 Jacqueline I. M. Brigagão
Jacqueline I. M. Brigagão Roselane Gonçalves
Roselane Gonçalves Vanda L. V. D. Nascimento
Vanda L. V. D. Nascimento- 1Midwifery, Universidade de São Paulo, São Paulo, Brazil
- 2Psychology, Centro Universitário São Camilo, São Paulo, Brazil
- 3Psychology, Universidade Paulista, São Paulo, Brazil
The main factor for the hospitalization of childbirth was the expansion of power-knowledge in eighteenth century medicine. In Brazil, throughout the twentieth century, public policies for women's health focused care on biological and reproductive dimensions, and birth control technologies. Technoscience advances in producing knowledge and interventions regarding women's bodies led to a medicalization of labor and birth, consolidating the hospital as an ideal space. This article aims to examine numbers of surgical-cesarean births in the municipality of São Paulo, and to discuss how racial, cultural, social, and economic inequalities influence forms of birth. The statistics have been problematized in their connections with the language of risk, actors, and materialities involved in producing surgical births: public policies for pregnancy, labor, and post-natal care, hospitals. Research was carried out in the repository of public data on births in the municipality of São Paulo, in the period between 2010 and 2016, focusing on types of birth, in relation to place of birth, and women's race/color and levels of education. The analysis indicated that the majority of births are surgical-cesarean, at a number five times higher than that recommended by the World Health Organization; the number is even higher at private hospitals and among women who declared themselves as white or asian. Higher levels of education are also linked to this elevated number of births. Vaginal birth numbers were greater in public hospitals for women who declared themselves as black, mixed race, and native Brazilian. The language of risk guides public policies, delivery practices, and childbirth in Brazil. The lack of investment in birth centers in the country encourages hospitalization. Health professionals attending births have a central role in maintaining the culture of surgical delivery. Surgical-cesarean birth as a woman's choice is an argument based on childbirth myths, on incorrect information about physiological and psychological processes, and lack of support from health professionals and families faced with the desire for vaginal birth. The complexity of the situation demands recognition that these realities are built on several factors, interconnected in the day-to-day of health services.
Introduction
In Brazil, up to the nineteenth century, assistance during labor was carried out by midwives until the beginning of medical training schools. Education in Obstetrics was for a long time merely theoretical and then, in 1832, midwifery courses aimed at women began, linked to medical schools. From the mid nineteenth century, medical discourse begun to emphasize the importance of hospitalization, using as a justification the possible risks associated with homebirths, leading to the disqualification of midwives. Brazilian women, however, resisted hospitalization and medical care, since it was understood that hospitals were shelters for the poor. In addition, there was a lack of trust in the still-precarious medical practices, and they did not want to be examined by men (Mott, 1998; Meloni Vieira, 1999). At the same time, in a medical context, not much relevance was given to the field of Obstetrics; doctors were only supposed to participate in cases of delivery complications that demanded surgical expertise (Meloni Vieira, 1999).
During the twentieth century, despite all this resistance, births moved to hospitals and women care became a field dominated mainly by men. Midwives began to disappear from society, direct entry courses for midwives were closed down, and Obstetrics became a nursing specialization. In other words, after learning all hospital rituals and procedures, and graduating in Nursing, these professionals would study, on average, an extra year in Obstetrics. In 2005, there was an attempt to bring back the direct entry model for professional midwives, when the University of São Paulo created a Midwifery course. The midwives graduating from this course have faced a lot of resistance, both from professional Nursing and Medical bodies, and from the professionals who work in this area in the country, since the proposed model for qualifying these professional midwives represents a break with the hegemonic biomedical and hospital-based model (Castro et al., 2017).
In regard to Brazilian health policies, care for the population's health only entered the government's political agenda at the beginning of the twentieth century. The General Office of Public Health (Diretoria Geral de Saúde Pública) was created, focusing mainly on the control of health conditions in the urban centers of the country's Southeast region, the central pillar of the economy. Medical-hospital assistance at the time was offered by charity, philanthropic, and religious organizations, often named Holy Houses (Santas Casas). During the first decades of the twentieth century there was an economic transition within Brazilian society, which shifted from agrarian/exports to urban/industrial, encouraging the implementation of a health care system (Risi and Nogueira, 2002). The high rates of mother and child morbidity and mortality started to pose problems, since in order to supply the necessary labor force it was crucial to guarantee survival of the population.
In the 1920s, women's health became a core issue for the public policies that were solidified in government programs with the Sanitary Reform carried out by Carlos Chagas1. Care actions focused on biological and reproductive dimensions and on planning, as well as on organizing care, mobilizing around the so-called “maternal-infant” binomial. Between 1940 and 1965, by means of the National Children's Department (Departamento Nacional da Criança, or DNCR), an office created exclusively for organizing maternal-infant care, guidelines were established that aimed at integrating actions for the protection of motherhood, childhood, and adolescence with public health care programs in general. The department's educational project was linked to childcare, and for this reason it emphasized protection of motherhood and childhood (Nagahama and Santiago, 2005).
From 1964 to 1985, Brazil was governed by a military dictatorship. During this period, actions were all developed by the central government, and there was little discussion about women's rights, living conditions, and health. In the 1970s and 1980s, there was a heavy investment by international agencies in birth control technology. The resurgence of Neo-Malthusian ideas on the need for population growth control of the so-called “third world countries” in the South, allied to medical research on family planning and on social-cultural conditions, validated the medicalization of women's bodies (Meloni Vieira, 1999; Perpetuo and Wong, 2009). According to Barroso (1984), the most common contraceptive methods in the country were the birth control pill and sterilization surgery, both regulated by health professionals and not by women, and strongly associated with the economic interests of the following groups: multinational pharmaceutical industries, the private hospital network, group medicine, and family planning institutions such as the Family Welfare Civil Society (Sociedade Civil do Bem-Estar Familiar no Brasil, or BEMFAM). These groups, interested in selling their services, emphasized the technological advances, the efficiency, and the safety of these two contraceptive methods, minimizing the possible collateral effects on women's health. From the 1970s, female sterilization surgeries became popular in Brazil and began to be linked to surgical-cesarean delivery. In other words, in a context of private clinics and/or clinics that attend the population by means of private health insurance, women and their doctors often planned, during pre-natal care, sterilization procedures to be carried out after surgical births, as we will see next (Janowitz et al., 1982).
Until the 1980s, women's health programs in Brazil had been focused mainly on childbirth and were vigorously criticized, in the context of the Brazilian feminist movement, for the reductionist perspective from which these programs treated women, guaranteeing access to health care only during the pregnancy/post-natal cycle, and leaving them without care for most of their lives (Costa, 2005). Concurrently, at the end of the 1970s and beginning of the 1980s, the Brazilian Sanitary Movement began to question the health care system implemented by the government, which was organized to benefit only waged worker, leaving many people aside. This movement placed the relation between health and sickness processes and the population's living conditions at the heart of the debate.
Within this context, the National Health Conferences established the premises about the health system to be adopted during the country's re-democratization process. In 1984, pressured by organized civil society movements, such as those of women, syndicates, health professionals, and academics, the Ministry of Health created the Program for Integral Care for Women's Health (Programa de Atenção Integral à Saúde da Mulher), with the goal of including health care for women at all stages of their life cycle, respecting their rights to exercise or not maternity and reproduction. Programa de Atenção Integral à Saúde da Mulher envisaged that actions should be widely applied within the basic health care system. At the same time, as from the 1980s, the worldwide movement for childbirth humanization placed under discussion the importance of incorporating new paradigms in health care, considering holistic aspects and science-based care that prioritized safety and efficiency in childbirth care (Tornquist, 2003; Nagahama and Santiago, 2005).
Still in the 1980s, during the country's re-democratization process, the 1988 Constitution was enacted, establishing that health-related issues were a responsibility of the State and a right of citizens, and leading to the creation of the Brazilian Unified Health System (Sistema Único de Saúde) in 1990. SUS led to widespread changes in the public health in Brazil. This system is guided by three basic principles: universality, equity, and integrality. Universality guarantees access to public health services for all citizens; equity guarantees that the system will attend the specific needs of the different segments of the population; and integrality presumes that people will be cared for without fragmentation, in other words, as an integral whole (De Mattos, 2009; Spink et al., 2014).
It is worth pointing out that, although the sexual and reproductive rights discourse permeated the entire process of political construction of SUS, in the day-to-day of health services, however, very little advance has been made in respect to guaranteeing women's rights and autonomy over their own bodies, since investment in health continues to be centered on actions controlled by doctors. Most births are still hospitalized, and the most used contraceptive methods continue to be the pill and sterilization surgery (Perpetuo and Wong, 2009).
Another exacerbating factor in health care for women at a reproductive age is how matters pertaining to abortion are dealt with. Regarding the issue, Brazilian public policies have focused on repression and criminalization and not on care for women's health. The Brazilian legislation is harmful to women's physical and mental health, because it obliges them to turn to unsafe clandestine services or to carry out procedures on their own, by means of abortive medications such as misoprostol, exposing them to health risks (Diniz et al., 2017).
The expansion process of public health policies in Brazil has always been closely linked to the power-knowledge of medicine, encompassing not only people, but also the population (Foucault, 1988). In this context, the debate on the benefits and risks of vaginal birth and of surgical-cesarean delivery takes place in the arena of control and of life policies. The uses of language of risk in medicine “scientific discursivity” is used to justify the idea that the hospital is the safe place to delivery any birth. According to Foucault (1988), discursive fields are always linked to institutions and power strategies that reproduce social order and mechanisms to control population and bodies (Dictionary of social sciences, 2002; Correia, 2017).
As the so-called technoscience broadens knowledge, and intervention technologies are increasingly applied to women's bodies, there occurs in Brazil a wide dissemination of notions that were crucial in the process of medicalizing childbirth and in consolidating hospitals as the ideal location for delivery. These are: harm caused by delivery and the lack of capacity for giving birth; the concept of risk; the hospital as only safe place. These notions are based upon three false arguments: that women's bodies are not capable of giving birth, and therefore require medical technologies to facilitate delivery; that childbirth is a risky event for women and babies; and that that homes and birth centers are contaminated and unsafe places. These notions were disseminated by the media, by health professionals in general, by medical corporations, and by the state bodies that invested in building hospitals and maternities all over the country. In this manner, pregnancy began to be seen and treated as a pathological process and labor, consequently, as an event that requires sophisticated surgical technologies (World Health Organization, 1985; Brasil, 2004; Diniz, 2005). Following this line of thought, Foucault (2008) argues that, in capitalist societies, biopower affects the manners of functioning of bodies and that, from a bio-political point of view, technologies, as well as liberal practices, are mechanisms for applying discourses of truths on life, birth, and death.
In this scenario, the rates of surgical-cesarean births in Brazil rose exponentially in 1970 it was 14.60, in 1980 it was 31% (Faundes and Cecatti, 1991) and, in 2010, 52% of the total of births in the country were surgical-cesarean (Brasil, 2012). Haraway (1997, p. 307), when discussing the modulations and effects of the new reproductive technologies, states:
“Actually, for the middle- and upper-class Brazilian women in this town, modern scientific birth meant delivery by cesarean section rather than the new reproductive Technologies favored by their Northern sisters. Scheper-Hughes recounts watching young girls play at giving birth by enacting the imagined surgical scenario. After the successful play-birth the new infant was immediately put in on intravenous feedings! Regional newspapers report that cesarean section delivery rates among private maternity patients in northeastern Brazil approach 70 percent” (Scheper-Hughes, 1992, p. 329).
Despite all social, political, and economic changes that have occurred in the country over the past three decades, the ideas and interventions guided by what Donna Haraway calls technoscience have turned surgical-cesarean births into the “norm” for a great many women. This article has as its aim to examine the numbers of surgical-cesarean births in the city of São Paulo, which has the largest population and the greatest wealth in the country, in the period between 2010 and 2016, and discuss the manners in which racial, cultural, social, and economic inequalities are present in types of birth, as well as discussing and pointing out gaps in public policies aimed at encouraging vaginal birth that the Brazilian government seeks to implement. We chose this specific period because it was the most recent consolidated data available which was possible to observe the effects of public policies on Brazilian birth that were implemented during the presidency of Dilma Roussef, who was the first woman to become president in Brazil.
Materials and Methods
Research was carried out in the repository of public data on birth, known as the Live Birth Information System (Sistema de Informação sobre Nascidos Vivos—SINASC), of the municipality of São Paulo, examining the entries corresponding to the period between 2010 and 2016. SINASC is a database created to study circumstances of childbirth in Brazil, allowing researchers to characterize the profile of women who had live births in the country's different regions (Pedraza, 2012).
SINASC is open to public consultation, accessed by a municipal government site2. This repository has data fed into it by the health services that carry out hospital births and by civil registry offices for births that occur outside hospitals (homebirths or in other locations). The data obtained was organized in tables in order to allow descriptions and analyses3. The descriptors used for search within the repository were: type and year of birth; type of birth and mother's educational level; type of birth and mother's race; type of birth and hospital management model.
It is important to point out that in the repository women are described as mothers, however in this research we will use the term “women” as we believe that this expands the dimensions of the discussion.
Ethical Considerations
This investigation was performed according to public domain data without the possibility of identifying subjects, thereby dispensing with the need for approval by an institutional review board for human research.
Results
Brazil, the largest country in Latin America, with a territorial area of 8,515,759.090 square kilometers, and a population of ~208,542,623 million people, is a federation with 26 states, besides the Nation's administrative capital “the Federal District” and 5,570 municipalities (IBGE, 2018).
The state of São Paulo has a territorial area of 248,219.63 square kilometers and the largest number of inhabitants: 44,749,699 people. Among its municipalities, the city of São Paulo has the biggest population, with 11,696,088 million inhabitants, an area of 1,521.11 square kilometers, and a demographic density of 7,689.18 inhabitants per square kilometers. In 2016, the registered birth rate was of 14.43:1,000 inhabitants (SEADE, 2018).
For statistical data on labor and childbirth in the municipality of São Paulo, the database used was the SINASC repository. The descriptive analysis of data was centered around the period from 2010 to 2016, focusing on the following aspects: types of births carried out, type and place of birth (public and private hospitals, and the two birth centers), types of birth and race/color, and the woman's educational level in relation to different types of birth.
Types of Births Carried Out
In Table 1, the data relating to different types of birth taking place between 2010 and 2016 allows us to visualize the amount of vaginal and surgical-cesarean deliveries taking place in the city of São Paulo, besides those that are unknown.
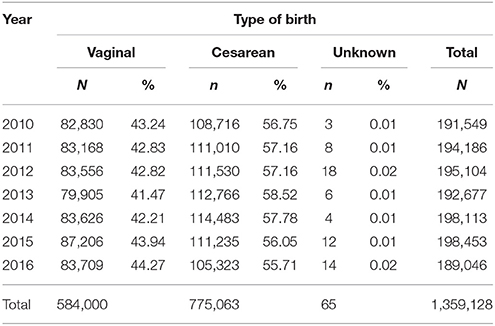
Table 1. Distribution of number and percentage of types of birth, between the years of 2010 and 2016, in the city of São Paulo Source: SINASC/CEInfo/SMS-SP, 2018.
A look at the number of vaginal births and of surgical-cesarean births carried out in the city of São Paulo, year by year, allows us to observe that the numbers remained stable with little variation. The year with the lowest number of surgical births in this period was 2016, with a total de 105,323 surgical-cesarean deliveries, equivalent to 55.71% of the total of births in the municipality. In the year of 2013 there were 112,766 surgical-cesarean births, corresponding to 58.52%, the highest number observed in the period studied. It is interesting to note that the majority of births occurred by means of surgical-cesarean delivery and these, from a Public Health viewpoint, are extremely high numbers that represent approximately five times more than the limit recommended by the World Health Organization. WHO established, in 1985, that the justifiable number for this procedure around the world should not be more than 10–15% of the total of births carried out (World Health Organization, 1985).
Regarding the Type of Birth and Places of Occurrence
Care during childbirth in Brazil predominantly occurs in hospitals. In the city of São Paulo there are 154 private hospitals and 60 public hospitals4 that register the births that take place in their facilities in SINASC. In the birth centers, delivery is always vaginal, due to the care model which relies on a team made up entirely of midwives and obstetric nurses. There are only two birth centers within the municipality5. The annual number of births that take place at the two birth centers is small, as demonstrated in Table 2.
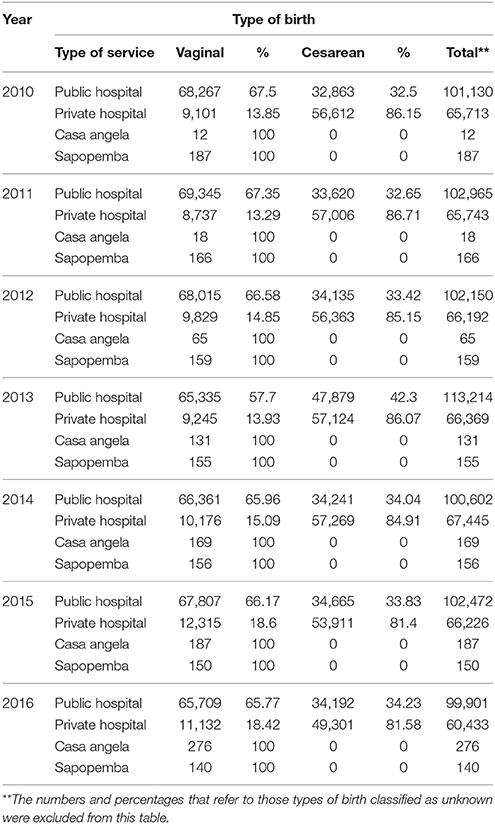
Table 2. Distribution of number and percentage of types of birth according to type of financing for care in the city of São Paulo, between the years 2010 and 2016 Source: SINASC/CEInfo/SMS-SP, 2018.
In Table 2, public hospitals represent the health care establishments with governmental funding, regardless of sphere of government (municipal or state), where services are completely free as they are funded by SUS. The hospitals described as private represent the health care establishments that attend the private health care network by means of health insurance (where women and their families and/or employers make monthly payments) and private institutions (those that take direct payment for services rendered).
As it is observed, the number of births carried out by the existing public services in the municipality is higher than the number of births carried out in private hospitals. However, even in public hospitals the number or surgical-cesarean births is high (over 30%) in all years. In private hospitals, the numbers of surgical-cesarean births are alarming, since they are over 80% in every year.
Regarding the Type of Birth and Race/Color6 of Women
In the city of São Paulo, women belong to different ethnic groups. The data in Table 3 indicates that the number of surgical-cesarean births is equally high in all groups.
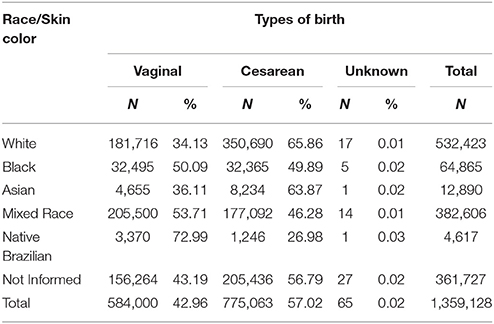
Table 3. Distribution of number and percentage of types of birth according to skin color of women attended within the city of São Paulo, between the years of 2010 and 2016 Source: SINASC/CEInfo/SMS-SP, 2018.
The data presented in Table 3 demonstrated that the rates for surgical-cesarean births in the population of women who declared themselves as White was 65.86%, followed by those who declared themselves Asian (63.87%). In São Paulo, there is a large community of East Asian descent, mainly of Japanese origin.
The number of vaginal births was higher for women who declared themselves black (50.09%), mixed race (53.71%), and native Brazilian (72.99%). These three groups include the majority of low-income women who are cared for by the public health network, as we will see next.
The group with the smallest number of surgical-cesarean births was that of native Brazilian women; it is important to point out that there are a number of families of indigenous origin scattered around the city, as well as three villages of the Guarani people at the outskirts of the municipality of São Paulo. Even among those indigenous women who have traditional cultural rituals regarding vaginal birth, the rate of surgical delivery was 26.98%, above the limit considered tolerable by the WHO (World Health Organization, 1985).
Regarding Women's Educational Levels in Relation to Types of Birth
Table 4 allows us to observe the distribution of types of birth within educational levels, showing that the higher the level of formal education of women, the higher the number of surgical-cesarean births, reaching 81.14% among women who finished high school or went to college.
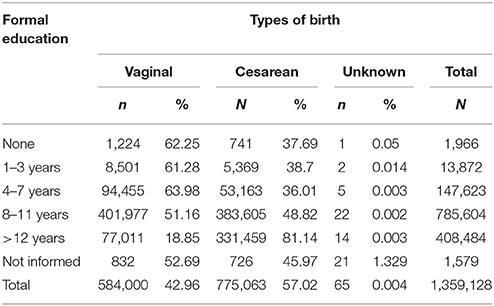
Table 4. Distribution of the number and percentage of types of birth according to educational level of women attended in the city of São Paulo, between the years of 2010 and 2016 Source: SINASC/CEInfo/SMS-SP, 2018.
The matter of educational level should be analyzed together with race/color and social and economic class. The data in this table confirms the numbers presented in the previous tables, in other words, in Brazil the number of surgical-cesarean births is high for all women, but within the group of white, middle/upper class women, who studied for longer and had economic resources that allowed them to pay for private insurance or services, the number was exorbitant.
Discussion and Conclusion
The permanence of this high rate of surgical-cesarean births in Brazil cannot be explained in a simplified manner. It is important to identify the multiple factors that contribute toward this situation, as well as to develop analytical strategies to expand the criticism about the ways in which technoscience have molded delivery and childbirth. As said by Haraway (1997), this type of analysis, which is focused on language, allows us to reach multiple dimensions that are presented to us in a hybrid way and in Woodward (2016): “The challenge is to unpack taken for granted assumptions, to disentangle what is natural, normal, normative, and empirically observable, in order to create new ways of understanding the intersection of different power axes, which retain a focus upon structural forces and social divisions” (p. 2).
The dissemination of high rates of surgical-cesarean births in Brazil, and the comparison with the directives of WHO directives, is a political strategy that has been used for some time, its effect seems limited and has not produced significant changes nor helped the process of informing the population of factors involved in surgical-cesarean births.
In this context, we have sought to problematize and understand the statistics in terms of their connections with the language of risk and with some of the main actors and materialities involved in the production of surgical births: the public policies for pregnancy, birth, and post-natal care; the hospital institutions; the health professionals who attend birth; and Brazilian women.
The language of risk has been present in Obstetric discourse since it was established as a scientific discipline in the field of medicine. Krakowski (2004), in his study on pathologizing pregnancy, points out that since before the 1930s, in the context of medical colleges, there were schools of thought that supported the pathological potential of childbirth and that indicated the “perils of birth,” both for the woman and the baby. This brought about an absence of women during deliveries, either in regard to the work performed by traditional midwives, or to the decreasing participation of women during labor (Mott, 2001; Rohden, 2002; Brigagão and Gonçalves, 2010).
Beginning in pregnancy, women are identified and labeled with a series of diagnostics that evaluate individual risks, based on personal characteristics such as race, genetic makeup, age, previous pregnancies, habits, and behaviors (Mahjouri, 2008). Evaluation of all these factors determines not only the “level of risk” of each woman, but also which monitoring strategy she will be subjected to. In this manner, the risks, the use of technologies in birth, and maternity are all quantified, accounted for, and thought of in probabilistic terms, with what Mahjouri (2008) denominates “technologically mediated pregnancy.”
Statistics and probabilities make up the discursive argument in the language of risk that sustains control strategies both for individuals and the population, since they are generally used to justify public policies (Spink, 2015). The health policies which address labor and birth are always in dialogue with the discourse of birth as a risky event. This explains the large investment in hospitals and the fact that the great majority of births occurring in the city of São Paulo take place in hospitals. Thus, the growth in number of hospitals and maternities is associated with the need to offer a safe place for the population, where the supposed risks are inexistent or can be controlled. From the point of view of brasilian health polices, this helps manage the lives of the population, for instance, by means of controlling fertility, birth rates, and childbirth. This power over the population's lives is achieved by producing truths about bodies that are naturalized and made essential. These are social constructions that medicine, in its scientific discourse, uses as a discourse strategy, reproduced by use of a number of institutional approaches (Foucault, 1988; Weeks, 2016).
In this process, doctors played a key role and, along with governments, established parameters and guidelines for birth. These notions were based on scientific descriptions of women's bodies as flawed, and of birth as a risky event (Martin, 1989; Rohden, 2002), and they are, in a Foucauldian sense, fixed to the “scientific discursivity” of the knowledge-power of medicine and doctors (Foucault, 1988).
Within this perspective, since women's bodies are seen as incapable, it becomes necessary to use medical technologies and interventions to correct this, so they may give birth in a manner that poses less risk for themselves and for the babies. Also, at the same time that scientific knowledge in pediatrics and neonatology advanced, a greater emphasis took place on the need for more doctors present during labor, as well as for specific technologies for newborns in a hospital context (Cardoso and Barbosa, 2012). Throughout time, the notion of birth as a risk event has taken on different forms and discourses, not always in an explicit manner, but which pervade many of the factors that lead to the hospitalization and medicalization of birth, and its transformation into an event that requires the use of “technoscience” tools (Haraway, 1997).
In Brazil, responsibility falls upon the federal government for formulating and following the execution of national health policies. The states are in charge of the more complex services, and of managing, formulating, and coordinating some policies. The municipalities are responsible for execution of actions and for carrying out direct services for the population. Thus, for the system to work, it is necessary for there to be interconnections between federal government, states, and municipalities (Abrucio and Franzese, 2007).
However, due to political and party issues, the states and municipalities often do not implement the policies created at the federal level. A good example of this lack of connectivity within the sphere of labor and birth was the attempt by the federal government to set up new birth centers. In 1999, the federal government created legislation that regulated the creation of birth centers all over the country. However, implementation of the centers did not advance; some of the main opposing forces were medical corporations and the Federal Council of Medicine (Conselho Federal de Medicina) who positioned themselves as radically against these health equipments, in a cooperative defense, since the law stated that, in these establishments, only midwives and obstetric nurses should assist delivery. The birth centers would be, accordingly, places that made vaginal birth without use of medical-hospital technologies possible. An example of the strategies used by the medical corporations in the country to boycott the implementation of other spaces destined for childbirth is recommendation by the Federal Council of Medicine (Conselho federal de medicina, 2012). This recommendation lists a series of arguments based on the notion of birth as an event of risk to women and babies and concludes that childbirth requires the safety of a hospital environment.
In the city of São Paulo, only two birth centers were implemented, both of which are small, in physical structure and in number of professionals. Although they are connected to SUS, the number of deliveries they carry out is tiny, as seen in Table 2, considering the total number of births that take place within the municipality. According to SINASC data, both birth centers together, in the period from 2010 to 2016, attendedo 1,971 births, out of a total of 1,359,128. In other words, only 0.1% of births occurring during the period. However, we must remember that these birth centers are important as they represent a resistance strategy for those women, midwives, and obstetric nurses who believe it is possible to implement a non-medicalized method for labor and delivery, and which respects the rights of women and their babies. Another strategy for resistance to the medicalization of birth in the municipality are the groups of health professionals who accompany homebirths; although they are few, they persist despite criticism from medical entities7.
Federal government's policies and guidelines over the past two decades explicitly encourage vaginal births in hospitals and are based on scientific evidence from the field of obstetrics. However, there has been no visible change in Brazil in the care model for women during labor and birth. We can confirm that they remain predominantly medicalized. In 2011, the government instituted a program named Stork Network (Rede Cegonha), with the aim of establish an interconnected network to guarantee women and children the right to health care during the pre-natal, labor and birth, post-natal, and infancy phases, at all SUS health services. The strategy for implementing and financing the Stork Network (Rede Cegonha) was based on training the professionals and health services that attend women and children. In addition, in the Rede Cegonha documentation, there is a clear recommendation for allowing low-risk vaginal births to be accompanied by midwives and obstetric nurses. Financial incentives included support for implementing the Centers for Vaginal Birth (Centros de Parto Normal) and the Centers for Pregnancy, Babies, and Post-Partum (Casas da Gestante, Bebê e Puérpera) (Brasil, 2012, 2014). Another strategy that this program tried to implement was producing manuals and guidelines for pregnancy, birth, and post-natal care, prioritizing care centered on women and their babies, and eliminating unnecessary interventions to women's bodies that often, as affirms Davies Floyd (2001), produce a ripple effect, in other words, one intervention leads to others.
It is important to note that Stork Network (Rede Cegonha) has many problems. From the beginning it was heavily criticized due to its name, which brings back into the public spotlight the traditional ideals of maternity, not as a right to be exercised, but as a biological destiny. In other words, it was not about women actively deciding on maternity, but about women “receiving the stork.” The name went against all the struggles of the different women's movements in the country, besides the feminists who defended broad health policies including all aspects of women throughout their lives. Another issue is that the main focus is hospital reform, and although reference is made to birth centers outside of hospitals, there is no investment in setting up these centers, let alone in fostering viable integration with teams who carry out homebirths within the public health network. In this manner, the policy effectively maintains and expands investments in hospital births.
Since the year 2000, there has been in Brazil a number of manuals and guidelines, based on scientific evidence and the so-called good obstetric practices, that seek to reduce the high number of surgical-cesarean births, breaking with hospital routines of excessive use of technologies and medication on women's bodies and on their babies. In this sense, it is possible to find midwives and obstetric nurses in public services caring for women during labor, which may explain the higher number of vaginal births in São Paulo's public network. But, even in the public network, where there are a series of regulations to guarantee that surgical-cesarean births will not be carried out without precise clinical reasons, the percentage of this type of birth is still over 30%, setting this indicator above the parameters established by WHO (World Health Organization, 1985). It is important to note that, despite scientific research in the field of “evidence-based medicine” having demonstrated how the excessive use of technologies during labor and birth is iatrogenic, these results have not resonated in Brazilian obstetric practices (Pasche et al., 2010). Although WHO guidelines have stated that childbirth is a physiological event, needing care and not control, the care model for birth in Brazil is still centered around the medical professional and is highly technocratic (Davies Floyd, 2001; Rabelo and Oliveira, 2010). Thus, we can affirm that the fact that the municipality of São Paulo has not invested in birth centers contributes greatly toward the high rates of surgical-cesarean births, since many of the births that could be vaginal become surgical in nature within the hospital context, with no justification based on scientific literature (Moreira et al., 2016).
In Table 2, it is possible to observe that the economic factor is also important, since over 80% of births that take place in private hospitals in the city of São Paulo are surgical-cesarean. Hopkins et al. (2014), in their study on the impact of payment source and hospital type upon rising cesarean section rates in Brazil, 1998–2008, found similar results, indicating that this is not a new tendency; on the contrary, this is a standard that is becoming more sophisticated over time. Some researchers explain this standard as the “cesarean section industry in Brazil” (Cardoso and Barbosa, 2012), others as the “cesarean culture” (Mandarino et al., 2009). Within this process, there is a clear commerce of health in private hospitals and of the obtainable profit, not just with the sale of medical services, but with a series of other products that are commercialized within the hospital context as part of the “labor package,” such as access to hospital technology resources, and the availability of restaurants, snack shops, beauty salons, and film and photography services inside hospitals (Nakano et al., 2016).
The use of technologies is not neutral as these both influence people and groups, and are in turn influenced and transformed as they are incorporated into daily life. In the case of surgical-cesarean births, both health professionals and women contribute so that this option remains as one of the main types of childbirth.
Research on the high numbers of surgical deliveries in private hospitals indicates that the economic dimension has an important role in the commitment of doctors to carrying out surgical-cesarean births (Hopkins, 2000; Poterr et al., 2003; Haddad and Cecatti, 2011; Hopkins et al., 2014; Hou et al., 2014). In public services and the supplementary network (health insurance), the values paid to obstetricians for assistance during vaginal births and surgical-cesarean births is the same, but in private practice there is no rule, and each obstetrician negotiates their fee with the women.
Looking at the economic past factors and the clientelist logic that guide the private health system in the country, a great majority of Brazilian doctors appear to believe that the higher the use of technology during labor and birth, the better the quality of care (Dias et al., 2008). This manner of thinking is adopted during undergraduate studies in medicine and strengthened during post-graduate obstetrics training.
Nakano et al. (2016), upon analyzing the three editions of the textbook Obstetrícia, by Jorge Resende, one of the most studied manuals in Brazilian universities, demonstrated that, in these, the debate on indications for surgical-cesarean birth moves away from clinical-obstetric recommendation criteria, to surgical birth planning, in order to eliminate the supposed risks of vaginal birth, and prioritizing the organization of the obstetrician's work time when choosing the ideal moment for the woman. In these books, surgical-cesarean births are described as having a prophylactic nature in relation to the supposed risks of vaginal birth.
In this manner, way, beginning from their university training, doctors are led to believe that the recommendation for surgical-cesarean delivery is not related to specific emergency situations, but instead it would be based on the doctor's ability to master surgical techniques, on the economy of time, and on the supposed desire of the woman when she requests a surgical-cesarean birth. Research on the reasons that lead obstetricians to recommend surgical-cesarean delivery suggests that they believe this is a birth that is planned, controlled, and directed by the doctor. Planned in the sense of predictability of actions during surgery, as well as organization of the professional's daily activities, since less time is spent on a surgical birth than in following a vaginal birth, so it is consequently more lucrative. Obstetricians affirm that mastering technical knowledge leads to safety during the procedure and the guarantee of a “good result,” since medical training favors surgery and the false idea that there is less risk for babies and mothers during the surgical-cesarean delivery.
Another argument often used in the 1980s and 1990s to justify surgical-cesarean births, both by women and by doctors, was that this made it easier to carry out sterilization surgery on women. To oppose this practice, Law 9.263 was issued on January 12th 1996, dealing with family planning and forbidding sterilization surgery to be carried out during surgical delivery. However, research shows that this practice was not abandoned in Brazil (Poterr et al., 2003; Carvalho et al., 2007; Castro et al., 2007). In addition to all of these reasons, obstetricians agree with the premise that this type of birth is not a medical recommendation in emergency cases, but a woman's “choice” (Faundes and Cecatti, 1991; Nakano et al., 2017).
Based on the Foucauldian perspective that power is relational, we must understand that women are not just defenseless victims of this system, but also wield power in the relationship with reproductive technologies and with health professionals, and are important agents in the increase of surgical births, as well as in the process of normalizing this type of birth in Brazil. In other words, health professionals and women construct together the reality of the surgical-cesarean birth; delivery is performed within the doctor-patient relationship, and realities are co-constructed in a partnership of interests (Martin et al., 2018). This highlights the importance of analyzing who these women are, and what are the reasons that lead them to surgical-cesarean births.
Brazil is a country full of inequality, and the black and mixed race population have the lowest levels of education and income, and use health services less (Travassos and Williams, 2004; Paixão et al., 2010). In order to understand the data on surgical deliveries, one must analyze the intersections between ethnic origins and education. It is not by chance that Table 3 shows that 65.86% of white women and 63.87% of women of East Asian origin had surgical births. And that, in Table 4, it is clear that 81.40% of women with 12 or more years of schooling, in other words, who finished high school and had access to higher education, and 48.82% of those with 8–11 years of schooling, had surgical-cesarean births. These women are those of higher social-economic class and who, in general, can pay for private health services. Research by the Applied Economic Research Institute (Instituto de Pesquisa Econômica Aplicada) on inequalities of gender and race in Brazil between 1995 and 2015, points out that, despite the expansion in access of Brazilians to higher education that occurred in recent years, distances between the ethnic-social-economic groups persist, since the white adult population with 12 years or more of schooling went from 12.50 to 25.90%. In the meantime, during the same time period, the black population with 12 years or more of schooling went from 3.30 to 12%; in other words, the difference in access for the two groups is still high (Instituto de Pesquisa Econômica Aplicada, 2018).
This makes the problem more complex, since the women from the country's economic elite with the highest levels of education, and who supposedly would be in an ideal position to negotiate types of birth with health professionals, are having surgical-cesarean births (Leal et al., 2009; Barros et al., 2011; Rattner and Moura, 2016).
One of the most disseminated arguments in the country, not just among obstetricians but in society as a whole, is that surgical-cesarean birth is a woman's choice. But, as Donna Haraway questions (Haraway, 1997, p. 192): “(…) choice is a term that has been incrusted by colonies of semiotic barnacles in the reproductive politics of the last quarter-century. What counts as a choice, for whom, and at what cost? What is the relation of ‘choice’ to ‘life’ and specially to ‘life’ itself”? In the case of surgical-cesarean birth, as demonstrated by Tables 3, 4, this possibility of choice is available only for the few Brazilians who can pay for surgical-cesarean births in the private system, in other words, this is more a result of social inequalities than of a supposed empowerment of women that would lead them to the conditions for making this choice. Riscado et al. (2016), in a recent revision of literature on decisions, choices, or preferences of type of birth in Brazil, found several studies that conclude that, in the private sector, a woman's “choice” is a result of the dialogues they establish with doctors during pre-natal care, when these doctors, either explicitly or implicitly, defend surgical delivery. These studies show that often women begin pre-natal care desiring a vaginal birth but, as their pregnancy progresses, obstetricians include the supposed perils of vaginal birth in their conversations during pre-natal visits, citing risks that the women already feared because they circulate in the social imaginary, such as “large babies” or “narrow hips.”
Although these arguments have no basis in scientific evidence, they continue to be present in medical discourse at pre-natal clinics, influencing women's options for surgical-cesarean births for fear of the “risks of birth.” Viellas et al. (2014) identified that the higher a woman's educational level, the greater the probability that they were attended by the same professional both in pre-natal care and in childbirth. The fact that in the private sector women traditionally carry out their pre-natal care with the same professional who will attend their delivery, establishing relationships of trust and admiration, serves in a way to strengthen this presupposed influence of doctors upon women's choices. Also, however highly educated the woman may be, relationships with specialists in matters of labor and childbirth are unequal, and power-knowledge is given to the doctor. Thus, analyses on surgical-cesarean births carried out “at the woman's request” demonstrate that these requests are carried out within a relational context with doctors, contributing toward naturalizing surgical-cesarean births in the private system, with many women adhering to this without question. According to Maureen O'Dougherty (2013), for Brazilian middle class women, surgical-cesarean births are the norm and vaginal birth is seen as alternative.
Another argument, present in specialized literature and in the social imaginary regarding the debate on choice of type of birth in Brazil, is that surgical-cesarean birth is an efficient strategy to preserve the vagina from supposed damage and from post-partum sexual dysfunctions. The fear of this supposed “damage” to the vagina is associated to factors such as a lack of understanding of a woman's body physiology and routine episiotomies often performed in vaginal births. Studies show that vaginal births with episiotomy can lead to a higher number of post-partum sexual dysfunctions (Hicks et al., 2004; Previatti and Souza, 2007; Progianti et al., 2008). However, some studies on post-natal sexuality have found no significant difference between women who had vaginal births and those who had surgical-cesarean deliveries (Klein et al., 2009; Belentani et al., 2011). Another fear of women is that of not being able to handle the pain associated with vaginal birth; a number of studies describe these fears and their associations with the images and stories that circulate in Brazil about vaginal birth in a family context, and in images divulged by the media, among others (Rodrigues and Siqueira, 2008; Pereira et al., 2011; Pinheiro and Lobo, 2012; Tostes and Seidl, 2016).
In this context, women's “choices” of surgical-cesarean births are based on the many myths and taboos on childbirth that circulate in Brazilian society, on the lack of correct information about the physiological and psychological processes involved in labor and birth, and also on the lack of support from health professionals and families when they express a desire for a vaginal birth (Zorzam, 2013; Copelli et al., 2015).
One of the limitations of this study is that it was carried out using only secondary statistical data present in the SINASC database. However, it is important to point out that this is a consistent database that allows a clear reading of how data was gathered.
The results of our analyses confirmed what several other studies cited throughout this work have been affirming over the last 20 years: that there is an abuse of surgical-cesarean births in Brazil, and that these have harmful effects on women's health, besides a potential for promoting complications that might not occur if these deliveries were carried out only when there were clinical-obstetric recommendations for them. Rattner and Moura (2016) points out that the high incidence of surgical-cesarean births was one of the contributing factors for Brazil not to reaching the 5th Millennium Development Goal8, which was to improve maternal health.
In our analysis, we sought to demonstrate that this is a complex reality which cannot be reduced to just one argument, such as that this is due to women's choices, or that the problem lies in the training of Brazilian obstetricians, or yet that it is due to the hospitalization of birth. On the contrary, we consider that it is all of these versions, connected in different ways in the day-to-day of health services that enact these realities.
At the same time we consider important to highlight that other studies of qualitative approach should be implemented considering their great potential to help deepen the understanding of the phenomena involving surgical surgical-cesarean births in Brazil.
Author Contributions
JB, RG, and VN contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
1. ^Carlos Chagas was one of the most recognized Brazilian sanitary physicians and bacteriologists. He discovered the American trypanosomiasis in 1909 and was director of the Department of Health in Brazil from 1920 to 1924.
2. ^http://tabnet.saude.prefeitura.sp.gov.br/cgi/deftohtm3.exe?secretarias/saude/TABNET/sinasc/nascido.def
3. ^The current form can be consulted at: http://www.prefeitura.sp.gov.br/cidade/secretarias/upload/saude/arquivos/publicacoes/Manual_DN_02fev2011.pdf
4. ^In this article we consider public all hospitals certified by SUS that attend births free of charge. Among these, many are private, but have agreements with the public health system, which pays for beds and services. In Brazil, the guarantee of universal access happens by means of implementation of public subsidiary strategies within the private sector. For a better understanding of this issue, see: SANTOS, Maria Angélica Borges dos; GERSCHMAN, Silvia. As segmentações da oferta de serviços de saúde no Brasil: arranjos institucionais, credores, pagadores e provedores. Ciênc. saúde coletiva, Rio de Janeiro, v. 9, n. 3, p. 795-806, Sept. 2004. Available online at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232004000300030&lng=en&nrm=iso. Accessed on February 23, 2018. http://dx.doi.org/10.1590/S1413-81232004000300030
5. ^The Sapopemba birth center has always been an equipment belonging to the Brazilian Unified Health System (SUS). Casa Angela is not a public equipment, and after an arduous struggle by the women and health professionals involved in the movement for humanization of birth, in 2015 the municipal government signed an agreement and included Casa Angela in SUS.
6. ^In this text we use the classification used by SINASC regarding race/color of Brazilian women. In Brazil, the classification of race adopted by official institutions is based on skin color and is self-determined; in other words, it is not up to researchers to attribute race to research subjects, but instead ask what race they consider themselves to be. The majority of the Brazilian population is of mixed race, which explains the high number of people who choose this option.
7. ^In São Paulo, the regional council of Medicine affirms by means of Ruling 142.401/10 that: “It is a consensus of this House, as also of FEBRASGO and the Brazilian Pediatrics Society, that vaginal births should be carried out in a hospital environment, aiming to prevent intercurrences from taking place during labor, by being able to be promptly attended.” Complete reference: http://www.cremesp.org.br/?siteAcao=Pareceres&dif=s&ficha=1&id=10813&tipo=PARECER&orgao=Conselho%20Regional%20de%20Medicina%20do%20Estado%20de%20S%E3o%20Paulo&numero=142401&situacao=&data=17-05-2012. To know more about the challenges faced by professionals who carry out homebirths see: Glauce Ferreira Soares. Caminhos e narrativas sobre a inserção profissional de obstetrizes no Brasil. Doctorate thesis. Interunidades Doctorate Program, Escola de Enfermagem da USP.
8. ^ The Millennium Development Goals (MDGs) were eight development goals that the United Nations estabilished in 2000 to be reached until the year 2015. Brazil was on of the countries that commited to achieve the MDGs and unfortunately was not able to improve maternal health and reach the 5th goal.
References
Abrucio, F. L., and Franzese, C. (2007). Federalismo e Políticas Públicas: O Impacto das Relações Intergovernamentais no Brasil. (São Paulo: Edições Fundap), 13–31.
Barros, A. J., Santos, I. S., Matijasevich, A., Domingues, M. R., Silveira, M., Barros, F. C., et al. (2011). Patterns of deliveries in a Brazilian birth cohort: almost universal cesarean sections for the better-off. Rev. Saúde Pública 45, 635–643. doi: 10.1590/s0034-89102011005000039
Barroso, C. (1984). Female sterilization: free choice and oppression. Rev. Saúde Pública 18, 170–180.
Belentani, L. M., Marcon, S. S., and Pelloso, S. M. (2011). Sexuality patterns of mothers with high-risk infants. Acta Paulista de Enfermagem 24 (1): 107–113. doi: 10.1590/S0103-21002011000100016
Brasil, K. (2004). Política Nacional de Atenção Integral à Saúde da Mulher: Princípios e Diretrizes. Ministério da Saúde. Available online at: http://bvsms.saude.gov.br/bvs/publicacoes/politica_nac_atencao_mulher.pdf
Brasil, K. (2012). Relatório Final do Plano de Qualificação das Maternidades e Redes Perinatais da Amazônia Legal e Nordeste/ Rede Cegonha. Ministério da Saúde. Available online at: http://www.scielo.br/scielo.php?script=sci_nlinks&pid=S1414-3283201400050109900018&lng=en
Brasil, K. (2014). Ministério da Saúde. Portaria: Institui diretrizes para a organização da atenção integral e humanizada ao recém nascido (RN) no Sistema Único de Saúde (SUS).
Brigagão, J., and Gonçalves, R. (2010). O uso das Teconologias em Obstetricia: Uma Leitura Crítica. In Fazendo Gênero 9, 11. Florianopólis. Available online at: http://www.fazendogenero.ufsc.br/9/resources/anais/1278302832_ARQUIVO_fg9_texto_completo%5BBrigagao;Goncalves%5D.pdf
Cardoso, J. E., and Barbosa, R. H. S. (2012). Disagreement between desire and reality: cesarean industry among middle class women in Rio de Janeiro, Brazil. Phys. Rev. Saúde Coletiva 22, 35–52. doi: 10.1590/S0103-73312012000100003
Castro, C., Cruz, E., Brigagão, J, Belli, M. A., Zarchi, N., Oliveira, R., et al. (2007). “A Formação de Profissionais para o Cuidado Integral a Saude da Mulher e da Criança no Pré-Natal, Parto e Pós-Parto: A Experiencia do Curso de Obstetricia da Universidade de São Paulo,” in Nascimento: Perspectivas Antropologicas, eds G. G. Dulce, C. Edemilson , P. Neide, and S. N. Ferreira (São Paulo: Icone editora), 301–318.
Carvalho, L. E. C, Osis, M. J. D., Cecatti, J. G., Bento, S. F., and Manfrinati, M. B. (2007). Esterilização cirúrgica voluntária na Região Metropolitana de Campinas, São Paulo, Brasil, antes e após sua regulamentação. Cad. Saúde Pública 23, 2906–2916. doi: 10.1590/s0102-311x2007001200012
Castro, C., Cruz, E., Brigagão, J., Belli, M. A., Zarchi, N., Oliveira, R., et al. (2017). “A Formação de Profissionais para o Cuidado Integral a Saude da Mulher e da Criança no Pré-Natal, Parto e Pós-Parto: A Experiencia do Curso de Obstetricia da Universidade de São Paulo,” in Nascimento: Perspectivas Antropologicas, eds D. Gualda, E. Campos, N. Praça, N. Salim, and G. Ferreira (São Paulo: Icone editora), 301.
Conselho federal de medicina (2012). Recomendação 1/2012. Conselho Federal de Medicina. Available online at: https://portal.cfm.org.br/images/Recomendacoes/1_2012.pdf
Copelli, F. H. S., Rocha, L., Zampieri, M. F. M., Gregório, V. R. P., and Custódio, Z. A. O. (2015). Determinants of women's preference for cesarean section. Texto e Contexto Enfermagem 24, 336–343. doi: 10.1590/0104-07072015000430014
Correia, T. (2017). Revisiting Medicalization: A Critique of the Assumptions of What Counts as Medical Knowledge. Front. Sociol. 2:14. doi: 10.3389/fsoc.2017.00014
Costa, A. A. (2005). O movimento feminista no Brasil: dinâmicas de uma intervenção política. Revista Labrys, Estudos Feministas/Études Féministes, Brasília, v.7.
Davies Floyd, R. (2001). The technocratic, humanistic and hoslistic paradigms of childbirth. Int. J. Gynecol. Obstetr. 75, S5–S23. doi: 10.1016/s0020-7292(01)00510-0
De Mattos, R. A. (2009). Princípios Do Sistema Único de Saúde (SUS) e a Humanização das Práticas de Saúde. Interface 13 (Suppl. 1), 771–780. doi: 10.1590/s1414-32832009000500028
Dias, M. A., Domingues, R. M., Pereira, A. P., Fonseca, S. C., da Gama, S. G., Theme Filha, M. M., et al. (2008). The decision of women for cesarean birth: a case study in two units of the supplementary health care system of the state of rio de janeiro. Ciência Saúde Coletiva 13, 1521–34. doi: 10.1590/S1413-81232008000500017
Dictionary of social sciences (2002). Dictionary of social sciences Edited by Craig Calhoun. Oxford University Press. (Accessed April 30, 2018). Available online at: http://www.oxfordreference.com/search?q=scientific+discursivity&searchBtn=Search&isQuickSearch=true
Diniz, D., Marcelo, M., and Alberto, M. (2017). Pesquisa Nacional de Aborto 2016. Ciência Saúde Coletiva 22, 653–660. doi: 10.1590/1413-81232017222.23812016
Diniz, S. (2005). Humanização da Assistência ao Parto no Brasil: Os Muitos Sentidos de Um Movimento. Ciência Saúde Coletiva 10, 627–637. doi: 10.1590/s1413-81232005000300019
Faundes, A., and Cecatti, J. G. (1991). A operação Cesárea no Brasil. Incidência, Tendências, Causas, Consequências e Propostas de Ação. Cadernos Saúde Publica 7, 150–173.
Foucault, M. (2008). Nascimento da biopolítica: curso dado no Collège de France (1978-1979), Transl. by E. Brandão (São Paulo: Martins Fontes).
Foucault, M. (1988). História da Sexualidade 1: a vontade de saber, Transl. by M. T. Albuquerque and, J. A. Guilhon Albuquerque (São Paulo: Paz and Terra).
Haddad, E. S. E. M., and Cecatti, J. G. (2011). Strategies Directed to Professionals for Reducing Unnecessary Cesarean Sections in Brazil. Revista Brasileira de Ginecologia and Obstetricia : Revista da Federacao Brasileira das Sociedades de Ginecologia e Obstetricia, 252–262. Available online at: http://repositorio.unicamp.br/bitstream/REPOSIP/199594/1/pmed_21860933.pdf
Haraway, D. J. (1997). Modest_Witness@Second_Millennium. FemaleMan_Meets_OncoMouse: Feminism and Technoscience. New York, NY: Routledge.
Hicks, T. L., Goodall, S. F., Quattrone, E. M., and Lydon-Rochelle, M. T. (2004). Postpartum sexual functioning and method of delivery: summary of the evidence. J. Midw. Women Health 49, 430–436. doi: 10.1111/j.1542-2011.2004.tb04437.x
Hopkins, K. (2000). Are Brazilian women really choosing to deliver by Cesarean? Soc. Sci. Med. 51, 725–740. doi: 10.1016/s0277-9536(99)00480-3
Hopkins, K., de Lima Amaral, E. F., and Mourão, A. N. (2014). The Impact of payment source and hospital type on rising cesarean section rates in Brazil, 1998 to 2008. Birthin Perinatal Care 41, 169–177. doi: 10.1111/birt.12106
Hou, X., Rakhshani, N. S., and Iunes, R. (2014). Factors associated with high cesarean deliveries in china and brazil - a call for reducing elective surgeries in moving towards universal health coverage. J. Hospital Admin. 3:67. doi: 10.5430/jha.v3n5p67
IBGE (2018). Instituto Brasileiro de Geografia e Estatística (IBGE). População. Portal do IBGE. (Accessed March 5, 2018). Available online at: https://www.ibge.gov.br/
Instituto de Pesquisa Econômica Aplicada, - IPEA. (2018). Retrato das Desigualdades de Gênero e Raça 1995 a 2015. Accessed March 6, 2018. Available online at: http://www.ipea.gov.br/portal/images/stories/PDFs/170306_retrato_das_desigualdades_de_genero_raca.pdf
Janowitz, B., Nakamura, M. S., Lins, F. E., Brown, M. L., and Clopton, D. (1982). Cesarean section in Brazil. Soc. Sci. Med. 16, 19–22.
Klein, K., Worda, C., Leipold, H., Gruber, C., Husslein, P., and Wenzl, R. (2009). Does the mode of delivery influence sexual function after childbirth? J. Women Health 18, 1227–1231. doi: 10.1089/jwh.2008.1198
Krakowski, L. (2004). História da Obstetrícia e a Patologização da Gravidez. Rio de Janeiro: Associação Nacional de História. [s/d]. Available online at: http://principo.org/a-histria-da-obstetrcia-e-a-patologizaco-da-gravidez.html
Leal, M., Gama, S. G. N., Domingues, R. N. S., Fonseca, S. C., Dias, M. A. B., Theme-Filha, M. M., et al. (2009). Cesarianas desnecessárias: causas, consequências e estratégias para sua redução,” in Regulação e modelos assistenciais em saúde suplementar: produção científica da Rede de Centros Colaboradores da ANS - 2006/2008, eds R. C. Pereira, and R. M. Silvestre (Brasília: Organização Pan-Americana da Saúde), 383–415.
Mahjouri, N. (2008). Techno-Maternity: rethinking the possibilities of reproductive technologies. In thirdspace. J. Femin. Theory Cult. 4, 6–12.
Mandarino, N. R., Chein, M. B. C., Júnior, F. G. M., Brito, L. M. O., Lamy, Z. C., Nina, V. J. S., et al. (2009). Aspectos Relacionados à Escolha do Tipo de Parto: Um Estudo Comparativo entre Uma Maternidade Pública e Outra Privada, em São Luís, Maranhão, Brasil. Cadernos Saúde Pública 25, 1587–1596. doi: 10.1590/s0102-311x2009000700017
Martin, D., Spink, M. J., and Pereira, P. P. G. (2018). Corpos múltiplos, ontologias políticas e a lógica do cuidado: uma entrevista com Annemarie Mol. Interface 22, 295–305. doi: 10.1590/1807-57622017.0171
Martin, E. (1989). The Woman in the Body: A Cultural Analysis of Reproduction. Milton Keynes: Open University Press.
Meloni Vieira, E. (1999). História, Política, Conceitos: a medicalização do corpo feminino. Scielo Books. Available online at: http://books.scielo.org/id/t4s9t/pdf/giffin-9788575412916-05.pdf
Moreira, B. R., Carvalho, P. L., Dutra, J. P., Coelho, P. B., Rocha, G. L., and Rocha, A. L. L. (2016). Determinants related to cesarean section in a public maternity hospital in the metropolitan region of belo horizonte-MG. Rev. Méd. Minas Gerais 26. doi: 10.5935/2238-3182.20160099
Mott, M. L. (1998). Parto, parteiras e parturientes no século XIX: Mme. Durocher e sua época. São Paulo: PhD Thesys - Faculdade de Filosofia, Letras e Ciências Humanas, Universidade de São Paulo, p.331.
Mott, M. L. (2001). Fiscalização e formação das parteiras em São Paulo (1880-1920). Rev. Esc. Enf. 35, 46–53. doi: 10.1590/S0080-62342001000100008
Nagahama, E. E. I., and Santiago, S. M. (2005). A institucionalização médica do parto no Brasil. Ciência Saúde Coletiva 10, 651–657. doi: 10.1590/S1413-81232005000300021
Nakano, A. R., Bonan, C., and Teixeira, L. A. (2016). Cesárea, Aperfeiçoando a Técnica e Normatizando a Prática. 2023 (21). História Ciências Saúde-Manguinhos 23, 155–172. doi: 10.1590/s0104-59702016000100010
Nakano, A. R., Bonan, C., and Teixeira, L. A. (2017). O trabalho de parto do obstetra: estilo de pensamento e normalização do “parto cesáreo” entre obstetras. Phys. Rev. Saúde Coletiva 27, 415–432. doi: 10.1590/s0103-73312017000300003
O'Dougherty, M. (2013). Plot and irony in childbirth narratives of middle-class Brazilian women. Med. Anthropol. Q. 27, 43–62.
Paixão, M. J., Rosseto, I., Montovanele, F., and Carvano, L. M. (2010). Relatório Anual Das Desigualdades Raciais no Brasil, 2009-10. Rio de Janeiro: Editora Garamond.
Pasche, D. F., Passos, E., and Hennington, E. A. (2010). Cinco anos da política nacional de humanização: trajetória de uma política pública. Ciência Saúde Coletiva 16 , 4541–4548. doi: 10.1590/s1413-81232011001200027
Pedraza, D. F. (2012). Qualidade do Sistema de Informações sobre Nascidos Vivos (SINASC): Análise Crítica da Literatura. Ciência Saúde Coletiva 17, 2729–2737.
Pereira, Rda, R., Franco, S. C., and Baldin, N. (2011). Pain and the protagonism of women in parturition. Rev. Brasil. Anestesiol. 61, 382–388. doi: 10.1016/s0034-7094(11)70045-9
Perpetuo, I., and Wong, L. (2009). “Desigualdade Socioeconômica na Utilização de Métodos Anticoncepcionais no Brasil: Uma Análise Comparativa com Base nas PNDS 1996 e 2006,” in Pesquisa Nacional de Demografia e Saúde da Criança e da Mulher PNDS 2006: Dimensões do Processo Reprodutivo e da Saúde da Criança. Ministério da Saúde e Centro Brasileiro de Análise e Planejamento, 87–105. Brasilia. Available online at: http://bvsms.saude.gov.br/bvs/publicacoes/pnds_crianca_mulher.pdf
Pinheiro, B., and Lobo, C. M. B. (2012). Percepções, expectativas e conhecimentos sobre o parto normal: relatos de experiência de parturientes e dos profissionais de saúde. Aletheia 212–227. Available online at: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1413–03942012000100015
Poterr, J. E., Perpétuo, I. H. O., Berquó, E., Hopkins, K., Leal, O. F., de Carvalho Formiga, M. C., et al. (2003). Frustrated demand for postpartum female sterilization. In:Brazil. Contraception 67, 385–390.
Previatti, J. F., and Souza, K. V. (2007). Episiotomia: em Foco a Visão das Mulheres. Rev. Bras. Enferm. 60, 197–201. doi: 10.1590/s0034-71672007000200013
Progianti, J. M., Araujo, L. M., and Mouta, R. J. O. (2008). Episiotomy repercussion on sexuality. Esc Anna Nery Rev Enferm 12, 45–49.
Rabelo, L., and Oliveira, D. (2010). Percepções de enfermeiras obstétricas sobre sua competência na atenção ao parto normal hospitalar. Rev. Escola Enfermagem 44, 213–220. doi: 10.1590/S0080-62342010000100030
Rattner, D., and Moura, E. C. (2016). Nascimentos no Brasil: associação do tipo de parto com variáveis temporais e sociodemográficas. Rev. Bras. Saude Mater. Infant. Recife 16, 39–47. doi: 10.1590/1806-93042016000100005
Riscado, L. C., Jannotti, C., and Barbosa, R. S. (2016). The route of delivery in Brazil: themes and trends in public health production. Texto Contexto Enferm 25, 2–10.
Risi, J., and Nogueira, R. P. (2002). “As condições de saúde no Brasil,” in Caminhos da saúde pública no Brasil, ed F. Jacob (Rio de Janeiro: Fiocruz), 117–234.
Rodrigues, A. V., and Siqueira, A. A. F. (2008). Sobre as dores e temores do parto: dimensões de uma escuta. Rev. Brasil. Saúde Materno Infantil 8, 179–186. doi: 10.1590/s1519-38292008000200005
Rohden, F. (2002). Ginecologia, gênero e sexualidade na ciência do século XIX. Horiz. Antropol. 8, 101–125. doi: 10.1590/s0104-71832002000100006
São Paulo, I. (2018). Secretaria Municipal da Saúde. Sistema de Informacao Sobre Nascidos Vivos – SINASC. (Accessed March 6, 2018). Available online at: http://www.prefeitura.sp.gov.br/cidade/secretarias/saude/epidemiologia_e_informacao/index.php?p=31247
Scheper-Hughes, N. (1992). Death Without Weeping; The Violence of Everyday Life in Brazil. Berkeley: University of California Press.
SEADE (2018). SEADE- Fundação SEADE Perfil dos Municípios Paulistas. (Accessed March 6, 2018). Available online at: http://www.perfil.seade.gov.br/
Spink, M. J. (2015). Clientes, cidadãos, pacientes: reflexões sobre as múltiplas lógicas de cuidado na atenção à saúde. Saúde e Sociedade 24(Suppl. 1), 115-123. doi: 10.1590/S0104-12902015S01010
Spink, M. J., Brigagão, J. I. M., and Nascimento, V. V. (2014). “Psicólogos no SUS: a convivência necessária com as políticas de saúde,” in Psicologia e políticas públicas: temas em debate, eds I. F. de Oliveira, O. Yamamoto (Belém: Ed. UFBA), 47–74.
Tornquist, C. S. (2003). Paradoxos da humanização em uma maternidade no Brasil. Cadernos Saúde Pública 19(Suppl. 2), S419–S427. doi: 10.1590/s0102-311x2003000800023
Tostes, N. A., and Seidl, E. M. F. (2016). Expectativas de gestantes sobre o parto e suas percepçães acerca da preparação para o parto. Temas Psicol. 24, 681–693. doi: 10.9788/tp2016.2-15
Travassos, C., and Williams, D. R. (2004). The concept and measurement of race and their relationship to public health: a review focused on Brazil and the United States. Cadernos Saúde Pública 20, 660–678. doi: 10.1590/s0102-311x2004000300003
Viellas, E. F., Domingues, R. M., Dias, M. A. B., Gama, S. G. M., Filha, M. M. T., Costa, J. V., et al. (2014). Prenatal care in Brazil. Cadernos Saúde Pública 30 (Suppl. 1). S85–S100.
Weeks, J. (2016). “O corpo e a sexualidade,” in O corpo Educado: Pedagogias da Sexualidade, eds G. L. Louro (Belo Horizonte: Autêntica), 35–84.
Keywords: women, childbirth, surgical-cesarean birth, vaginal birth, technoscience
Citation: Brigagão JIM, Gonçalves R and Nascimento VLVD (2018) The Language of Risk, Public Policies, and Childbirth in the Municipality of São Paulo: A Reading of Data From the Live Birth System 2010–2016. Front. Sociol. 3:12. doi: 10.3389/fsoc.2018.00012
Received: 11 March 2018; Accepted: 07 May 2018;
Published: 04 June 2018.
Edited by:
Kath Woodward, The Open University, United KingdomReviewed by:
Dawn Sarah Jones, Glyndwr University, United KingdomNicole Anderson, Brigham Young University, United States
Copyright © 2018 Brigagão, Gonçalves and Nascimento. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jacqueline I. M. Brigagão, amFjQHVzcC5icg==