 Klemen Čretnik1
Klemen Čretnik1 Jernej Pleša
Jernej Pleša Žiga Kozinc
Žiga Kozinc Nejc Šarabon
Nejc Šarabon- 1Faculty of Health Sciences, University of Primorska, Izola, Slovenia
- 2Andrej Marušič Institute, University of Primorska, Koper, Slovenia
- 3Ludwig Boltzmann Institute for Rehabilitation Research, St. Pölten, Austria
- 4Human Health Department, InnoRenew CoE, Izola, Slovenia
- 5Laboratory for Motor Control and Motor Behavior, S2P, Science to Practice, Ltd., Ljubljana, Slovenia
The effects of eccentric exercise (ECC) in older adults have received limited scientific attention, considering the ample evidence for its effectiveness in general and athletic populations. The purpose of this paper is to review the effects of ECC exercise modalities vs. traditional or concentric (CON) exercise on muscle strength, body composition and functional performance in older adults. Inclusion criteria regarding the age was >55 years. Three major scientific literature databases (PubMed, Scopus and Web of Science) were screened for trials comparing the effect of ECC and CON exercise programs, and 19 papers were included in the meta-analysis. ECC and CON training programs were typically matched by the duration of each session. The difference between ECC and CON was expressed as standardized mean difference (SMD). Regarding isometric knee strength, the pooled effect favored ECC (SMD = 0.50), but was not statistically significant (p = 0.160). ECC exercise elicited greater improvements in timed up and go test (SMD = −0.68; p = 0.004), 2-min sit-stand test (SMD = 0.53; p = 0.030) and 30-s sit-stand test (SMD = 0.81; p = 0.002), but not in 6-min walking test (SMD = 0.01; p = 0.960). The effects on body composition and muscle architecture were unclear (SMD = −1.44 to 1.95; p = 0.060–0.689). In conclusion, our literature review indicates that ECC exercise is superior to, or at least as good as CON exercise for preserving health and overall function in older adults.
Introduction
Aging is associated with numerous physiological and morphological changes, related to declines in functional abilities and susceptibility to age-related diseases, which negatively influences the quality of life and independency (Deschenes, 2004; Capodaglio et al., 2005). Exercise interventions have been shown to improve cardiovascular health, decrease occurrence of sarcopenia and decrease fragility and risk of falling (Macaluso and De Vito, 2004; Benichou and Lord, 2016). Structured exercise is regarded as an effective method to prevent, delay, or attenuate the effect of aging, especially in terms of functional ability and physiological changes (Viña et al., 2016).
A plethora of factors needs to be considered in exercise prescription. One of such important factors is the type of muscle contraction. Muscular actions during resistance exercise may be isometric (i.e., the muscle length is maintained during activation), concentric (i.e., the muscle shortens during activation) and eccentric (i.e., the muscle lengthens during activation), all of which present distinct physiological, neural and mechanical characteristics and responses (Peake et al., 2005; Raman et al., 2012). It has been argued that any training regime that maximizes muscle strength will ultimately improve functional abilities (Malbut-Shennan and Young, 1999). On the other hand, many studies indicate that eccentric-focused training on eccentric ergometer promotes greater gains in muscle strength and hypertrophy when compared to conventional strength training (slow concentric and eccentric actions) performed in “standard” training regime of 10 repetitions per set (LaStayo et al., 2003; Mueller et al., 2009). Furthermore, LaStayo et al. (2014) reported that low-intensity endurance-focused eccentric contractions in eccentric cycling can result in large muscle hypertrophy in older adults. On the other hand, the study by Lewis et al. (2018) showed that the strength gains may not differ between training modalities (ECC and CON cycling) when the intensities are matched in middle-aged sedentary males. Nevertheless, this information should be carefully considered, because the participants in the study are middle age males, which means that the results could be different for older adults. Moreover, Gault and Willems (2013), reported that endurance eccentric exercises (e.g., eccentric cycling, downstairs walking) are adequate for elderly adults to reduce risk of falls and to improve their quality of life. It is also important to note that many tasks that are associated with a high risk of falling, such as descending stairs, relay heavily on eccentric muscle contractions.
In addition to superior effect of eccentric over traditional resistance exercise regarding strength and hypertrophy adaptations, studies reporting lower rate of perceived effort in eccentric compared concentric exercise (Lindstedt et al., 2001; LaStayo et al., 2003). Similar results have been shown for eccentric cycling compared to concentric cycling at the same intensity at given heart rate or oxygen consumption (LaStayo et al., 1999; Peñailillo et al., 2014; Clos et al., 2019). The most important drawback of eccentric exercise is a the possibility of exercise-induced muscle damage (Hody et al., 2013; Jamurtas et al., 2013). Moreover, eccentric exercise is sometimes somewhat more difficult to implement in contrast to conventional exercise methods because a) of safety reasons (eccentric exercises are usually performed at higher intensity, thus it is recommended that exercise is performed with the help of exercise practitioner or “spotter”) and b) lack of appropriate equipment. Given that both advantages and drawbacks of eccentric exercise have been identified, investigating the effect of eccentric-focused exercise in contrast to conventional resistance exercise is important to provide practitioners with optimal and comprehensive guidelines.
In contrast to general and athletic populations, older adults have received less scientific attention in relation to the effect of eccentric exercise. The effect of exercise interventions in older adults has been evaluated through different testing methods, such as functional ability tests (timed-up-and go test (TUGT), 5-repetition sit-to-stand, walking speed, etc.), body composition (muscle mass, fat mass, muscle cross-section area, etc.) and tests of motor abilities (e.g., strength, endurance, balance, etc.). Performance in functional tasks such as TUGT and 5-repetition sit-to-stand can be used to predict the risk for recurrent falls (Buatois et al., 2008). Moreover, performance of everyday functional tasks such as crossing the road or carrying bags from the store are also, to some extent, associated with isokinetic strength (Doherty, 2003). Two very recent systematic reviews focused on the effect of eccentric training in healthy older adults (Molinari et al., 2019; Kulkarni et al., 2021). Molinari et al. (2019) included 5 studies with muscle strength outcomes, and reported similar effects of eccentric exercises and traditional resistance exercises, with the data slightly favoring the former. Kulkarni et al. (2021) examined 10 studies and reported that eccentric exercises can be as effective as conventional exercises in older adults for improving functional performance. In sum, existing reviews are showing the potential of eccentric exercise to elicit similar improvement in comparison to traditional resistance exercise. In light of advantages of eccentric exercise, such as lower energy expenditure, it could be suggested that eccentric exercise should be incorporated in resistance exercise programs for older adults. However, only limited number of variables have been included in existing reviews, thus further analysis is needed to provide broader view about the effects of eccentric exercise and eccentric training modalities compared to traditional training type on basic motor capabilities, body composition and functional ability in older adults. Based on that, the objective of this paper is to review the effects of eccentric exercise modalities vs. traditional resistance exercise on muscle strength, body composition and functional performance in older adults. In accordance with the previous evidence, we hypothesized that eccentric exercise will have similar effect on functional performance, muscle strength and body composition, compared to traditional resistance exercise.
Methods
Search Strategy
The search was performed in October 2021. Three major scientific literature databases (PubMed, Scopus and Web of Science) were screened, using the following search term: (eccentric exercise OR flywheel OR isoinertial exercise OR eccentric training) AND (older adults OR elderly OR elders OR old age OR aging). The records were imported into Mendeley (version 1.19.8) to remove the duplicates, and then exported into Microsoft Excel software. The search strategy was carried out in three stages: (1) assessing the eligibility of the papers based on the title, (2) assessing the eligibility of the papers based on the abstract and (3) assessing the eligibility of the papers based on the full text. Both reviewers assess all papers. At all three stages, two reviewers carried out the procedures independently. In case of non-agreement in stages 1.-2., any papers that were identified by only one reviewer were carried over to the next phase. In stage 3., potential disagreements were resolved by additional discussion and consultation of the third reviewer.
Inclusion Criteria
The inclusion criteria are structured according to the PICOS tool (Methley et al., 2014), as follows:
• P (population): older adults, aged > 55 years. We excluded patients with neurological diseases (e.g., Parkinson's disease), but we also considered patients with metabolic and cardio-vascular diseases.
• I (Intervention): Resistance exercise interventions focusing on (or emphasizing) eccentric contraction. This includes flywheel training and functional tasks such as loaded stair descent. Duration of the intervention > 4 weeks.
• C (Comparison): Resistance exercise interventions, performed in a traditional manner or emphasizing concentric contraction.
• (Outcome): Outcomes describing muscle performance (muscle strength or power), body composition outcomes (e.g., lean mass, muscle thickness, body fat mass) and functional performance tests (e.g., 6-min walking test, sit-stand tests, stair walking, etc.).
• S (Study design): Interventional clinical trials, with at least two groups (eccentric and traditional/concentric exercise groups).
Data Extraction
The data extraction was carried out independently by two reviewers and disagreements were resolved through consultation with other reviewers. The extracted data included: (a) baseline and post-intervention means and standard deviations for all eligible outcome measures for eccentric and concentric groups; percent changes were considered instead of pre-post data when available (b) baseline demographics of participants (gender, age, body height, body mass, body mass index); (c) intervention characteristics (target body area (upper, lower or whole-body), duration of the intervention, number of sessions per week, volume (number of exercises, sets, and repetitions), breaks between exercises and sets, supervision, and progression of exercise difficulty). Data were carefully entered into Microsoft Excel 2016 (Microsoft, Redmond, WA, USA). If the data were presented in a graphical rather than tabular form, we used Adobe Illustrator Software (version CS5, Adobe Inc., San Jose, CA, USA) to accurately determine the means and standard deviations. In case of missing data, the corresponding author of the respective article was contacted by e-mail. If no response was received after 7 days, the author was contacted again. If the author did not reply to the second inquiry, the data was considered irretrievable.
Assessment of the Quality of the Included Studies
Two reviewers evaluated the quality of the included studies using the PEDro scale (Maher et al., 2003), which assesses study quality based on a 0–10 scale. Potential disagreements between the reviewers were resolved by consulting the other authors. Studies scoring from 9 to 10 were considered as “excellent,” 6 to 8 as “good,” 4 to 5 as “fair,” and <4 as “poor” quality. The PEDro scale was selected because it was developed to assess the quality of clinical trial studies evaluating physical therapy interventions.
Data Analysis
The main data analyses were carried out in Review Manager (Version 5.3, Copenhagen: The Nordic Cochrane Center, The Cochrane Collaboration, London, UK). Before the results were entered into the meta-analytical model, the pre-post differences and pooled standard deviations were calculated according to the following formula SD = √[( + ) – (2 × r × SDpre × SDpost). The correction value (r), which represents the pre-test–post-test correlation of outcome measures, was conservatively set at 0.75. It should be noted that a change in the correction value in the range between 0.5 and 0.9 had little effect on the pooled SD and would not change the outcomes of the meta-analyses. For the meta-analysis, the inverse variance method for continuous outcomes with a random-effects model was used. The effect sizes were expressed as standardized mean difference (SMD). For SMD, the respective 95% confidence intervals were also calculated and reported.
The analysis compared the effects of the eccentric exercise and traditional resistance exercise or concentric exercise interventions. Statistical heterogeneity among studies was determined by calculating the I2 statistics. According to Cochrane guidelines, the I2 statistics of 0% to 40% might not be important, 30 to 60% may represent moderate heterogeneity, 50–90% may represent substantial heterogeneity, and 75–100% indicates considerable heterogeneity. The threshold for statistical significance was set at p ≤ 0.05 for the pooled effect size. Sensitivity analysis was performed by examining the effect of exclusion of studies one-by-one from the analyses.
Results
Search Summary
The initial search yielded 3,188 records (PubMed = 1,200; Scopus = 97; Web of science = 1,891). After the duplicates were removed, 2,521 records were left for examination. Based on the title, Reviewer 1 identified 264 potentially relevant papers, and Reviewer 2 identifies 242. Most of the papers were overlapping between the reviewers, thus, the sum of the identified papers was 332. In the next step, based on the abstract reading, Reviewer 1 identified 61 potentially relevant papers, and Reviewer 2 identified 57. At this stage, the reference lists of relevant reviews were also scrutinized, and 1 additional paper was included. In total, 73 papers were included for a full-text examination. Both reviewers identified 18 eligible papers with a complete agreement, thus, 19 papers were included into the meta-analysis. The search is summarized on the Flowchart in Figure 1. Supplementary Table 1 also includes the list of papers included at each stage, as well as the extracted data. Table 1 includes basic information regarding the included studies.
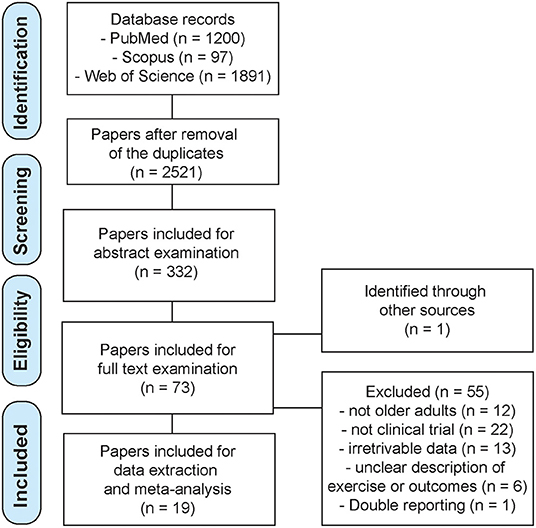
Figure 1. Flowchart with search protocol summary.

Table 1. Overview of the studies included into meta-analyses.
Assessment of Study Quality
All of the studies received the PEDro score in the 3–6 range. Two studies received a score of 3 points, indicating “poor” quality. One study received the score of 6, indicating “good” quality. The remaining studies were of “fair” quality (9 studies with a score of 4; 7 studies with a score of 5). The mean PEDro score was 4.4 ± 0.8. Overall, the evidence presented in this review may be considered to be of “fair” quality. The most common items that almost all studies failed to satisfy were blinding of the subjects, therapists and assessors. Exercise intensity and type of the exercise (whole body only or single-joint task) were not part of the sorting criteria.
Muscle Strength
Isometric muscle strength assessments were included in 12 studies, involving 149 participants in eccentric exercise groups and 148 participants in traditional resistance or concentric exercise groups (Figure 2). The overall effect, although favoring the eccentric exercise group (SMD = 0.50), was not statistically significant (p = 0.160). Moreover, the heterogeneity across the studies was high (I2 = 87 %). Sensitivity analysis showed that the exclusion of one study that favored concentric exercise (Onambélé et al., 2008) swayed the pooled effect enough to be statistically significant (p = 0.030) in favor of eccentric exercise (SMD = 0.71). Isometric ankle extension strength was assessed in two studies (with 33 participants in total for each group). The results are in favor of eccentric exercise with moderate effect (SMD = 0.92), but the difference between the exercise types was not statistically significant (p = 0,200), and the two studies were very heterogeneous (I2 = 84 %) (Figure 2).
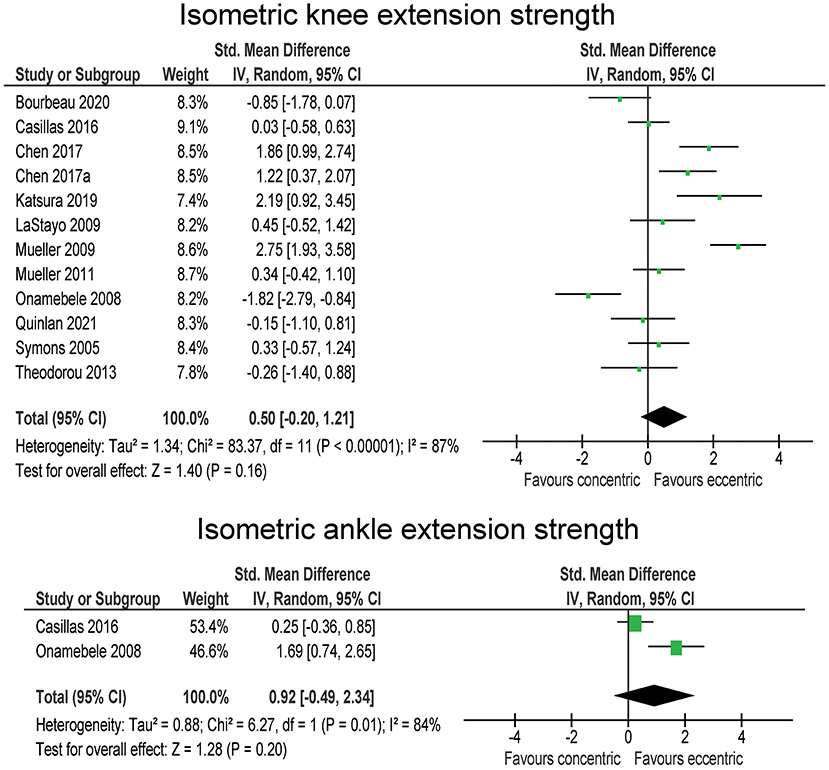
Figure 2. The effect of eccentric vs. concentric exercise on muscle strength outcomes.
Body Composition and Muscle Architecture
Body fat percentage and body fat mass were considered in three studies, with a total number of 47 participants in eccentric exercise groups and 48 participants in in traditional resistance or concentric exercise groups Although the overall effect was large (SMD = −1.44) and showing decreases in body fat with eccentric exercise, it was statistically not significant (p = 0.220). A closer inspection of the data revealed that two studies showed almost no difference between the exercise types, while one study pointed heavily toward fat-lowering effect of eccentric exercise in comparison to traditional resistance or concentric exercise. Accordingly, the heterogeneity between the studies was very high (I2 = 95 %). Lean leg mass was reported in two studies (with 50 and 49 participants in total for eccentric and concentric/traditional exercise groups, respectively) (Figure 3). The difference between the exercise modes was negligible (SMD = 0.08; p = 0.680).
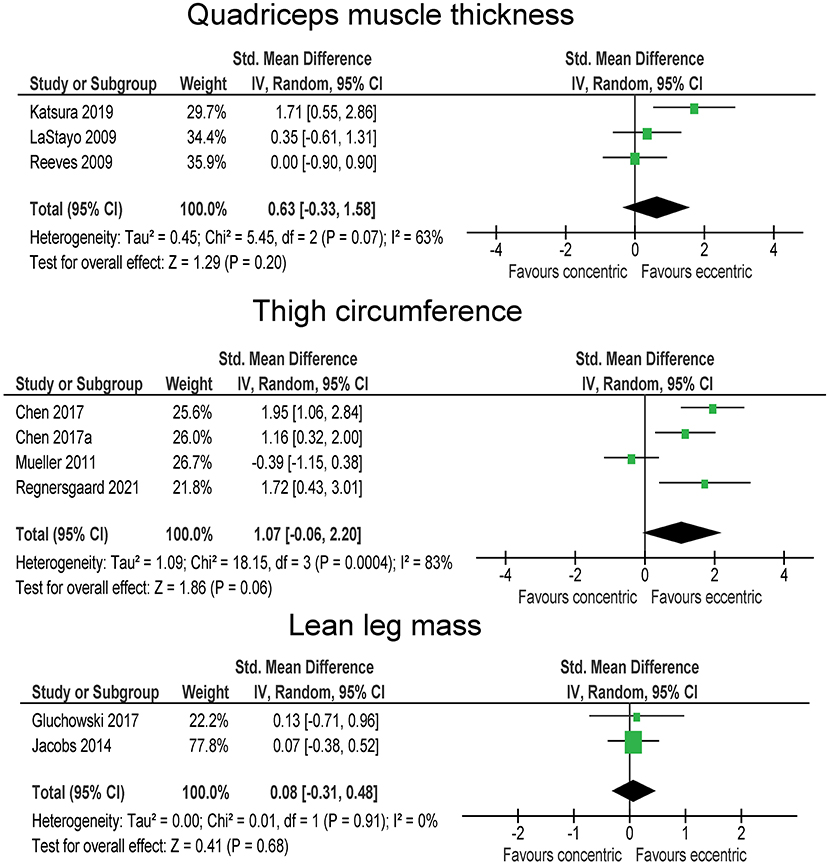
Figure 3. The effect of eccentric vs. concentric exercise on outcomes related to body composition.
Four studies compared the effect of eccentric and traditional resistance or concentric exercise on quadriceps muscle thickness (28 and 25 participants in total within eccentric and concentric/traditional groups, respectively) (Figure 3). The overall effect tended to support the superiority of eccentric exercise (SMD = 0.63), but was not statistically significant (p = 0.200) and the heterogeneity among the studies was high (I2 = 63 %). The results for thigh circumference and thigh mass were pooled together from four studies, involving a total of 48 and 49 participants in eccentric and traditional resistance or concentric exercise groups, respectively. Three studies indicated larger thigh circumference/mass increases in eccentric group with large effect sizes (SMD = 1.16–1.95), however, one study pointed in the opposite direction (SMD = −0.39), yielding a large pooled effect that tended toward better effects in eccentric groups (SMD = 1.07), but slightly above the threshold for statistical significance (p = 0.060). The heterogeneity among the studies was high (I2 = 63%) (Figure 3), with three studies favoring eccentric and one study favoring traditional resistance. In a sensitivity analysis, the exclusion of the latter study (Mueller et al., 2011) resulted in statistically significant effect (p < 0.001) favoring eccentric exercise (SMD = 1.57). One study also involved the measurement of pennation angle and fascicle length of the vastus lateralis muscle. There was a large effect in favor of traditional resistance or concentric exercise for pennation angle (SMD = 2.65), while the opposite was true for the fascicle length (SMD = 1.25) (both p < 0.01).
Mobility and Function
The 6-min walking test was performed in 7 studies, involving a total of 97 participants in each group. The studies indicate no difference between the intervention groups on 6-min walking test (SMD = 0.01; p = 0.960). The heterogeneity among the studies was moderate (I2 = 54 %). On the contrary, statistically significant (p = 0.002) moderate effect (SMD = 0.81) in favor of eccentric exercise was shown for the 30-s sit-stand test (Figure 4), which was tested in four studies, involving 44 participants in eccentric exercise groups and 43 participants in traditional resistance or concentric exercise groups. The heterogeneity among the studies was low (I2 = 19 %). Two studies (44 and 43 participants in eccentric and traditional resistance or concentric exercise groups) included the stair descent test and tended to support a somewhat favorable effect of eccentric compared to traditional resistance or concentric exercise (SMD = −0.46), but not reaching statistical significance (p = 0.179). The two studies were homogenous (I2 = 0%). Moreover, two studies (involving a total number of 19 participants in each group) reported the results of stair ascent test (Figure 4). The difference between the exercise modes was trivial (SMD = 0.03; p = 0.930). Three studies reported on the 2-min stepping test results (37 participants in eccentric exercise groups, 36 in traditional resistance or concentric exercise groups) (Figure 4). The overall effect favored the eccentric exercise (SMD = 0.53) and was statistically significant (p = 0.03). The studies reported very consistent results, as shown by negligible heterogeneity (I2 = 0 %). TUGT was included in six studies (82 and 78 participants in eccentric and traditional resistance or concentric exercise groups, respectively). Similar to 30-s sit-stand, the results for TUGT were also statistically significantly (p = 0.004) better after eccentric exercise than traditional resistance or concentric exercise interventions (SMD = −0.68), and the heterogeneity among the studies was low (I2 = 22 %).
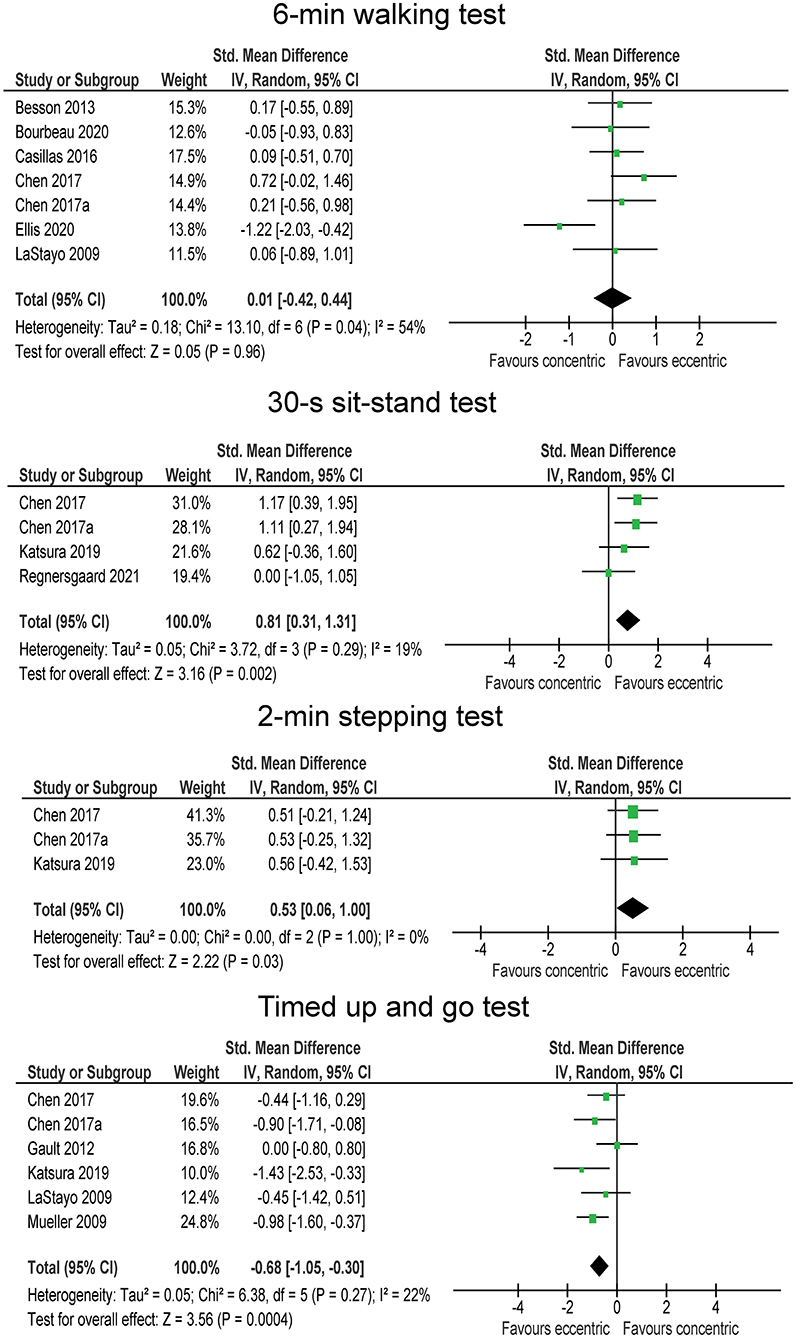
Figure 4. The effect of eccentric vs. concentric exercise on outcomes related to function and mobility.
Discussion
The purpose of this systematic review with meta-analysis was to examine the effects of eccentric exercise interventions in contrast to traditional resistance or concentric exercise interventions on muscle strength, body composition, muscle architecture, mobility, and function in older adults. We included 18 interventional clinical trials that had at least two intervention groups (eccentric and traditional resistance or concentric intervention group). The main findings of our systematic review are as follows: (a) for muscle strength, the pooled effect favored eccentric exercise, but the difference to traditional resistance or concentric was not statistically significant; (b) the results regarding body composition and muscle architecture were unclear and pooled from a smaller number of studies; (c) for mobility and function, the results were diverse, with the effects either in favor of eccentric exercise, or showing no difference between the intervention groups. In sum we examined a wide variety of tests and yielded different results. Because of this fact we cannot say with absolute certainty that eccentric exercises are superior to traditional resistance or concentric exercises and therefore cannot entirely reject nor accept our hypothesis. Although the results support the somewhat favorable effect of eccentric exercises, there are still a few questions that remain open.
The studies examined a wide variety of functional tests, including tests that emphasize aerobic capacity (6MWT, 2-min stepping test) and tests that assess functional performance and mobility (TUGT, 30-s sit-stand test, stair descending and stair ascending). Seven studies examined the effect of eccentric exercise on 6MWT. All the studies were in agreement that the effect of eccentric resistance training is similar to that of traditional resistance or concentric exercise. Some studies have speculated that the improvements in eccentric training are due to an increased contribution of anaerobic metabolism during eccentric training and a consequent improvement of its capacity. Adaptation of anaerobic capacity would particularly benefit shorter functional tests, such as 30-s sit-stand test (Besson et al., 2013; Laroche et al., 2013). On the other hand, it has been proposed that involvement of elastic components in eccentric exercise could improve movement efficiency, which is associated with reduced metabolic cost (LaStayo et al., 1999; Lindstedt et al., 2001) and could contribute to improvement in all functional tests. Namely, as eccentric exercise is associated with lower metabolic costs, it presumably enables higher force and power outputs to be reached during training, which would in turn elicit higher adaptations in muscle capacity. Even within endurance tests, such as 6MWT, greater anaerobic capacity could improve the performance, as resistance exercise interventions have been shown numerous times to improve economy of endurance activities (Hartman et al., 2007; Hunter et al., 2021). The 2-min stepping test was improved for ~10% in the eccentric exercise groups and ~5% in traditional resistance or concentric exercise group (Chen et al., 2017a,b; Katsura et al., 2019). Thus, both interventions improved the 2-min stepping test results, but the eccentric training group was even more effective (SMD = 0.53).
The TUGT and the 30-s sit-stand test are the among the most frequently used and scientifically supported tests for assessing overall function in older adults (Beauchet et al., 2011; Bennell et al., 2011; Barry et al., 2014). We found greater improvement in TUGT with eccentric exercise (p = 0.004; SMD = −0.68) compared to traditional resistance or concentric exercise. That was also the case with 30-s sit to stand test (p = 0.002; SMD = 0.81). However, it appears that the effects on maximal strength are similar in both groups although there was some tendency for larger effects in eccentric groups. One of the most common issues in older adults is sarcopenia, which is associated with a decreased quality of life, lower exercise tolerance and decreased levels physical activity levels in general (Maltais et al., 2014). Therefore, increasing or maintaining muscle mass and muscle strength need to be considered as a priority when planning training protocols for older adults. It is well-documented that resistance exercise is a very effective low-cost tool for preventing and treating sarcopenia and chronic diseases (Booth et al., 2012; Pedersen and Saltin, 2015; Ciolac and Rodrigues-da-Silva, 2016). As we can see from this systematic review, eccentric exercise can be as effective or even more effective than traditional resistance or concentric exercise. Of note, care should be taken when prescribing the quantity and intensity of exercise to avoid or minimize the risk of muscle damage and associated muscle soreness. Clos et al. (2021) came to a conclusion that when exercises are performed at the same power output, eccentric cycling elicits less intense perceptions of effort and muscle pain than concentric cycling. Maximal voluntary torque on the other hand showed a similar decline. When clinicians base the eccentric exercises on the rating of perceived exertion they should be very careful, given that most participants exhibit more neuromuscular performance decline after eccentric exercises (Clos et al., 2021).
The interventions considered in this review included either high-load eccentric resistance exercises, or low-load cyclic tasks performed in eccentric conditions or with accentuated eccentric portion of the movement (downhill walking, stair descending, and eccentric cycling). Downhill or downstairs walking is emerging as an effective type of eccentric exercise for the elderly. Assuming that training protocol is carried out where an elevator or any kind of assistance that helps the trainee to ascend is available, the intervention requires little additional equipment. Chen et al. (2017a) reported that descending stair walking improved muscle function, physical fitness, balance, cardiorespiratory fitness, lipid profiles, bone mineral density, and insulin sensitivity more than ascending stair walking in elderly obese women. In addition to providing great health and fitness benefits, downhill/downstairs walking is also metabolically less demanding than uphill/upstairs walking (Theodorou et al., 2013; Chen et al., 2017b; Regnersgaard et al., 2021). There is a wide variety of other means to perform eccentric exercise, such as working on resistance-training machines, performing everyday tasks in a way to emphasize eccentric contraction (e.g., sitting slowly down on a chair), or working on an eccentric cycle-ergometer. As said, one of the most important tasks of clinicians is that they dose the exercise correctly and that exercise is personalized by monitoring the rating of perceived exertion. Across the studies included in this review, the exercise was progressed gradually as fitness improved; either by pre-determined progression plan, or by tracking the rating of perceived exertion. Studies in this review mostly used the intensity corresponding to “somewhat hard” to “hard” exertion (between 9 and 13) on a Borg scale.
There are also a few limitations of this review to consider. The interventions were relatively short-term (6–12 weeks), which means that the differences between eccentric and traditional resistance or concentric exercise regarding long-term effects in older adults are not known. Moreover, several outcomes in the meta-analyses were pooled from a limited number of studies. In addition, subgroup analyses were not feasible due to the low number of studies. A few limitations also arise from the fact that there is sometimes hard to distinguish between ECC-only and ECC-emphasized exercise training protocols. It does raise an interesting question for further research on the topic, whether ECC-only training is more beneficial than merely emphasizing the ECC part of the exercise. Finally, the workload match between the exercise groups has to be questioned. Several studies used Borg scale, usually permitting some variation (e.g., 9–11 units). Some studies allowed participants to self-select the intensity (Gault and Willems, 2013) and very few used load prescription based on % repetition maximum (Reeves et al., 2009). It is not always clear how exercise programs should be matched to examine pure difference due to contraction type and maintain the ecological validity at the same time.
Conclusion
In conclusion, our literature review indicates that there are a few tests in which eccentric training is superior or at least equal to traditional resistance or concentric training in maintaining health and overall function in older adults. The tests that showed the most effects for shorter (anaerobic) tests such as 30-s sit-stand test and TUGT. On the other hand, longer (aerobic) tests showed less improvements. When examining the papers, we also came to a conclusion that eccentric exercise is safe for frail and sick individuals. This type of exercise has to be well-planned and constantly monitored by clinicians. When progressing the exercise, one of the more useful tools to use is a combination of RPE, increasing quantity and a gradual increase in amount and intensity within a training protocol.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Author Contributions
KČ, JP, SL, ŽK, and NŠ conceptualized the idea. KČ and JP carried out the review and wrote the manuscript. NŠ and ŽK were overviewing the review procedure. NŠ, SL, and ŽK analyzed the collected data and finalized the manuscript. All authors contributed to the article and approved the submitted version.
Funding
We want to acknowledge the support of the European Regional Development Fund and Physiko- and Rheumatherapie Institute through the Centre of Active Ageing project in the Interreg Slovakia–Austria cross-border cooperation program (partners: Faculty for Physical Education and Sports, Comenius University in Bratislava: Institute for Physical Medicine and Rehabilitation, Physiko- and Rheumatherapie GmbH). NŠ and ŽK acknowledge the University of Primorska's suppirt through internal research program KINSPO (2990-1-2/2021). The funders had no role in study conceptualization, data acquisition, data analysis or manuscript preparation.
Conflict of Interest
NŠ was employed by company S2P, Science to Practice, Ltd. The company hand no role in conceptualization of the study, data acquisition, article writing nor any other phase of the study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2022.873718/full#supplementary-material
References
Barry, E., Galvin, R., Keogh, C., Horgan, F., and Fahey, T. (2014). Is the Timed Up and Go test a useful predictor of risk of falls in community dwelling older adults: a systematic review and meta-analysis. BMC Geriatr. 14:14. doi: 10.1186/1471-2318-14-14
Beauchet, O., Fantino, B., Allali, G., Muir, S. W., Montero-Odasso, M., and Annweiler, C. (2011). Timed up and go test and risk of falls in older adults: a systematic review. J. Nutr. Heal. Aging 15, 933–938. doi: 10.1007/s12603-011-0062-0
Benichou, O., and Lord, S. R. (2016). Rationale for strengthening muscle to prevent falls and fractures: a review of the evidence. Calcif. Tissue Int. 98, 531–545. doi: 10.1007/s00223-016-0107-9
Bennell, K., Dobson, F., and Hinman, R. (2011). Measures of physical performance assessments: Self-Paced Walk Test (SPWT), Stair Climb Test (SCT), Six-Minute Walk Test (6MWT), Chair Stand Test (CST), Timed Up and Go (TUG), Sock Test, Lift and Carry Test (LCT), and car task. Arthritis Care Res. 63, S350–S370. doi: 10.1002/acr.20538
Besson, D., Joussain, C., Gremeaux, V., Morisset, C., Laurent, Y., Casillas, J. M., et al. (2013). Eccentric training in chronic heart failure: feasibility and functional effects. Results of a comparative study. Ann. Phys. Rehabil. Med. 56, 30–40. doi: 10.1016/j.rehab.2013.01.003
Booth, F. W., Roberts, C. K., and Laye, M. J. (2012). Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2, 1143–1211. doi: 10.1002/cphy.c110025
Bourbeau, J., Sena, R. D. S., Taivassalo, T., Richard, R., Jensen, D., Baril, J., et al. (2020). Eccentric versus conventional cycle training to improve muscle strength in advanced COPD: a randomized clinical trial. Respir Physiol Neurobiol. 276:103414. doi: 10.1016/j.resp.2020.103414
Buatois, S., Miljkovic, D., Manckoundia, P., Gueguen, R., Vançon, G., Perrin, P., et al. (2008). Five times sit to stand test is a predictor of recurrent falls in healthy community-living subjects aged 65 and older. J. Am. Geriatr. Soc. 56, 1575–1577. doi: 10.1111/j.1532-5415.2008.01777.x
Capodaglio, P., Capodaglio, E. M., Ferri, A., Scaglioni, G., Marchi, A., and Saibene, F. (2005). Muscle function and functional ability improves more in community-dwelling older women with a mixed-strength training programme. Age Ageing 34, 141–147. doi: 10.1093/ageing/afi050
Casillas, J. M., Besson, D., Hannequin, A., Gremeaux, V., Morisset, C., Tordi, N., et al. (2016). Effects of an eccentric training personalized by a low rate of perceived exertion on the maximal capacities in chronic heart failure: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 52, 159–168.
Chen, T. C., Hsieh, C. C., Tseng, K. W., Ho, C. C., and Nosaka, K. (2017b). Effects of descending stair walking on health and fitness of elderly obese women. Med. Sci. Sports Exerc. 49, 1614–1622. doi: 10.1249/MSS.0000000000001267
Chen, T. C. C., Tseng, W. C., Huang, G. L., Chen, H. L., Tseng, K. W., and Nosaka, K. (2017a). Superior effects of eccentric to concentric knee extensor resistance training on physical fitness, insulin sensitivity and lipid profiles of elderly men. Front. Physiol. 8:209. doi: 10.3389/fphys.2017.00209
Ciolac, E. G., and Rodrigues-da-Silva, J. M. (2016). Resistance training as a tool for preventing and treating musculoskeletal disorders. Sport. Med. 46, 1239–1248. doi: 10.1007/s40279-016-0507-z
Clos, P., Laroche, D., Stapley, P. J., and Lepers, R. (2019). Neuromuscular and perceptual responses to sub-maximal eccentric cycling. Front. Physiol. 10:354. doi: 10.3389/fphys.2019.00354
Clos, P., Mater, A., Laroche, D., and Lepers, R. (2021). Concentric versus eccentric cycling at equal power output or effort perception: neuromuscular alterations and muscle pain. Scand. J. Med. Sci. Sports 32, 45–59. doi: 10.1111/sms.14053
Deschenes, M. R. (2004). Effects of aging on muscle fibre type and size. Sport. Med. 34, 809–824. doi: 10.2165/00007256-200434120-00002
Doherty, T. J. (2003). Physiology of aging invited review: aging and sarcopenia. J. Appl. Physiol. 95, 1717–1727. doi: 10.1152/japplphysiol.00347.2003
Gault, M. L., Clements, R. E., and Willems, M. E. T. (2012). Functional mobility of older adults after concentric and eccentric endurance exercise. Eur. J. Appl. Physiol. 112, 3699–3707. doi: 10.1007/s00421-012-2338-4
Gault, M. L., and Willems, M. E. T. (2013). Isometric strength and steadiness adaptations of the knee extensor muscles to level and downhill treadmill walking in older adults. Biogerontology 14, 197–208. doi: 10.1007/s10522-013-9423-x
Gluchowski, A., Dulson, D., Merien, F., Plank, L., and Harris, N. (2017). Comparing the effects of two distinct eccentric modalities to traditional resistance training in resistance trained, higher functioning older adults. Exp. Gerontol. 98, 224–229. doi: 10.1016/j.exger.2017.08.034
Hartman, M. J., Fields, D. A., Byrne, N. M., and Hunter, G. R. (2007). Resistance training improves metabolic economy during functional tasks in older adults. J. Strength Cond. Res. 21, 91–5. doi: 10.1519/00124278-200702000-00017
Hody, S., Rogister, B., Leprince, P., Laglaine, T., and Croisier, J. L. (2013). The susceptibility of the knee extensors to eccentric exercise-induced muscle damage is not affected by leg dominance but by exercise order. Clin. Physiol. Funct. Imaging 33, 373–380. doi: 10.1111/cpf.12040
Hunter, G. R., Singh, H., Martins, C., Baranauskas, M. N., and Carter, S. J. (2021). Stretch-shortening cycle potentiation and resistance training-induced changes in walking economy/ease and activity-related energy expenditure in older women. J. Strength Cond. Res. 35, 1345–1349. doi: 10.1519/JSC.0000000000003975
Jacobs, J. L., Marcus, R. L., Morrell, G., and LaStayo, P. (2014). Resistance exercise with older fallers: Its impact on intermuscular adipose tissue. Biomed Res. Int. 2014:398960. doi: 10.1155/2014/398960
Jamurtas, A. Z., Garyfallopoulou, A., Theodorou, A. A., Zalavras, A., Paschalis, V., Deli, C. K., et al. (2013). A single bout of downhill running transiently increases HOMA-IR without altering adipokine response in healthy adult women. Eur. J. Appl. Physiol. 113, 2925–2932. doi: 10.1007/s00421-013-2717-5
Katsura, Y., Takeda, N., Hara, T., Takahashi, S., and Nosaka, K. (2019). Comparison between eccentric and concentric resistance exercise training without equipment for changes in muscle strength and functional fitness of older adults. Eur. J. Appl. Physiol. 119, 1581–1590. doi: 10.1007/s00421-019-04147-0
Kulkarni, D., Gregory, S., and Evans, M. (2021). Effectiveness of eccentric-biased exercise interventions in reducing the incidence of falls and improving functional performance in older adults: a systematic review. Eur. Geriatr. Med. doi: 10.1007/s41999-021-00571-8. [Epub ahead of print].
Laroche, D., Joussain, C., Espagnac, C., Morisset, C., Tordi, N., Gremeaux, V., et al. (2013). Is it possible to individualize intensity of eccentric cycling exercise from perceived exertion on concentric test? Arch. Phys. Med. Rehabil. 94, 1621–1627.e1. doi: 10.1016/j.apmr.2012.12.012
LaStayo, P., Marcus, R., Dibble, L., Frajacomo, F., and Lindstedt, S. (2014). Eccentric exercise in rehabilitation: safety, feasibility, and application. J. Appl. Physiol. 116, 1426–1434. doi: 10.1152/japplphysiol.00008.2013
LaStayo, P. C., Ewy, G. A., Pierotti, D. D., Johns, R. K., and Lindstedt, S. (2003). The positive effects of negative work: increased muscle strength and decreased fall risk in a frail elderly population. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 58, M419–424. doi: 10.1093/gerona/58.5.M419
LaStayo, P. C., Meier, W., Marcus, R. L., Mizner, R., Dibble, L., and Peters, C. (2009). Reversing muscle and mobility deficits 1 to 4 years after tka: A pilot study. Clin. Orthop. Relat. Res. 467, 1493–1500. doi: 10.1007/s11999-009-0801-2
LaStayo, P. C., Reich, T. E., Urquhart, M., Hoppeler, H., and Lindstedt, S. L. (1999). Chronic eccentric exercise: improvements in muscle strength can occur with little demand for oxygen. Am. J. Physiol. Regul. Integr. Comp. Physiol. 276, R611–615. doi: 10.1152/ajpregu.1999.276.2.R611
Lewis, M. C., Peoples, G. E., Groeller, H., and Brown, M. A. (2018). Eccentric cycling emphasising a low cardiopulmonary demand increases leg strength equivalent to workload matched concentric cycling in middle age sedentary males. J. Sci. Med. Sport 21, 1238–1243. doi: 10.1016/j.jsams.2018.05.009
Lindstedt, S. L., LaStayo, P. C., and Reich, T. E. (2001). When active muscles lengthen: properties and consequences of eccentric contractions. News Physiol. Sci. 16, 256–261. doi: 10.1152/physiologyonline.2001.16.6.256
Macaluso, A., and De Vito, G. (2004). Muscle strength, power and adaptations to resistance training in older people. Eur. J. Appl. Physiol. 91, 450–472. doi: 10.1007/s00421-003-0991-3
Maher, C. G., Sherrington, C., Herbert, R., Moseley, A. M., and Elkins, M. (2003). Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 83, 713–721. doi: 10.1093/ptj/83.8.713
Malbut-Shennan, K., and Young, A. (1999). The physiology of physical performance and training in old age. Coron. Artery Dis. 10, 37–42. doi: 10.1097/00019501-199901000-00007
Maltais, F., Decramer, M., Casaburi, R., Barreiro, E., Burelle, Y., Debigare, R., et al. (2014). An official American thoracic society/european respiratory society statement: update on limb muscle dysfunction in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 189, e15–62. doi: 10.1164/rccm.201402-0373ST
Methley, A. M., Campbell, S., Chew-Graham, C., McNally, R., and Cheraghi-Sohi, S. (2014). PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 14:579. doi: 10.1186/s12913-014-0579-0
Molinari, T., Steffens, T., Roncada, C., Rodrigues, R., and Dias, C. P. (2019). Effects of eccentric-focused versus conventional training on lower limb muscular strength in older adults: a systematic review with meta-analysis. J. Aging Phys. Act. 27, 823–830. doi: 10.1123/japa.2018-0294
Mueller, M., Breil, F. A., Lurman, G., Klossner, S., Flück, M., Billeter, R., et al. (2011). Different molecular and structural adaptations with eccentric and conventional strength training in elderly men and women. Gerontology 57, 528–538. doi: 10.1159/000323267
Mueller, M., Breil, F. A., Vogt, M., Steiner, R., Klossner, S., Hoppeler, H., et al. (2009). Different response to eccentric and concentric training in older men and women. Eur. J. Appl. Physiol. 107, 145–153. doi: 10.1007/s00421-009-1108-4
Onambélé, G. L., Maganaris, C. N., Mian, O. S., Tam, E., Rejc, E., McEwan, I. M., et al. (2008). Neuromuscular and balance responses to flywheel inertial versus weight training in older persons. J. Biomech. 41, 3133–3138. doi: 10.1016/j.jbiomech.2008.09.004
Peake, J., Nosaka, K., and Suzuki, K. (2005). Characterization of inflammatory responses to eccentric exercise in humans. Exerc. Immunol. Rev. 11, 64–85.
Pedersen, B. K., and Saltin, B. (2015). Exercise as medicine - Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sport. 25, 1–72. doi: 10.1111/sms.12581
Peñailillo, L., Blazevich, A., and Nosaka, K. (2014). Energy expenditure and substrate oxidation during and after eccentric cycling. Eur. J. Appl. Physiol. 114, 805–814. doi: 10.1007/s00421-013-2816-3
Quinlan, J. I., Franchi, M. V., Gharahdaghi, N., Badiali, F., Francis, S., Hale, A., et al. (2021). Muscle and tendon adaptations to moderate load eccentric vs. concentric resistance exercise in young and older males. GeroSci. 43, 1567–1584. doi: 10.1007/s11357-021-00396-0
Raman, J., MacDermid, J. C., and Grewal, R. (2012). Effectiveness of different methods of resistance exercises in lateral epicondylosis - a systematic review. J. Hand Ther. 25, 5–26. doi: 10.1016/j.jht.2011.09.001
Reeves, N. D., Maganaris, C. N., Longo, S., and Narici, M. V. (2009). Differential adaptations to eccentric versus conventional resistance training in older humans. Exp. Physiol. 94, 825–833. doi: 10.1113/expphysiol.2009.046599
Regnersgaard, S., Knudsen, A. K., Lindskov, F. O., Mratinkovic, M., Pressel, E., Ingersen, A., et al. (2021). Down stair walking: a simple method to increase muscle mass and performance in 65+ year healthy people. Eur. J. Sport Sci. 22, 279–288. doi: 10.1080/17461391.2020.1856936
Steiner, R., Meyer, K., Lippuner, K., Schmid, J. P., Saner, H., and Hoppeler, H. (2004). Eccentric endurance training in subjects with coronary artery disease: A novel exercise paradigm in cardiac rehabilitation? Eur. J. Appl. Physiol. 91, 572–578. doi: 10.1007/s00421-003-1000-6
Symons, T. B., Vandervoort, A. A., Rice, C. L., Overend, T. J., and Marsh, G. D. (2005). Effects of maximal isometric and isokinetic resistance training on strength and functional mobility in older adults. J. Gerontol. - Ser. A Biol. Sci. Med. Sci. 60, 777–781. Available online at: http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L40881186
Theodorou, A. A., Panayiotou, G., Paschalis, V., Nikolaidis, M. G., Kyparos, A., Mademli, L., et al. (2013). Stair descending exercise increases muscle strength in elderly males with chronic heart failure. BMC Res. Notes 6:87. doi: 10.1186/1756-0500-6-87
Keywords: elderly, sarcopenia, eccentric training, eccentric exercise, older adults
Citation: Čretnik K, Pleša J, Kozinc Ž, Löfler S and Šarabon N (2022) The Effect of Eccentric vs. Traditional Resistance Exercise on Muscle Strength, Body Composition, and Functional Performance in Older Adults: A Systematic Review With Meta-Analysis. Front. Sports Act. Living 4:873718. doi: 10.3389/fspor.2022.873718
Received: 11 February 2022; Accepted: 09 March 2022;
Published: 13 April 2022.
Edited by:
Rafael Reimann Baptista, Pontifical Catholic University of Rio Grande do Sul, BrazilReviewed by:
Masatoshi Nakamura, Niigata University of Health and Welfare, JapanPierre Clos, INSERM U1093 Cognition, Action et Plasticité Sensomotrice, France
Copyright © 2022 Čretnik, Pleša, Kozinc, Löfler and Šarabon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nejc Šarabon, bmVqYy5zYXJhYm9uQGZ2ei51cHIuc2k=