1092–5. doi: 10.1016/S0022-5347(17)54243-3
49. Hultén L, Rosencrantz M, Seeman T, Wahlqvist L, Ahrén C. Occurrence and localization of lymph node metastases in renal carcinoma. A lymphographic and histopathological investigation in connection with nephrectomy. Scand J Urol Nephrol. (1969) 3:129–33.
50. Johnsen JA, Hellsten S. Lymphatogenous spread of renal cell carcinoma: an autopsy study. J Urol. (1997) 157:450–3. doi: 10.1097/00005392-199702000-00005
51. Sherif AM, Eriksson E, Thörn M, Vasko J, Riklund K, Ohberg L, et al. Sentinel node detection in renal cell carcinoma. A feasibility study for detection of tumour-draining lymph nodes. BJU Int. (2012) 109:1134–9. doi: 10.1111/j.1464-410X.2011.10444.x
52. Briganti A, Giannarini G, Karnes RJ, Gandaglia G, Ficarra V, Montorsi F. What evidence do we need to support the use of extended pelvic lymph node dissection in prostate cancer? Eur Urol. (2015) 67:597–8. doi: 10.1016/j.eururo.2014.09.025
53. Higgins JPT, Green S (eds,.). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. (2011). Available online at: www.handbook.cochrane.org
Keywords: landmarks, lymphadenectomy, lymph node dissection, renal cell carcinoma, templates
Citation: Campi R, Sessa F, Di Maida F, Greco I, Mari A, Takáčová T, Cocci A, Fantechi R, Lapini A, Serni S, Carini M and Minervini A (2018) Templates of Lymph Node Dissection for Renal Cell Carcinoma: A Systematic Review of the Literature. Front. Surg. 5:76. doi: 10.3389/fsurg.2018.00076
Received: 12 October 2018; Accepted: 03 December 2018;
Published: 19 December 2018.
Edited by:
Umberto Capitanio, San Raffaele Hospital (IRCCS), ItalyReviewed by:
Boris Gershman, Rhode Island Hospital, United StatesMarco Roscigno, Azienda Socio-Sanitaria Territoriale Papa Giovanni XXIII, Italy
Christian Paul Meyer, University Medical Center Hamburg-Eppendorf, Germany
Copyright © 2018 Campi, Sessa, Di Maida, Greco, Mari, Takáčová, Cocci, Fantechi, Lapini, Serni, Carini and Minervini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Riccardo Campi, cmljY2FyZG8uY2FtcGlAZ21haWwuY29t; cmljY2FyZG8uY2FtcGlAdW5pZmkuaXQ=