 Dustin Z. Nowaskie
Dustin Z. Nowaskie Dehandra Blackwood
Dehandra Blackwood Frank Garcia3‡
Frank Garcia3‡
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sociol. , 12 February 2025
Sec. Medical Sociology
Volume 10 - 2025 | https://doi.org/10.3389/fsoc.2025.1488888
This article is part of the Research Topic Navigating Equality: Addressing Stigma and Discrimination Against Sexual and Gender Minorities in Access to Gender-Affirming Healthcare View all 3 articles
Introduction: Historically, LGBTQ+ people have and continue to endure discrimination across many contexts, including healthcare. Research and data from nationwide samples in the United States regarding medical-related stigma experienced by LGBTQ+ people are scant.
Methods: A cross-sectional survey was distributed online to a national sample of United States residents. Participants answered questions about their healthcare, including experiences with medical-related gaslighting, trauma, and trust.
Results: Compared to cisgender and heterosexual people (n = 857), LGBTQ+ people (n = 815) reported significantly higher rates of medical-related gaslighting (46.5% vs. 26.5%, ORs 1.75–2.80) and trauma (18% vs. 8.9%, ORs 1.63–2.66). Likewise, LGBTQ+ people conveyed significantly less trust (ORs 0.46–0.53) in primary care providers (59.8% vs. 74.1%), medical specialists (56.5% vs. 71.7%), pharmaceutical companies (17% vs. 28%), insurance companies (15.9% vs. 29.3%), and U.S. healthcare systems (17.8% vs. 30.4%).
Discussion: Medical-related gaslighting, trauma, and distrust are pervasive systemic disparities among LGBTQ+ people. Addressing these challenges will require ongoing, lifelong motivation, dedication, and commitment for LGBTQ+ education, advocacy, and leadership to dismantle current prejudiced practices and foster more inclusive, supportive, affirming healthcare environments.
Medical gaslighting is a term that is used to describe when healthcare professionals minimize, dismiss, or outright ignore a patient’s concerns and symptoms (Sebring, 2021). While engaging in gaslighting, healthcare professionals may indicate that symptoms originated from various factors such as stress, anxiety, weight, and/or a person’s identity or lifestyle rather than attempting to conduct a more thorough examination. The term “gaslighting” is from a 1940 screenplay by Patrick Hamilton, which tells the story of a man who manipulates his wife into doubting her sanity, thereby gaslighting her (Klein, 2023). Since then, the term has been popularized to explain similar instances of mistreatment and neglect, often stemming from biases and prejudices. As a result, medical gaslighting functions as a method in which healthcare professionals may consciously and/or subconsciously perform implicit and explicit forms of discrimination against individuals who may already be marginalized by social, political, and medical systems.
The term “medical gaslighting” received much more attention and was widely used in connection with individuals who suffered from long coronavirus disease 19 (COVID-19) (Wise, 2022). These individuals continued to experience symptoms of the COVID-19 virus longer than what medical professionals initially assumed. Subsequently, these patients were met with doubt as a consensus was that the coronavirus should parallel influenza and subside in days. This skepticism and invalidation were notable barriers to care for these individuals, who then helped popularize the term medical gaslighting on social media to explain the injustices that they received from healthcare professionals (Wise, 2022).
Medical gaslighting echoes Miranda Fricker’s work (Fricker, 2007) on “epistemic injustice,” a term used to refer to a wrong done to someone specifically in their capacity as a knower. Fricker states there are two kinds of epistemic injustice: testimonial and hermeneutical. Testimonial injustice occurs when someone is ignored or not believed because of their sex, sexuality, gender, race, disability, etc. Meanwhile, hermeneutical injustice refers to having some significant area of one’s social experience obscured from collective understanding due to a general absence of the collective hermeneutical resource (Fricker, 2007). Examples of this injustice include the historical lack of regard for postpartum depression and sexual harassment because both concepts, until fairly recently, were not largely acknowledged or known by society. In the case of long-term COVID-19, individuals were often not believed, likely because of a general lack of understanding or recognition of what long COVID-19 truly is. Judith Butler’s theory of performativity can be used to analyze the doctor-patient relationship and power structure in medicine (Butler, 1988; Butler, 2004). In receiving a patient’s testimony, a provider performs the role of spokesperson for the institution of medicine and science, which has the privilege and power to pronounce what is real and what is not, operating from a hierarchical understanding of knowledge and perpetuating presumed norms (Sebring, 2021). Therefore, not only is the patient represented as inferior in the deceivingly mutual doctor-patient relationship (note the historical ranking of “doctor” and “patient” in this phrasing), but if the patient declares symptoms that cannot be explained by science, they must, via scientific reasoning, not be real. Medical gaslighting functions under this arrangement as it is not only influenced by societal power structures that often invalidate individuals likely due to their social positions, but it also survives due to a general lack of recognition and regard as well as novelty and operationalization of the concept and its reality.
The power structures that are performed in the doctor-patient relationship are often further influenced by a person’s social positioning in society. Many individuals who are women, people of color, gender diverse, sexually diverse, with disability, and whose bodies are otherwise perceived as abnormal or inferior under a medical gaze often lack cultural, economic, and social capital which makes them particularly at risk to many forms of injustices (Sebring, 2021). Sebring refers to these individuals as “bio-Others” and introduces this concept as an additional element to Foucault’s biopower, the mechanisms of power that govern people and populations (Foucault, 2008). Medical gaslighting is one component of biopower used to subjugate bio-Others. It disproportionately and naively places the responsibility for health issues on the individual by writing off health concerns as simply a consequence of one’s race, gender, or social location (Busfield, 2017; Sebring, 2021). For example, common medical gaslighting behaviors include attributing patients’ symptoms solely to stress, poor nutrition, mental health, lack of exercise, and/or weight rather than conducting more thorough examinations (Durbhakula and Fortin, 2023). Furthermore, bio-Others such as lesbian, gay, bisexual, transgender, queer, and all sexually diverse and gender diverse (LGBTQ+) individuals especially are more likely to have their symptoms dismissed without full, comprehensive examinations (Wise, 2022).
Research and data from nationwide samples in the United States (U.S.) regarding medical-related stigma experienced by LGBTQ+ people are scant. As such, the primary goals of this study were to understand LGBTQ+ patients’ healthcare experiences and elucidate pervasive systemic disparities. Specifically, this study aimed to highlight the presence of medical-related gaslighting as a form of discrimination, overt medical-related traumas, and levels of distrust in healthcare providers and systems within the United States. Through identification, documentation, and discussion of these systemic disparities, this study hoped to educate and subsequently improve the affirmation of healthcare professionals and systems in order to foster safer, more trusting patient-doctor relationships and promote LGBTQ+ health and well-being.
In March 2023, an anonymous, self-report, cross-sectional survey was distributed online via a third-party vendor to a national sample of 2,600 U.S. residents. This work was undertaken through a partnership between OutCare Health (Nowaskie, 2021) and Healthgrades to amplify the healthcare experiences of LGBTQ+ people as well as promote LGBTQ+ affirming care.
Participation was voluntary and constituted consent. Participants self-disclosed their age, sexual orientation, gender identity, race/ethnicity, education, employment, household income, relationship status, household size, parenting status, and region of residence. Participants also answered questions about their healthcare experiences. This data was provided by Healthgrades, who commissioned the survey, to the corresponding author. Because data was deidentified, this study was deemed not human subjects research by the University of Southern California Institutional Review Board (Protocol #UP-24-00660).
For simplification of reporting, the variables education, employment, household income, relationship status, household size, and parenting status were categorized into groups. Participants were categorized into two groups based on their sexual orientation and gender identity: (1) LGBTQ+ people (N = 1,200) and (2) exclusively cisgender and heterosexual people (N = 1,400). Participants were then weighted to be nationally representative of the general U.S. population based on age, gender identity, race/ethnicity, and region of residence. Frequencies of demographic and healthcare experience questions were computed. Overall frequencies of any experience of medical-related gaslighting and trauma were also computed. Odds ratios were calculated to compare healthcare experiences between LGBTQ+ people and cisgender and heterosexual people. Given the survey length, question magnitude, and focus of this manuscript, items related to medical-related gaslighting, trauma, and distrust are reported here.
Additionally, it is well known that many demographic variables, including age, race/ethnicity, education, employment, individual annual income, and state of residence, may influence health outcomes. To avoid difficult interpretations due to analytical complexity, comparative analyses reported here are based solely on sexual orientation and gender identity, i.e., LGBTQ+ people compared to cisgender and heterosexual people.
Many LGBTQ+ people (n = 891) and cisgender and heterosexual people (n = 980) expressed their perspectives and voices (Table 1). After weighting, a representative sample of LGBTQ+ people (n = 815) and cisgender and heterosexual people (n = 857) were analyzed. More than half of LGBTQ+ people were between 18 to 34 years old, White/Caucasian, had higher education, employed, earned between $25,000–$100,000 annually, lived in a household of at least three people, and did not have children; nearly half of LGBTQ+ people were partnered; and they lived across the U.S.
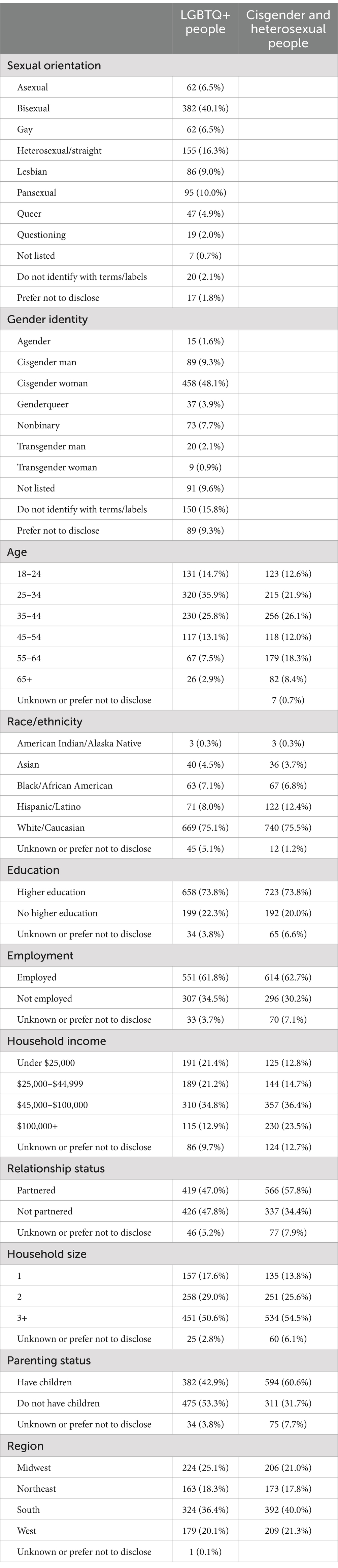
Table 1. Demographics.
Overall, significantly more LGBTQ+ people reported experiencing medical-related gaslighting (46.5% vs. 26.5%, ORs 1.75–2.80) and trauma (18% vs. 8.9%, ORs 1.63–2.66) than cisgender and heterosexual people (Table 2). Nearly half of LGBTQ+ people conveyed undergoing medical-related gaslighting by their providers. Individual items showed that compared to cisgender and heterosexual people, significantly more LGBTQ+ people felt dismissed, minimized, and ignored. Likewise, nearly one-fifth of LGBTQ+ people described enduring trauma, including emotional and physical traumas, at a multitude higher rate than cisgender and heterosexual people. Additionally, significantly less LGBTQ+ people (ORs 0.46–0.53) reported trusting primary care providers (59.8% vs. 74.1%), medical specialists (56.5% vs. 71.7%), pharmaceutical companies (17% vs. 28%), insurance companies (15.9% vs. 29.3%), and U.S. healthcare systems (17.8% vs. 30.4%) than cisgender and heterosexual people. Slightly more than half of LGBTQ+ people disclosed that they trusted individual providers, while less than one-fifth stated that they trusted larger healthcare systems.
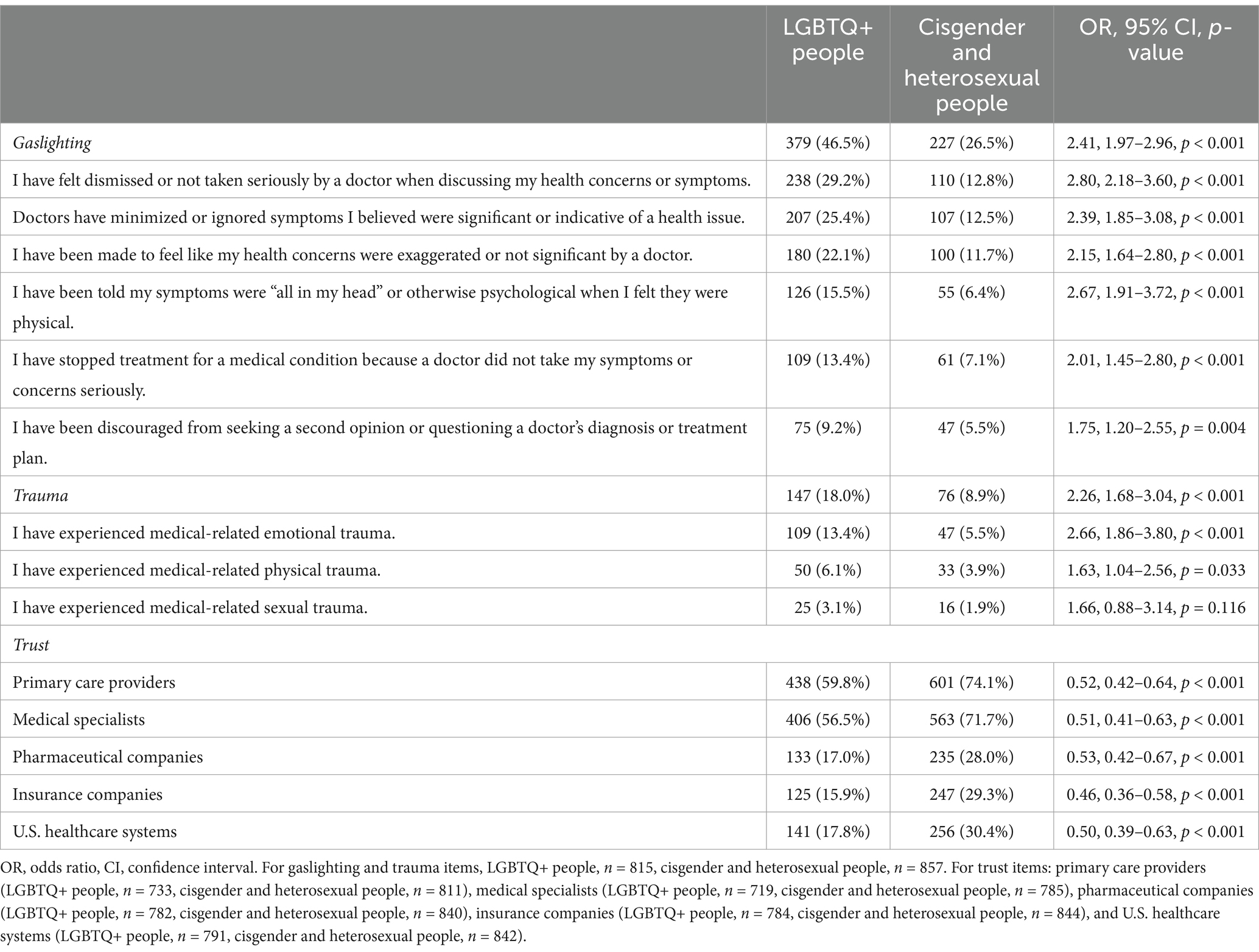
Table 2. Healthcare experiences.
The goal of this study was to examine medical-related gaslighting, trauma, and distrust among LGBTQ+ people. Overall, compared to cisgender and heterosexual people, LGBTQ+ people reported higher rates of medical-related gaslighting and trauma. Likewise, LGBTQ+ people conveyed less trust in healthcare providers and systems. These findings mirror existing literature that demonstrates that discrimination is widely experienced by LGBTQ+ people within healthcare (Casey et al., 2019).
Since the institutionalization—and subsequent power differentials—of healthcare, communities composed of marginalized identities have experienced increasing levels of stigma, discrimination, and iatrogenesis (Atuk, 2024). Iatrogenesis is chronic and pervasive harm, often originating from individual healthcare providers and staff themselves as well as systems at large. Individuals who identify as LGBTQ+ have historically had polarizing, iatrogenic relationships within healthcare. Gaslighting is one of many forms of ubiquitous medical-related harm and violence experienced by LGBTQ+ people. For example, during the initial discovery of human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS) in the 1980s, the disease was originally and commonly referred to as “Gay-Related Immune Deficiency” (Ayala and Spieldenner, 2021). This label fostered a false correlation between sexually diverse people and the virus, which led to discrimination and neglect as individuals with HIV/AIDS struggled to find medical care and faced medical gaslighting and victimization at the hands of medical professionals. Today, LGBTQ+ individuals often face significant health disparities such as increased rates of sexually transmitted infections, mental health conditions, substance use, and suicide (Lund and Burgess, 2021). These health disparities are strongly associated with direct and indirect consequences of oppression, prejudice, discrimination, and violence that LGBTQ+ people often face. This phenomenon that sociological aspects of a person’s life and experiences are directly linked to one’s health outcomes was eventually conceptualized and popularized in the minority stress model (Meyer, 2003). Minority stress refers to the additional stressors that individuals encounter as a direct result of their identification and association within marginalized groups (Lund and Burgess, 2021; Meyer, 2003). The model outlines two categories of minority stress: proximal stressors and distal stressors. Proximal stressors refer to internal experiences and stress related to self-concealment of sexual orientation, such as internalized homophobia. On the other hand, distal stressors refer to external negative experiences related to sexual orientation and gender identity including harassment, violence, and discrimination. Both types of processes lead to chronic stress, which over time can manifest as physical and mental health conditions (Meyer, 2003).
Utilizing a minority stress framework (Meyer, 2003), distal stressors such as gaslighting and trauma by healthcare providers and systems likely induces proximal stressors such as internal stress, poor self-esteem, and distrust within LGBTQ+ patients. Due to substantial lack of LGBTQ+ awareness, education, and training (Nowaskie, 2021), cissexism, cisgenderism, cisnormativity, and heterosexism are promoted throughout entire healthcare journeys, from start to finish. Many healthcare providers and systems do not obtain sexual orientation and gender identity information nor screen for or treat unique LGBTQ+ health risks and disparities (Lund and Burgess, 2021). Likewise, similar to the disparities of trauma documented in this study, overt violence from healthcare providers and staff can occur, as gender diverse people are four times more likely than cisgender people to experience victimization (Flores et al., 2021). Additionally, nearly one-third of gender diverse people report enduring at least one negative experience from their healthcare provider, such as verbal harassment or refusal of treatment, because of their identity. Moreover, these discriminatory forces continue to produce, perpetuate, and exacerbate health disparities (Ramos, 2021). These pervasive, vicious cycles of medical-related discrimination may then lead many LGBTQ+ people to avoid healthcare altogether due to anticipated stigma, fear, and distrust in providers and systems (Bullock, 2023; Casey et al., 2019; James et al., 2016). For example, due to verbal and physical harassment within healthcare, LGBTQ+ people may forego their care and obtain unregulated or even illegal forms of care such as hormones and surgical procedures (Chong et al., 2021). Because of this overt discrimination, it is not surprising that in this study, only half of LGBTQ+ people reported trusting providers and less than one-fifth conveyed trusting healthcare systems.
While this data offers cross-sectional insight into the current state of medical-related gaslighting, trauma, and distrust, it is descriptive of a point in time of the current stigma from and within particular contexts (i.e., providers and systems). Healthcare journeys involve many more staff and contexts than this data examined. Consequently, further considerations of medical-related gaslighting, trauma, and distrust from various healthcare professionals and staff and within specific teams, groups, departments, and communities are necessary. Additionally, this data does not account for the impact of social and political discriminations within healthcare. For example, past and current socio-politico-medico systemic and structural marginalizations, such as anti-LGBTQ+ proposals and laws, likely worsen medical-related gaslighting, trauma, and distrust and prevent their alleviation. Explorations into these complexities are paramount and will likely yield solutions-focused approaches for progress and affirmation.
While insufficient education, training, and affirmation among healthcare providers and systems are likely fundamental barriers to alleviating medical-related gaslighting, trauma, and distrust, such shortcomings can be targeted by advocacy, online resources, and organizations. For example, OutCare Health, an international nonprofit LGBTQ+ health equity organization, promotes affirming healthcare by educating current and future healthcare providers and systems (Nowaskie, 2021; Nowaskie and Garrison, 2024). Through multidisciplinary and multidimensional approaches, OutCare Health supports LGBTQ+ and healthcare communities worldwide with comprehensive information, resources, support, and education (Nowaskie, 2021; Nowaskie and Garrison, 2024; Nowaskie et al., 2024; Patel and Nowaskie, 2023).
There were notable study limitations. Although many demographic variables were collected in the survey, comparisons related to intersectionality were not undertaken. Rather, while acknowledging the multitude of diversity within LGBTQ+ populations, these data nonetheless present a homogenized perspective. Given the amount of data collected, it is appreciated that many various analyses incorporating several demographic variables could have been undertaken, reported, and interpreted in a myriad of ways, including investigations across specific sexual orientations and gender identities. Further comparative explorations, e.g., with LGBTQ+ subgroups such as gender diverse identities and LGBTQ+ people of color, are strongly encouraged to understand the similarities and differences in healthcare experiences among these groups.
Medical-related gaslighting, trauma, and distrust are pervasive systemic disparities among LGBTQ+ people. These forms of discrimination create significant barriers for equitable care for LGBTQ+ communities. Addressing these challenges will require ongoing, lifelong motivation, dedication, and commitment for LGBTQ+ education, advocacy, and leadership to dismantle current prejudiced practices and foster more inclusive, supportive, affirming healthcare environments.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by University of Southern California Institutional Review Board (Protocol #UP-24-00660). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
DN: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. DB: Writing – original draft, Writing – review & editing. FG: Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This article was funded by OutCare Health.
The authors would like to thank Healthgrades for commissioning the survey used in this study. The authors would also like to thank OutCare Health for supporting publication costs.
The author DN is the Founder and President of an organization referenced in this paper, OutCare Health, which is a nonprofit, 501(c)(3) LGBTQ+ health equity organization.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Atuk, T. (2024). “If I knew you were a travesti, I wouldn’t have touched you”: iatrogenic violence and trans necropolitics in Turkey. Soc. Sci. Med. 345:116693. doi: 10.1016/j.socscimed.2024.116693
Ayala, G., and Spieldenner, A. (2021). HIV is a story first written on the bodies of gay and bisexual men. Am. J. Public Health 111, 1240–1242. doi: 10.2105/AJPH.2021.306348
Bullock, C. G. (2023). Experiencing “epistemic injustice” within transgender healthcare. Sex. Gend. Policy 6, 47–50. doi: 10.1002/sgp2.12059
Busfield, J. (2017). The concept of medicalisation reassessed. Sociol. Health Illn. 39, 759–774. doi: 10.1111/1467-9566.12538
Butler, J. (1988). Performative acts and gender constitution: an essay in phenomenology and feminist theory. Theatre J. 40, 519–531. doi: 10.2307/3207893
Casey, L. S., Reisner, S. L., Findling, M. G., Blendon, R. J., Benson, J. M., Sayde, J. M., et al. (2019). Discrimination in the United States: experiences of lesbian, gay, bisexual, transgender, and queer Americans. Health Serv. Res. 54, 1454–1466. doi: 10.1111/1475-6773.13229
Chong, L. S., Kerklaan, J., Clarke, S., Kohn, M., Baumgart, A., Guha, C., et al. (2021). Experiences and perspectives of transgender youths in accessing health care. JAMA Pediatr. 175:1159. doi: 10.1001/jamapediatrics.2021.2061
Durbhakula, S., and Fortin, A. H. (2023). Turning down the flame on medical gaslighting. J. Gen. Intern. Med. 38, 3426–3427. doi: 10.1007/s11606-023-08302-4
Flores, A. R., Meyer, I. H., Langton, L., and Herman, J. L. (2021). Gender identity disparities in criminal victimization: national crime victimization survey, 2017–2018. Am. J. Public Health 111, 726–729. doi: 10.2105/AJPH.2020.306099
Fricker, M. (2007). Epistemic injustice: power and the ethics of knowing. New York, NY, United States: Oxford University Press.
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., and Anafi, M. (2016). The report of the 2015 U.S. transgender survey. Washington, DC: National Center for Transgender Equality.
Klein, W. (2023). A qualitative analysis of gaslighting in romantic relationships. Pers. Relatsh. 30, 1316–1340. doi: 10.1111/pere.12510
Lund, E. M., and Burgess, C. M. (2021). Sexual and gender minority health care disparities. Prim. Care 48, 179–189. doi: 10.1016/j.pop.2021.02.007
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol. Bull. 129, 674–697. doi: 10.1037/0033-2909.129.5.674
Nowaskie, D. Z. (2021). Development, implementation, and effectiveness of a self-sustaining, web-based LGBTQ+ national platform: a framework for centralizing local health care resources and culturally competent providers. JMIR Form. Res. 5:e17913. doi: 10.2196/17913
Nowaskie, D. Z., and Garrison, S. D. (2024). International solutions for continual gaps in LGBTQ+ education and exposure. J. Community Health 49, 951–953. doi: 10.1007/s10900-024-01384-z
Nowaskie, D. Z., Werner-Sleva, S. B., and Jacobs, A. K. (2024). It’s a start: an online, on-demand LGBTQ+ mental health training session for providers nationwide. Psychiatr. Serv. 75, 481–484. doi: 10.1176/appi.ps.20220473
Patel, A. U., and Nowaskie, D. Z. (2023). Affirmation of LGBTQ+ healthcare providers: a dynamic process, requiring ongoing education and training. J. Gay Lesbian Ment. Health 28, 415–423. doi: 10.1080/19359705.2023.2197848
Ramos, N. (2021). Medical trauma in LGBTQIA youth: adapting trauma-informed affirming clinical practices. Pediatr. Ann. 50, e379–e383. doi: 10.3928/19382359-20210818-02
Sebring, J. C. (2021). Towards a sociological understanding of medical gaslighting in western health care. Sociol. Health Illn. 43, 1951–1964. doi: 10.1111/1467-9566.13367
Keywords: gaslighting, LGBTQ+, pharma, provider, trauma, trust
Citation: Nowaskie DZ, Blackwood D and Garcia F (2025) Pervasive systemic disparities: medical-related gaslighting, trauma, and distrust among LGBTQ+ people in the United States. Front. Sociol. 10:1488888. doi: 10.3389/fsoc.2025.1488888
Edited by:
Foteini Tzavella, University of Peloponnese, GreeceReviewed by:
Tankut Atuk, Rensselaer Polytechnic Institute, United StatesCopyright © 2025 Nowaskie, Blackwood and Garcia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dustin Z. Nowaskie, ZHVzdGluLm5vd2Fza2llQG1lZC51c2MuZWR1
†These authors have contributed equally to this work and share first authorship
‡ORCID: Dustin Z. Nowaskie, https://orcid.org/0000-0003-1111-8357
Dehandra Blackwood, http://orcid.org/0009-0002-9949-7311
Frank Garcia, http://orcid.org/0009-0005-5891-0319
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.