
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Surg. , 16 February 2018
Sec. Visceral Surgery
Volume 5 - 2018 | https://doi.org/10.3389/fsurg.2018.00008
This article is part of the Research Topic Incisional and Stomal Hernia Prevention View all 6 articles
 Núria Argudo1,2,3Miguel Pera1,2
Núria Argudo1,2,3Miguel Pera1,2 Manuel López-Cano2,4Lourdes Hernández1Juan José Sancho1,2Luis Grande1,2
Manuel López-Cano2,4Lourdes Hernández1Juan José Sancho1,2Luis Grande1,2 José Antonio Pereira1,3*
José Antonio Pereira1,3*
One of the most common complications in abdominal surgery is the incisional hernia (IH), especially when following a midline laparotomy (1). This condition demands a considerable amount of health-care resources, as it can easily require a new surgery, due to IH complication or to alleviate symptomatology, which deeply affects the patients’ quality of life (2). Despite the advances in surgical techniques and materials, the prevalence of IH remains high, although figures in published studies show great variation, reporting rates of IH between 3 and 20% (3, 4). In high-risk patients, however, the incidence rate can be as high as 40% (1, 5).
In order to avoid the complications resulting from IH, many attempts have been made in the field of IH prevention (4). Initially, most studies focused their strategy in optimizing laparotomy closure (6, 7), with variations regarding suture material and technical advances like the use of retention sutures (8), but they have all proven insufficient. In recent years, a new approach has been introduced to prevent IH, the use of prophylactic synthetic meshes. To date, there are only a few widely accepted indications for a prophylactic mesh, all reserved for special subgroups such as aortic aneurysm surgery, bariatric surgery, or stoma placement (9–11). However, more recent studies suggest that prophylactic mesh augmentation in the closure of midline laparotomy could be a useful alternative to prevent IH in high-risk patients without adding significant morbidity (12, 13).
There are many risk factors identified for IH, such as old age, smoking, previous abdominal surgery, male gender, obesity, and comorbidities such as malnutrition, abdominal aortic aneurysm, chronic renal failure, diabetes, chronic obstructive pulmonary disease (COPD), and immunosuppression (1, 14, 15). Higher BMI is one of the factors strongly associated with IH (16–18).
In a retrospective study conducted in our institution, we reported an incidence rate of IH as high as 39.9% in a series of 338 patients undergoing colorectal resection, identifying two groups of patients with higher risk: obese patients and nonobese patients with the combination of several secondary risk factors for IH (1). These results showed that it was mandatory to come up with improvement measures to secure better outcomes for our patients.
We designed an algorithm, based on this previous study, to help surgeons decide which patients should receive a prophylactic mesh (19). All patients undergoing midline laparotomy for colorectal cancer resection with BMI greater than 29 [the median BMI of patients with IH in our previous study (1)] and those with BMI lower than 29 but with two or more risk factors for IH were considered for mesh augmentation. The rest were assigned to a regular closure.
The following variables were considered as risk factors for IH: BMI (kg/m2), smoking, serum creatinine, hemoglobin, serum albumin, COPD, diabetes mellitus, immunosuppression with steroids or previous radiotherapy/chemotherapy, and previous surgery through midline laparotomy.
After implementation of the protocol, we assessed the utility and cost-effectiveness of the algorithm for mesh augmentation.
A prospective cohort study was conducted including all patients undergoing a midline laparotomy for colorectal cancer resection between January 2011 and June 2015.
All the surgeons in the team were trained in the technique of mesh augmentation. The linea alba was closed by continuous long-term absorbable suture using polydioxanone n.1 thread (PDS® Ethicon, NJ, USA), following the recommended techniques about suture length, distance between stitches and amount of tissue (6, 7). In the cases with mesh augmentation, it was placed “onlay” after subcutaneous dissection of 3 cm in both sides of the incision. We used a low-weight, wide pore, partially absorbable mesh (Ultrapro®, Ethicon, NJ, USA) fixed with a double crown of fascia staples (DFS® Autosuture, Covidien, MA, USA). Closed suction subcutaneous drains were placed in all patients with mesh.
Postoperative complications were recorded according to the Clavien–Dindo classification (20), paying particular attention to wound complications such as evisceration, seroma, and superficial or deep surgical site infection.
Total hospital cost and resource expenses during index laparotomy and subsequent related hospital admissions or IH repairs were obtained. The sample was divided into two groups depending on the application of the algorithm in the initial operation.
The diagnostic criteria for IH were as follows: clinical diagnosis made by a trained surgeon, surgery for IH during the follow-up period, and/or IH detected by the CT-scan routinely performed during the follow-up period.
During the study period, 226 patients, mean age 77 (11) years, 61% male, were included in the analysis. The mean follow-up was 31.5 months (12–60). About 160 patients were treated following the algorithm at a mean cost of 10.057€ (4.339). In 66 patients, the algorithm was not followed and the cost was 10.921€ (4.758). The incidence rate of IH dropped from 43.9 to 10% when the algorithm was followed (P = 0.0001). The subgroup analysis according to the risk factors is shown in Table 1.
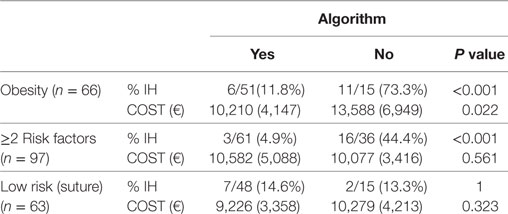
Table 1. Incidence of incisional hernia (IH) and average cost per patient in different risk groups.
Our results suggest that the use of a prophylactic mesh is an effective measure for the prevention of IH in patients undergoing a laparotomy for colorectal resection, at the expense of a significant increase of mild wound complications (seroma). We consider this disadvantage acceptable considering the great benefit it provides in the decrease of IH and the complications derived from this condition and its treatment. Our results are consistent with those previously reported in prospective randomized studies that included all types of laparotomies (3, 5).
The implementation of the algorithm to use prophylactic mesh augmentation in selected patients reduced the incidence of IH and the total hospital costs per patient. Based on our analysis, need for IH repair increases substantially total hospital costs and resource utilization.
In our opinion, not all patients benefit from the routine use of prophylactic mesh augmentation, it should be reserved for patients at increased risk to develop an IH; the rest can be safely closed following the latest recommendations on the published guidelines (6). High-risk cases can be identified with the use of an algorithm, as the one we proposed in our previous publication (19), or different approaches of scoring systems defined by other authors (16, 21).
The use of an algorithm as a therapeutic decision tool has clearly demonstrated its utility in obese patients (BMI > 29 kg/m2). In our opinion, there is enough evidence to consider that these patients should receive prophylactic mesh augmentation to prevent IH.
Indeed, if we use the HERNIAscore (HERNIAscore = 4 × L + 3 × HAL + 1 × COPD + 1 × BMI > 25) in our obese patients, we would obtain a minimum of eight points [4 × L + 4 × BMI (29 − 25)], this would be classified as Class III (high risk), resulting in an average risk of IH of 55% (16). When these patients had a prophylactic mesh placed, only 11.8% developed IH, while those who were not treated according to the algorithm presented IH is 73.3% (19).
A significant decrease in the IH rate was also achieved in patients with two or more risk factors associated with IH, other than obesity (1, 14, 15). In this group, we get from 44.4% of IH to 4.9% when the algorithm was applied correctly. In this last group, the algorithm was effective, but there clearly seem to be factors that either have not been considered or have been given an inadequate value. In fact, if we apply the HERNIAscore to these patients, a half of them would have been classified as Class II (moderate risk). This detail indicates that we need to deepen into the analysis of risk factors to elucidate more precisely those patients who benefit from the use of a prophylaxis or the group of patients in whom it is unnecessary, to avoid overtreatment using a mesh in all patients operated on colon and rectum cancer.
In conclusion, we consider that there is enough evidence to recommend the use of selective prophylactic mesh augmentation in high-risk patients, given this measure has proven to be safe and cost-effective in this population.
JP has designed the study, written the paper, compiled data, and revised final version. NA has written the paper and compiled data. LH has compiled and analyzed the data and revised the manuscript. ML-C has designed the study and revised the manuscript. MP has designed the study, compiled data, and contributed to discussion and revision of manuscript. JS has revised the manuscript and performed statistical analysis. LG has contributed to discussion and final revision of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Pereira A, Pera M, Grande L. Incidence of incisional hernia after open and laparoscopic colorectal cancer resection. Cir Esp (2013) 91:44–9. doi:10.1016/j.ciresp.2012.05.004
2. van Ramshorst GH, Eker HH, Hop WC, Jeekel J, Lange JF. Impact of incisional hernia on health-related quality of life and body image: a prospective cohort study. Am J Surg (2012) 204(2):144–50. doi:10.1016/j.amjsurg.2012.01.012
3. Caro-Tarrago A, Olona Casas C, Jimenez Salido A, Duque Guilera E, Moreno Fernandez F, Vicente Guillen V. Prevention of incisional hernia in midline laparotomy with an onlay mesh: a randomized clinical trial. World J Surg (2014) 38(9):2223–30. doi:10.1007/s00268-014-2510-6
4. Sanders DL, Kingsnorth A. The modern management of incisional hernias. BMJ (2012) 344:e2843. doi:10.1136/bmj.e2843
5. García-Ureña MÁ, López-Monclús J, Hernando LA, Montes DM, Valle de Lersundi AR, Pavón CC, et al. Randomized controlled trial of the use of a large-pore polypropylene mesh to prevent incisional hernia in colorectal surgery. Ann Surg (2015) 261(00):876–81. doi:10.1097/SLA.0000000000001116
6. Muysoms FE, Antoniou SA, Bury K, Campanelli G, Conze J, Cuccurullo D, et al. European Hernia Society guidelines on the closure of abdominal wall incisions. Hernia (2015) 19(1):1–24. doi:10.1007/s10029-014-1342-5
7. Israelsson LA, Millbourn D. Closing midline abdominal incisions. Langenbecks Arch Surg (2012) 397(8):1201–7. doi:10.1007/s00423-012-1019-4
8. Khorgami Z, Shoar S, Laghaie B, Aminian A, Hosseini Araghi N, Soroush A. Prophylactic retention sutures in midline laparotomy in high-risk patients for wound dehiscence: a randomized controlled trial. J Surg Res (2013) 180:238–43. doi:10.1016/j.jss.2012.05.012
9. Bevis PM, Windhaber RA, Lear PA, Poskitt KR, Earnshaw JJ, Mitchell DC. Randomized clinical trial of mesh versus sutured wound closure after open abdominal aortic aneurysm surgery. Br J Surg (2010) 97(10):1497–502. doi:10.1002/bjs.7137
10. Abo-Ryia M, El-Khadrawy O, Abd-Allah H. Prophylactic preperitoneal mesh placement in open bariatric surgery: a guard against incisional hernia development. Obes Surg (2013) 23(10):1571–4. doi:10.1007/s11695-013-0915-1
11. Bellón JM, López-Hervás P, Rodríguez M, García-Honduvilla N, Pascual G, Buján J. Midline abdominal wall closure: a new prophylactic mesh concept. J Am Coll Surg (2006) 203(4):490–7. doi:10.1016/j.jamcollsurg.2006.06.023
12. Argudo N, Pereira JA, Sancho JJ, Membrilla E, Pons MJ, Grande L. Prophylactic synthetic mesh can be safely used to close emergency laparotomies, even in peritonitis. Surgery (2014) 156(5):1238–44. doi:10.1016/j.surg.2014.04.035
13. Bhangu A, Fitzgerald JE, Singh P, Battersby N, Marriott P, Pinkney T. Systematic review and meta-analysis of prophylactic mesh placement for prevention of incisional hernia following midline laparotomy. Hernia (2013) 17:445–55. doi:10.1007/s10029-013-1119-2
14. Sørensen LT, Hemmingsen U, Kallehave F, Wille-Jørgensen P, Kjaergaard J, Møller LN, et al. Risk factors for tissue and wound complications in gastrointestinal surgery. Ann Surg (2005) 241(4):654–8. doi:10.1097/01.sla.0000157131.84130.12
15. Hidalgo MP, Ferrero EH, Ortiz MA, Castillo JM, Hidalgo AG. Incisional hernia in patients at risk: can it be prevented? Hernia (2011) 15:371–5. doi:10.1007/s10029-011-0794-0
16. Goodenough CJ, Ko TC, Kao LS, Nguyen MT, Holihan JL, Alawadi Z, et al. Development and validation of a risk stratification score for ventral incisional hernia after abdominal surgery: hernia expectation rates in intra-abdominal surgery (the HERNIA Project). J Am Coll Surg (2015) 220(4):405–13. doi:10.1016/j.jamcollsurg.2014.12.027
17. Itatsu K, Yokoyama Y, Sugawara G, Kubota H, Tojima Y, Kurumiya Y, et al. Incidence of and risk factors for incisional hernia after abdominal surgery. Br J Surg (2014) 101:1439–47. doi:10.1002/bjs.9600
18. Murray BW, Cipher DJ, Pham T, Anthony T. The impact of surgical site infection on the development of incisional hernia and small bowel obstruction in colorectal surgery. Am J Surg (2011) 202(5):558–60. doi:10.1016/j.amjsurg.2011.06.014
19. Argudo N, Iskra MP, Pera M, Sancho JJ, Grande L, ópez-Cano ML, et al. Un algoritmo para la colocación de malla profiláctica en pacientes de riesgo reduce la incidencia de hernia incisional tras laparotomía por cáncer colorrectal. Cir Esp (2017) 95(4):222–8. doi:10.1016/j.ciresp.2017.03.010
20. Dindo D, Demartines N, Clavien PA. Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg (2004) 240:205–13. doi:10.1097/01.sla.0000133083.54934.ae
Keywords: incisional hernia, colorectal surgery, prophylactic mesh, mesh augmentation, laparotomy
Citation: Argudo N, Pera M, López-Cano M, Hernández L, Sancho JJ, Grande L and Pereira JA (2018) Selective Mesh Augmentation to Prevent Incisional Hernias in Open Colorectal Surgery Is Safe and Cost-Effective. Front. Surg. 5:8. doi: 10.3389/fsurg.2018.00008
Received: 15 December 2017; Accepted: 30 January 2018;
Published: 16 February 2018
Edited by:
Gabriel Sandblom, Karolinska Institute (KI), SwedenReviewed by:
Nadia A. Henriksen, University of Copenhagen, DenmarkCopyright: © 2018 Argudo, Pera, López-Cano, Hernández, Sancho, Grande and Pereira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Antonio Pereira, ODY2NjRAcGFyY2Rlc2FsdXRtYXIuY2F0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.