 Cristina Camilo
Cristina Camilo Maria Luísa Lima
Maria Luísa Lima Rita Moura
Rita Moura Fátima Quintal2
Fátima Quintal2- 1Iscte-Instituto Universitário de Lisboa, CIS-Iscte, Lisbon, Portugal
- 2Universidade Federal do Paraná, Setor de Educação, Curitiba, Brazil
- 3Universidad de Barcelona, Departamento de Psicología Social y Psicología Cuantitativa, Barcelona, Spain
Introduction: It is well-known that social relationships positively impact health, but the direct and indirect ways these lead to better health outcomes remain understudied. Stemming from the concept of multiple levels of analysis, we address this problem by disentangling the links between different types of social relationships and health (including physical health, mental health, and well-being), and comparing the effects of multiple mediators based on two levels of analysis: interpersonal and group.
Methods: We propose a model that uses loneliness and social support as proxies of personal ties (mediators between close relationships and health), and social integration and multiple identities as proxies of group ties (mediators between group relationships and health). Likewise, we also propose a moderating effect of group identification on the association between group ties and health. We collected 848 responses through a self-report online survey and used structural equation modeling (SEM) analysis to assess the proposed model.
Results: Data yielded that close relationships are stronger predictors of better health outcomes than group relationships. Yet, more importantly, the results also provide strong evidence for the positive effects of the group-level variables. The effect of group relationships on health is significantly positive, and this association is stronger for those who identify more with their group.
Discussion: Our findings are closely aligned with the notion that increasing and improving people's social network is an effective way to contribute to better social determinants of health, while demonstrating that it is important to consider which type of relationship is being fostered.
1 Introduction
The notion that social relationships are an important asset for health has been endorsed by the World Health Organization (WHO) in its Conceptual Framework for the Social Determinants of Health (Solar and Irwin, 2010). The WHO framework recognizes that three main categories of social determinants significantly impact health and wellbeing: material (e.g., good living and working conditions), behavioral and biological (e.g., lifestyle behaviors), and the one under study, psychosocial, which includes social relationships. It should be noted, though, that social relationships and health are often conceptualized in a broad sense and inconsistent way. According to WHO (1948), health is a state of physical health, mental health, and social wellbeing. Despite being an often-cited definition, literature shows that health has been defined in several other ways, depending on the theoretical perspective taken (e.g., medical, psychological; see Seligman, 2011; Croom, 2015; Druten et al., 2023 for a review). In the present study, we consider three of the most frequently and widely assessed health domains, namely physical health, mental health, and subjective wellbeing, that have been shown to benefit greatly from positive social relationships (e.g., Lima et al., 2017). Research has been clear on the positive effects of the psychosocial determinants on multiple health outcomes, such as life expectancy (e.g., Holt-Lunstad et al., 2010), recovery from physical illness (e.g., Cohen and Syme, 1985; Cohen, 2005), promotion of mental health (e.g., Seeman, 1996; Cacioppo et al., 2006), and protection against cognitive decline in older age (e.g., Lövdén et al., 2005; Bennett et al., 2006; Haslam et al., 2014), which is why authors are calling attention to the importance of considering social isolation an urgent public health priority (e.g., Holt-Lunstad et al., 2017). Yet, the lack of a clear definition and measurement of social relationships hinders the advancement of knowledge in this study area. There is no consensus among studies on what is being considered as social relationships, as it is often used as an umbrella term that covers several associated psychosocial determinants (e.g., social ties, social support, social integration). We, however, defend that each of these determinants can, and should be, operationalized differently, which ultimately influences the way they are measured. Moreover, as we clarify further, social relationships can assume multiple forms (Holt-Lunstad, 2018), and the mechanisms linking these relationships to health can be quite diverse (Feeney and Collins, 2015).
Recently, the social capital notion has been used to explain the underlying processes in which social relationships benefit the different health domains. According to Bourdieu (1986) and Coleman (1994), social capital refers to the resources that result from close relationships and group belonging. Putnam (2000) took a step forward by proposing that social capital distinguishes between two types of relationships. First, bonding refers to reciprocal relationships and intimate and supportive forms of social connectedness (e.g., family and friends). These relationships entail deep interpersonal bonds, high social support, and loyalty (Jensen and Jetten, 2015; Hoffman et al., 2023). Second, bridging refers to casual relationships and relationships across group boundaries that provide external information of the immediate network and are based on mutuality that is central to shared identities (e.g., work hierarchies, Jetten et al., 2014; Hoffman et al., 2023). Distinguishing between these two types of social capital is important for understanding how the structural positions of individuals impact their health (see Uchino, 2004, 2009; Haslam et al., 2009; Jetten et al., 2012; Hoffman et al., 2023, for a review).
In this study, we address this problem by proposing and testing a model of how interpersonal and group-based social capital relationships impact health, following the concept of levels of analysis proposed by Doise (1986). According to the author, a way of unifying different conceptual approaches is to consider their levels of theoretical explanation (Doise, 1986; Doise and Valentim, 2015). This approach has been successfully applied to research in Social and Health Psychology (e.g., Murray, 2000; Bernardes et al., 2008), but has yet to be used to study the association between social relationships and health. Given that interpersonal (close) and group relationships are rarely differentiated in the literature despite their theoretical relevance, here we chose to focus specifically on these two levels of analysis. Following Doise (1986)'s framework, the interpersonal level refers to the interaction between individuals that occurs in a given context, for example, friendships, family ties, and other social ties that are deep and central to people's lives. The group level concerns the feeling of belonging to a collective entity, such as groups (e.g., hobbies), associations (e.g., sports), and organizations (e.g., political). From our perspective, the underlying processes associated with the two levels of relationships are different. Close relationships depend on disclosure, intimacy, care, and respect for unique attributes (Reis and Patrick, 1996), whereas group relationships are based on the synchronization of actions (e.g., Tunçgenç and Cohen, 2016), shared identity (e.g., Haslam et al., 2005), and a sense of responsibility to represent the group (e.g., McKimmie et al., 2019). Even though intimacy on the latter may be low, the perceived proximity and similarity of goals between group members is high, which leads to social integration. Thus, we can assume that the interpersonal level is closely linked to the bonding type relationships, where social mechanisms such as lower levels of loneliness and higher levels of social support can improve one's health (e.g., Uchino, 2009), and the group level is parallel to the bridging type relationships, in which higher levels of social integration and multiple identities also result in better health outcomes. Research carried out in other areas has already adopted a similar comparison framework, which reinforces our model proposal. For instance, Holt-Lunstad (2018), from a socio-ecological and systemic approach, proposes a differentiation between close relationships, occurring “over extended periods, emotionally laden, and characterized by idiosyncratic representations of others” (p. 439), and community relationships, that “extends to larger social contexts such as one's entire social network, neighborhood, or community” (p. 447). Our purpose is to distinguish the association between these two types of levels and social capital relationships and health.
1.1 Direct links between close and group relationships and health
The study of the impact of close relationships on health has a long tradition in Health Psychology. The work developed by Kiecolt-Glaser is a classic example of this line of research. The author typically studies couples, and her research shows that hostile marital relationships are detrimental to health because they increase the body's inflammatory response, diminish the immune response, and/or increase the time it takes to recover from wounds (see Kiecolt-Glaser et al., 2005; Kiecolt-Glaser and Wilson, 2017 for a review). In a complementary way, other authors have shown similar results. Couples with high-quality relationships showcase increased levels of oxytocin (Holt-Lunstad et al., 2014), and stable and intimate friendships predict happiness and better health outcomes (Holt-Lunstad, 2017; Dunbar, 2018). These effects tend to occur during personal, face-to-face interactions (Lima et al., 2017).
The impact of group relationships on health has been less explored, but existing evidence shows that participating in groups promotes social integration, social support, and a positive self-image that enhances the quality of life (Putnam, 1995; Rocco and Suhrcke, 2012). Moreover, Berkman and Syme (1979) showed that mortality is lower among those who participate in community life, and Cohen and Syme (1985) found a positive association between disease immunity and the number of social roles that a person plays. More recent research established a positive association between participation in associations and wellbeing (Fancourt and Steptoe, 2018), mental health (Seymour-Smith et al., 2017), and self-reported health (Gonzalez et al., 2020; Lima et al., 2021). Furthermore, shared group memberships impact health and wellbeing (Ysseldyk et al., 2018) by boosting individuals' self-esteem, belonging, meaning, sense of purpose, control, and efficacy in life (e.g., Cruwys et al., 2014; Greenaway et al., 2015; Jetten et al., 2017).
Previous work has aimed to compare the effects of close and group relationships on health, but we identified considerable gaps. An important meta-analysis (Gilbert et al., 2013) demonstrates that close relationships have a stronger impact on health than group relationships. Yet, none of the included studies simultaneously collected data from both levels of analysis (Doise, 1986; Doise and Valentim, 2015), thus not allowing a direct comparison. In a recent study, Gonzalez et al. (2020) showed that variables associated with personal relationships (e.g., interpersonal trust) are better predictors of self-reported health than social participation. But, while one of the variables referred to behavior (i.e., frequency of participation in associations), the other was an attitudinal variable, which, again, does not allow for a reliable comparison. As such, the first aim of our study is to directly compare the associations between close and group relationships and health using a similar predictor, that is, the estimation of the number of close and group relationships. Following previous research, we expect both levels of relationships to be positively associated with health, but we hypothesize a stronger association for closer relationships (H1).
1.2 Indirect links between social relationships and health
As we have briefly discussed, several psychosocial determinants are associated with better health outcomes in multiple ways (see Uchino, 2004, 2009; Haslam et al., 2009; Jetten et al., 2012, for a review). Reciprocal close relationships are associated with health because they represent a strong form of social control to decrease unhealthy behaviors (Wakefield et al., 2019), thus acting as social support, buffering the negative effect of stress on health, promoting positive emotions that strengthen the immune system, and providing the occasion to share important emotional events with significant others (Schwarzer and Knoll, 2007; Semmer et al., 2008). Uchino (2004) also defends that they help fight emotional loneliness. Similarly, group relationships act on health through different routes. For example, when people participate in community life and interact with others, there's an increase in awareness of social norms, which provides an opportunity to make social comparisons and gives access to relevant information, including health-related information (Uchino, 2009).
In this study, we advance this notion and test the mediating role of different psychosocial variables in the association between social relationships and health based on the selected levels of analysis. In particular, we use loneliness and social support as proxies of personal ties (mediators between close relationships and health), and social integration and multiple identities as proxies of group ties (mediators between group relationships and health).
On the interpersonal level (bonding), literature shows that loneliness, defined as the feeling of deficit in social relationships, influences health and wellbeing, and is associated with multiple poor health outcomes, for example, mental health problems (Meltzer et al., 2013), heart disease (Hawkley et al., 2003), and inflammatory responses (see Steptoe et al., 2004; Holt-Lunstad et al., 2010, for a review). Contrarily, social support, that is, people's beliefs about the quantity and quality of support potentially available to them, predicts mental health (e.g., Ozer et al., 2003), physical health (e.g., Nausheen et al., 2009), and wellbeing (e.g., Uchino et al., 1999; Uchino, 2009). On the group level (bridging), social integration is the subjective sense of belongingness to groups and bonding with others. This is based on recognizing the commonality of group ties and not upon interpersonal contact or mutual acquaintance among individuals (Haslam et al., 2017). Individuals who feel more connected to their community, neighborhood, or social groups are healthier and happier (Seeman, 1996; Berkman et al., 2000). The final mediator under study is multiple identities, which is the acknowledgment of the diversity of the social environments in which we live and act. Studies show that people with more social identities adapt better to life changes (e.g., retirement; Steffens et al., 2016), and are more physically resilient (Jones and Jetten, 2011).
Based on these findings, we expect the underlying processes that link these two types of relationships to health to be different. Close relationships are expected to positively influence health through a decrease in loneliness and an increase in social support (H2A), while group relationships are expected to positively influence health by increasing social integration and the number of multiple identities (H2B). Cacioppo and Patrick (2016) suggest that one of the ways to overcome loneliness is to join groups (e.g., dance, voluntary work) and develop close relationships within that space of social integration. It is also possible that good friends who share an interest (e.g., environmental protection) join others and create a group for it (e.g., clean beaches). So, we expect close and group relationships to be associated with and influence each other.
Finally, following the Social Identity Approach to Health (Haslam et al., 2009; Jetten et al., 2017; Ysseldyk et al., 2018) that suggests the active ingredient of group relationships that impact health is social identification, we also expect that the effects of group ties on health will be positively stronger for those with high levels of group identification (H3). Such identification is important to health assessment because the perception of similarity with others protects people from the impact of negative and stressful events (e.g., group-based discrimination; Jetten et al., 2017). We believe that in turn, this should amplify the effects of social integration on health.
2 Methods
2.1 Participants and procedure
We collected data from 848 individuals, of which 396 were from Portugal, 232 from Spain, and 318 from Brazil. The average age was roughly 44 years old (SD = 15.45). In total, 69.0% identified as female, 51.8% were married or in a civil union, and 55.7% had a university degree.
Our study was approved by the Iscte's Ethics Committee previous to its implementation. The data was collected online using a self-report survey on Qualtrics, shared via email and social media (e.g., Facebook), which resulted in a convenience non-probabilistic sample, collected with a “snowball” or “guided by the respondent” procedure. All participants gave their informed consent before answering the survey.
2.2 Measures
2.2.1 Close (bonding) relationships
We used the following two items to assess close relationships: “Approximately how many friends do you have?” (Helliwell and Huang, 2013), rated on response scale ranging from 1 (<5 friends) to 5 (more than 50 friends), and “How many persons do you have with whom you can discuss intimate and personal matters?” (European Social Survey, 2008), rated on response scale ranging from 1 (none) to 7 (10 or more). The first item was rescaled using the following rule: rescaled item = original item × 7 (maximum of the rescaled item) / 5 (maximum of the original item). The Pearson correlation between the two items was r (943) = 0.33, p < 0.001. The two items were then averaged to obtain the close relationships index.
Loneliness was assessed using four items from the USL-4-UCLA Loneliness Scale (short version, Russell et al., 1980), which includes items such as: “How often do you feel that people around you do not share your interests?,” rated on response scale ranging from 1 (never) to 5 (almost always). The four items were reversed and then averaged, resulting in the loneliness index (α = 0.78).
Social support was evaluated using four items from the short-range version of the Social Support Scale (Haslam et al., 2005; created from the dimensions identified by House, 1981). This scale includes items like: “To what extent do you think you have people with whom you can talk about your problems?” rated on a response scale ranging from 1 (not at all) to 5 (often). The social support index was calculated by computing the average of the four items (α = 0.79).
2.2.2 Group (bridging) relationships
We used the European Values Study (2008) to assess group relationships. We asked participants if they belonged to any groups out of a list of 11 types of groups (e.g., sports, religious, human rights, and political). For each type, participants could answer 1 (I don't belong), 2 (I belong but I'm not involved in group activities), and 3 (I belong, and I'm involved in group activities). We calculated the group relationship index by counting the number of groups to which participants belonged and were involved in group activities.
Social integration was assessed using two items retrieved from the social integration subscale of the Social Well-Being questionnaire (Keyes, 2007): “I feel close to the people that surround me” and “I am a member of my community,” both rated on response scale ranging from 1 (strongly disagree) to 5 (strongly agree). The Pearson correlation between the two items was r (941) = 0.39, p < 0.001. The two items were averaged to obtain the social integration index. The Social Well-Being questionnaire is a theoretically grounded scale used to evaluate the perceived quality of an individual's relationship with their society and community. Differently, the close relationships measure is a count of individuals' close relationships (European Social Survey, 2008). Nevertheless, item formulation between the two variables is very close. To overcome this, we tested the data for the collinearity assumption and found that multicollinearity was not a concern (Tolerance = 1.00, VIF = 1.00).
Multiple identities, that is, the extent to which people belonged to multiple social groups, were evaluated using three items adapted from Jetten et al. (2010) and Haslam et al. (2008): “I belong to many different groups”, “I participate in several different group activities,” and “I have friends from very different groups,” all rated on response scale ranging from 1 (strongly disagree) to 5 (strongly agree). The three items were averaged to calculate the multiple identities index (α = 0.67).
Group identification was measured using seven items adapted from the Social Identity Mapping procedure (Cruwys et al., 2014). This measure encompasses a suite of social identity constructs that are well correlated with the general way that people's self-concepts are based on their membership in social groups (Cruwys et al., 2014). The implemented items covered the following aspects: group importance, positivity, degree of group prototypically, group compatibility with other groups, identification with the group, meaning, and pride in belonging to the group (e.g., “from 0 to 10, indicate how representative do you think you are of what it means to be a member of the group”). Participants were asked to select the group they felt was most important to them and answer based on that group. Each item was rated on a response scale ranging from 1 (low identification) to 10 (high identification). All items were averaged, resulting in the group identification index (α = 0.80).
2.2.3 Health
To assess physical health, we used the item “How do you rate your health in general” (Eriksson et al., 2001), rated on a response scale ranging from 1 (very good) to 5 (very bad), and four additional items retrieved from the physical health dimension of the State of Health Questionnaire SF-36 (Ware and Sherbourne, 1992), as, “I seem to get sick a little easier than other people,” rated on response scale ranging from 1 (absolutely false) to 5 (absolutely true). The average of the five items resulted in the physical health index (α = 0.78).
Mental health was measured using nine items from the State of Health Questionnaire SF-36 (Ware and Sherbourne, 1992), such as “How often have you felt very nervous over the last 4 weeks?,” rated on a response scale ranging from 1 (never) to 5 (always). We calculated the mental health index by averaging the items (α = 0.89). Given the objectives of the study, we sought to use a quality-of-life measure focused on health, such as the SF-36, instead of a more general measure.
Wellbeing was evaluated using two items from the European Social Survey (Diener, 2000; Swift et al., 2014) focused on happiness (“Taking all things together, how happy would you say you are?”) and life satisfaction (“All things considered, how satisfied are you with your life as a whole nowadays?”), rated on a response scale ranging from 1 (unhappy or unsatisfied with life) to 10 (happy or satisfied with life). The Pearson correlation between the two items was r (946) = 0.80, p < 0.001. The two items were averaged to calculate the overall wellbeing index.
3 Results
3.1 Descriptive statistics
To understand the participants' network of relationships, central tendency, and dispersion measures were computed to summarize the data for the number of overall friends, close friends, and group relationships. The mean for the categorized number of friends was 4.40 (SD = 1.67); and the median value was 4.00 (IQR = 4.00, 5.00), meaning that half of the sample reported having between 10 and 30 friends. The mean for the categorized number of close friends was 4.21 (SD = 1.41); and the median value was 4.00 (IQR = 4.00, 5.00), revealing that 50% of the sample reported having between 3 and 6 intimate friends. The mean number of groups in which individuals were actively involved was 4.07 (SD = 3.75) and the median value was 4.00 (IQR = 4.00, 6.00), meaning that half of the sample reported being involved in between 4 and 6 groups).
Only loneliness did not correlate with group relationships. All remaining variables were positively associated with each other. The correlations were weak to moderate, indicating that different constructs were measured (see Table 1 for more details).
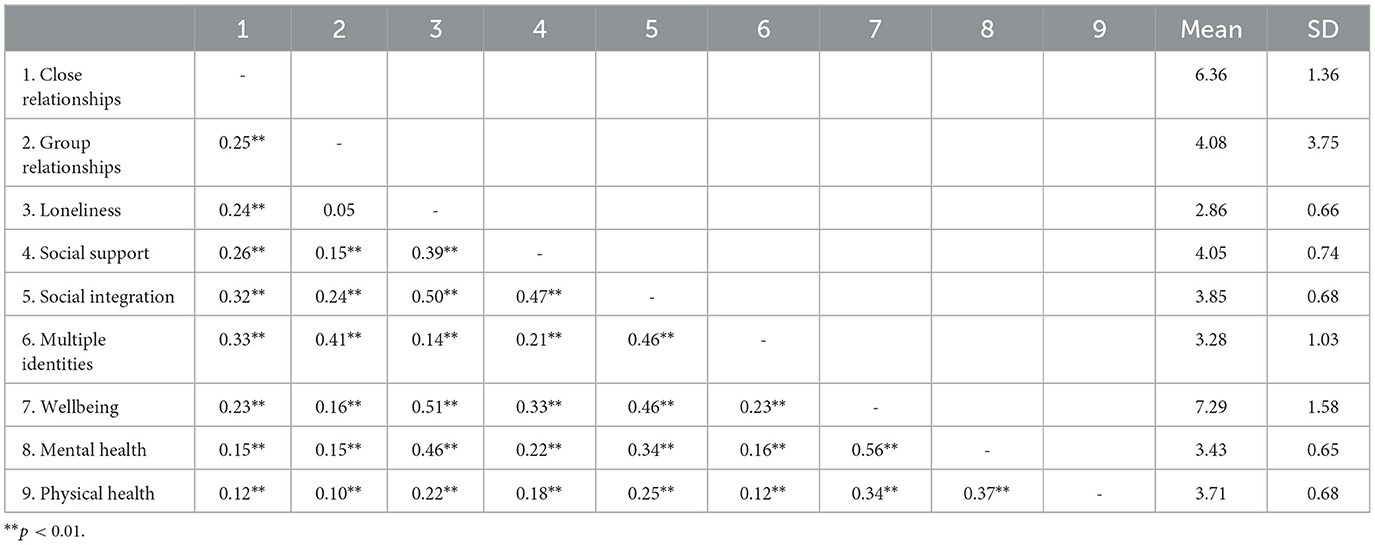
Table 1. Mean values, standard deviations, and bivariate correlations of study variables.
3.2 Links between social relationships and health
To test if close relationships are more strongly associated with health (including physical health, mental health, and wellbeing) than group relationships (H1), we used structural equation modeling (SEM) on AMOS 18.0 (see Figure 1). The same analysis was also used to test if close relationships are associated with health via personal ties composed of reserved loneliness and social support (H2a) and if group relationships are associated with health via group ties composed of social integration and multiple identities (H2b). Close and group relationships were entered as predictors of health, and loneliness, social support, social integration, and multiple identities as putative mediators for their respective levels of analysis. The model controlled for gender, age, and nationality, as literature shows that these variables tend to be highly associated with health outcomes (e.g., Deeks et al., 2009). No restrictions were imposed on the model. Following Baron and Kenny (1986) procedure, we conducted a bootstrapping method to evaluate the significance of the indirect effect.
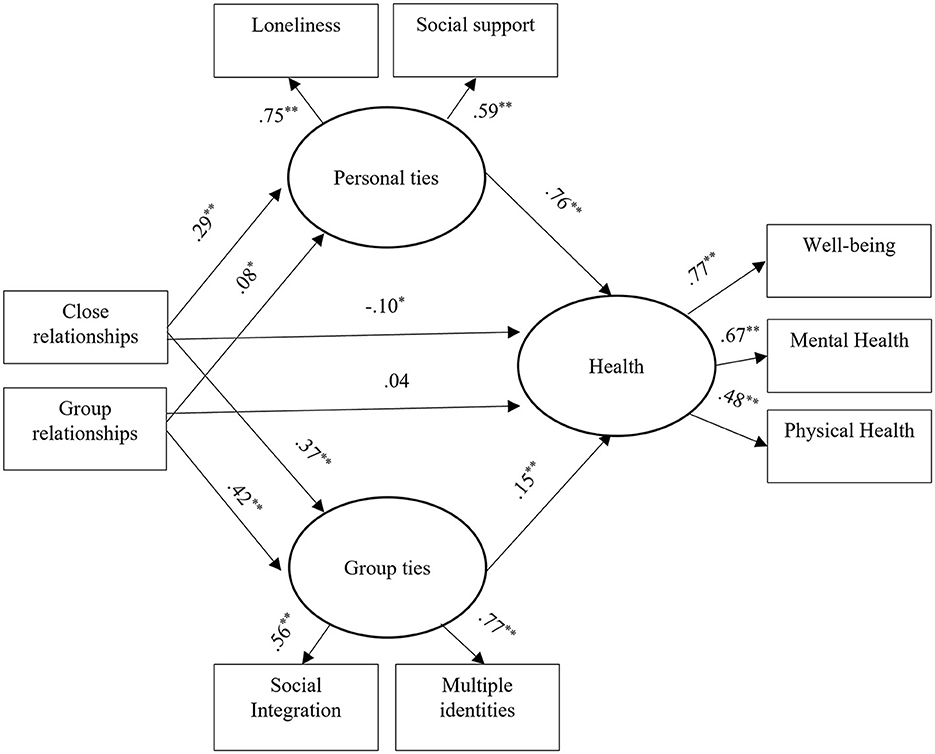
Figure 1. Links of close relationships and group participation with health and their mediators (SEM results). *p < 0.05, **p < 0.01.
To assess how well the model fits the data, RMSEA, CFI, and TLI were computed. The fit was overall good, χ2 = 127.51, DF = 26; χ2/DF = 4.90, NFI = 0.96; CFI = 0.97; RMSEA = 0.06, 90% CI [0.33, 0.41]). Both close and group relationships were significant direct predictors of health, β = 0.20, p ≤ 0.01, and β = 0.13, p ≤ 0.01, respectively. As hypothesized, close relationships had a stronger association with health than group relationships (H1). Likewise, the model also supported H2a and H2b. Personal ties significantly covaried with close relationships and health, and group ties significantly covaried with group relationships and health. We found positive and significant associations between friendship, personal ties, β = 0.29, p ≤ 0.001, and group ties β = 0.35, p ≤ 0.001, but only personal ties were positively and significantly related to health, β = 0.71, p ≤ 0.001. A similar but smaller effect was found for group relationships, which had a positive and significant association with personal and group ties, β = 0.45, p ≤ 0.001 and β = 0.05, p ≤ 0.05, correspondingly. Finally, the direct paths between close relationships and health and group relationships and health were reduced to non-significance when the mediators were included, β = −0.07 (n.s.) and β = 0.08 (n.s.), respectively.
The full mediation model accounted for 46% of the explained variance of health. The total regression weight, including direct and indirect effects, was β = 0.31, p ≤ 0.001, for the association between close relationships and health β = 0.25, p ≤ 0.001, for the association between group participation and health.
We found some significant results regarding the control variables. Nationality was significantly related to physical health, β = −0.15, p ≤ 0.001, and wellbeing, β = −0.11, p ≤ 0.001; gender was associated with mental health, β = 0.21, p ≤ 0.001; and age was related to mental health, β = 0.21, p ≤ 0.001 and well-being, β = 0.12, p ≤ 0.001.
3.3 Indirect link of group identification on health
We also tested the moderating role of group identification in the association between group ties and health (H3), using SEM on AMOS 18.0. The model revealed a good fit to the data, χ2 = 862.22, DF = 88; χ2/DF = 9.80, NFI = 0.85; CFI = 0.86; RMSEA = 0.10, 90% CI [0.09, 0.10], and again, gender, age, and nationality were controlled for (see Figure 2). Results supported H3, meaning that group identification significantly moderated the association between group ties and health. The positive impact of group ties on health is stronger for those that highly identify with their groups, β = −0.11, p ≤ 0.001. The moderated mediation model accounted for 47% of the explained variance of health.
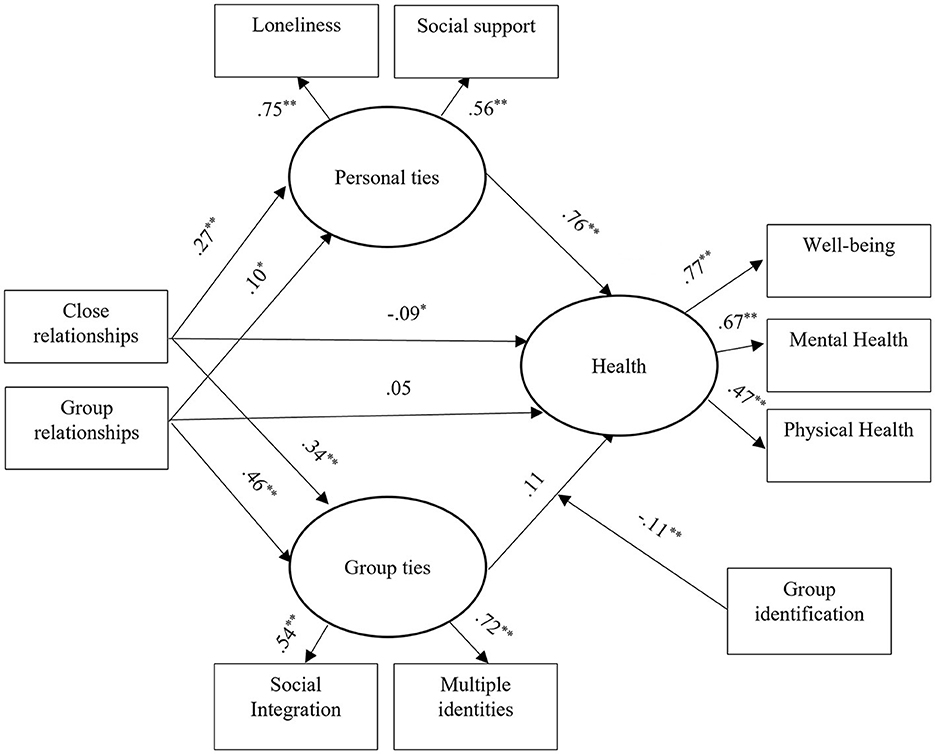
Figure 2. Group identification as a moderator in the association between group ties and health (SEM results). *p < 0.05, **p < 0.01.
As a validation check for our health operationalization, we ran three separate moderated mediation models with mental health, physical health, and wellbeing as outcome variables. The fit was overall good for the three models. Model fit was similar for mental health (NFI = 0.83; CFI = 0.84; RMSEA = 0.10), physical health (NFI = 0.83; CFI = 0.84; RMSEA = 0.10), or wellbeing (NFI = 0.84; CFI = 0.85; RMSEA = 0.10). The three models revealed that close relationships have significant associations with mental health, physical, and wellbeing, β = 0.50, p ≤ 0.01, β = 0.32, p ≤ 0.01, and β = 0.60, p ≤ 0.01, respectively. Also, we observed a significant moderated association between group ties and mental health, physical, and wellbeing, β = −0.05, p = 0.006, β = −0.07, p = 0.029, and β = −0.10, p = 0.018. In the three models, the positive impact of group ties was stronger for high identifiers with their groups.
4 Discussion
Social relationships have the ability to boost people's health. Previous research has tested the effect of close and group relationships (e.g., Slatcher and Selcuk, 2017; Smith and Weihs, 2019), but not in a direct comparison. Our study takes it a step further by directly comparing the direct and indirect ways close and group relationships impact physical health, mental health, and overall wellbeing. We found that both close and group relationships are significantly associated with better health. Yet, as we expected, close relationships appear to be a stronger predictor of health than group relationships, thus corroborating H1. These results are sound and were obtained while controlling gender, age, and nationality. This is particularly important because it was possible to replicate the pathways between social relationships and health in different geographical and cultural contexts.
A considerable amount of work has been dedicated to this study area, but surprisingly there is not much known about the indirect ways social relationships promote better health outcomes. For example, Farrell and Stanton (2019) defend that the mediating mechanisms remain understudied and that more evidence is needed to establish comparative mediators for different levels of social relationships. In our study, the unfolding of the mediators between close and group relationships and health reveals significant differences in the established links. Close relationships are associated with personal ties mediators, meaning that strong interpersonal relationships positively act on health because they can reduce loneliness and increase social support. Moreover, people's number of personal ties also impacts their perception of group ties, by increasing social integration and the number of multiple identities. Both results are an indication of the relative impact of close relationships on all the studied mediators. On the contrary, group relationships were the stronger predictor of group ties but revealed a weak link to personal ties. The effects of group ties seem to be more circumscribed and specific, as opposed to personal ties, which seem to be broader. These results are not exactly as hypothesized and reveal that close relationships have an impact on health through social and inter-individual factors, while group relationships impact health mainly through social factors.
Innovatively, our model considered the possibility of interdependence between interpersonal and group effects, which has been neglected in previous research (Häusser et al., 2020). Our adoption of the multiple-level analysis concept to study social relationships and health has shown that the two routes are independent but not separate, that is, better close relationships are strongly associated with loneliness and social support, but also with social integration and multiple identities. So, our hypotheses that close relationships are associated with health via reversed loneliness and social support (H2a), while group relationships are linked to health through social integration and multiple identities are only partially corroborated. Nonetheless, as we stated previously, there are several ways of articulation of the different levels of analysis since people can overcome loneliness by joining groups (Cacioppo and Patrick, 2016) or creating groups based on a common interest.
Finally, stemming from the Social Identity Approach to Health (Haslam et al., 2009; Jetten et al., 2017), we expected that the impact of group ties on health would be particularly strong for those with high levels of social identification (H3). Our model tested the moderating role of group identification, thus confirming that high group identifiers showed better health as compared to low identifiers. Once group identification changes the perception of received social support, such might account for this mediation (Häusser et al., 2020). Furthermore, group members interpret received social support via the identity-based relationships between those who give and receive support, so strongly identified group members tend to perceive group inputs more positively (Haslam et al., 2012).
Our study has limitations that need to be considered. First, as a cross-sectional study, our speculations regarding the causal links between social relationships and health should be viewed with caution. A longitudinal study would be particularly helpful to establish more robust links. Second, we only used self-reported health measures. We recommend future studies to combine subjective scales with more objective measures. Third, we recognize the lack of a real group-level measure in our model. As a way to facilitate the interpretation of the group identification measure, we asked participants to answer based on their most important group, which may have led to biased responses. Yet, it is quite challenging to measure this concept without referring to specific groups, and using a broader measure would generate more confusion and inconsistencies. Nevertheless, our ambition to establish a multilevel model would be more robust if we had been able to collect data that better reflects the group level of analysis. Fourth, our sample appears to be biased in the direction of higher education respondents which might have an effect on their social network and way of viewing it.
4.1 Final remarks
There are multiple types of social relationships, and all types appear to, under the right conditions, boost health and overall wellbeing. However, not all social relationships are equal, and not all act in the same way. The literature that focuses on this study area mostly assumes a partial version of the problem. In our study, we emphasized the importance of approaching the relationships-health links through a multilevel analysis perspective, which allowed us to compare the pathways by which our relationship with others positively impacts health. This is an approach of utmost importance that has yet to be consistently used to study the social determinants of health. We concluded, to different degrees, that close and group relationships are positively associated with health and the pathways between these types of relationships and health are different. Close relationships have a wide range of impacts and are associated with personal ties mediators, such as loneliness and social support, but also with group ties via social integration and multiple identities. However, group relationships have a more restricted spectrum of influence, and are strongly linked with group ties but weakly linked to personal ties. Finally, we also concluded that those with higher levels of group identification benefit more from the effects of strong group ties on health. We believe that these results are a step forward in our understanding of the fundamental connection between the integration of social groups and health.
Ultimately, our study is closely aligned with the notion that increasing and improving individuals' social network is a crucial health determinant, as defended by WHO (2017), while demonstrating that it is important to consider which type of relationship is being fostered. In the case of loneliness, for instance, it appears to be more fruitful to invest in close relationships. In the case of social support and integration, both types of relationships should be promoted. Following our results, psychosocial and health interventions and support groups, for instance, should not only foster group relationships, which tend to happen naturally in these circumstances, but also attempt to promote closer relationships (e.g., by involving a family member or a friend). Overall, social solutions (e.g., social prescribing) should become more globally used given their potential to boost people's health and reduce social and health iniquities.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of Iscte – Instituto Universitário de Lisboa. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CC: Conceptualization, Formal analysis, Methodology, Visualization, Writing—original draft, Writing—review & editing. ML: Conceptualization, Investigation, Methodology, Writing—original draft. RM: Formal analysis, Visualization, Writing—original draft, Writing—review & editing. FQ: Investigation, Methodology, Writing—original draft. MP-L: Investigation, Methodology, Writing—original draft.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Baron, R. M., and Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 51, 1173–1182. doi: 10.1037/0022-3514.51.6.1173
Bennett, D., Schneider, J., Tang, Y., Arnold, S., and Wilson, R. (2006). The effect of social networks on the relation between Alzheimer's disease pathology and level of cognitive function in old people: a longitudinal cohort study. Lancet Neurol. 5, 406–412. doi: 10.1016/S1474-4422(06)70417-3
Berkman, L., Glass, T., Brissette, I., and Seeman, T. (2000). From social integration to health: durkheim in the new millennium. Soc. Sci. Med. 51, 843–857. doi: 10.1016/S0277-9536(00)00065-4
Berkman, L., and Syme, S. (1979). Social networks and host resistance and mortality: a nine-year follow-up study of Alameda County residents. Am. J. Epidemiol. 109, 186–204. doi: 10.1093/oxfordjournals.aje.a112674
Bernardes, S., Keogh, E., and Lima, L. (2008). Bridging the gap between pain and gender research: a selective literature review. Eur. J. Pain 12, 427–440. doi: 10.1016/j.ejpain.2007.08.007
Bourdieu, P. (1986). “The forms of capital,” in Handbook of Theory and Research for the Sociology of Education, ed. J. Richardson (Westport, CT: Greenwood) 241–58.
Cacioppo, J., Hughes, M., Waite, L., Hawkley, L., and Thisted, R. (2006). Loneliness as a specific risk factor for depressive symptoms: Cross-sectional and longitudinal analyses. Psychol. Aging 21, 140–151. doi: 10.1037/0882-7974.21.1.140
Cacioppo, J., and Patrick, W. (2016). Loneliness: Human Nature and The Need for Social Connection. New York: W.W. Norton.
Cohen, S. (2005). Keynote presentation at the eight international congress of behavioral medicine: The Pittsburgh common cold studies: Psychosocial predictors of susceptibility to respiratory infectious illness. Int. J. Behav. Med. 12,123–131. doi: 10.1207/s15327558ijbm1203_1
Coleman, J. S. (1994). “Social capital, human capital, and investment in youth,” in Youth unemployment and society, eds. A. C. Petersen, and J. T. Mortimer (Cambridge: Cambridge University Press) 34–50. doi: 10.1017/CBO9780511664021.004
Croom, A. M. (2015). Music practice and participation for psychological well-being: a review of how music influences positive emotion, engagement, relationships, meaning, and accomplishment. Music Sci. 19, 44–64. doi: 10.1177/1029864914561709
Cruwys, T., Haslam, A., Dingle, G., Haslam, C., and Jetten, J. (2014). Depression and social identity. Pers. Soc. Psychol. Rev. 18, 215–238. doi: 10.1177/1088868314523839
Deeks, A., Lombard, C., Michelmore, J., and Teede, H. (2009). The effects of gender and age on health related behaviors. BMC Public Health 9, 213. doi: 10.1186/1471-2458-9-213
Diener, E. (2000). Subjective well-being – The science of happiness and a proposal for a national index. Am. Psychol. 55, 34–43. doi: 10.1037/0003-066X.55.1.34
Doise, W. (1986). Levels of Explanation in Social Psychology. Cambridge: Cambridge University Press.
Doise, W., and Valentim, J. (2015). “Levels of analysis in social psychology,” in International Encyclopedia of the Social and Behavioral Sciences ed. J. D. Wright (Amsterdam: Elsevier) 899–903. doi: 10.1016/B978-0-08-097086-8.24032-4
Druten, V.P., Bartels, E.A., van de Mheen, D., Vries, E., Kerckhoffs, A. P. M., and Nahar-van Venrooij, L. M. W. (2023). Concepts of health in different contexts: a scoping review. BMC Health Serv. Res. 22, 389. doi: 10.1186/s12913-022-07702-2
Dunbar, R. (2018). The anatomy of friendship. Trends Cogn. Sci. 22, 32–51. doi: 10.1016/j.tics.2017.10.004
Eriksson, I., Undén, A., and Elofsson, S. (2001). Self-rated health. Comparisons between three different measures. Results from a population study. Int. J. Epidemiol. 30, 326–333. doi: 10.1093/ije/30.2.326
European Social Survey (2008). ESS 4 - European Social Survey 2008. London: ESS. doi: 10.5878/002090
European Values Study (2008). European Values Study Longitudinal Data File 1981-2008 (EVS 1981-2008). GESIS Data Archive, Cologne. ZA4804 Data file Version 3.1. 0. doi: 10.4232/1.13486
Fancourt, D., and Steptoe, A. (2018). Community group membership and multidimensional subjective well-being in older age. J. Epidemiol. Commun. Health 72, 376–382. doi: 10.1136/jech-2017-210260
Farrell, A., and Stanton, S. (2019). Toward a mechanistic understanding of links between close relationships and physical health. Curr. Dir. Psychol. Sci. 28, 483–489. doi: 10.1177/0963721419855657
Feeney, B., and Collins, N. (2015). A new look at social support: a theoretical perspective on thriving through relationships. Pers. Soc. Psychol. Rev. 19, 113–147. doi: 10.1177/1088868314544222
Gilbert, K., Quinn, S., Goodman, R., Butler, J., and Wallace, J. (2013). A meta-analysis of social capital and health: a case for needed research. J. Health Psychol. 18, 1385–1399. doi: 10.1177/1359105311435983
Gonzalez, R., Fuentes, A., and Muñoz, E. (2020). On social capital and health: The moderating role of income inequality in comparative perspective. Int. J. Sociol. 50, 68–85. doi: 10.1080/00207659.2019.1709138
Greenaway, K., Haslam, A., Cruwys, T., Branscombe, N., Ysseldyk, R., and Heldreth, C. (2015). From “we” to “me”: Group identification enhances perceived personal control with consequences for health and well-being. J. Pers. Soc. Psychol. 109, 53–74. doi: 10.1037/pspi0000019
Haslam, A., Jetten, J., Postmes, T., and Haslam, C. (2009). Social identity, health and well-being: An emerging agenda for applied psychology. Appl. Psychol. 58, 1–23. doi: 10.1111/j.1464-0597.2008.00379.x
Haslam, A., O'Brien, A., Jetten, J., Vormedal, K., and Penna, S. (2005). Taking the strain: Social identity, social support, and the experience of stress. Br. J. Soc. Psychol. 44, 355–370. doi: 10.1348/014466605X37468
Haslam, A., Reicher, S., and Levine, M. (2012). “When other people are heaven, when other people are hell: how social identity determines the nature and impact of social support”, in The social cure: Identity, health, and well-being, eds. J. Jetten, C. Haslam, A. Haslam (London: Psychology Press) 157–174.
Haslam, C., Cruwys, T., Haslam, A., and Jetten, J. (2017). “Social connectedness and health”, in Encyclopedia of Geropsychology, ed. N. A. Pachana (Singapore: Springer). doi: 10.1007/978-981-287-082-7_46
Haslam, C., Haslam, A., and Jetten, J. (2014). “The social determinants of cognitive change: Identity processes as the source of both enhancement and decline,” in The Psychology of Change: Life contexts, experiences, and identities, eds. K. J. Reynolds and N. R. Branscombe (London: Psychology Press) 133–150.
Haslam, C., Holme, A., Haslam, A., Jetten, J., Bevins, A., Ravenscroft, S., et al. (2008). The social treatment: benefits of group reminiscence and group activity for the cognitive performance and wellbeing of older adults in residential care. Psychol. Aging 25, 157–167. doi: 10.1037/a0018256
Häusser, J., Junker, N., and Dick, R. (2020). The how and the when of the social cure: a conceptual model of group- and individual-level mechanisms linking social identity to health and well-being. Eur. J. Soc. Psychol. 50, 721–732. doi: 10.1002/ejsp.2668
Hawkley, L., Burleson, M., Berntson, G., and Cacioppo, J. (2003). Loneliness in everyday life: cardiovascular activity, psychosocial context, and health behaviors. J. Pers. Soc. Psychol. 85, 105–120. doi: 10.1037/0022-3514.85.1.105
Helliwell, J., and Huang, H. (2013). Comparing the happiness effects or real and on-line friends. PLoS ONE 8, e72754. doi: 10.1371/journal.pone.0072754
Hoffman, A., Mehrpour, A., and Staerklé, C. (2023). “The many faces of social connectedness and their impact on well-being,” in Withstanding Vulnerability Throughout Adult Life, eds. D. Spini, and E. Widmer (Singapore: Palgrave Macmillan) 169–187. doi: 10.1007/978-981-19-4567-0_11
Holt-Lunstad, J. (2017). “Friendship and health,” in The Psychology of Friendship, eds. M. Hojjat, and A. Moyer (Oxford: Oxford University Press) 233–248. doi: 10.1093/acprof:oso/9780190222024.003.0014
Holt-Lunstad, J. (2018). Why social relationships are important for physical health: A systems approach to understanding and modifying risk and protection. Annu. Rev. Psychol. 69, 437–458. doi: 10.1146/annurev-psych-122216-011902
Holt-Lunstad, J., Birmingham, W., and Light, K. (2014). Relationship quality and oxytocin. J. Soc. Pers. Relat. 32, 472–490. doi: 10.1177/0265407514536294
Holt-Lunstad, J., Robles, T., and Sbarra, D. (2017). Advancing social connection as a Public Health priority in the United States. Am. Psychol. 72, 517–530. doi: 10.1037/amp0000103
Holt-Lunstad, J., Smith, T. B., and Layton, J. (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Med. 7, e316. doi: 10.1371/journal.pmed.1000316
Jensen, D. H., and Jetten, J. (2015). Bridging and bonding interactions in higher education: Social capital and students' academic and professional identity formation. Front. Psychol. 6, 126. doi: 10.3389/fpsyg.2015.00126
Jetten, J., Haslam, A., Cruwys, T., Greenaway, K., Haslam, C., and Steffens, N. (2017). Advancing the social identity approach to health and well-being: Progressing the social cure research agenda. Eur. J. Soc. Psychol. 47, 789–802. doi: 10.1002/ejsp.2333
Jetten, J., Haslam, C., and Haslam, A. (2012). “The case for a social identity analysis of health and well-being”, in The social cure: Identity, health, and well-being, eds. J. Jetten, C. HaslAm. and A. HaslAm (London: Psychology Press) 3–19. doi: 10.4324/9780203813195
Jetten, J., Haslam, C., Haslam, S. A., Dingle, G., and Jones, J. M. (2014). How groups affect our health and well-being: the path from theory to policy. Soc. Issues Policy Rev. 8, 103–130. doi: 10.1111/sipr.12003
Jetten, J., Haslam, C., Pugliese, C., Tonks, J., and Haslam, A. (2010). Declining autobiographical memory and the loss of identity: effects on well-being. J. Clin. Exp. NeuroPsychol. 32, 408–416. doi: 10.1080/13803390903140603
Jones, J., and Jetten, J. (2011). Recovering from strain and enduring pain: multiple group memberships promote resilience in the face of physical challenges. Soc. Psychol. Personal Sci. 2, 239–244. doi: 10.1177/1948550610386806
Keyes, C. (2007). Promoting and protecting mental health as flourishing: a complementary strategy for improving national mental health. Am. Psychol. 62, 98–108. doi: 10.1037/0003-066X.62.2.95
Kiecolt-Glaser, J., Loving, T., Stowell, J., Malarkey, W., Lemeshow, S., Dickinson, S. L., et al. (2005). Hostile marital interactions, proinflammatory cytokine production, and wound healing. AMA Arch. Gen. Psychiatry 62, 1377–1384. doi: 10.1001/archpsyc.62.12.1377
Kiecolt-Glaser, J., and Wilson, S. (2017). Lovesick: couples' relationships and health. Ann. Rev. Clin. Psychol. 13, 421–443. doi: 10.1146/annurev-clinpsy-032816-045111
Lima, L., Camilo, C., Quintal, F., and Palacin-Lois, M. (2021). It is not enough to be a member: conditions for health benefits in associative participation. International Journal of Social Psychology 36, 458–486. doi: 10.1080/02134748.2021.1942682
Lima, L., Marques, S., Muiños, G., and Camilo, C. (2017). All you need is Facebook friends? Associations between online and face to face friendships and health. Front. Psychol. 8, 68. doi: 10.3389/fpsyg.2017.00068
Lövdén, M., Ghisletta, P., and Lindenberger, U. (2005). Social participation attenuates decline in perceptual speed in old and very old age. Psychol. Aging 20, 423–434. doi: 10.1037/0882-7974.20.3.423
McKimmie, B. M., Butler, T., Chan, E., Rogers, A., and Jimmieson, N. L. (2019). Reducing stress: social support and group identification. Group Proc. Inter. Relat. 23, 241–261. doi: 10.1177/1368430218818733
Meltzer, H., Bebbington, P., Dennis, M. S, Jenkins, R., McManus, S., and Brugha, T. S. (2013). Feelings of loneliness among adults with mental disorder. Soc. Psychiat. Psychiatr. Epidemiol. 48, 5–13. doi: 10.1007/s00127-012-0515-8
Murray, M. (2000). Levels of narrative analysis in health psychology. J. Health Psychol. 5, 337–347. doi: 10.1177/135910530000500305
Nausheen, B., Gidron, Y., Peveler, R., and Moss-Morris, R. (2009). Social support and cancer progression: a systematic review. J. Psychosom. Res. 67, 403–415. doi: 10.1016/j.jpsychores.2008.12.012
Ozer, E., Best, S., Lipsey, T., and Weiss, D. (2003). Predictors of posttraumatic stress disorder and symptoms in adults: a meta-analysis. Psychol. Bull. 129, 52–73. doi: 10.1037/0033-2909.129.1.52
Putnam, R. D. (1995). Bowling alone: America's declining social capital. J. Democr. 6, 65–78. doi: 10.1353/jod.1995.0002
Putnam, R. D. (2000). Bowling alone: The collapse and revival of American community. Touchstone Books/Simon and Schuster. doi: 10.1145/358916.361990
Reis, H., and Patrick, B. (1996). “Attachment and intimacy: component processes,” in Social psychology: Handbook of basic principles, eds. E. Higgins and A. Kruglanski (New York: Guilford Press), 523–563.
Rocco, L., and Suhrcke, M. (2012). Is Social Capital Good for Health? A European Perspective. WHO Regional Office for Europe. Copenhagen: World Health Organization.
Russell, D., Peplau, L., and Cutrona, C. (1980). The revised UCLA loneliness scale: concurrent and discriminate validity evidence. J. Person. Soc. Psychol. 39, 472–480. doi: 10.1037/0022-3514.39.3.472
Schwarzer, R., and Knoll, N. (2007). Functional roles of social support within the stress and coping process: a theoretical and empirical overview. Int. J. Psychol. 42, 243–252. doi: 10.1080/00207590701396641
Seeman, T. (1996). Social ties and health: the benefits of social integration. Ann. Epidemiol. 6, 442–451. doi: 10.1016/S1047-2797(96)00095-6
Seligman, M. E. P. (2011). Flourish: A Visionary New Understanding of Happiness and Wellbeing. London: Free Press.
Semmer, N. K., Elfering, A., Jacobshagen, N., Perrot, T., Boos, N., and Beehr, T. (2008). The emotional meaning of instrumental social support. Int. J. Stress Manage. 15, 235–251. doi: 10.1037/1072-5245.15.3.235
Seymour-Smith, M., Cruwys, T., Haslam, A., and Brodribb, W. (2017). Loss of group memberships predicts depression in postpartum mothers. Soc. Psychiat. Psychiatr. Epidemiol. 52, 201–210. doi: 10.1007/s00127-016-1315-3
Slatcher, R., and Selcuk, E. (2017). A social psychological perspective on the links between close relationships and health. Curr. Direct. Psychol. Sci. 26, 16–21. doi: 10.1177/0963721416667444
Smith, T., and Weihs, K. (2019). Emotion, social relationships, and physical health: concepts, methods, and evidence for an integrative perspective. Psychosom. Med. 81, 681–693. doi: 10.1097/PSY.0000000000000739
Solar, O., and Irwin, A. (2010). A conceptual framework for action on the social determinants of health. Social Determinants of Health Discussion Paper 2 (Policy and Practice). World Health Organization.
Steffens, N., Jetten, J., Haslam, C., Cruwys, T., and Haslam, A. (2016). Multiple social identities enhance health post-retirement because they are a basis for giving social support. Front. Psychol. 7, 1519. doi: 10.3389/fpsyg.2016.01519
Steptoe, A., Owen, N., Kunz-Ebrecht, S., and Brydon, L. (2004). Loneliness and neuroendocrine, cardiovascular, and inflammatory stress responses in middle-aged men and women. Psychoneuroendocrinology 29, 593–611. doi: 10.1016/S0306-4530(03)00086-6
Swift, H., Vauclair, C., Abrams, D., Bratt, C., Marques, S., and Lima, L. (2014). Revisiting the paradox of well-being: the importance of national context. J. Gerontol. B. 69, 920–929. doi: 10.1093/geronb/gbu011
Tunçgenç, B., and Cohen, E. (2016). Movement synchrony forges social bonds across group divides. Front. Psychol. 7, 782. doi: 10.3389/fpsyg.2016.00782
Uchino, B. (2004). Social Support and Physical Health. Understanding the Health Consequences of Relationships. Yale: Yale University Press. doi: 10.12987/yale/9780300102185.001.0001
Uchino, B. (2009). Understanding the links between social support and physical health. Perspect. Psychol. Sci. 4, 236–255. doi: 10.1111/j.1745-6924.2009.01122.x
Uchino, B., Uno, D., and Holt-Lunstad, J. (1999). Social support, physiological processes, and health. Curr. Direct. Psychol. Sci. 8, 145–148. doi: 10.1111/1467-8721.00034
Wakefield, J. R. H., Bowe, M., Kellezi, B., McNamara, N., and Stevenson, C. (2019). When groups help and when groups harm: Origins, developments, and future directions of the “Social Cure” perspective of group dynamics. Soc. Person. Psychol. Compass 13, e12440. doi: 10.1111/spc3.12440
Ware, J., and Sherbourne, C. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 30, 473–483. doi: 10.1097/00005650-199206000-00002
WHO (1948). Constitution of the World Health Organization. Am. J. Public Health 36, 1315–1323. doi: 10.2105/AJPH.36.11.1315
Keywords: health, social relationships, personal ties, group ties, group identification
Citation: Camilo C, Lima ML, Moura R, Quintal F and Palacin-Lois M (2024) Beyond close relationships: the positive effects of group relationships and group identification on health. Front. Soc. Psychol. 2:1310755. doi: 10.3389/frsps.2024.1310755
Received: 09 October 2023; Accepted: 04 January 2024;
Published: 22 January 2024.
Edited by:
Adam M. Croom, Case Western Reserve University, United StatesReviewed by:
Dario Spini, Université de Lausanne, SwitzerlandMatthew Andersson, Baylor University, United States
Copyright © 2024 Camilo, Lima, Moura, Quintal and Palacin-Lois. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Camilo, Y3Jpc3RpbmFfY2FtaWxvQGlzY3RlLWl1bC5wdA==