 Svein Barene
Svein Barene Patrick Foss Johansen
Patrick Foss Johansen Hege Eikeland Tjomsland2
Hege Eikeland Tjomsland2 Miranda Thurston
Miranda Thurston
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sports Act. Living , 13 January 2025
Sec. Physical Education and Pedagogy
Volume 6 - 2024 | https://doi.org/10.3389/fspor.2024.1460373
This article is part of the Research Topic Schools as an arena for health-promoting physical activity View all 18 articles
Introduction: Physical inactivity is a global health challenge, exacerbated by increased screen time and sedentary behaviors. Enhancing physical activity levels at schools offers a promising approach to promote lifelong healthy habits.
Methods: This protocol paper outlines the MOVE12 pilot study, a 12-week intervention study designed to increase physical activity among Norwegian upper secondary school students through 6–7-min daily MOVE-breaks integrated into lessons. Developed using the six-phase Intervention Mapping (IM) protocol, grounded in the social-ecological model and self-determination theory, the intervention focuses on fostering motivation and creating a supportive environment. Key steps include needs assessment, performance objectives, theoretical methods, and program structuring for sustainability.
Results: Linear mixed models, t-tests, and regression analyses will evaluate quantitative outcomes, while qualitative focus groups will explore engagement and behavior change.
Discussion: MOVE12 provides insights into scalable school-based interventions addressing physical inactivity, highlighting the potential of the IM framework to establish sustainable health promotion strategies.
Physical inactivity is associated with numerous non-communicable diseases and substantial economic costs globally (1, 2). Regular physical activity among children and young people has been associated with physical fitness, cardiometabolic health, bone health, cognitive outcomes such as academic performance and cognitive function (3, 4), as well as mental health (5–7), quality of life (8), and, to some extent, mental well-being (9).
Given such evidence, the World Health Organization (WHO) (10) has advocated for increasing physical activity and reducing sedentary behavior, particularly among young people, as part of preventive measures against non-communicable diseases. However, global physical activity levels remain below the WHO's recommended minimum of 60 min of moderate-to-vigorous physical activity per day for children and adolescents, with significant declines throughout childhood and adolescence, especially among lower socioeconomic groups, a trend that often persists into adulthood (11). The rise of digital platforms and increased screen time in recent years has exacerbated concerns about sedentary behaviors among children and adolescents (12). Although trends are complex, this shift towards inactivity in future generations could have detrimental impacts on their physical and mental health (13). Furthermore, sedentary behaviors may have persisted at elevated levels following the COVID-19 pandemic compared to before (14). The UN's 2030 Agenda for Sustainable Development also underscores youth health as a priority focus area, highlighting the urgency of addressing this issue.
In Norway, health authorities recommend that children and adolescents engage in at least 60 min of daily physical activity at moderate to high intensity, while also reducing sedentary behavior (15). Schools have been identified as critical venues for promoting regular physical activity, serving as the only mandatory setting for such activities until the age of 19 in many countries. However, the scope of compulsory physical education is limited. In Norway, for instance, this equates to just one session per week, with an effective duration of approximately 70–80 min. The typical timetable in Norwegian secondary schools consists of 90-min instructional blocks interspersed with 10–15-min breaks devoid of structured physical activity. During these intervals, most students remain inactive, often engaged with social media on their mobile devices (16).
In 2021, the Norwegian government introduced a policy for the gradual inclusion of daily physical activity within school programs, providing schools with the discretion to tailor these activities independently (17). In support of this policy, leading health organizations joined forces to create a political platform named the “Alliance for Physical Activity in Schools,” encapsulated by the motto: “Daily physical activity in schools for all students” (18). Although some review articles suggest that physical education classes, after-school sports programs, and accessible sports facilities in schools are linked to higher levels of physical activity (19), the observed effects are generally modest, and it remains unclear whether these improvements are sustained over time (11, 20).
Recent empirical evidence further underscores both the potential and complexity of school-based interventions. For example, the “Join the Healthy Boat” program in Germany aimed to reduce children's sedentary behavior but did not achieve significant reductions despite decreasing screen time (21). In contrast, a combined physical activity and nutrition intervention in the Netherlands led to improvements in children's moderate-to-vigorous physical activity (MVPA) levels and BMI (22). Similarly, school-based interventions in disadvantaged neighborhoods in France demonstrated positive effects on children's physical activity by targeting multiple levels of the socioecological model (23).
Previous studies have identified several problems relating to the implementation of school-based programs (24, 25), which are often conceptualized as common barriers to promoting physical activity in schools (26). These can be roughly divided into institutional factors (such as school policies, facilities, and administrative support), teacher-related factors (including teachers' beliefs and skills), and student-related factors (such as characteristics of the student population). These barriers are often specific to the school level (primary vs. upper secondary) and the level of teacher experience (specialist vs. non-specialist) (27). Moreover, a systematic review by Cassar et al. on the implementation of school-based physical activity interventions found that implementation models are often used primarily for interpreting results and analyses rather than being employed as planning tools throughout all study phases. This limited application of implementation models may contribute to the modest success of interventions in real-world conditions (24). Additionally, there is an increasing awareness of the importance of understanding implementation in terms of sustainability (28) and equity (20).
Given the widespread decline in adolescent physical activity and the need for systematically planned, evidence-based interventions, this study aimed to thoroughly document the planning process of a 12-week physical activity pilot intervention (MOVE12) using the Intervention Mapping (IM) protocol. The IM protocol emphasizes understanding the determinants of behavior and environmental conditions (29), and is guided by the social-ecological model (SEM). Detailed descriptions of such protocols are often missing in study designs, yet they are crucial for mapping intervention development, addressing identified problems, and testing potential solutions (29). The primary objective of MOVE12 is to promote short physical activity sessions (MOVE-breaks) during class time in Norwegian upper secondary schools (16–17 years of age), potentially leading to sustained health benefits and encouraging a more physically active lifestyle outside of school.
For the systematic development of the MOVE12, the stepwise methodology of the IM protocol was employed. IM is a widely recognized methodology for planning health promotion programs that are both theory-based and evidence-based (30). The IM protocol comprises six steps: (1) conducting a needs assessment, (2) defining performance objectives and creating a matrix of change objectives, (3) selecting theory-based intervention methods and practical applications, (4) organizing these methods and applications into an intervention program, (5) planning for the adoption, implementation, and sustainability of the program, and (6) generating an evaluation plan (30). It is important to note that the application of the IM protocol in the MOVE12 was not strictly linear as the six steps suggest. Instead, the process was characterized by iterative refinement through ongoing discussions and interactions with the literature and the planning group. This iterative approach involved moving back and forth between different steps, continuously revising and refining the methodology as new information and insights emerged. This flexibility is a fundamental aspect of the IM protocol, as emphasized by Eldredge et al., who state that program developers often “move back and forth between tasks and steps as they gain information and perspective from various activities” (29). Consequently, while the IM framework provides a structured guideline, its application in practice requires adaptation and responsiveness to the evolving context and feedback received during the planning and implementation phases.
The initial step in the IM process involved establishing a planning group that included key stakeholders to ensure comprehensive collaboration across all levels of the initiative. The MOVE12 planning group included diverse representatives: two from the current county municipality (the Head of the Department of Public Health and the Project Manager for MOVE12, three from the research team [the principal investigator (PI) from Inland Norway University of Applied Sciences (INN) and two from Østfold University College], and two from each participating school (a leader and a teacher ambassador with designated resources to support the implementation process). The role of the teacher ambassadors was to serve as key mediators between the project team and the schools throughout all three phases. They were previously engaged by the county municipality as part of a broader school health initiative focusing on sleep and nutrition that began in 2017. This prior engagement was both convenient and advantageous, as it enabled collaborative relationships to be formed with the participating schools, helping to foster a sense of ownership and commitment to the project at each individual school.
The initial step of the IM protocol involved developing a logic model to graphically represent causal relationships and guide the planning team in addressing key health challenges (30). This process was informed by the public health profile of the current county municipality and a comprehensive needs assessment, integrating evidence from multiple data sources. For example, the 2022 Youth Profile (31) for one of the counties contributing half of the study's participants revealed a higher proportion of adolescents living in households with persistent low income (<60% of median household income) compared to the national average. This socio-economic disadvantage significantly impacts life and developmental opportunities, resulting in lower performance on cognitive and language tests, reduced academic motivation, and diminished self-efficacy, increasing the risk of school dropout. Additionally, these adolescents face a heightened risk of future physical and mental health challenges, underscoring the need for targeted interventions to improve well-being and educational outcomes.
A targeted literature review of peer-reviewed studies and reports on adolescent physical activity behaviors identified key barriers, including insufficient knowledge, low self-efficacy, and inadequate school support. Regional public health data highlighted local trends in adolescent physical inactivity, emphasizing the urgency of addressing sedentary behaviors during school hours.
Stakeholder engagement with school leaders, teacher ambassadors, and public health representatives informed the intervention's practical components, addressing curricular constraints and equipment needs. The demographic diversity of students across schools and academic tracks (academic and vocational) ensured the intervention was tailored to varied educational contexts and social dynamics. This multi-faceted approach ensured a robust, evidence-based, and context-sensitive intervention design.
According to Figure 1, adolescents' engagement in physical activity at school is significantly influenced by intrapersonal factors such as their knowledge, predispositions, and previous experiences with physical activity (32). Key to this is providing students with up-to-date knowledge about the importance of physical activity for psychosocial well-being and maintaining good health. This educational aspect, combined with the unique format of MOVE12 (student-led sessions in pairs), aims to foster positive attitudes towards participation (33). Additionally, self-concept plays an important role in shaping how they perceive their abilities and the value they place on physical activity (34, 35). The MOVE12 includes exercises that all students can master regardless of their initial skill level, enhancing a sense of self-efficacy among students who may traditionally be reluctant to engage in physical activities (36, 37). Furthermore, for adherence to the program, it is vital that students find the activities enjoyable (motivation), which is facilitated by allowing some freedom in choosing the activities they participate in. According to self-determination theory (SDT), fulfilling the basic psychological needs of competence (feeling effective and mastering challenging tasks), autonomy (having a sense of initiative when participating voluntarily), and relatedness (feeling accepted and integrated within a social context) enhances adolescents' well-being and intrinsic motivation (38).
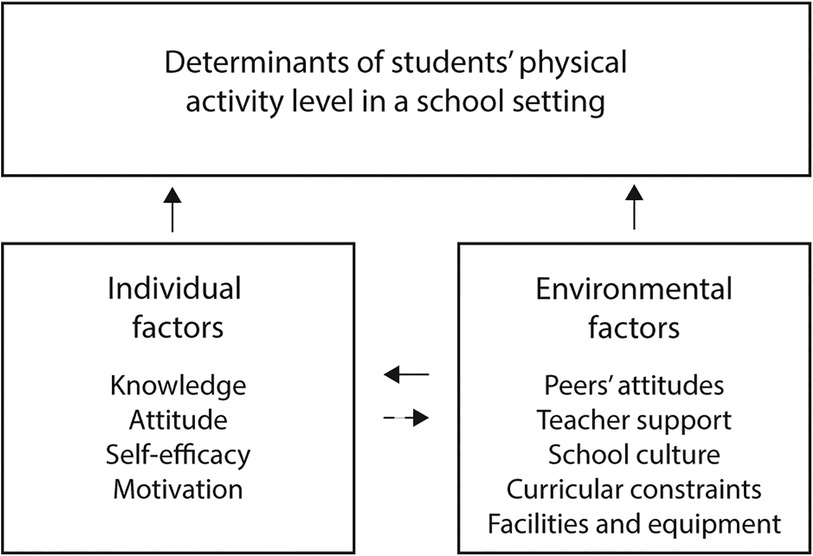
Figure 1. Logic model of the problem. Factors influencing students’ physical activity level at school.
At the interpersonal and organizational levels, several key factors have been identified as influencing physical activity levels among school-aged youth. Research highlights that social influences, including peer attitudes, can negatively impact not only adolescents’ physical activity levels but also their self-concept (39, 40). Moreover, the lack of adequate support from teachers and school leaders can further inhibit active engagement (35, 39, 41). These elements are essential in establishing a positive culture around class participation rates and individual student engagement, a responsibility that largely rests with the school management. To successfully implement MOVE12, it is crucial that school management collaborates with teachers to find effective ways to accommodate short MOVE-breaks during class time within a busy school schedule characterized by prolonged sedentary periods (curricular constraints) (42). Lastly, it is essential to address challenges such as limited access to appropriate equipment and suboptimal facilities, as these constraints could hinder the implementation of MOVE-breaks (37, 39).
The second step of the IM protocol process focused on identifying the targeted changes at both behavioral (who will change) and environmental (what will change) levels based in relation to the understanding of the problem outlined in Step 1. This was achieved by creating a logic model of change (Figure 2) that integrated elements from the social-ecological model (SEM) and self-determination theory (SDT). The SEM serves as a comprehensive framework that can be applied to help elucidate the complex interplay between individual and environmental factors in shaping behaviors at micro, meso and macro levels. Specifically, within the realm of physical activity, SEM underscores that individual behaviors are influenced not only by personal decisions but also by environmental factors such as social support, the physical environment, institutional policies, and community norms (43). Meanwhile, SDT focuses on the assumed psychological needs for autonomy, competence, and relatedness. By addressing these needs through physical activity in the school organizational context, SDT provides a foundation for designing interventions that enhance motivational factors, making physical activity both personally appealing and supported by social contexts (38).
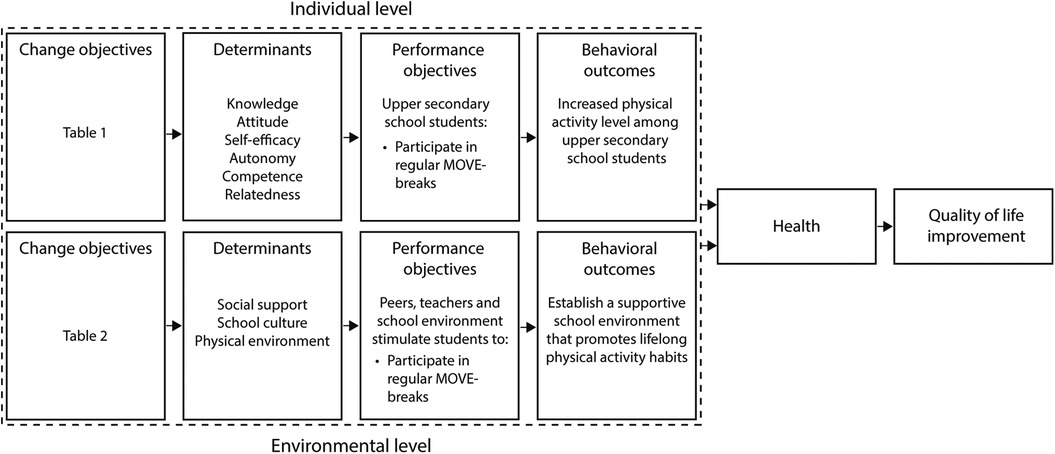
Figure 2. Logic model of change of the intervention.
At the individual (micro) level, the intervention focuses on enhancing intrinsic motivators for students' physical activity (PA) throughout the school day by promoting enjoyable and engaging activities. This strategy aims to cultivate lasting PA habits, which can improve health and overall quality of life. At the environmental (meso-organizational) level, the goal is to establish a supportive school environment that encourages lifelong physical activity habits. This involves integrating effective, inclusive, and multicomponent school-based interventions that enhance access to safe and appealing PA settings (36, 41). At the macro level, the intervention seeks to engage stakeholders, including local authorities, educational institutions, community organizations, and policymakers, to create supportive environments for physical activity in schools. It advocates for increased funding, improved infrastructure for accessible and safe exercise facilities near classrooms, and the integration of school-based physical activity into public health and education policies. Additionally, the project aims to raise awareness of schools as vital arenas for health-promoting physical activity through local, regional, and national initiatives. By fostering cross-sector collaboration, the project aims to achieve sustainable, systemic changes that encourage active lifestyles and enhance youth well-being.
In accordance with the IM protocol methodology, the final outcomes of the Move12 were subdivided into various components, with the desired changes in these components articulated as performance objectives (Figure 2). Based on the needs assessment derived from our literature review, the primary performance objective was to encourage students to participate in 1–2 daily MOVE-breaks, physical activity sessions lasting 6–7 min, integrated into 90-min class periods during regular school days. Several determinants identified through the IM process, were recognized as critical to achieving this objective. At the individual level, changeable determinants of PA participation, as identified in our literature review, included knowledge, attitude, and self-efficacy, as well as the three basic psychological needs: autonomy, competence, and relatedness. Stakeholder feedback, particularly from teacher ambassadors, revealed that while the initial objective focused on student participation and recognizing the benefits of MOVE-breaks, greater autonomy in activity planning was necessary to increase motivation. This led to a revision in which students were allowed to select activity content within structured guidelines, exemplifying how the IM protocol steps were iteratively refined. At the environmental level, modifiable determinants included social support, school culture, and the physical environment. Feedback from stakeholders highlighted logistical constraints in classroom environments. To address this, we refined the objectives to incorporate practical facilitation measures, such as introducing simple equipment like beanbags and dice, to expand the range of accessible and engaging activities. Following the IM protocol methodology, matrices of change objectives were developed by intersecting performance objectives with these determinants (Table 1). These matrices outlined the necessary achievements for meeting each performance objective. For example, one key change objective at the individual level was ensuring that students understood the potential benefits of participating in MOVE-breaks (knowledge). Feedback during the planning phase reinforced the importance of aligning these objectives with both student needs and environmental realities, demonstrating the iterative nature of the IM protocol.
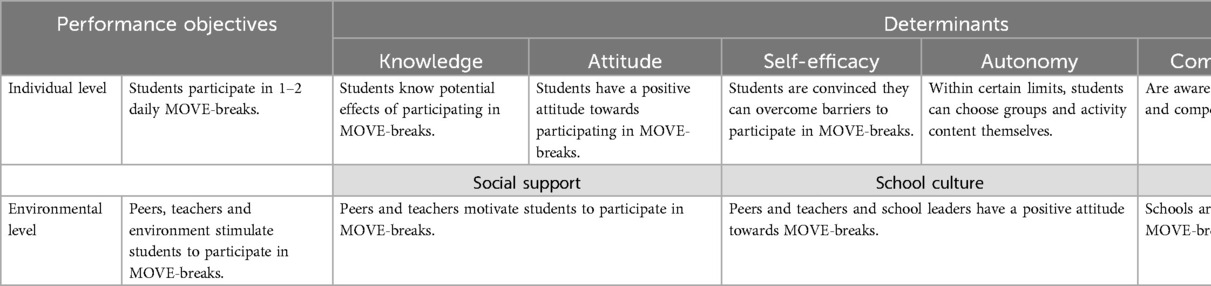
Table 1. Performance objectives and determinants for MOVE-break participation.
The third step of the IM process focused on selecting theory-based intervention methods and translating them into practical applications tailored to the MOVE12 intervention (Table 2). These applications were informed by insights gained from the comprehensive needs assessment and the Public Health Profile (31) described in Step 1. For instance, the 2022 Youth Profile highlighted persistent low household income and its adverse effects on adolescents' cognitive performance, motivation, and self-efficacy, which informed specific methods and applications. For example, goal-setting activities were introduced to foster autonomy by encouraging students to collaboratively plan MOVE-break sessions, selecting activities that aligned with their personal interest. Guided practice with feedback was used to build self-efficacy, with PE teachers and teacher ambassadors providing regular feedback during preparatory practice sessions. To enhance relatedness, social support was mobilized through peer encouragement, and teacher ambassadors served as key contacts to support students throughout the intervention. These methods were iteratively refined to align with the intervention's goal of increasing physical activity among diverse student populations.
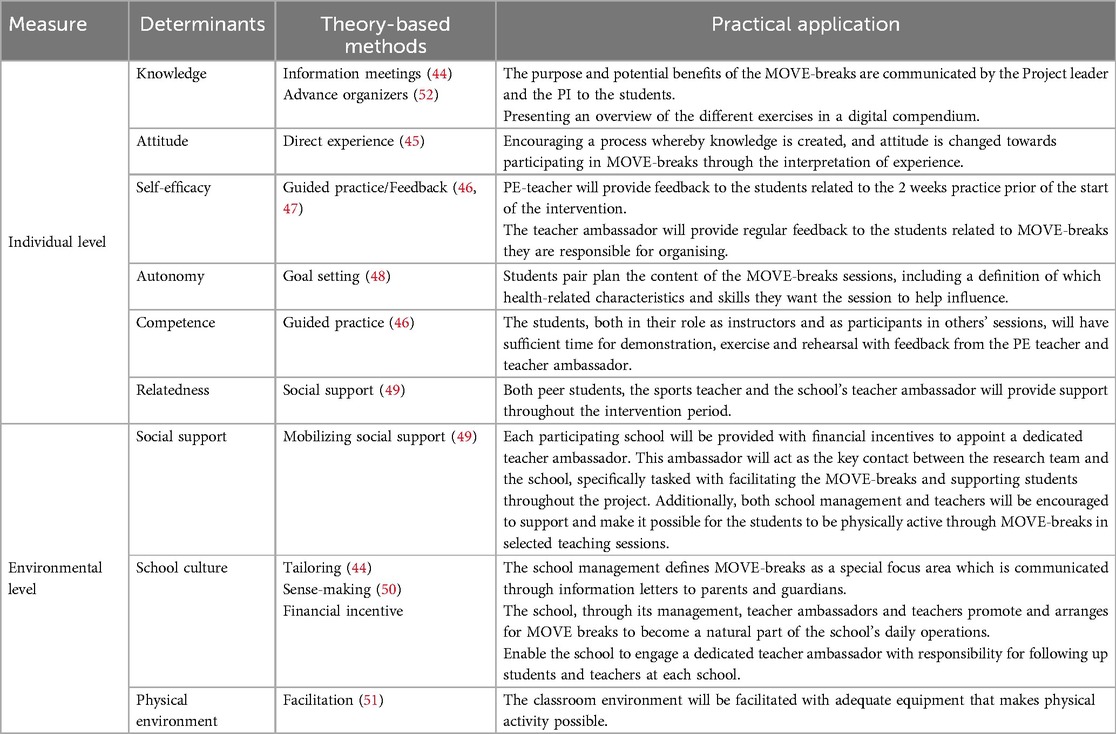
Table 2. Theory-based methods and applications for enhancing MOVE-break participation.
To strengthen students' self-efficacy, guided practice sessions with feedback from teacher ambassadors were incorporated, addressing the identified need for supportive school structures. Pairing students to co-lead MOVE-breaks fostered autonomy and relatedness, targeting the psychological needs for competence, autonomy, and social connectedness highlighted in Step 1.
MOVE12 aimed for sustainable changes at both individual and environmental levels, At the meso level, regular meetings with community leaders and county decision-makers were planned, who were also part of the MOVE12 planning group, were organized to strengthen local implementation. At the macro level, public health and educational policymakers were invited to review program data at a project conference six months after the intervention. These efforts aimed to secure ongoing support and funding by demonstrating the program's wide-ranging benefits, including improvements in students' physical and mental health, development of social skills, a better school climate, enhanced concentration (facilitating faster learning), and increased engagement in theoretical lessons.
In order to increase students’ knowledge and awareness of the importance of physical activity for a healthy life, introductory information meetings (44) will be held at the respective schools. These meetings, led by the project leader and Principal Investigator (PI), will focus on the purpose and potential benefits of the MOVE-breaks. Given the uniqueness of the MOVE-breaks (short student-led physical activity sessions as a break in ordinary teaching sessions), a sub-goal is to help students who may initially be negative about physical activity change their predisposition through positive participation experiences (45). To foster students' self-efficacy in organizing and implementing MOVE-break sessions, PE teachers will provide a comprehensive 2 × 90-min introductory course. This course will include practical training and ongoing feedback for students before the intervention begins (46, 47). Aligned with self-determination theory (SDT), students will be able to set their own goals for the MOVE-break they lead. This autonomy is expected to enhance their motivation for participation (48). Structured practice under the supervision of the PE teacher will help build students' competence in planning, organizing, and evaluating MOVE-breaks. This competence-building is reinforced through social comparisons with peer pairs who share similar responsibilities during the pilot study, fostering confidence in their physical activity abilities (46). Finally, the implementation of student pairs, along with support from PE and teacher ambassadors, is designed to provide mutual support, addressing the need for relatedness. These structures and processes aim to maintain motivation through social encouragement and accountability (49).
At the environmental level, school managers will be encouraged to focus on supporting and motivating both teachers and students in the implementation of the MOVE-break, with the goal of eventually integrating it into the school's routine. This effort can be facilitated by featuring it as an agenda item in upcoming leadership and staff meetings. Additionally, we will encourage physical education teachers and other relevant teachers to support students and ensure the regular implementation of MOVE-breaks 1–2 daily. Tailored information and promotion will be used to foster a positive school culture around MOVE-breaks, relying on social support from leadership down to the student level. Additionally, the project group will encourage school leaders to actively promote physical activity in the daily school routine, both internally and in external forums, drawing inspiration from organizational development theory, which involves ongoing, iterative adjustments and rebalancing within organizational routines and processes (50).
To further assist schools in fostering a positive culture for implementing regular MOVE-breaks throughout the school day, participating schools will receive financial incentives to allocate to dedicated teacher ambassadors (Table 2). In terms of the physical environment (51), a compendium of physical activities and exercises (52) have been developed for seamless implementation in classroom settings with minimal furniture modifications, such as rearranging desks and chairs. To support this process, the project team created a digital activity guide featuring strength- and endurance-based exercises tailored for classroom use. Students designed their own MOVE-break session plans, incorporating images and detailed descriptions, and utilized classroom projectors to play follow-along dance videos (e.g., “Just Dance”). Additionally, each intervention class was provided with simple, portable equipment, such as beanbags, cards, and dice, enabling a variety of basic games, team exercises, and relay activities that are easy to organize and integrate into lessons.
To address scheduling challenges and classroom disruptions in MOVE12, the implementation of MOVE-breaks was designed with flexibility to accommodate the unique traditions, practices, and challenges of individual schools and classes. This collaborative approach, grounded in research-based strategies, promotes effective integration into diverse educational settings. The study design incorporates peer-led sessions (Table 2), where student pairs co-lead MOVE-breaks to foster autonomy, reduce teacher workload, and enhance peer accountability while maintaining classroom order (33, 53). Integration into the curriculum, such as fixed 10-min breaks during natural transitions in 90-min lectures, minimizes disruptions and optimizes participation (49). Classroom management protocols, including clear guidelines, designated movement areas, and student role assignments, maintain structure and discipline during activities (50). Regular feedback mechanisms will gather input from teachers and students on scheduling preferences and activity formats, enabling iterative refinements to improve feasibility and satisfaction (51). Lastly, providing simple, minimal equipment, such as portable items like beanbags or dice, ensures activities are quickly initiated and cleared, minimizing logistical hurdles and interruptions. These strategies collectively enhance the adaptability, effectiveness, and sustainability of MOVE12 across varied school contexts.
To ensure the sustainability of MOVE12, stakeholder engagement (Table 2) will be a critical factor. Following the conclusion of MOVE12, a subsequent main intervention is planned, which will maintain the involvement of the same teacher ambassadors. Together with school leaders and additional teachers recruited for the main intervention, these stakeholders will receive close follow-up through regular meetings with the project leadership, both prior to and during the intervention period. After the main intervention, the project leader will establish ongoing collaboration by organizing periodic meetings with school leaders and teacher ambassadors, facilitated by the county municipality. These meetings aim to sustain engagement, share experiences, and develop strategies for integrating the intervention into long-term school routines.
Building on the methodologies and applications selected in Step 3, the fourth step of the IM protocol process entails the development of the intervention program, complemented by a detailed inventory of materials necessary for execution. The program production is divided into two primary phases:
This initial phase is dedicated to applying the findings from the previous theoretically based steps by developing a strategy to promote the initiative among students and teachers, and by preparing presentations and relevant tools/materials for the planned intervention. Distinct 60-min information sessions will be conducted for school leaders, teachers, and students to ensure each participant is thoroughly briefed on their roles and responsibilities. For these sessions, a PowerPoint presentation will be prepared, detailing the program's rationale, objectives, content, outcomes, and ethical considerations. Moreover, students will receive details on the MOVE-breaks, explaining its incorporation into a specific competency goal in physical education that requires planning, executing, and evaluating a personal training period. Additionally, a 5-min demonstration video showcasing various physical measurement techniques will be created for students. For teachers, we will create a promotional video lasting 5 min that emphasizes the benefits of incorporating brief MOVE-breaks into classroom settings (54).
The next phase focuses on giving students practical-methodological practice in various ways to conduct MOVE-break sessions. It includes two 90-min sessions where students, in pairs, use the exercise compendium as a reference to plan, conduct, and assess their own 6–7-min MOVE-breaks for their peers, under the guidance of the physical education teacher. These practice sessions can be held in classrooms or suitable indoor/outdoor spaces nearby.
The fifth step of the IM protocol process focused on planning the adoption, implementation, and sustainability of the intervention. This stage emphasizes engaging stakeholders to address barriers and refine strategies to maximize the intervention's reach and impact. Stakeholder discussions played a pivotal role in shaping the implementation plan. For example, feedback from school leaders and teacher ambassadors highlighted the need for financial incentives to encourage teacher ambassadors' active involvement. This input led to the allocation of dedicated funding to support their roles, ensuring consistent oversight and motivation during the intervention. Additionally, the needs assessment highlighted the importance of tailored communication strategies for parents to foster engagement and extend the program's impact beyond the classroom. In response, an information letter was developed to emphasize the benefits of MOVE-breaks in enhancing students' physical activity levels and overall well-being. As illustrated in Figure 3, the implementation of MOVE-breaks commenced following the completion of baseline measurements at the end of January 2023 and continued for a 12-week period, concluding in April 2023. This timeline allowed for a structured rollout while maintaining flexibility to address any unforeseen challenges. By incorporating the iterative refinements, the implementation plan was aligned with the practical needs of schools and stakeholders, enhancing the likelihood of sustained adoption and success.
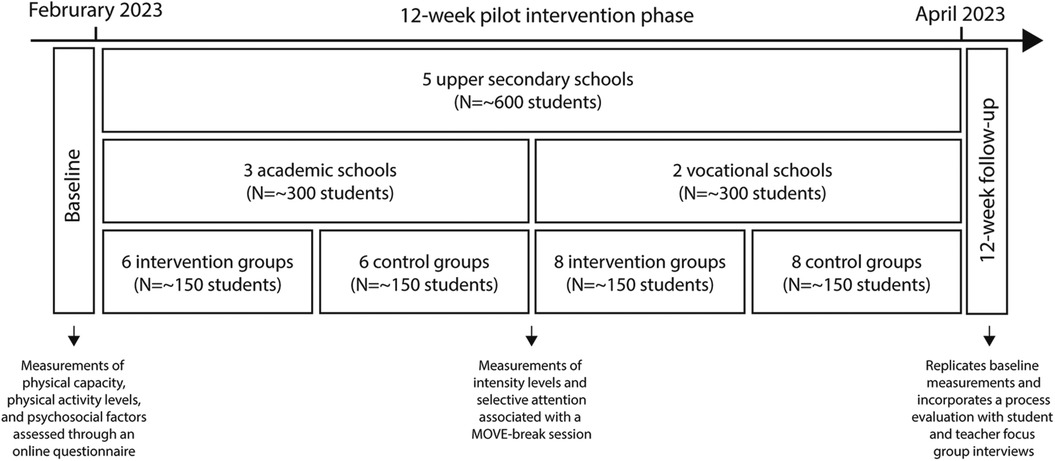
Figure 3. Timeline for the MOVE12 pilot intervention study.
This protocol paper, developed using the intervention mapping (IM) framework, describes the planning of a 12-week cluster-randomized mixed-methods pilot study, incorporating both quantitative and qualitative data collection and analysis. The target population included first-year upper secondary school students from a broad region in southeastern Norway (three counties), aiming for balanced representation of academic and vocational programs. Invitations were sent to 27 upper secondary schools, and five agreed to participate (three academic, two vocational). One vocational school, twice the size of the others, contributed approximately 200 students, while each of the remaining four contributed about 100 students. Of 739 eligible students, 519 provided consent. The inclusion criteria for participation were students aged 16–17 years, with exclusion criteria defined as disabilities preventing participation and/or illnesses posing health risks.
The MOVE12-pilot study was designed as a two-arm, three-level cluster randomized controlled trial (RCT), featuring an intervention group (IG) and a control group (CG), with participants organized within classrooms and schools. Participants were randomly assigned to either the IG or the CG (1:1) by the principal investigator (PI). At the three academic schools (class size: 25–30), four relatively homogeneous classes were identified, and randomization involved drawing from two boxes (one for group assignment, one for classes) in alternating turns until all classes were assigned. At the two vocational schools (class size: 12–17), classes were stratified by gender, size, and subject area before following the same procedure using four boxes (A–D). Twice as many groups were drawn from the vocational school that was double the size of the others.
During the intervention period, the intervention groups were encouraged to incorporate at least two 6–7-min MOVE-breaks into their daily classroom sessions. The PE teacher, in collaboration with the participating teachers, coordinated the rotation of student pairs responsible for leading these sessions in various lectures. Additionally, teacher ambassadors played a crucial role in assisting with the implementation of the intervention. They worked closely with the Principal Investigator (PI) to provide support and encouragement to both the teachers and participating students. To support this process, the project team developed a digital activity guide featuring strength- and endurance-based exercises for the classroom. Students created their own MOVE-break session plans, adding images and descriptions. They also used computers to play follow-along dance videos (e.g., “Just Dance”) via the classroom projector. In addition, each class received simple equipment (beanbags, cards, dice) for basic games, team exercises, and relay activities.
The aim of MOVE12 is to increase students' physical activity levels in school through participation in 1–2 daily MOVE-breaks lasting 6–7 min each. This goal is pursued by enhancing their knowledge, fostering positive attitudes, boosting self-esteem, and nurturing intrinsic motivation at the individual level, while also focusing on providing opportunities and social support from teachers and peers (see Table 1). The findings from our planned evaluation will be reported in accordance with the CONSORT 2010 guidelines for randomized trials (55).
The primary outcome measures align with the study's core objective: promoting student participation in 1–2 daily MOVE-breaks (6–7 min each) during regular class sessions (Table 1). Feasibility and implementation will be assessed by evaluating students' adherence to MOVE-breaks and gathering insights into the subjective experiences of both students and teachers. These evaluations will be guided by changeable determinants such as knowledge, attitude, self-efficacy, basic psychological needs (autonomy, competence, relatedness), social support, school culture, and the physical environment. Data will be collected through focus group discussions at the 12-week follow-up, providing a comprehensive understanding of the intervention's effectiveness.
Additionally, the study aims to evaluate potential effects of MOVE-breaks on physical fitness, psychosocial health parameters, and school-related factors through the following outcome measures:
- Attention and Concentration: Measured with the Eriksen Flanker Test (56) and the Stroop Test (57) before and after a designated MOVE-break session at the midpoint of the intervention.
- Heart Rate Measurements: Measured during a designated MOVE-break session at the midpoint of the intervention using the Polar Team Pro System (58).
- Physical Activity Level: Measured using the ActiGraph wGT3X-BT (59) at baseline and 12-week follow-up.
- Aerobic Fitness: Measured with the YMCA 3-min step test (60) at baseline and 12-week follow-up.
- Muscle Strength: Measured by (i) standing long jump (61) and ii) handgrip (dynamometer) (62) at baseline and 12-week follow-up.
- Postural Balance: Measured by two-leg standing, eyes closed (30 s) and one-leg standing, eyes open (30 s) (63) at baseline and 12-week follow-up.
- Flexibility: Measured by the sit-and-reach test (64) at baseline and 12-week follow-up.
- Sleep Quality: Measured by an online questionnaire (Nettskjema.no) at baseline and 12-week follow-up using four single items from a modified version of the Karolinska Sleep Questionnaire (65).
- Wellbeing: Measured by an online questionnaire (Nettskjema.no) at baseline and 12-week follow-up using the Warwick-Edinburgh Mental Wellbeing 7-item scale (66).
- Self-Efficacy: Measured by an online questionnaire (Nettskjema.no) at baseline and 12-week follow-up using a factor developed by Sørlie and Nordahl (67), based on Bandura (68).
- Learning Environment and Social Wellbeing in Class: Measured by an online questionnaire (Nettskjema.no) at baseline and 12-week follow-up using 13 items developed by Moos and Trickett (69), translated and processed by Sørlie and Nordahl (67).
- Social Isolation: Measured by an online questionnaire (Nettskjema.no) at baseline and 12-week follow-up using 21 items from the Social Skills Rating System by Gresham and Elliott (70), translated and processed by Sørlie and Nordahl (67).
Data analysis will combine quantitative and qualitative approaches. To examine between-group differences in continuous outcome measures from baseline to the 12-week follow-up, a linear mixed model (LMM) will be applied. LMM addresses the nested data structure of MOVE12 (students within classrooms, classrooms within schools) by incorporating random intercepts to account for intra-class correlation and hierarchical clustering effects (71). Additionally, LMMs handle missing data robustly under the assumption of missing at random (72), a common scenario in school-based interventions. Within-group changes will be assessed using dependent t-tests, and potential associations between ordinal outcome measures will be explored through multiple and binary regression analyses. All statistical analyses will be conducted using STATA version 18.0 (73).
Qualitative methods will be used to identify key themes from the planned focus group interviews, guided by determinants such as knowledge, attitude, self-efficacy, basic psychological needs (autonomy, competence, relatedness), social support, school culture, and the physical environment. This qualitative approach aims to deepen our understanding of how these factors influence participants' experiences and engagement with the intervention, thereby informing both practical implementation and theoretical implications. Qualitative data will be analyzed thematically using NVivo 14 software to support and manage the analytic process (74).
a priori sample size calculations with G-Power (75) suggested that a sample of 580 participants would be sufficient to detect a moderate effect size (d = 0.3), assuming a two-group design, 80% power, and an alpha of.05.
Recent meta-analyses and systematic reviews provide growing evidence supporting physical activity breaks in schools, demonstrating benefits for students' physical activity levels (76–78), attention (79), academic performance (80, 81), health-related quality of life (82), and aerobic fitness (19, 83). These findings underscore the classroom as a promising setting for promoting physical activity with potential benefits for learning outcomes and student well-being. However, it is equally important to recognize that some reviews report modest or inconsistent effects, including weak trends or null findings, particularly regarding long-term impact, feasibility, and contextual variations in implementation success. These inconsistencies reveal critical knowledge gaps that necessitate further investigation into targeted, sustainable, and scalable approaches (11).
The MOVE12 study addresses these gaps through the evaluation of a systematically designed, classroom-based intervention developed using the robust, theory-driven Intervention Mapping (IM) protocol. By targeting both individual and environmental determinants, MOVE12 promotes short, student-led physical activity breaks (MOVE-breaks) integrated seamlessly into the school day. The intervention incorporates evidence-based components, peer-led sessions, autonomy-supportive structures, and minimal resource requirements, to enhance feasibility, adaptability, and sustainability across diverse school settings. Its multi-level approach considers individual, interpersonal, and organizational factors, ensuring comprehensive evaluation while addressing real-world challenges that affect intervention effectiveness.
Guided by the socio-ecological model (SEM) and self-determination theory (SDT), MOVE12 represents an innovative approach to integrating physical activity into upper secondary school routines. The IM protocol enabled a systematic and theory-informed process for designing, implementing, and evaluating this health promotion intervention. One of the key strengths of using IM lies in its step-by-step framework, which ensures each phase is grounded in theoretical and empirical evidence (30). This structure is particularly valuable for addressing complex health behaviors like physical activity, which are influenced by interdependent factors at multiple levels, from individual motivation to school culture and broader policies.
The MOVE12 study aims to build on previous efforts by embedding regular, short physical activity breaks throughout the school day. While prior interventions have shown varying levels of success, the strategy seeks to create an environment that actively supports sustained physical activity. By incorporating MOVE-breaks into daily school routines, the intervention has the potential to enhance adherence to physical activity guidelines (84, 85), achieving the recommended 60 min of moderate-to-vigorous physical activity per day (76, 86). Additionally, the flexible design allows schools to tailor the program to their specific contexts, effectively addressing variations in resources, constraints, and classroom structures across academic and vocational programs.
This study also enhances the theoretical understanding of intervention design by integrating SEM and SDT to create supportive environments that not only allow, but actively encourage regular physical activity among adolescents (35, 87). The intervention emphasizes autonomy and peer support, core SDT constructs that are shown to enhance motivation, engagement, and sustainability of behavior change. Research supports this dual approach, as interventions fostering autonomy, competence, and relatedness are more likely to be effective and maintained over time (38, 43).
Despite its strengths, the application of the IM protocol in MOVE12 poses several challenges. A significant issue is ensuring the fidelity across diverse school environments, particularly given structural differences between academic and vocational study programs in terms of classroom (88). Academic students typically work at desks in traditional classrooms, whereas vocational students experience more diverse working methods, such as alternating between standing and sitting, and varied classroom environments like workshops, specialized workspaces, and classrooms that differ according to the subject area. Variations in resources, commitment, and existing cultures among schools could affect the consistency and effectiveness of the intervention's implementation. This highlights the need for adaptable yet structured implementation strategies that can accommodate various school environments/contexts without compromising the intervention's integrity (89, 90). Another challenge is securing engagement from all stakeholders, particularly teachers who are not directly involved as teacher ambassadors (91, 92). Their broader involvement is crucial for the sustainable integration of physical activity interventions in schools, as they play a significant role in shaping school culture and student behaviors (93).
The MOVE12 study offers valuable insights for the design and implementation of health promotion interventions in educational settings. Future research should focus on the scalability of such interventions, exploring factors like school size, diverse demographics, and varying levels of existing infrastructure. From a policy perspective, MOVE12 has the potential to inform school-based strategies that address physical inactivity, contributing to improved public health outcomes. The evaluation of the MOVE12 pilot intervention will assess the effectiveness of the intervention mapping protocol in establishing a foundation for sustainable, scalable, and impactful physical activity interventions in schools.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Before implementing the intervention, ethical approval was granted by the Local Ethics Committee for Research at Inland Norway University (Ref. 21/01894). The project was registered with the Norwegian Agency for Shared Services in Education and Research (Sikt; Ref. 349704) and retrospectively in the ISRCTN registry (ISRCTN10405415). Participation poses no greater risk than standard physical education, with injuries requiring medical attention covered by schools' self-insurance policies. Students with pre-existing health conditions will have their participation adapted to their functional capacity, consistent with accommodations in physical education classes. Written informed consent was obtained from schools and students. A robust data management plan ensures secure data storage and handling through the TSD portal (Service for Sensitive Data), compliant with the Personal Data Act and Health Research Act. Any deviations from the described methodology will be transparently reported in publications. Findings will be disseminated through peer-reviewed journals, conference presentations, and informal meetings to maximize accessibility and impact.
SB: Conceptualization, Methodology, Project administration, Writing – original draft, Writing – review & editing. PJ: Methodology, Writing – review & editing. HT: Writing – review & editing. RØ: Project administration, Writing – review & editing. MT: Conceptualization, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. MOVE12 was funded by the Savings Bank Foundation DNB, which had no involvement in the study design, data collection, analysis, interpretation, or manuscript preparation.
We would like to thank Elsie Brenne, Anders Farholm, Harald Oseland, Sigbjørn Litleskare, and the other members of the planning group from the respective five schools for their contributions to the development of the intervention.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ding D, Lawson KD, Kolbe-Alexander TL, Finkelstein EA, Katzmarzyk PT, Van Mechelen W, et al. The economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet. (2016) 388(10051):1311–24. doi: 10.1016/S0140-6736(16)30383-X
2. Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. (2012) 380(9838):219–29. doi: 10.1016/S0140-6736(12)61031-9
3. Archer T, Garcia D. Physical exercise influences academic performance and well-being in children and adolescents. Int J Sch Cogn Psychol. (2014) 1(1):e102. doi: 10.4172/2469-9837.1000e102
4. Torrijos-Niño C, Martínez-Vizcaíno V, Pardo-Guijarro MJ, García-Prieto JC, Arias-Palencia NM, Sánchez-López M. Physical fitness, obesity, and academic achievement in schoolchildren. J Pediatr. (2014) 165(1):104–9. doi: 10.1016/j.jpeds.2014.02.041
5. Biddle SJ, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med. (2011) 45:886–95. doi: 10.1136/bjsports-2011-090185
6. Biddle SJ, Ciaccioni S, Thomas G, Vergeer I. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychol Sport Exerc. (2019) 42:146–55. doi: 10.1016/j.psychsport.2018.08.011
7. Stubbs B, Vancampfort D, Hallgren M, Firth J, Veronese N, Solmi M, et al. EPA guidance on physical activity as a treatment for severe mental illness: a meta-review of the evidence and position statement from the European Psychiatric Association (EPA), supported by the International Organization of Physical Therapists in Mental Health (IOPTMH). Eur Psychiatry. (2018) 54:124–44. doi: 10.1016/j.eurpsy.2018.07.004
8. Marker AM, Steele RG, Noser AE. Physical activity and health-related quality of life in children and adolescents: a systematic review and meta-analysis. Health Psychol. (2018) 37(10):893–903. doi: 10.1037/hea0000653
9. Barth Vedøy I, Skulberg KR, Anderssen SA, Fagerland MW, Tjomsland HE, Thurston M. The longitudinal association between objectively measured physical activity and mental health among Norwegian adolescents. Int J Behav Nutr Phys Act. (2021) 18(1):149. doi: 10.1186/s12966-021-01211-x
10. World Health Organization. WHO guidelines on Physical Activity and Sedentary Behaviour. Geneva: World Health Organization (2020). Available from: https://iris.who.int/bitstream/handle/10665/336656/9789240015128-eng.pdf
11. van Sluijs EM, Ekelund U, Crochemore-Silva I, Guthold R, Ha A, Lubans D, et al. Physical activity behaviours in adolescence: current evidence and opportunities for intervention. Lancet. (2021) 398(10298):429–42. doi: 10.1016/S0140-6736(21)01259-9
12. Kwok C, Leung PY, Poon KY, Fung XCC. The effects of internet gaming and social media use on physical activity, sleep, quality of life, and academic performance among university students in Hong Kong: a preliminary study. Asian J Soc Health Behav. (2021) 4(1):36–44. doi: 10.4103/shb.shb_81_20
13. Hoare E, Milton K, Foster C, Allender S. The associations between sedentary behaviour and mental health among adolescents: a systematic review. Int J Behav Nutr Phys Act. (2016) 13(1):108. doi: 10.1186/s12966-016-0432-4
14. Jago R, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al. Short and medium-term effects of the COVID-19 lockdowns on child and parent accelerometer-measured physical activity and sedentary time: a natural experiment. Int J Behav Nutr Phys Act. (2023) 20(1):42. doi: 10.1186/s12966-023-01441-1
15. Helsedirektoratet. 2024. Nasjonale Faglige råd for Fysisk Aktivitet I Forebygging og Behandling [nettdokument]. Oslo: Helsedirektoratet. Available from: https://www.helsedirektoratet.no/faglige-rad/fysisk-aktivitet-i-forebygging-og-behandling (latest revision November 1, 2024, read December 16, 2024).
16. Kolhar M, Kazi RNA, Alameen A. Effect of social media use on learning, social interactions, and sleep duration among university students. Saudi J Biol Sci. (2021) 28(4):2216–22. doi: 10.1016/j.sjbs.2021.01.010
17. Statistics Norway. Sustainable Development Goals; Indicators for Norway, Statistical Annex to the Norwegian Voluntary National Review 2021. Oslo: Statistics Norway (2021). p. 79.
18. Nasjonalforeningen for folkehelsen. Politisk Plattform for Daglig Fysisk Aktivitet I Skolen. Oslo: Nasjonalforeningen for folkehelsen (2023). Available from: https://nasjonalforeningen.no/om-oss/vi-mener/prinsipprogrammer/en-times-fysisk-aktivitet-i-skolen/ (September 13, 2023).
19. Neil-Sztramko SE, Caldwell H, Dobbins M. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst Rev. (2021) 19(9):1465–858. doi: 10.1002/14651858.CD007651.pub3
20. Love R, Adams J, van Sluijs EM. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes Rev. (2019) 20(6):859–70. doi: 10.1111/obr.12823
21. Kobel S, Dreyhaupt J, Wartha O, Kettner S, Hoffmann B, Steinacker JM. Intervention effects of the health promotion programme “join the healthy boat” on objectively assessed sedentary time in primary school children in Germany. Int J Environ Res Public Health. (2020) 17(23):9029. doi: 10.3390/ijerph17239029
22. Verjans-Janssen SRB, Gerards SMPL, Kremers SPJ, Vos SB, Jansen MWJ, Van Kann DHH. Effects of the KEIGAAF intervention on the BMI z-score and energy balance-related behaviors of primary school-aged children. Int J Behav Nutr Phys Act. (2020) 17(1):105. doi: 10.1186/s12966-020-01012-8
23. Bernal C, Lhuisset L, Bru N, Fabre N, Bois J. Effects of an intervention to promote physical activity and reduce sedentary time in disadvantaged children: randomized trial. J Sch Health. (2021) 91(6):454–62. doi: 10.1111/josh.13022
24. Cassar S, Salmon J, Timperio A, Naylor P-J, Van Nassau F, Contardo Ayala AM, et al. Adoption, implementation and sustainability of school-based physical activity and sedentary behaviour interventions in real-world settings: a systematic review. Int J Behav Nutr Phys Act. (2019) 16:1–13. doi: 10.1186/s12966-019-0876-4
25. Richter A, Sjunnestrand M, Romare Strandh M, Hasson H. Implementing school-based mental health services: a scoping review of the literature summarizing the factors that affect implementation. Int J Environ Res Public Health. (2022) 19(6):3489. doi: 10.3390/ijerph19063489
26. Hickingbotham MR, Wong CJ, Bowling AB. Barriers and facilitators to physical education, sport, and physical activity program participation among children and adolescents with psychiatric disorders: a systematic review. Transl Behav Med. (2021) 11(9):1739–50. doi: 10.1093/tbm/ibab085
27. Hills AP, Dengel DR, Lubans DR. Supporting public health priorities: recommendations for physical education and physical activity promotion in schools. Prog Cardiovasc Dis. (2015) 57(4):368–74. doi: 10.1016/j.pcad.2014.09.010
28. Jago R, Salway R, House D, Beets M, Lubans DR, Woods C, et al. Rethinking children’s physical activity interventions at school: a new context-specific approach [perspective]. Front Public Health. (2023) 11:25–34. doi: 10.3389/fpubh.2023.1149883
30. Eldredge LKB, Markham CM, Ruiter RA, Fernández ME, Kok G, Parcel GS. Planning Health Promotion Programs: An Intervention Mapping Approach. San Fransisco, CA: John Wiley & Sons (2016).
31. Norwegian Institute of Public Health. Public health profiles for municipalities and counties (2022). Available online at: https://www.fhi.no/he/folkehelse/folkehelseprofil/ (Accessed December 10, 2024).
32. Karchynskaya V, Kopcakova J, Madarasova Geckova A, Katrusin B, Reijneveld SA, de Winter AF. Barriers and enablers for sufficient moderate-to-vigorous physical activity: the perspective of adolescents. PLoS One. (2024) 19(2):e0296736. doi: 10.1371/journal.pone.0296736
33. Christensen JH, Elsborg P, Melby PS, Nielsen G, Bentsen P. A scoping review of peer-led physical activity interventions involving young people: theoretical approaches, intervention rationales, and effects. Youth Soc. (2020) 53(5):811–40. doi: 10.1177/0044118X20901735
34. Pulido JJ, Tapia-Serrano MÁ, Díaz-García J, Ponce-Bordón JC, López-Gajardo MÁ. The relationship between students’ physical self-concept and their physical activity levels and sedentary behavior: the role of students’ motivation. Int J Environ Res Public Health. (2021) 18(15):1–14. doi: 10.3390/ijerph18157775
35. Hu D, Zhou S, Crowley-McHattan ZJ, Liu Z. Factors that influence participation in physical activity in school-aged children and adolescents: a systematic review from the social ecological model perspective. Int J Environ Res Public Health. (2021) 18(6):3147. doi: 10.3390/ijerph18063147
36. Martins J, Costa J, Sarmento H, Marques A, Farias C, Onofre M, et al. Adolescents’ perspectives on the barriers and facilitators of physical activity: an updated systematic review of qualitative studies. Int J Environ Res Public Health. (2021) 18(9):4954. doi: 10.3390/ijerph18094954
37. Garcia L, Mendonça G, Benedetti TRB, Borges LJ, Streit IA, Christofoletti M, et al. Barriers and facilitators of domain-specific physical activity: a systematic review of reviews. BMC Public Health. (2022) 22(1):1964. doi: 10.1186/s12889-022-14385-1
38. Ryan RM, Deci EL. Self-determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness. New York: Guilford Publications (2017).
39. Owen KB, Nau T, Reece LJ, Bellew W, Rose C, Bauman A, et al. Fair play? Participation equity in organised sport and physical activity among children and adolescents in high income countries: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. (2022) 19(1):27. doi: 10.1186/s12966-022-01263-7
40. Li R, Bunke S, Psouni E. Attachment relationships and physical activity in adolescents: the mediation role of physical self-concept. Psychol Sport Exerc. (2016) 22:160–9. doi: 10.1016/j.psychsport.2015.07.003
41. Duffey K, Barbosa A, Whiting S, Mendes R, Yordi Aguirre I, Tcymbal A, et al. Barriers and facilitators of physical activity participation in adolescent girls: a systematic review of systematic reviews. Front Public Health. (2021) 9:743935. doi: 10.3389/fpubh.2021.743935
42. Naylor P-J, Nettlefold L, Race D, Hoy C, Ashe MC, Wharf Higgins J, et al. Implementation of school based physical activity interventions: a systematic review. Prev Med. (2015) 72:95–115. doi: 10.1016/j.ypmed.2014.12.034
43. Sallis JF, Cervero RB, Ascher W, Henderson KA, Kraft MK, Kerr J. An ecological approach to creating active living communities. Annu Rev Public Health. (2006) 27:297–322. doi: 10.1146/annurev.publhealth.27.021405.102100
44. Werrij M, Ruiter R, van't Riet J, de Vries H. Message Framing. Writing Health Communication: An Evidence-Based Guide. London, UK: SAGE Publications Ltd. (2012).
45. Maibach EW, Cotton D. A staged social cognitive approach to message design. In: Maibach E, Parrot RL, editors. Designing Health Messages: Approaches from Communication Theory and Public Health. London: SAGE (1995). p. 41–64.
46. Kelder SH, Hoelscher D, Perry CL. How individuals, environments, and health behaviors interact. Health Behav Theory Res Pract. (2015) 159:144–9.
48. Latham GP, Locke EA. New developments in and directions for goal-setting research. Eur Psychol. (2007) 12(4):290–300. doi: 10.1027/1016-9040.12.4.290
49. Valente T. Social networks and health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health Behavior: Theory, Research and Practice. 5th ed. San Francisco, CA: John Wiley & Sons (2015). p. 204–22.
50. Weick KE, Quinn RE. Organizational change and development. Annu Rev Psychol. (1999) 50(1):361–86. doi: 10.1146/annurev.psych.50.1.361
51. Bandura A. Social Foundations of Thought and Action, Vol. 2. Englewood Cliffs, NJ: Prentice-Hall, Inc. (1986). p. 23–8.
52. Kools M, van de Wiel MW, Ruiter RA, Crüts A, Kok G. The effect of graphic organizers on subjective and objective comprehension of a health education text. Health Educ Behav. (2006) 33(6):760–72. doi: 10.1177/1090198106288950
53. McHale F, Ng K, Taylor S, Bengoechea E, Norton C, O’Shea D, et al. A systematic literature review of peer-led strategies for promoting physical activity levels of adolescents. Health Educ Behav. (2021) 49(1):41–53. doi: 10.1177/10901981211044988
54. Papadopoulos N, Mantilla A, Bussey K, Emonson C, Olive L, McGillivray J, et al. Understanding the benefits of brief classroom-based physical activity interventions on primary school-aged children’s enjoyment and subjective wellbeing: a systematic review. J Sch Health. (2022) 92(9):916–32. doi: 10.1111/josh.13196
55. Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. (2016) 2(1):64. doi: 10.1186/s40814-016-0105-8
56. Eriksen BA, Eriksen CW. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept Psychophys. (1974) 16(1):143–9. doi: 10.3758/BF03203267
57. Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. (1935) 18(6):643. doi: 10.1037/h0054651
58. Akyildiz Z, Yildiz M, Clemente FM. The reliability and accuracy of polar team pro GPS units. Proc Inst Mech Eng Part P J Sports Eng Technol. (2022) 236(2):83–9. doi: 10.1177/1754337120976660
59. Migueles JH, Cadenas-Sanchez C, Ekelund U, Delisle Nyström C, Mora-Gonzalez J, Löf M, et al. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: a systematic review and practical considerations. Sports Med. (2017) 47:1821–45. doi: 10.1007/s40279-017-0716-0
60. Bennett H, Parfitt G, Davison K, Eston R. Validity of submaximal step tests to estimate maximal oxygen uptake in healthy adults. Sports Med. (2016) 46:737–50. doi: 10.1007/s40279-015-0445-1
61. Castro-Piñero J, Ortega FB, Artero EG, Girela-Rejón MJ, Mora J, Sjöström M, et al. Assessing muscular strength in youth: usefulness of standing long jump as a general index of muscular fitness. J Strength Cond Res. (2010) 24(7):1810–7. doi: 10.1519/JSC.0b013e3181ddb03d
62. Castro-Piñero J, Artero EG, España-Romero V, Ortega FB, Sjöström M, Suni J, et al. Criterion-related validity of field-based fitness tests in youth: a systematic review. Br J Sports Med. (2010) 44(13):934–43. doi: 10.1136/bjsm.2009.058321
63. Donath L, Roth R, Zahner L, Faude O. Testing single and double limb standing balance performance: comparison of COP path length evaluation between two devices. Gait Posture. (2012) 36(3):439–43. doi: 10.1016/j.gaitpost.2012.04.001
64. Mayorga-Vega D, Merino-Marban R, Viciana J. Criterion-related validity of sit-and-reach tests for estimating hamstring and lumbar extensibility: a meta-analysis. J Sports Sci Med. (2014) 13(1):1–14.24570599
65. Åkerstedt T, Hume K, Minors D, Waterhouse J. The meaning of good sleep: a longitudinal study of polysomnography and subjective sleep quality. J Sleep Res. (1994) 3(3):152–8. doi: 10.1111/j.1365-2869.1994.tb00122.x
66. Ringdal R, Bradley Eilertsen M-E, Bjørnsen HN, Espnes GA, Moksnes UK. Validation of two versions of the warwick-Edinburgh mental well-being scale among Norwegian adolescents. Scand J Public Health. (2018) 46(7):718–25. doi: 10.1177/1403494817735391
67. Sørlie M-A, Nordahl T. Problematferd I Skolen: Hovedfunn, Forklaringer og Pedagogiske Implikasjoner: Hovedrapport fra Forskningsprosjektet” Skole og Samspillsvansker”. Oslo: Norsk institutt for forskning om oppvekst, velferd og aldring (1998).
68. Bandura A. Guide to construction of self-efficacy scales. In: Pajares F, Urdan T, editors. Self-Efficacy Beliefs of Adolescents, Vol. 5. Greenwich, CT: Information Age (2006). p. 307–37.
69. Moos RH, Trickett E. Classroom Environment Scale. Palo Alto, CA: Consulting Psychologists Press (1974).
71. Goldstein H, Scott M, Simonoff J, Marx B. Likelihood estimation in multilevel models. In: Scott MA, Simonoff JS, Marx BD, editors. The SAGE Handbook of Multilevel Modeling. London: SAGE (2013). p. 39–52.
72. Singer JD. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence. New York: Oxford university press (2003).
75. Faul F, Erdfelder E, Lang A-G, Buchner A. G*power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39(2):175–91. doi: 10.3758/BF03193146
76. Masini A, Ceciliani A, Dallolio L, Gori D, Marini S. Evaluation of feasibility, effectiveness, and sustainability of school-based physical activity “active break” interventions in pre-adolescent and adolescent students: a systematic review. Can J Public Health. (2022) 113(5):713–25. doi: 10.17269/s41997-022-00652-6
77. Carrasco-Uribarren A, Ortega-Martínez A, Amor-Barbosa M, Cadellans-Arróniz A, Cabanillas-Barea S, Bagur-Calafat MC. Improvement of in-school physical activity with active school-based interventions to interrupt prolonged sitting: a systematic review and meta-analysis. Int J Environ Res Public Health. (2023) 20(2):1636. doi: 10.3390/ijerph20021636
78. Alalawi A, Blank L, Goyder E. Umbrella review of international evidence for the effectiveness of school-based physical activity interventions. PLoS One. (2024) 19(6):e0304513. doi: 10.1371/journal.pone.0304513
79. Melguizo-Ibáñez E, Zurita-Ortega F, González-Valero G, Puertas-Molero P, Tadeu P, Ubago-Jiménez JL, et al. Active break as a tool for improving attention in the educational context. A systematic review and meta-analysis. Rev Psicodidáct (English ed). (2024) 29(2):147–57. doi: 10.1016/j.psicoe.2024.02.003
80. Muntaner-Mas A, Morales JS, Martínez-de-Quel Ó, Lubans DR, García-Hermoso A. Acute effect of physical activity on academic outcomes in school-aged youth: a systematic review and multivariate meta-analysis. Scand J Med Sci Sports. (2024) 34(1):e14479. doi: 10.1111/sms.14479
81. Chim HQ, Gijselaers HJM, de Groot RHM, Van Gerven PWM, oude Egbrink MGA, Savelberg HHCM. The effects of light physical activity on learning in adolescents: a systematic review. Int Rev Sport Exerc Psychol. (2024) 17(1):291–318. doi: 10.1080/1750984X.2021.2001837
82. Bermejo-Cantarero A, Sánchez-López M, Álvarez-Bueno C, Redondo-Tébar A, García-Hermoso A, Martínez-Vizcaino V. Are physical activity interventions effective in improving health-related quality of life in children and adolescents? A systematic review and meta-analysis. Sports Health. (2023) 0(0):19417381231190885. doi: 10.1177/19417381231190885
83. Rico-González M. The effect of primary school-based physical education programs: a systematic review of randomized controlled trials. J Phys Act Health. (2023) 20(4):317–47 (English). doi: 10.1123/jpah.2022-0452
84. Carlson JA, Engelberg JK, Cain KL, Conway TL, Mignano AM, Bonilla EA, et al. Implementing classroom physical activity breaks: associations with student physical activity and classroom behavior. Prev Med. (2015) 81:67–72. doi: 10.1016/j.ypmed.2015.08.006
85. Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet. (2012) 380(9838):272–81. doi: 10.1016/s0140-6736(12)60816-2
86. Watson R, Atkinson I, Egerton P. Successful Statistics for Nursing and Healthcare. New York: Bloomsbury Publishing (2017).
87. Ryan RM, Deci EL, Vansteenkiste M, Soenens B. Building a science of motivated persons: self-determination theory’s empirical approach to human experience and the regulation of behavior. Motiv Sci. (2021) 7(2):97–110. doi: 10.1037/mot0000194
88. Christiansen LB, Clausen K, Smedegaard S, Skovgaard T. A qualitative exploration of implementation, adaptation, and sustainability of a school-based physical activity intervention: move for well-being in school. Sage Open. (2021) 11(1):21582440211000053. doi: 10.1177/21582440211000053
89. Durlak JA, Mahoney JL, Boyle AE. What we know, and what we need to find out about universal, school-based social and emotional learning programs for children and adolescents: a review of meta-analyses and directions for future research. Psychol Bull. (2022) 148(11–12):765. doi: 10.1037/bul0000383
90. Tudor K, Maloney S, Raja A, Baer R, Blakemore S-J, Byford S, et al. Universal mindfulness training in schools for adolescents: a scoping review and conceptual model of moderators, mediators, and implementation factors. Prev Sci. (2022) 23(6):934–53. doi: 10.1007/s11121-022-01361-9
91. Tuhkala A. A systematic literature review of participatory design studies involving teachers. Eur J Educ. (2021) 56(4):641–59. doi: 10.1111/ejed.12471
92. Christodoulakis A, Bouloukaki I, Aravantinou-Karlatou A, Margetaki K, Zografakis-Sfakianakis M, Tsiligianni I. The effectiveness of teaching the teacher interventions in improving the physical activity among adolescents in schools: a scoping review. Healthcare. (2024) 12(2):151. doi: 10.3390/healthcare12020151
Keywords: school-based physical activity, intervention mapping, health promotion, high school, adolescents
Citation: Barene S, Johansen PF, Tjomsland HE, Ølberg RI and Thurston M (2025) Applying intervention mapping to develop a program for promoting short physical activity breaks during class time in upper secondary schools: the MOVE12 protocol study. Front. Sports Act. Living 6:1460373. doi: 10.3389/fspor.2024.1460373
Received: 6 July 2024; Accepted: 27 December 2024;
Published: 13 January 2025.
Edited by:
Luca Petrigna, University of Catania, ItalyReviewed by:
Richard Peter Bailey, UCSI University, MalaysiaCopyright: © 2025 Barene, Johansen, Tjomsland, Ølberg and Thurston. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Svein Barene, c3ZlaW4uYmFyZW5lQGlubi5ubw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.