 D. J. Oberlin
D. J. Oberlin- Department of Exercise Sciences and Recreation, City University of New York, Lehman College, Bronx, NY, United States
There are well known sex differences in parameters of physical fitness/performance due to changes occurring during sexual development. Thus, many sport and athletic events have regulations separating male and female participants. However, the inclusion or exclusion of transgender individuals in athletics has recently received outsized attention despite relatively few cases of transgender athletes. When determining which athletic gender category trans individuals should be permitted to compete in, it is important to understand the level of physical fitness/performance these individuals possess relative to their cisgender counterparts. Unfortunately, there are few studies investigating this topic, and several complications that confound this research. The current review seeks to discuss sex and gender as concepts, review sex differences in fitness/performance and how they develop, and then, consider how current evidence suggests that trans individuals compare to cis individuals. Finally, this review seeks to offer considerations for whether trans individuals should be excluded from sports and athletics, and how future research should proceed to better understand this marginalized population.
1. Introduction
While transgender individuals have likely always existed, they have recently received an outsized level of attention and scrutiny from governments and other regulatory bodies (1–5). This scrutiny spans multiple issues, one of which has been participation in sports and athletics (1, 2, 6, 7). Concerns have been raised for whether trans individuals should be allowed to compete in sports with cisgender individuals, suggesting they should not compete in the category that aligns with their gender identity or that they should participate in a separate category entirely (1, 3–6, 8–11). Addressing these concerns requires consideration of several concepts: sex and gender, how sports and athletics currently regulate participation by sex and gender, potential human right violations or discrimination coming from exclusionary approaches, what sex differences exist in athletics and how these develop and affect athletic performance, and whether trans individuals' participation in sports inherently leads to risks of either inequity or injury. This is not a systematic review, and makes no claim to “solve” this matter. The purpose of the current review is to better describe the modern landscape of how and why gender is used as criteria for inclusion/exclusion from sport and athletics, and to drive further considerations of how or whether transgender individuals should be excluded from these events. To achieve this, pubmed and google scholar were used to search for terms including: “trans”, “gender”, “transgender”, “sports”, “performance”, “exercise”, “athletics”. Articles were included if they met the following criteria: (1) original research rather than review, (2) research compared transgender individuals on gender affirming hormone therapy to cisgender individuals rather than comparing cis men and cis women, and (3) some measures of fitness or performance were measured. This was done to find articles that investigated transgender performance, accounting for hormonal differences, and comparing these with cisgender counterparts. Articles were excluded if no more than one trans individual was compared to cisgender individuals. These criteria were used for the following reasons. (1) Transgender individuals on gender affirming hormone therapy should not be equated to their pre-transition cisgender counter parts. Gender affirming hormone therapy can alter physiologic parameters (12–16). Thus, transgender individuals must be directly measured rather than assuming cisgender sex differences are analogous to cisgender and transgender differences. (2) To avoid assuming that a single transgender individual can be generalized to an entire population. While case studies can be informative, selecting an exceptional trans athlete or a sedentary trans individual and assuming they represent an entire community would likely lead to misleading conclusions.
2. Sex and gender
2.1. Distinguishing sex and gender
Before discussing gender as a criterion for sports participation, the concepts of sex and gender should be clearly understood. Although often used synonymously, sex and gender are two different terms used to describe related concepts. Sex is a biological concept having to do with chromosomes, genitalia, gonads, and hormones (17–19). While related to sex, gender has to do with behaviors, societal roles/expectations, and attributes which are valued or discouraged within a social group (19–21). These related concepts can be conflated, as biological sex and bodily appearance influences how members within a society interact with one another (20, 22). The various interactions among members of a community pressure individuals within the community to behave in a particular manner or display certain characteristics based on their perceived sex (20, 22). To a casual observer, the differences between sex and gender may seem trivial, however they address individual qualities which have wide variations even within what may be considered a single group. Thus, to further a discussion of transgender individuals in sport and athletics, the concepts of sex and gender must first be understood, although they may be impossible to entirely disentangle.
Prior to understanding chromosomes, sex was determined to be male or female based on the genitalia possessed by an individual and their secondary sex characteristics (23–25). However, by the early 20th century, scientists were beginning to understand that chromosomes shared between mother and father would determine something about the sex of the offspring, but it would still be decades before a greater understanding of the variety of possible outcomes could be better understood (26–29). Currently, chromosomes, gonads, hormones, and genitals (and to a lesser extent secondary sex characteristics) have all been used to describe the concept of biological sex in humans (18). While chromosomal varieties can certainly result in XY males and XX females, it is also possible for individuals to be born with sex chromosome aneuploidy leading to variations such as XXX, XXY, XYY, XXXX, XXYY, XXXY, XXXXY, or even XXXXX (30–34). Differences in sex chromosomes have also led to discoveries of sex chromosome dose effects leading to variations in gene regulation as well as in body size and other phenotypic differences (33, 34). Besides variations in chromosomes, there are other possible anatomical deviations from what is typically considered male or female, such as males with ambiguous external genitalia, a uterus, and fallopian tubes to females who also carry a Y chromosome, have ambiguous external genitalia, and possess both ovaries and testis (18, 35). Hormonal concentrations, particularly of testosterone, are also used to distinguish male from female (18, 36). Both males and females have some concentration of both testosterone and estrogen, and these concentrations vary among individuals (37–39). However, testosterone is frequently used as a marker to distinguish male from female as males have 15–20 × more testosterone than females (36–38, 40). Despite this, there are also wide variations within cisgender men and women which do not make them more or less male or female (36–38). Hence, even a biological concept of sex, whether based on chromosomes, anatomy, hormones, or other criteria, does not fit neatly into two rigid categories (17, 18).
Gender is a more complicated topic than biological sex, because gender, according to the World Health Organization, “refers to the characteristics of women, men, girls and boys that are socially constructed” (20–22). Due to being social constructs, the various characteristics and genders can change over time, and/or across various cultures (21, 22). Because of its societal nature, the treatment of individuals not adhering to gender norms have faced varying degrees of penalty depending upon the time period, geographic regions, and culture and politics (3, 21, 41). Attempting to review all permutations of all characteristics which are associated with gender is beyond the scope of this review. However, any individuals having characteristics, traits, or gender identities not aligned with the societal norms for their biological sex may be considered some degree of gender non-conforming and may be subjected to similar castigation as transgender individuals.
The term transgender is relatively modern and predated by terms such as transvestite or transsexual prior to the 20th century (42). However in the 1960s, the term transgenderism became more common as it was noted that sexuality was not necessarily related to being transgender (43). While transgender may not perfectly capture the range of possible gender identities, it expresses the idea of sex and gender being unaligned (17, 44). Thus, cisgender was coined to describe an individual whose sex and gender are the same (44). Discussion of cis and trans gender individuals, and their rights in society may seem to be a modern issue, however, these discussions date back, at least, to the 19th century (45). Historical studies from these times document individuals who may be considered transgender by modern understanding (45–47). Some historians and activists argue that examples of people assuming unconventional gender roles or breaking with gender norms have existed throughout history (46, 47). However, it is nearly impossible to determine the gender identities of historical figures, as these individuals likely had no concept of gender identity in the modern context; additionally, there were harsh consequences for those who deviated from societal gender norms at various points in history (45–47). Thus, the current review will only focus on modern issues of gender identity as they relate to participation in sports and athletics.
2.2. Sports and gender classifications
When discussing sex, gender, and participation in sports and athletics, the main point of contention seems to be who should or should not be allowed to participate. The International Olympic Charter states that “The practice of sport is a human right. Every individual must have the possibility of practicing sport, without discrimination of any kind…” (48). If taken on its face, this Olympic principle indicates that trans individuals should have no restrictions on access to sports and athletics, and that discrimination violates that human right. The International Olympic Committee follows this principle in their most recent framework on fairness, however leaves the final decision on inclusion of transgender individuals to the various international federations on the basis of fairness and safety (49). This departure from the IOC consensus meeting on sex reassignment and hyperandrogenism acknowledged that one set of regulations did not account for the variability in different sport and athletic requirements, thus international federations would be best placed to make final determinations (49–51). The IOC stressed the importance of an evidence-based approach to assessing under what circumstances trans individuals should be restricted from participation (49, 50). Many of the international federations do choose to restrict participation in their respective athletic events on the basis of either trans status or, based on the blood concentration of hormones for trans individuals (8, 11, 52). It is common for sport/athletic federations to cite certain scientific facts and studies to justify their provisions (8, 11, 52). However, while it is true that some average differences can be measured between cis and trans individuals, these can vary across different studies and different physiologic traits (15, 53–56). While the sport/athletic federations provisions focus on mean differences between cis and trans individuals, they tend to ignore differences amongst a cis only population that lead to advantages, disadvantages, or confer no advantage in athletics and sport performance (11, 38, 40, 57–59). The total number of cis individuals that are naturally advantaged or disadvantaged would likely exceed the total number of transgender individuals wishing to compete based on their low proportion of the total population (60). Hence, the exclusion of the transgender individuals from sports and athletics based solely on concerns of inequity or injury risk, may be a solution in search of a problem.
3. Physiologic sex differences and their effects on performance among cisgender individuals
To discuss differences in exercise and performance among cis and trans gender individuals, there must first be an understanding of biologic sex differences, and the concern over what traits are lost or retained following an individual's transition. These differences arise from a combination of developmental, morphological, and hormonal differences between males and females (61). Some of these differences occur as a result of growth and development in puberty, while others are a result of persistent endogenous hormone concentrations (62–66).
3.1. General differences from development through adulthood in cisgender individuals
Sex differences are not as pronounced among younger males and females but emerge among adult males and females (63–66). Prior to puberty, young males and females have similar aerobic capacity, strength, body composition, and overall athletic performance (63, 65, 66). However, studies do find slight advantages in anaerobic and strength performance, such as running and throwing, among young males compared to females, while young females have similarly slight advantages in flexibility (67, 68). It is uncertain to what extent this is a result of physiologic differences, rates of maturation, or sociologic differences, as young males are more likely to spend time engaged in physical activity compared to young females which may also lead to differences in performance (69, 70).
The magnitude of sex differences increases as individuals mature (65). Adolescent and adult males and females show average differences in aerobic capacity, body composition, and strength (61). These are interrelated but will be addressed individually. As children grow and move through puberty, both sexes have increases in body size, although to a greater extent among males, leading to greater male average mass and height (62, 71). During puberty, differences in body composition become apparent, with males having lower average body fat, and higher average muscle mass compared to age matched females (64, 72, 73). This difference in body composition leads to increasing strength and aerobic capacity to a greater extent among males than females (64, 74). Due to a greater proportion of lean mass to total body mass, males on average are able to produce greater force for their body size (75–77). This can lead to advantages in sports where strength and power are valued (56, 78). Despite average differences, it is worth noting that overlap exists between the normal upper and lower ranges of males and females (62). The differences in size and composition of the body do not only relate to strength and power, but also to aerobic focused athletics.
Prepubertal males and females have similar aerobic capacities relative to body mass (63, 79). However, post-pubertal males show greater aerobic capacity compared to females due to changes such as increased hemoglobin and leaner body composition (64, 73, 74, 80, 81). The average sex differences in body composition favors higher relative aerobic capacity among males whose greater muscle mass and lower fat mass allows for greater uptake of oxygen per kilogram of total body mass during physical activity (79, 82, 83). Additionally, males will surpass females in left ventricular end diastolic volume and ventricular wall thickness, allowing greater cardiac output at similar heart rates (84). This is aided by the greater average hematocrit/hemoglobin among males compared to females (85–87). From birth to the onset of puberty, hematocrit/hemoglobin values are generally similar, but during maturation, males have a greater increase in hematocrit/hemoglobin compared to age matched females, although there is still overlap in normal ranges between these groups (85, 87). The combination of greater proportion of lean mass, heart size, hemoglobin leading to greater aerobic capacity leads to generally faster race times in many aerobically focused events (88–91).
Despite these sex differences that develop during puberty, there are still large areas of overlap in performance, the degree of which is dependent upon the physical demands of the activity (56, 78, 92, 93). An example can be seen in Figure 1, showing the overlap in finish times of the San Francisco Marathon runners 12 years and older (94). The overlap in performance is due to variability in body sizes, individual training and preparation, genetics, proper diet and hydration status, and likely other variables. It is also worth noting that across the history of marathons, including the data from the San Francisco Marathon, fewer total women have participated (94). As more women become involved in sport and improve in training, the gap in performance may narrow further (95). However, males, on average, seem to enjoy an advantage in many athletic competitions, due largely to the effects of testosterone playing out during pubertal development and through adulthood (36, 56, 66).
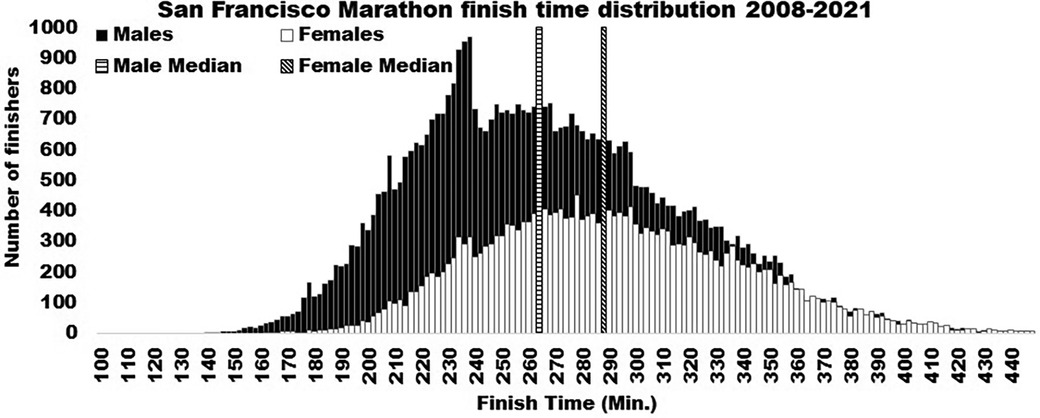
Figure 1. This figure shows the number of males and females finishing times for the San Francisco marathon from 2008 to 2021.
3.2. Hormonal differences in cisgender individuals from puberty and beyond
Many of the sex differences that become apparent during development are a result of hormonal differences that occur during puberty and persist beyond (66). In general, males will have higher testosterone concentrations than females, but lower estrogen concentrations relative to females (36, 37, 39, 96). However, the average difference in estrogen concentrations between males and females is less pronounced than the difference in testosterone (36, 37, 39, 96). Thus, it is important to understand how these different sex hormones contribute to physiologic factors associated with physical performance. Testosterone is known as an anabolic and androgenic hormone while estrogen is more commonly associated with soft tissue and bone health (36, 97, 98). Therefore, these will be discussed beyond the roles they play in development during puberty, to the characteristics they maintain in adults.
The effects of estrogen on performance have been studied predominantly in female athletes. How, or if, estrogen affects performance is not entirely understood due to changes in hormonal concentrations through the menstrual cycle, alterations of estrogen and progesterone resulting from oral contraceptive use, and changes in hormonal concentrations occurring around menopause (37, 99–101). Despite these limitations, several investigations have examined how performance may be influenced at different phases of the menstrual cycle (102, 103). While estrogen is associated with changes in cardiovascular function, respiratory function, thermoregulation, and substrate metabolism, the impact of the estrogen variations across the menstrual cycle have not shown consistent advantages or disadvantages in sports performance (92, 104). However, there are changes in estrogen before, during, and after athletic competitions in both males and females, thus future research may find that these changes are influencing performance (37, 96).
By contrast, testosterone, and its influence on athletic performance, has been intensely studied in both males and females. This is in part due to the abuse of testosterone, and/or closely related compounds, as ergogenic aids (105–107). The difference in testosterone concentration between sexes are wider than those seen with estrogen and are unlikely to overlap between sex groups with males having as much as 20 × the testosterone of females (36–38, 40). However, there is interindividual variation within sexes, with some males or females having as much as double the testosterone of their peers (36–38, 40). Despite the difference in hormone concentration between sexes, testosterone promotes muscle growth and strength in both males and females (106, 108–111). Even within a single group, such as cis men or cis women, serum testosterone concentrations seem to relate to enhanced muscle mass, strength, aerobic endurance, and possibly psychological advantages (108, 112–114). Although, the degree to which this influences performance is questionable and affected by the total difference in hormone concentrations and in sport specific demands (114–116). This issue can become contentious due to the variability in endogenous testosterone levels among athletes, even within a single cisgender category (113, 117). For example, there may be 2–3 × more or less testosterone within either elite male or female athletes and still be within normal ranges (59, 66). On the other hand, cis men with naturally occurring hyperandrogenism are not limited in their ability to compete while a cis woman with hyperandrogenism would be (118–120). This is despite the fact that this, as well as many other genetic/biologic factors, are beyond the control of the individual athletes (118, 121).
4. Cis and trans gender performance differences
Thus, there are clearly average differences in performance between males and females, despite an overlap in the average distribution (depending on the sport, age, and skill level). However, transgender individuals, particularly those who have undergone gender affirming hormone therapy and/or gender affirming surgical procedures, have physiologic and potentially morphologic differences from their pre-transition cisgender counterparts (16, 53, 54, 122). Therefore, it is not sufficient to examine sex differences among cis men and women and apply these directly to trans men and women, nor is it sufficient to examine pre to post transition without some cisgender comparisons. Unfortunately, there is a dearth of research on cis and trans gender differences. This lack of data are due to several factors: (1) trans individuals make up only 0.5% of the general population, and likely smaller proportion of highly trained athletes, making this population difficult to recruit and study, (2) highly trained individuals should not be compared to recreationally trained or untrained individuals and few highly trained trans individuals are able to be recruited within a single athletic discipline for a study (3) being trans does not necessitate gender affirming hormone therapy or surgeries, allowing various physiologic and morphologic possibilities amongst the trans community (50). Despite these limitations, attempts have been made to compare cis and trans gender individuals on many parameters of athletic performance, or proxies for these parameters (such as hand-grip strength) (12, 53–55, 122, 123).
In general, studies find that trans individuals, following gender affirming hormone therapy, become more similar to their gender identity (post-transition) cisgender counterparts, or are somewhere between the expected male and female averages (53–55, 122). Certain aspects of pre-transition-sex seem to be less malleable, such as total height and limb length (53, 122). However, there are changes in aerobic capacity, body composition, and muscular strength and endurance (12, 16, 53, 54, 122). Although these parameters may take months or years to complete this transition (12, 53, 54). The time to transition is relevant as (1) earlier in the process of transition, trans individuals may still retain traits more similar to their pre-transition gender, and (2) the effects of transitioning become confounded with the effects of aging and changes in training status (54, 55, 124–126). Due to all the potential pitfalls, a single definitive study of this topic is impossible, however, those which have been attempted can be used to glean better understanding of whether trans individuals' participation in sports and athletics is likely to lead to increased inequity or injury in sports and athletics.
Using a large sample among transgender exercise studies, Roberts et al. showed how the performance of both trans men and trans women on military physical fitness assessments changed over two years of gender affirming hormone therapy (54). Roberts et al. assessed number of push-ups and sit-ups performed as a field assessment of muscular strength and endurance (54). In addition, a 1.5-mile run was used as a field assessment of aerobic capacity (54). It was notable that neither trans men nor trans women aligned perfectly with their cisgender counterparts prior to gender affirming hormone therapy, with trans men performing more pushups and sit-ups (37.4 ± 2.03 and 50.4 ± 1.47) than cis women (32.6 ± 2.12 and 45.6 ± 1.51), and trans women performing fewer pushups than cis men (47.3 ± 1.34 vs. 53.5 ± 1.35) (54). Despite this, these groups were otherwise similar (54). Following two years of gender affirming hormone therapy, trans men showed no differences in pushups or 1.5 mile run time from cis men (56.1 ± 3.05 and 711 ± 34.91sec. vs. 51.5 ± 4.31 and 720 ± 35.71sec.), however they surpassed cis men for number of sit-ups performed (58.3 ± 2.20 vs. 52.4 ± 2.27) (54). For trans women following gender affirming hormone therapy, there were no differences in sit-ups or push-ups performed from cis women (44.8 ± 3.79 and 34.6 ± 4.21 vs. 45.7 ± 3.85 and 32.5 ± 4.31). However, post gender affirming hormone therapy, trans women still surpassed cis women for their 1.5 mile run time (765 ± 39.83 s. vs. 855 ± 40.56 s.), but performed significantly slower than cis men (720 ± 40.56 s.) unlike their pre hormone therapy assessment (54).
This study by Roberts et al. has also been used to support restricting trans individuals from participation in sport and athletic competitions (127, 128). As described above, following 2 years of gender affirming hormone therapy, trans women completed their 1.5 mile run slower than cis men, but still faster than cis women, raising potential concerns (54, 127). Fortunately, some of the original research team from the Roberts et al. study continued to follow-up for four years (129). However, the new analysis did not necessarily use the same participants as Roberts et al., having higher sample sizes for earlier years and lower sample sizes as they moved to year four. The follow-up study by Chiccarelli et al. noted that equivalence testing [the Two One-Sided Test (TOST)] should be used in addition to standard hypothesis testing to compare transgender individuals with their cisgender counterparts. The study also made comparisons of trans individuals' own pre-transition and post-transition performance as percentiles for men or women (129). Using these approaches, the researchers showed that trans women performance on the 1.5 mile run was not statistically different from cis women times following two years of gender affirming hormone therapy and remained equivalent to cis women out to year four (874 ± 133 s vs. 876 ± 111 s.) (129). Furthermore, the TOST analysis showed that the trans womens' female percentile scores were equivalent to their pre-transition male percentile scores (129). These findings are similar to a study by Harper et al. which showed similar age adjusted running scores pre and post transition (55). However, Chiccarelli et al. they did find that the pushup test for trans women did not decline enough to be equivalent to their pre-transition percentile ranking, and the number of push-ups performed were still greater than those performed by cis women (35.3 ± 7 vs. 30 ± 10) (129). Trans men also continually performed more like cis men and significantly better than cis women over the four years, and it is worth noting that by year four of follow-up, trans men were out performing cis men on both pushups and sit-ups (129). Based on these data, trans men and trans women continually performed more similarly to their affirmed cisgender performance averages, and approach their own pre-transition percentile scores over the four years of gender affirming hormone therapy (129). Although these findings seem to indicate that trans individuals may eventually reach equivalence with their cisgender counterparts, it should also be noted that the participant pool diminished over the four years of follow-up, increasing the risk of self-selection bias and increasing risk of potential error (14, 129).
A study by Jenkins et al. were able to account for more granular fitness parameters among trans women than those used by Roberts et al. and Chiccarelli et al., however this came at the cost of a small total sample of trans women of various ages and physical activity levels (53). To best account for these differences, trans individuals were matched with cis men and women of matched age and activity levels. All the trans women had been using gender affirming hormone therapy for at least two years allowing the researchers to compare many of their fitness attributes to cis men and women. Trans women indeed retained body mass and height significantly greater than cis women, and similar to cis men (53). However, their body composition (25.17 ± 8.57% body fat) was between that of cis men (17.12 ± 5.22%) and cis women (32.98 ± 9.06%), and not statistically different from either (53). Trans women were also shown to have higher grip-strength than cis women (93.0 ± 14.0 kg vs. 63.9 ± 9.5 kg) with no difference from cis men (112.7 ± 23.2 kg) (35). These findings do align with other studies that find strength and muscle mass do not adapt as quickly to gender affirming hormone therapy as cardiorespiratory parameters (14, 16, 54, 127, 129). However, on more performance related tests of: vertical jump height, pushups, and maximal aerobic capacity, trans women performed similarly to, or less than, cis women (33.98 ± 4.34 cm, 17.83 ± 5.46, and 29.43 ± 9.41 ml/kg/min compared to 34.24 ± 7.84 cm, 19.67 ± 11.64, and 30.43 ± 9.15 ml/kg/min), and significantly less than cis men (47.34 ± 6.43 cm, 48.0 ± 5.37, and 41.15 ± 13.77 ml/kg/min) (53). With such a small sample, this should not be overly interpreted, although it does seem to align with findings from Roberts et al. and Chiccarelli et al.
A slightly larger study by Alvares et al. also examined body compositional differences between cis men and women, and trans women (12). The study by Alvares et al., unlike data from Jenkins et al., showed a significantly higher percent body fat among trans women compared to cis men (29.5 ± 1.47% vs. 20.2 ± 1.52%), with no differences between trans women and cis women (32.9 ± 1.58) (12). Despite no differences in percent body fat, trans women still showed greater lean mass than cis women (30.7 ± 0.85 kg lean mass vs. 21.9 ± 0.67 kg lean mass) (12). Unlike the study by Jenkins et al., Alvares et al. measured a much smaller difference in grip strength between cis women and trans women (29.7 ± 1.0 kg vs. 35.2 ± 1.39 kg), with both being significantly lower than cis men (48.4 ± 1.79 kg) (12). Both studies seem to agree that relative aerobic capacity of trans women is decreased to levels similar to those of cis women (33.5 ± 1.21 ml/kg/min vs. 35.7 ± 1.30 ml/kg/min (12, 53). Alvares goes further and quantifies hemoglobin levels showing that trans women have similar hemoglobin to cis women (14.0 ± 0.15 g/dl vs. 13.8 ± 0.17 g/dl) and less than cis men (15.3 ± 0.29 g/dl) (12). These same findings for hemoglobin changes have been shown in other gender affirming hormone therapy treatments, and the subsequent changes in running performance are even shown among trans athletes (13, 55, 130).
Unfortunately, few studies are able to examine trans athletes due to the small population. A study by Harper et al. examined runners' race times across transition from men to women to determine how transitioning affected their performance (55). The study followed nine athletes over an average of 7 ± 1.9 years of transition (range of years of transition = 1–29). Harper found that there was a decrease in performance measured by race times (55). To account for the aging effect on running performance, Harper et al. used age grading, comparing run times to a standard run time accounting for race distance and sex. The age grades were on average, unchanged following transition (68.7% vs. 68.5%), suggesting that athletes as trans women did not enjoy an advantage compared to their pre-transition abilities. In other words, as trans women, they were performing at a similar competitive level, compared to other cis women, as they had as cis men compared to other cis men (55).
While data are still scarce, the limited information available does not suggest that trans men and trans women have much, if any, athletic advantage post-transition. Indeed, in most cases they perform more similarly to those matching their gender identity, or somewhere between cis men and women (12, 15, 53–55). If these individuals are performing somewhere between cis men and women on some performance parameters, does it pose a meaningful risk of inequity in sport or risk of athletic injuries, or are concerns for these problems misplacing blame to cover discrimination?.
5. Misplacing blame
As reviewed above, there are in fact sex differences on average performance values between males and females. However, too often, these differences are used as evidence to restrict trans individuals from sports and athletics (11, 52). The average differences observed between males and females are cited as problems leading to inequality and elevated risk in sports and athletics despite evidence that trans individuals do not match their pre-transition cisgender counterparts (11, 131). However, if these average differences lead to inequity or injury, restricting trans individuals from these sports and athletics may not be the best solution. This can be approached similar to a public health issue, assessing what important factors influence outcomes, and what effect would come from altering individual factors (i.e., the population attributable risk). For example, Transgender Guidelines by World Rugby state concern for the larger average mass of males relative to females, and how this influences the force of impact (i.e.,: mass × acceleration) (11). However, when looking at a sample distribution of players, >300 males sampled fall below the 2nd percentile of average male body mass and >300 females sampled are above the 98th percentile of average female body mass (11). If being too large or too small were a critical concern for rugby injuries, more injuries may be prevented by restricting those >600 players who fell far outside the average player mass than banning trans athletes. If average body mass values and their standard deviations for elite rugby players were used to generate a normal distribution of mass, there would still be areas of overlap among females and males. This can be seen in Figure 2 in which distributions were calculated from data reported by Ramos-Álvarez et al. using the following equation: (57). Injury in sport is a serious problem, however a ban on trans individuals does not solve this problem because there is already normal variation among cisgender individuals (53, 54). Using average pre-transition body sizes reported by Roberts et al., an estimation of the body mass distributions among cis and transgender men and women were estimated (assuming a normal distribution) showing large areas of overlap, even before gender affirming hormone therapy, as shown in Figure 3 (54). Perhaps in this case, if injuries are a primary concern, rugby should have weight classes similar to other sports where body mass is an important parameter rather than a ban on trans athletes.
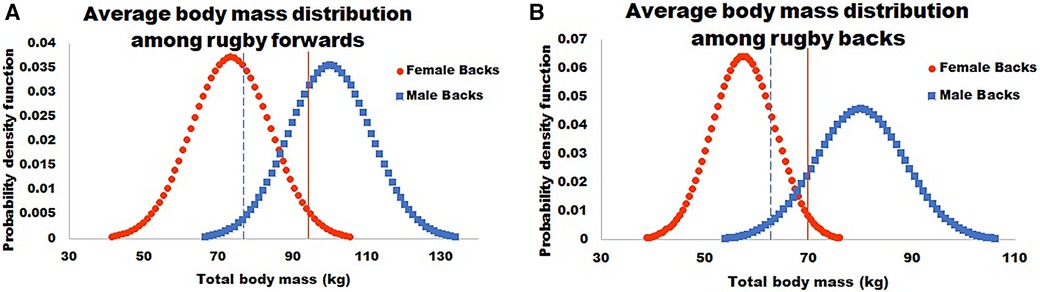
Figure 2. This figure shows the average body mass distribution among male (squares) and female (circles) rugby players. It also notes 2 standard deviations to the high end for females (solid line) and to the low end for males (dashed line). Data calculated based on values reported in Ramos-Álvarez et al. 2021 (12).
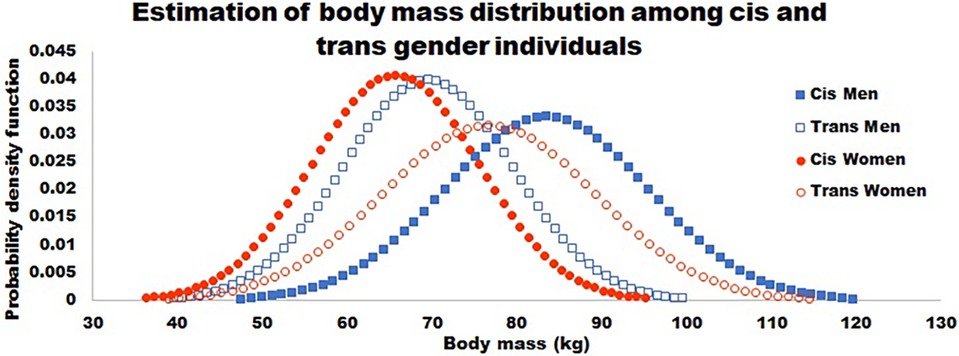
Figure 3. This figure shows an estimation of body mass distributions before gender affirming hormone therapy based on values reported by Roberts et al. 2020. Men and women are shown in squares and circles respectively, with cis and trans being denoted by closed or open symbols. As Roberts showed, there are not differences between the cisgender individuals and those who transitioned from that gender. However, there are large areas over overlap estimated among these populations even before gender affirming treatments.
Another example of misplaced blame would be concerns that trans women have too much testosterone or that trans men are gaining an unfairly advantage by taking testosterone (8, 11, 56, 127). Herein lies the myth that cis men, not on gender affirming hormone therapy, will claim to be a trans women to win at female sporting events. However, trans individuals use gender affirming hormone therapy to better match their gender identity, not to gain unfair sporting advantages (132). While it is true that certain morphological changes that occur during puberty may be irreversible, trans individuals on gender affirming hormone therapy clearly do not retain the same physiologic parameters as their pre-transition counterparts (12, 15, 16, 54–56, 129). It is unclear to what extent, or for how long, any hormone mediated advantages may persist once a trans individual begins regular gender affirming hormone therapy (12, 15, 53, 56, 129). It has been shown that parameters affecting aerobic performance transition more quickly than those affecting strength performance (16, 127, 129). However, excluding trans individuals does not prevent cases of athletes having hormonal advantages. The World Anti-Doping Agency (WADA) found 93 of the 4,422 athletes tested (2.1%) to have “adverse analytical finding” for steroid use (105). WADA does not report how many of those athletes were cis or trans, however, as transgender individuals are underrepresented in athletics, it is likely that these are cis athletes (60). Besides use of exogenous hormones, cisgender individuals naturally vary in their hormonal profiles (40, 59, 66, 133). Thus, restricting trans individuals is unlikely to prevent issues of ergogenic hormonal advantages in sports.
Finally, it is well known that within sports and athletics, competitive advantage is in large part influenced by genetic predisposition (121, 134, 135). It is accepted that some individuals are born with natural advantages, however, the suggestion that trans individuals may enjoy some advantage in certain cases is regarded as unacceptable. Yet there does not seem to be a domination of sports by trans athletes if their advantage is so great. When examining issues that allegedly arise by trans athletes' participation in sports and athletics, the solutions are more driven by a political/cultural divide rather than an honest attempt to actually mitigate inequities or risk of injuries that are occurring (1, 136).
6. Limitations and future directions
There are several limitations and future directions in this topic area. Many others have also noted that there is a need to study individuals who are both trans and elite athletes. Currently, the limited knowledge of athletic performance among trans men and women are limited to individuals who are either moderately active, recreationally trained, or military trained individuals (53–55, 129). Due to trans individuals making up such a small proportion of the total population, and their disproportionate rates of discrimination, recruitment of highly trained trans individuals is one of the greatest difficulties in this area of research (2, 7). In addition to difficulty in recruitment, the performance difference between males and females across different sports are not uniform (56, 92, 137). Individual components of fitness or task proficiency do not always translate to sport and athletic performance. Thus, fitness assessments do not account for training and skill at sports/athletics which may influence success as much as physiologic potential. Finally, there is the problem of neither sex nor gender being true binaries. This makes it nearly impossible to make comparisons among these individuals when classified into superimposed categories. As an example, even individuals who are cisgender, may have differences in sexual development, or have sexual aneuploidy, but would be simply classified based on their gender identity unless they were outed. Trans individuals, on the other hand, may have had various surgical procedures or take different gender affirming hormone therapy to better match assumed sex standards. All of these factors would need to be accounted for to truly understand what extent these individuals vary in sport and athletic performance. Future studies will be essential to gain a more comprehensive understanding of this population, and conclude whether and to what extent sex differences are retained post-transition.
7. Conclusion
Individuals should not have to make a choice between being their authentic selves or being athletes (138). While trans athletes competing in various sports and athletic events raises interesting considerations of how certain morphologic and physiologic factors affect performance, these questions are not exclusive to trans individuals. There are wide variations within cisgender populations, even when excluding individuals with differences in sexual development (121, 139). It is expected that about 2.3% of a normally distributed population is likely to fall above two standard deviations from a population mean. These exceptional individuals may be those who are gifted and excel at some sport or athletic performance (121, 135, 140). In contrast only 0.5%–0.6% of the population identify as trans (60). There is no concern for restricting individuals who are exceptionally large or small, those who are genetically gifted, or those with differing hormone concentrations or muscle mass, so long as their gender and biologic sex align (120, 121). The disproportionate focus on the relatively small portion of the population who are trans seems based on the belief that cis men, who cannot succeed in sports among other cis men, would choose to misidentify as trans women to gain an advantage in sports against cis women. However, there are no legitimate cases of this occurring. An individual's sex does not determine their success or failure at any athletic event despite the high level of competition. This can be demonstrated when looking at not average outcomes, but the level of overlap among outcomes. The exclusion of trans individuals also insults the skill and athleticism of both cis and trans athletes. While sex differences do develop following puberty, many of the sex differences are reduced, if not erased, over time by gender affirming hormone therapy. Finally, if it is found that trans individuals have advantages in certain athletic events or sports; in those cases, there will still be a question of whether this should be considered unfair, or accepted as another instance of naturally occurring variability seen in athletes already participating in these events.
Author contributions
DO performed the research and writing for this work.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sharrow EA. Sports, transgender rights and the bodily politics of cisgender supremacy. Laws. (2021) 10(3):63. doi: 10.3390/laws10030063
3. Rad MS, Shackleford C, Lee KA, Jassin K, Ginges J. Folk theories of gender and anti-transgender attitudes: gender differences and policy preferences. PLOS ONE. (2020) 14(12):e0226967. doi: 10.1371/journal.pone.0226967
4. Krishnakumar P. This record-breaking year for anti-transgender legislation would affect minors the most, in CNN Politics. 2021.
5. Nakajima K. Bills targeting trans youth are growing more common — and radically reshaping lives. In: Jin CH, editors. NPR. Washington DC: National Public Radio, Inc. (2022).
6. West-Sell SA, Van Ness JM, Ciccolella ME. Law, policy, and physiology as determinants of fairness for transgender athletes. Prof Exerc Physiol. (2019) 22(2):1–10. https://www.asep.org/index.php/download_file/view/1231/178/
7. James SE, Herman JL, Rankin S, Keisling M, Mottet L, Anafi M. 2015 U.S. Transgender Survey. 2016, National Center for Transgender Equality: Washington, DC.
8. World Athletics. World Athletics Eligibility Regulations for Transgender Athletes. 2023, World Athletics: The Principality of Monaco.
9. Alfonseca K. Young transgender athletes grappling with anti-trans sports legislation, in ABC News. 2021.
10. Natanson H. Va. Bill would bar trans student-athletes from teams matching gender identities. In: Vozzella L, editors. The Washington Post. Washington, D.C.: Washington Post Company's new media subsidiary, Washington post. Newsweek Interactive (2022). Available from: https://www.washingtonpost.com/dc-md-va/2022/11/15/virginia-bill-transgender-athletes-gender-identity/
12. Alvares LAM, Santos MR, Souza FR, Santos LM, de Mendonça BB, Frade Costa EM, et al. Cardiopulmonary capacity and muscle strength in transgender women on long-term gender-affirming hormone therapy: a cross-sectional study. Br J Sports Med. (2022) 56(22):1292–8. doi: 10.1136/bjsports-2021-105400
13. Antun A, Zhang Q, Bhasin S, Bradlyn A, Dana Flanders W, Getahun D, et al. Longitudinal changes in hematologic parameters among transgender people receiving hormone therapy. J Endocr Soc. (2020) 4(11):1–11. doi: 10.1210/jendso/bvaa119
14. Cheung AS, Zwickl S, Miller K, Nolan BJ, Wong AFQ, Jones P, et al. The impact of gender affirming hormone therapy on physical performance. J Clin Endocrinol Metab. (2023):dgad414. doi: 10.1210/clinem/dgad414. [Epub ahead of print]37437247
15. Harper J, O'Donnell E, Khorashad BS, McDermott H, Witcomb GL. How does hormone transition in transgender women change body composition, muscle strength and haemoglobin? Systematic review with a focus on the implications for sport participation. Br J Sports Med. (2021) 55(15):865–72. doi: 10.1136/bjsports-2020-103106
16. Wiik A, Lundberg TR, Rullman E, Andersson DP, Holmberg M, Mandić M, et al. Muscle strength, size, and composition following 12 months of gender-affirming treatment in transgender individuals. J Clin Endocrinol Metab. (2020) 105(3):e805–13. doi: 10.1210/clinem/dgz247
17. Karkazis K. The misuses of “biological sex”. Lancet. (2019) 394(10212):1898–9. doi: 10.1016/S0140-6736(19)32764-3
19. Mauvais-Jarvis F, Merz NB, Barnes PJ, Brinton RD, Carrero J-J, DeMeo DL, et al. Sex and gender: modifiers of health, disease, and medicine. Lancet. (2020) 396(10250):565–82. doi: 10.1016/S0140-6736(20)31561-0
20. 5050, G.H. Glossary. 2022 2023; Available at: https://globalhealth5050.org/glossary/
21. Shannon G, Jansen M, Williams K, Cáceres C, Motta A, Odhiambo A, et al. Gender equality in science, medicine, and global health: where are we at and why does it matter? Lancet. (2019) 393(10171):560–9. doi: 10.1016/S0140-6736(18)33135-0
22. World Health Organization, A.K. Gender and health. 2023; Available at: https://www.who.int/health-topics/gender#tab = tab_1 (Cited February 6, 2023).
24. Havelock E. Man and woman a study of human secondary and tertiary sexual characters. 8th ed., rev. London: W. Heinemann ltd (1934). 469.
25. Kellogg JH. Plain facts about sexual life. 1877, Battle Creek, Michigan: Office of the Health reformer. 356.
26. Pike FH. A critical and statistical study of the determination of sex, particularly in human offspring. Am Nat. (1907) 41(485):303–22. doi: 10.1086/278772
27. Hance RT. The determination of sex. Sci Mon. (1927) 24(1):25–30. https://www.jstor.org/stable/7794
28. Crow EW, Crow JF. 100 Years ago: walter sutton and the chromosome theory of heredity. Genetics. (2002) 160(1):1–4. doi: 10.1093/genetics/160.1.1
29. McClung CE. The accessory chromosome—sex determinant? Biol Bull. (1902) 3(1–2):43–84. doi: 10.2307/1535527
30. Jacobs PA, Baikie AG, Court Brown WM, Macgregor TN, Maclean N, Harnden DG Evidence for the existence of the human “super female”. Obstet Gynecol Surv. (1960) 15(3):440. doi: 10.1097/00006254-196006000-00052
31. Ford CE, Jones KW, Polani PE, De Almeida JC, Briggs JH. A sex-chromosome anomaly in a case of gonadal dysgenesis (Turner's syndrome). 1959.
32. Jacobs PA, Strong JA. A case of human intersexuality having a possible XXY sex-determining mechanism. Nature. (1959) 183:302–3. doi: 10.1038/183302a0
33. Raznahan A, Parikshak NN, Chandran V, Blumenthal JD, Clasen LS, Alexander-Bloch AF, et al. Sex-chromosome dosage effects on gene expression in humans. Proc Natl Acad Sci USA. (2018) 115(28):7398–403. doi: 10.1073/pnas.1802889115
34. Ottesen AM, Aksglaede L, Garn I, Tartaglia N, Tassone F, Gravholt CH, et al. Increased number of sex chromosomes affects height in a nonlinear fashion: a study of 305 patients with sex chromosome aneuploidy. Am J Med Genet Part A. (2010) 152(5):1206–12. doi: 10.1002/ajmg.a.33334
35. Sherwani AY, Shah AQ, Wani AM, Bashir AC, Bashir AK, Sofi FA, et al. Hysterectomy in a male? A rare case report. Int J Surg Case Rep. (2014) 5(12):1285–7. doi: 10.1016/j.ijscr.2014.10.020
36. Clark RV, Wald JA, Swerdloff RS, Wang C, Wu FCW, Bowers LD, et al. Large divergence in testosterone concentrations between men and women: frame of reference for elite athletes in sex-specific competition in sports, a narrative review. Clin Endocrinol (Oxf). (2019) 90(1):15–22. doi: 10.1111/cen.13840
37. Ginsburg GS, O'Toole M, Rimm E, Douglas PS, Rifai N. Gender differences in exercise-induced changes in sex hormone levels and lipid peroxidation in athletes participating in the Hawaii ironman triathlon: ginsburg-gender and exercise-induced lipid peroxidation. Clin Chim Acta. (2001) 305(1):131–9. doi: 10.1016/S0009-8981(00)00427-7
38. Crewther BT, Cook CJ. A longitudinal analysis of salivary testosterone concentrations and competitiveness in elite and non-elite women athletes. Physiol Behav. (2018) 188:157–61. doi: 10.1016/j.physbeh.2018.02.012
39. Ho KY, Evans WS, Blizzard RM, Veldhuis JD, Merriam GR, Samojlik E, et al. Effects of sex and age on the 24-hour profile of growth hormone secretion in man: importance of endogenous estradiol concentrations. J Clin Endocrinol Metab. (1987) 64(1):51–8. doi: 10.1210/jcem-64-1-51
40. Cook CJ, Beaven CM. Salivary testosterone is related to self-selected training load in elite female athletes. Physiol Behav. (2013) 116–117:8–12. doi: 10.1016/j.physbeh.2013.03.013
41. Castro-Peraza ME, García-Acosta JM, Delgado N, Perdomo-Hernández AM, Sosa-Alvarez MI, Llabrés-Solé R, et al. Gender identity: the human right of depathologization. Int J Environ Res Public Health. (2019) 16(6):978. doi: 10.3390/ijerph16060978
42. S O. Transgenderism: facts and fictions. Indian J Psychiatry. (2009) 51(1):73–5. doi: 10.4103/0019-5545.44917
43. Oliven JF. Sexual hygiene and pathology: A manual for the physician and the professions. 2nd edn. Lippincott (1965). 621 p.
44. Aultman B. Cisgender. TSQ: Transgender Stud Q. (2014) 1(1–2):61–2. doi: 10.1215/23289252-2399614
45. Beemyn G. A presence in the past: a transgender historiography. J Women’s Hist. (2013) 25(4):113–21. doi: 10.1353/jowh.2013.0062
46. Reis E. Teaching transgender history, identity, and politics. Radic Hist Rev. (2004) 88(1):166–77. doi: 10.1215/01636545-2004-88-166
47. DeVun L, Tortorici Z. Trans, time, and history. Transgender Stud Q. (2018) 5(4):518–39. doi: 10.1215/23289252-7090003
48. Committee IO. Olympic Charter. Lausanne, Switzerland: International Olympic Committee (2021). 112.
49. Committee IO. IOC Framework on Fairness, Inclusion and Non-Discrimination on the Basis of Gender Identity and Sex Variations 2021. p. 6.
50. Martowicz M, Budgett R, Pape M, Mascagni K, Engebretsen L, Dienstbach-Wech L, et al. Position statement: IOC framework on fairness, inclusion and non-discrimination on the basis of gender identity and sex variations. Br J Sports Med. (2023) 57(1):26. doi: 10.1136/bjsports-2022-106386
51. International Olympic Committee. IOC Consensus meeting on sex reassignment and hyperandrogenism. Lausanne, Switzerland: International Olympic Committee (2015). 015–1.
52. World Aquatics. Policy on eligibility for the men’s and women’s competiton categories. Lausanne, Switzerland: Fédération internationale de natation (FINA) (2022).
53. Jenkins CL, Ouellette K, Thompson B, Mullin EM, Leinung M. Performance in transgender females versus cisgender males and females. J Exerc Physiol Online. (2020) 23(6):62–76. https://www.asep.org/asep/asep/JEPonlineDECEMBER2020_Christine%20Jenkins.pdf
54. Roberts TA, Smalley J, Ahrendt D. Effect of gender affirming hormones on athletic performance in transwomen and transmen: implications for sporting organisations and legislators. Br J Sports Med. (2020) 55(11):577–83. doi: 10.1136/bjsports-2020-102329
55. Harper J. Race times for transgender athletes. J Sport Cult Identities. (2015) 6(1):1–9. doi: 10.18848/2381-6678/CGP/v06i01/54079
56. Hilton EN, Lundberg TR. Transgender Women in The Female Category of Sport: Is the Male Performance Advantage Removed by Testosterone Suppression? 2020: Preprints.
57. Ramos-Álvarez JJ, Montoya JJ, Solís-Mencia C, Miguel-Tobal F, López-Tapia P, Sánchez-Oliver AJ, et al. Anthropometric profile assessed by bioimpedance and anthropometry measures of male and female rugby players competing in the spanish national league. Appl Sci. (2021) 11(24):11759. doi: 10.3390/app112411759
58. Rønnestad BR, Nygaard H, Raastad T. Physiological elevation of endogenous hormones results in superior strength training adaptation. Eur J Appl Physiol. (2011) 111(9):2249–59. doi: 10.1007/s00421-011-1860-0
59. Balthazar CH, Garcia MC, Spadari-Bratfisch RC. Salivary concentrations of cortisol and testosterone and prediction of performance in a professional triathlon competition. Stress. (2012) 15(5):495–502. doi: 10.3109/10253890.2011.642033
60. Herman JLF, Andrew R, O'Neill KK. How Many Adults and youth Identify as Transgender in the United States? 2022, Williams Institute, UCLA School of Law.
61. Ansdell P, Thomas K, Hicks KM, Hunter SK, Howatson G, Goodall S. Physiological sex differences affect the integrative response to exercise: acute and chronic implications. Exp Physiol. (2020) 105(12):2007–21. doi: 10.1113/EP088548
62. Kuczmarski RJ. CDC growth charts for the United States: Methods and development. 2002, National Center for Health Statistics (2000).
63. Winsley RJ, Fulford J, Roberts AC, Welsman JR, Armstrong N. Sex difference in peak oxygen uptake in prepubertal children. J Sci Med Sport. (2009) 12(6):647–51. doi: 10.1016/j.jsams.2008.05.006
64. Wells JC. Sexual dimorphism of body composition. Best Pract Res Clin Endocrinol Metabo. (2007) 21(3):415–30. doi: 10.1016/j.beem.2007.04.007
65. Handelsman DJ. Sex differences in athletic performance emerge coinciding with the onset of male puberty. Clin Endocrinol (Oxf). (2017) 87(1):68–72. doi: 10.1111/cen.13350
66. Handelsman DJ, Hirschberg AL, Bermon S. Circulating testosterone as the hormonal basis of sex differences in athletic performance. Endocr Rev. (2018) 39(5):803–29. doi: 10.1210/er.2018-00020
67. Marta CC, Marinho DA, Barbosa TM, Izquierdo M, Marques MC. Physical fitness differences between prepubescent boys and girls. J Strength Cond Res. (2012) 26(7):1756–66. doi: 10.1519/JSC.0b013e31825bb4aa
68. Luz LGO, Cumming SP, Duarte JP, Valente-dos-Santos J, Almeida MJ, Machado-Rodrigues A, et al. Independent and combined effects of sex and biological maturation on motor coordination and performance in prepubertal children. Percept Mot Skills. (2016) 122(2):610–35. doi: 10.1177/0031512516637733
69. Trost SG, Pate RR, Sallis JF, Freedson PS, Taylor WC, Dowda M, et al. Age and gender differences in objectively measured physical activity in youth. Med Sci Sports Exerc. (2002) 34(2):350–5. doi: 10.1097/00005768-200202000-00025
70. Sallis JF. Epidemiology of physical activity and fitness in children and adolescents. Crit Rev Food Sci Nutr. (1993) 33(4–5):403–8. doi: 10.1080/10408399309527639
71. Cassola VF, Milian FM, Kramer R, de Oliveira Lira CAB, Khoury HJ. Standing adult human phantoms based on 10th, 50th and 90th mass and height percentiles of male and female caucasian populations. Phys Med Biol. (2011) 56(13):3749. doi: 10.1088/0031-9155/56/13/002
72. Taylor RW, Grant AM, Williams SM, Goulding A. Sex differences in regional body fat distribution from pre-to postpuberty. Obesity. (2010) 18(7):1410–6. doi: 10.1038/oby.2009.399
73. Veldhuis JD, Roemmich JN, Richmond EJ, Rogol AD, Lovejoy JC, Sheffield-Moore M, et al. Endocrine control of body composition in infancy, childhood, and puberty. Endocr Rev. (2005) 26(1):114–46. doi: 10.1210/er.2003-0038
74. Bredella MA. Sex differences in body composition. In: Mauvais-Jarvis F, editors. Sex and gender factors affecting metabolic homeostasis, diabetes and obesity. Cham: Springer (2017): doi: 10.1007/978-3-319-70178-3_2
75. Bishop P, Cureton K, Collins M. Sex difference in muscular strength in equally-trained men and women. Ergonomics. (1987) 30(4):675–87. doi: 10.1080/00140138708969760
76. Landen S, Hiam D, Voisin S, Jacques M, Lamon S, Eynon N. Physiological and molecular sex differences in human skeletal muscle in response to exercise training. J Physiol (Lond). (2023) 601(3):419–34. doi: 10.1113/JP279499
77. Monteiro E, Fernandes A, Bigio L, Palma A, dos Santos LG, Cavanaugh MT, et al. Male relative muscle strength exceeds females for bench press and back squat. J Exerc Physiol. (2016) 19:79–85. http://www.asep.org/asep/asep/JEPonlineOCTOBER2016_Monteiro_Bigio.pdf
78. Huebner M, Perperoglou A. Sex differences and impact of body mass on performance from childhood to senior athletes in Olympic weightlifting. PLOS ONE. (2020) 15(9):e0238369. doi: 10.1371/journal.pone.0238369
79. Armstrong N, Welsman JR. Assessment and interpretation of aerobic fitness in children and adolescents. Exerc Sport Sci Rev. (1994) 22(1):435–76. doi: 10.1249/00003677-199401000-00016
80. Krabbe S, Christensen T, Worm J, Christiansen C, Transbøl I. Relationship between haemoglobin and serum testosterone in normal children and adolescents and in boys with delayed puberty. Acta Pædiatrica. (1978) 67(5):655–8. doi: 10.1111/j.1651-2227.1978.tb17818.x
81. Thomsen K, Riis B, Krabbe S, Christiansen C. Testosterone regulates the haemoglobin concentration in male puberty. Acta Pædiatrica. (1986) 75(5):793–6. doi: 10.1111/j.1651-2227.1986.tb10292.x
82. Goran M, Fields DA, Hunter GR, Herd SL, Weinsier RL. Total body fat does not influence maximal aerobic capacity. Int J Obes. (2000) 24(7):841–8. doi: 10.1038/sj.ijo.0801241
83. Demirkan E, Can S, Arslan E. The relationship between body composition and aerobic fitness in boys and girls distance runners. Int J Sports Sci. (2016) 6(2):62–5. doi: 10.5923/j.sports.20160602.07
84. de Simone G, Devereux RB, Daniels SR, Meyer RA. Gender differences in left ventricular growth. Hypertension. (1995) 26(6):979–83. doi: 10.1161/01.HYP.26.6.979
85. Castro OL, Haddy TB, Rana SR. Age-and sex-related blood cell values in healthy black Americans. Public Health Rep. (1987) 102(2):232. PMID: 3104982; PMCID: PMC1477821.
86. Murphy WG. The sex difference in haemoglobin levels in adults—mechanisms, causes, and consequences. Blood Rev. (2014) 28(2):41–7. doi: 10.1016/j.blre.2013.12.003
87. Gligoroska JP, Gontarev S, Dejanova B, Todorovska L, Stojmanova DS, Manchevska S. Red blood cell variables in children and adolescents regarding the age and sex. Iran J Public Health. (2019) 48(4):704–12. PMCID: PMC6500523; PMID: 31110981
88. Lepers R. Sex difference in triathlon performance. Front Physiol. (2019) 10:973. doi: 10.3389/fphys.2019.00973
89. Senefeld JW, Clayburn AJ, Baker SE, Carter RE, Johnson PW, Joyner MJ. Sex differences in youth elite swimming. PLOS ONE. (2019) 14(11):e0225724. doi: 10.1371/journal.pone.0225724
90. Nikolaidis PT, Rosemann T, Knechtle B. Sex differences in the age of peak marathon race time. Chin. J. Physiol. (2018) 61:85–91. doi: 10.4077/CJP.2018.BAG535
91. Andersson EP, Govus A, Shannon OM, McGawley K. Sex differences in performance and pacing strategies during sprint skiing. Front Physiol. (2019) 10:295. doi: 10.3389/fphys.2019.00295
92. Tiller NB, Elliott-Sale KJ, Knechtle B, Wilson PB, Roberts JD, Millet GY. Do sex differences in physiology confer a female advantage in ultra-endurance sport? Sports Med. (2021) 51(5):895–915. doi: 10.1007/s40279-020-01417-2
93. Knechtle B, Dalamitros AA, Barbosa TM, Sousa CV, Rosemann T, Nikolaidis PT. Sex differences in swimming disciplines-can women outperform men in swimming? Int J Environ Res Public Health. (2020) 17(10):3651. doi: 10.3390/ijerph17103651
94. Das D. San Francisco Marathon 2008–2021: Open Data and Statistics. 2021, Available at: https://debarghyadas.com/writes/sanfrancisco-marathon-data/ (Cited September 26, 2021).
95. Joyner MJ. Physiological limits to endurance exercise performance: influence of sex. J Physiol (Lond). (2017) 595(9):2949–54. doi: 10.1113/JP272268
96. Sato K, Iemitsu M, Katayama K, Ishida K, Kanao Y, Saito M. Responses of sex steroid hormones to different intensities of exercise in endurance athletes. Exp Physiol. (2016) 101(1):168–75. doi: 10.1113/EP085361
97. Ohlsson C, Vandenput L. The role of estrogens for male bone health. Eur J Endocrinol. (2009) 160(6):883–9. doi: 10.1530/EJE-09-0118
98. Chidi-Ogbolu N, Baar K. Effect of estrogen on musculoskeletal performance and injury risk. Front Physiol. (2019) 9:1–11. doi: 10.3389/fphys.2018.01834
99. Lebrun CM. Effect of the different phases of the menstrual cycle and oral contraceptives on athletic performance. Sports Med. (1993) 16(6):400–30. doi: 10.2165/00007256-199316060-00005
100. Bruinvels G, Burden RJ, McGregor AJ, Ackerman KE, Dooley M, Richards T, et al. Sport, exercise and the menstrual cycle: where is the research? British Journal of Sports Medicine. (2017) 51(6):487–88. doi: 10.1136/bjsports-2016-096279
101. Fischetto G, Sax A. The menstrual cycle and sport performance. New Stud Athl. (2013) 28(3/4):57–69. doi: 10.1016/j.csm.2005.01.003
102. Carmichael MA, Thomson RL, Moran LJ, Wycherley TP. The impact of menstrual cycle phase on athletes’ performance: a narrative review. Int J Environ Res Public Health. (2021) 18(4):1667. doi: 10.3390/ijerph18041667
103. Constantini NW, Dubnov G, Lebrun CM. The menstrual cycle and sport performance. Clin Sports Med. (2005) 24(2):e51–82. doi: 10.1016/j.csm.2005.01.003
104. Meignié A, Duclos M, Carling C, Orhant E, Provost P, Toussaint J-F, et al. The effects of menstrual cycle phase on elite athlete performance: a critical and systematic review. Front Physiol. (2021) 12:1–10. doi: 10.3389/fphys.2021.654585
105. Agency WA-D. Anti-Doping testing figures report. Montréal (Québec), Canada: Anti-Doping Agency (2023) p. 311. Available from: https://www.wada-ama.org/sites/default/files/2023-01/2021_anti-doping_testing_figures_en.pdf
106. Bhasin S, Hatfield DL, Hoffman JR, Kraemer WJ, Labotz M, Phillips SM, et al. Anabolic-androgenic steroid use in sports, health, and society. Med Sci Sports Exerc. (2021) 53(8):1778–94. doi: 10.1249/MSS.0000000000002670
107. Parkinson AB, Evans NA. Anabolic androgenic steroids: a survey of 500 users. Med Sci Sports Exerc. (2006) 38(4):644–51. doi: 10.1249/01.mss.0000210194.56834.5d
108. Huang G, Basaria S. Do anabolic-androgenic steroids have performance-enhancing effects in female athletes? Mol Cell Endocrinol. (2018) 464:56–64. doi: 10.1016/j.mce.2017.07.010
109. Huo S, Scialli AR, McGarvey S, Hill E, Tügertimur B, Hogenmiller A, et al. Treatment of men for “low testosterone”: a systematic review. PLOS ONE. (2016) 11(9):e0162480. doi: 10.1371/journal.pone.0162480
110. Elashoff JD, Jacknow AD, Shain SG, Braunstein GD. Effects of anabolic-androgenic steroids on muscular strength. Ann Intern Med. (1991) 115(5):387–93. doi: 10.7326/0003-4819-115-5-387
111. Falqueto H, Júnior JLR, Silvério MNO, Farias JCH, Schoenfeld BJ, Manfredi LH. Can conditions of skeletal muscle loss be improved by combining exercise with anabolic–androgenic steroids? A systematic review and meta-analysis of testosterone-based interventions. Rev Endocr Metab Disord. (2021) 22(2):161–78. doi: 10.1007/s11154-021-09634-4
112. Friedl KE. Effects of testosterone and related androgens on athletic performance in men. IN: Kraemer WJ, Rogol AD, editors. The Endocrine System in Sports and Exercise. (2005). p. 525–43. doi: 10.1002/9780470757826.ch35
113. Bermon S. Androgens and athletic performance of elite female athletes. Curr Opin Endocrinol Diabetes Obes. (2017) 24(3):246–51. doi: 10.1097/MED.0000000000000335
114. Hirschberg AL, Knutsson JE, Helge T, Godhe M, Ekblom M, Bermon S, et al. Effects of moderately increased testosterone concentration on physical performance in young women: a double blind, randomised, placebo controlled study. Br J Sports Med. (2020) 54(10):599. doi: 10.1136/bjsports-2018-100525
115. Pielke R, Tucker R, Boye E. Scientific integrity and the IAAF testosterone regulations. Int Sports Law J. (2019) 19(1):18–26. doi: 10.1007/s40318-019-00143-w
116. Ahmetov II, Stepanova AA, Biktagirova EM, Semenova EA, Shchuplova IS, Bets LV, et al. Is testosterone responsible for athletic success in female athletes? bioRxiv, 2019: p. 557348. doi: 10.23736/S0022-4707.20.10171-3
117. Bermon S, Garnier PY, Hirschberg AL, Robinson N, Giraud S, Nicoli R, et al. Serum androgen levels in elite female athletes. J Clin Endocrinol Metab. (2014) 99(11):4328–35. doi: 10.1210/jc.2014-1391
118. Cooper J. Testosterone: ‘the best discriminating factor’. Philosophies. (2019) 4(3):36. doi: 10.3390/philosophies4030036
119. Sőnksen PH, Dawn Bavington L, Boehning T, Cowan D, Guha N, Holt R, et al. Hyperandrogenism controversy in elite women’s sport: an examination and critique of recent evidence. Br J Sports Med. (2018) 52(23):1481. doi: 10.1136/bjsports-2017-098446
120. Hirschberg AL. Female hyperandrogenism and elite sport. Endocr Connect. (2020) 9(4):R81–r92. doi: 10.1530/EC-19-0537
121. Kelly A, Côté J, Jeffreys M, Turnnidge J, editors. Birth advantages and relative age effects in sport: Exploring organizational structures and creating appropriate Settings. (1st ed). Newyork, NY: Routledge (2021). https://doi.org/10.4324/9781003163572
122. Gooren LJ, Bunck MC. Transsexuals and competitive sports. Eur J Endocrinol. (2004) 151(4):425–9. doi: 10.1530/eje.0.1510425
123. Hamilton BR, Lima G, Barrett J, Seal L, Kolliari-Turner A, Guppy FM, et al. The Effects of Gender Affirming Treatment on the Sporting Performance and Muscle Memory of Transgender Athletes. A Protocol for The Tavistock Transgender Athlete Study. 2021. doi: 10.31236/osf.io/4rc2b
124. Deschenes MR. Effects of aging on muscle fibre type and size. Sports Med. (2004) 34(12):809–24. doi: 10.2165/00007256-200434120-00002
125. Thompson LV. Effects of age and training on skeletal muscle physiology and performance. Phys Ther. (1994) 74(1):71–81. doi: 10.1093/ptj/74.1.71
126. Shvartz E, Reibold RC. Aerobic fitness norms for males and females aged 6 to 75 years: a review. Aviat Space Environ Med. (1990) 61(1):3–11. PMID: 2405832
127. Heather AK. Transwoman elite athletes: their extra percentage relative to female physiology. Int J Environ Res Public Health. (2022) 19(15):9103. doi: 10.3390/ijerph19159103
128. Imbrišević M. Patriarchy in disguise: burke on pike and world rugby. Sport Ethics Philos. (2022) 1(1):1–31. doi: 10.1080/17511321.2022.2114534
129. Chiccarelli E, Aden J, Ahrendt D, Smalley J. Fit transitioning: when can transgender airmen fitness test in their affirmed gender? Mil Med. (2023) 188(7–8):e1588–95. doi: 10.1093/milmed/usac320
130. Jacobeit JW, Gooren LJ, Schulte HM. Long-Acting intramuscular testosterone undecanoate for treatment of female-to-male transgender individuals. J Sex Med. (2007) 4(5):1479–84. doi: 10.1111/j.1743-6109.2007.00556.x
131. Pigozzi F, Bigard X, Steinacker J, Wolfarth B, Badtieva V, Schneider C, et al. Joint position statement of the international federation of sports medicine (FIMS) and European federation of sports medicine associations (EFSMA) on the IOC framework on fairness, inclusion and non-discrimination based on gender identity and sex variations. BMJ Open Sport Exerc Med. (2022) 8(1):e001273. doi: 10.1136/bmjsem-2021-001273
132. D'hoore L, T’Sjoen G. Gender-affirming hormone therapy: an updated literature review with an eye on the future. J Intern Med. (2022) 291(5):574–92. doi: 10.1111/joim.13441
133. Riachy R, McKinney K, Tuvdendorj DR. Various factors may modulate the effect of exercise on testosterone levels in men. J Funct Morphol Kinesiol. (2020) 5(4):81. doi: 10.3390/jfmk5040081
134. Antero J, Saulière G, Marck A, Toussaint J-F. A medal in the olympics runs in the family: a cohort study of performance heritability in the games history. Front Physiol. (2018) 9:1313. doi: 10.3389/fphys.2018.01313
135. Sanchis-Gomar F, Pareja-Galeano H, Rodriguez-Marroyo JA, de Koning JJ, Lucia A, Foster C. Olympic Genes on the podium? Int J Sports Physiol Perform. (2016) 11(7):973–4. doi: 10.1123/ijspp.2016-0421
136. Parker K, Horowitz JM, Brown A. U.S. Adults have Complex views on gender identity and transgender issues. Washington, DC, USA: Pew Research Center (2022).
137. Besson T, Macchi R, Rossi J, Morio CYM, Kunimasa Y, Nicol C, et al. Sex differences in endurance running. Sports Med. (2022) 52(6):1235–57. doi: 10.1007/s40279-022-01651-w
138. Semerjian TZ, Cohen JH. FTM Means female to me": transgender athletes performing gender. Women Sport Phys Act J. (2006) 15(2):28. doi: 10.1123/wspaj.15.2.28
139. Wolfarth B, Bray MS, Hagberg JM, Pérusse L, Rauramaa R, Rivera MA, et al. The human gene map for performance and health-related fitness phenotypes: the 2004 update. Med Sci Sports Exerc. (2005) 37(6):881–903. doi: 10.1249/01.mss.0000168663.55604.1d
Keywords: transgender, sports, gender, genderqueer, performance
Citation: Oberlin DJ (2023) Sex differences and athletic performance. Where do trans individuals fit into sports and athletics based on current research?. Front. Sports Act. Living 5:1224476. doi: 10.3389/fspor.2023.1224476
Received: 17 May 2023; Accepted: 10 October 2023;
Published: 27 October 2023.
Edited by:
Giuseppe D'Antona, University of Pavia, ItalyReviewed by:
Domenico Martone, Parthenope University of Naples, ItalyLindsay Pieper, University of Lynchburg, United States
© 2023 Oberlin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: D. J. Oberlin ZG91Z2xhcy5vYmVybGluQGxlaG1hbi5jdW55LmVkdQ==