 Astrid Gjelstad
Astrid Gjelstad Tine Marie Herlofsen3
Tine Marie Herlofsen3 Fredrik Lauritzen
Fredrik Lauritzen- 1Science and Medicine, Anti-Doping Norway, Oslo, Norway
- 2Department of Pharmaceutical Chemistry, School of Pharmacy, University of Oslo, Oslo, Norway
- 3Department of Pharmaceutics and Social Pharmacy, School of Pharmacy, University of Oslo, Oslo, Norway
Introduction: The aim of the study was to map the use of pharmaceuticals by Norwegian athletes registered on doping control forms (DCFs) in a five-year period to examine general and some class specific use of pharmaceuticals across sports and athlete levels.
Method: Anonymous data from DCFs collected in 2015-2019 were manually entered into a database using the Anatomical Therapeutic Chemical (ATC) system for classification of the pharmaceuticals. Variables entered were year of control, gender, age group, athlete level, sport, test type, nationality, and pharmaceuticals (and dietary supplements) used.
Results: Pain killers in the ATC groups M01 A (Nonsteroidal anti-inflammatory drugs - NSAIDs) and N02 B (other analgesics), and anti-asthmatics in ATC groups R03 A and R03 B were the most frequently used pharmaceuticals. National level athletes reported more use of pharmaceuticals (1.4 ± 1.7 pharmaceuticals per form) than recreational level athletes (0.9 ± 1.2). The highest proportion of DCFs containing information about at least one pharmaceutical were found in speed skating (79.1%), alpine skiing (74.0%), rowing (72.4%) and cross-country skiing (71.7%). Painkillers were most frequently used in muscular endurance sports (30.4% and 21.2 % for M01A and N02 B, respectively) and ball and team sports (17.9% and 17.0%). Use of hypnotics was reported from ice-hockey players and alpine skiers in around 8% of the cases.
Coclusion: Use of anti-asthmatics was most often reported amongst athletes specially exposed to cold, chemicals and heavy endurance training. Athletes in specialized sports requiring high levels of strength and/or endurance reported a higher use of pharmaceuticals out-of-competition compared to in-competition, while there was no such difference in complex sports, such as team, gymnastic, aiming and combat sports.
Introduction
Athletes, like everyone else, on occasion need treatment with pharmaceuticals, for chronic or acute conditions. Since the use of pharmaceuticals is normally linked to symptoms and diseases, athletes, often portrayed as embodiments of a healthy lifestyle, are thus expected to have a relatively low consumption of pharmaceuticals. Conversely, athletes are also often exposed to extreme stress during training and competition, which might lead to increased use of pharmaceuticals.
The World Anti-Doping Agency (WADA) annually publishes a list of substances and methods that are prohibited in sports (1). Many of these substances are found as Active Pharmaceutical Ingredients (APIs) in legal pharmaceuticals. Of all registered pharmaceuticals in The Norwegian Pharmaceutical Product Compendium (2), approximately 13% involve substances or methods prohibited by WADA. Being vigilant when using pharmaceuticals should be a part of active athletes' everyday life in order to avoid unintentional doping, similarly, as has been reported for dietary supplements [e.g., (3)]. The use of pharmaceuticals is thus a part of the athletes' exposome (4), and should also form a part of the athletes' health literacy (5, 6).
All pharmaceutical substances are classified in the Anatomic Therapeutic Chemical (ATC) classification system by The WHO collaborating center for drug statistics methodology (7). The system is intended for monitoring development in usage of pharmaceuticals and for comparison and is widely used for those purposes. It could also potentially be useful in classification of athletes' use of pharmaceuticals. Various studies have examined the use of pharmaceuticals in sports (8–10), within different sport disciplines (11–13), nationalities (14, 15), age groups (16), during major sports events (14, 17, 18) or with focus on specific pharmacological classes, e.g., analgesics (19–21), antibiotics (22, 23), anti-asthmatics (24), allergy medication (25) and decongestants (26). A challenge with the existing literature is the use of different methodologies to map and study the use of pharmaceuticals, making comparisons difficult. By using the ATC system for classification of pharmaceuticals in sport, data for pharmaceuticals down to substance level (fifth level) or pharmacological or therapeutic subgroup (third level) would be readily available.
A better knowledge about the use of pharmaceuticals in different sport disciplines is of high relevance for athletes, medical support personnel, and for anti-doping organizations who educate the athletes in correct use of pharmaceuticals and supplements to avoid unintentional doping. Furthermore, frequency and type of pharmaceuticals used in the different disciplines are essential knowledge for discussing a potential medicalization of sport. Claims about such medicalization appear regularly (27, 28). Several studies have reported athletes using painkillers before a competition to avoid possible pain from injuries (20), taking sleeping pills to cope with a tight match program or travel across time zones (29, 30) and using oral antibiotics liberally (8). By focusing on use of pharmaceuticals in sport, athletes and support personnel might be made aware of the potential harmful effects of incorrect use leading to more rational use and better health. Patterns of use of pharmaceuticals can also be a useful source of information for sports pharmacists in their assistance for athletes (31).
In this project, the use of pharmaceuticals by Norwegian athletes registered on doping control forms (DCFs) in a five-year period (2015–2019) is mapped to examine general and some class specific use of pharmaceuticals amongst athletes in Norway.
Method
Doping control forms (DCFs) from all doping controls where Anti-Doping Norway (ADNO) had been the Testing authority (i.e., the anti-doping organization that authorized testing on athletes it has authority over) from the period 2015–2019 were included in the study. The material included DCFs from doping controls of Norwegian athletes performing their sport in Norway or abroad, as well as from athletes from other countries exercising their sport in Norway under the jurisdiction of a Norwegian sport federation organized under the Norwegian confederation of sport, and Olympic and Paralympic Committee.
The DCFs included in the present study were collected from ADNOs own paper archives, stored according to Norwegian laws and in compliance with World Anti-Doping Code article 14.6 (32). Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
The study was approved by Regional Committees for Medical Research Ethics, ID 29318. As the data from the Doping Control Forms were fully anonymized, there was no need for the athletes to give informed consent.
Development of database
The following information from each DCF were manually registered into an electronic database using Microsoft Excel: Year of the control, gender, age group (<20; 20–24; 25–29; 30–34; 35–40; >40), athlete level (i.e., recreational level (RL) or national level athlete (NLA)), sport, sport discipline, type of test (i.e., whether the sample was collected in-competition (the period commencing at 11:59 p.m. on the day before a competition in which the athlete is scheduled to participate through the end of such competition and the sample collection process related to such competition) or out-of-competition) and nationality. Pharmaceuticals and dietary supplements noted by the athlete on the DCF were also recorded, as the athlete is required to register any pharmaceuticals and supplements taken the last seven days before the control. The data were registered fully anonymized, thus no identifiers like name, address, sample code and exact age or date of the control were included in the database.
To compare the use of pharmaceuticals across sport categories, sport disciplines were classified based on physiological characteristics and put into the following groups: Aiming sports, Ball and team sports, Combat sport, Gymnastic sports, Muscular Endurance sports, VO2max endurance sports, and Strength and Power sports (33) (see Table 2 for examples of sport disciplines in each category).
The number of DCFs retrieved from the paper archives per year was checked against the WADA Anti-Doping Administration and Management System (ADAMS) DCF report to ensure that the DCF paper copies reflected the actual number of doping tests performed in 2015–2019.
The pharmaceuticals were classified according to the Anatomical Therapeutic Chemical (ATC) Classification System. To easily associate the name of the pharmaceutical product with the ATC code, a matrix was developed in Excel; a list of all registered pharmaceutical products in Norway was obtained from The Norwegian Pharmaceutical Product Compendium (7,510 unique products per 11.06.2020). When a pharmaceutical product name was entered in one cell in Excel, the corresponding ATC code then appeared automatically in the neighbor cell.
The ATC codes were registered down to the substance level (level 5). However, for practical reasons, the ATC codes were recoded to the third level indicating the therapeutic/pharmacological subgroup and most of the data in this paper refers to the third level.
Statistics
IBM SPSS Statistics v. 28.0.0.0 were used for descriptive statistics. Continuous data and categorical variables are presented as mean ± SD and percentages, respectively. Pearson's chi-square tests were used to test associations between categorical variables. Analysis of variance (ANOVA) was used to compare trends in pharmaceutical use over time. The Mann-Whitney U Test were used to compare the numbers of pharmaceuticals between athlete levels. The threshold for statistical significance was set to p = 0.05.
Results
General population
Totally 10 418 DCFs (males: 76.2%, n = 7,939; females: 23.8%, n = 2,479) were included in the study. On average, 2,084 ± 96 annual number of DCFs were recorded from the period 2015–2019. Of the 10 418 DCFs registered, 40.6% of the forms were obtained from recreational athletes (n = 4,234), while 59.4% were national or international level athletes (n = 6,184) (Table 1). The majority of the athletes were in the age groups 20–24 (34.7%) and 25–29 years (32.2%). Athletes with Norwegian citizenship constituted 93.6% of the DCFs, while 6.4% were from athletes with other nationalities. In total, the material represents athletes from 67 different sport disciplines, where 25 of them encompass more than 100 DCFs each for the whole study period (Table 1). Of all DCFs, 45.6% were collected in-competition (IC), whereas 54.4% were obtained from athletes out-of-competition (OOC) (Table 2).
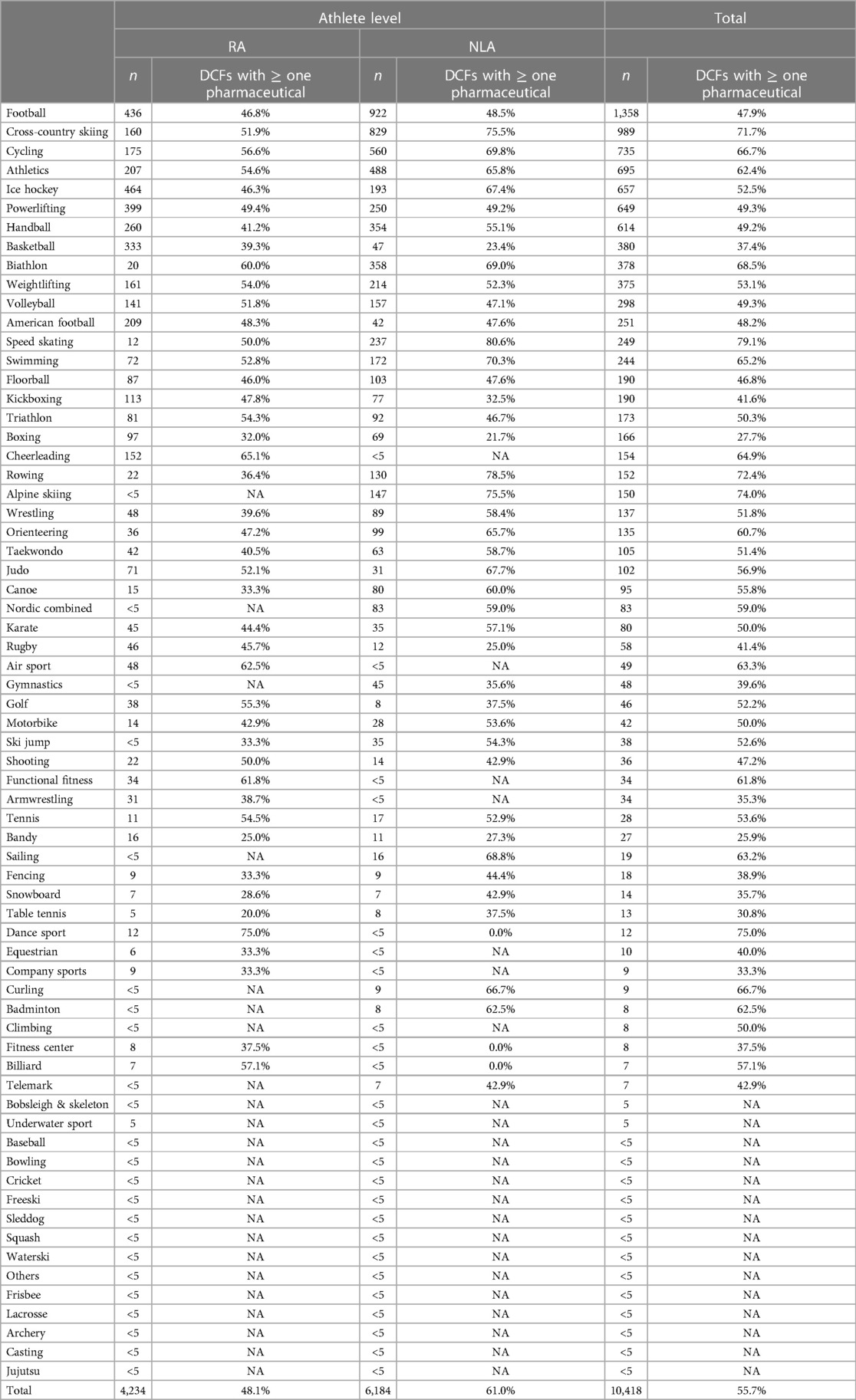
Table 1. Number of doping control forms (DCFs) (n) in each sport discipline and athlete level (RA: recreational athlete; NLA: national level athlete)—and proportion of the DCFs containing information about ≥one pharmaceutical (NA: not applicable).
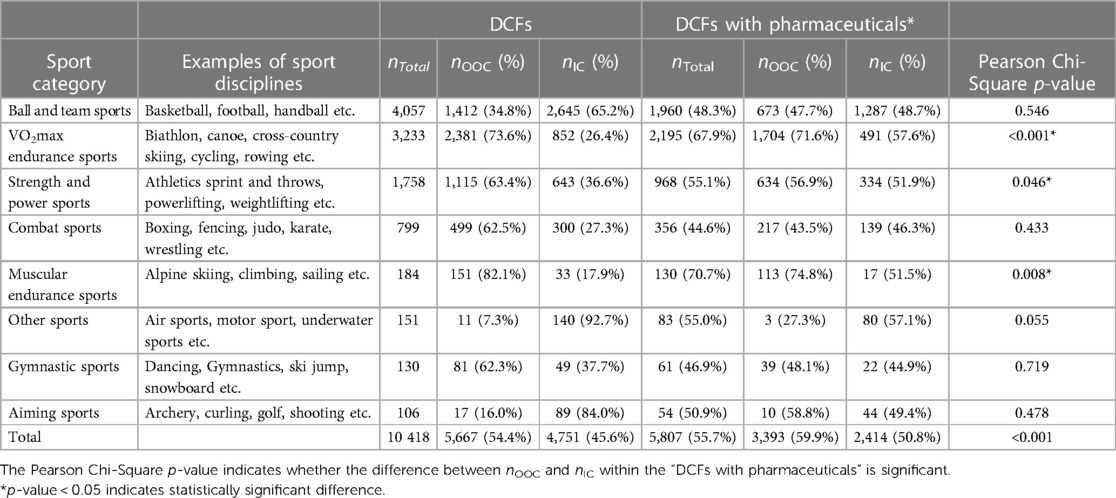
Table 2. Categorization of sport disciplines with associated total number of doping control forms (DCFs); number and proportion of DCFs with information aboutf ≥1 pharmaceutical divided into type of test (sampling out-of-competition (OOC) or in-competition (IC)).
Of all DCFs, 77.7% (n = 8,091) contained information about at least one product, that is either a pharmaceutical and/or a dietary supplement, whereof 3,012 forms (28.9%) included both a pharmaceutical and a dietary supplement. Overall, the average number of products per form was 2.4 ± 2.3, whereas the maximum number of products given on a single form was 22. Information about one or more pharmaceuticals were provided on 55.7% (n = 5,807) of the DCFs (1.2 ± 1.6), with a maximum of 15. The reported use of dietary supplements is further described in a separate paper (34).
Trends over time
The proportion of DCFs containing information about one or more pharmaceutical(s) was used as an indicator of general pharmaceutical use. In 2015, the percentage was 52.0% for all DCFs, while the highest percentage was registered in 2019 (58.4%). The difference between 2015 and 2019 is significant (p < 0.001) although a decrease was observed in 2018.
A difference between males and females appeared, as regards the degree of increase over time. In the period 2015–2019, the percentage of DFCs with one or more pharmaceutical were relatively constant around 50% for males with no significant differences within the years, whereas the DFCs obtained from female athletes increased significantly from 66.9% to 79.4% in the same period (p < 0.001). The mean of pharmaceuticals per DCFs also differed between the genders, even if the oral contraceptives are removed from the results (Figure 1).
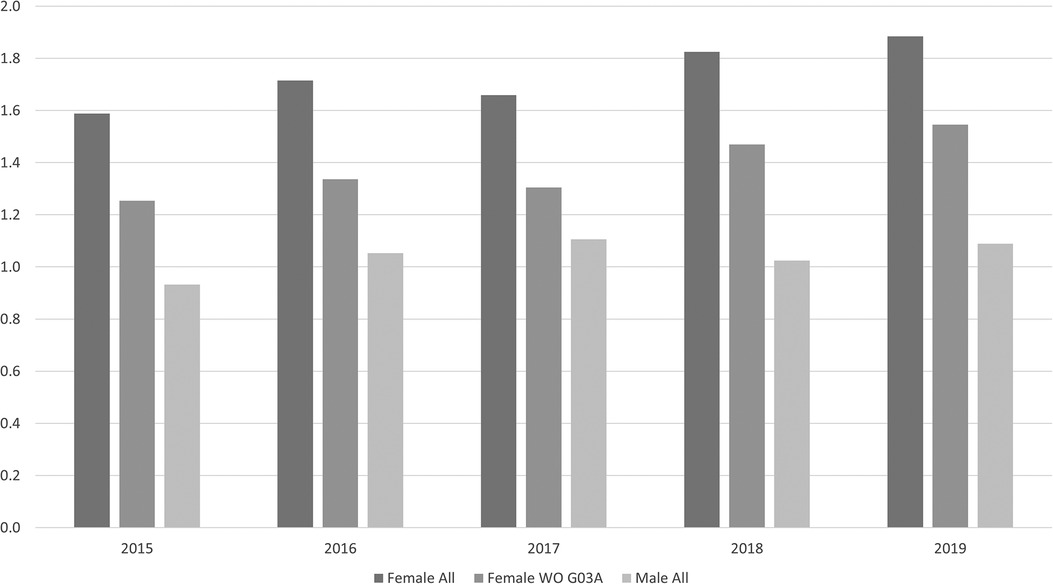
Figure 1. Mean number of pharmaceuticals per doping control form (DCF) from female athletes including (female All) and excluding contraceptives (without (WO) G03A) compared to male athletes (male All) in the period 2015-2019.
Overall registration of pharmaceuticals
Pharmaceuticals representing 126 different ATC codes at level 3 were identified. The most frequent ATC codes appearing in the database were R03B (Other drugs for obstructive airway diseases, inhalants) and M01 A (Anti-inflammatory and antirheumatic products, non-steroids), which were registered 1,731 and 1,730 times, respectively (on average at 16.6% of all DCFs) (Figure 2). Other pharmaceuticals mainly used in treatment of asthma, ATC code R03 A (Adrenergics, inhalants) constitute the third most frequent ATC code (13.5%), closely followed by Other analgesics and antipyretics (N02 B), which were found 1,397 times (13.4%). In total, 14 unique level 3 ATC codes appeared in the database 100 times or more (Figure 2).
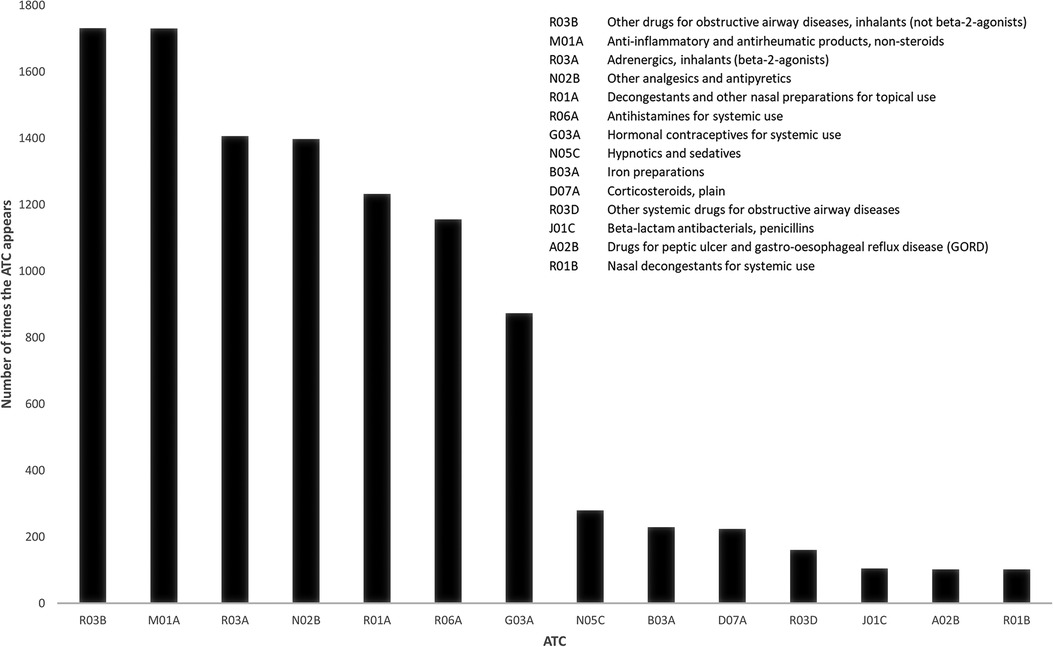
Figure 2. Frequencies of ATC codes (level 3) found on DCFs from the period 2015-2019. Only ATC codes appearing >100 times are included.
Athlete level
The average number of pharmaceuticals registered per DCF was higher amongst national level athletes (NLA) (1.4 ± 1.7) compared to recreational athletes (RA) (0.9 ± 1.2) (p < 0.001). The highest number of pharmaceuticals registered on a single DCF was 15 in the NLA group, and eight in the RA group. In 82 cases (1.9%), five or more pharmaceuticals were registered on a single DCF from RA, whereas the corresponding number was 360 (5.8%) from NLA. The same trend appeared when the results were further divided into genders. Female RA declared in average 1.46 ± 1.5 pharmaceuticals per DCFs, while female NLA declared in average 1.88 ± 1.8 pharmaceuticals. The corresponding results for male RA were 0.76 ± 1.1 and 1.26 ± 1.65 for the male NLA, respectively.
Sport type
Athletes from various sport disciplines display various use of pharmaceuticals (Table 1). The highest share of pharmaceutical use was found among speed skaters (79.1% (197 out of 249) of the DCFs contained information about at least one pharmaceutical), whereas the lowest use was found in boxing (27.7%; 46 out of 166). In general, endurance sport requiring a high VO2max used more pharmaceuticals than team- and ball sports.
The data was further split in sport categories for the top four of the most frequently used ATC codes, which include two groups of asthma medication (R01A and R01B) and to groups of pain killers (M01A and N02B), respectively (Table 3). In addition, the results for the hypnotics in ATC group N05C were included in the results, as pharmaceuticals within this ATC group appeared to be frequently used in certain sports. The differences between the sport categories regards to use of asthma medication range from 28.4% of R03B in the VO2max endurance sports down to 1.1% within the Ball and team sports. The use of pain killers did not follow a clear pattern between the sport categories; however, muscular endurance athletes tend to use slightly more than others.
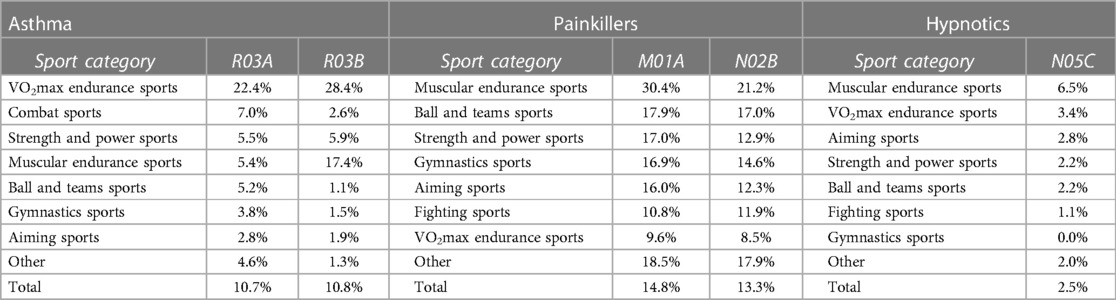
Table 3. Five of the most frequent ATC codes (level 3) per sport category. The numbers refer to proportion of the doping control forms containing information about ≥one of the respective ATC codes (R03A Adrenergics, inhalants (beta-2-agonists); R03B Other drugs for obstructive airway diseases, inhalants (not beta-2-agonists); M01A Anti-inflammatory and antirheumatic products, non-steroidal; N02B Other analgesics and antipyretics; N05C Hypnotics and sedatives).
Use of hypnotics ranges from 6.5% in the muscular endurance sport category to 0.0% in the gymnastic sport. The two sport disciplines ice hockey and alpine skiing differ from the other disciplines, were the proportion of DCFs with at least one hypnotic in ATC group N05C were 8.2% and 8.0%, respectively.
Ages, genders and type of test
A peak in the proportion of one or more pharmaceuticals appeared in the age group 25–29 for female national level athletes, with 83% of the DCFs including at least one pharmaceutical (Figure 3). Within the group of female recreational athletes, most pharmaceuticals were used in the group 30–34 years, with information of pharmaceuticals in 82% of the DCFs. For males, there were a slight increase in use of pharmaceuticals with age in both athlete level groups.
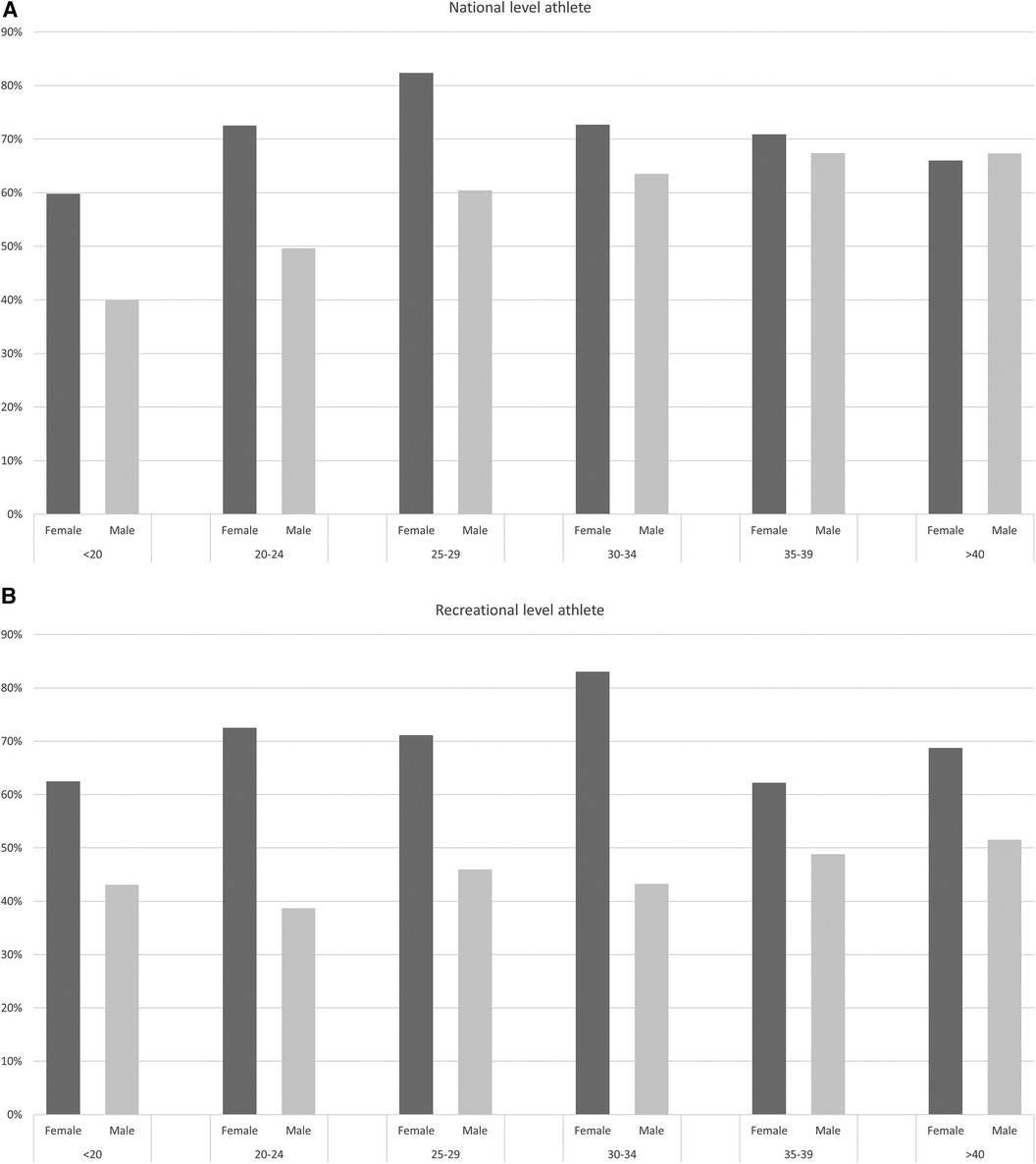
Figure 3. Proportion of doping control forms (DCFs) within age group and gender containing information about ≥one pharmaceutical for (A) national level athletes and (B) recreational level athletes, respectively.
For athletes in Ball and team sport, gymnastic sports, aiming sports and combat sports, there were no significant differences in the use of pharmaceuticals IC vs. OOC (Table 2). In contrast, athletes in VO2max endurance sports, Strength and Power sports and Muscular endurance sports used significantly more pharmaceuticals OOC vs. IC.
Discussion
The study examines the use of pharmaceuticals amongst recreational and national level athletes who participated in doping controls performed by ADNO in the period 2015–2019 as part of the national testing program in Norwegian sport. As the focus of this paper is to get a general overview of pharmaceutical usage based on doping control forms, a thorough comparison of the results with existing literature will not be done. Only some examples are given in the following discussion.
Differences in use of pharmaceuticals
The general trend in use of pharmaceuticals in the period was a slight increase, reflected by an increase in the portion of DCFs containing at least one pharmaceutical from 52.0% in 2015 to 58.4% in 2019. The trend is likely to reflect a general trend of increased use of pharmaceuticals in Norway in the period 2015–2019, even if the indicators are not directly comparable, i.e., number of DCFs vs. Defined Daily Dosages (DDD)) (35). The increasing trend in use of pharmaceuticals is also detected in sport in some reports (10, 36), while no significant increased trend was found in the football World Cups between 2002 and 2014 (21).
National level athletes tended to use a higher number of pharmaceuticals than recreational level athletes. As many NLA are professional athletes, they in most cases ten exercise more and harder than recreational athletes, thus, being more prone to extreme stress that can lead to injuries and other conditions that require pharmaceutical intervention, e.g., by painkillers or anti-asthmatics (8, 37, 38).
Pharmaceuticals were listed on a relatively high proportion of DCFs from female athletes compared to males. The difference in use of pharmaceuticals between men and women in the general population is well-known and reflected both in the national reports from the same period (35) and in the scientific literature (39–41). Differences in use of pharmaceuticals between men and women in sport is also reported (42, 43). The results from the present study are therefore in line with literature. Even if the ATC code G03A (i.e., hormonal contraceptives for systemic use) is excluded from the calculations, women report a higher mean number of pharmaceutical per DCF than men. A possible explanation is a more frequent doctor consultations amongst females, more seeking of preventive care, and differences in physicians' prescription of pharmaceuticals (44). Gender-related morbidity could also be a reason for the gender differences. For example, asthma incidence differs according to gender (45), as do use of pain killers (46). Since anti-asthmatics and pain killers are among the most frequently used pharmaceuticals in the present study, it could be one of the reasons why differences between gender were observed.
ATC codes
To our knowledge, no other mapping of pharmaceuticals in sport of comparable magnitude has used ATC codes as a classification system. However, the findings presented here are in line with other studies focusing on medication in sport, revealing high consumption of anti-asthmatics, NSAIDs and other pain killers and nasal preparations (8, 10, 13, 15, 42).
Anti-asthmatics (R03 A and R03 B) and pain killers (M01 A and N02 B) were the most reported pharmaceuticals in the present study. High prevalence of asthma medication is not very surprising, as strenuous aerobic exercise has the potential to induce asthma and thus the requirement of anti-asthmatics (47). This is particularly evident in sports which require constant physical exertion (e.g., triathlon, cycling, rowing), take place in cold weather (cross-country, biathlon, speed skating) or in environments with poor air quality (swimmers in chlorine swimming pools) (48). The same pattern appears in the presented data material, as the VO2max endurance sports tops the prevalence list of anti-asthmatics. The data suggests that there are some differences between sport types regarding the use of pharmaceutical IC vs. OOC. Interestingly, sports characterized by performances based on a few bio motor physiological skills rather technical and tactical skills, such as VO2max endurance sports, Strength and Power sports and Muscular endurance sports, report a higher degree of pharmaceutical drug use in training situations (OOC) compared to during competitions (IC). This should be investigated further.
The relative high prevalence of pain killers (NSAIDs, M01 A and paracetamol, N02 B) is comparable to what has been reported by other studies (15, 49). Nonsteroidal anti-inflammatory drugs are amongst others used by athletes to treat acute muscle- and tendon injuries and muscle soreness, which are typical conditions related to exercise and physical performance. It is therefore not surprising that these substances are used extensively in sports, although indicators of overuse exist (21, 50). One challenge is that these pharmaceuticals are often available as Over-The-Counter making it difficult for the athletés doctor to control what products and how much is used. Another aspect to consider is that NSAIDs cause deterioration in respiratory function in approximately 10% of adults with asthma (51). It does not appear that the inappropriateness of using NSAIDs for patients diagnosed with asthma is well-known amongst the athletes, as the use of NSAIDs in combination with anti-asthmatics from either ATC group R03A and/or R03B was detected in 9.1% of the DCFs reporting NSAIDs use.
Tramadol (N02 A X02) will be listed on the WADA Prohibited List from 1st of January 2024.The result from the present study suggest that tramadol use is limited, as only 24 of 10 418 DCFs (0.2%) contain information about the substance. It is thus no reason to suspect inappropriate use of this substance amongst Norwegian athletes, at least for the period of the data collection.
Among the most surprising findings in the present study were the relatively common use of hypnotics (reported by ice hockey players on 8.2% of all DCFs) and alpine skiers (8.0% of all DCFs). As these pharmaceuticals are potentially addictive, it is worrying that they are used regularly by relatively young, healthy athletes. In ice hockey, its prevalent use may be due to a tight match schedule, late matches, while extensive travelling across time zones throughout the year and consequently lack of sleep may be an explanation among alpine skiers. This should be examined more carefully in future studies. Use of hypnotics in sport in ATC class N05C is to the best of our knowledge not discussed in the literature. However, the use of benzodiazepines in sport is recently covered (52). These substances, found in ATC class N05B, were only mentioned on 0.3% on the DCFs in the present study.
The use of antibiotics does appear to be less common among Norwegian athletes compared to studies from other countries (8, 9, 22, 37). Only 1.0% of the DCFs contained information of use of the most common oral antibiotics (J01 C, penicillin). The use of antibiotics in Norway is well controlled, and the strategy of the Norwegian government is to be one of the three European countries that uses the least antibiotics in humans (53).
Information about pharmaceutical usage amongst the general population in Norway, as reported in the Norwegian Prescription Database (NorPD) (35) revealed that use of the corticosteroid asthmatics (R03B) was slightly increasing in Defined Daily Dose/Thousand Inhabitants per Day (DDD/TID) in the period 2015–2019, but the prevalence was steady. The adrenergic inhalants (R03A) had an increase of almost 10% in DDD/TID. The anti-inflammatory painkillers (M01A) were unchanged whereas other analgesics and antipyretics (N02B) were increasing by almost 20% in DDD/TID and 35% in number of individuals, indicating that in addition to more usage, people are getting more on prescriptions. It was practically no change in use of hypnotics (N05C) in the general population.
Strengths and limitations of the method
Using information about self-declared use of pharmaceuticals from DCFs is nothing new and has been used in several other studies (10, 54, 55). However, in the present study, the ATC system was used for classification of the pharmaceuticals. Few other studies have used the ATC system for classification of pharmaceuticals in sport (56), and none with comparable amount of data. By using ATC for classification, data for pharmaceuticals down to substance level (fifth level) or pharmacological or therapeutic subgroup (third level) the database will be a valuable source for information on specific substances or subgroups for e.g., anti-doping educators, sports physicians, and researchers.
The number of DCFs containing self-declared use of pharmaceuticals is the variable mainly used in this paper. A DCF with several pharmaceuticals could indicate anything from liberal use of pharmaceuticals to a period of health problems. Also, underreporting of the use of pharmaceuticals and supplements is a possible source of error in the data material. For many athletes, the doping control itself can be a stressful situation that leads to forgetfulness when, for example, it concerns which products they have used in the last seven days before the control. It is possible for the athlete to submit information about this to ADNO after the control. However, such post-registration of pharmaceuticals and supplement were not included in the present material, and there are no statistics on the extent to which this occurs. Another reason for underreporting may be that the athlete wants to hide the use of certain products. However, if it is related to prohibited substances, the use would be revealed in the urine sample anyway. The athlete therefore has everything to gain by being honest in the first instance. Another potential source of error is indistinct handwriting or misspelling of the products. With the paper based DCFs used during the study period, the handwriting of the athlete was crucial for the interpretation of the content. However, pharmacy students were doing the registration of the data, as they are skilled to interpret both pharmaceutical names and different handwritings. When in doubt, they discussed internally or with other members of the project group. Thus, the incorrect registration of the products as a source of error was then minimized.
Because of the fully anonymized database, DCFs from athletes being tested multiple times could not be merged. They often register the same pharmaceutical(s) on the DCFs of consecutive doping controls. Numbers and statistics in this paper refer to DCFs as a unit unless stated otherwise. As some athletes were tested more than once during the time-period, their data may disproportionally affect the mean values of the data material. This is particularly evident in sports with relative few athletes, where some athletes with a high use of prescription drugs and/or dietary supplements may affect the mean values of the sport/sport discipline.
Conclusion
The ATC classification system works well for the mapping of pharmaceuticals in the DCFs. Using the DCFs as a tool in the process of mapping and understanding the athletes' use of pharmaceuticals needs to be further developed. The data obtained from this study is expected to be useful for athletes and supporting personnel like physicians, physical therapists, and nutritionists as well as for sport federations. It also indicates some areas to be explored further and understood better, like the culture for use of pharmaceuticals in sports disciplines with seemingly high or unusual usage patterns.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical statement
The study was approved by Regional Committees for Medical Research Ethics, ID 29318. As the data from the Doping Control Forms were fully anonymized, there was no need for the athletes to give informed consent.
Author contributions
AG: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Software, Supervision, Writing – original draft. TH: Software, Writing – review & editing. A-LB: Software, Writing – review & editing. FL: Conceptualization, Investigation, Methodology, Software, Writing – review & editing. IB: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
The research was funded by an annual grant from the Norwegian Ministry of Culture and Equality to Anti-Doping Norway.
Acknowledgments
Thanks to Geir Holden for his contributions. Ellef and Ingrid Fange Gjelstad for the support in developing the matrices in Excel, leading to an easy task to classify the pharmaceuticals with their respective ATC codes.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. The 2023 Prohibited List. World Anti-Doping Agency. (2023). Available at: https://www.wada-ama.org/en/resources/world-anti-doping-program/2023-prohibited-list (Retrieved December 6, 2022).
2. The Norwegian Pharmaceutical Product Compendium. (2023). Available at: https://www.felleskatalogen.no/medisin
3. Lauritzen F. Dietary supplements as a major cause of anti-doping rule violations. Front Sports Act Living. (2022) 4:868228. doi: 10.3389/fspor.2022.868228
4. Thevis M, Kuuranne T, Fedoruk M, Geyer H. Sports drug testing and the athletes’ exposome. Drug Test Anal. (2021) 13(11–12):1814–21. doi: 10.1002/dta.3187
5. Timpka T, Fagher K, Bargoria V, Andersson C, Jacobsson J, Gauffin H, et al. Injury acknowledgement by reduction of sports load in world-leading athletics (track and field) athletes varies with their musculoskeletal health literacy and the socioeconomic environment. Br J Sports Med. (2023) 57:849–54. doi: 10.1136/bjsports-2022-106007
6. Vamos S, Steinmann A. Applying a health literacy lens to youth sport: a focus on doping prevention in Germany. Glob Health Promot. (2017) 26(1):95–9. doi: 10.1177/1757975916683380
7. ATC - Structure and principles. WHO collaborating centre for drug statistics methodology (2022). Available at: https://www.whocc.no/atc/structure_and_principles/ (Retrieved December 6, 2022).
8. Alaranta A, Alaranta H, Helenius I. Use of prescription drugs in athletes. Sports Med. (2008) 38(6):449–63. doi: 10.2165/00007256-200838060-00002
9. Ciocca M. Medication and supplement use by athletes. Clin Sports Med. (2005) 24(3):719–38, x–xi. doi: 10.1016/j.csm.2005.03.005
10. Thuyne WV, Delbeke FT. Declared use of medication in sports. Clin J Sport Med. (2008) 18(2):143–7. doi: 10.1097/JSM.0b013e318163f220
11. Pedrinelli A, Ejnisman L, Fagotti L, Dvorak J, Tscholl PM. Medications and nutritional supplements in athletes during the 2000, 2004, 2008, and 2012 FIFA futsal world cups. Biomed Res Int. (2015) 2015:870308. doi: 10.1155/2015/870308
12. Tscholl P, Alonso JM, Dollé G, Junge A, Dvorak J. The use of drugs and nutritional supplements in top-level track and field athletes. Am J Sports Med. (2010) 38(1):133–40. doi: 10.1177/0363546509344071
13. Tscholl P, Junge A, Dvorak J. The use of medication and nutritional supplements during FIFA world cups 2002 and 2006. Br J Sports Med. (2008) 42(9):725–30. doi: 10.1136/bjsm.2007.045187
14. Huang SH, Johnson K, Pipe AL. The use of dietary supplements and medications by Canadian athletes at the Atlanta and Sydney Olympic games. Clin J Sport Med. (2006) 16(1):27–33. doi: 10.1097/01.jsm.0000194766.35443.9c
15. Aavikko A, Helenius I, Vasankari T, Alaranta A. Physician-prescribed medication use by the finnish paralympic and olympic athletes. Clin J Sport Med. (2013) 23(6):478–82. doi: 10.1097/JSM.0b013e31829aef0f
16. Harnett J, Climstein M, Walsh J, Gifford J. The use of medications and dietary supplements by masters athletes—a review. Curr Nutr Rep. (2022) 11(2):253–62. doi: 10.1007/s13668-022-00398-0
17. Oester C, Weber A, Vaso M. Retrospective study of the use of medication and supplements during the 2018 FIFA world cup Russia. BMJ Open Sport Exerc Med. (2019) 5(1):e000609. doi: 10.1136/bmjsem-2019-000609
18. Vaso M, Weber A, Tscholl PM, Junge A, Dvorak J. Use and abuse of medication during 2014 FIFA world cup Brazil: a retrospective survey. BMJ Open. (2015) 5(9):e007608. doi: 10.1136/bmjopen-2015-007608
19. de Sire A, Marotta N, Lippi L, Scaturro D, Farì G, Liccardi A, et al. Pharmacological treatment for acute traumatic musculoskeletal pain in athletes. Medicina (Kaunas). (2021) 57:11. doi: 10.3390/medicina57111208
20. Melzer M, Elbe AM, Strahler K. Athletes’ use of analgesics is related to doping attitudes, competitive anxiety, and situational opportunity. Front Sports Act Living. (2022) 4:849117. doi: 10.3389/fspor.2022.849117
21. Tscholl PM, Vaso M, Weber A, Dvorak J. High prevalence of medication use in professional football tournaments including the world cups between 2002 and 2014: a narrative review with a focus on NSAIDs. Br J Sports Med. (2015) 49(9):580–2. doi: 10.1136/bjsports-2015-094784
22. Fayock K, Voltz M, Sandella B, Close J, Lunser M, Okon J. Antibiotic precautions in athletes. Sports Health. (2014) 6(4):321–5. doi: 10.1177/1941738113506553
23. Puccini V. Antibiotic therapy and athletes: is the mitochondrial dysfunction the real Achilles’ heel? Sports (Basel). (2022) 10:9. doi: 10.3390/sports10090131
24. Allen H, Price OJ, Hull JH, Backhouse SH. Asthma medication in athletes: a qualitative investigation of adherence, avoidance and misuse in competitive sport. J Asthma. (2022) 59(4):811–22. doi: 10.1080/02770903.2021.1881968
25. Dornquast C, Rotter G, Schollbach L, Binting S, Scherr J, Pfab F, et al. Allergic diseases in German competitive athletes: results of a cross-sectional study. J Sports Med Phys Fitness. (2022) 63(4):588–95. doi: 10.23736/s0022-4707.22.13825-9
26. Gałązka-Franta A, Jura-Szołtys E, Smółka W, Gawlik R. Upper respiratory tract diseases in athletes in different sports disciplines. J Hum Kinet. (2016) 53(1):99–106. doi: 10.1515/hukin-2016-0014
27. Kundu P. A medical sociological perspective of doping in sports. Int J Phys Educ Sports Sci. (2018) 13(3):32–7. doi: 10.29070/13/57122
28. Malcolm D. Concussion, chronic traumatic encephalopathy, and the medicalization of sport. In: Ventresca M, McDonald MG, editors. Sociocultural examinations of sports concussions. Taylor New York: Routledge (2019). p. 23–40.
29. Rebello LJ, Roberts AW, Fenuta AM, Cote AT, Bodner ME. Sleep quality and sleep behaviors in varsity athletes: a pilot study. Front Sports Act Living. (2022) 4:906663. doi: 10.3389/fspor.2022.906663
30. Taylor L, Chrismas BC, Dascombe B, Chamari K, Fowler PM. Sleep medication and athletic performance-the evidence for practitioners and future research directions. Front Physiol. (2016) 7:83. doi: 10.3389/fphys.2016.00083
31. International Pharmaceutical Federation (FIP). Sports pharmacy pratice and education: a global overview. The Hague: International Pharmaceutical Federation (2022). Available at: https://www.fip.org/file/5391
32. World Anti-Doping Code. World Anti-Doping Agency (WADA) (2021). Available at: https://www.wada-ama.org/en/resources/world-anti-doping-program/world-anti-doping-code (Retrieved September 23, 2022).
33. Lauritzen F, Holden G. Intelligence-based doping control planning improves testing effectiveness—perspectives from a national anti-doping organisation. Drug Test Anal. (2023) 15(5):506–15. doi: 10.1002/dta.3435
34. Lauritzen F, Gjelstad A. Trends in dietary supplement use among athletes selected for doping controls [Original Research]. Front Nutr. (2023) 10:1143187. doi: 10.3389/fnut.2023.1143187
35. The Norwegian Prescription Database. (2023). Available at: www.norpd.no
36. Kavukcu E, Burgazlı KM. Preventive health perspective in sports medicine: the trend at the use of medications and nutritional supplements during 5 years period between 2003 and 2008 in football. Balkan Med J. (2013) 30(1):74–9. doi: 10.5152/balkanmedj.2012.090
37. Ferry B, DeCastro A, Bragg S. Common prescription medications used in athletes. Prim Care. (2020) 47(1):49–64. doi: 10.1016/j.pop.2019.10.003
38. Thomas S, Wolfarth B, Wittmer C, Nowak D, Radon K. Self-reported asthma and allergies in top athletes compared to the general population—results of the German part of the GA2LEN-Olympic study 2008. Allergy Asthma Clin Immunol. (2010) 6(1):31. doi: 10.1186/1710-1492-6-31
39. Fernández-Liz E, Modamio P, Catalán A, Lastra CF, Rodríguez T, Mariño EL. Identifying how age and gender influence prescription drug use in a primary health care environment in Catalonia, Spain. Br J Clin Pharmacol. (2008) 65(3):407–17. doi: 10.1111/j.1365-2125.2007.03029.x
40. Orlando V, Mucherino S, Guarino I, Guerriero F, Trama U, Menditto E. Gender differences in medication use: a drug utilization study based on real world data. Int J Environ Res Public Health. (2020) 17:11. doi: 10.3390/ijerph17113926
41. Roe CM, McNamara AM, Motheral BR. Gender- and age-related prescription drug use patterns. Ann Pharmacother. (2002) 36(1):30–9. doi: 10.1345/aph.1A113
42. Alaranta A, Alaranta H, Heliövaara M, Alha P, Palmu P, Helenius I. Allergic rhinitis and pharmacological management in elite athletes. Med Sci Sports Exerc. (2005) 37(5):707–11. doi: 10.1249/01.Mss.0000162689.69517.60
43. Alaranta A, Alaranta H, Palmu P, Alha P, Pietilä K, Vaara MH, et al. Asthma medication in finnish olympic athletes: no signs of inhaled β2-agonist overuse. Med Sci Sports Exerc. (2004) 36(6):919–24. doi: 10.1249/01.Mss.0000128250.17793.47
44. Skoog J, Midlöv P, Borgquist L, Sundquist J, Halling A. Can gender difference in prescription drug use be explained by gender-related morbidity?: a study on a Swedish population during 2006. BMC Public Health. (2014) 14(1):329. doi: 10.1186/1471-2458-14-329
45. Zein JG, Erzurum SC. Asthma is different in women. Curr Allergy Asthma Rep. (2015) 15(6):28. doi: 10.1007/s11882-015-0528-y
46. Richardson J, Holdcroft A. Gender differences and pain medication. Womens Health (Lond). (2009) 5(1):79–90. doi: 10.2217/17455057.5.1.79
47. He T, Song T. Exercise-induced bronchoconstriction in elite athletes: a narrative review. Phys Sportsmed. (2022):1–9. doi: 10.1080/00913847.2022.2148137. [Epub ahead of print]
48. Fitch KD. An overview of asthma and airway hyper-responsiveness in Olympic athletes. Br J Sports Med. (2012) 46(6):413. doi: 10.1136/bjsports-2011-090814
49. Paoloni JA, Milne C, Orchard J, Hamilton B. Non-steroidal anti-inflammatory drugs in sports medicine: guidelines for practical but sensible use. Br J Sports Med. (2009) 43(11):863–5. doi: 10.1136/bjsm.2009.059980
50. Leyk D, Rüther T, Hartmann N, Vits E, Staudt M, Hoffmann MA. Analgesic use in sports: results of a systematic literature review. Dtsch Arztebl International. (2023) 120(10):155–61. doi: 10.3238/arztebl.m2023.0003
51. Levy S, Volans G. The use of analgesics in patients with asthma. Drug Saf. (2001) 24(11):829–41. doi: 10.2165/00002018-200124110-00004
52. Zandonai T, Peiró AM, Fusina F, Lugoboni F, Zamboni L. Benzodiazepines in sport, an underestimated problem: recommendations for sports medicine physicians’ practice. Front Psychiatry. (2022) 13:1066330. doi: 10.3389/fpsyt.2022.1066330
53. National Strategy against Antibiotic Resistance 2015–2020. (2015). Available at: https://www.who.int/publications/m/item/norway-national-strategy-against-antibiotic-resistance
54. Solheim SA, Nordsborg NB, Ritz C, Berget J, Kristensen AH, Mørkeberg J. Use of nutritional supplements by danish elite athletes and fitness customers. Scand J Med Sci Sports. (2017) 27(8):801–8. doi: 10.1111/sms.12704
55. Trinks S, Scheiff AB, Knipp M, Gotzmann A. Declaration of analgesics on doping control forms in German football leagues during five seasons. Deutsche Zeitschrift für Sportmedizin. (2021) 72(2):68–74. doi: 10.5960/dzsm.2020.474
Keywords: pharmaceuticals, sport, ATC system, doping control forms, anti-doping
Citation: Gjelstad A, Herlofsen TM, Bjerke A-L, Lauritzen F and Björnsdottir I (2023) Use of pharmaceuticals amongst athletes tested by Anti-Doping Norway in a five-year period. Front. Sports Act. Living 5:1260806. doi: 10.3389/fspor.2023.1260806
Received: 18 July 2023; Accepted: 22 September 2023;
Published: 4 October 2023.
Edited by:
Cornelia Blank, Private University for Health Sciences, Medical Informatics and Technology (UMIT), AustriaReviewed by:
Jakob Sehested Mørkeberg, Anti Doping Danmark (ADD), DenmarkThomas Zandonai, Miguel Hernández University of Elche, Spain
© 2023 Gjelstad, Herlofsen, Bjerke, Lauritzen and Björnsdottir. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Astrid Gjelstad YXN0cmlkZ2pAZmFybWFzaS51aW8ubm8=