 Ayrton Walshe
Ayrton Walshe Ed Daly
Ed Daly Lisa Ryan
Lisa Ryan- Department of Sport, Exercise and Nutrition, School of Science and Computing, Atlantic Technological University, Galway, Ireland
Introduction: Coaches, practitioners, and leadership in amateur female sport must navigate many obstacles in the pursuit of athlete availability and optimal performance. The present study aims to evaluate opportunities and challenges to both injury prevention and management in amateur female sport, as experienced by mixed-gender coaches, allied healthcare professionals, and general practitioners.
Methods: Semi-structured virtual interviews of coaches, allied healthcare professionals, and general practitioners (N = 25), recruited via convenience snowball sample. Data transcribed verbatim with reflexive thematic analysis through a critical realism framework.
Results: Female-specific issues, education, and resource capital were challenges to the implementation of injury prevention and management in amateur female sport, thus negatively impacting on performance, prevention, and rehabilitation. Opportunities for improved care for female athletes were developing communication and relationships, outsourcing responsibility, and providing greater education, in response to desires for such, and lastly exposure to elite sport and national governing bodies’ protocols.
Discussion: In amateur female sport, developing communication pathways and relationships, along with upskilling coaches, can help better support female athletes, coaches, and healthcare professionals. Leaders and stakeholders must advocate for and support greater education, resourcing, and an understanding of female-specific issues in amateur female sport. It is intended that these findings will provide evidence and opportunities for discourse between stakeholders in amateur female sport to improve standard of supports for female athletes, coaches, and healthcare professionals. These findings may also help practitioners better exploit opportunities and circumvent challenges to improve the welfare and performance of amateur female athletes.
1 Introduction
Female sport has experienced positive growth in participation and commercialization internationally as policymakers and governing bodies aim to improve equality of gender and address the historical male hegemony of sport (1–3). This challenge extends to sport science and medicine literature where a lack of female-specific research results in androcentric findings being implemented in female athletes (4, 5). Such obstacles also necessitate further development of female coaches to advocate and accelerate such change, but currently a lack of opportunities, gender-related issues (such as sexism or bullying), and a lack of governing body or club support commonly exist (6–8).
Despite female-specific research gaps, there is an understanding of distinct injury epidemiology and aetiology compared with for male athletes. Studies have highlighted high rates of knee, ankle, and sport-related concussions (SRCs) in female field-sport athletes (9–11). These injuries can result in significant time loss for female athletes. An SRC can take up to a month for female athletes (12, 13), while an ACL can take between 8.30 and 11.10 months for a full return to play (14). These injuries can also place financial burdens on athletes and insurance claims, supporting the need for injury prevention and management strategies in female athletes (11).
Injury prevention strategies may include appropriate warm-ups, load management, and strength and conditioning. Injury management strategies may include manual therapy, rehabilitation exercises, and graduated return to play (RTP). Both can improve athlete availability and enhance key performance indicators (KPIs) in female athletes (15, 16). These duties should ideally involve cross-disciplinary collaboration of suitably qualified strength and conditioning professionals, allied healthcare professionals (AHPs) (e.g., athletic therapists), and traditional medical professionals (e.g., general practitioners) (15, 17).
In amateur female sport, the availability of sport science and medicine professionals is limited. Qualitative research in Irish amateur female sport has found sub-standard or non-existent medical support in a number of sports, even where allied medical support may be available (18). Research in Gaelic games (native Irish sports including Gaelic football and camogie) athletes found only 11.10% of females had access to medical personnel at every training and match, while 26.10% never had access to such support (compared with 7.20% for males) (19).
The rates of strength and conditioning provision in amateur female sport are currently ambiguous. Research in the above Gaelic football and camogie cohort also found 55.70% of female athletes had no access to an athletic development coach, compared with 34.40% of male athletes (p < 0.01) (19). In elite international rugby union, qualitative research in strength and conditioning professionals acknowledged the lack of athletic development opportunities for their female athletes at their clubs compared with their male counterparts (20). This limited provision of professionals and resources often leads coaches and athletes to assume individual responsibility and resort to improvised injury prevention and management.
National and international governing bodies have acknowledged this challenge, developing injury prevention programmes in soccer (association football) (e.g., FIFA 11), rugby union (e.g., ENGAGE), and Gaelic games (e.g., GAA 15). These programmes have been effective in reducing non-contact injuries, in particular hamstring strain and overuse injuries (21–23). Pragmatic barriers (time, cost) often limit coach education towards such interventions to a single day, but effective implementation may be enhanced by future iterations involving greater support and feedback (24, 25). The rate at which such interventions are implemented in amateur female sport at present is also unclear (19).
Given the potential impact of injury prevention and management in amateur female sport, the following study aimed to explore the experiences of those who interact with amateur female athletes (coaches, allied healthcare professionals, and general practitioners). This exploration aimed to better understand the scope and implementation of injury prevention and management at present, and to determine the perceived challenges and opportunities of such strategies.
2 Materials and methods
2.1 Study background
This study implemented reflexive thematic analysis through critical realism. A critical realist framework was applied because of its suitability for explanatory research and the pursuit of casual relationships (26). The present study pursued a deeper understanding as to the causal relationships that encouraged or discouraged injury prevention and management in amateur female sport. This framework also allowed for explorations of depth reality, that is to say exploring reality through participants’ experiences and perception, the physical events they describe, and the mechanisms that create such scenarios (the casual relationships) (27). Reflexive thematic analysis also recognizes researcher subjectivity in the creation of meaning, thus this study has been prepared based on such experiences (28). AW is a male graduate in BSc Sport & Exercise Science and is embedded in the Irish Concussion Research Centre as a PhD student exploring and validating SRC-RTP in female sport.
The following methodology is prepared in accordance with the consolidated criteria for reporting qualitative research guidelines (COREQ), available in Supplementary Material S1. This study has also been prepared from a sister qualitative exploration of SRC management in amateur female sport (18). This study refers to females as a gendered term unless discussing physiology, in which case female sex is being referred to.
2.2 Sampling
Coaches of female athletes (N = 13), AHPs (N = 9), and general practitioners (GPs) (N = 3) were recruited; this sample included 15 men and 10 women. A convenience sample of six participants was initially recruited through email, text, or via LinkedIn (two per sub-group), with a snowball sampling approach applied thereafter whereby each participant would provide the name of another potential participant. This process was continued until data saturation was achieved (whereby no new themes emerged). Two of these participants were known to AW prior to study commencement.
Table 1 presents the summary data for each participant. To be included, coaches and AHPs were required to have a minimum of 1 year experience in coaching or providing pitch side care to female athletes. Many participants had participation, coaching, or professional experience in amateur male sport. As such, questioning was stated to be specific to their experience in female sport. No minimum requirements were placed on education as there was a desire to capture data on all persons who operate as AHPs and coaches in amateur female sport. Additional attempts to recruit GPs proved unsuccessful because of “lack of time”, and a belief that the study proposed topic of “injury experiences in female athletes” was not relevant to them. Two GPs and one AHP withdrew before interviews took place after initially agreeing to participate. The AHPs included physiotherapists, physical therapists, certified athletic therapists, and sports therapists. Coaches and practitioners worked with female athletes in rugby union, soccer, and native Irish sports within the GAA such as Gaelic football (See here), and camogie (See here). These experiences were at amateur club, provincial, and national league levels across the various sports.
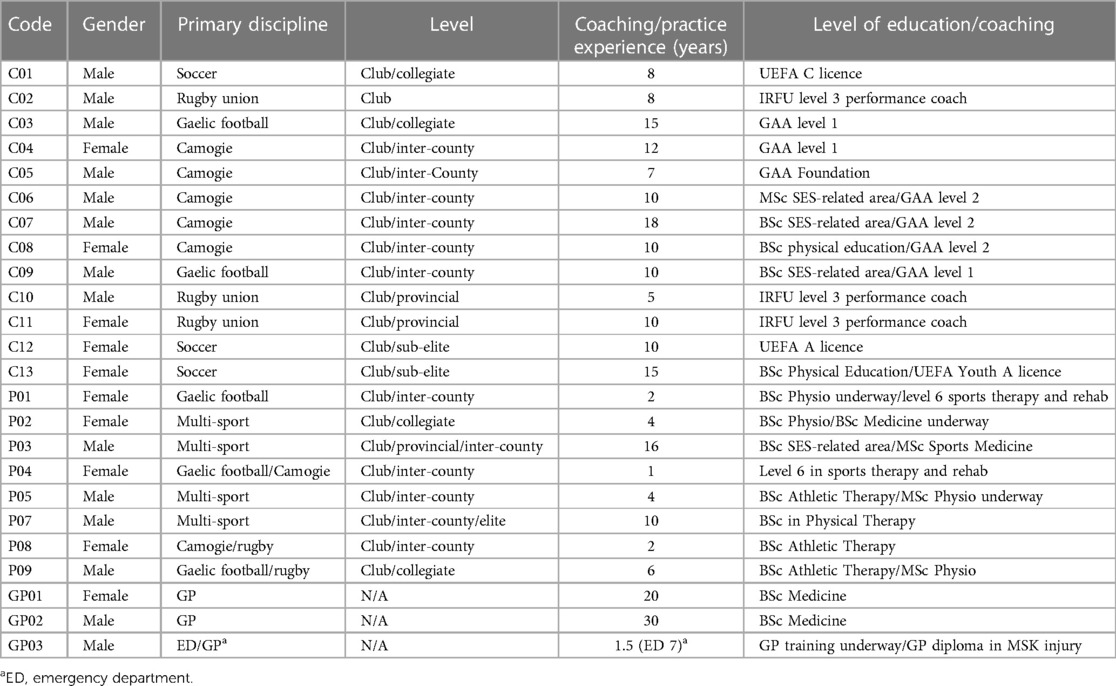
Table 1 Education and experience of coaches (C), allied healthcare practitioners (P), and general practitioners (GP).
2.3 Data collection
Semi-structured interviews were conducted to allow for adaptation depending on the individual's background and experiences; such interviews also allow interviewers to gather in-depth accounts of personal experiences (29). Participants were invited to participate in an informal interview exploring “injury experiences in female athletes”. This broad line of questioning encouraged open discourse and allowed participants to guide the conversation with minimal direction. A reflexive thematic analysis approach was utilized to explore themes across the entire data set. Reflexive thematic analysis provides an opportunity to approach qualitative research with malleable, accessible, and transparent guidelines that appreciates the role of researcher subjectivity and overall knowledge production rather than discovery within analysis (30).
Ethical approval was granted by ATU's Research Ethics Sub-Committee of Academic Council and each participant completed informed consent forms prior to attending virtual interviews on Microsoft Teams. AW conducted pilot interviews with non-eligible coaches to trial the interview format and ensure the interview questions flowed succinctly. Mock interviews were also held with the research team to train AW prior to study commencement. No changes were made following pilot interviews. Interviews averaged (mean ± SD) 47.17 ± 7.5 min in total, each interview commenced with AW explaining the study purpose and interview structure, which included participant background, current experiences and practices, and improving best practice in injury treatment in Irish amateur female sport. A standardized list of interview questions was utilized, but the questions were adapted depending on how each conversation developed. Interviews were recorded on Microsoft Teams and converted to text transcripts in Microsoft Word. The transcripts were compared with the original audio to allow for syntax amendments and to anonymize data; the transcripts were also verified by each member of the research team.
2.4 Data analysis
Data were analysed using reflexive thematic analysis. Semantic codes were included, but codes were primarily latent in nature to capture the underlying ideas, assumptions, and socially constructed beliefs of participants within their responses. This is ultimately necessary as critical realism is informative of reality, but not a direct reflection of it, and thus requires deeper analysis of conversations and codes (31). The transcripts were coded individually by AW in Microsoft Word (MS Corporation, USA) and later exported to Microsoft Excel (MS Corporation, USA); an initial coding framework was used to guide the coding process following familiarization with the interview transcripts. Initial interviews were also cocoded by LR to confirm agreement on the coding framework implemented; however, this framework was reflexively amended throughout the data collection process. As patterns emerged across the data set, codes were summated into sub-themes, which then formed into potential themes. These themes were redefined, revisited regularly, and their sub-themes restructured throughout the data analysis process before the final themes were summated and interwoven within shared meaning in the central organizing concept (30, 32). The data analysis process is available in Figure 1; all coding was manually completed and no coding software tools were utilized. To improve the trustworthiness of data, a number of steps were taken. A “critical friend approach” was implemented with ED and LR providing robustness, insight, and critique through data collection and analysis (33). The participants were provided the opportunity to review and amend their manuscripts to ensure accuracy of transcription and syntax; however, no such changes were required. AW also kept a reflexive diary that tracked interpretations, perceptions, and mind maps throughout the study duration to further support reflexivity in data analysis (33).
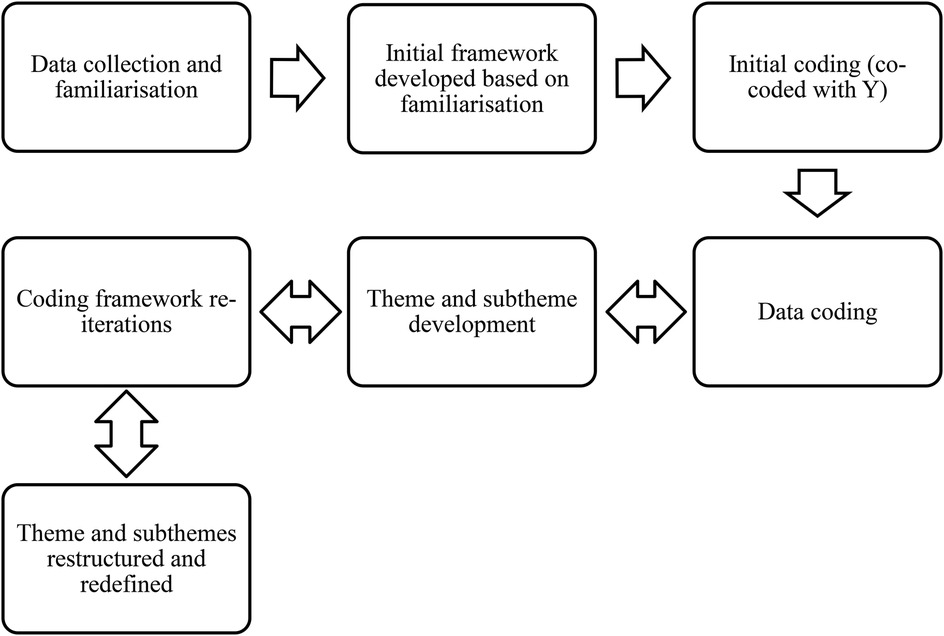
Figure 1 Study data analysis process following Braun and Clarke’s reflexive thematic analysis (30).
3 Results
Challenges and opportunities to injury prevention and management in amateur female sport were identified within participants’ interviews. Three categories and eight sub-categories are presented for each theme in Tables 2, 3, with associated quotes from participants.
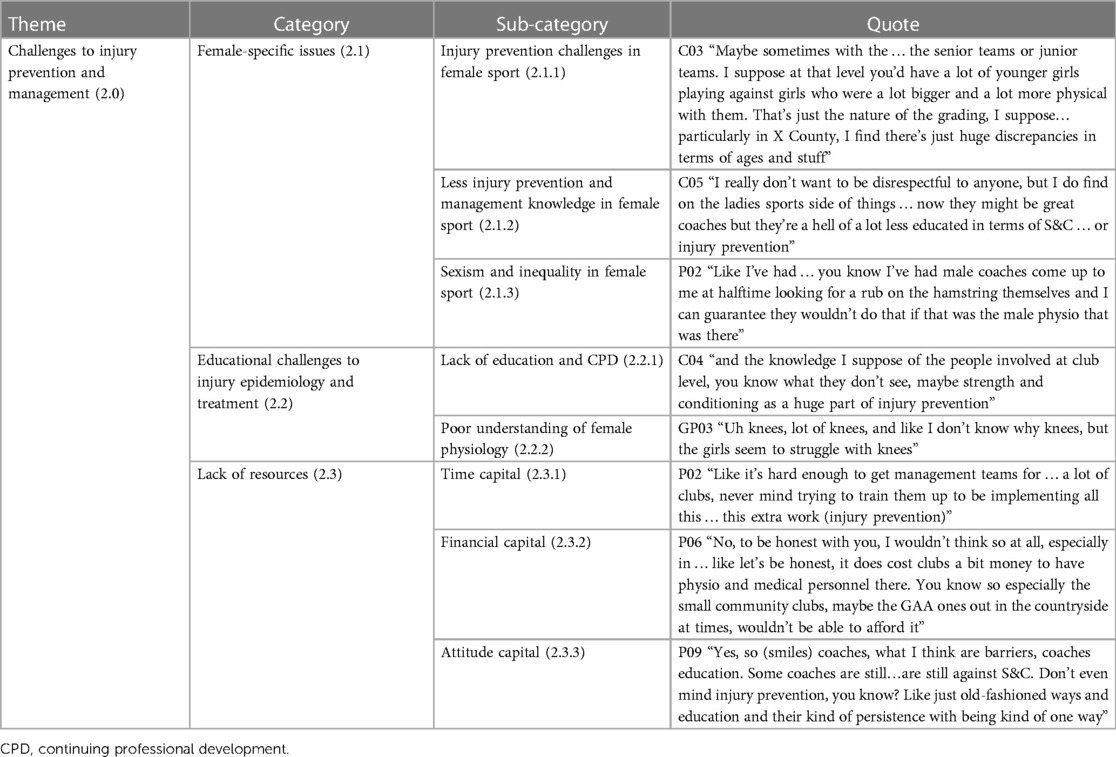
Table 2 Challenges to implementing injury prevention and management in amateur female sport.
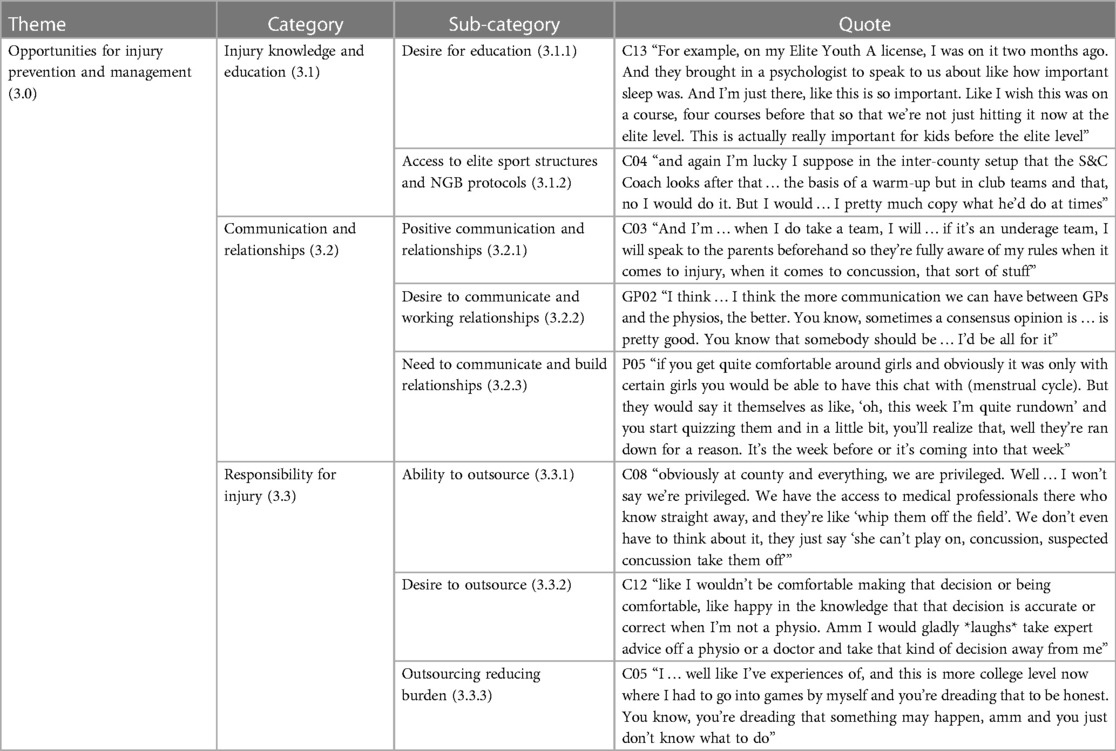
Table 3 Opportunities in implementing injury prevention and management in amateur female sport.
3.1 Theme 1—challenges to implementing injury prevention and management
The challenges to injury prevention and management were discussed by coaches and healthcare professionals alike in the present study, independent of the sport or playing level they operated at. These challenges included the following; female-specific issues, educational challenges, and a lack of resources (Table 2).
3.2 Female-specific issues
Across interviews, participants made references to a variety of challenges that were specific (or more prevalent) to female sport and the athletes they worked with. These issues were related to lesser injury prevention and management, and sexism/inequality in female sport (Category 2.1). All of these sub-categories interact and influence one another to impact female athletes.
Injury prevention challenges in amateur female sport were linked to gulfs between female athletes. Some coaches and practitioners discussed issues whereby two athletes in opposition may have had completely different physical preparation experiences within their sport, which influences injury risk and loading of the less experienced athlete. Although not a uniquely female experience, this may occur more often given the lower participation rates compared with male athletes in some sports/regions; C08 “if I'm an Inter-county (Elite GAA competition) player, and I'm going shouldering a girl who is only 17, and I'm 28, and I have had 10 years of S&C behind me, and this girl is only coming straight outta minor into adult” (Sub-category 2.1.1–2.1.2). These gulfs may not only occur due to age or playing level but may also occur due to positive but late entry into sport. Another challenge that bears the consequences from the abovementioned issue was loading challenges in female athletes; C05 “You know, they wouldn't see the harm in a girl training twice in a day and maybe d’ you know, and maybe doing three or four sessions, dependent on a weekend” (Sub-category 2.1.2).
Coaches also described poorer injury management strategies in female athletes. This was described by participants to be present in both coaches and athletes alike leading to poorer management strategies than their male counterparts; C06 “you often see that if you talk to a fella ‘Yeah I'm going to a physio tomorrow. These are the exercises I have, you know, I'm progressing well’ and then girls ‘Yeah I'm going to the physio for a rub tomorrow and hopefully it'll be OK’” (Sub-category 2.1.2).
Lastly, challenges of inequalities and negative perceptions of female sport impacted on the experiences of those involved. Hostile sexism could be experienced by female coaches and practitioners alike; C13 “So like even when I moved back, like I'm very experienced. And when I moved back, it was a lot of ‘oh, here I'll tell you what you can do now’. And it was something so simple as like make sure that there's footballs around the grid. ‘Ah, thank you’ *thumbs up*”. Such sexism also impacted on inequality in supports, which some teams were beginning to challenge; C08 “As I said, it does cost money and there was always one there for the men and I suppose it was kind of… the girls had brothers and things playing and that… They were like, ‘well, they're getting this. So, it's time now that we kind of follow suit and get what we should be getting’” (Sub-category 2.1.3). If sexism is present in amateur female sport, this may have broader consequences for the equality of resourcing and representation of female coaches and professionals.
3.3 Educational challenges to injury epidemiology and treatment
An anticipated barrier to the uptake of injury prevention and management in amateur female sport is education (Category 2.2). Without accessible education, there is limited stimulation for the uptake of such disciplines by all parties (athletes, coaches, practitioners, and GPs), which is detrimental to effective athlete welfare protocols and overall athletic performance. Coaches and GPs lacked education and understanding in the area of musculoskeletal (MSK) injuries in particular and displayed a clear desire to improve such if provided the opportunity. In addition, poor knowledge of SRC management as advised by national governing bodies (NGBs) was also evident in the interviews; C05 “I suppose then it falls, you know, the management have to try and take it upon themselves, and look, they really don't have the knowledge … the time isn't there? The resources aren't there” (Sub-category 2.2.1).
One key barrier within education was the lack of female-specific knowledge of injury epidemiology and treatment. This was particularly evident in an inability to recognize or understand the anatomical or physiological factors that result in greater risk of knee injuries in female athletes (Sub-category 2.2.2). As a result, the lack of understanding of female physiology in participants meant they regularly stated the sex of the athlete would not influence their approach to their treatment or prevention of injuries. However, in some cases participant demeanour and semantics did seem to indicate a reluctance to admit treating athletes different based on their sex in fear of this being portrayed as sexist; C01 “No, no, no. I've never. I've never treated anyone different based on their gender in terms of the training and the approach, I think it's, you know, it's … football is universal. Like, I think you just you, you're trying to do the same thing, doesn't matter who they I suppose.’
3.4 Lack of resources
Another common barrier that consistently seemed to impact on the perceived feasibility of injury prevention and management in amateur female sport was resources and the lack thereof (Category 2.3). A lack of time, capital, education, and positive injury attitudes were the most common reason for injury prevention, injury management, and strength and conditioning not being implemented in female squads. This was particularly indicated in rural areas where all of the above was amplified to a greater extent than in clubs located in towns and cities. The following quote helps emphasize how each of these can impact progress in introducing concepts like injury prevention in amateur female sport; C06 “I think most clubs would be negated to this sort of stuff, ‘what do we need it for?’, ‘jaysus that's a bit over the top’, ‘how much money does it cost?’ you know so there's definitely an educational ignorance to it. ‘Why do we need it?’ You know ‘why … why is this fella coming in here with this idea?’” (Sub-category 2.3.1–2.3.3).
3.5 Theme 2—opportunities for implementing injury prevention and management
Opportunities for injury prevention and management are evident in the present study, aiding in better procedures and care for athletes. These opportunities include the following: injury knowledge and education, communication and relationships, and responsibility for injury (Table 3).
3.6 Injury knowledge and education
Despite many gaps being evident in participants’ knowledge of injury prevention and management and an admittance of such in amateur female sport, there were favourable opportunities of education derived from participants (Category 3.1). For instance, across the board there was a clear desire among participants interviewed to improve their knowledge of injuries in order to better manage and support female athletes; C04 “On the injury prevention stuff … if there was workshops on, you know … this warm-up reduces the chances of hamstring or ACL injuries or make sure you're incorporating this in your warm-up … I would be straight away jumping at something like that. I've seen so many ACL injuries that you'd be like, am I doing something wrong or am I not including something that I need to include?”. This even led some of the coaches interviewed to attend higher education in pursuit of answers; C07 “That's why I kind of went back to X IT as well, to kind of figure out what the hell is going on with the body in women, more so than men. They're getting all these cruciate injuries, and we're not as much” (Sub-category 3.1.1).
Furthermore, despite acknowledging the limited knowledge and implementation of injury prevention and management strategies in amateur female sport, some participants interviewed did have exposure to NGB-researched injury prevention warm-up or more generalized warm-up protocols. Coaches and practitioners seemed to value the warm-up as a key tool in their arsenal to help prevent injury and improve performance; C11 “So, we work off their warm-up, the injury prevention warm-up. We use that a lot and it does work, like the likes of the single leg or … very important for the knees, for females definitely” (Sub-category 3.1.2). Although it was noted that generalized and loose descriptions (as above) were often used to describe such warm-ups, the actual translation of these protocols and understanding of such may be different in applied practice to those intended by the NGBs.
At least 16 participants in the present study had experience in both amateur and elite settings; this served as an apparent facilitator of awareness of sports science methods, in particular the need to monitor and manage training loads in athletes. While the associated technologies for such monitoring was not available in amateur sport, the coaches and practitioners could carry over this knowledge to help educate and better manage high-risk athletes within their squads; C09 “Take them out of certain things … you might be doing some conditioning stuff. You take them out of that ‘cause they wouldn't need it, you know, they'll be getting enough of that from the other sports/teams. So I … I suppose you would reduce the amount that they're doing … amount of kilometres … trying to keep them as fresh as possible’” (Sub-category 3.1.2).
3.7 Communication and relationships
Positive communication and relationships are paramount to the effective manifestation of injury prevention and management in amateur female sport. Positive communication discussed by interviewees encouraged injury disclosure and management pathways to form between athletes, coaches, and members of any potential multidisciplinary team (Category 3.2). This was prominent in underage athletes where developing communication and relationships with parents’ offered an opportunity for improved disclosure and parental education on the consequences of poor injury management; C03 “I'll talk to parents beforehand, especially the parents of younger kids and you kinda go ‘look, I'll do my best not to put you … put her in a position where I think she might get hurt’” (Sub-category 3.2.1)
It was clear from conversations that there was a desire or need to develop relationships and communicate with the various parties involved with injury management of female athletes. This was key to all parties understanding the loading of athletes each week, especially those in multiple squads or sports. Open communication and relationship development also allowed for discussion regarding the physiological health of female athletes. Only one practitioner alluded to having discourse with athletes regarding their menstrual cycle, which was dependent on rapport; P05 “if you get quite comfortable around girls and obviously it was only with certain girls you would be able to have this chat with (menstrual cycle). But they would say it themselves at like, ‘oh, this week I'm quite rundown’ and you start quizzing them and in a little bit, you'll realize that, well they're ran down for a reason. It's the week before or it's coming into that week” (Sub-category 3.2.2–3.2.3).
3.8 Responsibility for injury management
Overall, responsibility is something that was discussed across all interviews but was perceived differently based on numerous factors such as availability of allied healthcare, academic background, culture and attitudes, and perceived competency (Category 3.3). These variations in context meant some coaches were comfortable managing injuries, some wanted parents involved—others did not, but ultimately all shared a desire to outsource this responsibility to allied healthcare where possible; C03 “having someone there, not that it's a … caught ya or gotcha, but you can turn around and go ‘Is she alright?’ and you're relying on someone's professional ability and that's what they're there for” (Sub-category 3.3.1)
One caveat of responsibility and deciding where this resided was the potential for bias and improper practice influencing the decision-making processes. This links with the abovementioned communication sub-theme where some coaches held meetings with parents prior to the season commencing. These meetings facilitated clear boundaries on the decision-making responsibility for injuries such as SRCs. This in turn prevented parents from trying to overrule the coach's responsibility by attempting to allow their child to return early. From an allied healthcare point of view, each practitioner wanted to be the key instrument in the decision-making process, but also supported the inclusion of parents and coaches in the return to play process.
Many of the coaches, despite understanding the acceptance of some level of responsibility, felt burdened by the risks associated with such. This induced negative emotions when coaching, which could affect their ability to coach effectively, with some linking it to preventing athletes becoming involved in coaching within their sport; C01 “We didn't have a physio for example. We had this physio bag and, you know, someone got injured like or someone went down. It was very scary, you know, this is on me. I don't know anything about this. I mean you're … like, freaked out of your head”. One GP empathized with first aiders and even suggested pitch side care may be a risk to their own careers; GP01 “But it…it would be a big ask for someone to take it on, like asking a member of the community to become like … it's a minefield even for us, you know, even to volunteer to stand at the side of the pitch. It's really controversial. I mean, will our medical insurance cover us?” (Sub-category 3.3.2–3.3.3). While this burden may be perceived as negative, it was often this burden which encouraged coaches to pursue the provision of first aid or allied healthcare for their team.
4 Discussion
The present study aimed to identify challenges and opportunities for injury prevention and management in amateur female sport via the experiences of coaches, allied healthcare professionals, and general practitioners. It is intended that these findings may support coaches, professionals, and leadership in the pursuit of improved injury prevention and management of their female athletes. Through reflexive thematic analysis, the opportunities identified were as follows: access to injury education, development of positive communication and relationships, and ability to outsource responsibility. Challenges to the implementation of injury prevention and management were as follows: female-specific issues, educational challenges, and a lack of resources.
4.1 Overview of key findings
Across interviews, it was clear that participants believed further work is needed to support the integration of injury prevention and management in amateur female sport. Since these interviews were conducted, the GAA have launched a sport science framework that may help guide leadership towards better integration of disciplines for amateur female athletes in Gaelic football and camogie (34). Such a framework, if proven effective, could be adopted by similar NGBs to improve their own integration of sport science and hence injury prevention and management strategies. The lack of resources available was viewed as a primary limiting factor causing such issues in the present study (Category 2.3), a finding previously acknowledged in Irish female coaches (6). Lack of resources may indeed be linked to challenges such as difficulty understanding injury prevention and management and how it can impact amateur female athletes (Sub-category 2.2.1). However, it may also be affected by the investment or spread of such capital, personnel, and resources between male and female athletes seen in other countries (35–37), which has led to national and European projects being developed to improve gender equality and reduce hegemony of amateur and elite sport (38, 39). The experiences within the current study have mimicked recent qualitative research at the elite level of Irish women's soccer whereby financial and personnel restraints were leading to university students being used for medical coverage or clubs sharing pitch side medical care, which brings issues of trust into the injury treatment. This study also recognized the importance of clear communication and relationships between coaches, athletes, and AHPs to ensure injuries are fully disclosed and managed (40).
Opportunities for injury prevention and management were still present despite the challenges described above. Educational pathways and desires to interact with these were paramount to guiding the introduction of such disciplines in amateur female sport. Third level or professional education and exposure to elite sport practice helped shape and encourage any manifestation of injury prevention and management in amateur sport in coaches who had access to such. This emphasizes the need for leadership exposure and opportunities for progression of coaches in amateur female sport to be exposed to and subsequently translate even the fundamentals of injury prevention and management strategies to their amateur cohorts (6). Furthermore, having the ability to communicate and form working relationships with the various stakeholders in athlete welfare (coaches, parents, athletes, allied healthcare) provided the opportunity for informal data gathering and sharing regarding injuries, training loads, and procedures to help support better injury prevention and management of athletes.
Themes of communication have been evidenced in previous research whereby coach communication may be a predictor of concussion disclosure to coaches or sports medicine staff in collegiate athletes (41). Meanwhile research in female rugby union identified poor communication as a mediator of injury disclosure vertically (from amateur to elite programs) and horizontally (across a club program) (42). This study also found that female athletes lacked access to allied healthcare provision; this has also been observed in previous literature on female Gaelic games athletes (19, 43).
Responsibility as an opportunity to improve injury prevention and management was influenced by other sub-categories presented in Tables 2, 3. Where resources were lacking in sub-category 2.3, responsibility often fell to unqualified volunteers (i.e., coaches, parents) to manage injuries, while a coach's attitude to assuming responsibility would be further influenced by their education and experience (Sub-categories 2.2 and 3.1). The lack of provision or funding of support roles, paired with amateur coaches’ clear desire to outsource such responsibilities, presented conflict that inhibited best practice and welfare of athletes, while burdening the coaches volunteering in sport.
4.2 Contextualization to previous research
While novel findings do exist in the present study, the challenges of research and intervention implementation in female sport has been well established in the literature. Emmonds et al. propose a framework for evidence-based approaches in female sport that consider current literature, the female athlete, and the environment in which the athlete operates (44). Qualitative research on Ladies Gaelic football coaches and athletes exploring their injury prevention preferences indicated that interventions must prioritize education around the benefits of injury prevention and how to effectively implement such strategies (25). The present study found that while some participants had knowledge of NGB injury prevention warm-ups, there was brief, generalized language used when discussing such protocols. This may indicate that while participants knew these were useful, they may not have actually understood why and how these protocols impact injury prevention and, in some cases, simply copied what they may have seen coaches or practitioners do previously. Recent research on injury prevention programmes has also suggested that future research incorporate frameworks that support development of coach competency; however, current challenges of time and finance may limit the feasibility of such strategies without leadership advocacy and support of female coaches in this process (24).
Corrigan et al. also stated that stakeholder education was crucial to ensuring widespread uptake of and compliance with the implementation of injury prevention in female Gaelic football players (25). These conclusions were also corroborated by findings from a sister publication of the present study whereby stakeholder inaction was a limiting factor in the implementation of SRC rehabilitation protocols (18). It has been proposed that injury prevention responsibility should increase outward from children to parents, coaches, NGBs, and government bodies (45). It should be stated that the need for greater stakeholder support may not be unique to female sport. For example, a lack of support and resources has also been identified in qualitative research in Irish male field hockey athletes (46).
It is evident from current research that there is a need to develop research and education strategies in amateur female sport regarding injury prevention and management. Delphi research in female rugby union saw 86% of key stakeholders within the sport highlight injury prevention as a key research priority, with even greater priority being placed on the relationship between menstrual cycle and injury (90%), and SRC risk reduction and management (93%). The efficacy of current strength and conditioning practices in female athletes was also listed as a high priority (76%) (5).
Attempts have been made to summarize athletic performance and nutrition best practices for female athletes in Gaelic football (47) and camogie (48) that also improve injury prevention and management, but these works acknowledge that greater research is needed in this area. Previous research has identified gender-gaps in strength and conditioning provision for male and female athletes in American collegiate sport (49). Furthermore, it also found 60% of coaches working with male athletes did not believe gender should influence strength training practice, while 86% of coaches working with female athletes believed gender should have an influence on strength training. Regarding injury prevention and management, gaps in knowledge of female physiology were present among the participants interviewed. This is a pertinent point as the lack of representation of female athletes in sport science literature has led to translation of findings from male literature with little understanding of the impact on sex-differences in physiology on these methodologies (4). The treatment of female athletes similarly to males is also present in skill acquisition coaching as research in female rugby union has identified a limited, male-centred approach to tackle coaching that was perceived as the accepted norm for female participation within their sport (50). A male-centred approach to tackle technique does not take into account issues of breast injuries, which can be prevalent in female contact and collision sport athletes (51).
In the present study, participants were asked during interviews if they would individualize approaches based on athlete sex, and with the exception of one practitioner who acknowledged the menstrual cycle (Sub-category 3.2.3) the response was often “no”. Further interventions are needed to not only ascertain whether male sport science and medicine strategies transfer to female sport, but also to assess the efficacy of interventions to upskill and educate coaches and practitioners on sex-based differences in physiology and injury epidemiology.
4.3 Future research and practical applications
The present study has highlighted multiple avenues for future research in amateur female sport to better support coaches, professionals, and leadership in optimizing injury prevention and management of their athletes. Participants often discussed injury prevention as a broad concept with generalized connecting terms such as “warm-up”, or “recovery” with little understanding of what is attempted to be prevented and how to practically prevent it. Future injury prevention research should assess the efficacy of meshing education and competency development with injury prevention integration in amateur female coaches and athletes. The present study has also highlighted the presence of potential sexism towards female coaches and practitioners, which may be explored in subsequent research to assess the prevalence and manifestation of such instances in amateur female sport.
The practical applications of the present study are that it may inform practitioners working in amateur female sport as to the challenges and opportunities towards injury prevention and management to better aid them in addressing, circumventing, or incorporating these themes to increase adherence and best practices in their squads. This study may also act as a stimulus to encourage discourse between stakeholders, coaches, practitioners, and athletes to better develop appropriate procedures, identify areas for improvement in practice, and to ensure equality of resources to ensure male and female athletes achieve uniform access to personnel and support as required.
4.4 Limitations
Qualitative research requires an acceptance of inherent bias from researchers ontological and epistemological stances, which may also extend to each participants own viewpoints as they see the world. A limited sample size was included in this study and data are representative of participants current or historical experiences, therefore this cannot be representative of their entire sporting environment. Despite best efforts, it was not possible to include additional GPs in the present study. However, this may be indicative of the belief that sports medicine is not within their current scope. In conclusion, the findings of the current study emphasize that those involved in Irish amateur female sport require support in the education and implementation of injury prevention and management strategies. It is clear from the interviews conducted that access to resources, personnel, attitudes, and education were the primary drivers of encouraging or discouraging injury prevention and management.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Ethical approval was granted for the study involving humans by ATU's Research Ethics Sub-Committee of Academic Council and each participant completed and submitted their written informed consent forms to participate in this study prior to attending virtual interviews on Microsoft Teams. The studies were conducted in accordance with the local legislation and institutional requirements.
Author contributions
AW: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft. ED: Conceptualization, Supervision, Writing – review & editing. LR: Conceptualization, Data curation, Supervision, Writing – review & editing.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
AW is a recipient of an ATU (formerly GMIT) RISE MRes Scholarship, which funded this body of research.
Acknowledgments
The authors would like to thank each participant for their time and honesty in sharing their experiences and would like to acknowledge the importance of their work in supporting community sport.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2024.1430287/full#supplementary-material
References
2. Meier HE, Konjer MV, Krieger J. Women in international elite athletics: gender (in)equality and national participation. Front Sports Act Living. (2021) 3:1–20. doi: 10.3389/fspor.2021.709640
4. Cowley E, Olenick A, McNulty K, Ross E. “Invisible sportswomen”: the sex data gap in sport and exercise science research. Women Sport Phys Act J. (2021) 29:1–6. doi: 10.1123/wspaj.2021-0028
5. Heyward O, Emmonds S, Roe G, Scantlebury S, Stokes K, Jones B. Applied sports science and sports medicine in women’s rugby: systematic scoping review and Delphi study to establish future research priorities. BMJ Open Sport Exerc Med. (2022) 8(3):e001287. doi: 10.1136/bmjsem-2021-001287
6. Sport-Ireland. Women in Sport Coaching Research: Where Do Things Stand in Ireland? Dublin, Ireland: Sport Ireland (2020).
7. Barnes S, Adams ML. A large and troubling iceberg: sexism and misogyny in women’s work as sport coaches. Sports Coach Rev. (2022) 11(2):127–46. doi: 10.1080/21640629.2021.1975940
8. Norman L, Simpson R. Gendered microaggressions towards the “only” women coaches in high-performance sport. Sports Coach Rev. (2023) 12(3):302–22. doi: 10.1080/21640629.2021.2021031
9. Horan D, Büttner F, Blake C, Hägglund M, Kelly S, Delahunt E. Injury incidence rates in women’s football: a systematic review and meta-analysis of prospective injury surveillance studies. Br J Sports Med. (2022) 57:471–80. doi: 10.1136/bjsports-2021-105177
10. Peck KY, Johnston DA, Owens BD, Cameron KL. The incidence of injury among male and female intercollegiate rugby players. Sports Health. (2013) 5(4):327–33. doi: 10.1177/1941738113487165
11. O’Connor S, Whyte E, Fortington L, Corrigan J. The cost of injury in ladies Gaelic football: a nine-year analysis (2012–2020) of the LGFA’s injury fund. J Sci Med Sport. (2023) 26(1):31–6. doi: 10.1016/j.jsams.2022.10.007
12. Horan D, Blake C, Hägglund M, Kelly S, Roe M, Delahunt E. Injuries in elite-level women’s football—a two-year prospective study in the Irish women’s national league. Scand J Med Sci Sports. (2022) 32(1):177–90. doi: 10.1111/sms.14062
13. O’Connor S, Bruce C, Teahan C, McDermott E, Whyte E. Injuries in collegiate ladies Gaelic footballers: a 2-season prospective cohort study. J Sport Rehabil. (2020) 30(2):261–6. doi: 10.1123/jsr.2019-0468
14. Figueroa D, Figueroa ML, Figueroa F. Return to sports in female athletes after anterior cruciate ligament reconstruction: a systematic review and metanalysis. J ISAKOS. (2024)9(3):378–85. doi: 10.1016/j.jisako.2024.01.008
15. Calleja-González J, Mallo J, Cos F, Sampaio J, Jones MT, Marqués-Jiménez D, et al. A commentary of factors related to player availability and its influence on performance in elite team sports. Front Sports Act Living. (2022) 4:1077934. doi: 10.3389/fspor.2022.1077934
16. Duggan J, Collins K, Keane K. Factors influencing performance and injury risk in elite female Gaelic team sport players and future research directions: a narrative review. BMC Sports Sci Med Rehabil. (2022) 14:1–13. doi: 10.1186/s13102-022-00553-8
17. Aubrey B, Fulcher ML, Reid D. Defining the role of sport and exercise physicians: the experience of different referrer types in New Zealand. BMJ Open Sport Exerc Med. (2024) 10(2):e001968. doi: 10.1136/bmjsem-2024-001968
18. Walshe A, Daly E, Ryan L. Existence ≠ adherence. Exploring barriers to best practice in sports-related concussion return to play (SRC-RTP) in Irish amateur female sport. Phys Ther Sport. (2023) 63:1–8. doi: 10.1016/j.ptsp.2023.06.004
19. Teahan C, Whyte EF, O’Connor S. Gaelic games players’ awareness and use of, and attitudes towards injury prevention exercise programmes. Phys Ther Sport. (2023) 64:17–26. doi: 10.1016/j.ptsp.2023.08.003
20. Nolan D, Horgan P, MacNamara A, Egan B. “There’s a perfect way to do things, and there’s a real way to do things”: attitudes, beliefs and practices of strength and conditioning coaches in elite international women’s rugby union. Int J Sports Sci Coach. (2023) 18(5):1456–68. doi: 10.1177/17479541231169371
21. Dolan P, Comyns T, Glynn L, Purtill H, Kenny I. A customized warm-up design and controlled feasibility trial in adult amateur rugby union. Med Sci Sports Exercise. (2023) 55:724–5. doi: 10.1249/01.mss.0000986648.63958.5b
22. Soligard T, Myklebust G, Steffen K, Holme I, Silvers H, Bizzini M, et al. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. Br Med J. (2008) 337:a2469. doi: 10.1136/bmj.a2469
23. Schlingermann BE, Lodge CA, Gissane C, Rankin PM. Effects of the Gaelic athletic association 15 on lower extremity injury incidence and neuromuscular functional outcomes in collegiate Gaelic games. J Strength Cond Res. (2018) 32(7):1993–2001. doi: 10.1519/JSC.0000000000002108
24. Guilfoyle L, Kenny IC, O’Sullivan K, Campbell MJ, Warrington GD, Glynn LG, et al. Coaches of youth field sports as delivery agents of injury prevention programmes: how are we training the trainers? A scoping review. Br J Sports Med. (2024) 58(3):144–54. doi: 10.1136/bjsports-2023-106934
25. Corrigan J, O’Keeffe S, Whyte E, Connor S. A qualitative examination of injury prevention strategy and education in ladies Gaelic football: understanding the preferences of players and coaches. PLoS One. (2023) 18:e0281825. doi: 10.1371/journal.pone.0281825
26. Fryer T. A critical realist approach to thematic analysis: producing causal explanations. J Crit Realism. (2022) 21(4):365–84. doi: 10.1080/14767430.2022.2076776
27. Stutchbury K. Critical realism: an explanatory framework for small-scale qualitative studies or an “unhelpful edifice”? Int J Res Method Educ. (2022) 45(2):113–28. doi: 10.1080/1743727X.2021.1966623
28. Gough B, Madill A. Subjectivity in psychological science: from problem to prospect. Psychol Methods. (2012) 17(3):374–84. doi: 10.1037/a0029313
29. Braun V, Clarke V, Weate P. “Using thematic analysis in sport and exercise research”. In: Sparkes A, Smith B, editors. Routledge Handbook of Qualitative Research in Sport and Exercise. London: Routledge (2016). p. 213–27.
30. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qual Res Sport Exerc Health. (2019) 11(4):589–97. doi: 10.1080/2159676X.2019.1628806
31. Willig C. What can qualitative psychology contribute to psychological knowledge? Psychol Methods. (2019) 24:796–804. doi: 10.1037/met0000218
32. Byrne D. A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Qual Quant. (2021)56(2):1391–412. doi: 10.1007/s11135-021-01182-y
33. Mat Noor S, Shafee A. The role of critical friends in action research: a framework for design and implementation. Practitioner Research. (2021) 3:1–33. doi: 10.32890/pr2021.3.1
35. Hextrum K, Sethi S. Title IX at 50: legitimating state domination of women’s sport. Int Rev Sociol Sport. (2022) 57(5):655–72. doi: 10.1177/10126902211037843
36. Casey M, Fowlie J, Charity M, Harvey J, Eime R. The implications of female sport policy developments for the community-level sport sector: a perspective from Victoria, Australia. Int J Sport Policy Politics. (2019) 11(4):657–78. doi: 10.1080/19406940.2019.1618892
37. Parsons JL, Coen SE, Bekker S. Anterior cruciate ligament injury: towards a gendered environmental approach. Br J Sports Med. (2021) 55(17):984–90. doi: 10.1136/bjsports-2020-103173
38. European-Commission. Towards More Gender Equality in Sport. Recommendations and Action Plan From the High Level Group on Gender Equality in Sport. Brussels, Belgium: European Commission (2022).
39. Stapleton N. Sport Ireland women in sport. Stud Arts Humanit. (2021) 7:172–89. doi: 10.18193/sah.v7i1.207
40. Horan D, Kelly S, Hägglund M, Blake C, Roe M, Delahunt E. Players’, head coaches’, and medical personnels’ knowledge, understandings and perceptions of injuries and injury prevention in elite-level women’s football in Ireland. Sports Med Open. (2023) 9(1):64. doi: 10.1186/s40798-023-00603-6
41. Milroy JJ, Wyrick DL, Sanders L, Refisteck E, Beamon E. Student-athlete concussion disclosure and coach communication within collegiate athletics. J Concussion. (2019) 3:2059700219894104. doi: 10.1177/2059700219894104
42. Ryan L, Daly E, Blackett A. Sport-related concussion disclosure in women’s rugby—a social identity approach. Front Sports Act Living. (2023) 5:1–15. doi: 10.3389/fspor.2023.1058305
43. Walshe A, Daly E, Ryan L. Who has the Time? Improving Irish Amateur Female Athletes’ Knowledge and Attitudes Towards Sport-Related Concussion in Four-Minutes. TBC (2023).
44. Emmonds S, Heyward O, Jones B. The challenge of applying and undertaking research in female sport. Sports Med Open. (2019) 5(1):51. doi: 10.1186/s40798-019-0224-x
45. Emery CA, Hagel B, Morrongiello BA. Injury prevention in child and adolescent sport: whose responsibility is it? Clin J Sport Med. (2006) 16(6):514–21. doi: 10.1097/01.jsm.0000251179.90840.58
46. Rees H, Matthews J, McCarthy Persson U, Delahunt E, Boreham C, Blake C. The knowledge and attitudes of field hockey athletes to injury, injury reporting and injury prevention: a qualitative study. J Sci Med Sport. (2022) 25(10):820–7. doi: 10.1016/j.jsams.2022.07.001
47. Duggan J, Keane K, Moody J, Byrne P, Malone S, Collins K, et al. Strength and conditioning recommendations for female athletes: the Gaelic footballer. Strength Cond J. (2023). doi: 10.1519/SSC.0000000000000577
48. Duggan J, Moody J, Byrne P, Ryan L. Strength and conditioning recommendations for female GAA athletes: the camogie player. Strength Cond J. (2020) 42(4):105–24. doi: 10.1519/SSC.0000000000000577
49. Reynolds ML, Ransdell LB, Lucas SM, Petlichkoff LM, Gao Y. An examination of current practices and gender differences in strength and conditioning in a sample of varsity high school athletic programs. J Strength Cond Res. (2012) 26(1):174–83. doi: 10.1519/JSC.0b013e31821852b7
50. Dane K, Foley G, Hendricks S, Wilson F. “It’s always the bare minimum”—a qualitative study of players’ experiences of tackle coaching in women’s rugby union. J Sci Med Sport. (2023) 26(2):149–55. doi: 10.1016/j.jsams.2023.01.002
Keywords: female, qualitative, sports science, sports medicine, field-sport, injury
Citation: Walshe A, Daly E and Ryan L (2024) A qualitative exploration of perceived challenges and opportunities in the implementation of injury prevention and management in amateur female sport. Front. Sports Act. Living 6:1430287. doi: 10.3389/fspor.2024.1430287
Received: 9 May 2024; Accepted: 20 June 2024;
Published: 10 July 2024.
Edited by:
Aine MacNamara, Dublin City University, IrelandReviewed by:
Robin David Taylor, Dublin City University, IrelandUrvi Khasnis, University of Edinburgh, United Kingdom
© 2024 Walshe, Daly and Ryan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lisa Ryan, bGlzYS5yeWFuQGF0dS5pZQ==
†These authors have contributed equally to this work