 René Schilling1*
René Schilling1* Robyn Cody1
Robyn Cody1 Jan-Niklas Kreppke1
Jan-Niklas Kreppke1 Oliver Faude1
Oliver Faude1 Johannes Beck2
Johannes Beck2 Serge Brand1,3,4,5,6
Serge Brand1,3,4,5,6 Lars Donath7
Lars Donath7 Martin Hatzinger8
Martin Hatzinger8 Christian Imboden9,10Undine Lang11Sarah Mans9
Christian Imboden9,10Undine Lang11Sarah Mans9 Thorsten Mikoteit8Anja Oswald2Nina Schweinfurth-Keck3
Thorsten Mikoteit8Anja Oswald2Nina Schweinfurth-Keck3 Markus Gerber1
Markus Gerber1
- 1Department of Sport, Exercise and Health, University of Basel, Basel, Switzerland
- 2Psychiatric Clinic Sonnenhalde, Riehen, Switzerland
- 3Center for Affective, Stress and Sleep Disorders (ZASS), Psychiatric University Hospital of the University of Basel, Basel, Switzerland
- 4Sleep Disorders Research Center, Kermanshah University of Medical Sciences (KUMS), Kermanshah, Iran
- 5Substance Abuse Prevention Research Center, Kermanshah University of Medical Sciences (KUMS), Kermanshah, Iran
- 6School of Medicine, Tehran University of Medical Sciences, Tehran, Iran
- 7Department of Training Intervention Research, German Sport University Cologne, Cologne, Germany
- 8Psychiatric Services Solothurn and Faculty of Medicine, University of Basel, Solothurn, Switzerland
- 9Private Clinic Wyss, Münchenbuchsee, Switzerland
- 10Translational Research Center, University Hospital of Psychiatry and Psychotherapy, University of Bern, Bern, Switzerland
- 11Adult Psychiatric Clinics (UPKE), University of Basel, Basel, Switzerland
Introduction: Major depressive disorders (MDD) are a leading health concern worldwide. While first line medication treatments may fall short of desired therapeutic outcomes, physical activity (PA) interventions appear to be a promising and cost-effective add-on to improve symptoms of depression. This study aimed to address challenges in the assessment of PA in inpatients treated for MDD by examining the correspondence of self-reported and accelerometer-based PA.
Methods: In 178 inpatients treated for MDD (mean age: M = 41.11 years, SD = 12.84; 45.5% female) and 97 non-depressed controls (mean age: M = 35.24 years, SD = 13.40; 36.1% female), we assessed self-reported PA via the Simple Physical Activity Questionnaire (SIMPAQ) for one week, followed by a week where PA was monitored using an accelerometer device (Actigraph wGT3x-BT). Additionally, we examined correlations between PA levels assessed with the SIMPAQ and exercise determinants in both groups.
Results: Descriptively, inpatients treated for MDD showed lower levels of light PA on accelerometer-based measures, whereas they self-reported increased levels of certain types of PA on the SIMPAQ. More importantly, there was only a small degree of correspondence between self-reported and actigraphy-based PA levels in both in patients (r = 0.15, p < 0.05) and controls (r = 0.03, ns). Only few significant correlations were found for self-reported PA (SIMPAQ subscores) and perceived fitness, whereas self-reported PA and estimated VO2max were unrelated. Furthermore, only weak (and mostly statistically non-significant) correlations were found between exercise determinants and SIMPAQ-based exercise behavior in both populations.
Discussion: Our findings emphasize the intricate challenges in the assessment of PA, not only in inpatients treated for MDD, but also in non-depressed controls. Our findings also underline the necessity for a diversified data assessment. Further efforts are needed to refine and improve PA questionnaires for a more accurate data assessment in psychiatric patients and healthy controls.
1 Introduction
Major depressive disorders (MDD) are a leading health concern, ranking second in terms of years lost due to disability or premature death (DALY), and topping the list for years lived with disability for both genders, as outlined by the World Health Organization (1). As the prevalence of MDD escalates (2), the financial implications are felt profoundly, with tremendous treatment costs (3). The increasing burden of MDD underscores an urgent need for effective interventions.
Physical activity (PA) has been substantiated as a cost-effective and impactful intervention for ameliorating symptoms of depression, with effects comparable to that of antidepressants and psychotherapy (4, 5). Meta-analytical data reinforce these findings, with evidence of moderate to large significant effects of exercise training on reducing depressive symptoms compared to control conditions (6). Specific studies have shown that aerobic exercise for as little as 30 min a day over 10 days can produce substantial improvements in mood in patients with MDD (7).
PA plays a crucial role in mitigating the morbidity and mortality associated with MDD. Depressive symptoms have been associated with an increased mortality risk, a relationship partially explained by factors such as physical inactivity, physical illnesses, and impairments in physical and cognitive functioning (8). In older adults with depressive symptoms, physical inactivity significantly elevates the risk of cardiovascular mortality, regardless of coronary heart disease status (9).
Furthermore, patients with MDD exhibit altered autonomic function during resting conditions, exercise, and recovery from exercise, which may influence their cardiovascular morbidity and mortality (10). PA, particularly (regular) aerobic exercise, such as walking or cycling, performed at moderate intensity for at least 30 min per session, three to five times a week, can enhance the neuroprotective effect of antidepressants, potentially preventing cardiovascular diseases in patients with MDD (11). Exercise-based interventions have also been effective in reducing cardiovascular risk and mortality in depressed populations, while simultaneously improving depressive symptoms (12).
Studies indicate that PA, both as a stand-alone and as an add-on to standard treatment, is effective in reducing depressive symptoms. For instance, Blumenthal and colleagues (13, 14) showed significant improvements in depressive symptoms with exercise intervention. Dunn et al. (15) also found that exercise has a dose-response effect on depression symptoms.
Additionally, PA as an add-on to standard treatment has been shown to enhance treatment outcomes. Schuch et al. (16) reported preliminary results indicating that exercise can be an effective add-on treatment for severe depression. Imboden and colleagues (17) found similar antidepressant effects for aerobic exercise and stretching when added to inpatient treatment, with larger effects on working memory for aerobic exercise alone. Furthermore, Ravindran and da Silva (18) highlighted the benefits of complementary and alternative therapies, including exercise, as add-ons to pharmacotherapy for mood and anxiety disorders.
In sum, PA, including exercise and sport, emerges as a cost-effective and impactful add-on intervention to improve symptoms of depression beyond standard treatment (19, 20). Research indicates that combining PA with standard treatment results in a greater effect size compared to either treatment alone, making this combined approach more effective in reducing depressive symptoms and improving overall health outcomes (21).
While there are many tools available to assess PA (22), challenges remain in their application to specific populations such as those with MDD. In light of this, the importance of accurate assessment tools for PA within the MDD patient population has been emphasized (20). The current lack of stratification tools for the risk of physical inactivity is believed to pose a significant obstacle for clinicians to assess PA and plan specific interventions and coaching to improve PA and exercise participation (23). For clinicians, it is important to have access to brief and precise measures to monitor health factors over time, particularly as patients tend to be more compliant (24), report less missing data or errors due to fatigue or frustration (25) when assessment tools are less time-consuming.
PA is most commonly assessed via accelerometers and questionnaires (26, 27). While accelerometers provide objective data on PA behavior, they are unable to assess the context of PA and certain movements such as rowing, weight lifting, and bike riding. There is also a risk of measurement error due to non-wear time. Additionally, accelerometers are costlier than questionnaires, and they pose a higher burden for patients (wear time between days and weeks; personal privacy) as well as for clinicians, who need time and training to analyze the data. Accordingly, accelerometry is still not used very often in clinical practice (28–30). Questionnaires, on the other hand, are easy to use and bear relatively low costs (31). However, they rely on the respondent's ability to accurately recall the behavior of interest, a capability which may be impaired in patients with MDD (32). There is also a risk that data are biased due to social desirability. The poor agreement between the IPAQ (International Physical Activity Questionnaire) and ActiGraph data, as previously reported by do Nascimento et al. (33), highlights a significant gap in current assessment methodologies. It should also be noted that no distinction has been made in previous meta-analyses between device-based and self-reported PA when looking at the potential of PA to reduce the risk of mental illnesses, thus assuming that there is a sufficient degree of correspondence between both assessment techniques (34, 35).
Given this background, the aim of this paper is to address this research gap by examining the correspondence between self-reported and device-based PA measures in patients with MDD. More specifically, this paper will (i) examine in inpatients treated for MDD and non-depressed controls whether and to what degree self-reported PA (assessed via SIMPAQ) would be associated with accelerometer-based PA, (ii) explore how self-reported PA correlates with perceived fitness and estimated VO2max, and (iii) examine the relationships between SIMPAQ-based exercise behavior and selected cognitive exercise determinants including exercise-based self-efficacy, outcome expectancies, exercise intention, and intrinsic exercise motivation. The present study adds to the current literature in so far that few studies have provided data regarding the correspondence of the SIMPAQ with objective measures of PA. It should also be noted that most PA questionnaires have been tested in healthy and active populations (27), whereas in the present study, we focused on inpatients treated for MDD and initially insufficiently physically active individuals.
In a previous study with college students, we demonstrated a moderate-to-high correlation between the SIMPAQ and accelerometer data (r = 0.30–0.70) (36). In a separate study involving 1,010 participants with mental illness, the SIMPAQ exhibited good test-retest reliability (r = 0.63–0.76). Regarding MVPA, the overall correlation with accelerometer-based data was r = 0.25, with the correlation being lower for inpatients (r = 0.09) compared to outpatients (r = 0.43) (23). In another study, the SIMPAQ demonstrated sensitivity in detecting changes resulting from a PA counselling intervention (37).
As stated above, the ability to recall behavior accurately may be impaired to some degree in inpatients with MDD (32). Regarding our hypotheses, we took this finding into consideration, as well as previous evidence based on participants with MDD (33), and healthy samples, in which the SIMPAQ has been applied (36). As a consequence, we formulated the following cautious hypothesis:
We expected weak to moderate correlations between self-reported (SIMPAQ-based) and accelerometer-based PA in both inpatients treated for MDD and non-depressed controls (Hypothesis 1) (23, 32, 33). We further hypothesized that self-reported PA would be positively associated with perceived fitness and estimated VO2max (Hypothesis 2) (38). Finally, we assumed that the SIMPAQ (particularly the exercise/sport subscore) would be moderately correlated with cognitive exercise determinants such as self-efficacy, positive outcome expectancies, exercise intention, and intrinsic exercise motivation (Hypothesis 3) (39, 40).
2 Methods
2.1 Design
The present paper was based on baseline data from a multi-centric, two-arm randomized controlled trial (RCT), including an intervention group (extended personalized PA and exercise counselling program), a placebo control group (general instructions about health-enhancing PA) (19), and a non-depressed control group (being invited to the baseline assessments only). The study was initiated by the Department of Sport, Exercise and Health of the University of Basel, and carried out in cooperation with four Swiss psychiatric clinics (2 public, 2 private).
2.2 Participants
Recruitment lasted from June 2019 to October 2021. Based on a structured clinical interview conducted by two trained researchers, all inpatients fulfilled ICD-10 diagnosis for single episode (F32), recurrent MDD (F33) or bipolar disorder type II (F31.80). As part of the screening process, the 17-item Hamilton Depression Rating Scale (HAMD17) (41) was applied by a trained staff member, whereas inpatients completed the 21-item Beck Depression Inventory-II (BDI-II) (42, 43) to assess symptom severity. Information on PA during the last week before entering the clinic was collected via the short version of the International Physical Activity Questionnaire (IPAQ) (44). To be eligible for the present study, inpatients had to meet the following inclusion criteria: (a) inpatients treated for depression on a specialized ward at one of the study centers, (b) 18–65 years of age, (c) presence of MDD according to ICD-10 diagnostic criteria, (d) BDI ≥17 (at least self-rated moderate MDD), (e) current PA level assessed via IPAQ of less than 150 min/week of moderate-to-vigorous PA (MVPA), (f) signed written informed consent, and (g) ability to speak and read German and to comply with the study conditions. A sample of non-depressed controls was recruited via advertisements in newspapers and word-of-mouth recommendation. For non-depressed controls, the following inclusion criteria were considered: (a) 18–65 years of age, (c) HAMD17 ≤7, (d) BDI ≤13, (e) current MVPA level of less than 150 min/week (IPAQ), (f) written informed consent, and (g) ability to speak and read German.
In total, 210 inpatients and 125 non-depressed controls met all inclusion criteria and provided SIMPAQ and accelerometer-based data at baseline. The study was reviewed by the competent ethics committee (Ethikkommission Nordwest- und Zentralschweiz; ref approval no. 2018–00976) and all procedures were in line with the ethical principles of the Declaration of Helsinki. The intervention study was registered in the WHO trial register (trial number: ISRCTN10469580). Participants received information about the general goals of the study and provided informed written consent before study entry. Participation in the study was voluntary and withdrawal or discontinuation possible at any time.
2.3 Data assessment and measures
Screening of inpatients took place in the first week after admission to inpatient treatment, baseline data assessment after 2–3 weeks after admission in one of the four involved clinics. All assessment procedures for the here presented data were identical for the entire sample. Two distinct assessment methods were employed to evaluate PA over two consecutive weeks: initially, participants self-reported their activity for the past week via the SIMPAQ, followed by a week where their PA was monitored via accelerometer device. In the following, we describe the assessments socio-demographic background, depressive symptom severity, self-reported PA, accelerometer-based PA, perceived fitness, estimated VO2max, exercise-based self-efficacy and outcome expectancies, exercise intention, and intrinsic exercise motivation.
2.3.1 Sociodemographic characteristics
Participants reported on their gender at birth (male; female), age (years), civil status (single; married/in a partnership), nationality, highest level of education (none; obligatory schooling; apprenticeship; occupational training; high school; technical college/university; other); current employment status (employed; unemployed; retired), duration of employment (years), living with children (yes; no), and current smoking status (yes; no). For the assessment of body weight, a digital weighing scale (BC-545, Tanita, USA) was used (to the nearest 0.1 kg, in light cloths and without shoes). For the assessment of body height, a stadiometer (to the nearest 0.5 cm, without shoes) was used. Body Mass Index (BMI) was calculated as: weight (kg)/height (m2).
2.3.2 Self-reported depressive symptom severity
Depressive symptom severity was assessed with the 21-item Beck Depression Inventory-II (BDI-II) (42, 43). The Beck Depression Inventory-II (BDI-II) is a widely utilized 21-item tool (42) designed to measure unipolar depression symptoms, including affective, cognitive, behavioral, and somatic aspects (e.g., “I am so unhappy/sad that I can't stand it”). Each item is rated on a scale from 0 to 3, indicating progressively severe symptoms of depression. Scores on the BDI-II can vary from 0 to 63, where a higher score reflects more severe depressive symptoms. The reliability and validity of this instrument have been well-documented in prior research (45). This study involved the comparison of three patient groups categorized by depression severity into mild (BDI-II scores of 0–19), moderate (BDI-II scores of 20–28), and severe (BDI-II scores of 29–63) depression, in line with established categories of depression severity (46).
2.3.3 Self-reported physical activity
To assess self-reported PA, we employed the five-item Simple Physical Activity Questionnaire (SIMPAQ), a relatively new tool tailor-made for psychiatric patients (47). The SIMPAQ evaluated the average daily time spent in various physical activities over the preceding 7 days, referring to all domains of activity, including leisure, work, domestic, and transportation-related activities. Five items asked for participants' time (in hours) spent in bed, sitting, walking, participating in sports, and engaging in other activities, cumulatively approximating 24 h per day. Time spent walking and time spent exercising were combined to estimate total MVPA (23). To facilitate a more accurate comparison with the accelerometer data, we converted the daily time spent in various activities into minutes per week.
2.3.4 Accelerometer-based physical activity
Accelerometer-based PA was assessed via an Actigraph wGT3x-BT device (Shalimar, FL, USA), positioned around the hip. Participants wore the device for seven successive days to capture an entire week. The sampling frequency was 60 Hertz (48). The raw data was processed with the ActiLife software V.6.13.4 (ActiLife, Shalimar, FL, USA). We used cut-off based analysis with defined cut-points in counts per minute (cpm) for MVPA (49).
For the cut-off based evaluation, we used an epoch length of 60 s epochs (50). We applied the following cut-points to assess the time spent in different activity categories: sedentary activity was defined as less than 610 counts per minute (cpm), light PA ranged from 611 to 2,689 cpm, moderate PA spanned from 2,690 to 6,166 cpm, vigorous PA from 6,167 to 9,642 cpm, and very vigorous PA was categorized as exceeding 9,643 cpm (49, 51). Whenever participants could not wear the monitor, like during swimming, they recorded the activity in a separate non-wear time sheet. Activities mentioned were classified as MVPA based on criteria from the PA compendium (52, 53). For the data to be considered for analysis, participants had to record a minimum of four days, comprising at least three weekdays and one weekend day (54). As per Herrmann et al. (55), only recordings with 8 h or more were deemed valid. The accuracy of the Actigraph devices has been documented in prior research (56).
2.3.5 Perceived fitness
Participants rated their perceived fitness using a singular item (57). The question was: “How would you describe your physical condition?” They could select a score ranging from 1 (very poor) to 10 (excellent). This item's validity as a fitness perception indicator was backed by its high correlation with the 12-item Perceived Physical Fitness scale (58). It also showcased associations with objective fitness markers, well-being perceptions, and sleep patterns (57, 58).
2.3.6 Cardiorespiratory fitness
Cardiorespiratory fitness (CRF) was estimated with the Åstrand indirect test of maximal oxygen uptake (59). The test was performed on a bicycle ergometer (Technogym, Bike Forma) at the same time of the day (starting between 8 and 10 am). The pedalling frequency was set at 50 revolutions per minute (rpm), while the workload was adjusted so that the heart rate was kept between 130 and 160 beats per minute (bpm) in participants younger than 40 years old and between 120 and 150 bpm in participants older than 40 years old. The Borg Rating of Perceived Exertion scale (60) was used to ensure that participants maintain their exercise intensity level at 13 or 14 (slightly strenuous). Following stabilization of heart rate after 5 or 6 min, maximal oxygen uptake (L/min) was estimated based on mean steady-state, sex and power-output, using a nomogram (59) and including a correction factor for age. Maximal oxygen uptake was expressed as VO2max (ml/kg/min), after correction of body weight. Previous studies have demonstrated the reliability and validity of the Åstrand nomogram and the linear extrapolation for deriving VO2max (61). We applied the following formula instead of the nomogram: for men: VO2max = [(0.00212 × workload × 6.12 + 0.299)/(0.769 × heart rate−48.5) × 100] × 1,000/weight/age correction factor; for women: VO2max = [(0.00193 × workload × 6.12 + 0.326)/(0.769 × heart rate−56.1) × 100] × 1,000/weight/age correction factor (62). This formula is based on sex, workload, and mean steady-state value of heart rate and is corrected for weight and age. Maximal oxygen uptake is expressed relative to body mass (ml/min/kg). Participants using beta-blockers at the time of the assessments (inpatients: n = 13, non-depressed controls: n = 2) were excluded from the analysis (63).
2.3.7 Exercise-based self-efficacy
A trio of items touched upon starting, sustaining, and resuming exercise post-relapse, aiming to gauge self-efficacy in relation to exercise (e.g., “I feel confident to start with a new exercise activity”) (64). The answers ranged from 0 (not at all confident) to 5 (100% confident in myself). The three items were combined into a single (mean) score, with higher scores indicating greater self-efficacy. This scale proved to be psychometrically sound in previous studies (64) and was incorporated in prior intervention research (65–67).
2.3.8 Exercise-based outcome expectancies
To assess exercise outcome expectancies, we used nine positively phrased (“pros”) and seven negatively framed items (“cons”) (68). These items, rated on a scale of 1 (not true) to 4 (completely true), were combined to form two distinct (mean) scores. This tool proved to have sound psychometric properties in previous research (68).
2.3.9 Exercise intention
Exercise intention in the forthcoming weeks was assessed with the item “Strength of my intention to exercise regularly during the next few weeks and months”, with response options ranging from 0 (no intention) to 5 (very strong intention) (65, 69), and higher scores reflecting a stronger intention.
2.3.10 Intrinsic exercise motivation
Intrinsic exercise motivation was assessed with the referring subscale of the self-concordance scale (SSK-scale) (69). The scale aligns with Sheldon and Elliot's self-concordance model (70). Three items were used to assess intrinsic motivation. Answered were provided on a scale from 1 (not at all true) to 6 (completely true).
2.4 Statistical analyses
SIMPAQ data were checked for univariate outliers, defined at >3 standard deviations below/above the mean (71). Univariate outliers were excluded from all further analyses. Kolmogorov-Smirnov tests were used to test normality of the data. In the results section, we first present descriptive statistics to describe the characteristics of the sample and the level of self-reported and accelerometer-based PA. Given the non-normal distribution of some parameters, Spearman correlation analyses were used to examine pairwise associations between self-reported and accelerometer-based PA (controlling for accelerometer wear-time). Spearman correlations were also used to examine bivariate relationships between the SIMPAQ subscales, perceived fitness, estimated VO2max, exercise-based self-efficacy and outcome expectancies, exercise intention, and intrinsic exercise motivation. All correlation analyses were performed separately in inpatients treated for MDD and non-depressed controls, and within each sample, separate analyses were run for women and men. Following the recommendations of Cohen (72), correlations of rho <0.30 were considered small, with rho = 0.30–0.50 as medium and rho >0.50 as large. All analyses were performed with SPSS Statistics 23 for Windows (IBM Corporation, Armonk NY, USA) and the level of significance was set at p < 0.05 across all analyses.
3 Results
3.1 Sample characteristics of inpatients treated for MDD and non-depressed controls
41 participants (16 inpatients treated for MDD and 25 non-depressed controls) were identified as univariate outliers (>3 standard deviations below/above the mean of each SIMPAQ category). Furthermore, 43 participants did not have valid accelerometer data. Among the non-depressed controls, 17 had excessively high depression scores. Additionally, 5 participants (across both groups) did not provide valid BDI scores. After these exclusions, the sample was comprised of 178 inpatients treated for MDD and 97 non-depressed controls. Table 1 provides an overview of the sample characteristics for the total sample, inpatients and non-depressed controls. Both groups had a similar distribution of gender: 45.5% inpatients treated for MDD were female, compared to 36.1% in the non-depressed control group. The average age was 39.04 years (SD = 13.31), with inpatients being significantly older than non-depressed controls (mean age 41.11 years, SD = 12.84, compared to 35.24 years, SD = 13.40). The majority spoke German as their first language (85.8%), identified as Swiss nationals (77.8%), and were single (69.8%). Within the inpatient group, 34.3% had a first-episode MDD diagnosis (F32), 64.0% had recurrent MDD (F33 diagnosis), and 1.7% were diagnosed with bipolar disorder type II (F31.80). Notably, 162 inpatients were on antidepressants (no controls were on antidepressant medication). All participants met the screening criteria for self-reported insufficient PA; however, at baseline, 162 participants accumulated 150 min or more of accelerometer-based MVPA per week.
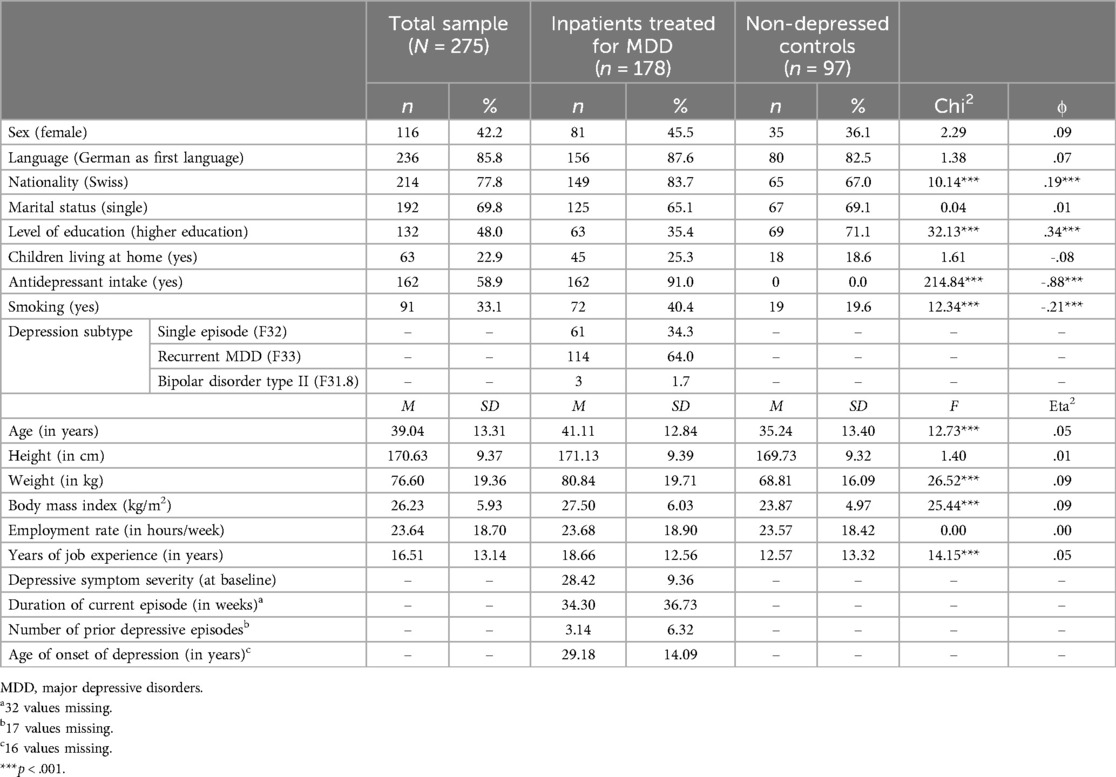
Table 1. Sample characteristics.
3.2 Descriptive statistics for inpatients treated for MDD and non-depressed controls
Table 2 presents the descriptive statistics for self-reported PA, accelerometer-based PA, self-perceived fitness, and estimated VO2max, exercise-related self-efficacy and outcome expectancies, exercise intention, intrinsic exercise motivation, separately for inpatients treated for MDD, non-depressed controls. In view of the fact that the two groups were assessed in different life circumstances (inpatients: during hospitalisation with structured therapy; controls: in their natural environment), we deliberately refrained from using inferential statistics to calculate differences.
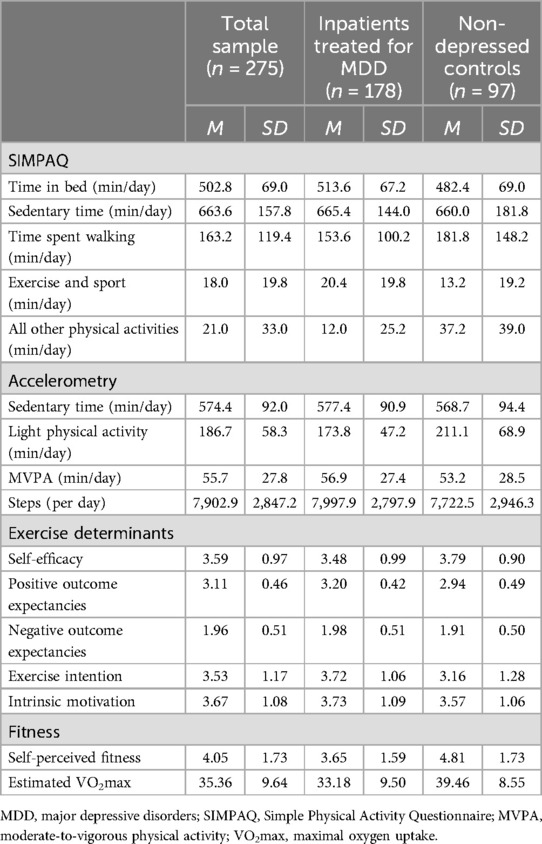
Table 2. Descriptive statistics for inpatients treated for MDD and non-depressed controls in main study variables.
3.3 Correspondence of SIMPAQ with accelerometer-based physical activity
Table 3 displays the bivariate correlations between SIMPAQ subscores and accelerometer-based PA for the total sample, inpatients treated for MDD and non-depressed controls. Broadly speaking, correlations between the SIMPAQ subscores and accelerometer-based PA were ranging from non-existent (zero) to moderate, with correlations only marginally differing between inpatients treated for MDD and non-depressed controls.
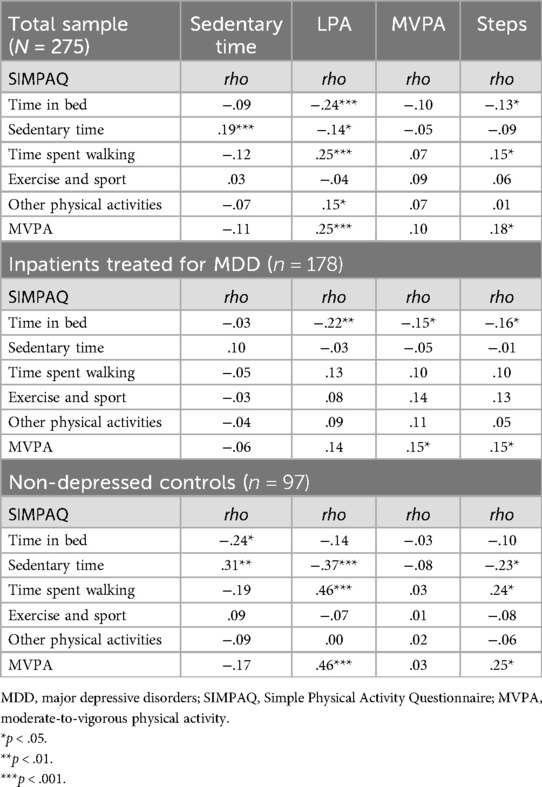
Table 3. Spearman correlations between SIMPAQ measures and accelerometer data for the total sample, and separately for inpatients treated for MDD and non-depressed controls.
For the total sample, correlations were small and mostly non-significant. There was a small significant positive correlation between sedentary time score from both measures. Similarly, time spent walking, as assessed with the SIMPAQ, correlated positively with accelerometer-based light PA. Accelerometer-based MVPA was not associated with any of the SIMPAQ subscores. Finally, two small positive correlations were found for accelerometer-based steps and the two SIMPAQ subscores “walking” and “MVPA”.
For inpatients, SIMPAQ-based time spent in bed correlated negatively with accelerometer-based LPA, MVPA and steps. Furthermore, SIMPAQ-based MVPA correlated positively (but weakly) with accelerometer-based MVPA and steps. All other correlations were not statistically significant.
For the non-depressed controls, two positive correlations were found between SIMPAQ-based subscores “walking” and “MVPA” and accelerometer-based light PA. Against our expectations, accelerometer-based MVPA was not associated with any of the SIMPAQ subscores. Finally, accelerometer-based steps correlated positively (but weakly) with the SIMPAQ-based “walking” and “MVPA”.
In summary, few statistically significant and only weak-to-moderate correlations were found between self-reported (SIMPAQ-based) and accelerometer-based PA indicators. Especially, only a low level of correspondence was observed between the SIMPAQ and accelerometer-based MVPA.
3.4 Correlations of SIMPAQ subscores with fitness measures
Table 4 presents the bivariate correlations between SIMPAQ subscores and self-perceived fitness, and estimated VO2max, for the total sample and separately for inpatients treated for MDD and non-depressed controls. In the total sample, a weak positive correlation was found between SIMPAQ-based MVPA and perceived fitness, whereas in both subpopulations, a weak positive correlation occurred between SIMPAQ-based exercise/sport and perceived fitness. Estimated VO2max was not correlated with any of the SIMPAQ subscores.
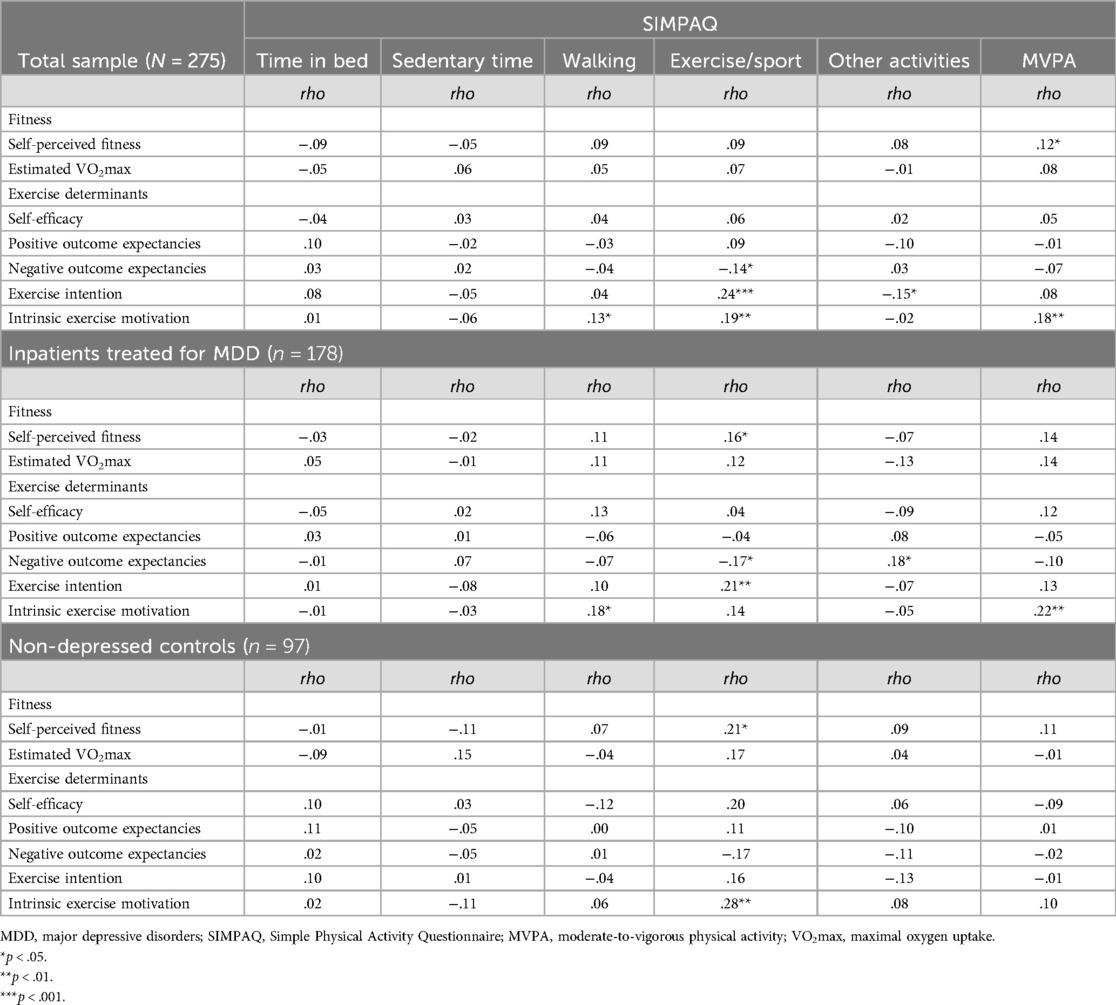
Table 4. Spearman correlations between SIMPAQ measures, fitness measures, and exercise determinants for the total sample, inpatients treated for MDD and non-depressed controls.
3.5 Correlations of SIMPAQ subscores with exercise determinants
Table 4 presents the bivariate correlations between SIMPAQ subscores and exercise determinants. Overall, only few statistically significant correlations were found. In inpatients, SIMPAQ-based exercise/sport correlated negatively with negative outcome expectancies and positively with exercise intention. SIMPAQ-based MVPA was associated with intrinsic exercise motivation. However, all three correlations were weak. In non-depressed controls, a positive but weak correlation was found between SIMPAQ-based exercise/sport and intrinsic exercise motivation. All other correlations were not statistically significant.
4 Discussion
This study aimed to address challenges in the assessment of PA. Therefore, we examined the correspondence between self-reported (SIMPAQ-based) and accelerometer-based PA in inpatients treated for MDD and non-depressed controls. We further examined the association between SIMPAQ-based PA, fitness measures and exercise determinants.
The key findings of the present study are that the subsequently assessed self-reported and accelerometer-based PA were only weakly associated with each other in both subpopulations. This result underscores the potential discrepancy between self-reported and device-based PA levels, especially within the MDD context (32, 73, 74). This finding is in line with previous research (33), highlighting the need for further research in accurate assessment tools for inpatients treated with MDD or non-depressed individuals with initially low PA levels.
Three hypotheses were formulated and each of them will now be addressed in turn. Hypothesis 1 expected weak-to-moderate relationships between self-reported and accelerometer-based PA in inpatients treated for MDD and non-depressed controls. Although some significant correlations occurred, our data did not support this hypothesis. Overall, there was a very poor correspondence between self-reported and accelerometer-based PA measures in both populations. Among inpatients, the reasons for these discrepancies with self-report measures might be attributable to cognitive biases associated with depression (32), including self-regulatory effects (75, 76). However, a similar pattern was observed in non-depressed controls, which is at odds with a previous study with a more physically active population (exercise and sport students), in which higher correlations were found between the SIMPAQ and the same accelerometer devices (36). It is thus possible that the SIMPAQ works better in people with higher PA levels; however, it is also possible that the higher level of agreement is due to the fact that in the study by Schilling et al. (36) the two assessments periods were fully in line, whereas in our study the two instruments were used one week apart. In the present study, this methodological issue probably had a stronger influence on the control group, as PA behavior may fluctuate more in a natural environment. The effect should be less significant in inpatients, as their everyday life is more structured due to the therapy programmes and often includes structured sport and exercise activities (77, 78).
Only limited support was found for our second hypothesis, which expected positive associations between self-reported PA and perceived fitness as well as estimated VO2max. Thus, few statistically significant associations were found between SIMPAQ subscores and perceived fitness, whereas SIMPAQ subscores and estimated VO2max were fully unrelated. Studies have shown that objective fitness measures, such as VO2max, often show low correlations with subjective fitness parameters (79). This discrepancy is particularly evident in populations with depression, where negative cognitive biases can distort self-assessments of fitness despite regular PA. Research suggests that cognitive factors like processing speed and working memory significantly influence how individuals perceive their health and fitness, highlighting the importance of considering cognitive processes in the evaluation and improvement of self-perceived fitness (80). Hypothesis 3 anticipated that some SIMPAQ measures (especially the “exercise/sport” subscore) would be associated with cognitive determinants of exercise behavior, such as exercise-related self-efficacy, outcome expectancies, exercise intention, and intrinsic motivation towards exercise. While some expected relationships emerged, others did not. Moreover, the strength of the associations was weak at best. Notably, self-efficacy and positive outcome expectancies were not associated with SIMPAQ-based PA and exercise behaviour across both groups. The missing relationship between self-efficacy and PA behavior in inpatients treated for MDD underscores the potential need for future research to differentiate subtypes of self-efficacy (task, maintenance and recovery self-efficacy) (81). Regarding outcome expectancies, there is no consensus in the literature. While some studies indicate that depressed individuals have lower positive outcome expectancies compared to non-depressed individuals (82), others suggest they actually exhibit reduced negative outcome expectancies, instead (81). Descriptively, inpatients treated for MDD reported higher levels of positive outcome expectancies compared to non-depressed controls in the present study. However, between-group differences must be interpreted with utmost caution as they may be attributable to a selection bias (in our study, all inpatients were willing to take part in a PA counselling intervention). As expected, in inpatients treated for MDD, stronger exercise intentions correlated positively with self-reported exercise and sport. By contrast, it is intriguing to note that their intrinsic motivation for exercise was not significantly correlated with their exercise and sport behavior (which was the case in non-depressed controls). This observation might be due to the fact that inpatients were assessed in a clinical setting, in which some exercise and sport activities are prescribed by a physician. As a result, participation in these activities might be based more on extrinsic than intrinsic motivation.
Several potential limitations of the current study are worth noting. Firstly, the findings may not be generalizable to the broader population of patients with MDD (e.g., outpatients). Secondly, as mentioned above, the measurement periods for the two instruments, SIMPAQ and accelerometers, were not fully synchronised. Thus, accelerometer-based data were prospectively gathered, whereas the SIMPAQ focused on PA patterns during the last week, as they were carried out on two consecutive weeks. This might have reduced the level of correspondence between the two measures, and explain why correlations were smaller than in previous validation studies. However, in research and clinical practice, both measures are used to assess habitual PA behavior. Thus, some level of correspondence would be expected even if the measures are not fully synchronized, particularly in inpatients, where daily routines are structured and subject to fewer changes than in normal life. Thirdly, the cross-sectional nature of our data does not enable us to examine causality between exercise determinants and actual behaviour. Lastly, given that inpatients and controls were assessed in different settings and due to a possible selection bias, we decided against calculating group differences based on inferential statistics. On the other hand, all inpatients were diagnosed with depression via structured clinical interviews by a psychiatrist, ensuring a rigorous and standardized assessment of pathology. Although structured clinical interviews are the only well-validated method to establish a clinical diagnosis of depression, in many studies, researchers used self-report questionnaires to assess depressive symptoms (83).
5 Conclusion
The present study shows a low level of correspondence between self-reported and accelerometer-based PA, applied on two different, subsequent weeks, in both inpatients treated for MDD, and non-depressed controls. Our data highlight that the assessment of PA remains a challenge in psychiatric patients and individuals with low PA levels. While the SIMPAQ was initially designed to overcome the shortcomings of existing PA questionnaires (particularly the IPAQ), our data points towards the ongoing need to refine and improve PA questionnaires like the SIMPAQ for a more accurate PA assessment in psychiatric populations. Additionally, the discrepancy between self-reported and accelerometer-based PA underlines the necessity for a diversified assessment of PA. The availability of accurate PA questionnaires is important from a clinical perspective, as the development of a physically active lifestyle has become an important treatment goal in psychiatry (84).
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request via the Ethics Committee of Northwestern and Central Switzerland (EKNZ). At the time of obtaining ethical clearance for the present study from the EKNZ, and in line with Swiss laws, we stated that only authorized researchers who are directly involved in the present project will have access to the raw data. Accordingly, and in line with this statement, we cannot grant access to the data for third parties, unless this is officially approved by the EKNZ.
Ethics statement
The studies involving humans were approved by Ethikkommission Nordwest- und Zentralschweiz. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RS: Data curation, Formal Analysis, Visualization, Writing – original draft, Writing – review & editing. RC: Conceptualization, Data curation, Project administration, Writing – review & editing. J-NK: Conceptualization, Data curation, Project administration, Writing – review & editing. OF: Conceptualization, Funding acquisition, Supervision, Writing – review & editing. JB: Conceptualization, Resources, Writing – review & editing. SB: Conceptualization, Resources, Validation, Writing – review & editing. LD: Conceptualization, Resources, Validation, Writing – review & editing. MH: Conceptualization, Resources, Writing – review & editing. CI: Conceptualization, Resources, Validation, Writing – review & editing. UL: Conceptualization, Resources, Writing – review & editing. SM: Conceptualization, Resources, Writing – review & editing. TM: Conceptualization, Resources, Writing – review & editing. AO: Conceptualization, Resources, Writing – review & editing. NS-K: Conceptualization, Resources, Writing – review & editing. MG: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was funded by the Swiss National Science Foundation (grant number 321003B-179353).
Acknowledgments
We thank all the participants, clinic personnel, and coaches for their significant contributions to the study activities and outcomes.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. WHO. Prevention of Mental Disorders. Effective Interventions and Policy Options: Summary Report. Geneva: World Health Organization (2004).
2. Greenberg PE, Fournier A-A, Sisitsky T, Simes M, Berman R, Koenigsberg SH, et al. The economic burden of adults with major depressive disorder in the United States (2010 and 2018). Pharmacoeconomics. (2021) 39(6):653–65. doi: 10.1007/s40273-021-01019-4
3. Tomonaga Y, Haettenschwiler J, Hatzinger M, Holsboer-Trachsler E, Rufer M, Hepp U, et al. The economic burden of depression in Switzerland. Pharmacoeconomics. (2013) 31(3):237–50. doi: 10.1007/s40273-013-0026-9
4. Kruisdijk FR, Hendriksen IJM, Tak ECPM, Beekman ATF, Hopman-Rock M. Effect of running therapy on depression (EFFORT-D). Design of a randomised controlled trial in adult patients [ISRCTN 1894]. BMC Public Health. (2012) 12:50. doi: 10.1186/1471-2458-12-50
5. Stubbs B, Vancampfort D, Smith L, Rosenbaum S, Schuch F, Firth J, et al. Physical activity and mental health. Lancet Psychiatry. (2018) 5(11):873. doi: 10.1016/S2215-0366(18)30343-2
6. Kvam S, Kleppe CL, Nordhus IH, Hovland A. Exercise as a treatment for depression: a meta-analysis. J Affect Disord. (2016) 202:67–86. doi: 10.1016/j.jad.2016.03.063
7. Dimeo F, Bauer M, Varahram I, Proest G, Halter U. Benefits from aerobic exercise in patients with major depression: a pilot study. Br J Sports Med. (2001) 35(2):114–7. doi: 10.1136/bjsm.35.2.114
8. White J, Zaninotto P, Walters K, Kivimaki M, Demakakos P, Shankar A, et al. Severity of depressive symptoms as a predictor of mortality: the English longitudinal study of ageing. Psychol Med. (2015) 45(13):2771–9. doi: 10.1017/S0033291715000732
9. Win S, Parakh K, Eze-Nliam CM, Gottdiener JS, Kop WJ, Ziegelstein RC. Depressive symptoms, physical inactivity and risk of cardiovascular mortality in older adults: the cardiovascular health study. Heart. (2011) 97(6):490–5. doi: 10.1136/hrt.2010.209767
10. Herbsleb M, Schumann A, Lehmann L, Gabriel HHW, Bär K-J. Cardio-respiratory fitness and autonomic function in patients with Major depressive disorder. Front Psychiatry. (2020) 10:980. doi: 10.3389/fpsyt.2019.00980
11. Fornaro M, Solmi M, Veronese N, De Berardis D, Buonaguro EF, Tomasetti C, et al. The burden of mood-disorder/cerebrovascular disease comorbidity: essential neurobiology, psychopharmacology, and physical activity interventions. Int Rev Psychiatry. (2017) 29(5):425–35. doi: 10.1080/09540261.2017.1299695
12. Belvederi Murri M, Folesani F, Zerbinati L, Nanni MG, Ounalli H, Caruso R, et al. Physical activity promotes health and reduces cardiovascular mortality in depressed populations: a literature overview. Int J Environ Res Public Health. (2020) 17(15):5545. doi: 10.3390/ijerph17155545
13. Blumenthal JA, Sherwood A, Babyak MA, Watkins LL, Smith PJ, Hoffman BM, et al. Exercise and pharmacological treatment of depressive symptoms in patients with coronary heart disease: results from the UPBEAT (understanding the prognostic benefits of exercise and antidepressant therapy) study. J Am Coll Cardiol. (2012) 60(12):1053–63. doi: 10.1016/j.jacc.2012.04.040
14. Blumenthal JA, Michael A, Babjak A. Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosom Med. (2007) 69(7):587–96. doi: 10.1097/PSY.0b013e318148c19a
15. Dunn AL, Trivedi MH, Kampert JB, Clark CG, Chambliss HO. Exercise treatment for depression. Efficacy and dose response. Am J Prev Med. (2005) 28(1):1–8. doi: 10.1016/j.amepre.2004.09.003
16. Schuch FB, Vasconcelos-Moreno MP, Borowsky C, Fleck MP. Exercise and severe depression: preliminary results of an add-on study. J Affect Disord. (2011) 133(3):615–8. doi: 10.1016/j.jad.2011.04.030
17. Imboden C, Gerber M, Beck J, Holsboer-Trachsler E, Pühse U, Hatzinger M. Aerobic exercise or stretching as add-on to inpatient treatment of depression: similar antidepressant effects on depressive symptoms and larger effects on working memory for aerobic exercise alone. J Affect Disord. (2020) 276:866–76. doi: 10.1016/j.jad.2020.07.106
18. Ravindran AV, da Silva TL. Complementary and alternative therapies as add-on to pharmacotherapy for mood and anxiety disorders: a systematic review. J Affect Disord. (2013) 150(3):707–19. doi: 10.1016/j.jad.2013.05.042
19. Gerber M, Beck J, Brand S, Cody R, Donath L, Eckert A, et al. The impact of lifestyle physical activity counselling in IN-PATients with major depressive disorders on physical activity, cardiorespiratory fitness, depression, and cardiovascular health risk markers: study protocol for a randomized controlled trial. Trials. (2019) 20(1):346. doi: 10.1186/s13063-019-3468-3
20. Gerber M, Holsboer-Trachsler E, Pühse U, Brand S. Exercise is medicine for patients with major depressive disorders: but only if the “pill” is taken!. Neuropsychiatr Dis Treat. (2016) 12:1977–81. doi: 10.2147/NDT.S110656
21. Lee J, Gierc M, Vila-Rodriguez F, Puterman E, Faulkner G. Efficacy of exercise combined with standard treatment for depression compared to standard treatment alone: a systematic review and meta-analysis of randomized controlled trials. J Affect Disord. (2021) 295:1494–511. doi: 10.1016/j.jad.2021.04.017
22. Dowd KP, Szeklicki R, Minetto MA, Murphy MH, Polito A, Ghigo E, et al. A systematic literature review of reviews on techniques for physical activity measurement in adults: a DEDIPAC study. Int J Behav Nutr Phys Act. (2018) 15(1):15. doi: 10.1186/s12966-017-0636-2
23. Rosenbaum S, Morell R, Abdel-Baki A, Ahmadpanah M, Anilkumar TV, Baie L, et al. Assessing physical activity in people with mental illness: 23-country reliability and validity of the simple physical activity questionnaire (SIMPAQ). BMC Psychiatry. (2020) 20(1):108. doi: 10.1186/s12888-020-2473-0
24. Aiyegbusi OL, Roydhouse J, Cruz Rivera S, Kamudoni P, Schache P, Wilson R. Key considerations to reduce or address respondent burden in patient-reported outcome (PRO) data collection. Nat Commun. (2022) 13(1):5796. doi: 10.1038/s41467-022-33826-4
25. Rolstad S, Adler J, Rydén A. Response burden and questionnaire length: is shorter better? A review and meta-analysis. Value Health. (2011) 14(8):1101–8. doi: 10.1016/j.jval.2011.06.003
26. Reichert M, Giurgiu M, Koch ED, Wieland LM, Lautenbach S, Neubauer AB. Ambulatory assessment for physical activity research: state of the science, best practices and future directions. Psychol Sport Exerc. (2020) 50:101742. doi: 10.1016/j.psychsport.2020.101742
27. Nigg CR, Fuchs R, Gerber M, Jekauc D, Koch T, Krell-Roesch J. Assessing physical activity through questionnaires—a consensus of best practices and future directions. Psychol Sport Exerc. (2020) 50:101715. doi: 10.1016/j.psychsport.2020.101715
28. Ward DS, Evenson KR, Vaughn A, Rodgers AB, Troiano RP. Accelerometer use in physical activity: best practices and research recommendations. Med Sci Sports Exerc. (2005) 37(11 Suppl):582–8. doi: 10.1249/01.mss.0000185292.71933.91
29. Lagerros YT, Lagiou P. Assessment of physical activity and energy expenditure in epidemiological research of chronic diseases. Eur J Epidemiol. (2007) 22(6):353–62. doi: 10.1007/s10654-007-9154-x
30. Leirós-Rodríguez R, García-Soidán JL, Romo-Pérez V. Analyzing the use of accelerometers as a method of early diagnosis of alterations in balance in elderly people: a systematic review. Sensors (Basel). (2019) 19(18):3883. doi: 10.3390/s19183883
31. Durante R, Ainsworth BE. The recall of physical activity: using a cognitive model of the question-answering process. Med Sci Sports Exerc. (1996) 28:1282–91. doi: 10.1097/00005768-199610000-00012
32. Dillon DG, Pizzagalli DA. Mechanisms of memory disruption in depression. Trends Neurosci. (2018) 41:137–49. doi: 10.1016/j.tins.2017.12.006
33. do Nascimento RB, Santos RPG, Gomes THS, França CN, Rossi FE, Natrielli-Filho DG, et al. Poor agreement between responses to the international physical activity questionnaire and objective ActiGraph® data among persons with major depressive or bipolar disorders. Int J Environ Res Public Health. (2022) 19(22):14913. doi: 10.3390/ijerph192214913
34. Vancampfort D, Rosenbaum S, Schuch FB, Ward PB, Probst M, Stubbs B. Physical activity and sedentary behavior in people with major depressive disorder: a systematic review and meta-analysis. J Affect Disord. (2017) 210:139–50. doi: 10.1016/j.jad.2016.10.050
35. Schuch FB, Vancampfort D, Firth J, Rosenbaum S, Ward PB, Silva ES, et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am J Psychiatry. (2018) 175(7):631–48. doi: 10.1176/appi.ajp.2018.17111194
36. Schilling R, Schärli E, Fischer X, Donath L, Faude O, Brand S, et al. The utility of two interview-based physical activity questionnaires in healthy young adults: comparison with accelerometer data. PLoS One. (2018) 13(9):1–12. doi: 10.1371/journal.pone.0203525
37. Fischer X, Kreppke JN, Zahner L, Gerber M, Faude O, Donath L. Telephone-based coaching and prompting for physical activity: short- and long-term findings of a randomized controlled trial (movingcall). Int J Environ Res Public Health. (2019) 16(14):2626. doi: 10.3390/ijerph16142626
38. Vancampfort D, Rosenbaum S, Schuch F, Ward PB, Richards J, Mugisha J, et al. Cardiorespiratory fitness in severe mental illness: a systematic review and meta-analysis. Sports Med. (2017) 47(2):343–52. doi: 10.1007/s40279-016-0574-1
39. Biddle SJH, Fuchs R. Exercise psychology: a view from Europe. Psychol Sport Exerc. (2009) 10(4):410–9. doi: 10.1016/j.psychsport.2009.02.012
40. Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. (2012) 380(9838):258–71. doi: 10.1016/S0140-6736(12)60735-1
41. Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. (1967) 6:278–96. doi: 10.1111/j.2044-8260.1967.tb00530.x
42. Beck AT, Steer RA, Carbin MG. Psychometric properties of the beck depression inventory: twenty-five years of evaluation. Clin Psychol Rev. (1988) 8:77–100. doi: 10.1016/0272-7358(88)90050-5
43. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. (1961) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
44. Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. (2003) 35:1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB
45. Richter P, Werner J, Heerlein A, Kraus A, Sauer H. On the validity of the beck depression inventory. Psychopathology. (1998) 31:160–8. doi: 10.1159/000066239
47. Rosenbaum S, Ward PB. The simple physical activity questionnaire. Lancet Psychiatry. (2016) 3(1):1. doi: 10.1016/S2215-0366(15)00496-4
48. Trost SG, McIver KL, Pate RR. Conducting accelerometer-based activity assessments in field-based research. Med Sci Sports Exerc. (2005) 37(11 Suppl):531–48. doi: 10.1249/01.mss.0000185657.86065.98
49. Sasaki JE, John D, Freedson PS. Validation and comparison of ActiGraph activity monitors. J Sci Med Sport. (2011) 14(5):411–6. doi: 10.1016/j.jsams.2011.04.003
50. Rowlands AV. Accelerometer assessment of physical activity in children: an update. Pediatr Exerc Sci. (2007) 19(3):252–66. doi: 10.1123/pes.19.3.252
51. Zisko N, Carlsen T, Salvesen Ø, Aspvik NP, Ingebrigtsen JE, Wisløff U, et al. New relative intensity ambulatory accelerometer thresholds for elderly men and women: the generation 100 study. BMC Geriatr. (2015) 15:97. doi: 10.1186/s12877-015-0093-1
52. Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. (2000) 32(9):498–516. doi: 10.1097/00005768-200009001-00009
53. Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR, Tudor-Locke C, et al. 2011 compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. (2011) 43(8):1575–81. doi: 10.1249/MSS.0b013e31821ece12
54. Trost SG, Pate RR, Freedson PS, Sallis JF, Taylor WC. Using objective physical activity measures with youth: how many days of monitoring are needed? Med Sci Sports Exerc. (2000) 25:426–31. doi: 10.1097/00005768-200002000-00025
55. Herrmann SD, Barreira TV, Kang M, Ainsworth BE. How many hours are enough? Accelerometer wear time may provide bias in daily activity estimates. J Phys Act Health. (2013) 10:742–9. doi: 10.1123/jpah.10.5.742
56. Herman Hansen B, Børtnes I, Hildebrand M, Holme I, Kolle E, Anderssen SA, et al. Validity of the actigraph GT1M during walking and cycling. J Sports Sci. (2014) 32(6):510–6. doi: 10.1080/02640414.2013.844347
57. Plante TG, LeCaptain SE, McLain HC. Perceived fitness predicts daily coping better than physical activity. J Appl Biobehav Res. (2000) 5:66–79. doi: 10.1111/j.1751-9861.2000.tb00063.x
58. Plante TG, Lantis A, Checa G. The influence of perceived versus aerobic fitness on psychological health and physiological stress responsitivity. Int J Stress Manag. (1998) 5:141–56. doi: 10.1023/A:1022924915768
59. Åstrand P-O, Rodahl K. Textbook of work physiology: physiological bases of exercise. Champaign: Human Kinetics (2003).
60. Borg G. Perceived exertion as an indicator of somatic stress. Scand J Rehabil Med. (1970) 2(2):92–8. doi: 10.1097/00005768-198208000-00012
61. Macsween A. The reliability and validity of the Åstrand nomogram and linear extrapolation for deriving VO2max from submaximal exercise data. J Sports Med Phys Fitness. (2001) 41:312–7.11533560
62. Buono MJ, Roby JJ, Micale FG, Sallis JF. Predicting maximal oxygen uptake in children: modification of the Åstrand-rhyming test. Pediatr Exerc Sci. (1989) 1:278–83. doi: 10.1123/pes.1.3.278
63. Wonisch M, Hofmann P, Fruhwald FM, Kraxner W, Hödl R, Pokan R, et al. Influence of beta-blocker use on percentage of target heart rate exercise prescription. Eur J Cardiovasc Prev Rehabil. (2003) 10(4):296–301. doi: 10.1097/00149831-200308000-00013
64. Fuchs R. Aufbau Eines Körperlich-Aktiven Lebensstils im Kontext der Medizinischen Rehabilitation: Ein Motivational-Volitionales Interventionskonzept (MoVo-LISA Projekt). Unveröffentlichter Endbericht. Freiburg: Universität Freiburg (2008).
65. Gerber M, Fuchs R, Pühse U. Follow-up of a short motivational and volitional exercise-intervention trial with overweight and obese individuals. Schweiz Z Sportmed Sporttraumatol. (2010) 58:108–14.
66. Fuchs R, Goehner W, Seelig H. Long-term effects of a psychological group intervention on physical exercise and health: the MoVo concept. J Phys Act Health. (2011) 8(6):794–803. doi: 10.1123/jpah.8.6.794
67. Gerber M, Fuchs R, Pühse U. Der Einfluss eines Kurz-Interventionsprogramms (MoVo-lisa) auf das Bewegungsverhalten und die Determinanten köperlich-sportlicher Aktivität bei Übergewichtigen und Fettleibigen Personen. Z Gesundh Psychol. (2010) 18:159–69. doi: 10.1026/1612-5010/a000026
69. Seelig H, Fuchs R. Messung der sport- und bewegungsbezogenen selbstkonkordanz. Z Sportpsychol. (2006) 13:121–39. doi: 10.1026/1612-5010.13.4.121
70. Sheldon KM, Elliot AJ. Goal striving, need-satisfaction, and longitudinal well-being: the self-concordance model. J Pers Soc Psychol. (1999) 76:482–97. doi: 10.1037//0022-3514.76.3.482
71. Dunn PK. Scientific Research and Methodology: An introduction to Quantitative Research in Science and Health. United States: RStudio, PBC (2021).
73. Wichers M, Peeters F, Rutten BP, Jacobs N, Derom C, Thiery E, et al. A time-lagged momentary assessment study on daily life physical activity and affect. Health Psychol. (2012) 31(2):135–44. doi: 10.1037/a0025688
74. Rock PL, Roiser JP, Riedel WJ, Blackwell AD. Cognitive impairment in depression: a systematic review and meta-analysis. Psychol Med. (2014) 44(10):2029–40. doi: 10.1017/S0033291713002535
75. Cody R, Beck J, Brand S, Donath L, Eckert A, Faude O, et al. Depression severity and psychosocial determinants of physical activity behavior in in-patients with major depressive disorders. Psychol Sport Exerc. (2022) 63:101743. doi: 10.1016/j.psychsport.2022.102294
76. Krämer L, Fuchs R. Barrieren und barrierenmanagement im prozess der sportteilnahme: zwei neue messinstrumente. Z Gesundh Psychol. (2010) 18:170–82. doi: 10.1026/1612-5010/a000019
77. Ehrbar J, Brand S, Colledge F, Donath L, Egger ST, Hatzinger M, et al. Psychiatric in-patients are more likely to meet recommended levels of health-enhancing physical activity if they engage in exercise and sport therapy programs. Front Psychiatry. (2018) 9:322. doi: 10.3389/fpsyt.2018.00322
78. Brand S, Colledge F, Beeler N, Pühse U, Kalak N, Sadeghi Bahmani D, et al. The current state of physical activity and exercise programs in German-speaking, Swiss psychiatric hospitals: results from a brief online survey. Neuropsychiatr Dis Treat. (2016) 12:1309–17. doi: 10.2147/NDT.S107313
79. Kreppke JN, Cody R, Gerber M, Faude O. Association between depression severity and fitness in in-patients with major depressive disorders. Curr Issues Sport Sci. (2023) 8(2):012. doi: 10.36950/2023.2ciss012
80. Dostálová R, Stillman C, Erickson KI, Slepička P, Mudrák J. The relationship between physical activity, self-perceived health, and cognitive function in older adults. Brain Sci. (2021) 11(4):492. doi: 10.3390/brainsci11040492
81. Krämer LV, Helmes AW, Seelig H, Fuchs R, Bengel J. Correlates of reduced exercise behaviour in depression: the role of motivational and volitional deficits. Psychol Health. (2014) 29:1206–25. doi: 10.1080/08870446.2014.918978
82. Pomp S, Fleig L, Schwarzer R, Lippke S. Depressive symptoms interfere with post-rehabilitation exercise: outcome expectancies and experience as mediators. Psychol Health Med. (2012) 17:698–708. doi: 10.1080/13548506.2012.661864
83. Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. (2017) 14:145–55. doi: 10.1038/nrcardio.2016.181
Keywords: assessment, exercise, measurement, mental illness, physical activity, sedentary behaviour, accelerometry, fitness
Citation: Schilling R, Cody R, Kreppke J-N, Faude O, Beck J, Brand S, Donath L, Hatzinger M, Imboden C, Lang U, Mans S, Mikoteit T, Oswald A, Schweinfurth-Keck N and Gerber M (2024) Correspondence between the Simple Physical Activity Questionnaire (SIMPAQ) and accelerometer-based physical activity in inpatients treated for major depressive disorders in comparison to non-depressed controls. Front. Sports Act. Living 6:1447821. doi: 10.3389/fspor.2024.1447821
Received: 12 June 2024; Accepted: 7 August 2024;
Published: 6 September 2024.
Edited by:
Luis Cid, Polytechnic Institute of Santarém, PortugalReviewed by:
Teresa Bento, Polytechnic Institute of Santarém, PortugalMiguel Jacinto, Polytechnic Institute of Leiria, Portugal
Copyright: © 2024 Schilling, Cody, Kreppke, Faude, Beck, Brand, Donath, Hatzinger, Imboden, Lang, Mans, Mikoteit, Oswald, Schweinfurth-Keck and Gerber. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: René Schilling, cmVuZS5zY2hpbGxpbmdAdW5pYmFzLmNo