
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Stroke, 28 March 2024
Sec. Acute Stroke and Interventional Therapies
Volume 3 - 2024 | https://doi.org/10.3389/fstro.2024.1363140
This article is part of the Research TopicTelestroke and Stroke Care Networks beyond the Comprehensive Stroke CenterView all 6 articles
 Sherita N. Chapman1,2*
Sherita N. Chapman1,2* Theandra Madu3
Theandra Madu3 Nisha Dabhi1
Nisha Dabhi1 Jackson A. Narrett4Necrisha N. Roach1
Jackson A. Narrett4Necrisha N. Roach1 Haydon M. Pitchford5
Haydon M. Pitchford5 Marcus C. Divers6
Marcus C. Divers6 Andrew M. Southerland1,7
Andrew M. Southerland1,7Background: Ambulance-based telemedicine is an innovative strategy through which transport time can be used to rapidly and accurately triage stroke patients (i.e., mobile telestroke). The acute phase of stroke is a time-sensitive emergency, and delays in care during this phase worsen outcomes. In this literature review, we analyzed studies that investigated the feasibility and reliability of ambulance based telestroke.
Methods: We followed PRISMA guidelines to perform a keyword-based search of PubMed, Web of Science, CINHAL, and Academic Search Complete databases. We reviewed references of search-identified articles to screen for additional articles. Articles for inclusion were selected according to author consensus in consideration of the studies' investigation of feasibility, reliability, or validity of ambulance-based telestroke.
Results: We identified 67 articles for secondary screening from which 19 articles were selected for full text review. The selected studies reported diverse methods of development, implementation, and assessment of ambulance-based telestroke systems. Although the methods and results varied among these studies, most concluded that the implementation of ambulance based telestroke is feasible.
Conclusion: This topical review suggests that ambulance based telestroke is a feasible method for enhanced prehospital stroke care in a variety of settings. Further prospective research is needed to assess the real-world challenges and to identify additional strategies that bolster rapid and accurate prehospital assessment of acute stroke patients.
Stroke is a leading cause of death and disability worldwide (Feigin et al., 2017; GBD 2017 Causes of Death Collaborators, 2018; Tsao et al., 2023). The most effective treatment for acute ischemic stroke is early reperfusion therapy, for which earlier treatment is associated with better recovery outcomes (Saver et al., 2016; Kim et al., 2017; Agarwal et al., 2018). Pre- and in-hospital factors including limited resources, pre-hospital diagnostic inaccuracy, geographic barriers, and lack of expertise can delay treatment and contribute to poor outcomes (National Institute of Neurological Disorders and Stroke, 2022; Chari et al., 2023; Oostema et al., 2023; Zachrison et al., 2023). The application of telemedicine to stroke care brings vascular neurology expertise to the emergency room setting (i.e., telestroke). Hospitals that access stroke expertise via telestroke have increased administration of thrombolysis to eligible patients and decreased door to treatment times, and randomized trials have shown that video-based telemedicine consultation outperformed telephone-only consultation in terms of accurate thrombolysis decision making (Meyer et al., 2008; Demaerschalk et al., 2012; Bladin and Cadilhac, 2014; Barlinn et al., 2017).
Approximately half of all patients with acute stroke present to the healthcare system via emergency medical services (EMS; Adeoye et al., 2009). Therefore, stroke recognition by EMS providers in the field is a critical early step in the stroke care continuum. Despite the development of multiple validated prehospital stroke scales, the accuracy of stroke assessment by EMS providers varies widely (Brandler et al., 2014; Pitchford et al., 2019). In addition, advancements in stroke treatment to include endovascular therapy for patients with large vessel occlusion (LVO) have presented an additional need for innovation in prehospital stroke diagnosis and triage (Smith et al., 2018; Keigher, 2020; Jauch et al., 2021). A 2009 scientific statement from the American Heart Association–American Stroke Association suggested that ambulance-based telemedicine for stroke might offer a novel solution to improving the accuracy of prehospital stroke assessment and diagnosis and the timeliness of treatment but that further research was needed (Schwamm et al., 2009). Early research in ambulance-based telestroke yielded conflicting results, for which limited technological and broadband capabilities were implicated as potential barriers (LaMonte et al., 2000, 2004; Liman et al., 2012). However, recent advances in wireless cellular technologies and mobile teleconferencing platforms have increased the capacity for implementing an ambulance-based telestroke system (Akbik et al., 2017). These findings indicate the potential of ambulance-based telestroke as an ultra-early, reliable, and valid prehospital stroke assessment method that can facilitate appropriate triage, decrease time to treatment, and improve patient outcomes.
In this context, we performed a topical literature review using a systematic search strategy to summarize the body of research on the feasibility and reliability of ambulance-based, prehospital telestroke assessment. The goals of this review were to describe previously studied ambulance-based telestroke technologies, assess the accuracy and reliability of ambulance-based telestroke clinical assessments, and identify persistent knowledge gaps and future research opportunities.
Using the query string “[telestroke or (telemed* AND stroke) or (telehealth AND stroke)] AND (prehospital OR ambulanc* OR mobile OR EMS OR emergency medical services),” we searched the MEDLINE/PubMed, Web of Science, CINAHL, and Academic Search Complete databases for articles published through February 2022. Our search followed the Preferred Reporting Items of Systematic Review and Meta-Analyses (PRISMA) methodology. Search results were curated to include only publications in English (Figure 1), manually de-duplicated, and uploaded to Rayyan, a web-based collaborative abstract screening platform.
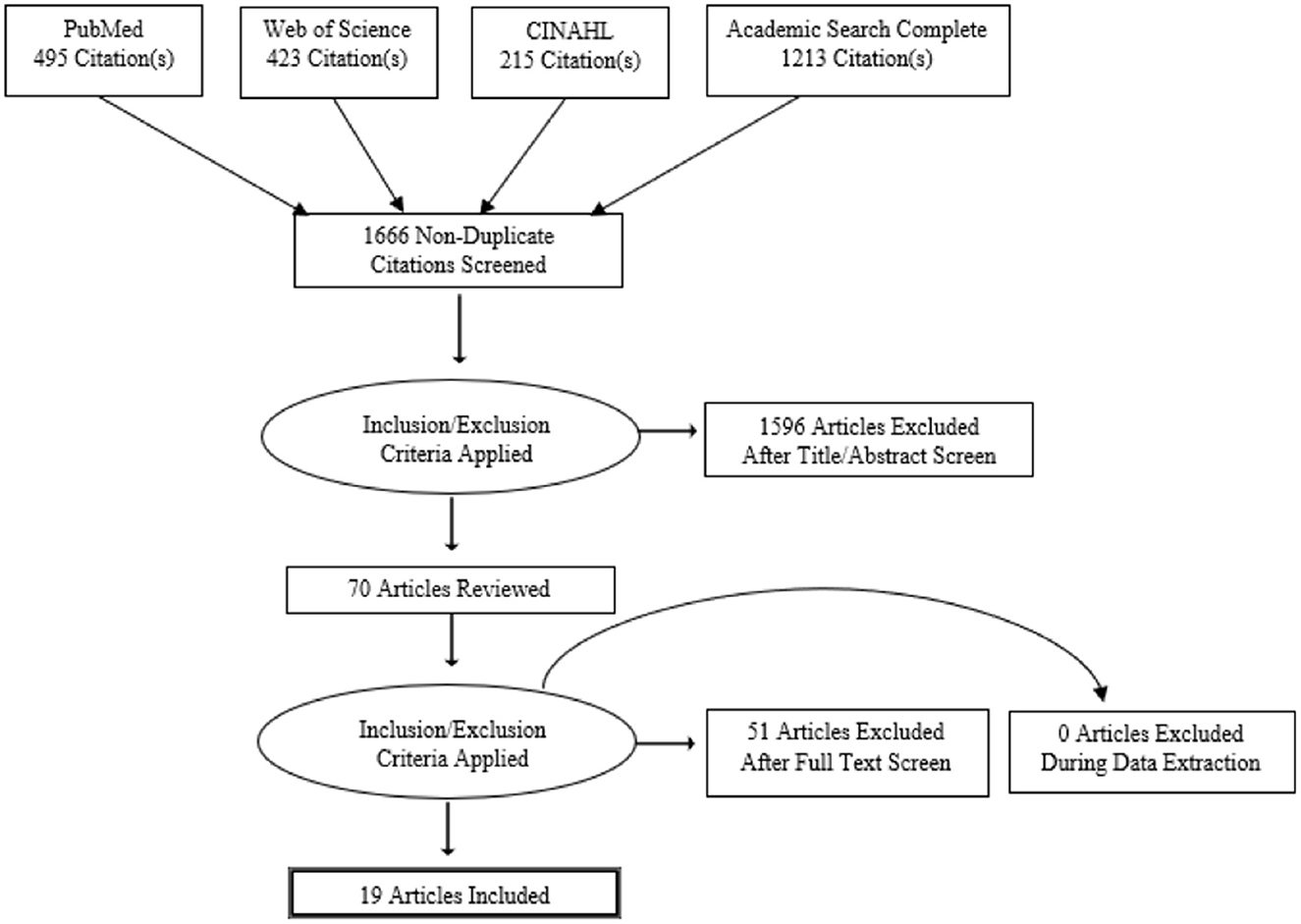
Figure 1. Article review process flow chart.
To identify candidate articles eligible for full-text screening, four of the authors of the current study (HMP, JAN, MCP, and TCM) independently applied the predetermined study inclusion and exclusion criteria (Table 1) during screening of the articles' titles and abstracts. Five of the authors (HXP, JAN, MCP, TCM, and SNC) then independently applied the inclusion and exclusion criteria during full-text review of selected articles and evaluated whether the candidate study reported quantified data regarding the feasibility, reliability, or validity of prehospital telestroke technology or assessment. Final decisions regarding an article's inclusion for review were unanimous, and consensus was achieved through collaborative review and discussion.
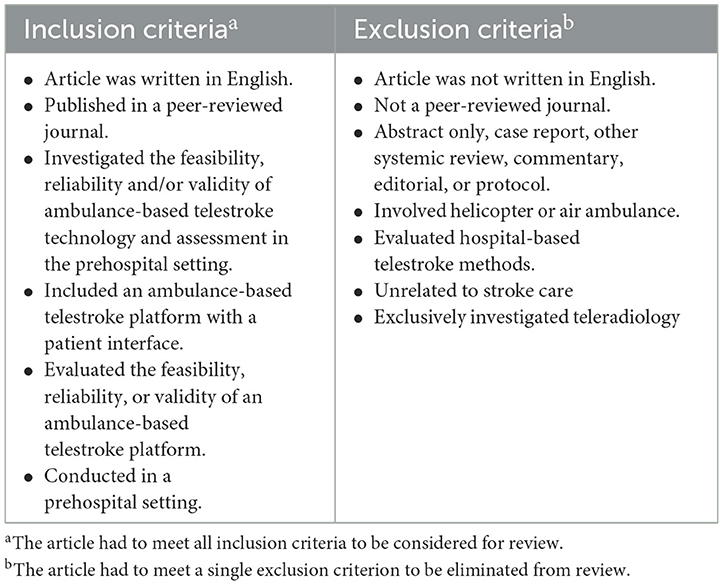
Table 1. Criteria applied to articles identified through keyword searches of databases.
Labeling of rural vs. urban vs. suburban was defined by the authors.
The PRISMA flow diagram (Figure 1) graphically displays the systematic review, selection, and inclusion of the 19 studies discussed in this review. Table 2 summarizes the characteristics of these studies (LaMonte et al., 2000, 2004; Bergrath et al., 2012; Liman et al., 2012; Van Hooff et al., 2013; Wu et al., 2014, 2017; Eadie et al., 2015; Belt et al., 2016; Chapman Smith et al., 2016, 2019; Itrat et al., 2016; Lippman et al., 2016; Valenzuela Espinoza et al., 2016; Barrett et al., 2017; Geisler et al., 2019; Johansson et al., 2019; Winter et al., 2019; Al Kasab et al., 2021). The earliest study identified was published in 2000, while 17 (89%) were published between 2010 and 2021 after the advancement of wireless broadband technology with the introduction of 4G. We identified eight studies (42%) that investigated the feasibility and/or reliability of ambulance-based telestroke techniques using only simulated patient encounters (i.e., the role of the patient was played by a healthy volunteer, medical trainee, or standardized actor). Additionally, of the studies reviewed, eight studies (42%) investigated ambulance based telestroke by evaluating only live patients being transported in ambulances. A combination of simulation and live patient encounters occurred in two studies (11%) and one study (5%) investigated technical feasibility only.
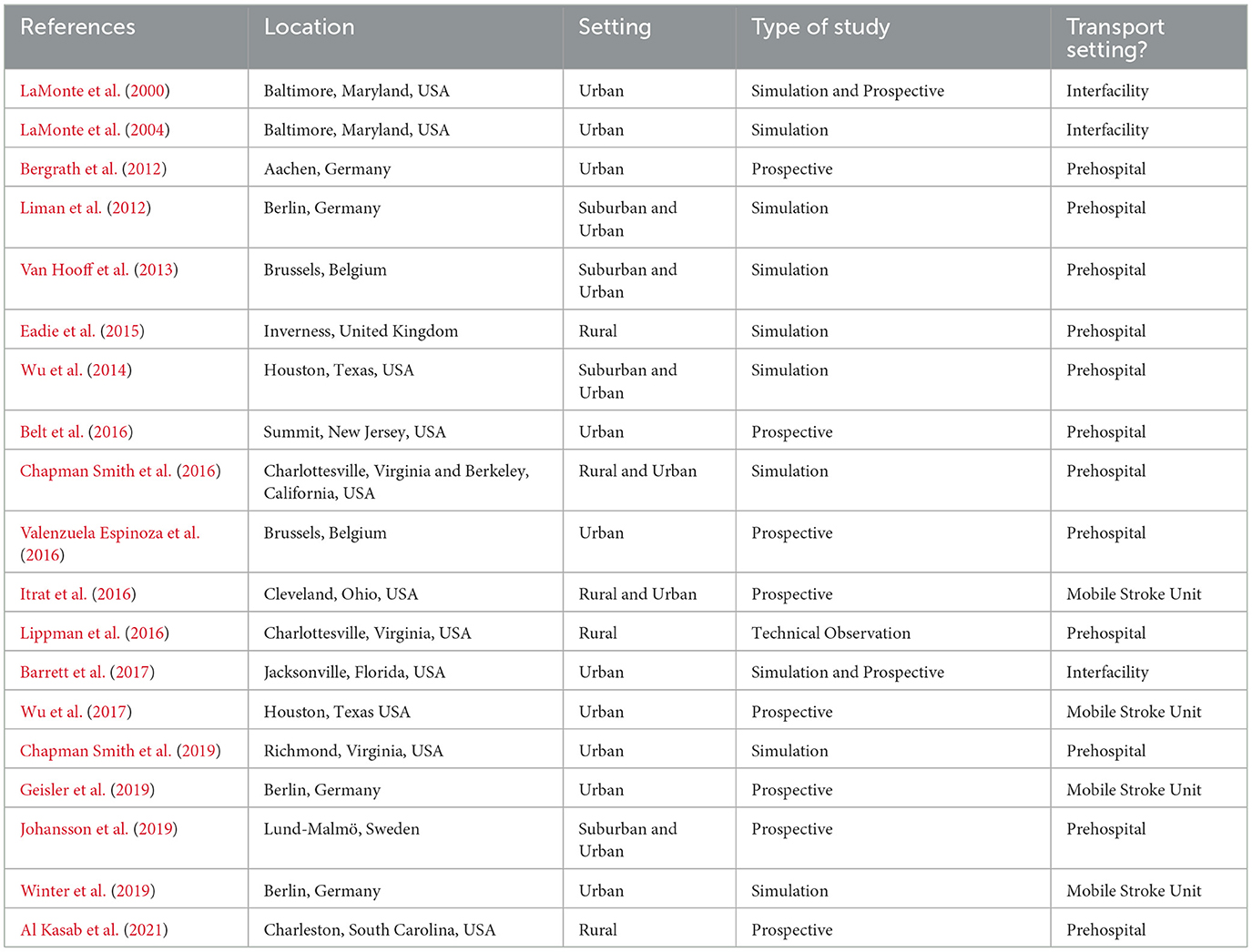
Table 2. Study characteristics included in the topical review.
The geographical settings of each of the studies are demonstrated in Table 2 with over half conducted in North America and in urban settings. While there was no variability in the mode of transport used to bring the patients to the hospital, there were differences in the setting from which patients were selected to participate.
A variety of mobile telestroke hardware, software, and networks were used and are shown in Table 3. These systems included custom telemedicine systems engineered from commercially available devices, mobile telemedicine specific hardware (prototypical or commercially available), and off –the- shelf consumer technology. A vast majority (89%) used synchronous real-time video-conferencing technology. Over half (58%) used a 4G/4G LTE wireless data network. Additional studies used a combination of networks (21%). Six studies reported the price of their telemedicine hardware with a wide range of $565–$72,000 per ambulance. Irrespective of the equipment used, each of the studies experienced some technical difficulties ranging from issues related to transmission instability, deficiencies in audio-video quality, and human error.
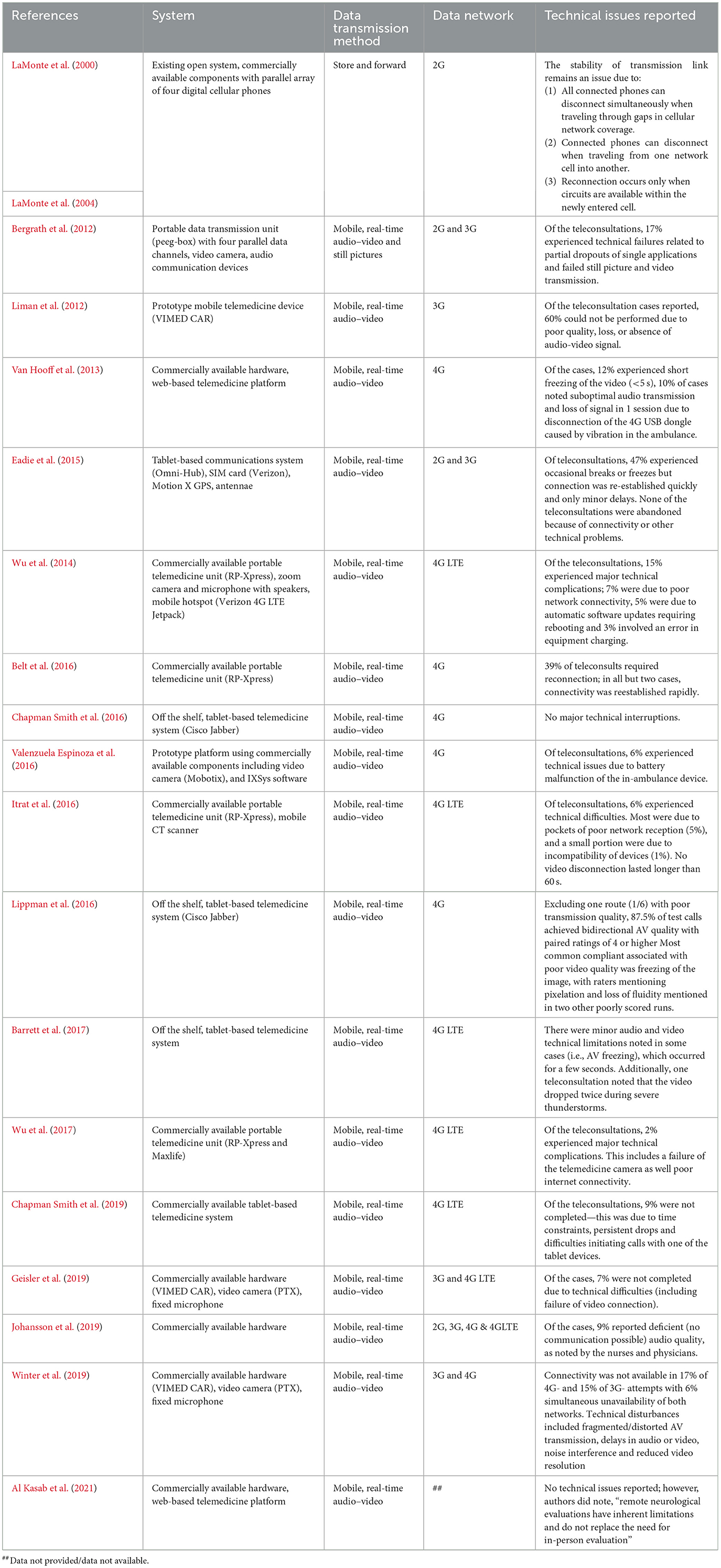
Table 3. Technology used for ambulance-based telestroke in reviewed studies.
All of the studies but one reported some metrics regarding clinical outcomes and applicability. These studies involved a variety of different assessment tools as detailed in Table 4. Fourteen studies (74%) used some version of the NIH Stroke Scale. Two studies (11%) included a complete neurologic examination via the mobile telemedicine system. Two studies (11%) utilized a novel telestroke assessment called the Unassisted TeleStroke Scale (UTSS). The training level and role of the personnel that functioned as either telepresenters (i.e., an individual present with the patient who operate the telehealth equipment and assist the remote physician with the examination) or remote telestroke providers varied widely. An EMS provider served in the role of ambulance-based telepresenter in most of the studies (74%). One study using the UTSS (5%) required no assistance from a telepresenter. The majority of studies (89%) utilized a stroke physician or an advanced practice provider as the remote examiner. In four studies (21%), stroke physicians were supported by either a neuroradiologist or a technologist.
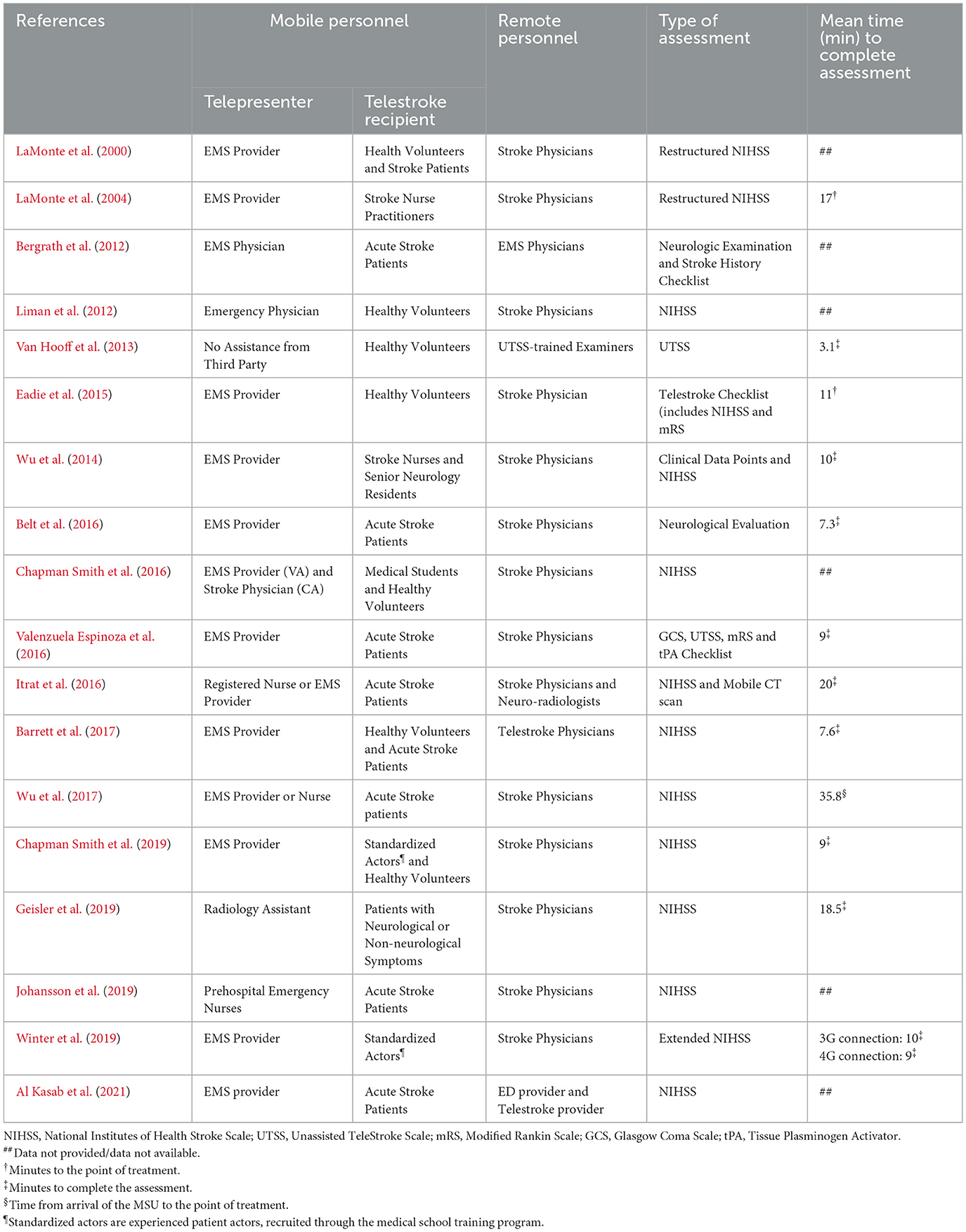
Table 4. Clinical features of reviewed studies.
Ten studies evaluated the use of a mobile telestroke platform during clinical simulations for a total of 306 encounters. One of the studies conducted clinical simulations within a mobile stroke unit and compared the technical parameters of 4G and 3G connectivity. Over half of the studies (70%) were able to perform >80% of their mobile teleconferencing encounters without prohibitive technical interruptions. There was variability in the evaluation of reliability of neurologic assessments, including agreement in the clinical diagnosis and treatment decisions as demonstrated in Table 5. Most of the studies (70%) reported the reliability of the mobile teleconferencing clinical assessment using either interrater reliability or intraclass correlation. Three studies revealed moderate to excellent reliability. Two studies evaluated the agreement in treatment decisions using different assessment techniques. Five of the studies conducted surveys with healthcare providers concerning satisfaction, AV quality, efficacy of providing valuable information, usability, and acceptability of technology with favorable responses.
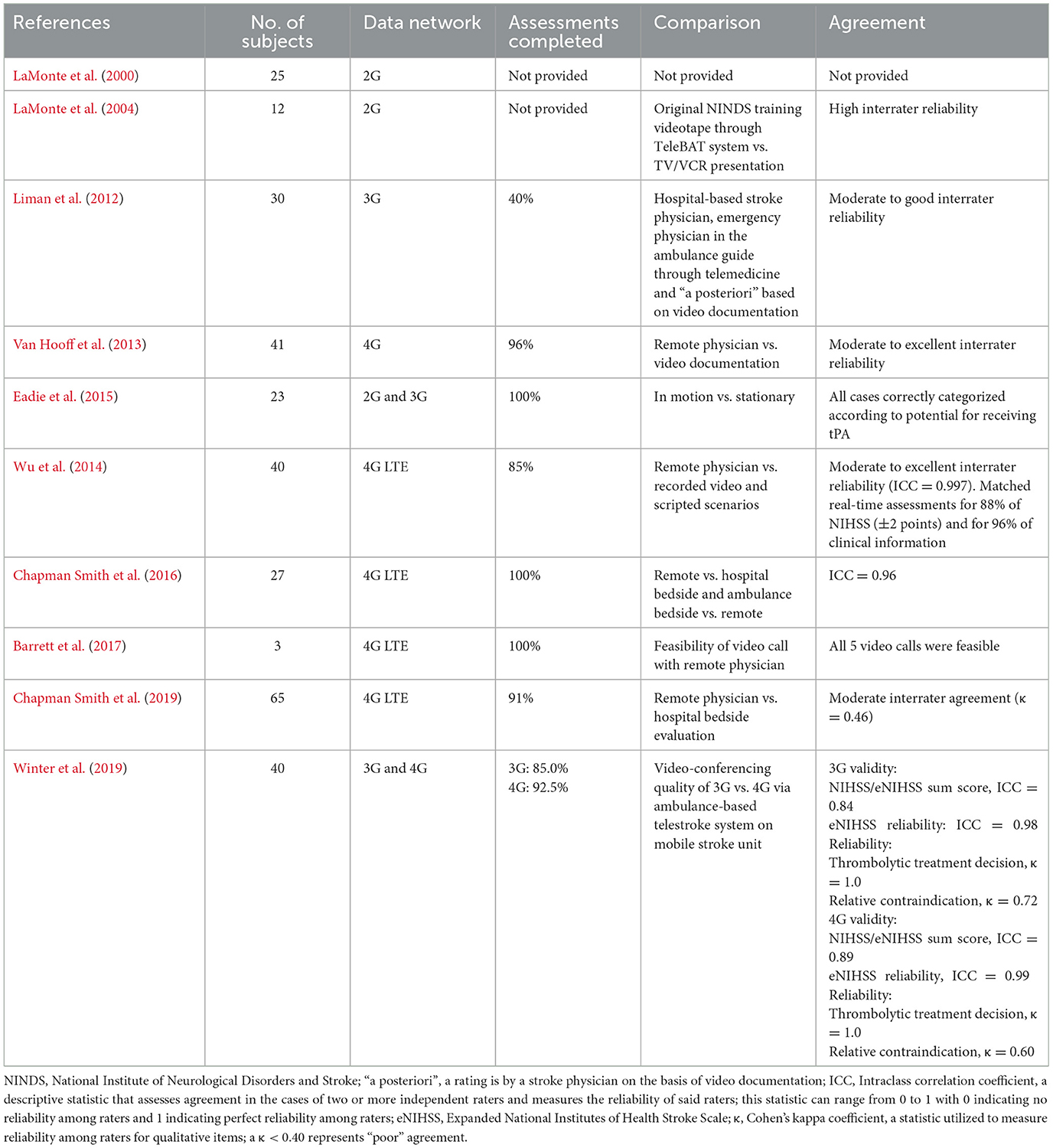
Table 5. Reviewed studies involving clinical simulations.
Seven studies evaluated the use of a mobile telestroke platform in a prospective feasibility study with actual patients for a total of 194 encounters. All of the studies except one reported the percentage of mobile teleconferencing encounters without prohibitive technical interruptions with all noting >80% of their encounters completed. There were variations in the measured outcomes of each of the studies noted in Table 6. Results mainly focused on the clinical value of conducting an ambulance-based telestroke assessment, feasibility of assessment, and accuracy of the prehospital diagnosis. Two studies demonstrated a reduction in door-to-needle times when compared with standard bedside assessments.
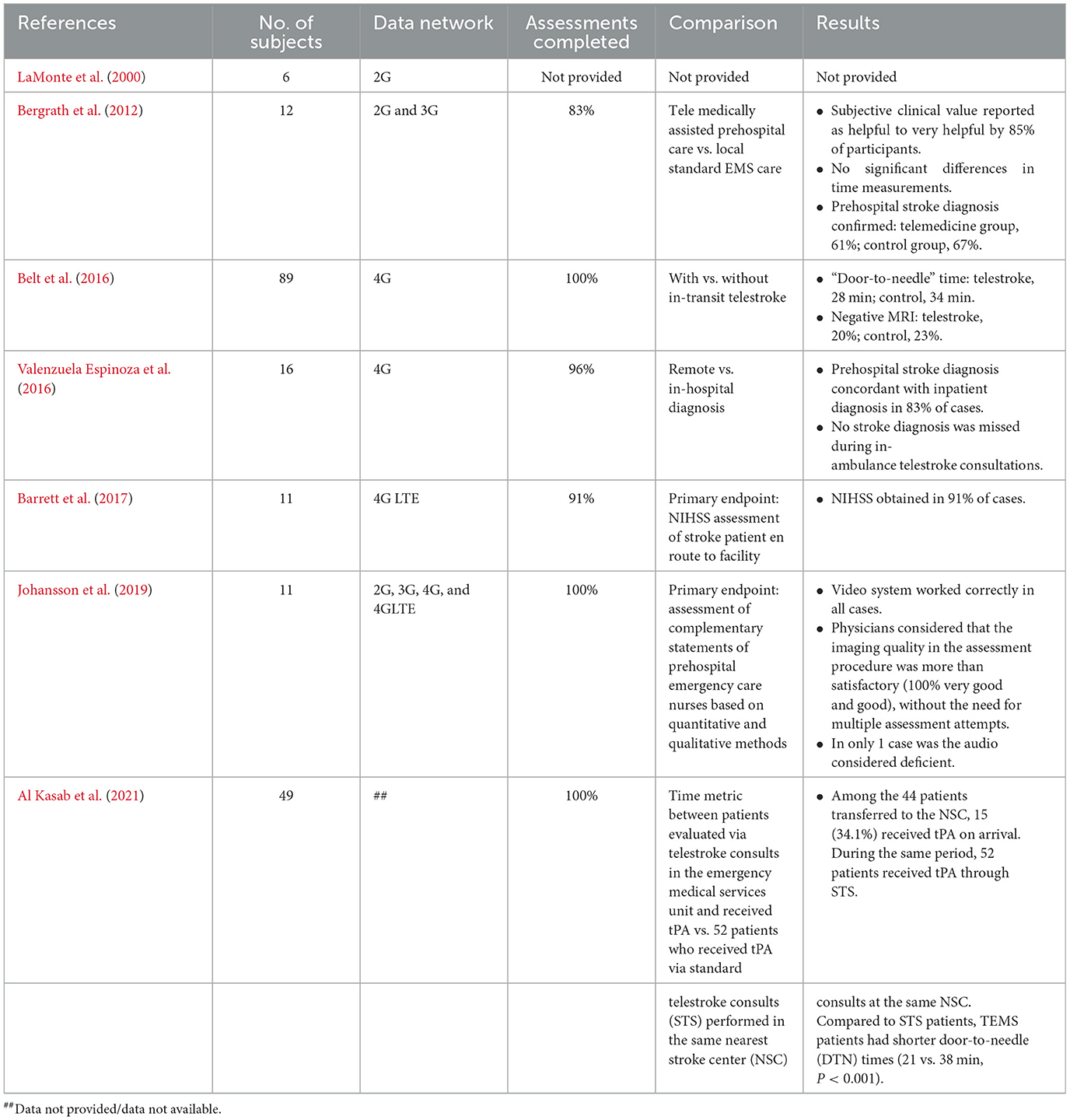
Table 6. Reviewed studies involving live clinical testing on patients.
Three studies have evaluated the use of mobile ambulance-based telestroke in mobile stroke units prospectively (Table 7). There were a total of 377 encounters with all studies reporting a successful assessment completion rate of at least 85%. Two of the studies compared the remote telemedicine evaluation with an on-board bedside evaluation. One compared remote telemedicine evaluation with the emergency room bedside evaluation. Two of the studies evaluated the reliability of the neurological assessment with a high interrater reliability and an NIHSS intraclass correlation of at least 0.87. One study noted a reduction in onset-to-needle time of 26 min compared to control.
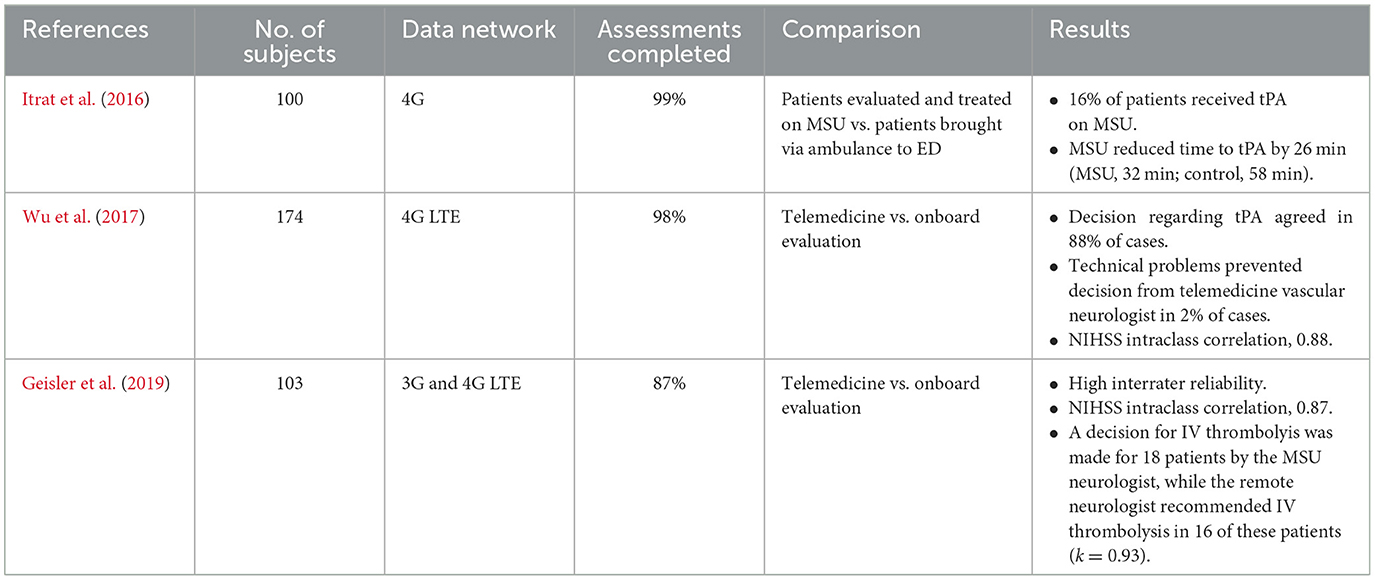
Table 7. Reviewed articles involving live prehospital telestroke on mobile stroke unit (MSU).
This literature review suggests that ambulance-based telestroke is a feasible and reliable method for prehospital stroke assessment. Since the early 2000's, the technical feasibility of conducting real-time, mobile telemedicine in a moving ambulance has largely improved due to refinements in mobile technology and the wider availability of high-speed mobile broadband. Nevertheless, advances in acute stroke treatments have added complexity to stroke systems of care and incurred an even greater requirement on the accuracy of prehospital stroke diagnosis to inform triage decisions, particularly for patients with large vessel occlusions. However, there remains a great deal of variability in the practice and usability of ambulance-based telestroke given the challenges of integrating in modern emergency stroke workflows.
Here we described the current literature regarding the accuracy and reliability of ambulance-based telestroke technologies and clinical assessments. Despite the evidence supporting the feasibility and reliability, the medical literature is still lacking in several areas regarding the use of such novel technology in the prehospital arena. One area is related to the significant amount of variability within the studies evaluated. There were variations in the type of equipment, stroke assessment, clinical evaluator, methodology, and outcomes assessed. While the heterogeneity among studies makes comparisons challenging, this variability reflects the challenges of real-world prehospital clinical practice.
Despite these significant variations among the studies in this review, the feasibility, reliability, and validity data remain favorable as technology has improved. In a recent cluster randomized controlled trial comparing the diagnostic accuracy of prehospital telestroke with that of in-person emergency department (ED) assessment, telestroke was 100% accurate in predicting reperfusion candidates compared with preimaging ED examination. Additionally, telestroke was found to be 80 and 88.6% accurate in predicting intervention with IV thrombolytic and endovascular treatment, respectively, suggesting that telestroke can be an effective option to reduce delays to definitive stroke care (Scott et al., 2022).
In addition, more than half of the studies reviewed were conducted within a simulated environment. These studies opted for this style of investigation for several reasons. The condition of real patients can change during transport, making it impossible to define a definitive stroke scale score with which to compare telestroke assessments. Simulation offered these investigators the standardization needed to draw conclusions about the technology and assessments used in these studies. However, the use of standardized patients creates gaps in knowledge of the performance of a telestroke system. For example, the simulated scenarios tested may not have captured the variety of patient presentations that stroke providers encounter in clinical practice. Also, the use of standardized patients may have facilitated an easier exam for the providers. Some studies used medical students, nurses, or neurology residents as actors. A standardized patient that has a sophisticated understanding of stroke presentations might bias toward easier assessments.
Furthermore, an important factor that may impact the feasibility, reliability, and accuracy of stroke assessments is transport setting (i.e., interfacility and prehospital). Specifically, telestroke in a prehospital setting may have a higher rate of stroke mimics compared to those undergoing interhospital transfer, where patients often have screened positive for stroke and undergo transport to a comprehensive stroke center. Notably, in our review, the transport setting in a majority of studies was pre-hospital, where the need for telestroke as a triage tool is likely greater. However, telestroke use in interfacility transfer can be useful to expedite in -hospital workflows to reduce further delays to treatment.
Regarding technical feasibility of ambulance-based telemedicine, the majority of the barriers encountered were related to modifiable human and operational errors (e.g., unscheduled software updates, unchanged batteries/devices, and attempted use of incompatible equipment). Examples included a case in which an automatic software update required rebooting of the device, while another case was infeasible due to the Wi-Fi hotspot being out of battery after being charged with an improper charger. Although these instances prevented the completion of the prehospital assessment, they represent modifiable factors that can be addressed easily with a more standardized and streamlined approach to integration and prehospital workflow.
Suffice it to say, human factors and ease-of-use play a significant role in the sustainability of telemedicine systems in the healthcare environment, particularly in time sensitive scenarios such as acute stroke (Rogers et al., 2021). Healthcare systems seeking to implement prehospital telemedicine may need to rely on technical support from established telemedicine programs to effectively process and interpret mobile telestroke assessments in real time. Alternatively, as used in the emergency room setting during times of technical failure, mobile phone devices could be used in cases of telemedicine failure. However, further investigation is required to understand best practices for these mobile devices in this setting.
An in depth understanding of wireless network capabilities within a particular catchment region is also crucial to the success of ambulance-based telestroke services. While the potential for real time ambulance-based telemedicine has been made possible by the advancement of cellular networks, mobile broadband remains fragmented in many parts of the world. Clearly, the sustainability of ambulance-based telemedicine programs will require partnering with local telecommunications providers and government officials to strengthen regional broadband capability, particularly for rural and underserved areas.
Integrating ambulance-based telestroke capability for healthcare systems will require additional cost-utility analysis. Only a few studies commented on the cost of outfitting an ambulance with a telemedicine system, ranging widely depending on the type of technology and human resources employed within each system. Hopefully, the ongoing advancement of mobile health technology and access will continue to provide cheaper options for performing ambulance telemedicine encounters, including the use of commercially available platforms incorporating mobile phones and tablet-based devices. Ambulance-based telemedicine has also enhanced the cost-effectiveness of implementing CT-capable mobile stroke units as well, becoming an essential component of the prehospital clinical assessment needed to avoid overextending costly-human resources on these units.
We acknowledgethat our study has several limitations. Individual patient data and subgroup analysis were not possible, as a study-level analysis was performed. Furthermore, as mentioned, the included studies were heterogenous in type of equipment, stroke assessment, clinical evaluator, methodology, and outcomes assessed, making full interpretation of the available data challenging. Additionally, since the time of search for this review, additional studies have evaluated the feasibility and reliability of ambulance-based telestroke that were not included in this review. However, overall, these studies do endorse the feasibility and reliability of telestroke, finding that telestroke does allow for correct stroke and large vessel occlusion identification in the majority of cases (https://pubmed.ncbi.nlm.nih.gov/37941577/, https://pubmed.ncbi.nlm.nih.gov/36240100/, https://pubmed.ncbi.nlm.nih.gov/35720454/, https://pubmed.ncbi.nlm.nih.gov/33690029/). A majority of these more recent studies also focus on reviewing telestroke in the context of improving times to reperfusion in the setting of acute stroke interventions (i.e., IV thrombolytics and endovascular treatment).
This topical review using a systematic search strategy suggests that ambulance-based telestroke is a feasible strategy to provide reliable and accurate stroke assessment to patients in the prehospital and interfacility settings. Further prospective research is needed to further assess cost-effectiveness and utility for prehospital stroke triage, particularly for endovascular therapy, and confirm generalizability of implementation across diverse geographic regions and prehospital systems of care.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
SC: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Supervision, Writing—original draft, Writing—review & editing. TM: Data curation, Writing—original draft, Writing—review & editing. ND: Data curation, Writing—original draft, Writing—review & editing. JN: Data curation, Formal analysis, Writing—original draft, Writing—review & editing. NR: Data curation, Writing—original draft, Writing—review & editing. HP: Data curation, Writing—original draft, Writing—review & editing. MD: Data curation, Writing—original draft, Writing—review & editing. AS: Conceptualization, Supervision, Writing—original draft, Writing—review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
HP was employed by All-In-Solutions, LLC. MD was employed by Virginia Health Information. SC and AS disclose Patent no. US 10,846,370 B2, Techniques Facilitating Mobile Telemedicine For Stroke Patients. AS discloses U.S. Provisional Patent Application No. 62/620,096, System and Method for Automated Stroke of Neurological Deficits, receives research support from the American Heart Association regarding augmented video-based stroke sign detection, and performs paid expert legal consultation in acute stroke cases.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adeoye, O., Lindsell, C., Broderick, J., Alwell, K., Jauch, E., Moomaw, C. J., et al. (2009). Emergency medical services use by stroke patients: a population-based study. Am. J. Emerg. Med. 27, 141–145. doi: 10.1016/j.ajem.2008.02.004
Agarwal, S., Bivard, A., Warburton, E., Parsons, M., and Levi, C. (2018). Collateral response modulates the time-penumbra relationship in proximal arterial occlusions. Neurology 90, e316–e322. doi: 10.1212/WNL.0000000000004858
Akbik, F., Hirsch, J. A., Chandra, R. V., Frei, D., Patel, A. B., Rabinov, J. D., et al. (2017). Telestroke-the promise and the challenge. Part one: growth and current practice. J. NeuroInterventional. Surg. 9, 357–360. doi: 10.1136/neurintsurg-2016-012291
Al Kasab, S., Almallouhi, E., Grant, C., Hewitt, D., Hewitt, J., Baki, M., et al. (2021). Telestroke consultation in the emergency medical services unit: a novel approach to improve thrombolysis times. J. Stroke Cerebrovasc. Dis. 30:105710. doi: 10.1016/j.jstrokecerebrovasdis.2021.105710
Barlinn, J., Gerber, J., Barlinn, K., Pallesen, L. P., Siepmann, T., Zerna, C., et al. (2017). Acute endovascular treatment delivery to ischemic stroke patients transferred within a telestroke network: a retrospective observational study. Int. J. Stroke 12, 502–509. doi: 10.1177/1747493016681018
Barrett, K. M., Pizzi, M. A., Kesari, V., TerKonda, S. P., Mauricio, E. A., Silvers, S. M., et al. (2017). Ambulance-based assessment of NIH Stroke Scale with telemedicine: a feasibility pilot study. J. Telemed. Telecare 23, 476–483. doi: 10.1177/1357633X16648490
Belt, G. H., Felberg, R. A., Rubin, J., and Halperin, J. J. (2016). In-transit telemedicine speeds ischemic stroke treatment. Stroke 47, 2413–2415. doi: 10.1161/STROKEAHA.116.014270
Bergrath, S., Reich, A., Rossaint, R., Rörtgen, D., Gerber, J., Fischermann, H., et al. (2012). Feasibility of prehospital teleconsultation in acute stroke—a pilot study in clinical routine. PLoS ONE 7:e36796. doi: 10.1371/journal.pone.0036796
Bladin, C. F., and Cadilhac, D. A. (2014). Effect of telestroke on emergent stroke care and stroke outcomes. Stroke 45, 1876–1880. doi: 10.1161/STROKEAHA.114.003825
Brandler, E. S., Sharma, M., Sinert, R. H., and Levine, S. R. (2014). Prehospital stroke scales in urban environments. Neurology 82, 2241–2249. doi: 10.1212/WNL.0000000000000523
Chapman Smith, S. N., Brown, P. C., Waits, K. H., Wong, J. S., Bhatti, M. S., Toqeer, Q., et al. (2019). Development and evaluation of a user-centered mobile telestroke platform. Telemed. J. E Health 25, 638–648. doi: 10.1089/tmj.2018.0044
Chapman Smith, S. N., Govindarajan, P., Padrick, M. M., Lippman, J. M., McMurry, T. L., Resler, B. L., et al. (2016). A low-cost, tablet-based option for prehospital neurologic assessment. Neurology 87, 19–26. doi: 10.1212/WNL.0000000000002799
Chari, S. V., Cui, E. R., Fehl, H. E., Fernandez, A. R., Brice, J. H., Patel, M. D., et al. (2023). Community socioeconomic and urban-rural differences in emergency medical services times for suspected stroke in North Carolina. Am. J. Emerg. Med. 63, 120–126. doi: 10.1016/j.ajem.2022.10.039
Demaerschalk, B. M., Raman, R., Ernstrom, K., and Meyer, B. C. (2012). Efficacy of telemedicine for stroke: pooled analysis of the stroke team remote evaluation using a digital observation camera (STRokE DOC) and STRokE DOC Arizona Telestroke Trials. Telemed. e-Health 18, 230–237. doi: 10.1089/tmj.2011.0116
Eadie, L., Regan, L., Mort, A., Shannon, H., Walker, J., MacAden, A., et al. (2015). Telestroke assessment on the move. Stroke 46, e38–e40. doi: 10.1161/STROKEAHA.114.007475
Feigin, V. L., Abajobir, A. A., Abate, K. H., Abd-Allah, F., Abdulle, A. M., Abera, S. F., et al. (2017). Global, regional, and national burden of neurological disorders during 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 16, 877–897. doi: 10.1016/S1474-4422(17)30299-5
GBD 2017 Causes of Death Collaborators (2018). Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392, 1736–1788. doi: 10.1016/S0140-6736(18)32203-7
Geisler, F., Kunz, A., Winter, B., Rozanski, M., Waldschmidt, C., Weber, J. E., et al. (2019). Telemedicine in prehospital acute stroke care. J. Am. Heart Assoc. 8:e011729. doi: 10.1161/JAHA.118.011729
Itrat, A., Taqui, A., Cerejo, R., Briggs, F., Cho, S. M., Organek, N., et al. (2016). Telemedicine in prehospital stroke evaluation and thrombolysis: taking stroke treatment to the doorstep. J. Am. Med. Assoc. Neurol. 73, 162–168. doi: 10.1001/jamaneurol.2015.3849
Jauch, E. C., Schwamm, L. H., Panagos, P. D., Barbazzeni, J., Dickson, R., and Dunne, R. (2021). Recommendations for regional stroke destination plans in rural, suburban, and urban communities from the prehospital stroke system of care consensus conference: a consensus statement from the American Academy of Neurology, American Heart Association/American Stroke Association, American Society of Neuroradiology, National Association of EMS Physicians, National Association of State EMS Officials, Society of NeuroInterventional Surgery, and Society of Vascular and Interventional Neurology: Endorsed by the Neurocritical Care Society. Stroke 52, e133–e152. doi: 10.1161/STROKEAHA.120.033228
Johansson, A., Esbjörnsson, M., Nordqvist, P., Wiinberg, S., Andersson, R., Ivarsson, B., et al. (2019). Technical feasibility and ambulance nurses' view of a digital telemedicine system in pre-hospital stroke care—a pilot study. Int. Emerg. Nurs. 44, 35–40. doi: 10.1016/j.ienj.2019.03.008
Keigher, K. M. (2020). Large vessel occlusion in the acute stroke patient: identification, treatment, and management. Crit. Care Nurs. Clin. North Am. 32, 21–36. doi: 10.1016/j.cnc.2019.11.007
Kim, J. T., Fonarow, G. C., Smith, E. E., Reeves, M. J., Navalkele, D. D., Grotta, J. C., et al. (2017). Treatment with tissue plasminogen activator in the golden hour and the shape of the 4.5-hour time-benefit curve in the National United States get with the guidelines-stroke population. Circulation 135, 128–139. doi: 10.1161/CIRCULATIONAHA.116.023336
LaMonte, M. P., Cullen, J., Gagliano, D. M., Gunawardane, R., Hu, P., Mackenzie, C., et al. (2000). TeleBAT: mobile telemedicine for the brain attack team. J. Stroke Cerebrovasc. Dis. 9, 128–135. doi: 10.1053/jscd.2000.5867
LaMonte, M. P., Xiao, Y., Hu, P. F., Gagliano, D. M., Bahouth, M. N., Gunawardane, R. D., et al. (2004). Shortening time to stroke treatment using ambulance telemedicine: TeleBAT. J. Stroke Cerebrovasc. Dis. 13, 148–154. doi: 10.1016/j.jstrokecerebrovasdis.2004.03.004
Liman, T. G., Winter, B., Waldschmidt, C., Zerbe, N., Hufnagl, P., Audebert, H. J., et al. (2012). Telestroke ambulances in prehospital stroke management. Stroke 43, 2086–2090. doi: 10.1161/STROKEAHA.112.657270
Lippman, J. M., Smith, S. N. C., McMurry, T. L., Sutton, Z. G., Gunnell, B. S., Cote, J., et al. (2016). Mobile telestroke during ambulance transport is feasible in a rural EMS setting: the iTREAT study. Telemed. J. E Health 22, 507–513. doi: 10.1089/tmj.2015.0155
Meyer, B. C., Raman, R., Hemmen, T., Obler, R., Zivin, J. A., Rao, R., et al. (2008). Efficacy of site-independent telemedicine in the STRokE DOC trial: a randomised, blinded, prospective study. Lancet Neurol. 7, 787–795. doi: 10.1016/S1474-4422(08)70171-6
National Institute of Neurological Disorders and Stroke (2022). Brain Attack Coalition Symposium: Inequities in Access and Delivery of Acute Stroke Care. Available online at: https://www.ninds.nih.gov/news-events/events/brain-attack-coalition-symposium-inequities-access-and-delivery-acute-stroke-care (accessed December 29, 2023).
Oostema, J. A., Nickles, A., Luo, Z., and Reeves, M. J. (2023). Emergency medical services stroke care performance variability in michigan: analysis of a statewide linked stroke registry. J. Am. Heart Assoc. 12:e026834. doi: 10.1161/JAHA.122.026834
Pitchford, H. M., Divers, M. C., Chapman, S. N., and Southerland, A. M. (2019). Prehospital telemedicine and EMS integration. Telemedicine 16, 281–305. doi: 10.1007/978-3-030-11569-2_16
Rogers, H., Madathil, K. C., Joseph, A., Holmstedt, C., Qanungo, S., McNeese, N., et al. (2021). An exploratory study investigating the barriers, facilitators, and demands affecting caregivers in a telemedicine integrated ambulance-based setting for stroke care. Appl. Ergon. 97:103537. doi: 10.1016/j.apergo.2021.103537
Saver, J. L., Goyal, M., van der Lugt, A., Menon, B. K., Majoie, C. B. L. M., Dippel, D. W., et al. (2016). Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. Cerebrovasc. Dis. J. Am. Med. Assoc. Netw. 2016:13647. doi: 10.1001/jama.2016.13647
Schwamm, L. H., Holloway, R. G., Amarenco, P., Audebert, H. J., Bakas, T., and Chumbler, N. R. (2009). A review of the evidence for the use of telemedicine within stroke systems of care. Stroke 40, 2616–2634. doi: 10.1161/STROKEAHA.109.192360
Scott, I. M., Manoczki, C., Swain, A. H., Ranjan, A., McGovern, M. G., Shyrell Tyson, A. L., et al. (2022). Prehospital telestroke vs. paramedic scores to accurately identify stroke reperfusion candidates. Neurology 99:201104. doi: 10.1212/WNL.0000000000201104
Smith, E. E., Kent, D. M., Bulsara, K. R., Leung, L. Y., Lichtman, J. H., Reeves, M. J., et al. (2018). Accuracy of prediction instruments for diagnosing large vessel occlusion in individuals with suspected stroke: a systematic review for the 2018 guidelines for the early management of patients with acute ischemic stroke. Stroke 49, e111–e122. doi: 10.1161/STR.0000000000000160
Tsao, C. W., Aday, A. W., Almarzooq, Z. I., Anderson, C. A. M., Arora, P., Avery, C. L., et al. (2023). Heart disease and stroke statistics-2023 update: a report from the American Heart Association. Circulation 147, e93–e621. doi: 10.1161/CIR.0000000000001123
Valenzuela Espinoza, A., Van Hooff, R. J., De Smedt, A., Moens, M., Yperzeele, L., Nieboer, K., et al. (2016). Development and pilot testing of 24/7 in-ambulance telemedicine for acute stroke: prehospital stroke study at the Universitair Ziekenhuis Brussel-Project. Cerebrovasc. Dis. 42, 15–22. doi: 10.1159/000444175
Van Hooff, R. J., Cambron, M., Van Dyck, R., De Smedt, A., Moens, M., Espinoza, A. V., et al. (2013). Prehospital unassisted assessment of stroke severity using telemedicine. Stroke 44, 2907–2909. doi: 10.1161/STROKEAHA.113.002079
Winter, B., Wendt, M., Waldschmidt, C., Rozanski, M., Kunz, A., Geisler, F., et al. (2019). 4G versus 3G-enabled telemedicine in prehospital acute stroke care. Int. J. Stroke 14, 620–629. doi: 10.1177/1747493019830303
Wu, T. C., Nguyen, C., Ankrom, C., Yang, J., Persse, D., Vahidy, F., et al. (2014). Prehospital utility of rapid stroke evaluation using in-ambulance telemedicine. Stroke 45, 2342–2347. doi: 10.1161/STROKEAHA.114.005193
Wu, T. C., Parker, S. A., Jagolino, A., Yamal, J. M., Bowry, R., Thomas, A., et al. (2017). Telemedicine can replace the neurologist on a mobile stroke unit. Stroke 48, 493–496. doi: 10.1161/STROKEAHA.116.015363
Zachrison, K. S., Nielsen, V. M., de la Ossa, N. P., Madsen, T. E., Cash, R. E., Crowe, R. P., et al. (2023). Prehospital stroke care part 1: emergency medical services and the stroke systems of care. Stroke 54, 1138–1147. doi: 10.1161/STROKEAHA.122.039586
The authors of this review agreed upon the following definitions to be used in the reporting of the data found in the included articles. These definitions were used to categorize studies and analyze data.
Ambulance-based telestroke: any system designed to allow remote personnel with stroke expertise to examine a patient in an ambulance using audio, video, photo, or other means of digital information transfer.
Ambulance-based telestroke technical feasibility study: A study that investigates the likelihood that the technological solutions employed by an experimental ambulance-based telestroke system could support use during real-world emergencies.
Ambulance-based telestroke simulation study: A study that makes use of actors to play the role of stroke patients to investigate the feasibility of an ambulance-based telestroke system.
Ambulance-based telestroke assessment reliability/validity study: A study that investigates the results of telestroke assessment by measuring agreement between raters (reliability) or agreement with a gold-standard method of stroke assessment
Ambulance-based telestroke observational study: A study that employs telestroke in an emergency medical system and gathers data from telestroke encounters.
Mobile stroke unit: an ambulance that furnishes services to diagnose, evaluate, and/or treat symptoms of an acute stroke (CITE).
Stroke Physician: expertise in stroke.
EMS provider: An individual trained specifically in the prehospital treatment and transport of patients, level of credentialing and expertise is variable.
Prehospital ambulance: a vehicle that responds to emergency calls in the community and transports patients to the hospital prior to tPA treatment decisions being made.
MSU: ambulances that respond to emergency calls however they are designed to obtain CT images and deliver IV thrombolysis in the field.
Interfacility ambulance: An ambulances that does not respond to emergency calls in the community but rather transports patients from one healthcare facility to another.
Keywords: stroke, telemedicine, telestroke, mobile health, emergency medical services, prehospital
Citation: Chapman SN, Madu T, Dabhi N, Narrett JA, Roach NN, Pitchford HM, Divers MC and Southerland AM (2024) A topical review of the feasibility and reliability of ambulance-based telestroke. Front. Stroke 3:1363140. doi: 10.3389/fstro.2024.1363140
Received: 29 December 2023; Accepted: 19 February 2024;
Published: 28 March 2024.
Edited by:
Imama Ali Naqvi, Columbia University, United StatesReviewed by:
Ritvij Bowry, University of Texas Health Science Center at Houston, United StatesCopyright © 2024 Chapman, Madu, Dabhi, Narrett, Roach, Pitchford, Divers and Southerland. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sherita N. Chapman, c2MyYmRAdXZhaGVhbHRoLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.