
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Sports Act. Living , 16 April 2024
Sec. Exercise Physiology
Volume 6 - 2024 | https://doi.org/10.3389/fspor.2024.1371723
 S. von Stengel1
S. von Stengel1 M. Fröhlich2
M. Fröhlich2 O. Ludwig2
O. Ludwig2 C. Eifler3
C. Eifler3 J. Berger3
J. Berger3 H. Kleinöder4
H. Kleinöder4 F. Micke4
F. Micke4 B. Wegener5C. Zinner6
B. Wegener5C. Zinner6 F. C. Mooren7
F. C. Mooren7 M. Teschler7
M. Teschler7 A. Filipovic8S. Müller9K. England9,10J. Vatter8,11S. Authenrieth9,12M. Kohl13
A. Filipovic8S. Müller9K. England9,10J. Vatter8,11S. Authenrieth9,12M. Kohl13 W. Kemmler1*†
W. Kemmler1*†
Whole-body electromyostimulation has proven to be a highly effective alternative to conventional resistance-type exercise training. However, due to adverse effects in the past, very extensive contraindications have been put in place for the commercial, non-medical WB-EMS market. Considering recent positive innovations e.g., federal regulation, mandatory trainer education, revised guidelines, and new scientific studies on WB-EMS application, we believe that a careful revision of the very restrictive contraindications on WB-EMS is needed. This applies all the more because many cohorts with limited options for conventional exercise have so far been excluded. During a first meeting of an evidence-based consensus process, stakeholders from various backgrounds (e.g., research, education, application) set the priorities for revising the contraindications. We decided to focus on four categories of absolute contraindications: “Arteriosclerosis, arterial circulation disorders”, “Diabetes mellitus” (DM), “Tumor and cancer” (TC), “Neurologic diseases, neuronal disorders, epilepsy”. Based on scientific studies, quality criteria, safety aspects and benefit/risk assessment of the category, DM and TC were moved to the relative contraindication catalogue, while arteriosclerosis/arterial circulation disorders and neurologic diseases/neuronal disorders/epilepsy were still considered as absolute contraindications. While missing evidence suggests maintaining the status of neurologic diseases/neuronal disorders as an absolute contraindication, the risk/benefit-ratio does not support the application of WB-EMS in people with arteriosclerosis/arterial circulation diseases. Despite these very cautious modifications, countries with less restrictive structures for non-medical WB-EMS should consider our approach critically before implementing the present revisions. Considering further the largely increased amount of WB-EMS trials we advice regular updates of the present contraindication list.
Whole-body electromyostimulation (WB-EMS) is a recognized training technology that focuses mainly on functional, body composition and health-related outcomes in nonathletic adults (1). Due to its joint friendliness and time efficiency, WB-EMS can be considered as an attractive option for users otherwise unable or unmotivated to exercise conventionally. However, the unique feature of WB-EMS being able to stimulate large muscle areas simultaneously but with dedicated in excess supra-maximum impulse intensity for each region carries the inherent risk of over-straining and adverse effects at least after inadequate WB-EMS application (2, 3). In this context, “the recommended contraindications for the use of non-medical WB-Electromyostimulation” was released by a German expert group in 2019 (4), in order to prevent WB-EMS application in vulnerable cohorts. The limited regulation of WB-EMS, non-mandatory instructor education and evidence gaps on conditions and diseases considered particularly critically for WB-EMS application in essence led to a very restrictive list of absolute contraindications being advised (Table 1). In the last few years however, several positive innovations have fundamentally impacted the commercial non-medical German WB-EMS market. This includes in particular a federal ordinance1 regulating WB-EMS application (5) and mandatory trainer education (6), but also to updated international consensus recommendations for safe and effective whole-body electromyostimulation (7). Considering further that new studies have provided evidence for safe WB-EMS application in cohorts with conditions and diseases absolutely contraindicated to WB-EMS so far, we feel that a revision of the present contraindications is called for so as to carefully open WB-EMS application to people with otherwise limited options and/or motivation for conventional exercise. This might particularly refer to people with arteriosclerosis/arterial circulation disorders, diabetes mellitus, tumor and cancer, neurologic diseases, all absolutely contraindicated to commercial, non-medical WB-EMS. Thus, the aim of the present article is to critically revise the present list of contraindications for WB-EMS application and finally release an updated list of contraindications for WB-EMS based on an evidence driven consensus approach.
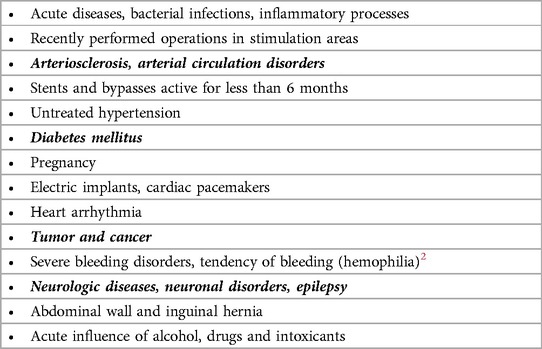
Table 1. Absolute contraindications for WB-EMS (2016). Contraindications printed in bold and italic were subjected to the revision process.
The present revision of the German contraindications on WB-EMS (4) was coordinated by the Institute of Radiology, University Hospital Erlangen, Germany. For the consensus-based decision-making processes on WB-EMS contraindications, we invited German stakeholders of varying backgrounds. Apart from the leading (German) research groups on WB-EMS, we contacted all accredited educational institutions responsible for the education of WB-EMS trainers. Additionally, two selected WB-EMS studios with long experience of commercial, non-medical WB-EMS were included in the consensus process.
During a kick-off meeting in March 2023, our consortium decided to focus on the revision of absolute contraindications for WB-EMS. The list of present absolute contraindications was discussed and the priorities for revisions were fixed (Table 1). Due to their high prevalence, socioeconomic impact, limited options for intensive conventional exercise and their persistent character (in contrast to the acute or rapidly reversible contraindications listed in Table 1), we decided to focus on four categories of absolute contraindications: “Arteriosclerosis, arterial circulation disorders”, “Diabetes mellitus”, “Tumor and cancer”, “Neurologic diseases, neuronal disorders, epilepsy” (Table 1)23.
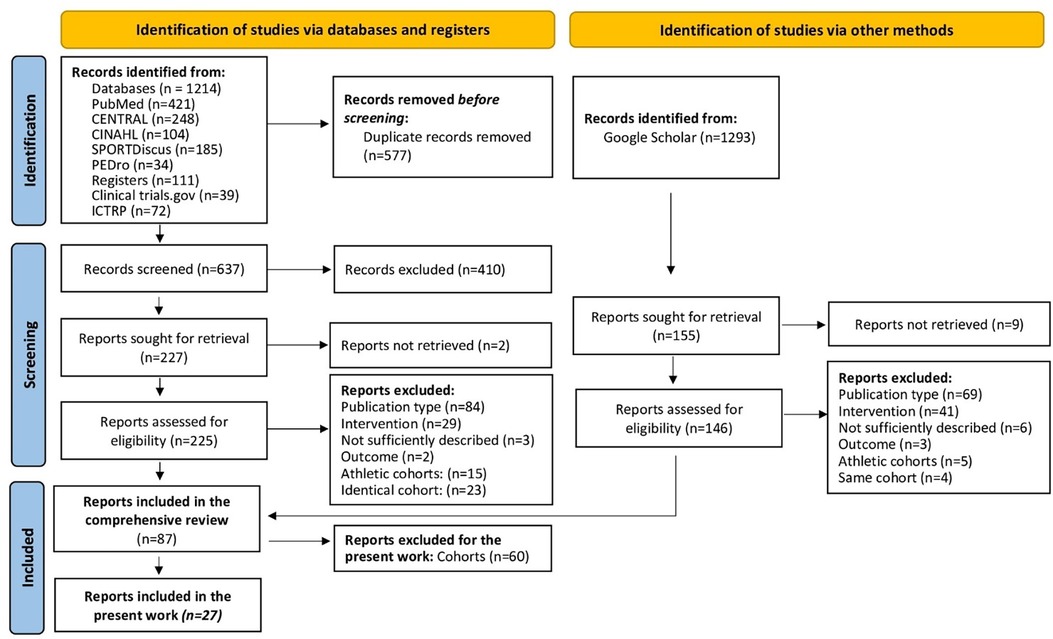
The generation of evidence for WB-EMS application based on a systematic review and evidence map of the literature in the area of WB-EMS intervention studies described in detail in a previous study (1). Briefly, study reports from five electronic databases (Medline [PubMed], The Cochrane Central Register of Controlled Trials [CENTRAL], Cumulative Index to Nursing & Allied Health [CINAHL via Ebsco Host], SPORTDiscus (via Ebsco Host) and The Physiotherapy Evidence Database), two study registers [Clinical trial.gov and the WHO's International Clinical Trials Registry Platform (ICTRP)] published up to 6th March 2023 were searched without language restrictions. To identify additional study reports, we searched Google Scholar manually on the same date as the medical databases.
Eligibility criteria structured according to PICOS (8) were: (Population) Studies with sedentary to non-athletic adult cohorts on average 45 years and older. Studies with athletes or sport students were excluded (Figure 1).
Of importance, for the present work we extended our eligibility criteria and focus to cohorts with “Arteriosclerosis, arterial circulation disorders”, “Diabetes mellitus”, “Tumor and cancer”, “Neurologic diseases, neuronal disorders, epilepsy” and closely related conditions (e.g., the Metabolic Syndrome) (Figure 1) using the comprehensive search process (1) as a basis. (Intervention) Studies that applied Whole-Body Electromyostimulation [WB-EMS (10)] or other kinds of electromyostimulation that can stimulate large muscle areas simultaneously4. Studies that applied local EMS or focus on single muscle groups were not considered. (Comparators) Type or even presence of a control group was not considered as an eligibility criterion. (Outcomes) With few exceptions (e.g., “Anti-G-Straining”) the search process (1) included eligible studies independently of the outcomes addressed (Figure 1). Special emphasis was placed on adverse effects of WB-EMS application. We defined “adverse event” as any untoward medical occurrence, unintended disease or injury. Muscular soreness, discomfort with the stimulation, or increased CK values without clinical relevance were not considered adverse effects. (Study design) All types of longitudinal studies with an interventional study designs (11), i.e., randomized or non-randomized clinical trials and intervention studies with or without control groups, were included. Only peer reviewed research was considered.
Titles, abstracts and full texts were independently screened by two reviewers according to the pre-specified eligibility criteria listed above. Diseases and conditions were classified according to the International Statistical Classification of Diseases and Related Health Problems (ICD-10 GM). We also recorded whether the outcome was defined as the primary/main study outcomes or as secondary/subordinate study endpoints by the authors. To properly address this issue we carefully checked the article but also the study registration and databases where applicable. Disagreements were solved by discussion or with the help of a third reviewer. Reasons for excluding ineligible studies were recorded. In the case of missing data or doubtful information, authors were contacted for a maximum of three times within a 6-week period. We applied the latest version of the DeepL pro translator (Cologne, Germany) for the translation of articles not in English or German language.
Studies identified by the search process (Figure 1) were screened and categorized for study, cohort, participant, exercise and stimulation characteristics (Table 2).
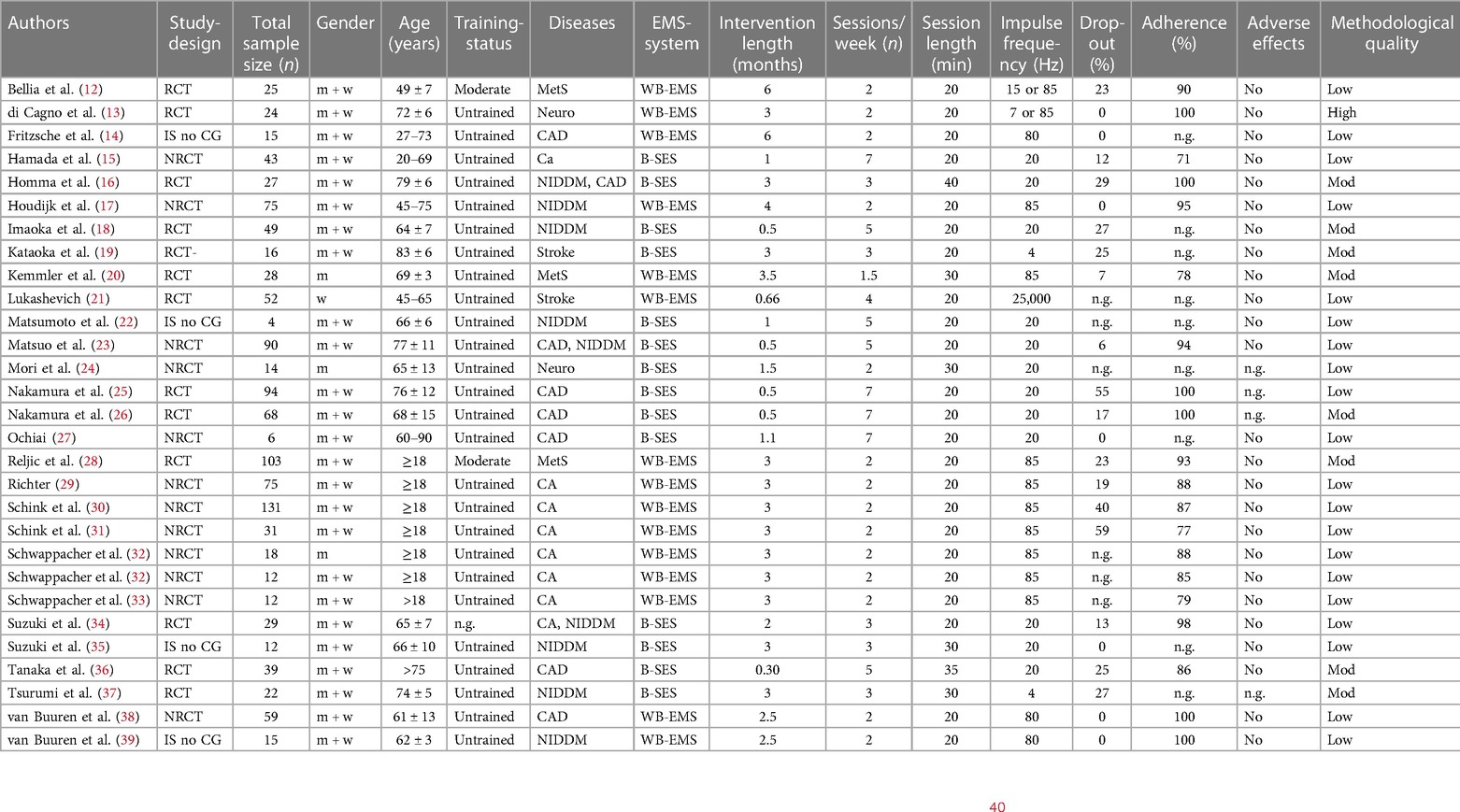
Table 2. Selected characteristics of the included studies.
Methodological quality was rated applying the Physiotherapy Evidence Database (PEDro) Scale Risk of Bias Tool (41), specifically dedicated to physiotherapy and/or exercise studies. Studies with >7 score points were classified as high, 5–7 score points moderate and <5 score points as low methodological quality studies respectively (40) (Table 2). In parallel to the approach listed above, in case of missing data or doubtful information, the authors were contacted for a maximum of three times within a 6-week period.
To provide a quick overview, bubble charts with four dimensions were created with the x-axis listing the correspondent contraindication and with the y-axis presents the number of studies that focus on the corresponding cohort. The shading of the bubble represents whether the health status of the cohort was applied as a criterion for inclusion or reported as a simple co-morbidity (Figure 2).
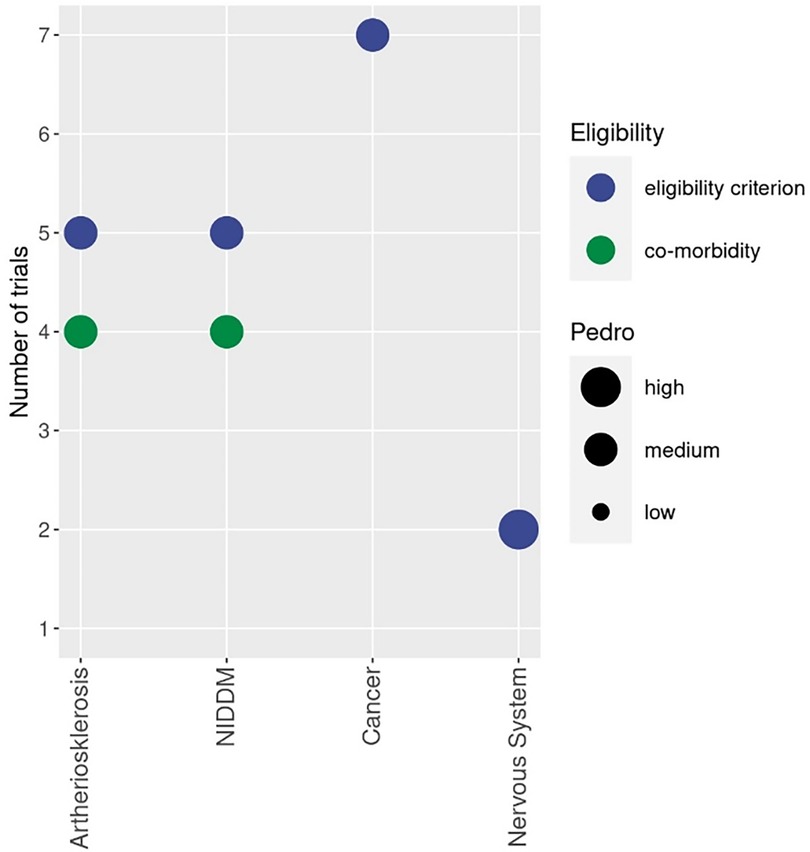
Figure 2. Bubble chart of cohorts with diseases related to the absolute contraindication addressed by WB-EMS studies. Different colours indicate whether the health status of the cohort was applied as a criterion for inclusion (blue) or reported as a simple comorbidity (green). The size of the bubble indicates the methodologic quality according to PEDro (41).
Finally, the size of the bubble indicates the methodologic quality according to PEDro (41). The biggest size indicates at least one study of high methodologic quality [i.e., PEDro Score ≥8 score points (40)] in the category. The lowest size of the bubble chart represents at least one study of low methodologic quality.
Based on the final analysis, the consortium carefully discussed absolute contraindications prioritized for revision (Table 1). The decision of the consortium was based on the number of studies that addressed the corresponding cohort, quality criteria of the trial and safety aspects with specific regard for adverse effects related to the WB-EMS intervention (Figure 2). The decisive factor was finally the benefit/risk assessment of the category. It was agreed that the recommendation must be made in full consensus and agreement within the consortium.
Table 2 provided a rough overview of study, cohort, participant, exercise and stimulationcharacteristics of the 27 reports (Figure 1) included in the present work. For a more detailed overview the reader is kindly refered to the comprehensive publication of Beier et al. (1).
Figure 2 displays cohorts, addressed by WB-EMS in the area of absolute contraindication prioritized for revision.
Cohorts with atherosclerosis, arterial circulation disorders and related diseases were addressed by several studies (Figure 2). One non-controlled cohort study of 10 weeks (14) and a further non-randomized clinical trial of 4 months (38) included solely participants with chronic heart failure (14, 38). Matsuo et al. (23) and Tanaka et al. (36) selected acute heart failure as an eligibility criterion and applied 10 and 14 days of B-SES during hospitalization in their moderate quality studies. In parallel, about 50% of the critically ill patients of Nakamura et al. (25, 26) and 70% of the hemodialysis patients included in the moderate quality RCT of Homma et al. (16) reported heart failure, cardiopulmonary arrest or had a history of ischemic heart disease (16). The same studies reported that about half of their patients suffered from stroke or displayed a history of cerebrovascular events/disease. Stroke patients <6 months after the stroke event were exclusively addressed by the 3-week RCT of Lukashevich et al. (21). In parallel, about 90% of the bedridden older participants of the RCT of Kataoka et al. (19) suffered from cerebral infarction, cerebral or subarachnoid hemorrhage or hypoxic ischemic encephalopathy. Peripheral arterial diseases/severe ischemia of the lower limbs were an eligibility criterion in two studies (22, 27). Two of the studies (25, 26) with critically ill patients failed to report unintended side effects, none of the studies reported adverse effects related to the intervention. Further, the low methodologic quality of most studies that addressed atherosclerosis/arterial circulation disorders linked diseases as an eligibility criterion for inclusion unfortunately dilutes evidence for applying WB-EMS in conditions related to atherosclerosis and arterial circulation and linked diseases.
Five randomized and non-randomized trials or intervention studies without CG applied WB-EMS for two to four months in cohorts with non-insulin dependent Diabetes Mellitus (NIDDM) (17, 18, 35, 37, 39)5. Two of the studies included hospitalized cohorts with end-stage diabetes kidney disease (37) or diabetic ulcers undergoing minor amputation (18). Additionally, four other trials did not focus on, but included a large proportion of participants with NIDDM (16, 22, 23, 34). Of importance, a further three moderate to high quality RCTs (12, 20, 28) focused on cohorts with the Metabolic Syndrome (MetS) applying WB-EMS for 3–6 months. Unfortunately, one study (37) on NIDDM and the MetS failed to report adverse effects. In summary however, evidence for EMS application in NIDDM can be considered moderate-high. Additionally, three low-moderate quality RCTs that applied MetS as a criterion for inclusion (12, 20, 28) and did not observe adverse effects might increase evidence for WB-EMS application in people with cardiometabolic diseases.
In summary, six studies with seven study groups (15, 29–33) addressed cohorts with malignant neoplasms. In particular, the research group of Zopf et al. (29–33) focused on this issue applying WB-EMS for 12 weeks each. So far, the authors have published data on their ongoing advanced cancer project (30) with subgroup analyses on hematological malignancies (31), gastro-intestinal (29), pancreatic (33), prostate (32) and colorectal cancer (32). According to the authors, results for other tumor entities will be published in the newest future. Hamada et al. (15) focused on patients in the early stage of allogeneic stem cell transplant predominately in people with acute leukemia applying WB-EMS for four post-transplantation weeks6. Another study did not focus on, but included cancer patients (34). Of importance, none of the studies reported adverse effects during the intervention. Evidence for WB-EMS application in cancer patients provided by the studies and subgroup-analysis can be considered moderate.
Unfortunately, only a few studies focused on cohorts with diseases of the nervous system (13, 24). The high-quality RCT of di Cagno et al. (13) focused on stage 1 (mild) to 3 (moderate) Parkinson's disease in 50–80 years old patients for 12-week. The NRCT of Mori et al. (24) addressed Huntington patients during dialysis with WB-EMS-application for 6 weeks7. While di Cagno et al. (13) observed no adverse effects; unfortunately Mori et al. (24) did not report unintended effects of WB-EMS application.
Four (24–26, 36) of the 27 included studies did not report adverse effects and did not respond to our corresponding queries. Two of these studies addressed the domain of “arteriosclerosis, arterial circulation disorders” (25, 26), one study focused on the domain of “Diabetes Mellitus” (37) and one study addressed “Neurologic diseases, neuronal disorders, epilepsy” (24). All of the studies applied B-SES in a hospital setting with critically ill patients (25, 26), end stage diabetic disease (37) or Huntington patients during hemodialysis (24).
After a discussion covering (a) the present regulatory framework of WB-EMS in Germany, (b) scientific results on absolute contraindications prioritized by our group and (c) potential harm and negative side effects that could arise if the conditions were to occur, our consortium unanimously decided to move two absolute contraindications, “Diabetes Mellitus” (Type I and II) and “tumor/cancer” to the area of relative contraindications. In particular, due to evidence gaps and severe consequences of adverse effects, we decided to maintain the status of “arteriosclerosis, arterial circulation disorders” and “Neurologic diseases, neuronal disorders, epilepsy” as absolute contraindications (Table 3).
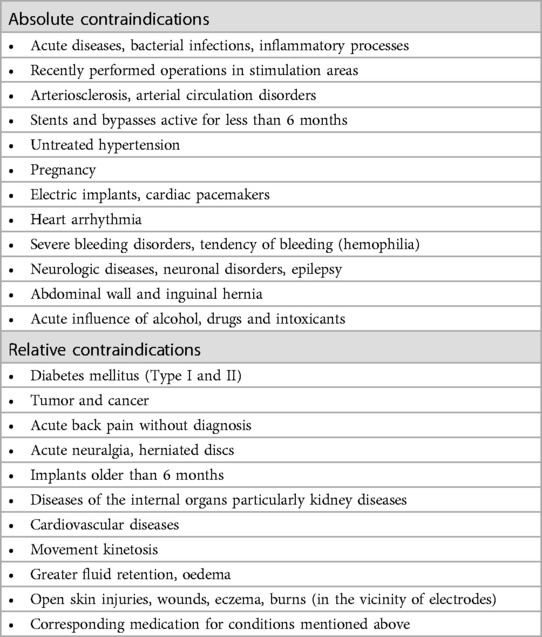
Table 3. Revised list of absolute and relative German contraindications for WB-EMS (2024).
In this context, we define “relative contraindications” as contraindications for which WB-EMS training may only be applied after physician's approval and only with special expertise, licensed education or an adequate medical qualification according to the mandatory NiSV ordinance.
In the present work, our consensus group undertook a very cautious revision of the WB-EMS contraindication list. Finally, only two absolute contraindications, Diabetes Mellitus and tumor/cancer were shifted to the relative contraindication catalogue. Of note, there was an intense discussion about whether cancer/tumor should be completely removed from the contraindications catalog. However due to an ongoing disagreement, the consortium choose the more cautious option. In contrast, arteriosclerosis, arterial circulation disorders and Neurologic diseases, neuronal disorders, epilepsy, were still considered as absolute contraindication. Particularly for the latter cohort a release would have been very welcome considering the low amount of training options for several neurologic limitations and diseases. Nevertheless, we think the rationale for our decision is clear: While missing evidence suggests maintaining the status of Neurologic diseases/neuronal disorders as an absolute contraindication and awaiting further research, in contrast more than a few publications focus on diseases and consequences related to arteriosclerosis/arterial circulation disorders. Nonetheless, considering the severe consequences of adverse effects potentially induced by WB-EMS, the risk/benefit-ratio does not support the use of WB-EMS in people with arteriosclerosis/arterial circulation diseases.
Reviewing other absolute contraindications excluded during round one of the consensus process, i.e., “acute diseases, bacterial infections, inflammatory processes”, “recently performed operations in stimulation areas”, “stents and bypasses active for less than 6 months”, “untreated hypertension”, “pregnancy”, “abdominal wall and inguinal hernia”, “acute influence of alcohol, drugs and intoxicants” should be considered as acute and/or “reversible” contraindications. The latter refer to “untreated hypertension” and in particular “abdominal wall and inguinal hernia” which should receive mandatory medical treatment completely independent of WB-EMS application. Due to severe consequences in case of adverse effects, “electric implants, cardiac pacemakers”, “heart arrhythmia” and “severe bleeding disorders” were also not subjected to the revision. One may argue that our approach was too cautious and there is no or little reason for excluding some cardiovascular and Neurologic diseases from WB-EMS application. We partially agree; however, the present list of contraindication focuses on the use of non-medical whole-body-electromyostimulation. Considering the fast dissemination of medical WB-EMS8 in Germany, we think that people with the few remaining absolute contraindications and limited options for other exercises will be able to exercise in this particularly safe setting.
We do not revise the list of relative contraindications so as to retain the physician as the gatekeeper of the process. In this context, one may criticize that most physicians might be unable to estimate the risk and benefits of WB-EMS well enough to release a WB-EMS application. Here, we do not agree. Considering the commercial application since 2007 with thousands of studios, millions of clients and hundreds of publications (1), most physicians are well aware of WB-EMS. We further feel that the physician's willingness to approve WB-EMS application is significantly supported by the reliable framework of German federal directives (5), mandatory trainer education (6) and (hopefully) the non-mandatory guidelines on safe WB-EMS publication (7, 45). In this context, we would like to explicitly point out that our consortium does not endorse any non-physically supervised WB-EMS application (7, 45). This is even more the case for people with limitations, disabilities and diseases who particularly benefit from close supervision and guidance through well-educated trainers.
We would like to draw the reader's attention to a few special features of our approach. Firstly, we also included studies that applied “Belt Electrode-Skeletal Muscle Electrical Stimulation” (B-SES), a neuromuscular stimulation technique that stimulates large muscle areas, and focuses predominately on frail cohorts in a hospital setting9. While many features are comparable to WB-EMS (1), B-SES uses a monophasic, exponentially climbing pulse. Most importantly however, in contrast to WB-EMS that stimulates all main muscle groups, B-SES focuses on hip and lower extremity muscle groups, applying five [e.g., (16)] or six [e.g., (15)] belt electrodes fixed at the waist/lower back, thigh and ankles. Duration of WB-EMS and B-SES sessions were comparable, while training frequency of B-SES in the included studies is about twice as high. Stimulus intensity of B-SES was consistently described as the maximum tolerable impulse intensity without pain (or discomfort); i.e., largely in line with the specification applied by WB-EMS. For both methods, acute stimulation effects on deeper muscle layers of the thigh and lower legs were reported (46, 47). (2) As a key limitation of the systematic search, we cannot be sure that we identified all eligible articles, particularly due to poor information provided, difficulties in proper translation and, in some cases, missing author responses to our queries. This also applies for “adverse effects” that were not consistently listed by all publications or answered upon request (n = 4). Unfortunately, these included particularly important studies with very vulnerable cohorts (24–26, 36). (3) Due to the specific situation in Germany i.e., federal directives, mandatory trainer education and a medical WB-EMS market, we decided not to include other, non-German working groups on WB-EMS in the consensus process. In parallel, it would be inappropriate to simply transfer the present contraindications to other markets with diverging regulatory structures for non-medical WB-EMS. This particularly refers to countries with non-mandatory specific trainer qualification. (4) Similar to the 2019 list of contraindications (4), our evidence-based, consensus-generated recommendations have no mandatory character. Nevertheless, we recommend all parties to respect the present contraindications to ensure safe WB-EMS application and thus avoid an even more severe restriction (next stage) at a European Union level. (5) Even this updated list of contraindications should not be regarded as the final version. Considering the largely increased amount of WB-EMS trials with a majority of studies that focus on cohorts with limitations or diseases (1), we feel that another update of the contraindications should be performed no later than in 3–4 years.
SS: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Resources, Writing – original draft, Writing – review & editing, Software. MF: Conceptualization, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing, Validation. OL: Conceptualization, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing. CE: Conceptualization, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. JB: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, Formal Analysis, Visualization. HK: Conceptualization, Investigation, Writing – original draft, Writing – review & editing, Data curation, Funding acquisition, Validation. FM: Conceptualization, Investigation, Validation, Writing – original draft, Writing – review & editing, Methodology, Resources. BW: Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing, Formal Analysis. CZ: Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing, Project administration. FM: Methodology, Resources, Writing – original draft, Writing – review & editing, Conceptualization, Validation. MT: Conceptualization, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing. AF: Conceptualization, Methodology, Resources, Writing – original draft, Writing – review & editing, Formal Analysis. SM: Conceptualization, Methodology, Resources, Writing – original draft, Writing – review & editing, Validation. KE: Methodology, Resources, Validation, Writing – original draft, Writing – review & editing, Investigation. JV: Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing, Conceptualization. SA: Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing. MK: Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal Analysis, Software. WK: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing, Funding acquisition, Project administration, Supervision.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We thank all of the authors who provided missing data.
The authors declare the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
1Ordinance on Protection against the Harmful Effects of Non-Ionising Radiation in Human Applications (NiSV).
2Although the 2019 version of the contraindications (20) did not define the severity of the bleeding disorder, it is evident that only severe and life-threatening bleeding disorders should be considered as an absolute contraindication for WB-EMS. For clarity, this aspect has now been added.
3The reasons for focusing on the selected medical conditions are explained again in more detail in the discussion.
4≥50% of skeletal muscle mass.
5Unfortunately, no data on insulin dependent Diabetes Mellitus (DM Type I) was available.
6A further B-SES case control study (42) not included in the evidence map focused on the same cohort.
7Another case control study (43) not included in the evidence map focused on B-SES and virtual reality-guided balance training (30 days) for managing paraplegia after spinal cord infarction.
8According to our definition, medical WB-EMS can be considered as (1) primarily therapeutic intervention (2) based on an existing diagnosis (3) that is provided by qualified medical–therapeutic personnel (4) in compliance with current guidelines and (5) using medical device (44).
9According to the manufacturer (HOMERION, Japan), more than thousand hospitals and care facilities in Japan applied B-SES.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Beier M, Schoene D, Kohl M, von Stengel S, Uder M, Kemmler W. Non-athletic cohorts enrolled in longitudinal whole-body electromyostimulation trials—an evidence map. Sensors (Basel). (2024) 24:972. doi: 10.3390/s24030972
2. Stollberger C, Finsterer J. Side effects of whole-body electro-myo-stimulation. Wien Med Wochenschr. (2019) 169:173–80. doi: 10.1007/s10354-018-0655-x
3. Teschler M, Weissenfels A, Bebenek M, Frohlich M, Kohl M, von Stengel S, et al. Very high creatine kinase CK levels after WB_EMS. Are there implications for health. Int J Clin Exp Med. (2016) 9:22841–50. doi: 10.1007/s10354-015-0394-1
4. Kemmler W, Weissenfels A, Willert S, Fröhlich M, Ludwig O, Berger J, et al. Recommended contraindications for the use of non-medical WB-electromyostimulation. Dtsch Z Sportmed. (2019) 70:278–81. doi: 10.5960/dzsm.2019.401
5. Bundesministerium für Umwelt, Naturschutz, nukleare Sicherheit und Verbraucherschutz, editor. Verordnung zum Schutz vor Schädlichen Wirkungen Nichtionisierender Strahlung bei der Anwendung am Menschen (NiSV) (Vol. Teil I Nr. 41). Bonn: Bundesanzeiger Verlag (2019). p. 1–13.
6. Bundesministerium für Umwelt, Naturschutz, nukleare Sicherheit und Verbraucherschutz, editor. Anforderungen an den Erwerb der Fachkunde für Anwendungen Nichtionisierender Strahlungsquellen am Menschen. Bonn: Bundesanzeiger Verlag (2020). p. 1–54.
7. Kemmler W, Fröhlich M, Ludwig O, Eifler C, von Stengel S, Willert S, et al. Position statement and updated international guideline for safe and effective whole-body electromyostimulation training-the need for common sense in WB-EMS application. Front Physiol. (2023) 14:1174103. doi: 10.3389/fphys.2023.1174103
8. Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al. Cochrane handbook for systematic reviews of interventions version 6.2. Cochrane. (2021) 2021. Available online at: www.training.cochrane.org/handbook.www.training.cochrane.org/handbook (updated February 2021).
9. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:71. doi: 10.1136/bmj.n71
10. Kemmler W, Kleinoder H, Fröhlich M. Editorial: whole-body electromyostimulation: a training technology to improve health and performance in humans? Front Physiol. (2020) 11:523. doi: 10.3389/fphys.2020.00523
11. Thiese MS. Observational and interventional study design types; an overview. Biochem Med (Zagreb). (2014) 24:199–210. doi: 10.11613/BM.2014.022
12. Bellia A, Ruscello B, Bolognino R, Briotti G, Gabrielli PR, Silvestri A, et al. Whole-body electromyostimulation plus caloric restriction in metabolic syndrome. Int J Sports Med. (2020) 41:751–8. doi: 10.1055/a-1171-2003
13. di Cagno A, Buonsenso A, Centorbi M, Manni L, Di Costanzo A, Casazza G, et al. Whole body-electromyostimulation effects on serum biomarkers, physical performances and fatigue in Parkinson’s patients: a randomized controlled trial. Front Aging Neurosci. (2023) 15:1086487. doi: 10.3389/fnagi.2023.1086487
14. Fritzsche D, Fruend A, Schenk S, Mellwig K, Keinöder H, Gummert J, et al. Elektromyostimulation (EMS) bei kardiologischen patienten. Wird das EMS-training bedeutsam für die sekundärprävention? Herz. (2010) 35:34–40. doi: 10.1007/s00059-010-3268-8
15. Hamada R, Sato S, Miyasaka J, Murao M, Matsushita M, Kajimoto T, et al. Belt electrode-skeletal muscle electrical stimulation during early hematopoietic post-transplantation to prevent skeletal muscle atrophy and weakness. Transplant Cell Ther. (2023) 29:51.e51–7. doi: 10.1016/j.jtct.2022.09.030
16. Homma M, Miura M, Hirayama Y, Takahashi T, Miura T, Yoshida N, et al. Belt electrode-skeletal muscle electrical stimulation in older hemodialysis patients with reduced physical activity: a randomized controlled pilot study. J Clin Med. (2022) 11:6170. doi: 10.3390/jcm11206170
17. Houdijk APJ, Bos N, Verduin WM, Hijdendaal MM, Zwartkruis MAL. Visceral fat loss by whole-body electromyostimulation is attenuated in male and absent in female older non-insulin-dependent diabetes patients. Endocrinol Diabetes Metab. (2022) 5:e377. doi: 10.1002/edm2.377
18. Imaoka S, Kudou G, Tsugiyama K, Minata S, Teroh T, Ootsuka M, et al. Efficacy of belt electrode skeletal muscle electrical stimulation in the postoperative rest period in patients with diabetes who have undergone minor amputations: a randomized controlled trial. Int J Low Extrem Wounds. (2022):15347346221077491. doi: 10.1177/15347346221077491
19. Kataoka H, Nakashima S, Aoki H, Goto K, Yamashita J, Honda Y, et al. Electrical stimulation in addition to passive exercise has a small effect on spasticity and range of motion in bedridden elderly patients: a pilot randomized crossover study. Health. (2019) 11:1072–86. doi: 10.4236/health.2019.118084
20. Kemmler W, Birlauf A, von Stengel S. Einfluss von Ganzkörper-Elektromyostimulation auf das Metabolische Syndrom bei älteren Männern mit metabolischem Syndrom. Dtsch Z Sportmed. (2010) 61:117–23.
21. Lukashevich VА, Ponomarev VV, Tarasevich MI, Zhivolupov SА. Functional reciprocal neuromuscular electric stimulation in adaptive kinesitherapy in post-stress patients. Sci Healthc. (2020) 22:80–8. doi: 10.34689/SH.2020.22.3.010
22. Matsumoto JM, Terabe SY, Sakaki RH. Experience of belt electrode skeletal muscle electrical stimulation method for severe lower limb ischemic patients: a case report. Phys Ther Clin Pract Res Educ. (2020) 27:81–5.
23. Matsuo K, Yoneki K, Tatsuki H, Mibu K, Furuzono K, Kobayashi K, et al. Effect of electrical muscle stimulation on the reduction of muscle volume loss in acute heart failure patients. Int Heart J. (2022) 63:1141–9. doi: 10.1536/ihj.22-207
24. Mori K, Tamura Y, Deguchi K, Miura Y, Yura Y, Koizumi T. Effect of belt electrode skeletal muscle electrical stimulation during hemodialysis on the endothelial function in hemodialysis patients. [透析患者に対する透析中のベルト電極式骨格筋電気刺激が血管内皮機能に及ぼす影響]. Jpn J Electrophys Agents. (2020) 27:78–81.
25. Nakamura K, Kihata A, Naraba H, Kanda N, Takahashi Y, Sonoo T, et al. Efficacy of belt electrode skeletal muscle electrical stimulation on reducing the rate of muscle volume loss in critically ill patients: a randomized controlled trial. J Rehabil Med. (2019) 51:705–11. doi: 10.2340/16501977-2594
26. Nakamura K, Nakano H, Naraba H, Mochizuki M, Takahashi Y, Sonoo T, et al. High protein versus medium protein delivery under equal total energy delivery in critical care: a randomized controlled trial. Clin Nutr. (2021) 40:796–803. doi: 10.1016/j.clnu.2020.07.036
27. Ochiai K, Tamura Y, Ehara K, Shimizu R, Matushita Y, Yasu T. Bridging therapy using B-SES for peripheral arterial disease patients with severe lower limb ischemia. J Phys Ther Sci. (2018) 33:545–8.
28. Reljic D, Herrmann HJ, Neurath MF, Zopf Y. Iron beats electricity: resistance training but not whole-body electromyostimulation improves cardiometabolic health in obese metabolic syndrome patients during caloric restriction-A randomized-controlled study. Nutrients. (2021) 13:1640. doi: 10.3390/nu13051640
29. Richter H. Einfluss von Elektromyostimulationstraining und Proteinreicher Ernährung auf Gastrointestinale Tumorpatienten in Palliativer und Kurativer Behandlungssituation. [Effect of Electromyostimulation Training and High-Protein Diet on Gastrointestinal Tumor Patients in Palliative and Curative Treatment Settings]. (Doctor (MD)). Erlangen, Germany: Friedrich-Alexander-University Erlangen-Nürnberg (2019).
30. Schink K, Herrmann HJ, Schwappacher R, Meyer J, Orlemann T, Waldmann E, et al. Effects of whole-body electromyostimulation combined with individualized nutritional support on body composition in patients with advanced cancer: a controlled pilot trial. BMC Cancer. (2018) 18:886. doi: 10.1186/s12885-018-4790-y
31. Schink K, Reljic D, Herrmann HJ, Meyer J, Mackensen A, Neurath MF, et al. Whole-body electromyostimulation combined with individualized nutritional support improves body composition in patients with hematological malignancies—a pilot study. Front Physiol. (2018) 9:1808. doi: 10.3389/fphys.2018.01808
32. Schwappacher R, Schink K, Sologub S, Dieterich W, Reljic D, Friedrich O, et al. Physical activity and advanced cancer: evidence of exercise-sensitive genes regulating prostate cancer cell proliferation and apoptosis. J Physiol. (2020) 598:3871–89. doi: 10.1113/JP279150
33. Schwappacher R, Dieterich W, Reljic D, Pilarsky C, Mukhopadhyay D, Chang DK, et al. Muscle-derived cytokines reduce growth, viability and migratory activity of pancreatic cancer cells. Cancers (Basel). (2021) 13:3820. doi: 10.3390/cancers13153820
34. Suzuki T, Ikeda M, Minami M, Matayoshi Y, Nakao M, Nakamura T, et al. Beneficial effect of intradialytic electrical muscle stimulation in hemodialysis patients: a randomized controlled trial. Artif Organs. (2018) 42:899–910. doi: 10.1111/aor.13161
35. Suzuki Y, Suzuki H, Yato S, Iwasaki H, Eguchi K, Haneda K, et al. Medium-term effects of skeletal muscle electrotherapy with belt electrodes on glucose and lipid metabolism, body composition, muscle strength and muscle endurance in patients with type 2 diabetes. [型糖尿病患者における糖・脂質代謝および体組成, 筋力, 筋持久力に及ぼすベルト電極式骨格筋電気刺激療法の中期的効果]. Phys Ther Sci. (2019) 26:1–10.
36. Tanaka S, Kamiya K, Matsue Y, Yonezawa R, Saito H, Hamazaki N, et al. Effects of electrical muscle stimulation on physical function in frail older patients with acute heart failure: a randomized controlled trial. Eur J Prev Cardiol. (2022) 29:e286–8. doi: 10.1093/eurjpc/zwac022
37. Tsurumi T, Tamura Y, Nakatani Y, Furuya T, Tamiya H, Terashima M, et al. Neuromuscular electrical stimulation during hemodialysis suppresses postprandial hyperglycemia in patients with end-stage diabetic kidney disease: a crossover controlled trial. J Clin Med. (2022) 11:6239. doi: 10.3390/jcm11216239
38. van Buuren F, Mellwig KP, Prinz C, Korber B, Frund A, Fritzsche D, et al. Electrical myostimulation improves left ventricular function and peak oxygen consumption in patients with chronic heart failure: results from the exEMS study comparing different stimulation strategies. Clin Res Cardiol. (2013) 102:523–34. doi: 10.1007/s00392-013-0562-5
39. van Buuren F, Horstkotte D, Mellwig K, Fruend A, Bogunovic N, Dimitriadis Z, et al. Electrical myostimulation (EMS) improves glucose metabolism and oxygen uptake in type 2 diabetes Mellitus patients—results from the EMS study. Diabetes Technol Ther. (2015) 17:413–9. doi: 10.1089/dia.2014.0315
40. Ribeiro de Avila V, Bento T, Gomes W, Leitao J, Fortuna de Sousa N. Functional outcomes and quality of life after ankle fracture surgically treated: a systematic review. J Sport Rehabil. (2018) 27:274–83. doi: 10.1123/jsr.2016-0199
41. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. (2003) 83:713–21. doi: 10.1093/ptj/83.8.713
42. Asano T, Hamada R, Sato S, Miyasaka J, Murao M, Matsushita M, et al. Effects of early post-transplant belt electrode skeletal muscle electrical stimulation therapy on an allogeneic hematopoietic stem cell transplant recipient: a case study. Jpn J Tranplant. (2022) 11:206–10. doi: 10.7889/tct-22-008
43. Michibata A, Haraguchi M, Murakawa Y, Ishikawa H. Electrical stimulation and virtual reality-guided balance training for managing paraplegia and trunk dysfunction due to spinal cord infarction. BMJ Case Rep. (2022) 15:e244091. doi: 10.1136/bcr-2021-244091
44. Berger J, Fröhlich M, Kemmler W. WB-EMS market development—perspectives and threats. Int J Environ Res Public Health. (2022) 19:14211. doi: 10.3390/ijerph192114211
45. DIN. DIN 33961-5. Fitness-Studio—anforderungen an Studioausstattung und -Betrieb—teil 5: Elektromyostimulationstraining [DIN 33961-5. Fitness Studio—requirements for Studio Equipment and Operation—part 5: Electromyostimulation Training]. Berlin: Beuth (2019).
46. Gotz M, Heiss R, von Stengel S, Roemer F, Berger J, Nagel A, et al. Spatial distribution of muscular effects of acute whole-body electromyostimulation at the mid-thigh and lower leg-A pilot study applying magnetic resonance imaging. Sensors (Basel). (2022) 22:10017. doi: 10.3390/s222410017
47. Numata H, Nakase J, Inaki A, Mochizuki T, Oshima T, Takata Y, et al. Effects of the belt electrode skeletal muscle electrical stimulation system on lower extremity skeletal muscle activity: evaluation using positron emission tomography. J Orthop Sci. (2016) 21:53–6. doi: 10.1016/j.jos.2015.09.003
Keywords: whole-body electromyostimulation, contraindications, diabetes mellitus, cancer, neurologic diseases, arteriosclerosis
Citation: von Stengel S, Fröhlich M, Ludwig O, Eifler C, Berger J, Kleinöder H, Micke F, Wegener B, Zinner C, Mooren FC, Teschler M, Filipovic A, Müller S, England K, Vatter J, Authenrieth S, Kohl M and Kemmler W (2024) Revised contraindications for the use of non-medical WB-electromyostimulation. Evidence-based German consensus recommendations. Front. Sports Act. Living 6:1371723. doi: 10.3389/fspor.2024.1371723
Received: 23 January 2024; Accepted: 1 April 2024;
Published: 16 April 2024.
Edited by:
Alessandra Di Cagno, Università degli Studi di Roma Foro Italico, Italy© 2024 von Stengel, Fröhlich, Ludwig, Eifler, Berger, Kleinöder, Micke, Wegener, Zinner, Mooren, Teschler, Filipovic, Müller, England, Vatter, Authenrieth, Kohl and Kemmler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: W. Kemmler d29sZmdhbmcua2VtbWxlckBmYXUuZGU=
†ORCID W. Kemmler orcid.org/0000-0003-3515-0669
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.