 A. Kayeye
A. Kayeye I. Triantafyllou
I. Triantafyllou S. Mathur
S. Mathur T. Janaudis-Ferreira
T. Janaudis-Ferreira
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Sports Act. Living , 24 September 2024
Sec. Physical Activity in the Prevention and Management of Disease
Volume 6 - 2024 | https://doi.org/10.3389/fspor.2024.1439399
This article is part of the Research Topic Exercise and Transplant Sport: The journey to a more active life View all 6 articles
Objectives: High intensity exercise in individuals post solid organ transplant (SOT) remains a largely understudied phenomenon, with potential risks and benefits. Additionally, the optimal training protocols are still unclear. This narrative review aimed to explore the impact of high-intensity exercise training and strenuous sports on solid organ transplant recipients (SOTRs).
Methods: We conducted a narrative review of intervention studies of any design that included high-intensity exercise training and cross-sectional studies of strenuous sports and activities. Additionally, we reviewed individual reports documenting post-SOT performance at highly competitive or physiological levels. We used MEDLINE to search for relevant articles followed by a manual search for additional articles. Data were extracted and results were summarized.
Results: High-intensity and strenuous exercise appears to be safe among stable SOTRs. High-intensity protocols consistently demonstrated improvements in VO2peak and a reduction in coronary artery disease prevalence, though findings related to body composition, health-related quality of life outcomes, and cardiovascular exercise variables were inconsistent. Pre-transplant athletes showcase notable achievements and physiological adaptations post-transplantation, highlighting the capacity for athletic performance among this population. However, caution is warranted in interpreting the findings from these studies due to limitations in generalizability and other methodological limitations.
Conclusion: As evidenced by current literature, high intensity exercise emerges as a promising exercise method for safely improving various physiological parameters, and reducing the prevalence of coronary heart disease in SOTRs. It can induce similar or greater effects to moderate intensity exercise, however follow-up studies indicate low retention. Further research of higher methodological rigor is warranted in this field to advance understanding, and to guide evidence-based practice.
Solid organ transplant (SOT) allows for an enhanced quality of life for individuals with end-stage organ failure (1). However, Immunosuppressive medications used for post-transplant management have several side effects including, increased infection risk, reduced cardiopulmonary function and muscle strength, increased osteoporosis and risk fracture, and increased obesity prevalence (2, 3).
Furthermore, depression affects up to 60% of solid organ transplant recipients (SOTRs) and is associated with increased medication non-compliance and graft loss (4). These negative side effects can be counteracted with exercise as it has been shown to lower psychological stress, increase cardiovascular capacity, and increase bone mineral density in the general and osteoporotic population (5, 6). While moderate intensity exercise offers clear benefits in the factors related to common health risks. The safety and efficacy of high intensity exercise programs remains understudied and has sparked considerable debate and deliberations within the transplant community (7, 8). High-intensity training, defined as a workload of 85% or more of an individual’s VO2max, can yield comparable or superior results compared to moderate-intensity exercise (workload of 60%–80% of an individual's VO2max) within the general population (9–11). High intensity training has demonstrated enhancement of cardiovascular function, bone strength, immune function, body composition, and physical capacity in patients with coronary artery disease, heart failure, and immune system dysregulation (12). High intensity interval training (HIIT) is associated with greater enjoyability, and time efficiency compared to moderate intensity exercise. It has prompted researchers and clinicians to explore its potential application in the rehabilitation and fitness regimens of SOTRs (9, 12). However, HIIT (exercise involving short bursts of intense exercise) and strenuous exercise (activities lasting over 90 min with high cardiovascular demands) have immunosuppressive effects in healthy populations which may pose a potential risk for SOTRs (13). The combination of their immunosuppressive medication with the additional immunosuppressant effects of exhaustive exercise could heighten susceptibility to infections, presenting a significant concern (14).
Some SOTRs embrace vigorous exercise regimens, despite the challenges they may entail. Organizations such as the World Transplant Games Federation, Canadian Transplant Games and Transplant Sports, emphasize the importance of maintaining an active and healthy lifestyle post-Transplant. They promote participation in sports and activities that can be physically demanding for some SOTRs (7, 15). Evidence from surveys conducted among participants in the Canadian Transplant Games reveals a strong desire for structured training programs. A significant proportion of participants expressed interest in general conditioning programs to enhance physical preparedness (15). In response to these findings, the development of tailored pre-competition training programs emerges as a potential strategy to incentivize participation and facilitate higher training intensities.
However, these programs still need to be developed and undergo testing to determine their efficacy and safety. For example, in a self-perspective written by a kidney transplant recipient, they describe their uncertainty in which training regimens to undertake in order to begin competitively swimming (16). Establishing comprehensive and personalized training guidelines can offer valuable support to transplant recipients aiming to engage in athletic pursuits, ensuring both their safety and optimal performance.
Given the nuanced nature of SOT, which involves variables such as the specific organ transplanted, the recipient's pre-transplant exercise capacity level, the complexity of immunosuppressive drug protocols, and the presence of comorbidities, participation in high-intensity exercise protocols warrants careful scrutiny. This narrative review aims to explore the impact of high-intensity exercise protocols and strenuous sports on SOTRs, while prioritizing safety. We conducted a comprehensive review of the physiological and health related quality of life, clinical outcomes, and safety considerations associated with high intensity training interventions or strenuous sporting activities among this distinctive population.
A systematic search of MEDLINE along with a manual search from inception to January 18, 2024 was conducted. The key words and subject headings used are presented in Table 1. We included intervention studies of any design that included high-intensity exercise training in SOTRs. High-intensity exercise was defined as physiological intensities of vigorous to maximal effort (HRR >60 bpm, HRmax > 77%, VO2max > 64%, RPE > 14) (17). High intensity interval training (HIIT) was also considered and is typified by periods of short bursts of intense exercise, followed by rest periods. We also included cross-sectional and case studies of strenuous sports and activities performed by SOTRs. Strenuous sports were defined as activities lasting more than 90 min involving challenging tasks such as, steep altitude accession, prolonged physical exertion, or high cardiovascular demand. Outcomes of interest were: VO2peak, endothelial function and inflammatory markers, blood pressure, cardiopulmonary exercise variables, physical activity and sedentary time, body composition, health related quality of life, immunological response, inflammation and kidney response, and implications of strenuous altitude ascension.
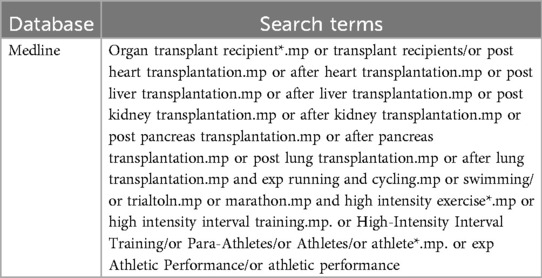
Table 1. Medline keywords.
The search from MEDLINE produced 100 articles (Figure 1) with no duplicates, and 37 full text articles were reviewed by 1 author (A.K) for eligibility in which 16 met the criteria. An additional 18 articles were identified through manual searches, resulting in 34 articles in total. Overall, 17 high intensity (Table 2), 6 strenuous sports and activities (Table 3) and 9 individual reports of post-SOT performance at highly competitive or physiological levels (Table 4) were retrieved.
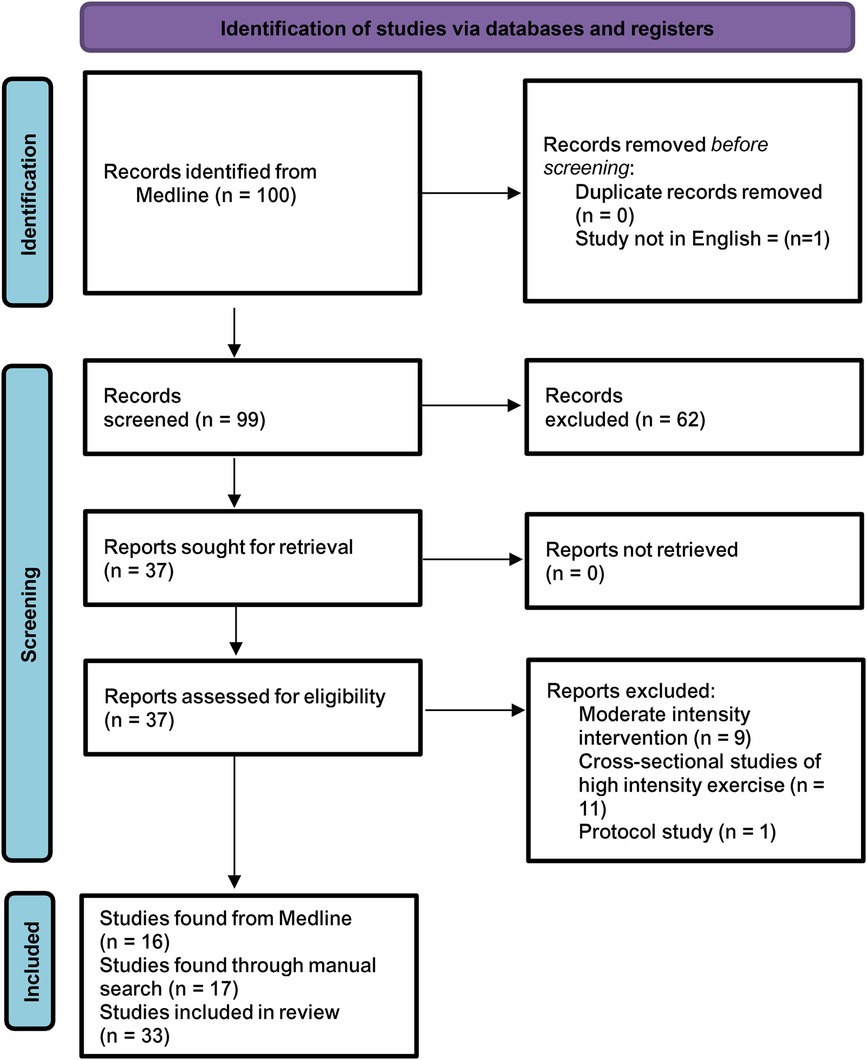
Figure 1. Prisma flow diagram.

Table 2. High intensity interval training.
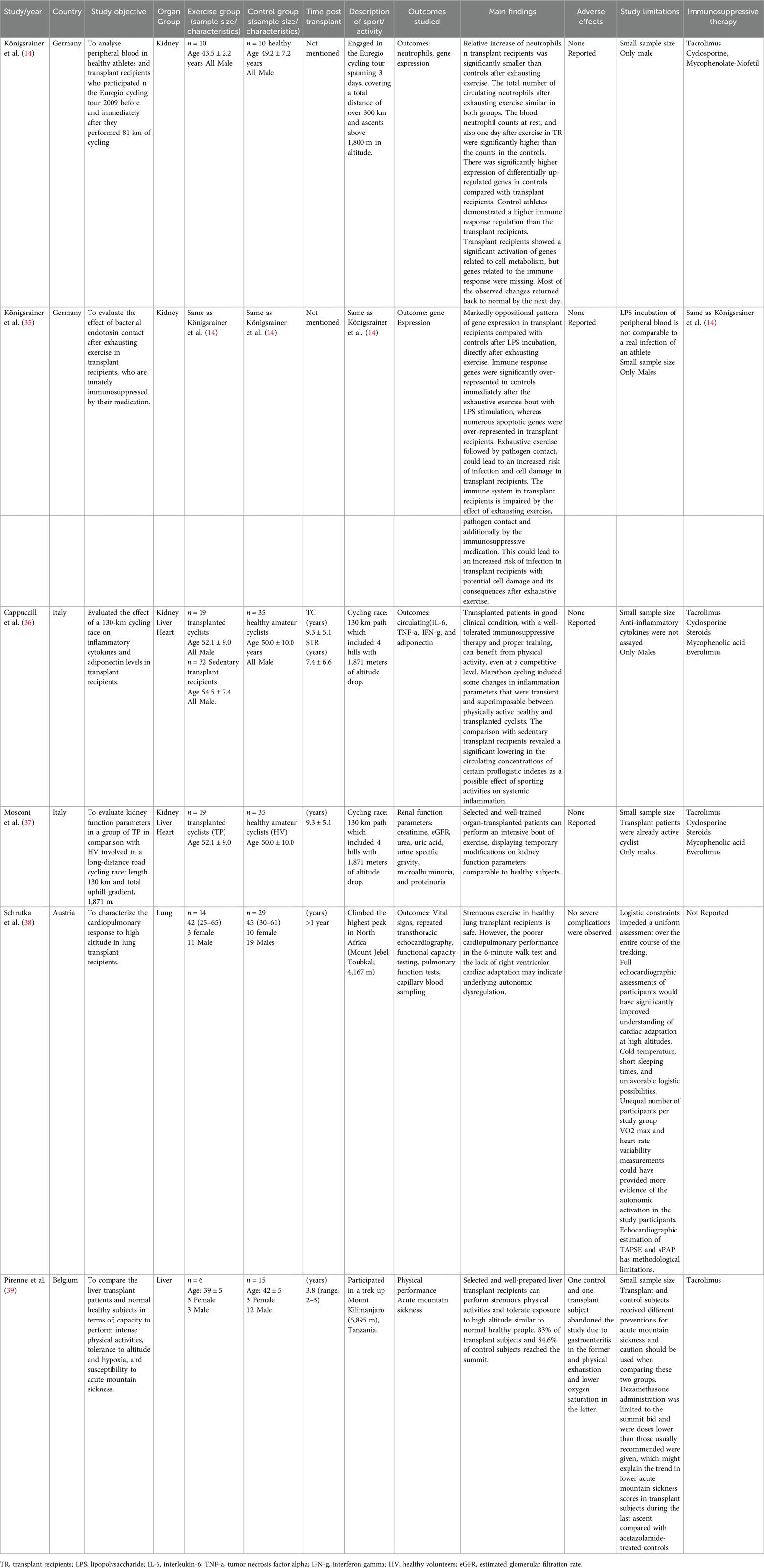
Table 3. Strenuous exercise.
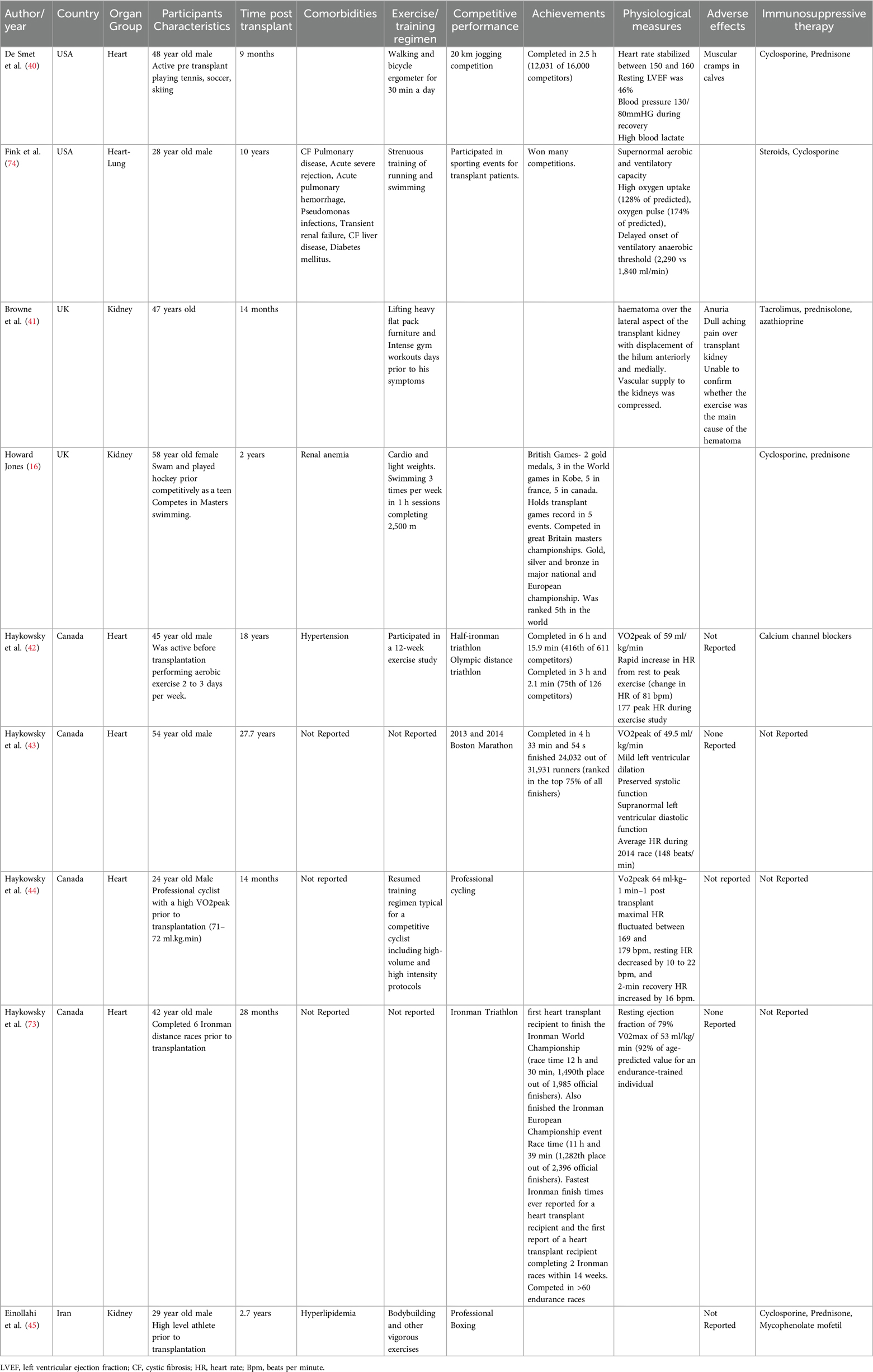
Table 4. Case studies.
When comparing HIIT against moderate intensity continuous exercise (MICT) protocols, or standard care, HeartTx (Tx = transplantation) recipients have demonstrated a significantly greater mean improvement in VO2peak throughout all studies with HIIT (HIIT; + 4.17 ml/kg/min, Control; + 2.07 ml/kg/min,) (19, 20, 23, 28, 46). However, high baseline VO2peak values in Nytroen et al. 2012 may reflect bias in the population chosen (20). A 1-year follow up of participants from Nytroen et al. 2012 found the favorable increases in VO2peak within the HIIT group persisted, (HIIT; + 3.2 ml/kg/min, Control; 0 ml/kg/min), with a statistically significant between group difference (21). Although, 5-years later the HIIT abstinence resulted in a loss of the improvement in VO2peak, suggesting the importance of maintaining a HIIT exercise routine (22). A 3-year follow up of Nytroen et al. (23) which compared HIIT to MICT demonstrated that the HIIT group kept their superior effects compared to the MICT group, but this difference was not significant between groups (24). In LungTx recipients, HIIT increased VO2peak but this was not a significant improvement compared to the standard care group. This may be attributed to the little adherence to the exercise protocol within the HIIT group (26). These benefits appear to be the greatest if the intervention is undertaken within 2 years after Tx (26). This highlights the importance of implementing interventions aimed at preserving, or improving aerobic fitness early in the post-transplant period, which may consequently decrease coronary heart disease risk. In a single armed intervention including LungTx, HeartTx, KidneyTx, and LiverTx recipients, HIIT showed a significant overall increase in VO2peak (+3.2 ml/kg/min), with the greatest increase in HeartTx recipients (+4.6 ml/kg/min) (30). There was no significant increase in VO2peak within LiverTx recipients which could be due to their high baseline values and their steroid free regimen (30). Billany et al. on the other hand found a greater increase with MICT (+3.72 ml/kg/min) compared to HIIT A (+2.78 ml/kg/min) and HIIT B (+2.83 ml/kg/min) in KidneyTx recipients (32). However, this may be attributed to their higher-than-normal baseline VO2peak values compared to HIIT A and HIIT B (HIIT A: 30 min of 4-, 2-, and 1-min intervals; 80%–90% watts at V̇O2peak with 2 min active rest; HIIT B: 30 min of 4 × 4 min intervals at 80%–90% V̇O2peak with 3 min rest and 5 min active stage). While HIIT holds promise for improving cardiovascular health markers such as VO2peak in SOTRs, particularly early post-transplant, there is a need to explore long-term adherence and the effects of diverse high intensity exercise protocols across different transplant types. Additionally, determining optimal training protocols remains an area necessitating further investigation.
In HeartTx recipients, cardiac allograft vasculopathy emerges as a progressive atherosclerotic manifestation (47). Unlike typical atherosclerosis, cardiac allograft vasculopathy distinguishes itself by the thickening of the inner arterial wall, and a widespread constriction of smaller blood vessels leading to elevated rates of health complications and mortality (48). Studies have shown physical activity to offer atheroprotective effects, with HIIT demonstrating even greater benefits in populations with coronary artery disease (20, 47). This is by way of reduction in chronic inflammation which is associated with endothelial dysfunction, and increased formation and progression of atherosclerotic plaques (49). An 8-week HIIT intervention in HeartTx recipients significantly increased flow mediated dilation of the brachial artery compared to sedentary individuals, (HIIT; + 3.1%, Control; + 0.3%) with a statistically significant difference between control and intervention groups (19). The patients were although treated with vasodilators which could interfere with the effect of exercise on flow mediated dilation making it more challenging to draw concrete conclusions (19). Likewise, 12 weeks of high intensity supervised exercise training did not have an impact on brachial artery endothelial-dependent, or -independent vasodilation compared to no training (46). Interestingly, when compared to MICT, HIIT does not seem to elicit significantly greater improvements in flow mediated dilation, arterial stiffness, and endothelial function (23, 28). Modulation of low-grade inflammation in HeartTx recipients by exercise training could have a positive impact on endothelial function, and potentially, long-term outcomes (19). Yet, the superior effects of HIIT compared to MICT or usual care on the reduction of inflammatory biomarkers yields mixed results. In comparison to MICT, HIIT shows no significant effect on inflammatory activity including, tumor necrosis factor-alpha, orosomusciod, interleukin 6, and interleukin 10, or adiponectin levels in HeartTx or KidneyTx recipients (29, 33, 50). However, when compared to sedentary controls, HIIT resulted in a significantly greater mean reduction in inflammatory responses in HeartTx recipients (19). These included, high-sensitivity c-reactive protein (HIIT; −0.60 mg/ml, Control; −0.27 mg/ml) and pro-atrial natriuretic peptide (HIIT; −73.2 nmol/ml, Control; −12.1 nmol/ml) (19). Using intravascular ultrasound analysis 3 months post innervation, Nyotrean et al. found HIIT among maintenance HeartTx recipients resulted in a significantly slowed rate of cardiac allograft vasculopathy progression compared to usual care (50). This was evident by a significantly smaller mean increase the percent atheroma volume (PAV) (HIIT; + 0.9%, Control; + 2.5%), and total atheroma volume (TAV) (HIIT; 0.3 mm3/mm, Control; 1.1 mm3/mm) with significant differences between the groups (50). It should be noted that baseline intravascular ultrasound parameters were numerically higher in the control group at baseline suggesting population homogeneity was not met (50). A 3-year follow-up showed mild cardiac allograft vasculopathy in the HIIT group remained stable (5 n), while the control group saw a decrease (8 to 7 n). Similar results were evident when HIIT was compared to usual care during a 5-year follow-up (22, 24). The effects were lost in parallel to decline in VO2peak suggesting a potential need for exercise maintenance (22). However, conflicting evidence exists. A 6-month intervention in HeartTx recipients comparing HIIT to MICT found a greater cardiac allograft vasculopathy prevalence following exercise, increasing by 50% in both groups at follow up (HIIT; 4–8 n, MICT; 6–12 n) (31). These findings may potentially be explained by the usage of coherence tomography which produces images with 10 times the spatial resolution of intravascular ultrasound, providing a clear delineation of the arterial vessel and in vivo vessel histological analysis (51). Additionally, while physical activity offers well-documented cardiovascular benefits, these advantages may follow a curvilinear dose-response relationship. Engaging in exercise beyond an “optimal dose” in terms of duration and intensity could potentially increase the risk of coronary plaque development, but this remains debated with inconclusive data (52, 53). Given the elevated cardiovascular risk in SOTRs, stricter pre-participation screening, including cardiopulmonary exercise testing, functional imaging, and potentially coherence tomography scans may be warranted before engaging in vigorous exercise (54). Furthermore, the atheroprotective benefits of HIIT and MICT seem to coincide, while HIIT only shows superior effects compared to usual care or sedentary protocols.
Hypertension and its clinical complications are common amongst SOTRs with a prevalence of 50%–80% (55). In healthy subjects, regular cardiovascular exercise has been shown to lower resting blood pressure. The heart is strengthened allowing for a greater volume of blood to be pumped with less effort (17). A HITT intervention compared to sedentary controls in HeartTx recipients significantly reduced resting systolic blood pressure (HIIT; −15 mmHg, Control; + 1 mmHg) (19). No significant changes were evident in either group for resting diastolic blood pressure (19). When compared to MICT, HIIT again induced a greater reduction in systolic blood pressure in HeartTx recipients, but these differences were again not statistically significant (28). Likewise, no changes in diastolic blood pressure were evident (28). However, these studies should be interpreted with caution as they were not powered to detect changes in blood pressure (19, 28). In KidneyTx recipients both MICT and HIIT interventions led to an overall decrease in systolic blood pressure (−6 mmHg) with the greatest decrease in MICT (−10 mmHg) (32). Unlike the previous studies diastolic blood pressure also decreased overall (−5 mmHg) with the greatest decrease in MICT (−8 mmHg). This may be explained by group heterogeneity as the MICT group had higher baseline values (32). It should be noted that hypertensive individuals should take precaution when engaging in high intensity exercises as it induces a sudden spike in blood pressure (8). The combination of high blood pressure and the intense stress of HIIT can increase the risk of cardiovascular events such as myocardial infarctions and strokes (11). Hypertensive SOTRs should do their due diligence in regular blood pressure monitoring and talk to their physician regarding potential medication alteration before engaging in HIIT.
An improvement in cardiopulmonary variables through exercise is crucial for SOTRs due to its significant implications for cardiovascular health. Enhanced heart rate response, increased cardiac output, and improved systolic function are indicators of improved cardiovascular fitness, which can mitigate the risk of cardiovascular complications post-transplantation (56). Furthermore, these responses are often blunted in SOTRs, especially in HeartTx recipients (56). For individuals aspiring to compete recreationally or professionally, optimizing these variables through exercise interventions becomes not just desirable, but imperative. Dall et al. reported a greater increase in heart rate peak with HIIT (+4.3 bpm), contrasting with MICT (+1.2 bpm) in HeartTx recipients (28). Additionally, HIIT exhibited a significant decrease in resting heart rate with no change in the MICT exercise group, and no significant between group differences (28). Heart rate reserve had a marginal increase with HIIT (+5.3 bpm), but not with MICT (+0.7 bpm) while showing a significant between group difference (28). When compared to MICT, HIIT did not result in significantly greater improvements in cardiac output, VE/VCO2slope, ejection fraction, left ventricular end-diastolic diameter, heart rate max, peak heart rate, heart rate reserve, and left ventricular end-systolic diameter (23). These results remained consistent during a 3-year follow-up (22). However, in comparison to usual care, HIIT resulted in a significant increase in peak heart rate (+4 bpm) with no change in the control group (0 bpm), and a significant in between group difference 1 year post intervention in HeartTx recipients (21). Moreover, HIIT improved left ventricular movement but did not have a major impact on diastolic function (21). This suggest that while HIIT might improve some aspects of left ventricular function in HeartTx, it likely does not directly enhance the heart muscles contractility or significantly increase the amount of blood pumped per beat (24). Haywosky et al. found during rest and exercise, HIIT did not result in significant changes in cycle exercise end-diastolic cavity area, end-systolic cavity area, stroke area and area ejection fraction after 12 weeks of supervised exercise training or no training in HeartTx recipients (46). In KidneyTx recipients both HIIT and MICT were able to decrease resting heart rate in all interventions by (−5 bpm) with the greatest decrease in HIIT B (−11 bpm) (32). Stroke volume had an overall increase (+3.59 ml/beat) in all interventions with HIIT B having the highest increase (+3.77 ml/beat) (32). Cardiac output had an overall decrease (+0.52 ml/beat) but only significantly increased in HIIT A (+0.07) (32). Moreover, total peripheral resistance decreased overall (−110.74 dyn s cm5), with the greatest decrease in MICT (−37.08 dyn s cm5) (32). In an intervention comparing all transplant groups, peak heart rate, and VE/VCO2 slope did not change within any of the groups, while resting heart rate did decrease significantly (−4.7 bpm) (30). LungTx and KidneyTx had the greatest drop in resting heart rate (−5.9 bpm and −4.4 bpm, respectively) (30). HIIT appears to be a promising strategy for improving some aspects of cardiovascular health in SOTRs. Literature shows significant increases in peak heart rate, and heart rate reserve following HIIT compared to controls in SOTRs. Additionally, HITT may improve left ventricular annular systolic displacement, indicating better overall heart movement. However, the impact on other key markers seems less consistent.
A significant proportion of SOTRs struggle to meet recommended physical activity levels (9), and HIIT may present a potential solution. HIIT is time efficient and has demonstrated greater enjoyability compared to traditional exercise throughout the general active population (57). This could lead to increased adherence and reduced sedentary time which remains a problem in the SOT population (58). However, existing research on the impact of HIIT on daily physical activity in SOTRs paints a complex picture. Follow-up studies 1- and 5-years post HIIT in HeartTx recipients demonstrated that most of the participants only engaged in moderate-intensity daily activity levels (30–60 min) (21, 22, 24). Similarly, Ulvestad et al. found no significant difference in physical activity or sedentary time among LungTx recipients following HIIT or usual care (32). Likewise, in KidneyTx both HIIT and MICT led to an increase in physical activity levels post intervention but without significant between group differences (32). A cycling and hiking intervention consisting of HeartTx, LungTx, KidneyTx, and LiverTx recipients found the continuation of a physically active lifestyle in sedentary transplant recipients will require physical activity and exercise interventions tailored closely to their needs (34). The intervention led to an increase in physical activity at follow-up but the results should be interpreted with caution as social desirability bias might have inflated self-reported data in some studies (24, 34). The current evidence regarding the effect of HIIT on daily physical activity and sedentary time in SOTRs is inconclusive. While HIIT holds promise for promoting activity in this population, retention of HIIT seems to be minimal. Studies provide supervision and group cohesivity which can bolster motivation. Further research needs to focus on how to translate these factors post interventions to address adherence challenges.
Post-SOT patients are often prescribed corticosteroid medication and calcineurin inhibitors which are associated with muscle atrophy and osteoporosis (59). This is most prevalent after LungTx as they have a 12%–15% bone mineral density reduction within the first 2 months (60). This entails a higher incidence of fractures at four to five times compared to the general population (61, 62). Likewise, by 12 months post-transplant, there is a trend indicating higher proportion of overweight or obese individuals among transplant recipients as categorized by the World Health Organization guidelines: kidney (53.4%), liver (51.5%), heart (51.7%), and lung (33.1%) (63). HIIT combined with strength training in LungTx and HeartTx recipients led to increased trabecular bone score of the lumbar spine density, increased total body mass and leg lean tissue mass, and decreased subcutaneous fat compared to usual care (27, 46). However, other body composition measures such as lean body mass, bone mineral density, and fat body mass did not differ significantly from standard care (27, 46). This was coupled with greater increases in the HIIT group's leg press, quadriceps, hamstrings, and chest press maximal strength. However, there were no significant differences between groups or changes in arm curl or latissimus dorsi pulldown (20, 27, 46). In various transplant groups (heart, lung, kidney, liver) HIIT significantly decreased body weight (−1.1 kg) and BMI (−0.4 kg/m2), while increasing Wmax (maximal work capacity) in all groups (+12.8 W) (30). Nytroen et al. 2019 found no significant differences in any body composition measures between HIIT and MICT in HeartTx recipients, with these results persisting over several years (22, 23). Moreover, HIIT participants showed a significantly higher mean change in muscular exercise capacity (muscles ability to generate force and sustain effort over a period of time) 1 year post intervention, but these results were not significant 5 years later (21, 22, 24). Body composition and HIIT in KidneyTx recipients showed contradicting results, with one study finding increased body fat (+0.83%), BMI (+0.10 kg/m2), and decreased lean muscle mass (−0.45 kg) after both HIIT and MICT, highlighting potential exercise intensity-dependent effects (32). While HIIT shows promise in potentially improving bone health and muscle mass in some SOTR, the results across studies are inconsistent. Regular screening practices and bone mineral density measurements should be undertaken in SOTRs wishing to participate in high intensity endeavors that require high impact.
In SOTRs, a higher perceived health related quality of life (an individual's perceived physical and mental health over time) has been associated with greater motivation to adhere to medication schedules, follow-up appointments, and healthy lifestyle changes (64). This can lead to better long-term graft survival and overall health (64). HIIT interventions have demonstrated significant improvements in physical and mental health, and overall health related quality of life (small-to-moderate effect size) in clinical and non-clinical populations (65). Notably HIIT appears to be equally effective as MICT in enhancing health related quality of life, offering a time-efficient alternative in the general population (65). A 12-month intervention in HeartTx recipients comparing HIIT and usual care found no significant changes in health-related quality of life (20). However, a 9-month exercise protocol in HeartTx recipients showed both HIIT and MICT groups increased anxiety but decreased depression, but these results were not significantly different between groups (23). Likewise, there was a significant increase in PCS scores within both groups, but this was not significantly different between groups (23). The same participants 3 years later significantly increased physical functioning and role scores (25). Vitality only significantly increased in MICT group, while only the HIIT group significantly increased in role emotional with a significant in between group difference (25). Compared to usual care, 5 years post a HIIT intervention, HIIT had higher scores in all variables as assessed by the SF-36 version 2 but only the role physical score was significantly higher (24). All patients showed higher depression rates from baseline to 5-year follow-up with but with no between group differences. Anxiety decreased in the HIIT group (−1%) and increased in the control (+9%) group but these differences were not significant (24). LungTx recipients undergoing HIIT scored significantly greater on the SF-36 MCS compared to usual care (32). Both HIIT and continuous moderate exercise led to significant improvements in physical function, energy and general health, while reducing markers of anxiety and depression (32). None of these variables showed between group differences and had a significant loss of their positive responses during the washout period (29). In various transplant groups (lung, heart, kidney, liver) participating in hiking and cycling, the exercises initially led to significantly improved health-related quality of life and mental health scores compared to the transplant control group. However, the benefits were not sustained in the long term (25). Additionally, seasonal variations appeared to influence the results, with some improvements observed before or after the summer months. Despite some transient improvements, stress levels remained largely unchanged across all groups (25). Long-term follow-up studies present mixed findings: some show sustained improvements in specific health related quality of life domains like physical functioning and role emotional, while others observe no significant differences between HIIT and control groups. Most of these studies although had missing participants at follow-up and lacked disease specific HRQOL questionnaires which could have been more sensitive in detecting differences between groups.
Research conducted in healthy populations has demonstrated that prolonged exercise exceeding 60% of VO2peak can induce transient immunosuppression (66). These consequences are further amplified for SOTRs who can experience slower recovery time from infections, potentially leading to serious illnesses, or worse, organ rejection due to their already immunosuppressed state (67). This is by way of reduction in leukocyte function and alteration in inflammatory parameters (68). KidneyTx recipients undergoing a cycling tour spanning over 300 km revealed a small relative increase in neutrophils compared to controls with a majority of cell activation being found in cell metabolism while genes related to immune function were not expressed (68). When bacterial endotoxin was introduced to their blood sample after exhausting exercise, 86 up-regulated and 4 down-regulated genes were detected in transplant recipients, while 151 up regulated and 18 differentiated downregulation genes were detected in controls (35). Immune response genes were immediately overrepresented in the control group and the KidneyTx recipients had an overrepresentation of apoptotic genes (35). The immune system in SOTR seems to be impaired by the effect of exhausting exercise, pathogen contact and additionally by the immunosuppressive medication (35). This could lead to an increased risk of infection in transplant recipients with potential cell damage and its consequences after exhaustive exercise (35). More research is needed for a definite conclusion, but if strenuous exercise does further transiently suppress SOTRs immune function, a reduction in medication dosage before engaging in the strenuous activity should be evaluated.
A 130 km cycling race in KidneyTx, LungTx, and HeartTx recipients found marathon cycling induced similar inflammation effects compared to healthy individuals (36). When compared to sedentary SOTRs, they had lowered circulating concentration of certain proflogisitc indexes, indicating reduced systemic inflammation (36). Data regarding the functional kidney adaptations that occur during intense and prolonged physical exercise in SOTRs receiving immunosuppressive therapy with nephrotoxic effects remains understudied (69). Mosconi et al. found SOTRs displayed similar positive trends in renal function blood values compared to healthy controls except for urine specific gravity (37). Kidney function seemed to fail in concentrating urine at the peak intensity of the race, and this difference was again more evident 18–24 h after. This was attributed to possible tubular impairment, but overall, it was determined that SOTRs with no cardiovascular contraindications can safely participate in a long-distance road cycling race without acute signs of kidney damage (37).
LungTx and LiverTx recipients have successfully summited high-altitude peaks such as Kilimanjaro (Tanzania) and Jebel Toubkal (Morocco) (38, 39). At their peaks at 5,895 m and 4,167 m above sea level, acute mountain sickness had a high prevalence rate among as ascenders at around 80% (38, 39). Functional pulmonary tests, echocardiographic and vital parameters all displayed similar results to healthy controls which is a favourable indication. However, LungTx recipients displayed poorer cardiopulmonary performance in the 6-minute walk test and the lack of right ventricular cardiac adaptation may indicate underlying autonomic dysregulation (38). It also should be noted that high altitude exposure could have a negative impact on the kidneys as hypoxia may trigger the development of acute and chronic kidney failure (70).
Rare instances stand out as noteworthy exceptions to the prevailing observations regarding comprised exercise capacity among individuals’ post-SOT (71). Alonzo Mourning and Sean Elliot, returned to play in the NBA after a kidneyTx, and Howard Jones won gold, silver and bronze at the European aquatic games after a kidneyTx as well (16). This showcases the potential for remarkable athletic achievements post SOT. A retrospective analysis of the retrieved case studies reveals intriguing insights into the outcomes and challenges encountered by SOTRs across various sporting disciplines, and post-transplant periods. Notable findings include instances of enhanced aerobic and ventilatory capacities among athletes, as evidenced by supernormal oxygen uptake and delayed onset of ventilatory aerobic threshold (18, 42–44, 72). However, these favorable physiological adaptations may be accompanied by challenges such as muscular cramps, hematoma formation, and altered renal function, potentially attributable to immunosuppressive therapies and pre-existing comorbidities (40, 41). Despite these hurdles, several transplant recipients have demonstrated remarkable achievements in competitive sports, ranging from marathons and triathlons, cycling, swimming and bodybuilding, underscoring the potential for post-transplant individuals to engage in high-level athletic pursuits. Of particular interest are the cases of athletes achieving notable milestones, such as completing Ironman distance races spanning over 12 h and professional boxing competitions (45, 73). A major caveat throughout all of these cases is that the accomplishments were attained by individuals who were physically active, or already competing professionally pre-transplantation. Such physiological recuperations are therefore not expected to be attained by recipients who were inactive pre-transplantation. They are indicative of the exceptional dedication, resilience, and pre-existing athletic capacity possessed by the individuals.
None of the identified studies reported any adverse effects following exercise, suggesting high intensity and strenuous exercise is generally well-tolerated and safe for stable SOTRs. This however should be interpreted carefully as all the studies lacked a priori definition of adverse effects.
None of the high intensity interventions or cross-sectional strenuous activity studies found adverse effects post exercise. However, Styelmans et al. hypothesized that most studies relied on retrospective self-reporting of adverse events. This approach may have led to the omission of harms that patients considered insufficiently severe or significant, as well as those they did not perceive as connected to the study (7). They further state that not only are the safety parameters poorly defined and described, but the authors also fail to inform the reader whether dropouts may have been related to adverse events (7). Future studies should implement a priori definitions for adverse events and include a prospective evaluation of potential harms. Additionally, researchers should clearly describe whether dropouts could potentially be related to the applied intervention. Furthermore, some studies lacked active control groups, were underpowered, and had insufficient durations. They also included heterogeneous populations and showed low adherence to protocols. Many studies were not powered to detect secondary outcomes and exhibited bias in selection criteria, as only stable, healthy SOTRs were chosen. These factors make it challenging to generalize the findings to the entire transplant population. Additionally, some participants were not able to attain the required power output demands, and many follow up studies had participant attrition. Lastly, social desirability bias might have led to skewed responses in self-reports, especially for physical activity levels.
The existing body of literature suggests high-intensity exercise presents a viable avenue for safely enhancing various physiological parameters while reducing coronary heart disease prevalence. It is also able to elicit greater than, or equal benefits compared to moderate intensity exercise. Individuals who were active pre-transplantation are able to attain physiological measures equivalent to their healthy counterparts, and in rare instances surpass their pre-transplant thresholds. Furthermore, SOTRs were able to complete strenuous exercises with no reported adverse effects. However, in high intensity exercises, follow-ups indicate low retention rates for HIIT, which resulted in a loss in adaptations. Both strenuous exercises and HIIT interventions had no priori definitions of adverse effects. Future studies should therefore not only address methodological limitations, but also explore strategies to enhance the long- term high intensity exercise adherence. This would provide a more comprehensive understanding of HIIT’s efficacy and sustainability as a therapeutic exercise approach in clinical settings.
AK: Conceptualization, Investigation, Methodology, Project administration, Data curation, Formal Analysis, Writing – original draft. IT: Conceptualization, Data curation, Writing – review & editing. SM: Conceptualization, Methodology, Writing – review & editing. TJ-F: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wiltshire G, Clarke NJ, Phoenix C, Bescoby C. Organ transplant recipients’ experiences of physical activity: health, self-care, and transliminality. Qual Health Res. (2021) 31(2):385–98. doi: 10.1177/1049732320967915
2. Miller WL. Cardiovascular toxicities of immunosuppressive agents. Am J Transplant. (2002) 2(9):807–18. doi: 10.1034/j.1600-6143.2002.20902.x
3. Williams TJ, McKenna MJ. Exercise limitation following transplantation. Compr Physiol. (2012) 2:1937–79. doi: 10.1002/cphy.c110021
4. Corbett C, Armstrong MJ, Parker R, Webb K, Neuberger JM. Mental health disorders and solid-organ transplant recipients. Transplantation. (2013) 96(7):593–600. doi: 10.1097/TP.0b013e31829584e0
5. Chekroud SR, Gueorguieva R, Zheutlin AB, Paulus MP, Krumholz HM, Krystal JH, et al. Association between physical exercise and mental health in 1.2 million individuals in the USA between 2011 and 2015: a cross-sectional study. Lancet Psychiatry. (2018) 5(9):739–46. doi: 10.1016/S2215-0366(18)30227-X
6. Benedetti MG, Furlini G, Zati A, Letizia Mauro G. The effectiveness of physical exercise on bone density in osteoporotic patients. Biomed Res Int. (2018) 2018:4840531. doi: 10.1155/2018/4840531
7. Stylemans D, Vandecruys M, Leunis S, Engelborghs S, Gargioli D, Monbaliu D, et al. Physical exercise after solid organ transplantation: a cautionary tale. Transpl Int. (2024) 37:12448. doi: 10.3389/ti.2024.12448
8. Bednarczyk C, Tansey CM, Fontaine S, Baker S, Laberge É, Mathur S, et al. Community-based exercise program for solid organ transplant recipients: views of exercise professionals and patients. Mcgill J Med. (2021) 19(1):218. doi: 10.26443/mjm.v19i1.218
9. Coates AM, Joyner MJ, Little JP, Jones AM, Gibala MJ. A perspective on high-intensity interval training for performance and health. Sports Med. (2023) 53(Suppl 1):85–96. doi: 10.1007/s40279-023-01938-6
10. Villelabeitia-Jaureguizar K, Vicente-Campos D, Senen AB, Jiménez VH, Garrido- Lestache MEB, Chicharro JL. Effects of high-intensity interval versus continuous exercise training on post-exercise heart rate recovery in coronary heart-disease patients. Int J Cardiol. (2017) 244:17–23. doi: 10.1016/j.ijcard.2017.06.067
11. Rojhani-Shirazi Z, Abolahrari-Shirazi S, Kojuri J, Bagheri Z. Efficacy of combined endurance-resistance training versus endurance training in patients with heart failure after percutaneous coronary intervention: a randomized controlled trial. J Res Med Sci. (2018) 23:12. doi: 10.4103/jrms.JRMS_743_17
12. Oliveira Carvalho V, Guimarães GV, Vieira ML, Catai AM, Oliveira-Carvalho V, Ayub- Ferreira SM, et al. Determinants of peak VO2 in heart transplant recipients. Rev Bras Cir Cardiovasc. (2015) 30(1):9–15. doi: 10.5935/1678-9741.20140055 Erratum in: Rev Bras Cir Cardiovasc. 2015 Mar-Apr;30(2):287. Campos-Vieira, Marcelo Luiz [corrected to Vieira, Marcelo Luiz Campos].25859862
13. Pederson BK, Hoffman-Goetz L. Exericse and the immune system—regulation, integration, and adaptation. Physiol Rev. (2000) 80(3):1055–81. doi: 10.1152/physrev.2000.80.3.1055
14. Königsrainer I, Zieker D, Löffler M, Bühler S, Walter M, Beckert S, et al. Influence of exhaustive exercise on the immune system in solid organ transplant recipients. Exerc Immunol Rev. (2010) 16:184–93.
15. D'Ambrosio A, Toulouse C, Bélanger-Marceau S, Savary S, Mathur S, Segatto B, et al. Characteristics and motivation of solid organ transplant recipients attending the Canadian transplant games. Transplant Proc. (2021) 53(2):581–9. doi: 10.1016/j.transproceed.2020.06.041
17. American College of Sport Medicine. ACSM’s Guidelines for Exercise Testing and Prescription. Amsterdam, Netherlands: Wolters Kluwer (2018). Available online at: https://www.acsm.org/education-resources/books/guidelines-exercise-testing-prescription (cited 2024-05-26).
18. Haykowsky MJ, Riess K, Burton I, Jones L, Tymchak W. Heart transplant recipient completes ironman triathlon 22 years after surgery. J Heart Lung Transplant. (2009) 28:415. doi: 10.1016/j.healun.2008.12.024
19. Hermann TS, Dall CH, Christensen SB, Goetze JP, Prescott E, Gustafsson F. Effect of high-intensity exercise on peak oxygen uptake and endothelial function in long-term heart transplant recipients. Am J Transplant. (2011) 11:536–41. doi: 10.1111/j.1600-6143.2010.03403.x
20. Nytrøen K, Rustad LA, Aukrust P, Ueland T, Hallén J, Holm I, et al. High-intensity interval training improves peak oxygen uptake and muscular exercise capacity in heart transplant recipients. Am J Transplant. (2012) 12:3134–42. doi: 10.1111/j.1600-6143.2012.04221.x
21. Rustad LA, Nytrøen K, Amundsen BH, Gullestad L, Aakhus S. One year of high-intensity interval training improves exercise capacity, but not left ventricular function in stable heart transplant recipients: a randomized controlled trial. Eur J Prev Cardiol. (2014) 21(2):181–91. doi: 10.1177/2047487312469477
22. Yardley M, Gullestad L, Bendz B, Bjørkelund E, Rolid K, Arora S, et al. Long-term effects of high-intensity interval training in heart transplant recipients: a 5-year follow-up study of a randomized controlled trial. Clin Transplant. (2017) 31(1). doi: 10.1111/ctr.12868
23. Nytrøen K, Rolid K, Andreassen AK, Yardley M, Gude E, Dahle DO, et al. Effect of high-intensity interval training in de novo heart transplant recipients in Scandinavia. Circulation. (2019) 139(19):2198–211. doi: 10.1161/CIRCULATIONAHA.118.036747
24. Rolid K, Andreassen AK, Yardley M, Gude E, Bjørkelund E, Authen AR, et al. Long-term effects of high-intensity training vs moderate intensity training in heart transplant recipients: a 3-year follow-up study of the randomized-controlled HITTS study. Am J Transplant. (2020) 20(12):3538–49. doi: 10.1111/ajt.16087
25. Rolid K, Andreassen AK, Yardley M, Gude E, Bjørkelund E, Authen AR, et al. High-intensity interval training and health-related quality of life in de novo heart transplant recipients—results from a randomized controlled trial. Health Qual Life Outcomes. (2020) 18(1):283. doi: 10.1186/s12955-020-01536-4
26. Ulvestad M, Durheim MT, Kongerud JS, Lund MB, Edvardsen E. Effect of high-intensity training on peak oxygen uptake and muscular strength after lung transplantation: a randomized controlled trial. J Heart Lung Transplant. (2020) 39(9):859–67. doi: 10.1016/j.healun.2020.06.006
27. Ulvestad M, Godang K, Durheim MT, Kongerud JS, Brit Lund M, Bollerslev J, et al. Effect of high-intensity training on bone health and body composition in lung transplant recipients: a secondary analysis of a randomized controlled trial. Clin Transplant. (2021) 35(8):e14375. doi: 10.1111/ctr.14375
28. Dall CH, Snoer M, Christensen S, Monk-Hansen T, Frederiksen M, Gustafsson F, et al. Effect of high-intensity training versus moderate training on peak oxygen uptake and chronotropic response in heart transplant recipients: a randomized crossover trial. Am Transplant. (2014) 14(10):2391–9. doi: 10.1111/ajt.12873
29. Dall CH, Gustafsson F, Christensen SB, Dela F, Langberg H, Prescott E. Effect of moderate- versus high-intensity exercise on vascular function, biomarkers and quality of life in heart transplant recipients: a randomized, crossover trial. J Heart Lung Transplant. (2015) 34(7):1053–2498. doi: 10.1016/j.healun.2015.02.001
30. Cappelle M, Masschelein E, Vos R, Van Remoortel H, Smets S, Vanbekbergen J, et al. High-intensity training for 6 months safely, but only temporarily, improves exercise capacity in selected solid organ transplant recipients. Transplant Proc. (2021) 53(6):1836–45. doi: 10.1016/j.transproceed.2021.03.040
31. Rafique M, Solberg OG, Gullestad L, Bendz B, Holm NR, Neghabat O, et al. A randomized clinical study using optical coherence tomography to evaluate the short-term effects of high-intensity interval training on cardiac allograft vasculopathy: a HITTS substudy. Clin Transplant. (2022) 36(1):e14488. doi: 10.1111/ctr.14488
32. Billany RE, Smith AC, Hutchinson GM, Graham-Brown MPM, Nixon DGD, Bishop NC. Feasibility and acceptability of high-intensity interval training and moderate-intensity continuous training in kidney transplant recipients: the PACE-KD study. Pilot Feasibility Study. (2022) 8(1):106. doi: 10.1186/s40814-022-01067-3
33. Hutchinson GM, Cooper AM RE, Nixon DGD, Bishop NC, Smith AC. Effect of high intensity interval training and moderate intensity continuous training on lymphoid, myeloid and inflammatory cells in kidney transplant recipients. Exerc Immunol Rev. (2022) 28:100–15.35452395
34. Masschelein E, De Smet S, Denhaerynck K, Ceulemans LJ, Monbaliu D, De Geest S. Patient- reported outcomes evaluation and assessment of facilitators and barriers to physical activity in the transplantoux aerobic exercise intervention. PLoS One. (2022) 17(10):e0273497. doi: 10.1371/journal.pone.0273497
35. Königsrainer I, Löffler M, Bühler S, Walter M, Schafbuch L, Beckert S, et al. Impact of endotoxin exposure after exhausting exercise on the immune system in solid organ transplant recipients. Exerc Immunol Rev. (2012) 18. cited in: Ovid MEDLINE(R) at. Available online at: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med9&NEWS=N&AN=22876728 (accessed April 04, 2024).
36. Cappuccilli M, Mosconi G, Roi GS, De Fabritiis M, Totti V, Merni F, et al. Inflammatory and adipose response in solid organ transplant recipients after a marathon cycling race. Transplant Proc. (2016) 48(2):408–14. doi: 10.1016/j.transproceed.2016.02.001
37. Mosconi G, Angelini ML, Balzi W, Totti V, Roi GS, Cappuccilli M, et al. Can solid-organ-transplanted patients perform a cycling marathon? Trends in kidney function parameters in comparison with healthy subjects. Transplant Proc. (2016) 48(2):415–9. doi: 10.1016/j.transproceed.2015.12.042
38. Schrutka L, Slama A, Muehlbacher J, Bessa V, Lichtenegger P, Ghimessy Á, et al. Cardiopulmonary response to high-altitude mountaineering in lung transplant recipients-The Jebel Toubkal experience. Scand J Med Sci Sports. (2021) 31(10):1941–8. doi: 10.1111/sms.14008
39. Pirenne J, Van Gelder F, Kharkevitch T, Nevens F, Verslype C, Peetermans WE, et al. Tolerance of liver transplant patients to strenuous physical activity in high-altitude. Am J Transplant. (2004) 4:554–60. doi: 10.1111/j.1600-6143.2004.00363.x
40. De Smet JM, Niset G, Degre S, Primo G. Jogging after heart transplantation. N Engl J Med. (1983) 309(24):1521–2. doi: 10.1056/NEJM198312153092415 (make AMA).6358889
41. Browne G, Allan P, Madhavan KK, Winney R. Exercise-induced anuria in a renal allograft recipient. Nephrol Dial Transplant. (2001) 16(12):2431–3. doi: 10.1093/ndt/16.12.2431
42. Haykowsky M, Tymchak W. Superior athletic performance two decades after cardiac transplantation. N Engl J Med. (2007) 356:2007–8. doi: 10.1056/NEJMc070061
43. Haykowsky MJ, Riess KJ, Baggish AL. Heart transplant recipient finishes the 118th Boston marathon 27 years post-surgery. J Heart Lung Transplant. (2014) 33(11):1197. doi: 10.1016/j.healun.2014.07.013
44. Haykowsky MJ, Halle M, Baggish A. Upper limits of aerobic power and performance in heart transplant recipients: legacy effect of prior endurance training. Circulation. (2018) 137(7):650–2. doi: 10.1161/CIRCULATIONAHA.117.031445
45. Einollahi B, Nafar M, Taheri S, Nemati E. Renal allograft in a professional boxer. Saudi J Kidney Dis Transpl. (2008) 19(2):241–3. doi: 10.4239/sjcdt.2008.241
46. Haykowsky M, Taylor D, Kim D, Tymchak W. Exercise training improves aerobic capacity and skeletal muscle function in heart transplant recipients. Am J Transplant. (2009) 9(7):734–9. doi: 10.1111/j.1600-6143.2008.02531.x
47. Arora S. Immunological and non-immunological markers of cardiac allograft vasculopathy amongst heart transplant recipients (Thesis No. 934). University of Oslo, Oslo, Norway (2010).
48. Ramzy D, Rao V, Brahm J, Miriuka S, Delgado D, Ross HJ. Cardiac allograft vasculopathy: a review. Can J Surg. (2005) 48(4):319–27.16149368
49. Henein MY, Vancheri S, Longo G, Vancheri F. The role of inflammation in cardiovascular disease. Int J Mol Sci. (2022) 23(21):12906. doi: 10.3390/ijms232112906
50. Nytrøen K, Rustad LA, Erikstad I, Aukrust P, Ueland T, Lekva T, et al. Effect of high-intensity interval training on progression of cardiac allograft vasculopathy. J Heart Lung Transplant. (2013) 32(9):925–31. doi: 10.1016/j.healun.2013.06.023
51. Kubo T, Akasaka T, Shite J, Suzuki T, Uemura S, Yu B, et al. OCT compared with IVUS in a coronary lesion assessment: the OPUS-CLASS study. JACC Cardiovasc Imag. (2013) 6(10):1095–104. doi: 10.1016/j.jcmg.2013.04.014
52. Franklin BA. Preventing exercise-related cardiovascular events: is a medical examination more urgent for physical activity or inactivity? Circulation. (2014) 129(10):1081–4. doi: 10.1161/CIRCULATIONAHA.114.007641
53. Eijsvogels TMH, Thompson PD, Franklin BA. The “extreme exercise hypothesis": recent findings and cardiovascular health implications. Curr Treat Options Cardiovasc Med. (2018) 20(10):84. doi: 10.1007/s11936-018-0674-3
54. Barman PM, VanWagner LB. Cardiac risk assessment in liver transplant candidates: current controversies and future directions. Hepatology. (2021) 73(6):2564–76. doi: 10.1002/hep.31647
55. Nassar M, Nso N, Lakhdar S, Kondaveeti R, Buttar C, Bhangoo H, et al. New onset hypertension after transplantation. World J Transplant. (2022) 12(3):42–54. doi: 10.5500/wjt.v12.i3.42
56. Kourek C, Karatzanos E, Nanas S, Karabinis A, Dimopoulos S. Exercise training in heart transplantation. World J Transplant. (2021) 11(11):466–79. doi: 10.5500/wjt.v11.i11.466
57. Thum JS, Parsons G, Whittle T, Astorino TA. High-intensity interval training elicits higher enjoyment than moderate intensity continuous exercise. PLoS One. (2017) 12(1):e0166299. doi: 10.1371/journal.pone.0166299
58. Leunis S, Vandecruys M, Cornelissen V, Van Craenenbroeck AH, De Geest S, Monbaliu D, et al. Physical activity behaviour in solid organ transplant recipients: proposal ofTheory-driven physical activity interventions. Kidney and Dialysis. (2022) 2(2):298–329. doi: 10.3390/kidneydial2020029
59. Mathur S, Levy RD, Reid WD. Skeletal muscle strength and endurance in recipients of lung transplants. Cardiopulm Phys Ther J. (2008) 19(3):84–93. doi: 10.1097/01823246-200819030-00003
60. Braith RW, Conner JA, Fulton MN, Lisor CF, Casey DP, Howe KS, et al. Comparison of alendronate vs alendronate plus mechanical loading as prophylaxis for osteoporosis in lung transplant recipients: a pilot study. J Heart Lung Transplant. (2007) 26(2):132–7. doi: 10.1016/j.healun.2006.11.004
61. Nikkel LE, Hollenbeak CS, Fox EJ, Uemura T, Ghahramani N. Risk of fractures after renal transplantation in the United States. Transplantation. (2009) 87(12):1846–51. doi: 10.1097/TP.0b013e3181a6bbda
62. Lim WH, Ng CH, Ow ZGW, Ho OTW, Tay PWL, Wong KL, et al. A systematic review and meta-analysis on the incidence of osteoporosis and fractures after liver transplant. Transpl Int. (2021) 34(6):1032–43. doi: 10.1111/tri.13863
63. WHO BMI Classification. Global Database on Body Mass Index. Available online at: http://www.who.int/bmi/index.jsp (accessed August 25, 2014).
64. Milaniak I, Dębska G, Król B, Wierzbicki K, Przybyłowski P. Health locus of control and health behaviors in organ transplant recipients: a multicenter. Transplant Proc. (2022) 54(4):995–1001. doi: 10.1016/j.transproceed.2022.02.058
65. Yu H, Zhao X, Wu X, Yang J, Wang J, Hou L. High-intensity interval training versus moderate-intensity continuous training on patient quality of life in cardiovascular disease: a systematic review and meta-analysis. Sci Rep. (2023) 13(1):13915. doi: 10.1038/s41598-023-40589-5
66. Nieman DC, Wentz LM. The compelling link between physical activity and the body’s defense system. J Sport Health Sci. (2019) 8(3):201–17. doi: 10.1016/j.jshs.2018.09.009
67. Patel R, Paya CV. Infections in solid-organ transplant recipients. Clin Microbiol Rev. (1997) 10(1):86–124. doi: 10.1128/CMR.10.1.86
68. Souza D, Vale AF, Silva A, Araújo MAS, de Paula Júnior CA, de Lira CAB, et al. Acute and chronic effects of interval training on the immune system: a systematic review with meta-analysis. Biology (Basel). (2021) 10(9):868. doi: 10.3390/biology10090868
69. Malthur S, Janaudis-Ferreira T, Wickerson L, Singer LG, Patcai J, Rozenberg D, et al. Meeting report: consensus recommendations for a research agenda in exercise in solid organ transplantation. Am J Transplant. (2014) 14:2235e45.
70. Wang B, Li ZL, Zhang YL, Wen Y, Gao YM, Liu BC. Hypoxia and chronic kidney disease. EBioMedicine. (2022) 77:103942. doi: 10.1016/j.ebiom.2022.103942
71. McKenzie KJ, McKenzie DC, Yoshida EM. Solid organ transplant recipients: clinical considerations in the application of exercise. BJSM Online. (2015) 49(2):76–8. doi: 10.1136/bjsports-2014-093583
72. Anselmi F, Cavigli L, Pagliaro A, Valente S, Valentini F, Cameli M, et al. The importance of ventilatory thresholds to define aerobic exercise intensity in cardiac patients and healthy subjects. Scand J Med Sci Sports. (2021) 31(9):1796–808. doi: 10.1111/sms.14007
73. Haykowsky MJ, Riess KJ, Schneider CA. Ironman triathlon performance pre- and post-heart transplant. J Heart Lung Transplant. (2015) 34(5):756. doi: 10.1016/j.healun.2014.12.015
Keywords: high intensity exercise, sports, athletic performance, swimming, cycling, running, transplantation, transplant recipients
Citation: Kayeye A, Triantafyllou I, Mathur S and Janaudis-Ferreira T (2024) The impact of high intensity training and sports on recipients of solid organ transplants: a narrative review. Front. Sports Act. Living 6:1439399. doi: 10.3389/fspor.2024.1439399
Received: 27 May 2024; Accepted: 30 August 2024;
Published: 24 September 2024.
Edited by:
Andrea Ermolao, Università di Padova, ItalyReviewed by:
Ronald Evans, Virginia Commonwealth University, United StatesCopyright: © 2024 Kayeye, Triantafyllou, Mathur and Janaudis-Ferreira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: T. Janaudis-Ferreira, dGFuaWEuamFuYXVkaXMtZmVycmVpcmFAbWNnaWxsLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.