 Elena Rubini1*
Elena Rubini1* Monica Trentin1,2
Monica Trentin1,2 Martina Valente1,3
Martina Valente1,3 Stefano Cenati4,5Antonella Canavese6,7Paola Castagna6
Stefano Cenati4,5Antonella Canavese6,7Paola Castagna6 Luca Ragazzoni1,3
Luca Ragazzoni1,3 Sarah Gino4,8
Sarah Gino4,8- 1CRIMEDIM—Center for Research and Training in Disaster Medicine, Humanitarian Aid and Global Health, Università del Piemonte Orientale, Novara, Italy
- 2Department of Translational Medicine, Università del Piemonte Orientale, Novara, Italy
- 3Department for Sustainable Development and Ecological Transition, Università del Piemonte Orientale, Vercelli, Italy
- 4Department of Health Sciences, Università del Piemonte Orientale, Novara, Italy
- 5Emergency Department, Azienda Socio-Sanitaria Territoriale della Valle Olona, Busto Arsizio (Varese), Italy
- 6Centro Soccorso Violenza Sessuale, Presidio Ospedaliero Sant’Anna, Città della Salute e della Scienza, Torino, Italy
- 7Department of Surgical Sciences, University of Turin, Torino, Italy
- 8Direzione Medica dei Presidi Ospedalieri, AOU Maggiore della Carità, Novara, Italy
Introduction: The Sexual Violence Relief center Soccorso Violenza Sessuale (SVS) is a specialist service, situated in Sant’Anna Hospital, an Obstetrics and Gynecology facility in Turin, North-West Italy. The study aimed to qualitatively analyze the transcripts of interviews routinely conducted by gynecologist and midwife in the first part of the medical examination of migrant patients accessing care at SVS after being subjected to conflict-related sexual violence (CRSV) in their home country or during migration and to explore the adverse outcomes of such violence on their health.
Methods: Interview transcripts were purposely selected to include adult migrant patients (age > 18) subjected to CRSV in the different phases of migration and accessing SVS from January 1st, 2014, to September 4th, 2023. Data was extracted from the SVS archive, anonymized, and thematically analyzed.
Results and discussion: In total, 43 interview transcripts were eligible for inclusion. All of them were related to cisgender women of Sub-Saharan origin describing different forms of violence as a driver for migration. CRSV was disclosed by 18 survivors as occurring in their home country and by 31 in transit (e.g., Libya), the most reported type being rape. 49% of the patients described adverse physical outcomes of CRSV, while 72% reported psychological sequelae. The findings confirm high levels and different modalities of violence throughout the migratory route. Qualitative analysis of interview transcripts served as a valuable source for understanding how survivors described the CRSV they endured, its consequences, as well as other violence encountered during migration.
1 Introduction
Conflicts put individuals at risk of different forms of human rights violations, including gender-based violence (GBV), namely “any harmful act perpetrated against a person’s will and based on socially determined gendered roles” (IASC Task Force on Gender and Humanitarian, Assistance, 2005). Conflict-related sexual violence (CRSV) is a specific form of GBV temporally, geographically, or causally connected to a conflict (Preventing Sexual Violence in Conflict Initiative, 2017), a violation of the Sexual and Reproductive Health and Rights (SRHRs) of individuals (Starrs et al., 2018), and a public and global health issue (Heise et al., 1994; Öhman et al., 2020; Sanjel, 2015; WHO, 2002, 2003). GBV, including CRSV, disproportionately affects women and girls (IASC Task Force on Gender and Humanitarian, Assistance, 2005; Pertek and Phillimore, 2022), with 94% of the 2,455 reported cases of CRSV in 2022 affecting these groups (UN, 2022).
The concept of “continuum of violence” traces back to the work of Kelly, who used this expression to highlight the interconnections occurring between different forms of violence and warned against making a distinction between criminal acts and “minor” episodes of GBV (Kelly, 1988). It has been employed also to describe the continuity of violence between the private and public sphere (Gray, 2019; Swaine, 2015) as well as that occurring in times of peace and of conflict (Cockburn, 2004).
For these reasons, conflicts as well as the different forms of violence perpetrated against civilians and other actors should not be understood as punctual events, but rather as a continuum of violence, extending in space and time through flight and displacement (Ferris, 1990; Krause, 2015). Violence affecting migrants must be understood in its structural dimension as deriving from the inequalities and discrimination faced by individuals based on different and intersecting identities (e.g., related to gender, race, ethnic origin, socioeconomic status, legal status), which are instrumentalized against migrants by different institutional actors directly or by failure to protect them from abuse or to support them after its occurrence (Crenshaw, 1989; Davies and True, 2015; Nixon, 2019; Simon-Butler and Mcsherry, 2019; Tastsoglou et al., 2021; Trentin et al., 2024). Research focusing on specific types of GBV in conflict, including CRSV, should equally describe other co-occurring types of abuse, to avoid a hierarchization of violence as well as to understand the cumulative effect of various forms of abuse (Menjívar and Perreira, 2019; Swaine, 2015). Moreover, in contrast to research that solely focused on CRSV used as a weapon of war (e.g., perpetrated by armed actors in a conflict-affected home country), literature is now shifting its attention to other kinds of perpetrators (e.g., smugglers, police, paramilitaries) and geographical locations (e.g., transit countries; Hourani et al., 2021; IOM, 2019; Reques et al., 2020). This encompasses the emerging research focusing on migrants affected by conflict in the different phases of their migratory journey and describing the various forms of violence, including GBV, they experience (Borges, 2024; Hourani et al., 2021; Phillimore et al., 2023; Rubini et al., 2023; Tan and Kuschminder, 2022). As for what concerns migrant women in transit, sexual violence and other types of GBV have been documented in the literature in the Mediterranean Routes and especially through Libya (Amnesty International, 2020; Malakooti, 2019; Reques et al., 2020), as well as in the route Latin America—Mexico—USA (e.g., Mexican migration corridor; Cleaveland and Kirsch, 2020; Infante et al., 2020; Obinna, 2021; Pries et al., 2024; Soria-Escalante et al., 2022). These can take various forms, from rape, to other types of sexual violence, transactional sex, sexual trafficking, up to the point of femicide (Soria-Escalante et al., 2022).
Conflict, violence, GBV, and CRSV can act as drivers for resettling or can occur or be reiterated in the different phases of the migratory route (Morgen, 2013; Pertek and Phillimore, 2022; Pries et al., 2024; WHO, 2022). CRSV provokes negative consequences on the physical, psychological, and social dimensions of health of victims (Rubini et al., 2023; Starrs et al., 2018; WHO, 2002), which may be exacerbated by delayed access to care due to the weakening or the disruption of health systems occurring in conflict-affected settings; for some migrant survivors access to care may occur after a longer time span in transit or host countries, often hindered by restrictive health policies (Acquadro-Pacera, 2024; Castagna et al., 2018; Footer and Rubenstein, 2013; IASC Task Force on Gender and Humanitarian, Assistance, 2005; IOM, 2006; Spitzer et al., 2019). Moreover, the exposure to abuse and violence in the different phases of migration, the possibility to use legal or illegal routes, as well as their safety, equally influence migrants’ health (IOM, 2006).
The Council of Europe Convention on preventing and combating violence against women and domestic violence (e.g., Istanbul Convention) establishes that cases of GBV should be managed by general [e.g., Emergency Departments (EDs)] and specialist services (Council of Europe, 2018, 2011a, 2011b). Specialist support services aim to ensure the empowerment of survivors through allocation of high-quality support and assistance through different forms of provision (e.g., shelters, telephone helplines, counselling centers, support for victims of sexual violence; Council of Europe, 2018, 2011a, 2011b). Among the latter are sexual violence referral or relief centers, which can be managed by non-governmental organizations (NGOs; e.g., anti-violence centers) or by government authorities (Council of Europe, 2018). Anti-violence centers operate with a multi-agency perspective by providing support to survivors of GBV, including referral to the ED.
In Italy, the Ministry of Health adopted in 2017 guidelines for the promotion of an integrated and multidisciplinary approach (e.g., socio-sanitary, legal, and cultural mediation needs) in the management of refugees or individuals with subsidiary protection victims of torture, rape, or other forms of physical, psychological, or sexual violence, also highlighting the role of the medico-legal report in documenting the abuses they endured (Ministero della Salute, 2017).
In Italy, the Soccorso Violenza Sessuale (SVS) at Sant’Anna Hospital in Turin and Soccorso Violenza Sessuale e Domestica (SVSeD) at Mangiagalli Clinic in Milan, are both situated in two public hospitals in the North-West region. In particular, SVS created a dedicated healthcare pathway for migrant survivors of GBV, including CRSV, regardless of their legal status. Italy is a transit and destination country for migrants, and, even though no exact figures are available, we can presume by using their home countries as a proxy that conflict constitute the reason for fleeing for many of them (Fondazione ISMU, 2023). In specialist centers, the transcript of patients’ interviews on their history of violence, which constitutes the first phase of the medical examination, consists of a detailed report, useful for the clinical and forensic management of cases. To our knowledge, the two specialist centers only published quantitative studies focusing on epidemiological and clinical findings retrieved from databases and medical records concerning the top-to-toe and gynecological examination (Castagna et al., 2018; Gino et al., 2017; Margherita et al., 2021; Simonaggio et al., 2024). Even though this data allows us to understand the epidemiological characteristics of their pool of users, subjective elements emerging through patients’ interviews, which are crucial for health providers to contextualize the episodes of violence suffered by victims of GBV, have never been investigated.
Our research team previously conducted a systematic literature review analyzing qualitative peer-reviewed evidence of CRSV, with an inclusive operational definition encompassing also abuses occurring during migration, as well as describing other types of co-occurring violence (Rubini et al., 2023). We also conducted another systematic review, on the health sequelae of CRSV documented during forensic medical examination, which showed that studies on this matter are generally conducted in high income destination countries (Rubini et al., 2024). In this study we relied on original data to investigate the health outcomes of CRSV, thus complementing the findings of our previous secondary data analyses.
The aims of this study are to qualitatively examine episodes of CRSV endured by migrant women as disclosed by them during admission at SVS of Sant’Anna Hospital in Turin, North-West Italy, including the adverse outcomes on their health, and to investigate how CRSV affected women over the different phases of migration.
The research was guided by the questions “How do migrant women survivors of CRSV describe their history of violence during admission at the SVS of Sant’Anna Hospital in Turin?” and “How did CRSV affect them during the different phases of migration?.” Giving an answer to these questions will contribute to understanding how episodes of CRSV are depicted by victims at access to care and will serve to document what kind of CRSV was endured by migrant women patients of SVS in their home and transit countries.
2 Methods
A retrospective qualitative analysis of the transcripts of interviews conducted prior to medical examination was performed to capture how victims of CRSV reported their history of assault at the time of accessing care at SVS and the negative consequences of such violence described by them.
2.1 Study setting
In the metropolitan area of Turin, North-West Italy, half of the migrant population among those who have a permit to stay is female (Ministero del lavoro e delle politiche sociali, 2021). The most recent data available showed that among those who have this permit, 11.3% are under some form of protection (Ministero del lavoro e delle politiche sociali, 2021). Namely, 51.5% of them are refugees or asylum seekers, 32.7% have subsidiary protection, and 15.7% have humanitarian protection (Ministero del lavoro e delle politiche sociali, 2021).
Since May 2003, SVS is one of the two specialized centers in Italy offering free assistance, 24/7, to women of 14 years of age or older subjected to different forms of GBV. The service is situated in the ED of Sant’Anna Hospital, an Obstetrics and Gynecology facility in Turin. It provides clinical, forensic, psychological, legal, and social support to survivors in the immediate aftermath of abuse and in the longer period, with a 3 months follow up after the first admission. Gynecologists, obstetric nurses, psychologists, cultural mediators, and social assistants manage in a multidisciplinary perspective the needs of survivors. Access to SVS can occur through the ED, scheduled appointment, referral from other facilities in the metropolitan area of Turin, as well as from public or private third sector organizations operating in the same territory (e.g., anti-violence centers, anti-trafficking networks, migrant shelters, and reception centers). Third sector organizations working with migrant women serve as a contact point between them and SVS, thus integrating the management of their needs as migrants and as survivors of GBV. SVS does not operate in direct contact with border services for migrant women victims of violence, but indirectly through the mediation of third sector organizations working in the migrant reception system as well as in other areas (e.g., GBV, sexual trafficking). After collection of the history of assault and informed consent, the top-to-toe examination is conducted, together with the collection of biological material for forensic genetics and toxicology analyses, clinical screening for STI, and pregnancy test. Consultations take 5 h on average. With a patient-centered, as well as a culturally, trauma, and gender sensitive approach, the service cares for and holistically cures about 100 patients per year.
2.2 Data collection, screening, and eligibility criteria
This study qualitatively analyzed the transcripts of the interviews of patients accessing SVS routinely conducted by gynecologist and midwife, with the presence of a cultural mediator, in the first part of the medical examination.
At times, details on symptoms and signs connected to psychological sequelae were also described. Text fragments from the medical records were translated for publication purposes from Italian into English and added to the Results section to enhance the understanding of the study findings.
Interview transcripts were purposely selected to include adult migrant patients (age > 18) subjected to non-partner violence (NPV) in their home country or during migration (see “Operational definitions”) and who accessed care at SVS from January 1st, 2014, to September 4th, 2023. This initial screening was performed by one of the research team members (AC) who works as a midwife in the facility. To ensure compliance with eligibility criteria, a second screening was performed (ER, MT). Histories of violence that did not describe episodes of sexual violence, and those not mentioning conflict in any of the phases of migration were excluded, together with accounts where it was not possible to understand whether violence was related to conflict or who the perpetrators were. The interviews whose transcripts were considered eligible for inclusion were extracted from the SVS archive, anonymized, and transferred to a Word file for qualitative analysis.
2.3 Data analysis
Thematic data analysis was used (Braun and Clarke, 2006). Researchers familiarized with data by actively reading accounts multiple times. A coding table was created (Additional file 1) with the aim to capture information on conflict, survivors’ demographics, CRSV and its consequences, as well as other experiences of violence and GBV, and migration. To ensure coding accuracy and consistency, each code was given an explicit definition and precise instructions. Interview transcripts were transferred on software Atlas.ti [version 23.4.0.29360]. Coding was performed by two investigators (ER, MT) in the months of October and November 2023. The codes were then inductively organized into patterns and themes.
2.4 Operational definitions
For the purpose of the present study, CRSV was understood as “temporally, geographically, or causally” related to conflict (Preventing Sexual Violence in Conflict Initiative, 2017; UN Security Council, 2023). Not only CRSV endured in the home country and possibly provoking displacement and episodes of re-victimization was included, but also CRSV in conflict-affected transit countries, also considering individuals who migrate due to non-conflict related reasons.
Conflict encompasses the International Humanitarian Law definitions of international and non-international armed conflict (ICRC, 2008), but also persecution (MSF, n.d.), political violence (Balcells, 2015; Kalyvas, 2001), violence due to cults (EASO, 2021), terrorism (Sinai, 2008; Teichman, 1989), and gang violence (Applebaum and Mawby, n.d.; Rodríguez Serna, 2016) when not contrasted by State authority. As for what concerns Libya, we understand this State in the Maghreb region of North Africa as conflict-affected by civil war in the years 2011–2021, and up to the present day as under the control of different armed groups and militias (Non-international armed conflicts in Libya, 2022; US Department of State, Office to monitor and combat trafficking in persons, n.d.). Data related to Libya was collected when hostilities were directly mentioned or when specific terms were used (e.g., militia men, rebels, men in military uniforms, policemen, detention centers or prisons, Asma Boys).
The terms “survivor” and “victim” will be used interchangeably to refer to individuals subjected to SV; the first term serves to highlight the process of recovery, while the second calls attention to the criminal nature and the severity of acts of GBV (Rubini et al., 2023).
“Migrant” is intended as an umbrella term to refer to individuals who move away from their place of usual residence for a variety of reasons (IOM, n.d.).
2.5 Ethics
The study was approved by the Ethics Committee of the AOU Città della Salute e della Scienza di Torino—AO Ordine Mauriziano di Torino (CE 112/2020) and complies with the Declaration of Helsinki for experiments involving humans (2013), to the General Data Protection Regulation (2018), and to the Provision no. 146/2019 of the Italian Privacy Guarantor. For information about consent to participate, please see the Informed Consent Statement.
3 Results
In total, 43 interview transcripts were eligible for inclusion. Other 44 were excluded since they did not describe episodes of CRSV. This section will explore the demographic characteristics as well as conflict and migratory experience of survivors, including the reason for fleeing their home country, the CRSV sustained, the adverse outcomes of CRSV on their health, as well as other violence endured (e.g., conflict- and migration-related nonsexual violence and other GBV).
3.1 Characteristics of survivors
All 43 patients in our sample were cisgender women of Sub-Saharan origin living in Italy at the time of accessing SVS. When seeking care, their self-reported age ranged from 19 to 48, with the median age being 31. Among them, 20 were mothers, and only 5 fled with their children.
Means of livelihood in home or transit countries were mentioned only by 15 patients. While two survivors were, respectively, a social educator and a nurse, most women had informal jobs. They were housemaids (n = 7), street sellers (n = 5), hairdressers (n = 2), babysitters (n = 1), farmers (n = 1), dishwashers (n = 1), caregivers (n = 1), or sex workers (n = 1).
3.2 Migratory experience
For 37 women (86%) Libya was the last disclosed transit country before arrival in Italy. Figure 1 provides a map of the migratory route as described by survivors accessing care at SVS.
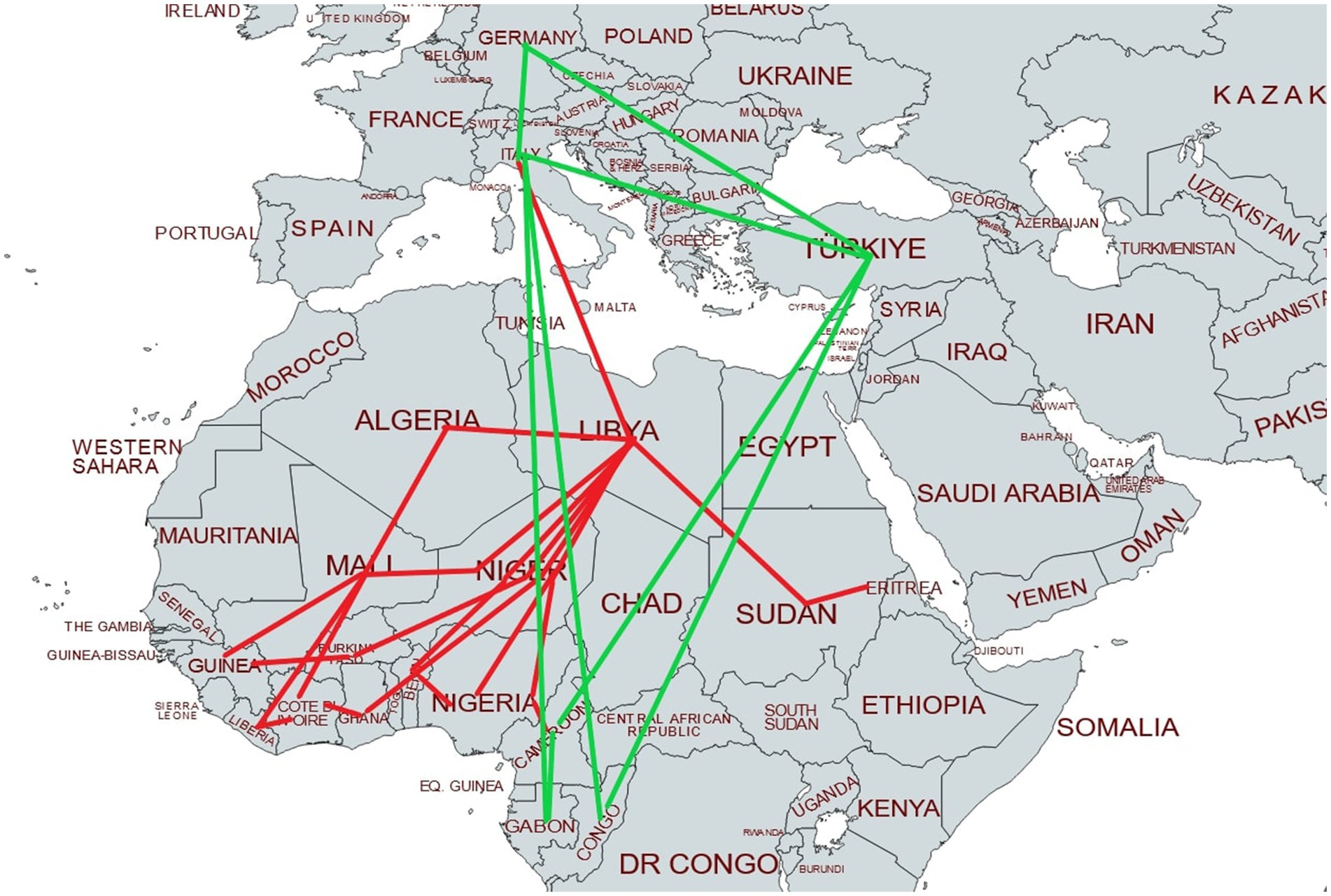
Figure 1. Migratory route of survivors accessing care at SVS. Please note that it represents only the journey of patients who described all phases of migration. A green line represents travel by plane, while a red line stands for other means of transport (e.g., car, bus, taxi, van, and pick up).
When mentioned, migrant women whose last transit country was Libya reported means of transportation used to arrive in Italy were “boats” (n = 20) or “rubber boats” (n = 7). A small number of survivors described traveling by plane (n = 4, 9%) directly from their home country (Congo, n = 2), or from transit countries (Gabon and Türkiye, n = 1 each).
Information on year of admission at SVS and home country can be found in Table 1 (Additional file 2).

Table 1. Characteristics of the pool of users of SVS survivors of CRSV.
3.3 Conflict in home and transit country
Information on the country where survivors encountered hostilities, type of conflict, and number of survivors who reported it can be found in Table 2. Conflict was described as occurring in their home countries by 25 patients, while 31 encountered hostilities in Libya.
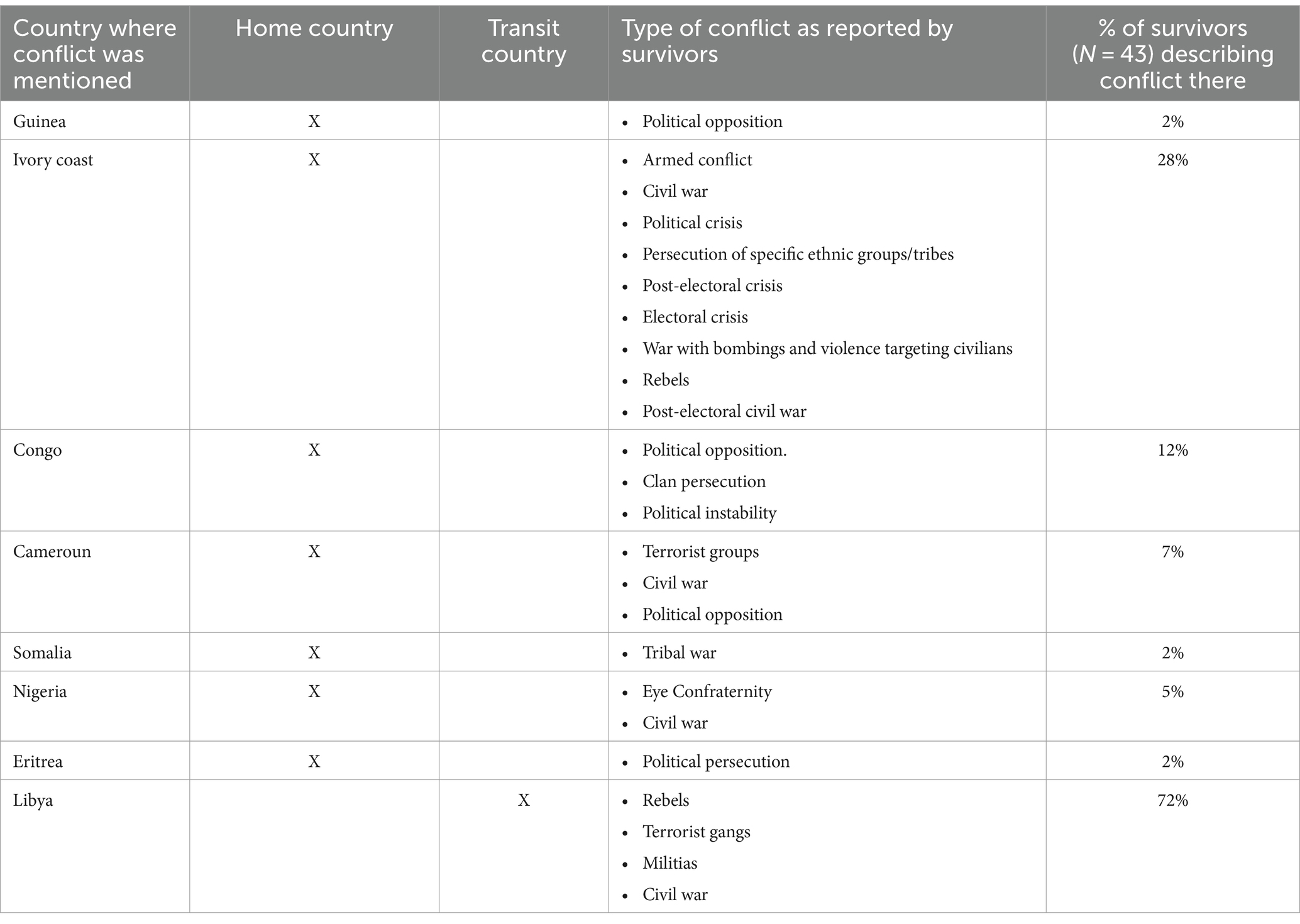
Table 2. Table showing the countries where survivors encountered conflict and type.
3.4 Reason for fleeing
For most women, disclosed causes for migration were connected to different forms of GBV (n = 9, 21%) and to conflict (n = 26, 60%). In the first case, violence targeted both survivors of CRSV as well as other members of their family (e.g., husband).
Occasionally, migrants described economic (e.g., poverty and lack of economic safety for their children), work-related reasons, and search for better healthcare as strategic drivers for migration.
3.5 CRSV
3.5.1 Description of CRSV
During the interview, the history of assault was collected in first (n = 28) or third person (n = 15). In most cases the history of violence as reported in the medical records was narrated by enumerating the different episodes of violence (CRSV, other violence, and other GBV) endured by survivors in an objective and detached manner. At times, professionals working in SVS described the difficulties patients had in disclosing the violence they suffered. One survivor accessed SVS multiple times since the suffering prevented her from retelling the events. The psychological sequelae emerged through signs’ annotations taken by the gynecologist or midwife.
3.5.2 CRSV in home country
CRSV occurring in the home country was mentioned by 18 survivors (42%), of which 14 described being subjected to co-occurring nonsexual violence (78%).
All of them described being raped, with different modalities (e.g., single episodes and perpetrators, multiple or gang rape, transactional sex). Some disclosed being pregnant at the time of assault, with aggressors attempting to induce miscarriage.
“We were taken hostage for 10 days. I was pregnant. We were subjected to physical violence — beatings with the use of hands, feet, sticks I still have the scars of — and to sexual violence: I was vaginally abused multiple times by different men.” (Cameroun)
Others described policemen trying to force the victim’s brothers to rape her and her sister. SV was sometimes associated with witnessed rape of family members or witnessed instrumentation, and unwanted sexual touching.
Witnesses of episodes of CRSV were family members, including children.
Perpetrators were described as members of armed forces, police officers, Boko Haram members, rebels, individuals who broke into the victim’s home (e.g., “men” or “rebels,” “supporters of a different political party”), and were at times defined in generic terms (e.g., “men”, “a group of men,” “armed men”).
CRSV was reportedly perpetrated in a variety of locations: a stadium, indoors, the perpetrators’ car, terrorist groups’ hideouts or other secluded places, the street, police centers, and in prison. A pattern of CRSV occurring in the survivors’ home emerged (n = 8, 44%).
“One day, the rebels broke into our home and beat us. My niece was beaten to death, my sister-in-law and I were raped.” (Ivory Coast)
Reported co-occurring nonsexual violence included use of blunt force (through use of natural weapons, sticks, and belts), grabbing, pushing, hair dragging, ejection from a vehicle, imprisonment, kidnapping and being taken hostage, death threats, including with weapons, torture, being tied with a rope, witnessed killing of family members, and kidnapping of family members.
In particular, one survivor described excruciating physical and sexual violence. After being subjected to CRSV on more than one occasion, she endured 6 years of prison where she was constantly sexually victimized and other 5 years in a different detention facility where she was raped daily. Co-occurring violence encompassed forced labor in inhuman conditions, including being forced to throw dead bodies of other prisoners into a river, beatings with a burning machete, denial of water, care, and of access to sanitation facilities (e.g., showers and toilets). During episodes of CRSV she was tortured and beaten. The survivor expressed living in a state of constant fear:
"They told us we were sentenced to death, and we lived with that terror. I lost any hope, I wanted my life to end, I wanted to die." (Congo)
3.5.3 CRSV in transit country
CRSV in transit countries was reported by 31 survivors (72%), of which 22 described co-occurring nonsexual violence (51%). Overall, six women disclosed victimization both in home and transit countries (14%).
Survivors described being subjected to rape (e.g., single episodes and perpetrators, gang and multiple rape, penile, with fingers, and instrumentation, vaginal, oral, and anal) including while being pregnant, attempted forced abortion, torture-induced miscarriage, forced nudity, and unwanted sexual touching.
A common reported pattern was being kidnapped, scammed, or arrested and sold to brothels (also described as “houses,” “prisons,” or “detention houses”) together with other women, and being brought to other places during the night to be sexually exploited.
“When we arrived at the other house, we understood something was wrong: there were many women. Some men beat and rape us every day. Often a group of men did that from 10 pm until 6 am.” (Ivory Coast)
At times, individuals who paid for victims’ release from detention centers were the ones who sold them to brothels. A survivor described being forced into prostitution while pregnant, with a “madame” attempting unwanted pharmacological abortion on her. Another reported being trafficked and sold to a “mentally disturbed Arab man” together with other women, and enduring physical abuse.
Other women victims of violence, the survivors’ husbands, or their children witnessed episodes of CRSV.
“Groups of men,” members of terrorist gangs, “men,” “rebels,” police officers, camp staff, Asma Boys, “boys gangs,” madames, smugglers, “armed militia” men, and militia men were identified as perpetrators of CRSV.
“The first time I attempted to come to Italy by boat I was arrested by the Libyan police and brought to prison. […] At night, policemen came and raped us. Men were beaten and we were also beaten if we refused to have intercourse with policemen.” (Nigeria)
CRSV was perpetrated indoors (e.g., the victim’s or other acquaintances or family members’ home), outdoors (e.g., street), as well as in enclosed or secluded spaces (e.g., concentration points, prisons, brothels, holding locations, camps, detention houses, on occasions generally defined as “houses” or “abandoned houses”).
"One day some Arab men came to our house and kidnapped us. They put us in a prison where there were many women […]. Some men arrived, took us away, raped us, and we couldn't fight back. This happened ceaselessly. I couldn't take it any longer, so I told them: "Just kill me, I am tired, I cannot do this anymore". But these men took me and dragged me on the floor […], hit me hard on my right arm, which still hurts to this day, and on my head. Sometimes I still feel dizzy because of this act of violence." (Ivory Coast)
Disclosed co-occurring acts of violence were blunt force injuries, ejection from a moving car, dragging, denial of care, witnessed death or violence on family members, death-related or other threats, housebreaking, theft, house destruction, detention, threat of guns, sharp force injuries, scourging, denial of food, burning, torture, and extortion.
3.5.4 Negative consequences of CRSV
Negative outcomes of CRSV are reported in Table 3.

Table 3. Table showing the health consequences of CRSV.
3.6 Other violence
In addition to CRSV, other episodes of conflict and migration related nonsexual violence and GBV were described by patients.
3.6.1 Conflict and migration related nonsexual violence
In many instances, other violence was connected to the conflict encountered in victims’ home country or in transit, as well as to their migration experience.
In their home country, survivors reported personal and property offenses against themselves and family members. A woman reported her son dying during migration:
“I fled together with my younger child and other people to Sudan. At the border, soldiers started to shoot us and I fell. My son violently hit his head and died of a hemorrhage.” (Eritrea)
Violence on the move and in a transit country was described by 22 survivors (51%) and included property and personal offenses against themselves and family members. Some survivors who disclosed working as housemaids, or were labor trafficked, reported a variety of mistreatments, including physical violence, not being paid, and being sent out to the streets.
Arrests were mostly reported as occurring through policemen breaking into a victim’s home. At times they were connected to racism, or to migration control in concentration points or on while trying to leave for Italy. Survivors disclosed being sent to detention or prison camps or centers and being moved between different locations.
In this context, many victims described forceful separation from family members, attempted forced separation from children, beatings, torture, exploitation and mistreatment, threats, and starvation. One reported undergoing cesarean delivery in prison and being told her baby was dead. Extortion and money lent by strangers used as a form of ransom were also described.
"Every day they asked for extortion money. If people didn't have money, they threw water on them and then connected them to an electric plug and poured melted plastic on them. They hit people with sticks and raped them." (Ivory Coast)
Smuggling of migrants was described especially for what concerns the last phases before departure from the Libyan coast, occasionally connected to paying ransoms. Survivors disclosed receiving death threats, including with guns, while being forced to get on a boat and witnessing the murder of those who refused.
"One night, some Arab men arrived and under the threat of weapons they told me I had to go out of that house [and follow them]. During the route I was feeling very cold. Then I heard the sound of sea waves. Still under the threat of weapons, they made us get out of the car and we found ourselves on the shore. There were many people. With the use of force, they pushed us on a rubber boat, I didn't know where I was going." (Nigeria)
One reported being forced on a rubber boat and being sent adrift with the engine not working, those trying to get down being shot. Another disclosed being left on the shore because she was laboring.
Violence in the host country (n = 5) was related in most cases to their vulnerable condition after migration, with some of them reporting becoming unhoused. Survivors became aware of threats or extortion targeting relatives when living in the host country or in transit.
3.6.2 Other GBV
In addition to experiences of CRSV, survivors encountered other instances of GBV during their lifetime. We separated GBV during childhood (n = 2), NPV (n = 6), and relational GBV, encompassing domestic and intimate partner violence (n = 7).
Before CRSV, some patients described being sexually trafficked (n = 3) or prior episodes of sexual violence victimization (n = 4).
4 Discussion
This study analyzed the interview transcripts of victims of CRSV accessing care at the sexual violence relief center Soccorso Violenza Sessuale (SVS) in Sant’Anna Hospital in Turin, North-West Italy. The most reported countries of origin of migrants were Ivory Coast, Nigeria, and Cameroun. In this study, 25 patients described their home country as conflict-affected, while 31 reported encountering hostilities in Libya. CRSV was disclosed by 18 survivors as occurring in their home country, where a commonly described pattern was perpetrators breaking into victims’ homes and assaulting them. All those transiting through Libya (n = 31) were subjected to CRSV there. This is coherent with data addressing the high prevalence of violence endured by migrants transiting this country (Castagna et al., 2018; Reques et al., 2020). CRSV was experienced in both home and transit countries by 14% of patients. Among the different types of CRSV, rape was the most disclosed. Perpetrators were hard to identify and, in most cases, had some form of authority over survivors, confirming other studies’ findings (Reques et al., 2020; Tan and Kuschminder, 2022).
Almost half of the patients described physical consequences of CRSV, the most disclosed one being pregnancy, in agreement with other literature findings (Rubini et al., 2023; Svallfors et al., 2024), and 72% reported psychological outcomes, in particular fear, crying, and sadness. Feelings of detachment and avoidance as perceived by members of the research team during the thematic analysis may also be connected to the effect of multiple traumatic events on victims (Lijtmaer, 2022; Verelst et al., 2020). While the Biopsychosocial Model proposed by Engel also encompasses the social dimension of health and even though negative consequences in this sphere are highly represented in populations affected by CRSV (Rubini et al., 2023), no SVS patient described social consequences. This could be related to social outcomes not being considered as part of their general health status by survivors and consequently not being disclosed or could be connected to providers not asking direct questions concerning this dimension of health during the interview, limiting the depth of our findings.
Many survivors described different forms of violence, including conflict and CRSV, as a driver for leaving their home country. A smaller number of patients traced back the cause for migration to economic reasons.
The majority of migratory flows in the years 2012–2017 occurred on the Central Mediterranean Route, the world’s deadliest migratory journey (Malakooti, 2019; Missing migrants project, n.d.). Patients from SVS described partially or entirely their migration route, which for the majority coincides with the Mediterranean one, with Libya being the last transit country for 86% of them. There, as documented by survivors’ accounts, conflict intertwines with the system of control, detention, exploitation, extortion, and smuggling of migrants (Reques et al., 2020). In addition, individuals who could be eligible for international protection in other States are identified in Libya as “irregular migrants,” since no law on asylum has been implemented and entering illegally in the country is a criminal offense punishable with imprisonment (Mancini, 2018). This situation presents some similarities with the context of the Mexico-USA migration corridor, characterized by high levels of violence and danger, as well as by captivity in “safe houses” and the presence of smugglers (e.g., coyotes). Moreover, migrants passing through Mexico are considered “irregular” and can be subjected to deportation, even though conflicts, organized crime, and GBV often constitute their reason to migrate (Cleaveland and Kirsch, 2020; Infante et al., 2020). Punitive measures enforced against irregular migrants render them at higher risk of abuse (Soria-Escalante et al., 2022).
In the years 2017–2023 there was a drastic reduction in the number of accesses at SVS, which can partially be traced to the decrease in the amount of arrivals in Italy, influenced by a Memorandum of Understanding signed between Italy and Libya in 2017 in which migration is framed as a “security issue” and where Italy agreed to provide financial and technical support to the Libyan Coastal Guard in order to increase their maritime surveillance capacity (Memorandum of understanding on cooperation in the fields of development, the fight against illegal immigration, human trafficking and fuel smuggling and on reinforcing the security borders between the State of Libya and the Italian Republic, 2017; MSF, 2022). The figure dropped in 2018 and 2019 (e.g., from 119,369 arrivals in 2017 to 23,370 and 11,471, respectively, in 2018 and 2019; UNHCR, n.d.), reaching the lowest number of arrivals since 2012 (Malakooti, 2019). This also coincided with the increase in the number of migrants intercepted at sea by the Libyan Coastal Guard and transferred into detention facilities (IRC, 2021).
The findings of the present study align with the notion of “conflict-affected women on the move” conceptualized by Holvikivi and Reeves, highlighting the long-term impact of conflict (Holvikivi and Reeves, 2020). In fact, the hostilities often constituted the first of a series of events carrying a negative impact on survivors’ well-being (e.g., forced migration, violent death of family members, detention, and torture). This also aligns with the concept of “ultraviolence,” namely the great level and different types of brutality employed by a variety of stakeholders in distinct moments in space and time, encompassing the conflict-related nonsexual violence, as well as CRSV and nonsexual violence inflicted during sexual assault, together with violence experienced in its aftermath (Rubini et al., 2023).
In Italy, in recent years, new protocols and trainings have been implemented for the management of GBV cases (Linee guida nazionali per le Aziende sanitarie e le Aziende ospedaliere in tema di soccorso e assistenza socio-sanitaria alle donne vittime di violenza, 2017; Ministero della Salute, 2023; Presidenza del consiglio di ministri Dipartimento Pari Opportunità, 2021), including laws on triage, with the mandatory assignment of at least a “yellow code” or equivalent (e.g., urgent care needed; Linee guida nazionali per le Aziende sanitarie e le Aziende ospedaliere in tema di soccorso e assistenza socio-sanitaria alle donne vittime di violenza, 2017). However, operator- (e.g., awareness of GBV, personal beliefs, and training) and health system-dependent (e.g., limited resources to conduct clinical and forensic tasks) obstacles still exist (Cattaneo et al., 2024; Gino and Caenazzo, 2020; Mtaita et al., 2023; Progetto REVAMP 2018, Istituto Superiore di Sanità, 2018). In addition, only two centers situated in the North-West area provide specialist care for GBV survivors, with only one of them accessible to cisgender men victims of violence (Margherita et al., 2021; Policlinico Milano, n.d.). This figure echoes the limited number of specialist centers available for the management of GBV in Europe, highlighting a gap between the needs of survivors and health services availability and accessibility (Rajan et al., 2021). Taking into consideration that the Explanatory report of the Council of Europe Convention on Preventing and Combating Violence against Women and Domestic Violence (e.g., Istanbul Convention) recommends one specialist service to be available to every 200.000 inhabitants (Council of Europe, 2018, 2011a, 2011b), with a geographic spread guaranteeing their accessibility in cities and rural areas, this objective is far to be met. Of the 1,400 hospitals on the Italian territory, 6151 have an ED (Pronto soccorso in Italia: Agenas presenta i dati alla Camera, 2023), each providing care for a pool of users of at least 80.000–150.000 inhabitants. This means that, according to the Explanatory report, roughly every ED in Italy should host a specialist service for the management of GBV cases. However, it would be more realistic for a smaller number of these centers to be present either at regional level or to cover large territorial areas.
The creation of intrahospital and centralized specialist services could reduce the pressure on general as well as on obstetrics and gynecological EDs, which constitute the main entry point for survivors of GBV (Ministero della Salute, 2023; Progetto REVAMP 2018, Istituto Superiore di Sanità, 2018; Regione Lombardia, 2021), including SV, alleviating the burden on the health system and on providers, who need to take care of patients presenting with a variety of health issues necessitating emergency and urgent care (Regione Lombardia, 2021). Implementing specialist services could ultimately result in better health outcomes and higher quality of care for survivors (Morley et al., 2018), also in terms of dedicated spaces within hospitals as well as longer consultation time for complex cases. In the meantime, better training for forensic and clinical management of patients accessing care due to GBV should be implemented in EDs (Cattaneo et al., 2024). This should also encompass continuous training for health providers on laws regulating the management of victims of GBV, including the legal requirements for reporting, also in cases of undisclosed abuse (Albert Henry, 2023).
As highlighted in the gatekeeping model proposed by Rajan et al. (2021), barriers in healthcare-seeking in cases of sexual abuse encompass external elements related to the healthcare systems as well as internal ones, connected to the patient (Rajan et al., 2021). The latter include difficulties in understanding the correlation between symptoms and violence, as well as shame, fear, and the effects of trauma on brain functions and abilities (Rajan et al., 2021). For migrant survivors, these difficulties intersect with other levels of obstacles in accessing care connected to language barriers (Trentin et al., 2023) and navigating the new health system in the host country (Pandey et al., 2022), as well as lack of confidence in the legal and healthcare systems (Rodella Sapia et al., 2020). For these reasons, it is plausible that the number of migrant women who need to access GBV-related care is larger compared to the current pool of users of specialist and general services within this population. Moreover, since continuity of care is hindered during the migration process, migrant women may suffer from health conditions exacerbated by delay in access to care (UNHCR, n.d.).
Given the high number of migrants arriving in Italy who encountered conflict and possibly CRSV, and taking into consideration that this population is among those at higher risk of GBV victimization (Progetto REVAMP 2018, Istituto Superiore di Sanità, 2018; Rodella Sapia et al., 2020), implementing specialist services for the management of GBV could also serve their complex health needs (Rubini et al., 2024) and guarantee the high quality of forensic practice that is needed to document the abuses they endured, possibly influencing the determination of protection outcomes (Rubini et al., 2024). They should also receive support in navigating the health system (Presidenza del consiglio di ministri Dipartimento Pari Opportunità, 2021), including GBV-related services, through dissemination of informative materials (e.g., in shops, reception venues, counseling centers), with language- and cultural-specific communication campaigns on the use of the National Helpline “Violence and Stalking” 1522 (Presidenza del consiglio di ministri Dipartimento Pari Opportunità, 2021), and the stable presence of cultural mediators in health facilities (Presidenza del consiglio di ministri Dipartimento Pari Opportunità, 2021). Culturally sensitive and migrant inclusive policies and protocols should be developed and implemented in all EDs. Migrants should also be aware of their entitlement to primary healthcare (Acquadro-Pacera, 2024).
Systems caring for migrants and anti-trafficking networks should act as a contact point between individuals seeking international protection belonging to the category of vulnerable persons, including victims of trafficking, and GBV-related services (Disposizioni urgenti in materia di flussi di ingresso legale dei lavoratori stranieri e di prevenzione e contrasto all’immigrazione irregolare, 2023; Ministero della Salute, 2017). These initiatives enabling access to care should equally target undocumented migrants who are victims of GBV, prioritizing their health needs and human rights over migration control (PICUM, 2024). The best practices implemented by SVS at Sant’Anna hospital in Turin, including fostering the connection with NGOs and other third sector organizations working with migrants, as well as the culturally sensitive approach to GBV, together with the positive results obtained through these practices in terms of equity in access to care, highlight the necessity of creating similar services in Italy in order to offer high quality care to migrants survivors of GBV, including CRSV. It is therefore crucial to integrate the systems taking care of migrant women with those managing the sequelae of GBV.
Implementing these recommendations could contribute towards the achievement of the United Nations’ 2030 SDGs, in particular number three—Healthy Lives and Well-Being, number five—Gender Equality, and number 16—Peaceful and Inclusive Societies (UN, 2015).
The study findings carry some limitations, as physical and psychological consequences refer to those described or manifested by patients during the interview and do not encompass those emerging through top-to-toe and gynecological examination. Moreover, they reflect the experiences of the pool of users of SVS and may not be generalizable.
5 Conclusion
This paper analyzed the history of violence as presented by cisgender women survivors of CRSV accessing care at the specialist center SVS in Sant’Anna hospital in Turin. The study confirmed the high level and different modalities of violence, including CRSV, experienced by patients in their home country as well as during their migratory journey, in particular in Libya. Many patients described being raped. More reported psychological outcomes were fear, crying, and sadness, while the most disclosed physical consequence was pregnancy. Qualitative analysis of interview transcripts was a valuable source for understanding how survivors described the CRSV they endured, its consequences, as well as other violence encountered during their migratory route. More studies should employ this methodology, also exploring the experiences of other populations affected by CRSV.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Requests to access these datasets should be directed to Elena Rubini, ZWxlbmEucnViaW5pQHVuaXVwby5pdA==.
Ethics statement
The studies involving humans were approved by Ethics Committee of the AOU Città della Salute e della Scienza di Torino—AO Ordine Mauriziano di Torino (CE 112/2020). The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
ER: Conceptualization, Data curation, Formal analysis, Investigation, Writing – original draft. MT: Data curation, Formal analysis, Investigation, Writing – original draft. MV: Conceptualization, Methodology, Writing – review & editing. SC: Writing – review & editing. AC: Data curation, Supervision, Writing – review & editing. PC: Supervision, Writing – review & editing. LR: Supervision, Writing – review & editing. SG: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
This manuscript is the result of a study conducted in the framework of the International PhD in Global Health, Humanitarian Aid, and Disaster Medicine organized by Università del Piemonte Orientale (UPO).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AO, Azienda ospedaliera; AOU, Azienda ospedaliera universitaria; CAV, centro antiviolenza; CRSV, Conflict-related sexual violence; ED, Emergency department; GBV, Gender-based violence; NPV, Non-partner violence; PNRR, Piano nazionale ripresa resilienza; SDG, Sustainable development goal; SRHR, Sexual and reproductive health and rights; SVS, Soccorso violenza sessuale; SV, Sexual violence; SVSeD, Soccorso violenza sessuale e domestica.
Footnotes
1. ^This figure represents the total number of hospitals with an ED, including secondary- and tertiary- level hospitals.
References
Acquadro-Pacera, G. (2024). Exploring differences in the utilization of the emergency department between migrant and non-migrant populations: A systematic review. BMC Public Health 24:963. doi: 10.1186/s12889-024-18472-3
Albert Henry, T. (2023). You suspect a patient is being abused. What should you do? AMA J. Ethics. Available at: https://www.ama-assn.org/delivering-care/patient-support-advocacy/you-suspect-patient-being-abused-what-should-you-do (Accessed March 3, 2024).
Amnesty International (2020). “Between life and death”: Refugees and migrants trapped in Libya’s cycle of abuse. Available at: https://www.amnesty.org/en/documents/mde19/3084/2020/en/ (Accessed August 28, 2024).
Applebaum, A., and Mawby, B., (n.d.). Gang violence as armed conflict. Available at: https://giwps.georgetown.edu/resource/gang-violence-as-armed-conflict/ (Accessed August 28, 2024).
Balcells, L. (2015). “Political violence. An institutional approach” in Routledge handbook of comparative political institutions. eds. J. Ghandi and R. Ruiz-Rufino (Abingdon: Routledge).
Borges, G. M. (2024). Journey of violence: refugee Women’s experiences across three stages and places. J. Int. Migr. Integr. 25, 673–693. doi: 10.1007/s12134-023-01102-z
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Castagna, P., Ricciardelli, R., Piazza, F., Mattutino, G., Pattarino, B., Canavese, A., et al. (2018). Violence against African migrant women living in Turin: clinical and forensic evaluation. Int. J. Legal Med. 132, 1197–1204. doi: 10.1007/s00414-017-1769-1
Cattaneo, C., Tambuzzi, S., De Vecchi, S., Maggioni, L., and Costantino, G. (2024). Consequences of the lack of clinical forensic medicine in emergency departments. Int. J. Legal Med. 138, 139–150. doi: 10.1007/s00414-023-02973-8
Cleaveland, C., and Kirsch, V. (2020). “They took all my clothes and made me walk naked for two days so I couldn’t escape”: Latina immigrant experiences of human smuggling in Mexico. Qual. Soc. Work. 19, 213–228. doi: 10.1177/1473325018816362
Cockburn, C. (2004). “The continuum of violence – a gender perspective on violence and peace” in Sites of violence – Gender and conflict zones. eds. W. Giles and J. Hyndmann (Los Angeles: University of California Press, Berkeley).
Council of Europe (2011a). Council of Europe convention on preventing and combating violence against women and domestic violence. Available at: https://www.coe.int/en/web/gender-matters/council-of-europe-convention-on-preventing-and-combating-violence-against-women-and-domestic-violence (Accessed August 28, 2024).
Council of Europe (2011b). Explanatory report to the Council of Europe Convention on preventing and combating violence against women and domestic violence. Available at: http://conventions.coe.int/Treaty/EN/Reports/Html/210.htm (Accessed August 28, 2024).
Council of Europe (2018). Mapping support services for victims of violence against women in line with the Istanbul convention standards. Methodology and tools. Available at: https://rm.coe.int/final-vaw-support-2019-eng-forms/168093b8b9 (Accessed August 28, 2024).
Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: a black feminist critique of antidiscrimination doctrine, Feminist Theory and Antiracist Politics. Univ. Chic. Leg. Forum 1989.
Davies, S. E., and True, J. (2015). Refraiming conflict-related sexual and gender-based violence: bringing gender analysis back. Secur. Dialogue 46, 495–512. doi: 10.1177/0967010615601389
Disposizioni urgenti in materia di flussi di ingresso legale dei lavoratori stranieri e di prevenzione e contrasto all’immigrazione irregolare (2023). Available at: https://www.gazzettaufficiale.it/eli/id/2023/05/18/23A02728/sg (Accessed August 28, 2024).
EASO (2021). Nigeria security situation - country of origin information report. Available at: https://reliefweb.int/report/nigeria/nigeria-security-situation-country-origin-information-report-june-2021 (Accessed August 28, 2024).
Ferris, E. G. (1990). Refugee women and violence. Geneva: Presented at the World Council of Churches.
Fondazione ISMU (2023). Ventinovesimo Rapporto sulle migrazioni 2023. Available at: https://www.ismu.org/ventinovesimo-rapporto-sulle-migrazioni-2023/ (Accessed August 28, 2024).
Footer, K. H. A., and Rubenstein, L. S. (2013). A human rights approach to health care in conflict. Int. Rev. Red Cross 95, 167–187. doi: 10.1017/S1816383113000349
Gino, S., and Caenazzo, L. (2020). “Forensic implications in the management of sexual violence in hospitals” in Victims of violence: support, challenges and outcomes. Ed. M. L. Knudsen. (New York: Nova Science), 79–98.
Gino, S., Canavese, A., Pattarino, B., Robino, C., Omedei, M., Albanese, E., et al. (2017). 58 cases of sexual violence bearing forensic interest: congruence between the victim’s report and the data from laboratory analyses. Int. J. Legal Med. 131, 1449–1453. doi: 10.1007/s00414-017-1602-x
Gray, H. (2019). The ‘war’/‘not-war’ divide: domestic violence in the preventing sexual violence initiative. Br. J. Polit. Int. Rel. 21, 189–206. doi: 10.1177/1369148118802470
Heise, L. L., Raikes, A., Watts, C. H., and Zwi, A. B. (1994). Violence against women: a neglected public health issue in less developed countries. Soc. Sci. Med. 39, 1165–1179. doi: 10.1016/0277-9536(94)90349-2
Holvikivi, A., and Reeves, A. (2020). Women, peace and security after Europe’s ‘refugee crisis. Eur. J. Int. Secur. 5, 135–154. doi: 10.1017/eis.2020.1
Hourani, J., Block, K., Phillimore, J., Bradby, H., Ozcurumez, S., Goodson, L., et al. (2021). Structural and symbolic violence exacerbates the risks and consequences of sexual and gender-based violence for forced migrant women. Front. Hum. Dyn. 3:769611. doi: 10.3389/fhumd.2021.769611
IASC Task Force on Gender and Humanitarian, Assistance (2005). Guidelines for gender-based violence interventions in humanitarian settings focusing on prevention of and response to sexual violence in emergencies.
ICRC (2008). How is the term “armed conflict” defined in international humanitarian law? Available at: https://www.icrc.org/en/doc/resources/documents/article/other/armed-conflict-article-170308.htm (Accessed May 9, 2023).
Infante, C., Leyva-Flores, R., Gutierrez, J. P., Quintino-Perez, F., Torres-Robles, C. A., and Gomez-Zaldívar, M. (2020). Rape, transactional sex and related factors among migrants in transit through Mexico to the USA. Cult. Health Sex. 22, 1145–1160. doi: 10.1080/13691058.2019.1662088
IOM (2006). Migration: a social determinant of the health of migrants. Available at: https://migrant-integration.ec.europa.eu/sites/default/files/2009-10/docl_9914_392596992.pdf (Accessed August 28, 2024).
IOM (2019). Four decades of cross Mediterranean undocumented migration to Europe: a review of the evidence. Available at: https://publications.iom.int/system/files/pdf/four_decades_of_cross_mediterranean.pdf (Accessed August 28, 2024).
IOM (n.d.) About migration. Available at: https://www.iom.int/about-migration (Accessed May 9, 2023).
IRC (2021). Libya: record numbers intercepted at sea and detained; IRC calls for their immediate release. Available at: https://reliefweb.int/report/libya/libya-record-numbers-intercepted-sea-and-detained-irc-calls-their-immediate-release (Accessed February 22, 2024).
Kalyvas, S. N. (2001). “New” and “old” civil wars: a valid distinction? World Polit. 54, 99–118. doi: 10.1353/wp.2001.0022
Krause, U. (2015). A continuum of violence? Linking sexual and gender-based violence during conflict, flight, and encampment. Refug. Surv. Q. 34, 1–19. doi: 10.1093/rsq/hdv014
Lijtmaer, R. M. (2022). Social trauma, nostalgia and mourning in the immigration experience. Am. J. Psychoanal. 82, 305–319. doi: 10.1057/s11231-022-09357-8
Linee guida nazionali per le Aziende sanitarie e le Aziende ospedaliere in tema di soccorso e assistenza socio-sanitaria alle donne vittime di violenza (2017). Available at: https://www.gazzettaufficiale.it/eli/id/2018/01/30/18A00520/SG (Accessed August 28, 2024).
Malakooti, A. (2019). The political economy of migrant detention in Libya: Understanding the players and the business models. Available at: https://globalinitiative.net/analysis/migrant-detention-libya/ (Accessed August 28, 2024).
Mancini, M. (2018). Italy’s new migration control policy: stemming the flow of migrants from Libya without regard for their human rights. Ital. Yearb. Int. Law Online 27, 259–281. doi: 10.1163/22116133-02701015
Margherita, M., Franceschetti, L., Maggioni, L., Vignali, G., Kustermann, A., and Cattaneo, C. (2021). Male victims of sexual abuse and domestic violence: a steadily increasing phenomenon. Med. Sci. Law 61, 54–61. doi: 10.1177/0025802420947003
Memorandum of understanding on cooperation in the fields of development, the fight against illegal immigration, human trafficking and fuel smuggling and on reinforcing the security borders between the State of Libya and the Italian Republic. (2017). Available at: https://www.asgi.it/wp-content/uploads/2017/02/ITALY-LIBYA-MEMORANDUM-02.02.2017.pdf (Accessed August 28, 2024).
Menjívar, C., and Perreira, K. M. (2019). Undocumented and unaccompanied: children of migration in the European Union and the United States. J. Ethn. Migr. Stud. 45, 197–217. doi: 10.1080/1369183x.2017.1404255
Ministero del lavoro e delle politiche sociali (2021). La presenza dei migranti nella città metropolitana di Torino. Available at: https://www.lavoro.gov.it/documenti-e-norme/studi-e-statistiche/ram-2021-torino.pdf (Accessed August 28, 2024).
Ministero della Salute (2017). Linee guida per la programmazione degli interventi di assistenza e riabilitazione nonché per il trattamento dei disturbi psichici dei titolari dello status di rifugiato e dello status di protezione sussidiaria che hanno subito torture, stupri o altre forme gravi di violenza psicologica, fisica o sessuale. Available at: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2599_allegato.pdf (Accessed August 28, 2024).
Ministero della Salute (2023). Violenza sulle donne - La formazione degli operatori sociosanitari. Salute Della Donna. Available at: https://www.salute.gov.it/portale/donna/dettaglioContenutiDonna.jsp?lingua=italiano&id=4498&area=indennizzo&menu=vuoto&tab=4 (Accessed March 22, 2024).
Missing migrants project (n.d.), Migration within the Mediterranean. Available at: https://missingmigrants.iom.int/region/mediterranean (Accessed March 22, 2024).
Morgen, A. (2013). Community rejection following sexual assault as ‘forced migration. Forced Migr. Rev. 44, 87–88.
Morley, C., Unwin, M., Peterson, G. M., Stankovich, J., and Kinsman, L. (2018). Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One 13:e0203316. doi: 10.1371/journal.pone.0203316
MSF (2022). Italy-Libya agreement: five years of EU-sponsored abuse in Libya and the Central Mediterranean. Available at: https://www.msf.org/italy-libya-agreement-five-years-eu-sponsored-abuse-libya-and-central-mediterranean (Accessed March 22, 2024).
MSF (n.d.). Persecution. Pract. Guide Humanit. Law. Available at: https://guide-humanitarian-law.org/content/article/3/persecution-1/ (Accessed May 9, 2023).
Mtaita, C., Safary, E., Simwanza, K., Mpembeni, R., Likindikoki, S., and Jahn, A. (2023). Knowledge, implementation, and gaps of gender-based violence management guidelines among health care workers. Int. J. Environ. Res. Public Health 20:5409. doi: 10.3390/ijerph20075409
Nixon, S. A. (2019). The coin model of privilege and critical allyship: implications for health. BMC Public Health 19:1637. doi: 10.1186/s12889-019-7884-9
Non-international armed conflicts in Libya (2022). Rulac Geneva Acad. Available at: https://www.rulac.org/browse/conflicts/non-international-armed-conflicts-in-libya#collapse2accord (Accessed March 22, 2024).
Obinna, D. N. (2021). Seeking sanctuary: violence against women in El Salvador, Honduras, and Guatemala. Viol. Women 27, 806–827. doi: 10.1177/1077801220913633
Öhman, A., Burman, M., Carbin, M., and Edin, K. (2020). ‘The public health turn on violence against women’: analysing Swedish healthcare law, public health and gender-equality policies. BMC Public Health 20:753. doi: 10.1186/s12889-020-08766-7
Pandey, M., Kamrul, R., Michaels, C. R., and McCarron, M. (2022). Identifying barriers to healthcare access for new immigrants: a qualitative study in Regina, Saskatchewan, Canada. J. Immigr. Minor. Health 24, 188–198. doi: 10.1007/s10903-021-01262-z
Pertek, S., and Phillimore, J. (2022). “Nobody helped me” forced migration and sexual and gender-based violence: Findings from the SEREDA project. Available at: https://www.birmingham.ac.uk/documents/college-social-sciences/social-policy/iris/2022/sereda-international-report.pdf (Accessed August 28, 2024).
Phillimore, J., Block, K., Bradby, H., Ozcurumez, S., and Papoutsi, A. (2023). Forced migration, sexual and gender-based violence and integration: effects, risks and protective factors. J. Int. Migr. Integr. 24, 715–745. doi: 10.1007/s12134-022-00970-1
PICUM (2024). New EU directive on violence against women leaves out migrant women. Available at: https://picum.org/blog/new-eu-directive-on-violence-against-women-leaves-out-migrant-women/ (Accessed July 15, 2024).
Policlinico Milano, (n.d.). Centro di Riferimento Centro di riferimento di assistenza per i problemi della violenza alle donne e ai minori (Soccorso Violenza Sessuale e Domestica – SVSeD). Available at: https://www.policlinico.mi.it/centri-di-riferimento/23/centro-di-riferimento-di-assistenza-per-i-problemi-della-violenza-alle-donne-e-ai-minori-soccorso-violenza-sessuale-e-domestica-svsed (Accessed March 22, 2024).
Presidenza del consiglio di ministri Dipartimento Pari Opportunità (2021). Piano strategico nazionale sulla violenza maschile contro le donne. Available at: https://www.pariopportunita.gov.it/media/1952/piano-nazionale-violenza-2021-2023.pdf (Accessed August 28, 2024).
Preventing Sexual Violence in Conflict Initiative (2017). Preventing sexual violence in conflict initiative. Principles for Global Action: Preventing and Addressing Stigma Associated with Conflict-related Sexual Violence. Available at: https://assets.publishing.service.gov.uk/media/5a82a842ed915d74e3402e70/PSVI_Principles_for_Global_Action.pdf (Accessed August 28, 2024).
Pries, L., Calderón Morillón, O., and Estrada Ceron, B. A. (2024). Trajectories of forced migration: central American migrants on their way toward the USA. J. Migr. Hum. Secur. 12, 39–53. doi: 10.1177/23315024231216109
Progetto REVAMP 2018, Istituto Superiore di Sanità (2018). Riconoscere, accogliere e accompagnare le persone vittime di violenza relazionale donne e minori in particolare. Manuale per operatori di Pronto Soccorso. Available at: http://www.sossanita.it/doc/2017_11_violenza-guida-report_progetto-revamp.pdf (Accessed August 28, 2024).
Pronto soccorso in Italia: Agenas presenta i dati alla Camera, (2023). Farma7. Available at: https://farma7.it/2023/12/01/pronto-soccorso-in-italia-agenas-presenta-i-dati-alla-camera/ (Accessed March 22, 2024).
Rajan, G., Wahlström, L., Philips, B., Wändell, P., Wachtler, C., Svedin, C.-G., et al. (2021). Delayed healthcare access among victims of sexual abuse, understood through internal and external gatekeeping mechanisms. Nord. J. Psychiatry 75, 370–377. doi: 10.1080/08039488.2020.1868573
Regione Lombardia (2021). Manuale triage intraospedaliero regione Lombardia. Available at: https://simeup.it/wp-content/uploads/2022/12/Allegato-1-Manuale-di-Triage.pdf (Accessed August 28, 2024).
Reques, L., Aranda-Fernandez, E., Rolland, C., Grippon, A., Fallet, N., Reboul, C., et al. (2020). Episodes of violence suffered by migrants transiting through Libya: a cross-sectional study in “Médecins du Monde’s” reception and healthcare Centre in seine-Saint-Denis. France. Confl. Health 14:12. doi: 10.1186/s13031-020-0256-3
Rodella Sapia, M. D., Wangmo, T., Dagron, S., and Elger, B. S. (2020). Understanding access to professional healthcare among asylum seekers facing gender-based violence: a qualitative study from a stakeholder perspective. BMC Int. Health Hum. Rights 20:25. doi: 10.1186/s12914-020-00244-w
Rodríguez Serna, N. (2016). Fleeing cartels and Maras: international protection considerations and profiles from the northern triangle. Int. J. Refug. Law 28, 25–54. doi: 10.1093/ijrl/eev061
Rubini, E., Valente, M., Sguazzi, G., Trentin, M., Ragazzoni, L., and Gino, S. (2024). Forensic medical examination after CRSV: a scoping review of the literature. J. Forensic Leg. Med. 106:102736. doi: 10.1016/j.jflm.2024.102736
Rubini, E., Valente, M., Trentin, M., Facci, G., Ragazzoni, L., and Gino, S. (2023). Negative consequences of conflict-related sexual violence on survivors: a systematic review of qualitative evidence. Int. J. Equity Health 22:227. doi: 10.1186/s12939-023-02038-7
Sanjel, (2015). Gender-based violence: a crucial challenge for public health. Kathmandu Univ. Med. J. 11, 179–184. doi: 10.3126/kumj.v11i2.12499
Simonaggio, C., Rubini, E., Facci, G., Castagna, P., Canavese, A., Scotti, L., et al. (2024). Victims of drug facilitated sexual assault aged 13-24: a cross sectional study on the pool of users of a sexual violence relief Centre in northern Italy. Int. J. Legal Med. 138, 1593–1602. doi: 10.1007/s00414-024-03197-0
Simon-Butler, A., and Mcsherry, B., (2019). Defining sexual and gender-based violence in the refugee context. IRiS Work. Pap. Ser. Birm. Inst. Res. Superdiversity 2. University of Birmingham. Available at: https://socialequity.unimelb.edu.au/__data/assets/pdf_file/0020/3012176/Defining-Sexual-and-Gender-Based-Violence-in-the-Refugee-Context.pdf (Accessed August 28, 2024).
Sinai, J., (2008). How to define terrorism. Perspectives on Terrorism. Vol 2. Available at: https://www.universiteitleiden.nl/binaries/content/assets/governance-and-global-affairs/isga/perspectives-on-terrorism/2008-4.pdf (Accessed August 28, 2024).
Soria-Escalante, H., Alday-Santiago, A., Alday-Santiago, E., Limón-Rodríguez, N., Manzanares-Melendres, P., and Tena-Castro, A. (2022). “We all get raped”: sexual violence against Latin American women in migratory transit in Mexico. Viol. Women 28, 1259–1281. doi: 10.1177/10778012211013909
Spitzer, D. L., Torres, S., Zwi, A. B., Khalema, E. N., and Palaganas, E. (2019). Towards inclusive migrant healthcare. BMJ 366:l4256. doi: 10.1136/bmj.l4256
Starrs, A. M., Ezeh, A. C., Barker, G., Basu, A., Bertrand, J. T., Blum, R., et al. (2018). Accelerate progress—sexual and reproductive health and rights for all: report of the Guttmacher–Lancet commission. Lancet 391, 2642–2692. doi: 10.1016/S0140-6736(18)30293-9
Svallfors, S., Båge, K., Ekström, A. M., Elimian, K., Gayawan, E., Litorp, H., et al. (2024). Armed conflict, insecurity, and attitudes toward women’s and girls’ reproductive autonomy in Nigeria. Soc. Sci. Med. 348:116777. doi: 10.1016/j.socscimed.2024.116777
Swaine, A. (2015). Beyond strategic rape and between the public and private: violence against women in armed conflict. Hum. Rights Q. 37, 755–786. doi: 10.1353/hrq.2015.0043
Tan, S. E., and Kuschminder, K. (2022). Migrant experiences of sexual and gender based violence: a critical interpretative synthesis. Glob. Health 18:68. doi: 10.1186/s12992-022-00860-2
Tastsoglou, E., Petrinioti, X., and Karagiannopoulou, C. (2021). The gender-based violence and Precarity Nexus: asylum-seeking women in the eastern Mediterranean. Front. Hum. Dyn. 3:660682. doi: 10.3389/fhumd.2021.660682
Teichman, J. (1989). How to define terrorism. Philosophy 64, 505–517. doi: 10.1017/S0031819100044260
Trentin, M., Rubini, E., Bahattab, A., Loddo, M., Dellacorte, F., Ragazzoni, L., et al. (2023). Vulnerability of migrant women during disasters: a scoping review of the literature. Int. J. Equity Health 22:135. doi: 10.1186/s12939-023-01951-1
Trentin, M., Rubini, E., Facci, G., Ragazzoni, L., Valente, M., and Della Corte, F. (2024). The impact of the COVID-19 pandemic on migrant women in Milan, Italy: a qualitative study involving key informants working in third sector organizations and public hospitals. Int. J. Disaster Risk Reduct. 110:104658. doi: 10.1016/j.ijdrr.2024.104658
UN (2015). Transforming our world: the 2030 agenda for sustainable development. Available at: https://sdgs.un.org/publications/transforming-our-world-2030-agenda-sustainable-development-17981 (Accessed August 28, 2024).
UN (2022). 14th report of the United Nations secretary-general on conflict-related sexual violence January - December 2022 (S/2023/413).
UN Security Council (2023). Conflict-related sexual violence report of the secretary general (2023).
UNHCR (n.d.). Mediterranean situation/ Italy. Oper. Data Portal. Available at: https://data.unhcr.org/en/situations/mediterranean/location/5205 (Accessed July 15, 20.24).
UNHCR (n.d.). Access to healthcare. Available at: Available at: https://www.unhcr.org/what-we-do/protect-human-rights/public-health/access-healthcare (Accessed March 22, 2024).
US Department of State, Office to monitor and combat trafficking in persons (n.d.) 2023 trafficking in persons report: Libya. Available at: Available at: https://www.state.gov/reports/2023-trafficking-in-persons-report/libya/ (Accessed March 22, 2024).
Verelst, A., Bal, S., De Schryver, M., Say Kana, N., Broekaert, E., and Derluyn, I. (2020). The impact of avoidant/disengagement coping and social support on the mental health of adolescent victims of sexual violence in eastern Congo. Front. Psychol. 11:382. doi: 10.3389/fpsyt.2020.00382
WHO (2002). World report on violence and health. Available at: https://iris.who.int/bitstream/handle/10665/42495/9241545615_eng.pdf?sequence=1 (Accessed August 28, 2024).
WHO (2003). Guidelines for medico-legal care for victims of sexual violence. Available at: https://iris.who.int/bitstream/handle/10665/42788/924154628X.pdf?sequence=1&isAllowed=y (Accessed August 28, 2024).
WHO (2022). World report on the health of refugees and migrants. Available at: https://iris.who.int/bitstream/handle/10665/360404/9789240054462-eng.pdf?sequence=1 (Accessed August 28, 2024).
Keywords: conflict-related sexual violence, gender-based violence, sexual violence, conflict, migration
Citation: Rubini E, Trentin M, Valente M, Cenati S, Canavese A, Castagna P, Ragazzoni L and Gino S (2024) Migrant survivors of conflict-related sexual violence accessing a specialist health service in Turin, Italy: a qualitative analysis of clinical forensic interview transcripts. Front. Sociol. 9:1454700. doi: 10.3389/fsoc.2024.1454700
Edited by:
Jane Freedman, Université Paris 8, FranceReviewed by:
Fabio Perocco, Ca’ Foscari University of Venice, ItalyPaola Degani, University of Padua, Italy
Copyright © 2024 Rubini, Trentin, Valente, Cenati, Canavese, Castagna, Ragazzoni and Gino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elena Rubini, ZWxlbmEucnViaW5pQHVuaXVwby5pdA==