 Bekan Gudata Gindaba1*
Bekan Gudata Gindaba1* Tesfaye Abera Gudeta1
Tesfaye Abera Gudeta1 Lemane Dereje Sebu1
Lemane Dereje Sebu1 Ebisa Zerihun Gindaba2
Ebisa Zerihun Gindaba2 Misgana Tesgara Abdisa3
Misgana Tesgara Abdisa3
- 1School of Nursing and Midwifery, Wallaga University, Nekemte, Ethiopia
- 2Department of Nursing, Oda Bultum University, Chiro, Ethiopia
- 3Department of Nursing, Mettu University, Mettu, Ethiopia
Background: Primary dysmenorrhea is a common gynecological problem characterized by recurrent, periodical, and cramping pain in the lower abdomen that occurs before or during menstruation, usually without pelvic disease. Its magnitude has not been well studied; some of the associated factors are inconclusive. Therefore, the goal of this study was to fill gaps on the magnitude, and associated factors of primary dysmenorrhea among female high school students in Nekemte town.
Objectives: To assess the magnitude of primary dysmenorrhea, its associated factors among high school students in Nekemte town, East Wallaga, Western Oromia, Ethiopia, 2023.
Methods: An institutional-based cross-sectional study was conducted among high school students in Nekemte town from June 05 to 19, 2023. The calculated total sample size was 534, and data were collected from four governmental high schools and one private high school that were selected by multistage stratified sampling. The collected data were entered into Epi Info version 3.1 and analyzed using SPSS version 25. Binary and multivariable logistic regressions were used to find associations between dependent and independent variables.
Results: The magnitude of primary dysmenorrhea was 68.4% (95% CI = 64.3%, 72.0%). Anxiety (AOR = 2.41, 95% CI = 1.31, 4.43), family history of primary dysmenorrhea (AOR = 4.64, 95% CI = 2.74, 7.86), sexual intercourse (AOR = 0.34, 95% CI = 0.21, 0.55), drinking tea <4 cups per day (AOR = 0.38, 95% CI = 0.22, 0.60), and physical activity (AOR = 0.06, 95% CI = 0.03, 0.11) were factors associated with primary dysmenorrhea.
Conclusion: The magnitude of primary dysmenorrhea was high among high school students in the study area. Sexual intercourse, physical activity, drinking tea, anxiety, and family history of primary dysmenorrhea were significantly associated with primary dysmenorrhea.
Introduction
Primary dysmenorrhea (PD) is a pain during the menstrual cycle characterized by recurrent, periodical and cramping pain in the lower abdomen that occurs before or during menstruation, usually without pelvic disease (1, 2). This abdominal pain usually starts 1–2 days before the onset of menses or just after the menstrual flow, typically lasts for 8–72 days (2, 3), and may radiate to the back and thighs (4, 5). In addition, the onset of primary dysmenorrhea usually occurs in adolescents and begins within a few months or within 2 years of menarche (3, 5).
Although the pathophysiological mechanisms of PD are not well established (6, 7), several studies have revealed that it is a complex process that may depend on hormonal many factors (8–10). Among those factors, prostaglandin plays a major role in the pathophysiological mechanism of PD (4–6).
Prostaglandins' production leads to muscle and vein contraction, which causes uterine ischemia and the production of anaerobic metabolites. As a result, pain during menses occurs. These prostaglandins are synthesized via the arachidonic acid mediated by the cyclooxygenase (COX) pathway. Progesterone levels control the arachidonic acid, which is mediated by COX pathways and is responsible for the production of prostaglandins (4, 6). In addition, vasopressin and other proinflammatory factors contribute to the development of primary dysmenorrhea (5, 7).
In addition to hormonal changes that occur in the body, non-hormonal factors, such as increasing age, early age at menarche, anxiety, length, and severity of menstruation, social disruption, drinking tea, sexual intercourse, marital status, and parity, may also contribute to the pathomechanism of PD (9–15). Moreover, many researchers propose that social, living, and psychology have added to this patho-mechanism of PD (4, 5, 8, 10).
PD is the most prevalent problem among adolescent girls (13, 16–20), globally, previous findings have reported that the magnitude of PD ranges from 51.1% to 92.3% of reproductive-age women, with 2%–29% experiencing severe pain, and a higher percentage (70%–90%) of younger women (<24 years of age) are generally reported (6, 21, 22). In Africa, the prevalence of PD varies from 51.1% to 78.35% (23, 24). In Ethiopia, the magnitude of PD ranges from 51.5% to 85.4% (10, 20).
Moreover, diagnose of PD does not require specializing in women's health or pelvic pain, and management can be started based on a typical history of painful menses without physical examination (3, 5).
In addition, different studies revealed that PD is the most frequently reported gynecological and menstrual problem and is the leading menstrual problem affecting 90% of adolescent girls and more than 50% of menstruating women (8, 10, 12, 25).
Additionally, primary dysmenorrhea is severe enough to result in significant socioeconomic problems, particularly in adolescents and young women (15). Different studies have shown that PD usually affects individuals' relationships, functioning, and productivity; contributes to absenteeism in class/work; and reduces daily life activities (11, 12, 26, 27). For example, in the United States, 600 million work hours and 2 billion dollars of cost-effective loss are likely associated with painful menses (3), and other studies have revealed that these losses have a significant negative impact on students' academic performance (10, 16, 27). Moreover, it also affects psychology, quality of life, and patterns of sleep and leads to central nervous system sensitization, which results in chronic pain syndrome (5).
In Ethiopia, a studies found that there are cultural taboos about menstruation like believing PD is a natural phenomenon, tolerated, and embarrassing (19, 28). In addition, the Ethiopia had School Health Program Framework which includes social and behavioral change communication and life skills development, school nutrition services, water, sanitation and hygiene (WASH) provision, Management of common infections, infestations, and disorders, Sexual and reproductive health services, and others but it did not incorporate about PD under sexual and reproductive health services (29).
Moreover, pain during menses is the most prevalent but conceivably the least recognized, neglected and least managed of all menstrual illnesses, and study participants may experience symptoms as a predictable response to menstruation (3, 4). So this study can help students, school authorities, and organizations working on school menstrual hygiene management program develop a better understanding of primary dysmenorrhea. In Ethiopia, specifically in Nekemte town among high school students, the magnitude of dysmenorrhea, especially primary dysmenorrhea, which is the most common problem, has not been well studied (10). Moreover, some of the factors associated with PD are inconclusive and controversial (11, 30). Therefore, the goal of this study was to assess the magnitude, and risk factors for primary dysmenorrhea among female high school students in Nekemte town.
Methods and materials
Study design, area, and period
Institution based cross sectional study was conducted in Nekemte town, East Wallaga Zone, Oromia Regional State, Ethiopia, from June 05 to 19, 2023. Nekemte is the capital city of the East Wallaga Zone and is located in the western part of the country at a distance of 324 km from Addis Ababa, the capital city of Ethiopia. According to the report of the Nekemte town educational bureau, there were 16,379 high school students, of which 8,887 were female students and 7,492 were male students. In the town, there are eight public high schools namely, Nekemte secondary school, Biftu Nekemte secondary school, Dalo secondary school, Darge secondary school, Dire Jato secondary school, Kumsa Moroda secondary school, Leka Nekemte secondary school, and Ifa Boru Boarding School. In addition, there are three private high schools in the town, namely, Bethel Academy, Kidanemihiret (Catholic Academy), and Onesmosnasib Academy.1
Population, sample size, and sampling technique
All female high school students in Nekemte town who were pursuing their education were the source population. On other hand, all female students from five selected high schools in Nekemte town were the study population. The inclusion criterion for this study was all female students from five selected high schools. However, a female student who had a known pelvic pathology was excluded from thew study which was reported by the students.
The sample size was determined using Epi Info 7 by taking the expected proportion of primary dysmenorrhea (70%) from a study of Wolaita Sodo Town Secondary School Students (31) with a 5% margin of error and a 95% confidence interval. Considering the design effect of 1.5 and a nonresponse rate of 10%, the total sample size was 534. Study participants were selected from all Nekemte town high schools using a multistage stratified sampling technique. First, the eleven schools were stratified into eight public and three private schools. Then, the public schools were classified based on their location as East (Nekemte Secondary Shool and Dalo Secondary School), West (Leka Nekemte Secondary School and Ifa Boru Boarding School), South (Biftu Nekemte Secondary School, Dire Jato Secondary School, and Darge Secondary School), and North (Kumsa Moroda Secondary School). Again from all directions one school was selected by lottery method. The selected four Schools were Nekemte Secondary School; Biftu Nekemte Secondary School; Leka Nekemte Secondary School; and Kumsa Moroda Secondary School. Finally, we selected one from a private school, Bethel Academy. The selected schools were again stratified and a new sampling frame were constructed. Finally, the study participants were selected using a simple random sampling technique via the lottery method.
Study variables
The dependent variable was primary dysmenorrhea. Whereas, socio-demographic factors included age, marital status, residence, educational status of the mother, and educational status of the father, psychosocial and behavioral factors: smoking, physical exercise, attempted weight loss, anxiety, drinking coffee, drinking tea, drinking soft drinks, chocolate consumption, sexual intercourse, and social disruption, reproductive factors included age at menarche, parity, menses flow, menses interval, duration of menses, and family history of dysmenorrhea were independent variables.
Operational definition
Primary dysmenorrhea was considered to indicate PD if she said “Yes” about pain during menses and had one or more of the following complaints: abdominal pain, groin pain, pelvic pain, back pain, or thigh pain before and/or during her menstrual periods within the past 6 months (15).
The visual analog scale (VAS) was used to assess students' degree of menstrual pain on a 10-cm line. One extremity of the line represented “unimaginably pain”, and the other extremity represented “no pain at all”. The participants were asked to rate the degree of pain by making a mark on the line. Study participants were classified as mild pain if they were between 1 and 3 points, moderate if they were between 4 and 7 points, and severe if they were between 8 and 10 points (32).
Physical activity: The habit of physical activity was measured by the participants' self-reports of not at all, irregularly or regularly (31).
The menstrual characteristics were as follows: long cycle: cycle returning once every >35 days; short (frequent) cycle: cycle recurring once every <21 days; short duration: duration of menses <3 days; and long duration: duration of period >7 days. Heavy menses were considered if a student changed 3 or more sanitary/vulvar pads per day but was scant if one or less (10, 15).
Social disruption was considered if a student said yes to trouble in social networks such as with family, friends, or people you loved in the past 6 months.
Sexually active: considered if students had at least one genital-to-genital contact.
Family history: Study participants with a positive family history of PD, where a first-degree relative (either mother, sister or grandmother) had a history of menstrual pain (33).
Attempted Weight loss: The habit of attempted weight loss was measured by the participants' self-reports of yes or no.
Ethical concern
Ethical approval was obtained from the Institutional Review Board (IRB) of Wallaga University (WU). The selected school's directors were formally requested with a written letter to ensure their consent before starting the data collection. Written and signed consent and assent was obtained from the students regarding their agreement to participate in the study after the objective of the study was explained to them. All appropriate ethical principles under the Helsinki declaration were followed and respected.
Data quality assurance and analysis
The quality of the data was ensured during collection, coding, entry, and analysis. The principal investigator and supervisor were included in the observation of how the study participants administered the questionnaires. The questionnaire and each School's section during the data collection were coded so that any identified errors could be traced back using the codes.
The facilitators, supervisors, and principal investigators checked the questionnaire daily for completeness. The pretest was administered to 27 (5%) female Gute High School students. In addition, experts in the field checked the faces' validity.
The questionnaire was first manually checked for completeness, after which the data were coded, entered in Epi Data version 3.1 and subsequently exported to SPSS version 25 for data analysis. Descriptive statistics, such as frequency, percentage, mean, and standard deviation, were used to describe the study population and their management practices. Both bivariable and multivariable logistic regression analyses were used to identify factors associated with the outcome variable. For the bivariable logistic regression, the crude odds ratio (COR) and 95% CI were calculated, and for the multivariable logistic regression, the adjusted odds ratio (AOR) and 95% CI were calculated. In the bivariable analysis, all variables with p values less than 0.25 were considered candidates for multivariate analysis (19). Hosmer and Lemeshow's goodness-of-fit test was performed to assess whether the required assumptions were fulfilled, and the variance inflation factors were used to assess the presence of multicollinearity. An adjusted odds ratio (OR) with 95% confidence intervals (CIs) and a p value less than 0.05 were considered to indicate a statistically significant association. Finally, text, tables, and graphs were used to present the results.
Results
Sociodemographic characteristics
In this study, 534 self-administered questionnaires were distributed, and almost all of the questionnaires were completed, for a response rate of 532 (99.6%). Two participants did not voluntarily participate in the study. The students involved in the study were aged between 15 and 22 years, with a mean age and standard deviation of 17.76 ± 1.5 years.
With regard to the ethnicity of the study participants, five hundred (94.0%) were Oromo, and 370 (69.5%) were protestant in religion. Five hundred fifteen (96.8%) and 480 (90.2%) of the study participants were single and urban residents, respectively.
Data relating to parents' educational status showed that 144 (27.1%) of the fathers had a diploma and above, while only 73 (13.7%) of the mothers had a diploma and above (Table 1).
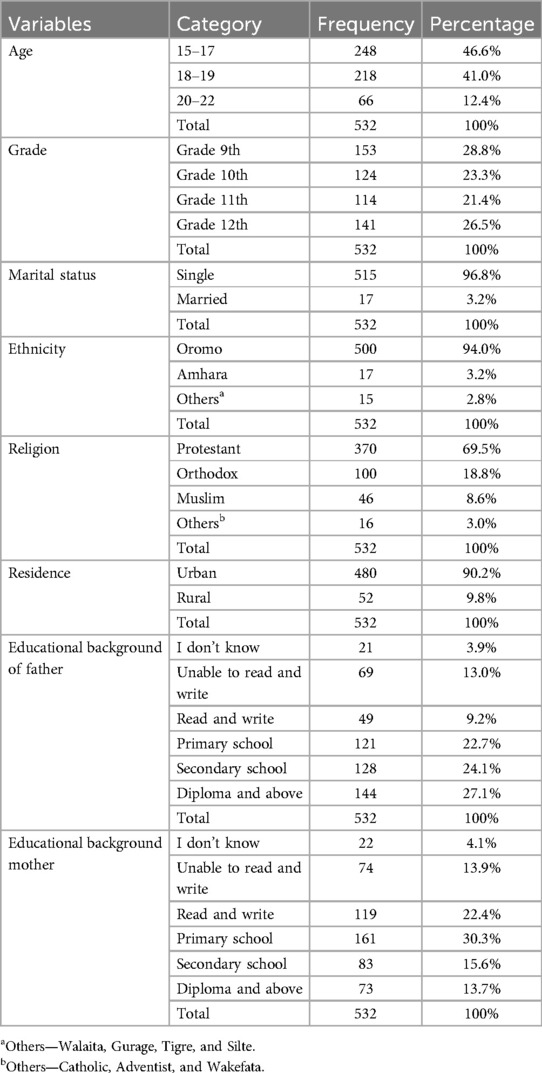
Table 1. Sociodemographic characteristics of female high school students in Nekemte Town, Western Oromia, Ethiopia, 2023.
Psychosocial and behavioral characteristics
Among the study participants, 141 (26.5%) attempted weight loss, and 231 (43.4%) started sexual intercourse. Concerning physical activity, approximately two-tenths of the 105 (19.7%) participants exercised regularly, and none of them chewed khat or smoked cigarettes.
Regarding drinking habits, more than nine-tenths (484; 91.0%) of the study participants had never drank alcohol, approximately one-third (164; 30.8%) had never drank tea at all, and nearly half (260; 48.8%) had never drank coffee at all.
More than half (278; 52.3%) of the study participants did not drink soft drinks, and 246 (46.2%) of them did not consume chocolate.
Regarding the history of anxiety of the study participants, the majority (443; 83.3%) had a history of anxiety, and more than half (236; 55.6%) of them did not have a history of social disruption, such as family, friends or loved ones, in the past 6 months (Table 2).
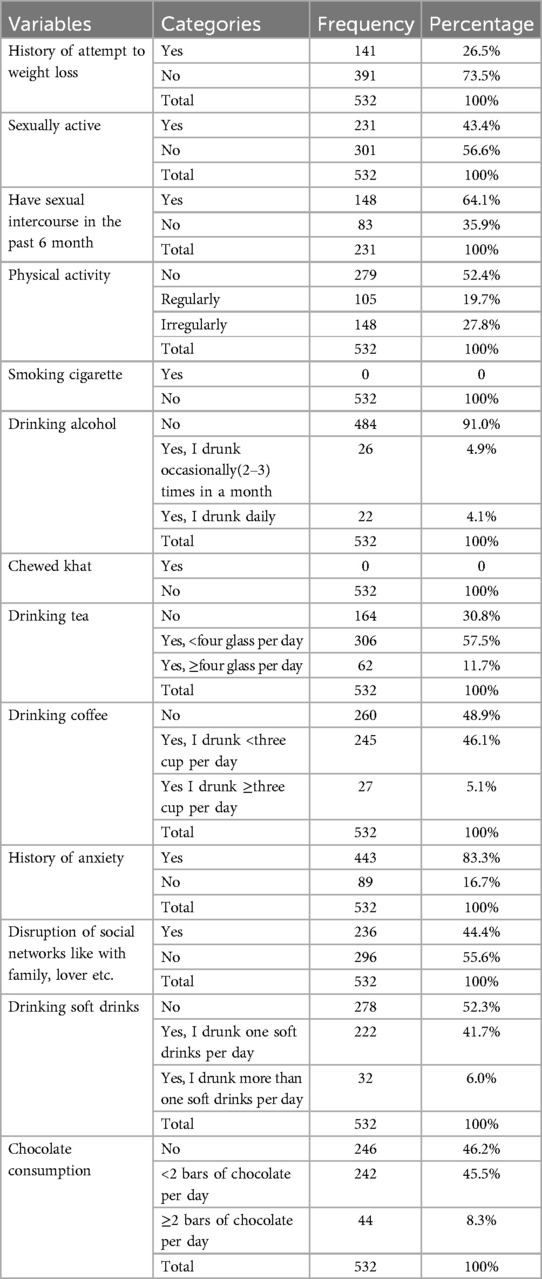
Table 2. Psychosocial and behavioral characteristics of female high school students in Nekemte Town, Western Oromia, Ethiopia, 2023.
Reproductive characteristics
The mean age at menarche of the study participants was 13.11 ± 1.18 years (SD). Among them, more than half (317; 59.6%) started their first menstruation between the ages of 13 and 14 years.
Two hundred seventy-one (50.9%) of the study participants had irregular menstruation, and more than half (304; 57.1%) of the menstrual cycle was between 21 and 35 days, which lasted for 2–5 days in 375 (70.5%) of the study participants. Three hundred and sixty-six (68.8%) of them had changed ≥3 pads per day per cycle.
Concerning the family history of the study participants, 226 (42.5%) had a family history of PD, and 509 (95.7%) had never given birth (Table 3).

Table 3. Reproductive characteristics of female high school students in Nekemte Town, Western Oromia, Ethiopia, 2023.
The magnitude and menstrual characteristics of PD
In this study, the magnitude of PD was 364 (68.4%) (95% CI (64.3%, 72.0%). Among the students who had PD, the majority (249; 68.4%) had moderate to severe pain (Figure 1).

Figure 1. Magnitude of primary dysmenorrhea among female high school students in Nekemte Town, East Wallaga, Western Oromia, Ethiopia, 2023.
Among the dysmenorrheic study participants, 96 (26.4%) had been missing from school in the past 6 months due to pain during menstruation.
Of the dysmenorrhic study participants, 157 (43.1%) had started experiencing pain within 3 months of puberty; 159 (43.7%) had pain starting from the first day of menses, which persisted for 2–3 days 288 (79.1%) and was located in the lower back 232 (63.7%). In addition, 149 (40.9%) of the study participants experienced headache, and 117 (32.1%) felt restless or anxious during their painful period (Table 4), (Figure 2).
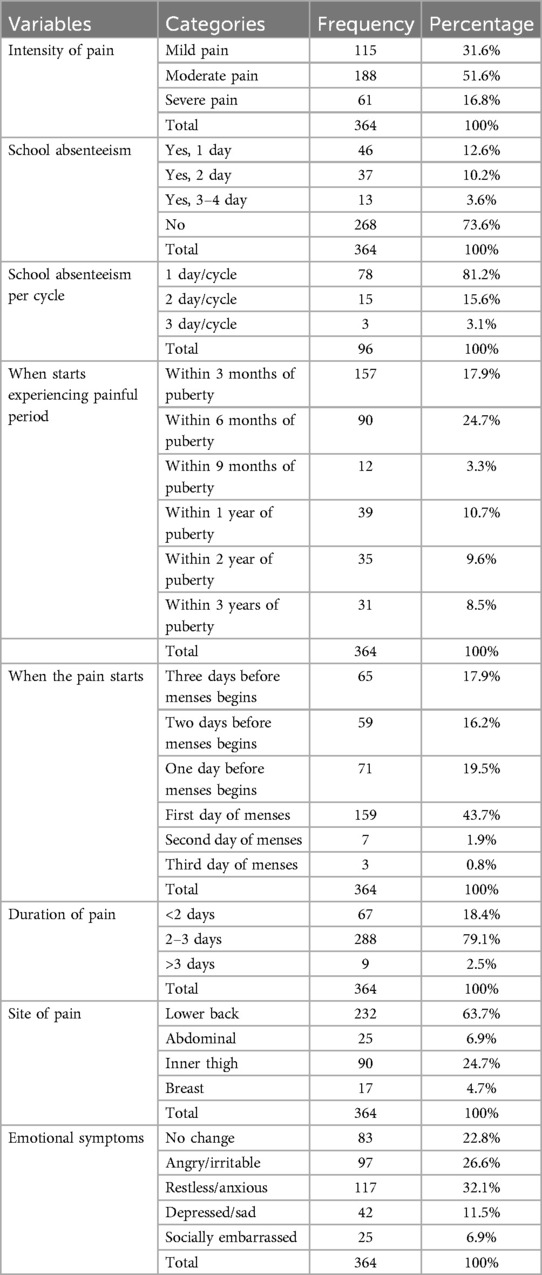
Table 4. Magnitude and menstrual characteristics of female high school students in Nekemte Town, Western Oromia, Ethiopia, 2023.
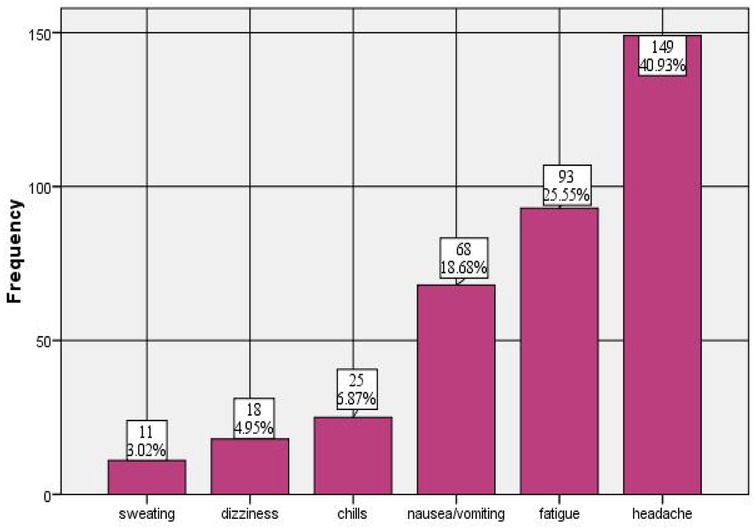
Figure 2. Symptoms of primary dysmenorrhea among female high school students in Nekemte Town, Western Oromia, Ethiopia, 2023.
Bivariate and multivariable logistic regression analysis
The results from the multivariate logistic regression analysis showed that sexual intercourse, drinking tea, history of anxiety, family history, and physical activity were variables that were significantly related to primary dysmenorrhea.
The results of the analysis showed that the odds of having PD were 4.64 times greater for students with a positive family history of primary dysmenorrhea than for those who did not have a family history of PD (AOR 4.64, 95% CI: 2.74, 7.86). Similarly, the odds of having PD were 2.41 times greater for those with a history of anxiety than for their counterparts (AOR 2.41, 95% CI = 1.31, 4.43).
Students who performed regular physical activities were 0.06 less likely to develop PD than were those who did not perform any physical activities (AOR 0.06, 95% CI = 0.03, 0.11). In addition, students who drank less than four glasses per day were 0.38 less likely to develop PD than were those who did not drink tea at all (AOR = 0.38, 95% CI = 0.22, 0.60). In addition, those who had sexual intercourse were 0.34% less likely to develop PD than were those who had not had sexual intercourse in the past 6 months (AOR = 0.34, 95% CI = 0.21, 0.55) (Table 5).
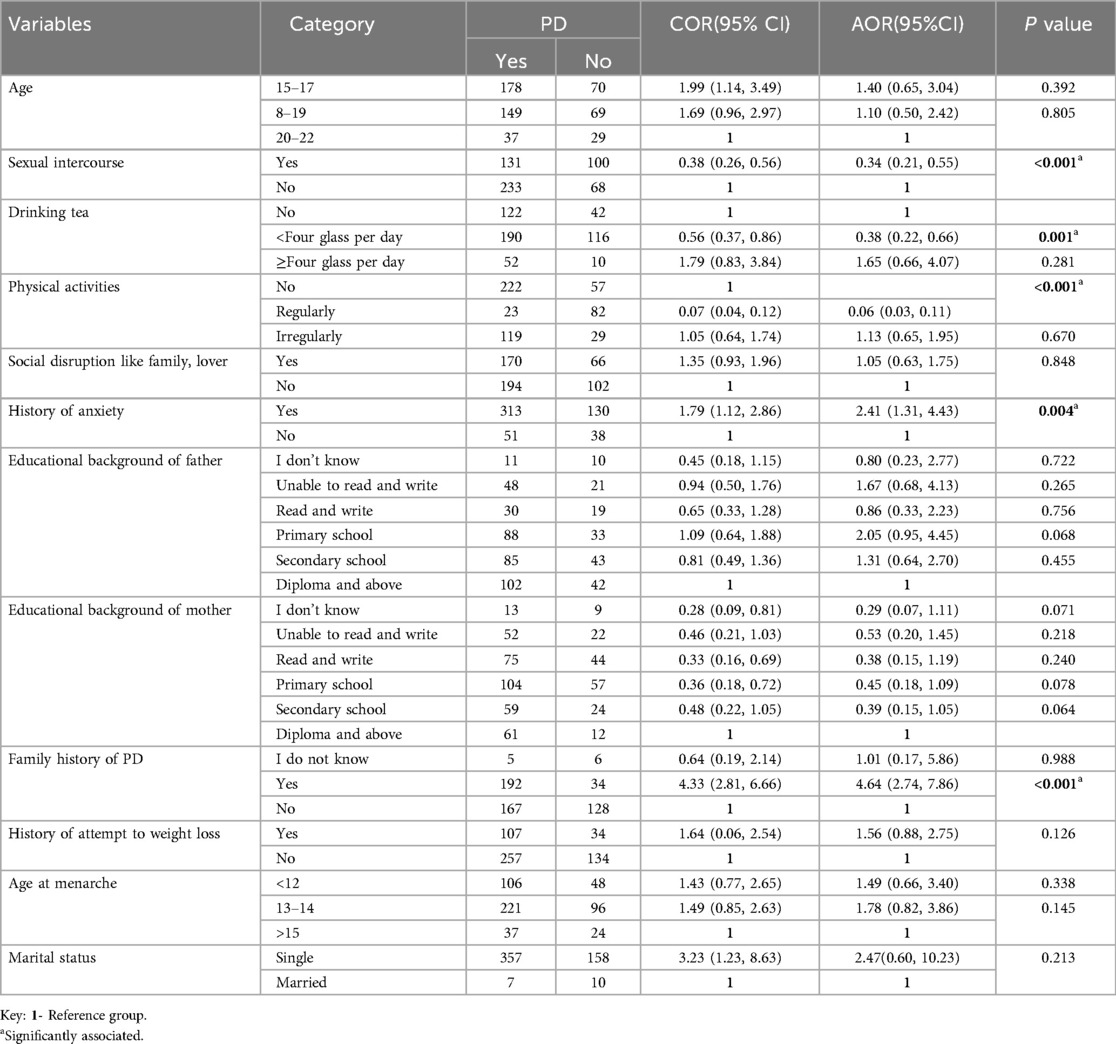
Table 5. Multiple logistic regression results for female high school students in Nekemte Town, Western Oromia, Ethiopia, 2023.
Discussion
Primary dysmenorrhea is often disregarded by affected adolescents who believe pain to be a normal part of the menstrual cycle. Thus, many study participants fail to seek treatment (6). It has adverse consequences for personal, family, and social life, resulting in short-term school and work absenteeism (3, 10). Having a better understanding of this problem will improve the understanding of primary dysmenorrhea among adolescents even at the family, school and community levels and help to improve the quality of life and academic performance of adolescent girls. Therefore, this study aimed to assess the magnitude of primary dysmenorrhea, its associated factors, and management practices among female high school students in Nekemte town, Western Oromia, Ethiopia.
This study showed that the magnitude of primary dysmenorrhea was 68.4%, which means that out of 100 students, 68 had PD. This magnitude was in line with previous studies conducted in the East Hararghe Zone (69.3%) (31), Wolaita Sodo town (70%) (19), Haramaya University (64.7%) (34), Debremarkos town (69.26%) (15) and Debra Berhan University (66.8%) (27) in Ethiopia and Ghana (68.1%) (35).
However, this percentage was slightly greater than that reported in studies conducted at Hawassa University (51.5%) (20) in Ethiopia; Enugu State; Nigeria (51.1%) (24); and Chinese college students (51.1%) (22). This variation may be due to differences in the operational definitions, study population, age and factors like diet, local health care and stress. This implies that PD affects a significant proportion of the students, so health policy may be applied in Schools.
On the other hand, the prevalence of bias in this population was slightly lower than that reported in studies of Gondar university students (77.6%) (14) and Debra Berhan University (85.4%) in North Ethiopia (10); Benin (78.35%) (23); Ibadan State; Nigeria (73%) (12); and Parakou, Benin (72.6%) (36). Furthermore, the proportions of studies conducted in Riyadh, King Dom of Saudi Arabia (92.3%) (21), King Saud University, Riyadh, Saudi Arabia (80.1%) (18), Iran (89.1%) (37), and Lebanon (80.9%) (33) were much greater than those in this study. A reason for the variation in this study could be age variation and the operational definition of primary dysmenorrhea; many studies use the definition of dysmenorrhea in general. Another reason for the variation could be differences in sociocultural, ethnic and lifestyle factors among the study participants.
In this study, the odds of PD were approximately 2.41 times greater for students who had a history of anxiety than for those with no history of anxiety. This finding was supported by studies performed at Haramaya University, Eastern Ethiopia, and Debra Berhan University, North Ethiopia (10, 13). However, no statistically significant association was reported between anxiety and PD in Hawassa University students (20). This may be because of differences in the measurements used; i.e., in this study, anxiety was measured by students' self-reports as yes or no for the past 6 months, whereas at Hawassa University, students were asked about anxiety only related to tests or assignments. Therefore, it would be helpful if the schools taught students ways of overcoming stress, like deep relaxation, muscle relaxation (exercise), cultivating positive relationships with their friends and teachers, and engaging in enjoyable activities.
This study revealed that sexual intercourse decreased the risk of primary dysmenorrhea by 66% compared with that of their counterpart, which is comparable with the findings of studies performed in Debremarkos town, northwestern Ethiopia (15). The reason may be that during the orgasm of sexual intercourse, the muscle of the uterus contracts and then relaxes, which leads to some relief from pain. In addition, sex activates the release of chemical endorphins, which make individuals feel good, and engaging in sexual activity exacerbates menstrual discomfort (38).
In this study, students with a family history of dysmenorrhea had an approximately 4.6-fold greater risk of developing PD than did those without dysmenorrhea. These findings are in line with those of other studies from Ethiopia (10, 15, 19, 20, 31), Iran (37), Lebanon (33), Saudi Arabia (16), and Australia (30). This could be related to coping behaviors from mothers to control pain. A genetics might also have a psychological impact, as girls may react to menstruation similarly to their mothers, and they may share the same outlook on menstruation (39). Therefore, there would be a strategy for educating families of students about PD.
This study revealed that students who drank tea tended to experience primary dysmenorrhea alleviation. Those who consumed <4 cups/day of tea were 53% less likely to report having mild PD than nondrinkers were. Different studies support these results; case control study done at Debra Berhan town (40), cross sectional study Debra Berhan university (10), and Shanghai, China (41). However, other studies contradict this finding: a study was performed at Debre Markos town (15) and Haramaya University (13). This possibility requires further study.
In this study, regular physical activity was found to be significantly associated with the occurrence of PD (AOR = 0.06; 95% CI = 0.22, 0.60), which was in line with the findings in Debre Markos town (15) and Lebanon (33). Nevertheless, no statistically significant associations were reported between physical activity and PD in Saudi Arabia (18) or at Haramaya University (13). This difference may be because of differences in physical activity. In this study, physical activity was self-reported by the participants as not at all, irregularly, or regularly. Similarly, in Saudi Arabia, participants were asked whether they had not participated, 1–2 times per week, 3–4 times per week, or 5–6 times per week and daily, respectively. In addition, Haramaya University asked respondents if they were yes or no questions. This reqquires further studies.
Limitation of the study
The diagnosis of primary dysmenenorrhea was made only by history of the students.
Recall bias and over or under reporting of the condition may be present.
Conclusion
In this study, the overall magnitude of primary dysmenorrhea among Nekemte town high school students was found to be high.
Individuals with a positive family history and anxiety were more likely to be symptomatic, and those who drank <4 cups of tea per day and who had sexual intercourse and physical activity were less likely to have primary dysmenorrhea.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Wollega university review committee. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
BG: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. TA: Conceptualization, Data curation, Project administration, Resources, Software, Validation, Visualization, Writing – review & editing. LS: Conceptualization, Data curation, Formal Analysis, Project administration, Resources, Software, Supervision, Validation, Writing – review & editing. EZ: Conceptualization, Data curation, Formal Analysis, Methodology, Validation, Writing – original draft. MA: Investigation, Methodology, Project administration, Resources, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article. The lack of funding was transparent, and none of the authors received any form of credit. However, Wallaga University is acknowledged for its contribution to data collection.
Acknowledgments
Authors acknowledge study participants and data collectors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnote
1. ^Bureau NE. Data of Nekemte town high school students (2023).
References
1. Burnett M, Lemyre M. No. 345-Primary dysmenorrhea consensus guideline. J Obstet Gynaecol Can. (2017) 39(7):585–95. doi: 10.1016/j.jogc.2016.12.023
2. Committee on Adolescent Health Care, Geri D, Hewitt MA, Karen R, Gerancher M. ACOG committee opinion no. 760: dysmenorrhea and endometriosis in the adolescent. Obstet Gynecol. (2018) 132(6):e249–58. doi: 10.1097/AOG.0000000000002978
3. Kho KA, Shields JK. Diagnosis and management of primary dysmenorrhea. JAMA. (2020) 323(3):268–9. doi: 10.1001/jama.2019.16921
4. Iacovides S, Avidon I, Baker FC. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update. (2015) 21(6):762–78. doi: 10.1093/humupd/dmv039
5. Ferries-Rowe E, Corey E, Archer JS. Primary dysmenorrhea. Obstet Gynecol. (2020) 136(5):1047–58. doi: 10.1097/AOG.0000000000004096
6. Itani R, Soubra L, Karout S, Rahme D, Karout L, Khojah HMJ. Primary dysmenorrhea: pathophysiology, diagnosis, and treatment updates. Korean J Fam Med. (2022) 43(2):101–8. doi: 10.4082/kjfm.21.0103
7. Barcikowska Z, Rajkowska-Labon E, Grzybowska ME, Hansdorfer-Korzon R, Zorena K. Inflammatory markers in dysmenorrhea and therapeutic options. Int J Environ Res Public Health. (2020) 17(4):1191. doi: 10.3390/ijerph17041191
8. Bernardi M, Lazzeri L, Perelli F, Reis FM, Petraglia F. Dysmenorrhea and related disorders. F1000Res. (2017) 6:1645. doi: 10.12688/f1000research.11682.1
9. Sharghi M, Mansurkhani SM, Larky DA, Kooti W, Niksefat M, Firoozbakht M, et al. An update and systematic review on the treatment of primary dysmenorrhea. JBRA Assist Reprod. (2019) 23(1):51–7. doi: 10.5935/1518-0557.20180083
10. Hailemeskel S, Demissie A, Assefa N. Primary dysmenorrhea magnitude, associated risk factors, and its effect on academic performance: evidence from female university students in Ethiopia. Int J Women’s Health. (2016) 8:489–96. doi: 10.2147/IJWH.S112768
11. Al-Matouq S, Al-Mutairi H, Al-Mutairi O, Abdulaziz F, Al-Basri D, Al-Enzi M, et al. Dysmenorrhea among high-school students and its associated factors in Kuwait. BMC Pediatr. (2019) 19(1):80. doi: 10.1186/s12887-019-1442-6
12. Femi-Agboola DM, Sekoni OO, Goodman OO. Dysmenorrhea and its effects on school absenteeism and school activities among adolescents in selected secondary schools in Ibadan, Nigeria. Niger Med J. (2017) 58(4):143–8. doi: 10.4103/nmj.NMJ_47_17
13. Mesele TT, Dheresa M, Oljira L, Wakwoya EB, Gemeda GM. Prevalence of dysmenorrhea and associated factors among haramaya university students, eastern Ethiopia. Int J Women’s Health. (2022) 14:517–27. doi: 10.2147/IJWH.S333447
14. Gebeyehu MB, Mekuria AB, Tefera YG, Andarge DA, Debay YB, Bejiga GS, et al. Prevalence, impact, and management practice of dysmenorrhea among university of gondar students, northwestern Ethiopia: a cross-sectional study. Int J Reprod Med. (2017) 2017:1. doi: 10.1155/2017/3208276
15. Muluneh AA, Nigussie TS, Gebreslasie KZ, Anteneh KT, Kassa ZY. Prevalence and associated factors of dysmenorrhea among secondary and preparatory school students in debremarkos town, north-west Ethiopia. BMC Women’s Health. (2018) 18(1):57. doi: 10.1186/s12905-018-0552-x
16. Ali A, Ali A, Alotaibi N, Alsufyani M, Alotaibi A, Almutairi M, et al. Prevalence, impact, and management perception of dysmenorrhea among university students: a cross-sectional study. Braz J Pharm Sci. (2022) 58. doi: 10.1590/s2175-97902022e20458
17. de Las Mercedes Villa Rosero CY, Mazin SC, Nogueira AA, Vargas-Costales JA, Rosa ESJC, Candido-Dos-Reis FJ, et al. Prevalence of chronic pelvic pain and primary dysmenorrhea in women of reproductive age in Ecuador. BMC Womens Health. (2022) 22(1):363. doi: 10.1186/s12905-022-01948-y
18. Hashim RT, Alkhalifah SS, Alsalman AA, Alfaris DM, Alhussaini MA, Qasim RS, et al. Prevalence of primary dysmenorrhea and its effect on the quality of life amongst female medical students at king saud university, Riyadh, Saudi Arabia. A cross-sectional study. Saudi Med J. (2020) 41(3):283–9. doi: 10.15537/smj.2020.3.24988
19. Mammo M, Alemayehu M, Ambaw G. Prevalence of primary dysmenorrhea, its intensity and associated factors among female students at high schools of Wolaita Zone, Southern Ethiopia: cross-sectional study design. Int J Women’s Health. (2022) 14:1569–77. doi: 10.2147/IJWH.S384275
20. Tadese M, Kassa A, Muluneh AA, Altaye G. Prevalence of dysmenorrhoea, associated risk factors and its relationship with academic performance among graduating female university students in Ethiopia: a cross-sectional study. BMJ Open. (2021) 11(3):e043814. doi: 10.1136/bmjopen-2020-043814
21. Bakhsh H, Algenaimi E, Aldhuwayhi R, AboWadaan M. Prevalence of dysmenorrhea among reproductive age group in Saudi women. BMC Women’s Health. (2022) 22(1):78. doi: 10.1186/s12905-022-01654-9
22. Chen L, Tang L, Guo S, Kaminga AC, Xu H. Primary dysmenorrhea and self-care strategies among Chinese college girls: a cross-sectional study. BMJ Open. (2019) 9(9):e026813. doi: 10.1136/bmjopen-2018-026813
23. Sidi I, Hounkpatin B, Obossou AAA, Salifou K, Vodouhe M, Denakpo J, et al. Primary dysmenorrhea in the schools of Parakou: prevalence, impact and therapeutic approach. Gynecol Obstet (Sunnyvale). (2016) 6:376. doi: 10.4172/2161-0932.1000376
24. Onu A, Aluh D, Ikehi M. Prevalence and management of dysmenorrhea among secondary school adolescents in Enugu State, Nigeria. Res Square. (2020). doi: 10.21203/rs.3.rs-109221/v1
25. Ballantyne JC, Cousins MJ. Primary dysmenorrhea: an urgent mandate. (2013). https://api.semanticscholar.org/CorpusID:269398699
26. Chen CX, Shieh C, Draucker CB, Carpenter JS. Reasons women do not seek health care for dysmenorrhea. J Clin Nurs. (2018) 27(1–2):e301–8. doi: 10.1111/jocn.13946
27. Derseh B, Hailegiorgies K, Afessa N, Temesgen M. Prevalence of dysmenorrhea and its effects on school performance: a cross-sectional study. J Womens Health Care. (2017) 6(2):6. doi: 10.4172/2167-0420.1000361
28. Azagew AW, Kassie DG, Walle TA. Prevalence of primary dysmenorrhea, its intensity, impact and associated factors among female students’ at Gondar town preparatory school, Northwest Ethiopia. BMC Women’s Health. (2020) 20(1):5. doi: 10.1186/s12905-019-0873-4
29. Ethiopian Minister of Education and Minister of Health. Ethiopia-School-Health-Program-Framework. Ministry of Health (2017). p. 27–32.
30. Ju H, Jones M, Mishra G. The prevalence and risk factors of dysmenorrhea. Epidemiol Rev. (2014) 36:104–13. doi: 10.1093/epirev/mxt009
31. Mohammed H, Hassen N, Musa A. Dysmenorrhea and associated factors among secondary school students in East Hararghe zone, Eastern Ethiopia. East Afr. J. Health Biomed Sci. (2019) 3(1):39–48.
32. Sung YT, Wu JS. The visual analogue scale for rating, ranking and paired-comparison (VAS-RRP): a new technique for psychological measurement. Behav Res Methods. (2018) 50(4):1694–715. doi: 10.3758/s13428-018-1041-8
33. Karout S, Soubra L, Rahme D, Karout L, Khojah HMJ, Itani R. Prevalence, risk factors, and management practices of primary dysmenorrhea among young females. BMC Women’s Health. (2021) 21(1):392. doi: 10.1186/s12905-021-01532-w
34. Mesele TT, Ayalew HG, Syoum AT, Antehneh TA. Impact of dysmenorrhea on academic performance among Haramaya university undergraduate regular students, eastern Ethiopia. Front Reprod Health. (2022) 4:939035. doi: 10.3389/frph.2022.939035
35. Acheampong K, Baffour-Awuah D, Ganu D, Appiah S, Pan X, Kaminga A, et al. Prevalence and predictors of dysmenorrhea, its effect, and coping mechanisms among adolescents in Shai Osudoku District, Ghana. Obstet Gynecol Int. (2019) 2019:1. doi: 10.1155/2019/5834159
36. Vodouhe M, Imorou R, Atade R, Salifou K, Vignonzan U, Hounkponou N, et al. Prevalence and factors associated with dysmenorrhea in Parakou, Benin. Open J Obstet Gynecol. (2020) 10:1000–10. doi: 10.4236/ojog.2020.1080095
37. Habibi N, Huang MS, Gan WY, Zulida R, Safavi SM. Prevalence of primary dysmenorrhea and factors associated with its intensity among undergraduate students: a cross-sectional study. Pain Manag Nurs. (2015) 16(6):855–61. doi: 10.1016/j.pmn.2015.07.001
38. Mollazadeh S, Sadeghzadeh Oskouei B, Kamalifard M, Mirghafourvand M, Aminisani N, Jafari Shobeiri M. Association between sexual activity during menstruation and endometriosis: a case-control study. Int J Fertil Steril. (2019) 13(3):230–5. doi: 10.22074/ijfs.2019.5601
39. Shiferaw MT, Wubshet M, Tegabu D. Menstrual problems and associated factors among students of Bahir Dar university, Amhara national regional state, Ethiopia: a cross-sectional survey. Pan Afr Med J. (2014) 17:246. doi: 10.11604/pamj.2014.17.246.2230
40. Zeru AB, Muluneh MA. Thyme tea and primary dysmenorrhea among young female students. Adolesc Health Med Ther. (2020) 11:147–55. doi: 10.2147/AHMT.S280800
Keywords: primary dysmenorrhea, associated factors, Nekemte, Ethiopia, high school
Citation: Gindaba BG, Abera Gudeta T, Sebu LD, Zerihun Gindaba E and Abdisa MT (2025) Primary dysmenorrhea and its associated factors among female high school students in Nekemte town, East Wallaga Zone, Western Oromia, Ethiopia: a cross-sectional study. Front. Reprod. Health 6:1451551. doi: 10.3389/frph.2024.1451551
Received: 20 June 2024; Accepted: 16 December 2024;
Published: 7 January 2025.
Edited by:
Astawus Alemayehu, Haramaya University, EthiopiaReviewed by:
Azna Zuberi, Northwestern University, United StatesSamal Nauhria, St. Matthew's University, Cayman Islands
Copyright: © 2025 Gindaba, Abera Gudeta, Sebu, Zerihun Gindaba and Abdisa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bekan Gudata Gindaba, YmVrYW5ndWRhdGExNTBAZ21haWwuY29t