 Talia Barrow
Talia Barrow Bryan Yu1
Bryan Yu1 Carly Cooper
Carly Cooper Elaina DaLomba
Elaina DaLomba- 1U.S. Army-Baylor University Doctor of Science in Occupational Therapy Program, Brooke Army Medical Center, Fort Sam Houston, TX, United States
- 2U.S. Army-Baylor University Physical Therapy Doctorate Program, U.S. Army Medical Center of Excellence, Joint Base San Antonio, Fort Sam Houston, TX, United States
Most U.S. Servicemembers (SMs) get less than the recommended amount of sleep per night, which has been shown to be directly influenced by local leadership. Previous research demonstrated that a brief sleep leadership training (SLT) protocol resulted in improved knowledge and attitudes regarding sleep among U.S. Army leaders, and improvements in the sleep health of their SMs. Human Performance Teams (HPT) offer one solution to propel the cultural change related to sleep, however, little is known about HPT members' own sleep related knowledge, practices, attitudes, and beliefs. This mixed-methods study determined the effect of (SLT) on the sleep-related knowledge, practices, attitudes, beliefs, and perceived competency of HPT members, explored their experiences addressing SM sleep, and gauged their perceived value in receiving the training. Thirty-one individuals received 2 days of SLT. Baseline and 6-week post training follow-up measures were collected, and participants were invited to participate in semi-structured interviews to explore their unique experiences addressing sleep, as well as their perceived value in receiving SLT. Training had no significant effects on HPT members' sleep practices or sleep beliefs, some significant effects on their attitudes and knowledge about sleep, and significant effects on their perceived competence to address sleep in their units. Results suggest that HPT members benefited from the training through enhancement of their competence to address sleep with leadership. However, they struggle to obtain sufficient sleep themselves. More research is needed to identify methods of overcoming specific barriers to sleep imposed on SMs.
1 Introduction
The Department of Defense's 2018 Health Related Behaviors Survey indicates that between 54–69% of Servicemembers (SMs) report getting < 6 h of sleep per night during the workweek, with 31% of those getting 5 h or less (Harrison et al., 2022). Insufficient sleep in a population which the nation relies upon to be combat ready can significantly hamper the higher cognitive skills that are vital for combat effectiveness (LoPresti et al., 2016; Petrofsky et al., 2022). Additionally, impaired sleep corresponds with suicidal ideation and other behavioral health conditions in the military population including post-traumatic stress disorder, generalized anxiety disorder and major depression (Taylor et al., 2014).
Rates of insufficient sleep are high in SMs both with, and without deployment experience (Troxel et al., 2015). This indicates that factors unique to the military but unrelated to war, may contribute to sleep difficulties, or barriers to obtaining sufficient sleep (Troxel et al., 2015). Another factor unique to SMs is the encroachment of leadership into one's personal life (Gunia et al., 2015). Cultural norms related to sleep in a military unit may be influenced by a leader's own attitudes, beliefs and/or lack of knowledge about sleep. Because of this, subordinate SMs may have little personal control over their own sleep routines.
Studies suggest that good leadership skills can at least partially buffer against the barriers to sleep that SMs encounter (Gunia et al., 2015). Army doctrine states that “while good leadership is essential for a wide range of unit outcomes, leadership behaviors that target sleep can improve the sleep habits of unit members and the unit's overall culture” (FM 7–22, p. 11–5). In fact, a 2021 randomized controlled trial by Adler et al. (2021) found that a brief sleep intervention, SLT, designed to educate mid-level Army leaders about sleep health resulted in their subordinates being more likely to sleep 7 or more hours per night when compared to subordinates assigned to leaders in the control group. The study concluded that leadership focused training interventions may “be able to shift sleep health and the cultural perspective on sleep” (Adler et al., 2021, p. 29). The authors recommended that future research focus on expanding upon ways to target cultural change and to reinforce sleep education to Army leaders over time.
One solution to reinforce education and to contribute to cultural change is to ensure that all Army healthcare providers are competent to address sleep. A study by Abdelwadoud et al. (2022) which examined the perceptions of key military stakeholders including economic-decision makers, primary care managers and SMs themselves found the current state of military sleep management practices to be neither satisfactory nor maximally effective. The authors noted many barriers to managing sleep in the military population including a lack of sleep knowledge among healthcare providers, the need for more qualified providers capable of addressing sleep, the need for behavioral approaches to address sleep, and the need for standardized sleep education materials and tools for provider utilization.
To address some of these issues, needed cultural changes, and other problems related to SM health and wellbeing, the Army recently implemented a system of care known as Holistic Health and Fitness (H2F). H2F represents a paradigm shift from a reactive to a proactive system of care that now formally recognizes non-physical domains of health, including sleep, as vital to wellbeing and, equally as important to health as physical preparedness. H2F programs consist of human performance team (HPT) members from varied fields including physical therapy, dietetics, occupational therapy, certified strength and conditioning, athletic training, and cognitive performance, to provide a more holistic approach to care than what was historically valued by the Army.
These novel, multidisciplinary groups of allied health and performance professionals, embedded throughout the Army, offer one solution to address sleep issues in this population. However, little is currently known about the sleep related knowledge, practices, attitudes, beliefs, and competency of HPT members to address sleep. In fact, much of the literature suggests that healthcare providers receive minimal education related to sleep and are inadequately prepared by their educational programs to address sleep (Ye and Smith, 2015; Meaklim et al., 2020). Further, healthcare providers themselves are considered a population at increased risk for sleep deprivation (Siddalingaiah et al., 2017; Parry et al., 2018). Some evidence suggests a decrement in the performance and productivity of healthcare providers who suffer from sleep deprivation, making them less effective at performing their assigned duties (Shaik et al., 2022). Thus, the present study sought to determine the current state of the sleep-related knowledge, practices, attitudes, beliefs, and perceived competency of HPT members, to determine the effects of SLT on these characteristics and to explore the experiences of HPT members addressing sleep in this innovative system of care. We hypothesized that SLT would affect the sleep characteristics and perceived competence of HPT members.
2 Materials and methods
2.1 Design
This study utilized a quasi-experimental, concurrent triangulation mixed methods design. Quantitative and qualitative data were collected during one phase and weighted equally. Data were analyzed separately and then compared to assess for convergence, differences, or a combination. Data were then analyzed collectively to determine existing relationships. This study was approved by the San Antonio Institutional Review Board (IRB #957424).
2.2 Subjects
HPT members in various H2Fs throughout the continental United States were scheduled to participate in SLT. Participants enrolled in the training were recruited via flyers and e-mail briefings. Inclusion criteria were: (1) current Army HPT members (2) age 17–64 and (3) can read, speak, and understand English. Exclusion criteria were (1) self-reported diagnosis of insomnia, (2) self-reported diagnosis of obstructive sleep apnea, (3) currently taking any prescription sleep medications, (4) unable to complete all aspects of the study and (5) unwilling to disclose information on outcome measures.
2.3 Study procedures
Figure 1 depicts the methodological procedures outlined in this section. Research subjects interested in participating in this study notified the research team and were pre-screened based on eligibility requirements. Eligible subjects were emailed a Qualtrics weblink to complete the questionnaire packet. The packet contained basic demographic data and (1) components of the Sleep Practices and Attitudes Questionnaire (SPAQ), (2) questions related to sleep leadership knowledge and attitudes, and (3) a sleep leadership perceived competence scale. The outcome measures took ~10–15 min to complete, and participants were able to complete them on their home computers or mobile devices.
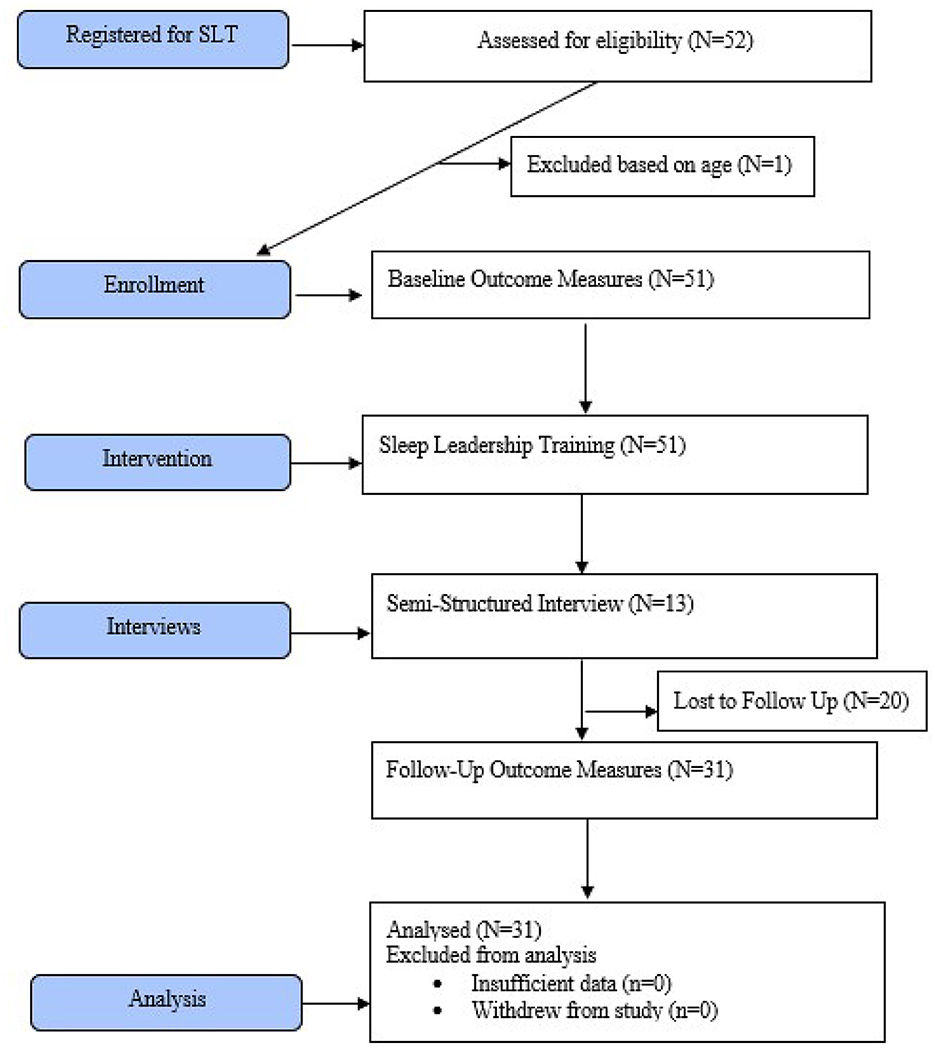
Figure 1. CONSORT diagram demonstrating methodological procedures.
Following completion of the packet, standardized SLT was provided by instructors who had received specialized SLT training from the Walter Reed Army Institute of Research (WRAIR) (Adler et al., 2021). The training was conducted virtually, using Microsoft Teams, over 2 days. Following the training, participants were invited to participate in telephonic semi-structured interviews, related to their experience addressing sleep in their brigades, and in their experience receiving SLT. Purposive sampling continued until saturation was reached. Each interview was audio-recorded and transcribed verbatim. Six weeks following the completion of the training participants received a follow-up Qualtrics web links consisting of the same measures.
2.4 Measures
Sleep knowledge and attitudes were measured using 15 items based on a previous literature assessing the impact of SLT on military leaders (Adler et al., 2021). Participants were asked to indicate their strength of agreement for eight items which measured sleep knowledge and seven items which measured sleep attitudes (1 = strongly disagree to 5 = strongly agree). In keeping with the original research, responses to all 15 questions were categorized such that a score of four or five were rated as agreement with the statement. No psychometric properties have been reported for these questions (Adler et al., 2021).
Sleep practices were assessed using the Sleep Duration, Sleep Debt, Sleep Quality and the Sleepiness/Tiredness Subscales from the Sleep Practices and Attitudes Questionnaire (SPAQ) (Grandner et al., 2014). Sleep duration was assessed by asking HPT members how many hours of sleep they achieve on weekdays/ workdays, and how many hours of sleep they achieve on weekends/ vacation days. Sleep debt was assessed by asking HPT members how many hours of sleep they think they need each night and then subtracting the average number of sleep duration from their identified sleep needs as described in Grandner et al. (2014). A mean sleep quality score was established by asking HPT members to rate their quality of sleep over the last week, as well as their strength of agreement with the statement “I have difficulty related to sleep,” on five-point scales. A mean subscale score for sleepiness/ tiredness was determined by using three dichotomous items (yes/no) to determine if they are sleepy/ tired/ refreshed throughout the day, and one item rating their strength of agreement with the statement, “I never feel sleepy.” Sleep beliefs were assessed using the sleep and health subscale from the SPAQ. This subscale has been used in previous research to determine beliefs about sleep health and asks respondents to rate their degree of belief about how sleep loss affects 15 different variants of their health (Khader et al., 2021). All items were rated on a five-point scale. Most subscales in the SPAQ demonstrate moderate to high internal consistency (α = 0.25 to 0.86), when estimated in a population of 124 participants aged 18–80 years (Grandner et al., 2014). Concurrent and divergent validity were demonstrated by comparing various subscales to existing measures (Grandner et al., 2014).
Perceived competence to address sleep was assessed with four items that were created for this study using a modifiable perceived competence scale (Williams et al., 1998). In previous studies, modified versions of the scale demonstrated excellent internal consistency with Cronbach's alpha between 0.80 and 0.94 (Williams et al., 1998). For the current study, items were designed to capture the perceived competence of HPT members to address sleep with Army leaders and were rated on a 7-point scale (1 = not at all true to 7 = very true). Responses were categorized such that a score of five, six or seven were rated as agreement with each statement.
2.4.1 Data analysis
Descriptive statistics were used to summarize demographic data. All quantitative variables were analyzed in Statistical Package for Social Science (SPSS® version 29.0.0.0) using non-parametric tests. Raw pre-training and post-training data for each question pertaining to sleep practices, knowledge, attitudes, beliefs, and perceived competency related to sleep were examined for any significant differences using Wilcoxon Signed Ranks Tests. These are displayed in Table 2, along with associated significances and percent agreement for some variables.
Qualitative data from the semi-structured interviews were analyzed using semantic thematic analysis following the Braun and Clarke (2006) method, and was managed using NVivo® software (release 1.7.1).
3 Results
3.1 Demographics
Demographic items were included to identify any potential covariates. Demographic variables consisted of age, gender, profession, employment status, year of graduation, sleep education status and sleep supplement or over the counter medications (Table 1). Seventy-one HPT members who signed up to complete SLT were briefed about the study. Fifty-one HPT members were enrolled in the study, completed baseline measures, and received 2 days of SLT. Twenty HPT members were lost to follow up. A final sample of 31 pre/ post-test results were statistically analyzed. Purposive sampling for qualitative interviews continued until saturation was reached. Thirteen interviews were conducted and qualitatively analyzed.
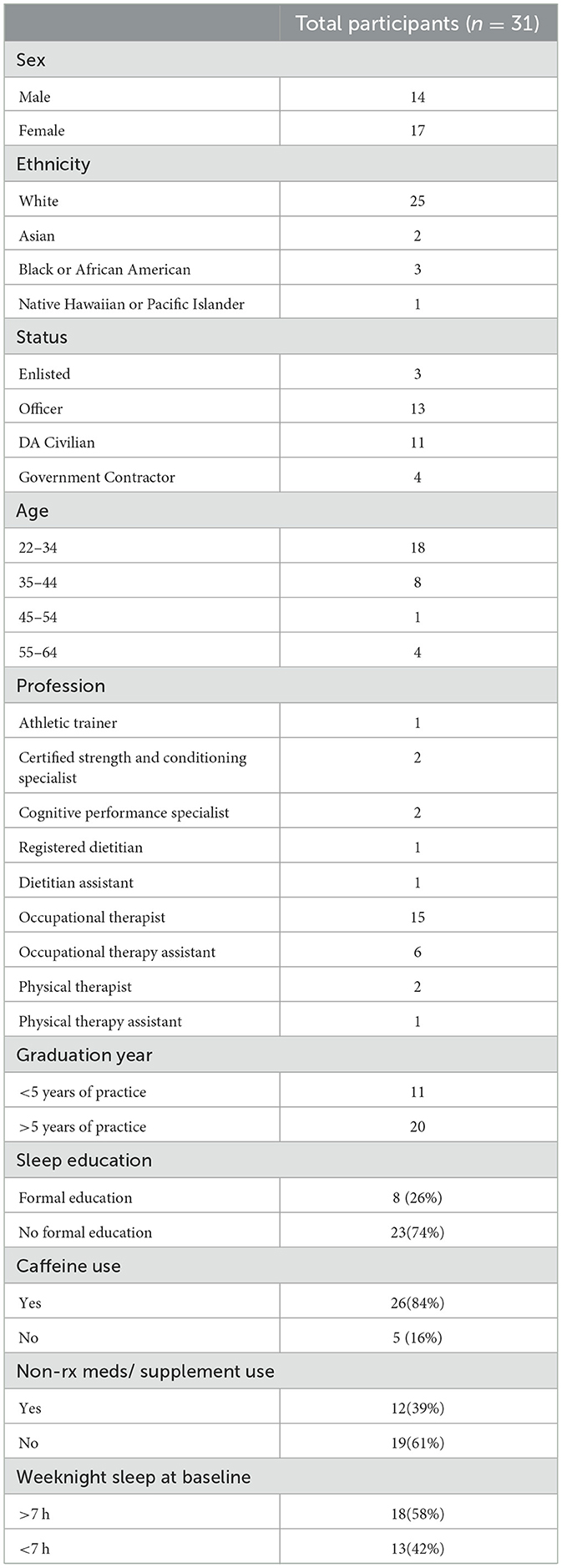
Table 1. Demographics for HPT members.
Demographic analysis revealed that most participants were in the occupational therapy profession (68%) (the profession responsible for sleep readiness in the military), had been practicing more than 5 years (65%) and had received no formal education related to sleep in their degree granting programs (74%). At the time baseline measurements were collected, 39% of HPT members used a non-prescription sleep aid, or supplement to promote sleep in their own lives and, 42% were getting < 7 h of sleep per night on weeknights.
3.2 Sleep knowledge and attitudes
Comparisons in sleep-related knowledge and attitudes are provided in Table 2. Aside from one sleep knowledge question pertaining to the normalcy of Soldiers waking throughout the night (p = 0.006), and one sleep attitude question pertaining to a Soldier's ability to train themselves to go without sleep (p = 0.046), there were no significant differences in sleep knowledge/ attitudes between pre/ posttest.
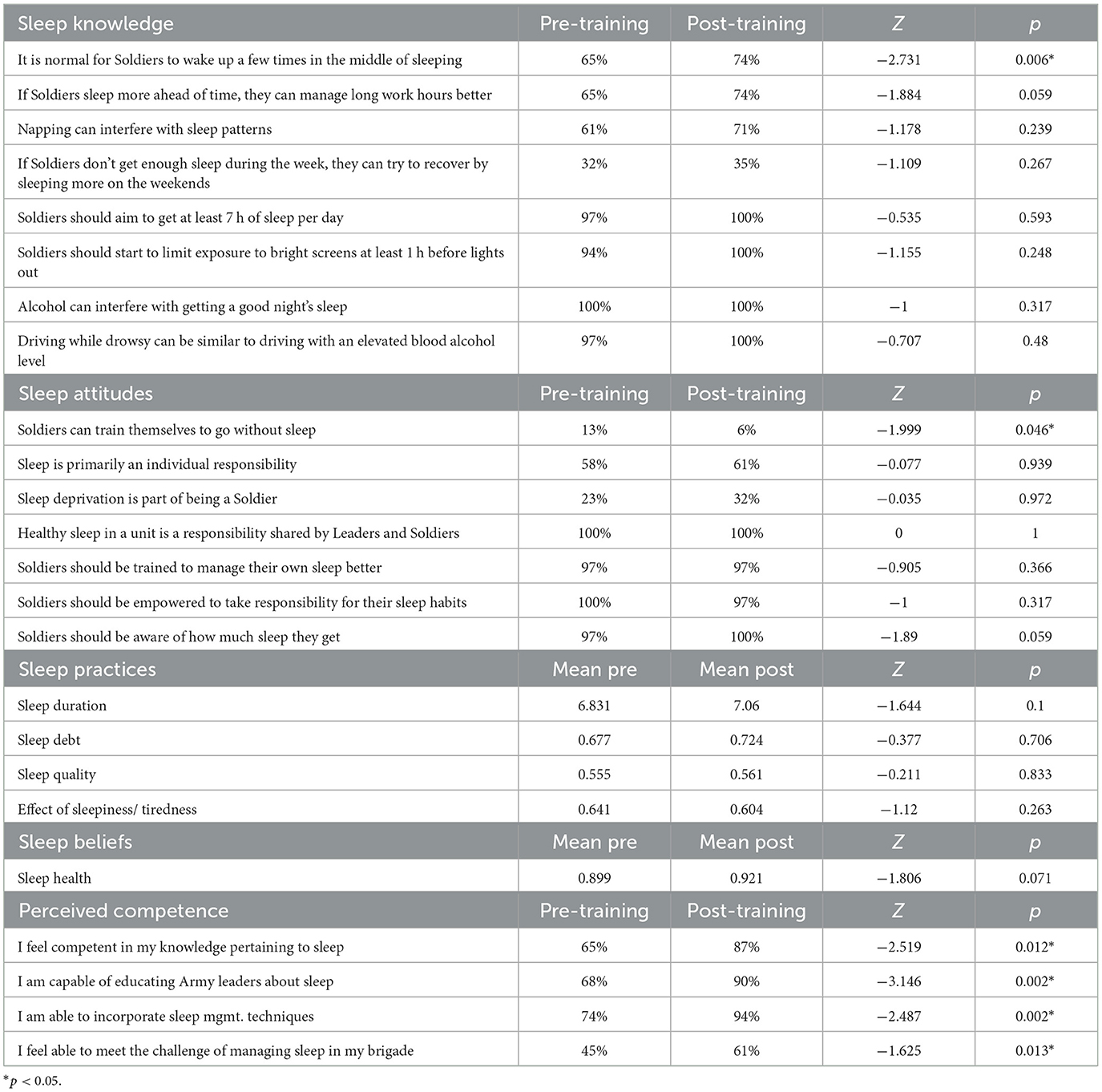
Table 2. Sleep knowledge, attitudes, practices, beliefs, and perceived competence.
3.3 Sleep practices and sleep beliefs
Comparisons in sleep practices and sleep beliefs are provided in Table 2. There were no significant differences between sleep duration subscale scores at baseline (6.83) and sleep duration posttest subscale scores (7.06-) (p = 0.100). Before receiving SLT, 42% of HPT members endorsed getting < 7 h of sleep per night on worknights (average 6.63 h) with 13% getting < 7 h of sleep on weekends/ holidays (average 7.3 h). Six weeks after the delivery of SLT, these numbers decreased to 39% (average 6.83 hours), and increased to 16% (average 7.60 h), respectively.
There were no significant differences in sleep debt subscale scores at baseline (0.677) compared to posttest scores (0.724) (p = 0.706). Accumulated sleep debt ranged from −0.14 (14 min more than needed per night) to 3.71 h pre SLT and −0.64 to 2 h post SLT. All other aspects of sleep practices including sleep quality as well as the effect of sleepiness/ tiredness were insignificant (p = 0.833 and p = 0.263 respectively). Finally, comparisons between subscale scores for sleep beliefs were also found to be insignificant (p = 0.071).
3.4 Perceived competence
Regarding perceived competence, scores for all four questions improved from pre to posttest, with each one demonstrating a significant change (Table 2). At the conclusion of the study, 39% of HPT members continued to feel unable to meet the challenge of managing sleep in their brigades (p = 0.013).
3.5 Participant interviews
Thirteen participants were interviewed by the first author and three co-authors aided with reviewing and refining 412 data extracts and 14 collated codes. The research team met virtually throughout the process to collectively refine analysis of the data. Four themes emerged from the data: (1) intrinsic motivation leading to self-directed learning, (2) military culture, (3) revenge sleep procrastination (RSP) and (4) structure and confidence (Table 3).
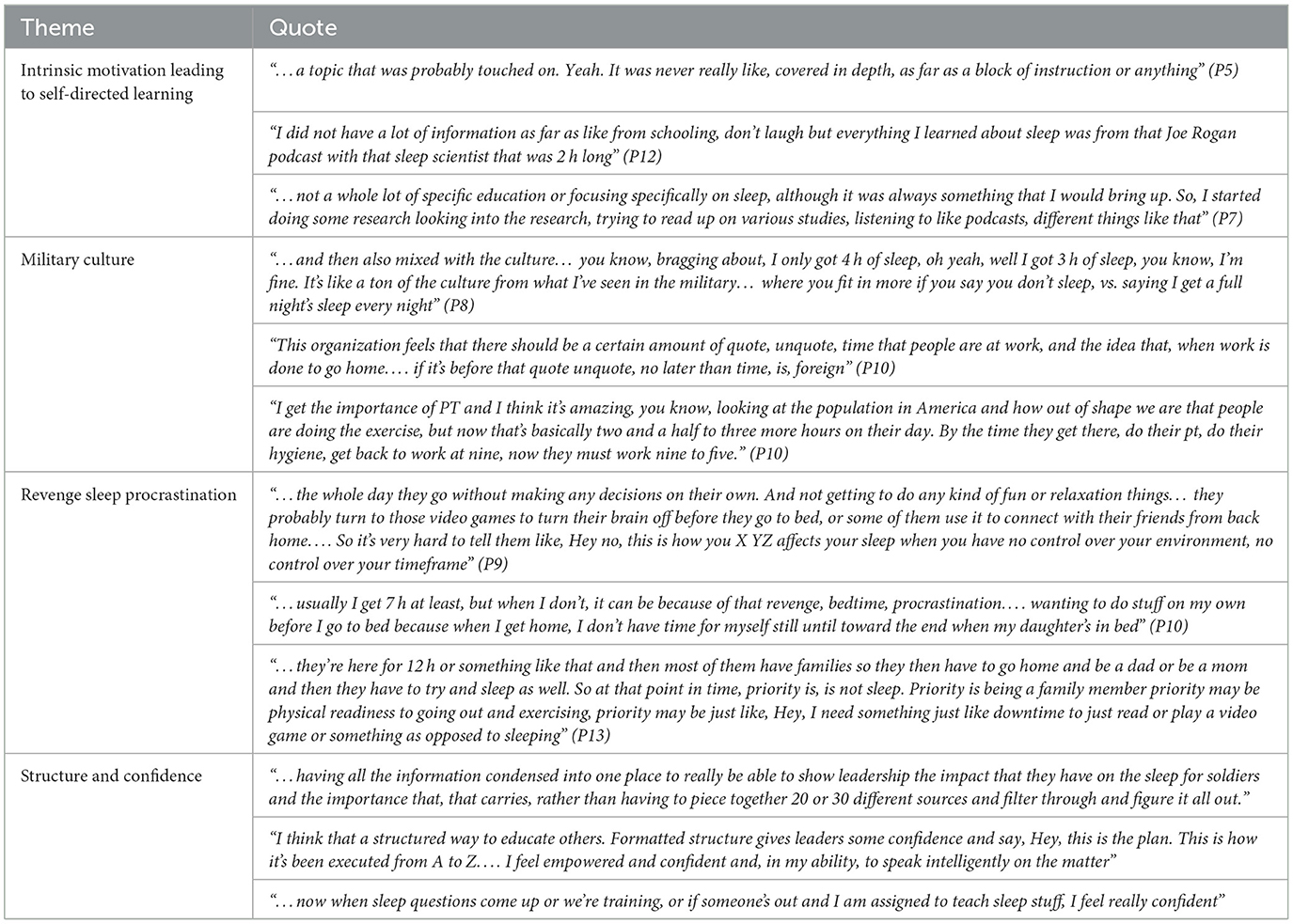
Table 3. Qualitative results from semi-structured interviews.
3.5.1 Intrinsic motivation leading to self-directed learning
Participants reported being underprepared to shift from their typical roles to that of a provider who addresses sleep. Many reported that their degree-granting programs did not include content related to the importance of sleep, or how to address sleep problems. HPT members expressed a desire to do well in their new roles, despite a lack of foundational education and many reported seeking out alternative methods to enhance their own knowledge about sleep. Some HPT members sought out other professionals to serve as peer-mentors or conducted personal research on the matter. Several HPT members reported reading books and listening to popular podcasts about sleep to enhance their skills in this area.
3.5.2 Military culture
HPT members expressed challenges to addressing sleep in the Army due to the culture. They openly discussed unspoken rules such as feeling the need to stay late in the evening if one's supervisor was still present or staying late despite having no further work to do. They reported that SMs have routinely extended work hours that are accepted and normalized as part of their service to the nation, and that it was more common for SMs to get < 7 h of sleep a night, than >7 h. HPT members reported that work schedules are generally inefficient with many unproductive gaps in the day which increase the hours of work exponentially and leave SMs with little personal time to manage their own affairs.
3.5.3 Revenge sleep procrastination
Several HPT members discussed the concept of RSP as a barrier to sleep. RSP, also referred to as revenge bedtime procrastination is defined by Kroese et al. (2016, p. 93) as “the phenomenon of postponing going to bed, typically resulting in a lack of sleep,” or an act of defiance against the increasing demands at home and at work, that leaves one with minimal time for leisure activities. HPT members reported recognizing SMs engaging in RSP response to having little personal control over their own day-to-day schedules. They noted that when SMs finally had the opportunity to sleep in the evenings, they often willingly delayed sleep, instead staying awake to participate in other activities such as playing video games, spending time with their spouses or children, or communicating with family members in different time zones. They discussed that SMs work long hours in stressful jobs and require time before bed to quiet their minds, in preparation for sleep. Serval of the HPT members interviewed endorsed RSP as a barrier to sleep in their own lives.
3.5.4 Structure and confidence
Finally, HPT members reported benefiting from the structure and organization of SLT. They noted that the information they received from the training validated the information they had garnered through self-directed learning and that this affirmed the ways they had taught themselves to address sleep in their units, contributing to enhanced confidence. The packaged, condensed materials made it easy to present the topic of sleep and contributed to their comfort in teaching the materials despite their lack of foundational education on the topic.
4 Discussion
This study sought to determine the effect of SLT on the sleep-related knowledge, practices, attitudes, beliefs, and perceived competence of HPT members and to explore their experiences addressing SM sleep. Overall, the training had no significant effects on HPT members' sleep practices or sleep beliefs and limited effects on their attitudes and knowledge about sleep. Despite this, the training did appear to improve the perceived competence of HPT members to address the complex sleep issues faced by SMs.
HPT members in this study were selected for their positions despite 74% having no formal education related to sleep or sleep interventions. Much of the current evidence suggests that healthcare providers receive minimal education related to sleep and are inadequately prepared by their educational programs to address sleep (Ye and Smith, 2015; Meaklim et al., 2020; Abdelwadoud et al., 2022). Some authors suggest that this lack of preparedness might even be contributing to the sleep crisis that is occurring in the United States (Meaklim et al., 2020). Interviews with HPT members illuminated that they recognize their lack of preparedness and frequently sought out alternative ways to enhance their capabilities.
Regardless of their lack of formal education, when compared to general SMs, HPT members had higher sleep-related knowledge and better sleep-related attitudes at baseline. For example, Adler et al. (2021) assessed the knowledge of Army leaders prior to the delivery of SLT and found that only 22.9% agreed that it was normal for Soldiers to wake a few times in the middle of the night, whereas this number was as high as 65% in baseline measures of HPT members. When she assessed their attitudes, 28.6% of her leaders agreed that Soldiers can train themselves to go without sleep, whereas only 13% of HPT members agreed with this statement. Because HPT members were more educated about sleep at baseline, they may have had less room for improvement in their sleep-related knowledge and attitudes.
At baseline, HPT members were achieving a mean sleep duration approximately one-half hour less than the amount of sleep recommended by the American Academy of Sleep Medicine (2015). SLT had no significant effect on sleep duration in this study. Even after delivery of a sleep-educational intervention, almost 40% of HPT members, who are themselves, designated to address sleep in the Army, continued to be unable to achieve adequate sleep. HPT members interviewed in this study endorsed complex barriers to sleep in their own lives including long work hours, balancing work and family demands and difficulty detaching from work. The unique barriers to sleep faced by SMs are profound and will likely require much more than an educational course to overcome. This is congruenrt with current literature which demonstrated that that healthcare workers in general are known to be susceptible to insufficient sleep and disorders of their sleep (Hittle et al., 2023).
The concept of SMs engaging in RSP was an interesting finding in this study. Regularly extended hours at work may interfere with one's ability to perform needed personal activities and still achieve adequate sleep. It can be expected then that SMs who are required to routinely work beyond 8 h a day may need to delay their bedtime, thereby decreasing their sleep, to create the opportunity to engage in activities which provide one's life with purpose and meaning. HPT members endorsed that RSP occurs in both the SMs they treat, and in their own lives Sleep procrastination is common in non-military connected populations also. Kroese et al. (2016) found that over 53% of young adults reported delaying sleep to engage in watching television, using computers, or socializing.
At baseline, more than half of HPT members felt competent in their sleep-related knowledge, their ability to educate leaders about sleep, and their ability to incorporate sleep management practices, however, only 45% felt capable of managing sleep issues in their brigade. SLT had a significant effect on these perceived competencies. Competence is enhanced by education or experience which provides advanced knowledge, traits skills and/or abilities (Kak et al., 2001). HPT members appeared to benefit from the opportunity to receive, what was for many, their first formal sleep education, and the opportunity to practice the delivery of sleep education to Army leaders in this virtual group setting. In their interviews, HPT members regarded the structure and format of the training, as well as the provided materials as empowering, and noted it contributed to their competence in their ability to address sleep with Army leaders.
4.1 Study limitations and recommended future research
One of the main limitations of this study is that it lacked the use of a control group. It was not possible to utilize a control group in this study as the training was mandated for all HPT members. Future studies may wish to consider randomized controlled trials which compare the effects of SLT to other sleep education programs. Further, we used only self-report questionnaires. Self-reported data can be subject to several types of biases. Future studies may consider using actigraphy or wearable sleep devices to assess any objective differences in measures of sleep health after SLT.
Strengths of this study include a high retention rate and collection of follow-up data a month after training. Unfortunately, no outcome measures exist which adequately capture nuances specific to military populations, such as the impact of a palpable but immeasurable culture. In fact, many commonly used psychosocial, or sleep outcome measures are not validated for use in military populations. This may be a goal for researchers interested in understanding sleep in military SMs. Our use of a mixed-methods design added depth and context to questionnaire results. The qualitative findings from this study can be particularly helpful for Army leaders, healthcare workers and policy makers. This study utilized a brief (two day), multimodal (mix of didactic and practicum) virtual (computer-based) means of delivering sleep education. Virtual education has expanded significantly, although its utility and efficacy remain questionable. This study demonstrated that a virtual intervention resulted in significant improvements in perceived competence. Because sleep education is sparse in many degree-granting programs, delivering this education virtually may be an effective means of enhancing the number of healthcare providers who are both qualified and competent to address sleep in this unique population.
5 Conclusion
To the authors' knowledge, this is the first study to assess the effect of SLT on the sleep characteristics of Army HPT members. The study demonstrated that SLT is an effective method of enhancing the perceived competence of Army HPT members to address sleep, despite a lack of foundational training. Most SMs and HPT members get less than the recommended amount of sleep per night. HPT members endorsed the same barriers to sleep faced by the SMs they treat. The military imposes unique challenges to sleep, even for those responsible for managing the sleep readiness of the force. Additional research is needed to determine what interventions might be most effective for overcoming longstanding cultural barriers to sleep in this unique subset of the population.
Data availability statement
The datasets presented in this article are not readily available because data is property of a U.S. Government employee. Requests to access the datasets should be directed to Y2FybHlyY29vcGVyQHlhaG9vLmNvbQ==.
Ethics statement
The studies involving humans were approved by San Antonio Review Board/Brooke Army Medical Center. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
TB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Writing – original draft, Writing – review & editing. BY: Data curation, Investigation, Methodology, Software, Writing – review & editing. CC: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. ED: Data curation, Formal analysis, Investigation, Supervision, Writing – review & editing. JU: Formal analysis, Methodology, Software, Writing – review & editing. BG: Investigation, Methodology, Resources, Writing – review & editing. MB: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to acknowledge the U.S. Army Occupational Therapy leadership and Human Performance Team members who delivered materials and training to make this research possible.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Author disclaimer
The views expressed herein are those of the author(s) and do not necessarily reflect the official policy or position of the Defense Health Agency, Brooke Army Medical Center, the Department of Defense, nor any agencies under the U.S. Government.
References
Abdelwadoud, M., Collen, J., Edwards, H., Mullins, C. D., Jobe, S. L., Labra, C., et al. (2022). Engaging stakeholders to optimize sleep disorders' management in the US military: a qualitative analysis. Military Med. 187, e941–e947. doi: 10.1093/milmed/usab341
Adler, A. B., Bliese, P. D., LoPresti, M. L., McDonald, J. L., and Merrill, J. C. (2021). Sleep leadership in the army: a group randomized trial. Sleep Health 7, 24–30. doi: 10.1016/j.sleh.2020.06.001
American Academy of Sleep Medicine (2015). 7 or More Hours of Sleep a Night: A Health Necessity for Adults. Available online at: https://aasm.org/seven-or-more-hours-of-sleep-per-night-a-health-necessity-for-adults/ (accessed June 7, 2023).
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Q. Res. Psychol. 3, 77–71. doi: 10.1191/1478088706qp063oa
Grandner, M. A., Jackson, N., Gooneratne, N. S., and Patel, N. P. (2014). The development of a questionnaire to assess sleep-related practices, beliefs, and attitudes. Behav. Sleep Med. 12, 123–142. doi: 10.1080/15402002.2013.764530
Gunia, B. C., Sipos, M. L., LoPresti, M., and Adler, A. B. (2015). Sleep leadership in high-risk occupations: an investigation of soldiers on peacekeeping and combat missions. Military Psychol. 27, 197–211. doi: 10.1037/mil0000078
Harrison, E. M., Schmied, E. A., Hurtado, S. L., Easterling, A. P., and Glickman, G. L. (2022). The development, implementation, and feasibility of a circadian, light, and sleep skills program for shipboard military personnel (CLASS-SM). Int. J. Environ. Res. Pub. Health 19:3093. doi: 10.3390/ijerph19053093
Hittle, B. M., Hils, J., Fendinger, S. L., and Wong, I. S. (2023). A scoping review of sleep education and training for nurses. Int. J. Nurs. Stu. 12:104468. doi: 10.1016/j.ijnurstu.2023.104468
Kak, N., Burkhalter, B., and Cooper, M. A. (2001). Measuring the competence of healthcare providers. Operations Res. Issue Paper 2, 1–28.
Khader, W. S., Fernandez, F. X., Seixas, A., Knowlden, A., Ellis, J., Williams, N., et al. (2021). What makes people want to make changes to their sleep? Assessment of perceived risks of insufficient sleep as a predictor of intent to improve sleep. Sleep Health 7, 98–104. doi: 10.1016/j.sleh.2020.07.003
Kroese, F. M., Nauts, S., Kamphorst, B. A., Anderson, J. H., and de Ridder, D. T. (2016). Bedtime Procrastination: A Behavioral Perspective on Sleep Insufficiency. Procrastination, Health, and Well-being. London: Academic Press, 93–119.
LoPresti, M. L., Anderson, J. A., Saboe, K. N., McGurk, D. L., Balkin, T. J., and Sipos, M. L. (2016). The impact of insufficient sleep on combat mission performance. Militar. Behav. Health 4, 356–363. doi: 10.1080/21635781.2016.1181585
Meaklim, H., Jackson, M. L., Bartlett, D., Saini, B., Falloon, K., Junge, M., et al. (2020). Sleep education for healthcare providers: addressing deficient sleep in Australia and New Zealand. Sleep Health 6, 636–650. doi: 10.1016/j.sleh.2020.01.012
Parry, D. A., Oeppen, R. S., Amin, M. S. A., and Brennan, P. A. (2018). Sleep: its importance and the effects of deprivation on surgeons and other healthcare professionals. Br. J. Oral Maxillofacial Surg. 56, 663–666. doi: 10.1016/j.bjoms.2018.08.001
Petrofsky, L. A., Heffernan, C. M., Gregg, B. T., and Smith-Forbes, E. V. (2022). Effects of sleep deprivation in military service members on cognitive performance: a systematic review. Military Behav. Health 10, 202–220. doi: 10.1080/21635781.2021.1982088
Shaik, L., Cheema, M. S., Subramanian, S., Kashyap, R., and Surani, S. R. (2022). Sleep and safety among healthcare workers: the effect of obstructive sleep apnea and sleep deprivation on safety. Medicina 58:1723. doi: 10.3390/medicina58121723
Siddalingaiah, H. S., Chandrakala, D., and Singh, A. (2017). Sleep pattern, sleep problems and comorbidities among resident doctors at a tertiary care institution in India: a cross sectional study. Int. J. Commun. Med. Pub. Health 4, 4477–4484. doi: 10.18203/2394-6040.ijcmph20175165
Taylor, M. K., Hilton, S. M., Campbell, J. S., Beckerley, S. E., Shobe, K. K., Drummond, S. P. A., et al. (2014). Prevalence and mental health correlates of sleep disruption among military members serving in a combat zone. Military Med. 197, 744–751. doi: 10.7205/MILMED-D-13-00551
Troxel, W., Shih, R., Pedersen, E., Geyer, L., Fisher, M., Griffin, B., et al. (2015). Sleep in the Military: Promoting Healthy Sleep Among U.S. Servicemembers. New York, NY: RAND Corporation.
Williams, G. C., Freedman, Z. R., and Deci, E. L. (1998). Supporting autonomy to motivate glucose control in patients with diabetes. Diab. Care 21, 1644–1651. doi: 10.2337/diacare.21.10.1644
Keywords: sleep, leadership, military, holistic health, sleep procrastination, military sleep assessment
Citation: Barrow T, Yu B, Cooper C, DaLomba E, Gregg B, Barefield M and Umlauf J (2024) The effect of Sleep Leadership Training on U.S. Army human performance team members. Front. Sleep 3:1351691. doi: 10.3389/frsle.2024.1351691
Received: 06 December 2023; Accepted: 11 March 2024;
Published: 08 April 2024.
Edited by:
Michelle Perfect, University of Arizona, United StatesReviewed by:
Brandy A. Brown Perkl, University of Arizona, United StatesAdam T. Newton, Western University, Canada
Copyright © 2024 Barrow, Yu, Cooper, DaLomba, Gregg, Barefield and Umlauf. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carly Cooper, Y2FybHlyY29vcGVyQHlhaG9vLmNvbQ==
†These authors have contributed equally to this work and share third authorship