
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Reprod. Health , 18 April 2024
Sec. HIV and STIs
Volume 6 - 2024 | https://doi.org/10.3389/frph.2024.1323926
 Alice Manjate1,2
Alice Manjate1,2 Gladys Sergon1
Gladys Sergon1 Darlenne Kenga2
Darlenne Kenga2 Daniel Golparian3
Daniel Golparian3 Yuriy Tyulenev4
Yuriy Tyulenev4 Osvaldo Loquilha5Fabião Mausse2Alexander Guschin4
Osvaldo Loquilha5Fabião Mausse2Alexander Guschin4 José Carlos Langa2Alfeu Passanduca2
José Carlos Langa2Alfeu Passanduca2 Jahit Sacarlal2
Jahit Sacarlal2 Magnus Unemo1,3,6*
Magnus Unemo1,3,6*
In Mozambique, sexually transmitted infections (STIs) are estimated to be prevalent, but diagnosis and treatment of curable STIs rely only on syndromic management. We examined the prevalence of four non-viral STIs and HIV-1/2, based on etiological diagnosis, associations with sociodemographic and behavioural factors, and the STI diagnostic accuracy of the vaginal discharge syndromic management in women with urogenital complaints in Maputo, Mozambique. A cross-sectional study was performed in Maputo, Mozambique, February 2018–January 2019, enrolling 924 women of reproductive age with urogenital complaints. Endocervical/vaginal swabs were sampled and chlamydia, gonorrhoea, trichomoniasis and Mycoplasma genitalium infections were diagnosed using a multiplex real-time PCR (AmpliSens; InterLabServices). Serological testing was performed for HIV-1/2. A structured questionnaire collected metadata. All data were analyzed in STATA/IC 12.1 using descriptive statistics, chi-square tests and logistic regression model. About 40% of the women were less than 24 years old, 50.8% were single, 62.1% had their sexual debut between 12 and 17 years of age, and the main complaint was vaginal discharge syndrome (85%). The prevalence of chlamydia was 15.5%, trichomoniasis 12.1%, gonorrhoea 4.0%, M. genitalium 2.1%, and HIV-1/2 22.3%. The vaginal discharge syndrome flowchart had a sensitivity of 73.0%–82.5% and a specificity of 14%–15% for the detection of any individual non-viral STI in women with urogenital complaints. In total, 19.2% of the symptomatic women with chlamydia, trichomoniasis or gonorrhoea would not be detected and accordingly treated using the vaginal discharge syndromic management (missed treatment) and 70.0% of the women would be treated despite not being infected with any of these three STIs (overtreatment). In conclusion, a high prevalence of especially chlamydia, trichomoniasis, and HIV-1/2 was found in women of childbearing age with urogenital complaints in Maputo, Mozambique. Syndromic management of vaginal discharge revealed low accuracy in the detection of STIs in symptomatic women, especially low specificity, which resulted in under-treatment of STI-positive cases and incorrect or over-treatment of women with urogenital complaints, many of whom were negative for all the non-viral STIs. Etiological diagnosis is imperative for effective management of STIs in symptomatic and asymptomatic women.
Sexually transmitted infections (STIs), including HIV-1/2, remain neglected public health problems with a significant burden of mortality and especially morbidity worldwide (1–4). The World Health Organization (WHO) estimates that more than 1 million new global cases of curable STIs are acquired every day, i.e., 374 million estimated global cases of trichomoniasis (etiological agent: Trichomonas vaginalis), chlamydia (Chlamydia trachomatis), gonorrhoea (Neisseria gonorrhoeae), and syphilis (Treponema pallidum subspecies pallidum) among adults in 2022 (3, 4). Sub-Saharan Africa is the most affected subregion, with about 40% of the global burden of non-viral STIs, i.e., approximately 60 million new gonorrhoea, chlamydia and trichomoniasis cases estimated annually, with the 15–24 years age group being the most affected (5–7). In Mozambique, the estimated prevalence of non-viral STIs, based on interviews in the population of reproductive age, was in 2015 7% among women and 5% among men (8), however, no STI prevalence or incidence data based on etiological diagnosis of STIs are available. Furthermore, Mozambique is among the top ten countries in the world with the highest HIV-1/2 prevalence rates (9).
Undetected, untreated, and/or inappropriately treated STIs can lead to complications and sequelae, which disproportionally affect women, including pelvic inflammatory disease, ectopic pregnancy, foetal or neonatal death, premature birth, infertility, and increased acquisition and transmission of HIV-1/2 (1, 7, 10). Early diagnosis and appropriate treatment are essential for the prevention of transmission, complications, and sequelae of STIs. However, in countries with limited resources, etiological diagnosis of most non-viral STIs (syphilis is the main exception) remains difficult due to the lack of facilities, qualified technical personnel and financial resources (11, 12).
In 1985, due to the limited access to and funding for etiological STI diagnosis in many less-resourced settings, WHO published the first guidelines regarding syndromic management of four common STI syndromes (urethral discharge, vaginal discharge, genital ulcers, and lower abdominal pain or pelvic inflammatory disease). Current WHO guidelines address six syndromes, the above four, which have been further optimized, plus scrotal swelling and neonatal conjunctivitis (13). These guidelines, sometimes slightly adjusted to local settings, are still used by many less-resourced countries for the management of STIs (1, 11, 14–16). Briefly, the syndromic management consists of grouping similar symptoms and signs caused by different STI pathogens and then using a combination of antimicrobial agents to treat these STIs (11, 13, 15, 17). Syndromic management is inexpensive, easy to perform and can be useful for immediate treatment of symptomatic patients at the point of care (POC). However, the diagnostic accuracy of the syndromic management of vaginal discharge has been shown highly suboptimal and a majority of urogenital chlamydial, gonorrhoea, and trichomoniasis cases are not detected and treated (because they are asymptomatic), while many cases are unnecessarily or incorrectly treated due to a suboptimal specificity (11, 14, 18–27), and Mycoplasma genitalium infections are not taken into account. The reasons for the poor performance of the syndromic management of vaginal discharge include both that STIs are frequently asymptomatic in women (1, 11, 17, 19, 23, 24, 28–30), and that vaginal discharge can additionally be caused by, for example, bacterial vaginosis and candidiasis (1, 11).
Accordingly, the syndromic management of vaginal discharge results in lack of treatment, incorrect treatment, and/or over-treatment, which promote the emergence of antimicrobial resistance (AMR) in STI agents, other pathogens and bystander commensal bacterial species, as well as negatively affect the normal vaginal microbiome (11, 14, 16, 26, 31). The increasing rates of AMR in N. gonorrhoeae and M. genitalium have made therapeutic options limited, and treatments of these and other STIs should ideally be informed by etiologic diagnoses (1, 17, 20, 32–34).
In Mozambique, as in most other Sub-Saharan African countries, only syndromic management of STIs has been used for more than three decades (3, 4, 35, 36). Consequently, data on prevalence of specific STIs, risk factors associated with these STIs, and the etiology of STI syndromes are completely lacking. This information is urgently needed to assess the effectiveness of the syndromic management of STIs, understand the burden of these STIs particularly in women of reproductive age, and inform revisions of STI treatment guidelines (37).
The aims of the present study were to examine women in reproductive age with urogenital complaints in Maputo, Mozambique to: (i) describe the prevalence of trichomoniasis, chlamydia, gonorrhoea, and M. genitalium infections using a real-time multiplex PCR (38) and HIV using serology, (ii) identify the sociodemographic and behavioural factors among the women associated with these STIs, and (iii) assess the accuracy (sensitivity and specificity) of the vaginal discharge syndrome management in use in Mozambique (Figure 1) to diagnose STIs and reproductive tract infections.
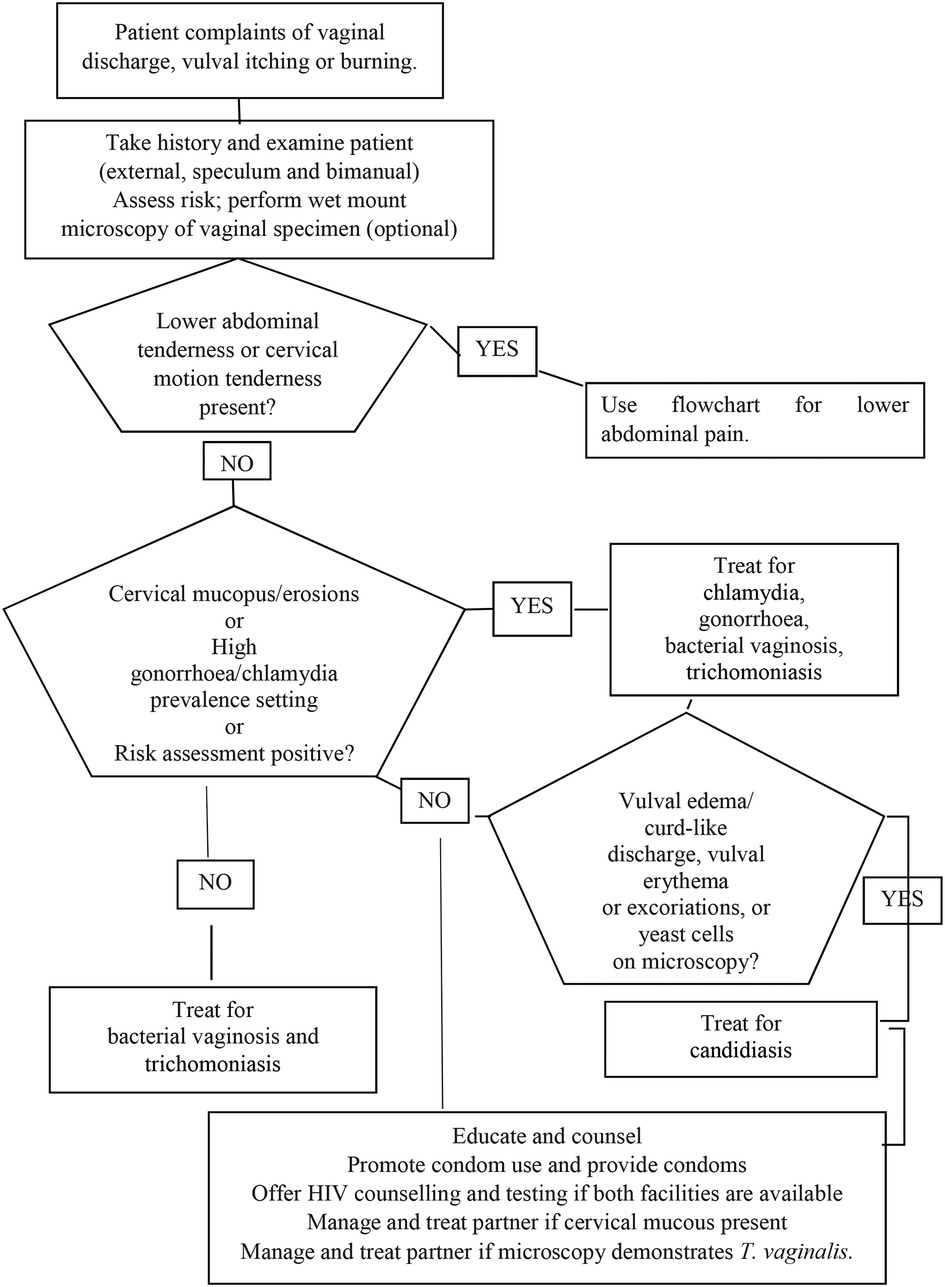
Figure 1. Flowchart for the management of vaginal discharge with bimanual and speculum examination.
This cross-sectional study was carried out in primary healthcare units belonging to the Mavalane sanitary area in Maputo, Mozambique, from February 2018 to January 2019, when 924 women were recruited. The Mavalane sanitary area comprises 12 health centres, namely Polana Caniço, Polana Cimento, 1° de Maio, 1° de Junho, Mavalane, Albazine, Romão, Pescadores, Hulene, Malhagalene, Inhaca, and Katembe. The province of Maputo had a population of about 2.22 million in 2017, of which 1.07 million were men and 1.15 million were women (39), with an estimated HIV-1/2 prevalence of 15.0% in women of reproductive age in 2021 (40).
Since maternal health nurses are generally the frontline health care providers for women with urogenital complaints, cervical cancer screening, and prenatal and family planning consultations in Mozambique, they were eligible researchers. Consequently, the selection of study sites was based on the existence of conditions for gynaecological examination and the availability of maternal health nurses as the main providers of reproductive health services for women. Thus, one hospital [Mavalane General Hospital (suburban)] and three primary health centres, i.e., 1° Junho Health Centre (rural), 1° Maio Health Centre (urban) and, Polana Caniço Health Centre (suburban) were selected because they were having the highest number of consultations for patients with gynaecological complaints.
A patient was eligible if she was between 18 and 49 years of age, had any urogenital complaints such as vaginal discharge, vaginal itching with/without burning, dyspareunia (pain during sexual intercourse), and/or lower abdominal pain, and signed the informed consent form. Fingerprints were collected for those who did not know how to sign. Women who were pregnant, menstruating at the time of consultation, had a positive cervical cancer screening result, reported having used antibiotics or vaginal douches in the last 15 days, had an indication for gynaecological surgery or had symptoms indicating the development of PID, such as spontaneous pelvic pain, were excluded from the study. All participants received counselling before and after a gynaecological examination by community health workers at each study site.
Investigators were trained in study procedures, data collection, and updated on WHO syndromic management for vaginal discharge.
Sociodemographic, behaviour and clinical data, such as previous STI infections, genital hygiene habits, STI symptoms at the time of interview, number of sexual partners in the last three months, age at first sexual intercourse, and others, were collected at enrolment using a framework standardized questionnaire.
Physical and gynaecological examinations, including speculum examination, were performed. All clinical information was recorded and transferred to the questionnaire. During the speculum examination, samples were collected from the lateral and posterior vaginal fornix and the endocervical canal according to standard procedures. Cell phone numbers were also recorded to allow for follow-up care. Women with symptoms of vaginal discharge syndrome were treated free of charge during the visit according to the national syndromic management guidelines (Figure 1), and women without symptoms of vaginal discharge syndrome were treated based on the results of Gram-stained microscopy.
Ethical approval for the study was obtained from the Mozambican National Bioethics Committee for Health (reference number 405/CNBS/2014). This approval has been renewed annually with the current renewal number ref 180/CNBS/23.
For the diagnosis of the non-viral STIs, from each participant, specimens from the lateral posterior vaginal fornix and endocervix were collected using sterile swabs, placed in Amies liquid transport medium, and frozen at −70°C. The vaginal/endocervical swab specimens were subsequently sent frozen on dry ice to the WHO Collaborating Centre for Gonorrhoea and Other STIs, Örebro University Hospital, Sweden for DNA extraction and multiplex PCR for diagnosis of chlamydia, gonorrhoea, trichomoniasis and M. genitalium infection. For diagnosis of HIV-1/2, 10 ml of venous blood was collected, using the vacutainer system. All samples were placed in a thermal box with ice blocks and transported daily to the Microbiology Laboratory of the Faculty of Medicine of the Eduardo Mondlane University, Maputo, Mozambique, where they were stored at −70°C prior to processing.
Whole blood samples were centrifuged at 8,000 rpm for 10–15 min. HIV-1/2 diagnosis was performed using the national serological testing algorithm, which is based on the use of two 3rd-generation rapid diagnostic tests (RDTs), namely, Alere Determine™ HIV-1/2 (Alere Medical Co. Ltd, Japan) and Uni-Gold™ HIV-1/2 (Trinity Biotech, Wicklow, Ireland). Discordant results were retested using the Enzygnost® HIV-1/2 Integral 4 ELISA (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany).
DNA was extracted from all the vaginal/cervical swab specimens using the QIAamp® DNA Mini Kit (Qiagen, GmbH, Hilden, Germany), in accordance with the manufacturer's instructions. Briefly, 300 µl of each vaginal/cervical swab specimen was centrifuged for 5 min at 5,000 × g (7,500 rpm), and the pellets were used for DNA extraction and purification with the QIAamp® DNA Mini Kit (Qiagen). The final elution was performed using 50 µl of elution buffer. The DNA extracts were stored at −20°C prior to real-time PCR (see below).
The CE/IVD-marked multiplex real-time AmpliSens N.gonorrhoeae/C.trachomatis/M.genitalium/T.vaginalis-MULTIPRIME-FRT PCR assay (InterLabService Ltd, Moscow, Russia) was performed, according to the manufacturer's instructions, for diagnosis of gonorrhoea, chlamydia, trichomoniasis and M. genitalium infections. This multiplex PCR assay has been previously evaluated with adequate results compared to the Aptima Combo 2 assay (detecting C. trachomatis and N. gonorrhoeae), Aptima T. vaginalis assay and Aptima M. genitalium assay (Hologic, San Diego, California, USA) (38). The AmpliSens N.gonorrhoeae/C.trachomatis/M.genitalium/T.vaginalis-MULTIPRIME-FRT PCR assay (InterLabService) is based on the amplification of regions of N. gonorrhoeae, C. trachomatis, M. genitalium, and/or T. vaginalis DNA using specific primers, which have been previously described (38). The PCR amplified product(s) is detected using fluorescent dyes linked to specific oligonucleotide probes, which bind specifically to the amplified product during PCR thermocycling, and these probes have also been previously described (38). Additionally, an internal control is added to the extraction procedure to control the extraction process and identify possible PCR inhibition. Briefly, 10 µl of extracted DNA template was added to each reaction tube and the final reaction volume was 25 µl. All PCR amplification reactions were carried out on the Rotor-Gene Q 6000 (QIAGEN, Hilden, Germany).
By the syndromic approach, women who had vaginal discharge, itching, or burning in the vulva, without lower abdominal pain were classified as having vaginal and/or cervical infection and received treatment for gonorrhoea, chlamydia, trichomoniasis, and bacterial vaginosis (Figure 1).
An external physical examination of the vulva and examination of the endocervix using a speculum was performed.
Data analysis was performed using multiple logistic regression in STATA/IC 12.1 (StataCorp LP, USA) with calculation of a 95% confidence intervals and odds ratio (OR). Pearson's χ2 test or Fisher's exact test (<5 observations) was used to determine statistically significant relationships between categorical variables. Significance was set at a p-value <0.05 for inference.
From February 2018 to January 2019, 1,048 women met the inclusion criteria. Of these, 47 (4.5%) women were excluded because they were menstruating at the time of consultation (n = 13), had used antimicrobials in the last 15 days (n = 11), were pregnant (n = 8), did not consent (n = 6), or accepting the gynaecological examination using speculum (n = 9). Seventy-seven additional cases were excluded from data analysis because they were missing sociodemographic and behavioural data or appropriate samples. The sociodemographic and behavioural characteristics of the final study participants (n = 924) are summarized in Table 1. Briefly, the age of the participants ranged from 18 to 49 years, with a median (mean) age of 28 (30) years. Many participants were under 24 years old (38.9%), more than half were single (50.8%), had secondary school level of education (54.4%), lived in rural areas (54.0%), and had their sexual debut between 12 and 17 years of age (62.1%) (Table 1).
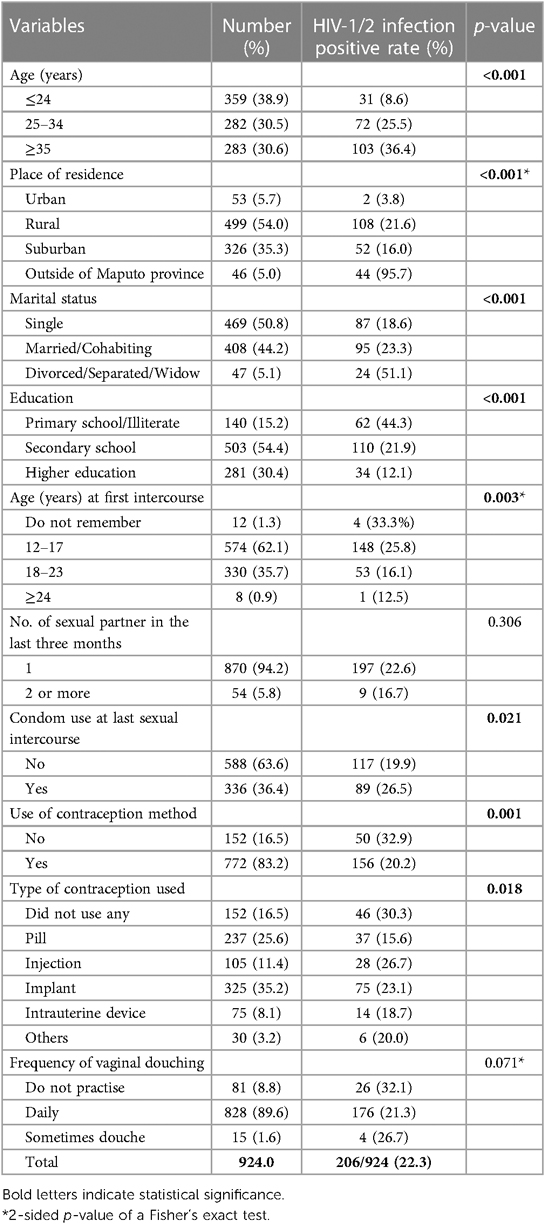
Table 1. Sociodemographic characteristics and prevalence of HIV-1/2 in sexually active women (n = 924) with urogenital complaints in Maputo, Mozambique.
A high proportion of participants presented with vaginal discharge syndromes (85.0%), followed by lower abdominal pain complaints (11.3%). Other common clinical conditions were cervical ectopia (17.4%) and a low percentage had genital warts (1.2%). The prevalence of HIV-1/2 infection was 22.3% (95% CI: 20%–25%).
Several sociodemographic and/or behavioural variables of the study participants showed a significant association with HIV-1/2 infection, Table 1. Regarding HIV-1/2 infection, the proportions of positivity were significantly higher among women aged ≥35 years than among younger groups (36.4% (103/283) vs. 8.6% (31/359) and 25.5% (72/282), respectively, p < 0.001); among those who lived outside Maputo province than among Maputo residents (95.7% (44/46) vs. urban 3.8% (2/53), rural 21.6% (108/499), and suburban 16.0% (52/326), respectively, p < 0.001); among the divorced/separated/widowed than among the single and married/cohabiting (51.1% (24/47) vs. 18.6% (87/469) and 23.3% (95/408), respectively, p < 0.001); among those with only primary school or being illiterate than those with secondary school or higher education (44.3% (62/140) vs. 21.9% (110/503) and 12.1% (34/281), respectively, p < 0.001); among women having their first intercourse at the age of 12–17 years compared to 18–23 years and ≥24 years (25.8% (148/574) vs. 16.1% (53/330) and 12.5% (1/8), respectively, p = 0.003); among those using condom at their last sexual intercourse (26.5% (89/336) vs. 19.9% (117/588), p = 0.021); and among women not using contraception (32.9% (50/152) vs. 20.2% (156/772), p = 0.001). Notably, after excluding the 46 women from outside of Maputo province (95.7% HIV positivity, which was likely because many were referred to Maputo for higher level of health care), most of the significant associations remained. However, HIV positivity was no longer associated with lower age (12–17 years) at the first intercourse (p = 0.15) or with not using contraception (p = 0.16). Furthermore, the HIV prevalence decreased from 22.3% (206/924) to 18.5% (162/878).
The prevalence of chlamydia, trichomoniasis, gonorrhoea and M. genitalium infections was 15.5% (95% CI: 13%–18%); 12.1% (95% CI: 10%–14%), 4.0% (95% CI: 3.0%–5.0%), and 2.1% (95% CI 1.0%–3.0%), respectively (Table 2). The proportion of concomitant non-viral STIs was as follows: chlamydia/gonorrhoea 1.5%, chlamydia/trichomoniasis 1.5%, chlamydia/M. genitalium 0.8%, gonorrhoea/trichomoniasis 0.9%, and trichomoniasis/M. genitalium 0.4%.
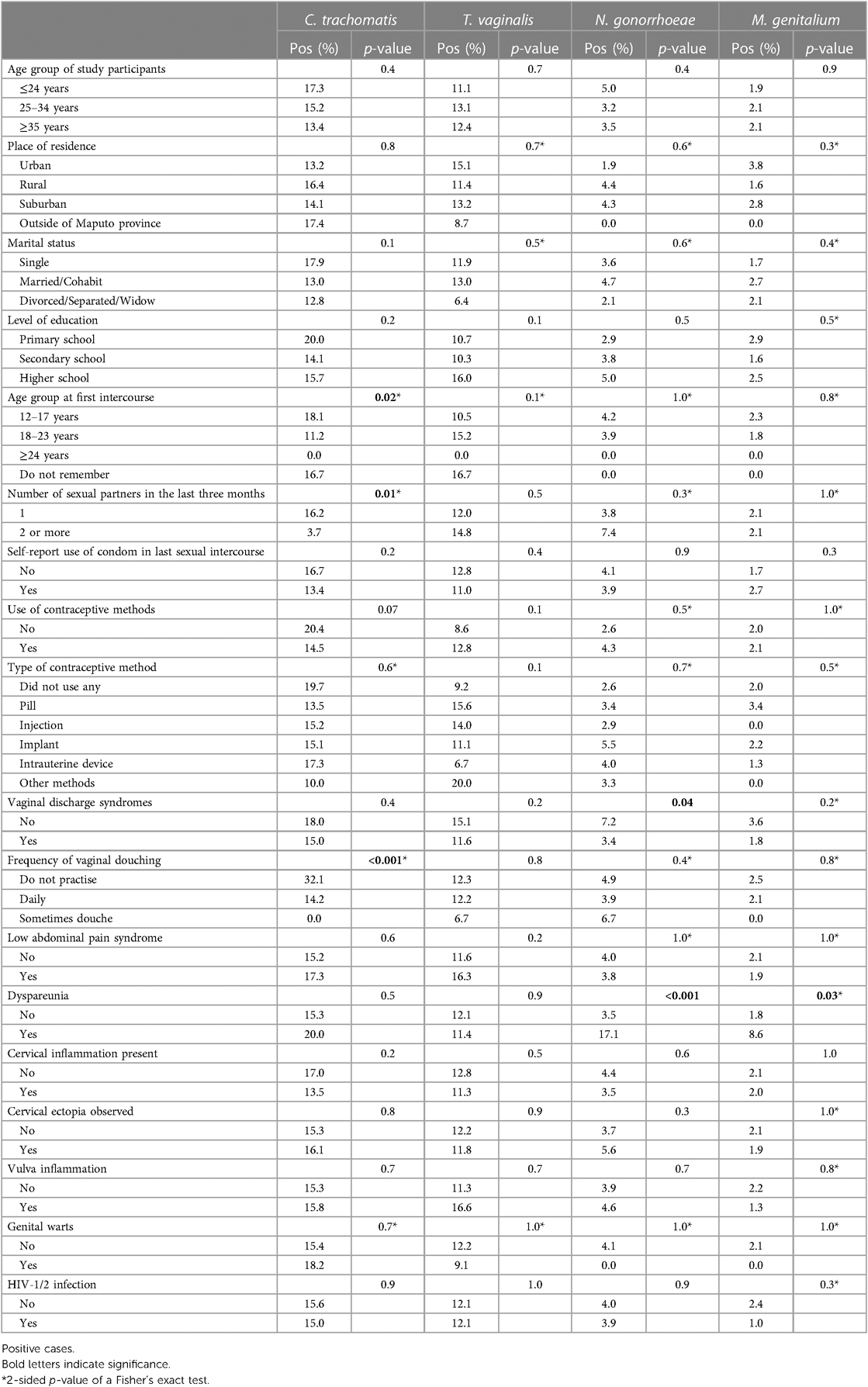
Table 2. Prevalence of STIs and bivariate tests of association between the etiological diagnosis of the four STIs, and sociodemographic, behavioural and clinical variables, among sexually active women with urogenital complaints in Maputo, Mozambique.
The proportions of C. trachomatis cases were significantly higher among women with early sexual debut (12–17 years, 18.1% (104/574) vs. 11.2% (37/330) and 0.0% (0/20), respectively, p = 0.02), in women who had a single sexual partner in the last three months (16.2% (141/870) vs. 3.7% (2/54), p = 0.01), and in women that did not practice vaginal douching daily (32.1% (26/81) vs. 14.2% (117/826), p < 0.001), Table 2. The proportions of gonorrhoea cases were significantly higher among women who did not have vaginal discharge syndrome (7.2% (10/139) vs. 3.4% (27/785), p = 0.04), and among those who reported dyspareunia (17.1% (6/35) vs. 3.5% (31/889), p < 0.001). Regarding M. genitalium infection, a higher proportion of positive cases was found only among women who reported dyspareunia (8.6% (3/35) vs. 1.8% (16/889), p = 0.03). Trichomoniasis was not significantly associated with any of the examined variables, Table 2. All these associations remained significant after excluding the 46 women from outside of Maputo province (95.7% HIV positivity, which was likely because many were referred to Maputo for higher level of health care).
Supplementary Table S1 summarizes the accuracy (sensitivity and specificity) of the vaginal discharge syndrome management compared with the etiological laboratory diagnosis of the four STIs.
Briefly, the syndromic approach based on vaginal symptoms or signs (Figure 1) had a sensitivity ranging from 73.0% to 82.5% and specificity of 14%–15% in the detection of women with urogenital chlamydia, trichomoniasis, gonorrhoea, or M. genitalium infection. The sensitivity and specificity of the vaginal syndromic approach to detect women with any of the three STIs chlamydia, trichomoniasis and gonorrhoea (which are treated in the vaginal discharge syndromic management) was 80.8% and 13.1%, respectively. Consequently, 19.2% of the women with any of these three STIs would not be detected and accordingly treated using the vaginal discharge syndromic management (missed treatment) and 70.0% of the women would be treated despite not infected with any of these three STIs (overtreatment). The sensitivity and specificity for detection of the different single STIs ranged from 73.0% to 82.5%, and from 14.5% to 14.8%, respectively (Supplementary Table S1).
We investigated the prevalence of STIs (chlamydia, gonorrhoea, trichomoniasis, M. genitalium and HIV-1/2) in women with urogenital complaints that attended for care at four different health facilities in Maputo province, Mozambique. A high prevalence of non-viral STIs, and HIV-1/2 infection was observed, with chlamydia being the most common non-viral STI, followed by trichomoniasis. Risk factors associated with STIs included younger age at first sexual intercourse, not using vaginal douching, absence of vaginal syndrome and dyspareunia. Older age of the women, living in non-urban ares, being divorced/separated/widowed, having low level of education, and condom use at last sexual intercourse were associated with HIV-1/2 positivity. Furthermore, we show that the syndromic management of vaginal discharge has a low accuracy in the detection of STIs in Mozambique, especially low specificity, which results in under-treatment of STI-positive cases and incorrect or over-treatment of women with urogenital complaints, many of whom are negative for all the non-viral STIs. Finally, the resistance to ciprofloxacin in N. gonorrhoeae is exceedingly high globally (33) and it is imperative that ciprofloxacin is replaced by, for example, ceftriaxone 500 mg in the syndromic management of vaginal discharge as well as in other syndromic management flowcharts used in Mozambique.
Comparing to some previous studies on symptomatic women in other sub-Saharan African countries, such as Zimbabwe (41), South Africa (42) as well as Kenya (31), the prevalence of chlamydia (15.5%) and trichomoniasis (12.1%) in the present study were similar. However, these prevalences were lower than those previously found in pregnant women in South Africa (43) and higher than that recorded in Senegal in symptomatic women (44). The prevalence of gonorrhoea, however, was consistent with that reported among pregnant women in Ethiopia (45), but lower than that among symptomatic women in Kenya (46), women of reproductive age in Swaziland (47), and young women in Zimbabwe and South Africa (48). However, the gonorrhoea prevalence was higher than those recorded, for example, among female students in Tanzania (49). High prevalences of the most common non-viral STIs (chlamydia, gonorrhoea, trichomoniasis and M. genitalium infection) were also found in studies including a mixed population in Botswana, Namibia, and South Africa (6). M. genitalium infection was less common in our study, which was inconsistent with results reported in Kenya among women with lower genital tract symptoms (46).
The proportions of non-viral STI co-infections were comparable to those reported in previous community-based randomised trials and cross-sectional studies, carried out in Guinea-Bissau (50), Ethiopia (45), Kenya (Maina et al., 2016), Australia (51) and Brazil (52), in which the prevalence of concomitant STIs infections in women were 0.6%–2.0% of chlamydia/gonorrhoea, 0.3%–2.8% of chlamydia/trichomoniasis, 0.2%–1.3% of chlamydia/M. genitalium and 0.2%–2.4% of gonorrhoea/trichomoniasis. These results suggest that the proportions of non-viral STI co-infections may vary but are in general low in this population. Results are also influenced by the diagnostic methods used and which population groups that have been studied. It is frequently higher in specific risk groups such as sex workers (53) and women living with HIV-1/2 (43, 54).
For non-viral STIs, we identified an association between chlamydial infection and sexual behaviour, with early age of sexual debut and/or number of sexual partners being risk factors for this infection. These findings were in agreement with previous studies (42, 55), which reported an increased risk of infection in women who initiated sexual activity under the age of 18 years. Discussing relations is an extremely private, sensitive issue and considered a taboo subject in very conservative contexts in Mozambique. Thus, the high prevalence of chlamydia infections in participants who reported having had only one sexual partner in the last three months may be attributed to a social desirability bias (42, 56, 57), however, we cannot exclude that some of these women were aware of their risk behaviour and more regularly used condoms to protect themselves during sexual intercourse. There were no significant differences in STI burden between women living with HIV-1/2 compared to other women, i.e., in contrast to the findings of previous studies in which STI prevalence was higher among African women living with HIV-1/2 (43, 54, 58–64). This may reveal different risk behaviours among populations in different countries that increase the risk of contracting HIV-1/2 and STIs. Previous studies (65–68) have stated that individuals over 20 years of age were more likely to test positive for HIV-1/2 than adolescents (15–19 years), which is consistent with our findings. In general, more adults engage in risky sexual behaviour, for many reasons, than adolescents, in addition to most likely having more sexual experiences in their longer life and a higher risk of being infected. Since sexual intercourse is the main route of HIV-1/2 transmission, the risk in adults is even greater (66). Furthermore, being divorced/separated/widowed, uneducated, or less educated was associated with higher HIV-1/2 prevalence, which is consistent with previous studies in Mozambique (66), and in other countries (69, 70). People with lower education are less likely to seek information about healthcare and therefore more likely to have poor health outcomes (71).
However, several sociodemographic factors, sexual behaviour and contraceptive use did not show any associations with the presence of single or concomitant non-viral STIs. This has been shown also in other studies in sub-Saharan Africa in different population groups, which concluded that age (31, 42, 72), place of residence (72), level of education (73), marital status (31), contraceptive use and lifetime partners (73) were not risk factors for a single or co-infections with non-viral STIs. Nevertheless, in populations living with HIV in the African region, multiple sexual partners (74–76), lack of condom use and low level of education (49, 77) have been highlighted as risk factors for viral as well as non-viral STIs. Correct condom use is known to be very effective in preventing the transmission of HIV-1/2 and other STIs (78, 79). We found a lower prevalence of women living with HIV-1/2 among women who reported not using a condom at last intercourse, which has also been described among women in South Africa (80). These results indicate that condom use during intercourse may not have been a consistent practice in their sexual relationships, and perhaps condom use, regular and irregular, indicates a higher sexual risk behaviour (more partners, more casual sex, sex work etc.) resulting in higher HIV-1/2 prevalence in this group. In addition, it has been reported that most women in sub-Saharan Africa are unable to negotiate with their sexual partners for the consistent use of male or female condoms (81). Understanding the cultural and social factors that determine sexual partnerships in Mozambique may be useful in identifying why women are more likely to be infected with HIV-1/2 and STIs.
Although vaginal discharge syndrome was the most common complaint of the participating symptomatic women, we found no significant positive association with any of the four non-viral STIs, which is in line with previous studies in the sub-Saharan region (42, 46), but inconsistent with previous findings from Ethiopia (45). Vaginal douching or cleansing with soap, water or other substances is a common practice among women in many Sub-Saharan African countries (82–84), including Mozambique. In the present study, there was no positive association between vaginal douching and any STIs/HIV. However, several other studies have shown that frequent vaginal douching can be a risk factor associated with STIs, including HIV-1/2 (83, 85–88). This may be because it causes changes in the normal vaginal flora or causes dryness or burning, disturbance and inflammation of the mucous membranes (89). The vaginal douching practice has also been shown to promote the spread of microorganisms to the upper genital tract (84, 90, 91).
In our study, the sensitivity of the vaginal discharge syndrome algorithm to detect the four diagnosed non-viral STIs was relatively high (reflecting the studied population of women with urogenital complaints), but the specificity was very low, resulting in high rates of overtreatment and incorrect treatment, as most women reporting vaginal syndromes did not require treatment because they did not have an STI and instead may have been suffering from bacterial vaginosis, Candida vaginitis, or similar. The inclusion of risk assessment in the syndromic management of vaginal discharge has been shown to decrease overtreatment in pregnant and non-pregnant women in Tanzania (92). This is because women with vaginal discharge would only receive treatment for chlamydia and gonococcal infection if the risk assessment is positive. In Mozambique, the diagnosis of non-viral STIs in women is based entirely on self-reported vaginal discharge syndromes and the women's physical examination when necessary. However, in most health facilities providing primary health care in Mozambique, physical examination with a genital speculum is not routinely performed due to lack of examination rooms and adequate equipment such as gynaecological beds, speculum, autoclaves, etc., in addition to limited and overstretched human resources.
Also in previous studies, the vaginal discharge syndrome approach has demonstrated low diagnostic accuracy, i.e., with sensitivity ranging between 14 and 92.9%, specificity varying between 2.4%–33% and PPV of 8%–38% (31, 72, 93) in diagnosing non-viral STIs in women with urogenital complaints. Indeed, several authors have reported the poor performance of vaginal discharge syndrome approaches in the diagnosis of non-viral STIs in different regions (11, 21, 22, 25, 27, 36, 94–97). The lack of detection of asymptomatic STIs (11, 22, 75, 98, 99), risk of selecting AMR due to the overtreatment, which is linked to the low specificity, strongly emphasize the need for etiological STI diagnosis in women with urogenital complaints as well as asymptomatic women that have been exposed to a risk of being infected by an STI.
Rapid point-of-care tests (POCTs) for HIV-1/2 and syphilis have already been successfully integrated into many antenatal screening programmes in several Sub-Saharan African countries aiming to eliminate mother-to-child transmission of HIV-1/2 and syphilis (100–105). While there are available adequate POCTs for the two non-viral STIs syphilis and trichomoniasis, there are currently no appropriate rapid, affordable, and effective POCTs for chlamydia, gonorrhoea, or M. genitalium infection (106, 107). Accordingly, rapid, affordable, and effective POCTs for all non-viral STIs are essential to develop for detection of these infections in symptomatic and asymptomatic males and females. Several such POCTs are in the pipeline, especially for chlamydia and gonorrhoea (106).
This was the first study to evaluate the accuracy of any of the syndromic management flowcharts for STIs in Mozambique, and previously evaluated, standardized and quality-assured techniques and assays for etiological diagnosis were used. However, the study also included some limitations. First, we used a cross-sectional study design and non-random convenience sampling, which may have introduced some biases in the measurement of certain variables. Second, the selection of participants with urogenital complaints and the exclusion of 75 women due to missing sociodemographic and behavioural data or appropriate samples may have introduced selection biases. Accordingly, a large study using population-based sampling and including both symptomatic and asymptomatic women with less women excluded would be ideal to provide more accurate STI prevalence figures and sensitivity and specificity of the vaginal discharge syndrome flowchart used in Mozambique. This study should also ideally include antimicrobial susceptibility testing for N. gonorrhoeae and M. genitalium, which would provide data to inform recommended treatment and such data are totally lacking in Mozambique. Furthermore, it is important to evaluate, compared to etiological diagnosis, the accuracy of also the other STI-related syndromic management flowcharts in Mozambique, i.e., urethral discharge, genital ulcer, lower abdominal pain or pelvic inflammatory disease, and neonatal conjunctivitis flowcharts. Finally, in the present study the data regarding sociodemographics, sexual behaviour and symptoms were self-reported and may potentially be prone to social desirability bias and recall bias.
In conclusion, we found a high prevalence of especially chlamydia, trichomoniasis, and HIV-1/2 in women with urogenital complaints in reproductive age, mostly single, with secondary schooling, and with sexual debut between 12 and 17 years old in Maputo, Mozambique. Syndromic management of vaginal discharge revealed low accuracy for diagnosis of non-viral STIs, especially low specificity, resulting in undertreatment of STI-positive cases and incorrect or overtreatment in STI-negative cases, since many women with vaginal discharge syndromes were negative for all tested non-viral STIs and likely suffered from other etiologies, for example, bacterial vaginosis. Our findings strongly emphasize the urgent need for enhanced etiological testing of non-viral STIs in less-resourced settings and, ideally, rapid, affordable, and accurate POCTs for diagnosis of non-viral STIs in both symptomatic and asymptomatic individuals. This etiological diagnosis needs to be linked to access to evidence-based appropriate treatment for all those infected, which would require the availability and accessibility of health services in communities that have free effective antimicrobials available. Furthermore, it is important to strengthen prevention strategies to reduce the prevalence of STIs/HIV in this setting. Prevention strategies should include improved sexual health education campaigns (and sexual health education in school), including STIs/HIV, and promoting condom use, with the participation of community health workers, health authorities and researchers. It is also imperative to reduce the stigma and discrimination related to STIs/HIV among women and young adults, as well as to ensure confidentiality and privacy to increase the uptake of sexual partner notification. Finally, introduction of regular and quality-assured antimicrobial susceptibility surveillance for especially N. gonorrhoeae, but ideally also M. genitalium, is important to provide evidence-based resistance data that can inform refinements of the treatment recommendations.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Mozambican National Bioethics Committee for Health (reference number 405/CNBS/2014). This approval has been renewed annually with the current renewal number ref 180/CNBS/23. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
AM: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. GS: Data curation, Formal Analysis, Investigation, Writing – original draft, Writing – review & editing. DK: Conceptualization, Data curation, Formal Analysis, Investigation, Writing – review & editing. DG: Data curation, Formal Analysis, Investigation, Methodology, Writing – review & editing. YT: Data curation, Formal Analysis, Methodology, Software, Writing – review & editing. OL: Data curation, Formal Analysis, Methodology, Software, Writing – review & editing. FM: Data curation, Formal Analysis, Investigation, Methodology, Writing – review & editing. AG: Investigation, Methodology, Writing – review & editing. JL: Investigation, Methodology, Writing – review & editing. AP: Data curation, Investigation, Writing – review & editing. JS: Conceptualization, Investigation, Methodology, Writing – review & editing. MU: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article.
The present study was supported by grants from the SIDA (Swedish International Development Cooperation Agency), EDCTP programs (European and Developing Countries Clinical Trials Partnership), Örebro County Council Research Committee, and the Foundation for Medical Research at Örebro University Hospital, Sweden.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frph.2024.1323926/full#supplementary-material
1. Unemo M, Bradshaw S, Hocking S, de Vries C, Francis C, Mabey D, et al. Sexually transmitted infections: challenges ahead. Lancet Infect Dis. (2017) 17:e235–79. doi: 10.1016/S1473-3099(17)30310-9
2. Rowley J, Vander Hoorn S, Korenromp E, Low N, Unemo M, Abu-Raddad LJ, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ. (2019) 97:548–62. doi: 10.2471/BLT.18.228486
3. World Health Organisation [WHO]. Global health sector strategy on sexually transmitted infections, 2022–2023. (2022a). Available online at: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/strategies/global-health-sector-strategies (accessed September 3, 2023).
4. World Health Organization [WHO]. Report on Global Sexually Transmitted Infection Surveillance. Geneva: WHO (2022b). Available online at: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis) (accessed September 3, 2023).
5. Torrone EA, Morrison CS, Chen PL, Kwok C, Francis SC, Hayes RJ, et al. Prevalence of sexually transmitted infections and bacterial vaginosis among women in sub-Saharan Africa: an individual participant data meta-analysis of 18 HIV prevention studies. PLoS Med. (2018) 15:e1002511. doi: 10.1371/journal.pmed.1002511
6. Jarolimova J, Platt LR, Curtis MR, Philpotts LL, Bekker LG, Morroni C, et al. Curable sexually transmitted infections among women with HIV in sub-Saharan Africa. AIDS. (2022) 36:697–709. doi: 10.1097/QAD.0000000000003163
7. Dadzie LK, Agbaglo E, Okyere J, Aboagye RG, Arthur-Holme F, Seidu AA, et al. Self-reported sexually transmitted infections among adolescent girls and young women in sub-Saharan Africa. Int Health. (2022) 14:545–53. doi: 10.1093/inthealth/ihab088
8. IMASIDA. Inquérito de Indicadores de Imunização, Malária e HIV/SIDA em Moçambique. Ministério da Saúde (MISAU), Instituto Nacional de Estatística (INE), e ICF. 2019. Relatório Suplementar Incorporado os Resultados de Biomarcadores de Antiretrovirais. Maputo, Moçambique. Rockville, Maryland, EUA: INS, INE, e ICF. (2015). Available online at: https://dhsprogram.com/pubs/pdf/AIS12/AIS12_SP.pdf (accessed September 3, 2023).
9. Dwyer-Lindgren L, Cork MA, Sligar A, Steuben KM, Wilson KF, Provost NR, et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature. (2019) 570:189–93. doi: 10.1038/s41586-019-1200-9
10. Newman L, Rowley J, Vander Hoorn S, Wijesooriya NS, Unemo M, Low N, et al. Global estimates of the prevalence and incidence of four curable sexually transmitted infections in 2012 based on systematic review and global reporting. PLoS One. (2015) 10:e0143304. doi: 10.1371/journal.pone.0143304
11. Wi TE, Ndowa FJ, Ferreyra C, Kelly-Cirino C, Taylor MM, Toskin I, et al. Diagnosing sexually transmitted infections in resource-constrained settings: challenges and ways forward. J Int AIDS Soc. (2019) 22:e25343. doi: 10.1002/jia2.25343
12. Martin K, Wenlock R, Roper T, Butler C, Vera JH. Facilitators and barriers to point-of-care testing for sexually transmitted infections in low- and middle-income countries: a scoping review. BMC Infect Dis. (2022) 22:561. doi: 10.1186/s12879-022-07534-9
13. World Health Organization [WHO] (2003). Guidelines for the Management of Sexually Transmitted Infections. Available online at: https://apps.who.int/iris/handle/10665/42782 (accessed September 3, 2023).
14. Bosu WK. Syndromic management of sexually transmitted diseases: is it rational or scientific? Trop Med Int Health. (1999) 4:114–9. doi: 10.1046/j.1365-3156.1999.00360.x
15. Gupta V, Sharma VK. Syndromic management of sexually transmitted infections: a critical appraisal and the road ahead. Natl Med J India. (2019) 32:147–52. doi: 10.4103/0970-258X.278691
16. World Health Organization [WHO]. Guidelines for the Management of Symptomatic Sexually Transmitted Infections. Geneva: World Health Organization (2021). Available online at: https://www.who.int/publications-detail-redirect/9789240024168 (accessed September 3, 2023).
17. Toskin I, Govender V, Blondeel K, Murtagh M, Unemo M, Zemouri C, et al. Call to action for health systems integration of point-of-care testing to mitigate the transmission and burden of sexually transmitted infections. Sex Transm Infect. (2020) 96:342–7. doi: 10.1136/sextrans-2019-054358
18. Boonstra E, Lindbaek M, Klouman E, Ngome E, Romøren M, Sundby J. Syndromic management of sexually transmitted diseases in Botswana’s primary health care: quality of care aspects. Trop Med Int Health. (2003) 8:604–14. doi: 10.1046/j.1365-3156.2003.01076.x
19. Msuya SE, Uriyo J, Stray-Pedersen B, Sam NE, Mbizvo EM. The effectiveness of a syndromic approach in managing vaginal infections among pregnant women in northern Tanzania. East Afr J Public Health. (2009) 6:263–7. PMID: 20803916
20. Wi T, Lahra MM, Ndowa F, Bala M, Dillon JR, Ramon-Pardo P, et al. Antimicrobial resistance in Neisseria gonorrhoeae: global surveillance and a call for international collaborative action. PLoS Med. (2017) 14:e1002344. doi: 10.1371/journal.pmed.1002344
21. Verwijs MC, Agaba SK, Sumanyi JC, Umulisa MM, Mwambarangwe L, Musengamana V, et al. Targeted point-of-care testing compared with syndromic management of urogenital infections in women (WISH): a cross-sectional screening and diagnostic accuracy study. Lancet Infect Dis. (2019) 19:658–69. doi: 10.1016/S1473-3099(18)30724-2
22. Chaponda EB, Bruce J, Michelo C, Chandramohan D, Chico RM. Assessment of syndromic management of curable sexually transmitted and reproductive tract infections among pregnant women: an observational cross-sectional study. BMC Pregnancy Childbirth. (2021) 21:98. doi: 10.1186/s12884-021-03573-3
23. Peters R, Klausner JD, de Vos L, Feucht UD, Medina-Marino A. Aetiological testing compared with syndromic management for sexually transmitted infections in HIV-infected pregnant women in South Africa: a non-randomised prospective cohort study. BJOG. (2021) 128:1335–42. doi: 10.1111/1471-0528.16617
24. Sharma M, Rewari BB, Aditama TY, Turlapati P, Dallabetta G, Steen R. Control of sexually transmitted infections and global elimination targets, South-East Asia Region. Bull World Health Organ. (2021) 99:304–11. doi: 10.2471/BLT.20.254003
25. Sonkar SC, Arora G, Wasnik K, Ali M, Mittal P, Saluja D. Improved management can be achieved by introducing additional parameters in the syndromic diagnosis of nonviral sexually transmitted infections at low-resource settings. AJOG Glob Rep. (2021) 2:100037. doi: 10.1016/j.xagr.2021.100037
26. Kopkin R, Grenvik JM, Chiweza C, Iwuh I, Wilkinson J. Syndromic treatment of STIs in low-income countries is inadequate: current threats and future directions. Clin Obstet Gynecol. (2022) 65:717–32. doi: 10.1097/GRF.0000000000000714
27. Yadav D, Singh S, Dhawan B, Sood S, Gupta S. Laboratory detection of bacterial pathogens and clinical and laboratory response of syndromic management in patients with cervical discharge: a retrospective study. Indian J Dermatol Venereol Leprol. (2023) 89:431–5. doi: 10.25259/IJDVL_506_2021
28. Ray K, Muralidhar S, Bala M, Kumari M, Salhan S, Gupta SM, et al. Comparative study of syndromic and etiological diagnosis of reproductive tract infections/sexually transmitted infections in women in Delhi. Int J Infect Dis. (2009) 13:e352–9. doi: 10.1016/j.ijid.2008.11.021
29. Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR. (2021) 70:1–187. doi: 10.15585/mmwr.rr7004a1
30. Wihlfahrt K, Günther V, Mendling W, Westermann A, Willer D, Gitas G, et al. Sexually transmitted diseases-an update and overview of current research. Diagnostics (Basel). (2023) 13:1656. doi: 10.3390/diagnostics13091656
31. Maina AN, Mureithi MW, Ndemi JK, Revathi G. Diagnostic accuracy of the syndromic management of four STIs among individuals seeking treatment at a health centre in Nairobi, Kenya: a cross-sectional study. Pan Afr Med J. (2021) 40:138. doi: 10.11604/pamj.2021.40.138.25166
32. Machalek DA, Tao Y, Shilling H, Jensen JS, Unemo M, Murray G, et al. Prevalence of mutations associated with resistance to macrolides and fluoroquinolones in Mycoplasma genitalium: a systematic review and meta-analysis. Lancet Infect Dis. (2020) 20:1302–14. doi: 10.1016/S1473-3099(20)30154-7
33. Unemo M, Lahra M, Escher M, Eremin S, Cole J, Galarza P, et al. WHO Global antimicrobial resistance surveillance for Neisseria gonorrhoeae 2017–18: a retrospective observational study. Lancet Microbe. (2021) 2:e627–36. doi: 10.1016/S2666-5247(21)00171-3
34. Tuddenham S, Hamill M, Ghanem G. Diagnosis and treatment of sexually transmitted infections: a review. JAMA. (2022) 327:61–172. doi: 10.1001/jama.2021.23487
35. Mayaud P, Mabey D. Approaches to the control of sexually transmitted infections in developing countries: old problems and modern challenges. Sex Transm Infect. (2004) 80:174–82. doi: 10.1136/sti.2002.004101
36. van Gemert C, Hellard M, Bradshaw CS, Fowkes FI, Agius PA, Stoove M, et al. Syndromic management of sexually transmissible infections in resource-poor settings: a systematic review with meta-analysis of the abnormal vaginal discharge flowchart for Neisseria gonorrhoea and Chlamydia trachomatis. Sex Health. (2018) 15:1–12. doi: 10.1071/SH17070
37. World Health Organization [WHO]. Global health sector strategy on Sexually Transmitted Infections, 2016–2021. (2016). Available online at: https://www.who.int/reproductivehealth/publications/rtis/ghss-stis/en/ (accessed September 3, 2023).
38. Rumyantseva T, Golparian D, Nilsson CS, Johansson E, Falk M, Fredlund H, et al. Evaluation of the new AmpliSens multiplex real-time PCR assay for simultaneous detection of Neisseria gonorrhoeae, Chlamydia trachomatis, Mycoplasma genitalium, and Trichomonas vaginalis. APMIS. (2015) 123:879–86. doi: 10.1111/apm.12430
39. INE. Instituto Nacional de Estatística, Moçambique. IV Recenseamento geral da população e habitação 2017. Resultados definitivos, Maputo, Moçambique. (2019). Available online at: http://mozdata.microdatahub.com/index.php/catalog/98 (accessed September 3, 2023).
40. INSIDA. Inquérito Nacional sobre o Impacto do HIV e SIDA em Moçambique. Ministério da Saúde (MISAU), Instituto Nacional de Saude (INS). Maputo, Moçambique. (2021). Available online at: https://ins.gov.mz/wp-content/uploads/2022/12/53059_14_INSIDA_Summary-sheet_POR.pdf (accessed September 3, 2023).
41. Chirenje ZM, Dhibi N, Handsfield HH, Gonese E, Tippett Barr B, Gwanzura L, et al. The etiology of vaginal discharge syndrome in Zimbabwe: results from the Zimbabwe STI etiology study. Sex Transm Dis. (2018) 45:422–8. doi: 10.1097/OLQ.0000000000000771
42. Kularatne R, Muller E, Maseko V, Dias BDC, Kufa T. Etiological surveillance of vaginal discharge syndrome in South Africa: 2019 to 2020. Sex Transm Dis. (2022) 49:565–70. doi: 10.1097/OLQ.0000000000001646
43. Joseph Davey DL, Nyemba DC, Gomba Y, Bekker LG, Taleghani S, DiTullio DJ, et al. Prevalence and correlates of sexually transmitted infections in pregnancy in HIV-infected and -uninfected women in Cape Town, South Africa. PLoS One. (2019) 14:e0218349. doi: 10.1371/journal.pone.0218349
44. Diadhiou M, Ba Diallo A, Barry MS, Alavo SC, Mall I, Gassama O, et al. Prevalence and risk factors of lower reproductive tract infections in symptomatic women in Dakar, Senegal. Infect Dis (Auckl). (2019) 12:1178633719851825. doi: 10.1177/1178633719851825
45. Zenebe MH, Mekonnen Z, Loha E, Padalko E. Prevalence, risk factors and association with delivery outcome of curable sexually transmitted infections among pregnant women in Southern Ethiopia. PLoS One. (2021) 16:e0248958. doi: 10.1371/journal.pone.0248958
46. Omosa-Manyonyi GS, de Kam M, Tostmann A, Masido MA, Nyagah N, Obimbo MM, et al. Evaluation and optimization of the syndromic management of female genital tract infections in Nairobi, Kenya. BMC Infect Dis. (2023) 23:547. doi: 10.1186/s12879-023-08442-2
47. Ginindza TG, Stefan CD, Tsoka-Gwegweni JM, Dlamini X, Jolly PE, Weiderpass E, et al. Prevalence and risk factors associated with sexually transmitted infections (STIs) among women of reproductive age in Swaziland. Infect Agent Cancer. (2017) 12:29. doi: 10.1186/s13027-017-0140-y
48. Delany-Moretlwe S, Mgodi N, Bekker LG, Baeten JM, Li C, Donnell D, et al. High prevalence and incidence of gonorrhoea and chlamydia in young women eligible for HIV pre-exposure prophylaxis in South Africa and Zimbabwe: results from the HPTN 082 trial. Sex Transm Infect. (2023) 99:433–9. doi: 10.1136/sextrans-2022-055696
49. Mcharo RD, Kisinda A, Njovu L, Mcharo M, Mbwilo F, Mihale G, et al. Prevalence of and risk factors associated with HIV, Herpes Simplex Virus-type 2, Chlamydia trachomatis and Neisseria gonorrhoeae infections among 18–24-year-old students attending Higher Learning Institutions in Mbeya-Tanzania. PLoS One. (2022) 17:e0266596. doi: 10.1371/journal.pone.0266596
50. Cowley G, Milne G, Teixeira da Silva E, Nakutum J, Rodrigues A, Vasileva H, et al. Prevalence of and risk factors for curable sexually transmitted infections on Bubaque Island, Guinea Bissau. Sex Transm Infect. (2019) 97:51–5. doi: 10.1136/sextrans-2019-054351
51. Guy R, Ward J, Wand H, Rumbold A, Garton L, Hengel B, et al. Coinfection with Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis: a cross-sectional analysis of positivity and risk factors in remote Australian Aboriginal communities. Sex Transm Infect. (2015) 91:201–6. doi: 10.1136/sextrans-2014-051535
52. Silveira MF, Bruni MP, Stauffert D, Golparian D, Unemo M. Prevalence and risk factors associated with Chlamydia trachomatis, Neisseria gonorrhoeae, and Mycoplasma genitalium among women in Pelotas, Southern Brazil. Int J STD AIDS. (2020) 31:432–9. doi: 10.1177/0956462419898982
53. Tovo SF, Zohoncon TM, Dabiré AM, Ilboudo R, Tiemtoré RY, Obiri-Yeboah D, et al. Molecular epidemiology of human papillomaviruses, Neisseria gonorrhoeae, Chlamydia trachomatis and Mycoplasma genitalium among female sex workers in Burkina Faso: prevalence, coinfections and drug resistance genes. Trop Med Infect Dis. (2021) 6:90. doi: 10.3390/tropicalmed6020090
54. Smullin CP, Green H, Peters R, Nyemba D, Qayiya Y, Myer L, et al. Prevalence and incidence of Mycoplasma genitalium in a cohort of HIV-infected and HIV-uninfected pregnant women in Cape Town, South Africa. Sex Transm Infect. (2020) 96:501–8. doi: 10.1136/sextrans-2019-054255
55. Wand H, Reddy T, Dassaye R, Moodley J, Naidoo S, Ramjee G. Estimating prevalence and incidence of sexually transmitted infections among South African women: implications of combined impacts of risk factors. Int J STD AIDS. (2020) 31:1093–101. doi: 10.1177/0956462420915388
56. Kelly CA, Soler-Hampejsek E, Mensch BS, Hewett PC. Social desirability bias in sexual behavior reporting: evidence from an interview mode experiment in rural Malawi. Int Perspect Sex Reprod Health. (2013) 39:14–21. doi: 10.1363/3901413
57. King BM. The influence of social desirability on sexual behavior surveys: a review. Arch Sex Behav. (2022) 51:1495–501. doi: 10.1007/s10508-021-02197-0
58. Venkatesh KK, van der Straten A, Mayer KH, Blanchard K, Ramjee G, Lurie MN, et al. African Women recently infected with HIV-1 and HSV-2 have increased risk of acquiring Neisseria gonorrhoeae and Chlamydia trachomatis in the methods for improving reproductive health in Africa trial. Sex Transm Dis. (2011) 38:562–70. doi: 10.1097/OLQ.0b013e31820a8c2c
59. Mavedzenge NS, Müller EE, Lewis DA, Chipato T, Morrison CS, Weiss HA. Mycoplasma genitalium is associated with increased genital HIV type 1 RNA in Zimbabwean women. J Infect Dis. (2015) 211:1388–98. doi: 10.1093/infdis/jiu644
60. Vandepitte J, Weiss HA, Bukenya J, Kyakuwa N, Muller E, Buvé A, et al. Association between Mycoplasma genitalium infection and HIV acquisition among female sex workers in Uganda: evidence from a nested case-control study. Sex Transm Infect. (2014) 90:545–9. doi: 10.1136/sextrans-2013-051467
61. Mudau M, Peters RP, De Vos L, Olivier DH, Davey D, Mkwanazi ES. High prevalence of asymptomatic sexually transmitted infections among human immunodeficiency virus-infected pregnant women in a low-income South African community. Int J STD AIDS. (2018) 29:324–33. doi: 10.1177/0956462417724908
62. Roxby AC, Yuhas K, Farquhar C, Bosire R, Mbori-Ngacha D, Richardson BA, et al. Mycoplasma genitalium infection among HIV-infected pregnant African women and implications for mother-to-child transmission of HIV. AIDS. (2019) 33:2211–7. doi: 10.1097/QAD.0000000000002335
63. Medina-Marino A, Mudau M, Kojima N, Peters RP, Feucht UD, Vos L, et al. Persistent Chlamydia trachomatis, Neisseria gonorrhoeae or Trichomonas vaginalis positivity after treatment among human immunodeficiency virus-infected pregnant women, South Africa. Int J STD AIDS. (2020) 31:294–302. doi: 10.1177/0956462419898612
64. Ngobese B, Swe-Han KS, Tinarwo P, Abbai NS. Significant associations between Chlamydia trachomatis and Neisseria gonorrhoeae infections in human immunodeficiency virus-infected pregnant women. Infect Dis Obstet Gynecol. (2022) 2022:7930567. doi: 10.1155/2022/7930567
65. Chernyshov PV. Risk factors for HIV transmission and HIV testing among medical students. Acta Dermatovenerol Croat. (2020) 28:2–8. PMID: 32650844
66. Nutor JJ, Duodu PA, Agbadi P, Duah HO, Oladimeji KE, Gondwe KW. Predictors of high HIV+ prevalence in Mozambique: a complex samples logistic regression modeling and spatial mapping approaches. PLoS One. (2020) 15:e0234034. doi: 10.1371/journal.pone.0234034
67. Marson K, Ndyabakira A, Kwarisiima D, Camlin CS, Kamya MR, Havlir D, et al. HIV Retesting and risk behaviors among high-risk, HIV-uninfected adults in Uganda. AIDS Care. (2021) 33:675–81. doi: 10.1080/09540121.2020.1842319
68. Muravha T, Hoffmann CJ, Botha C, Maruma W, Charalambous S, Chetty-Makkan CM. Exploring perceptions of low-risk behaviour and drivers to test for HIV among South African youth. PLoS One. (2021) 16:e0245542. doi: 10.1371/journal.pone.0245542
69. Rumbwere Dube BN, Marshall TP, Ryan RP, Omonijo M. Predictors of human immunodeficiency virus (HIV) infection in primary care among adults living in developed countries: a systematic review. Syst Rev. (2018) 7:82. doi: 10.1186/s13643-018-0744-3
70. Schwitters A, McCracken S, Frederix K, Tierney R, Koto M, Ahmed N, et al. High HIV prevalence and associated factors in Lesotho: results from a population-based survey. PLoS One. (2022) 17:e0271431. doi: 10.1371/journal.pone.0271431
71. Feinberg I, Frijters J, Johnson-Lawrence V, Greenberg D, Nightingale E, Moodie C. Examining associations between health information seeking behavior and adult education status in the U.S.: an analysis of the 2012 PIAAC data. PLoS One. (2016) 11:e0148751. doi: 10.1371/journal.pone.0148751
72. Kaida A, Dietrich JJ, Laher F, Beksinska M, Jaggernath M, Bardsley M, et al. A high burden of asymptomatic genital tract infections undermines the syndromic management approach among adolescents and young adults in South Africa: implications for HIV prevention efforts. BMC Infect Dis. (2018) 18:499. doi: 10.1186/s12879-018-3380-6
73. Menezes LJ, Pokharel U, Sudenga SL, Botha MH, Zeier M, Abrahamsen ME, et al. Patterns of prevalent HPV and STI co-infections and associated factors among HIV-negative young Western Cape, South African women: the EVRI trial. Sex Transm Infect. (2018) 94:55–61. doi: 10.1136/sextrans-2016-053046
74. Chemaitelly H, Weiss HA, Smolak A, Majed E, Abu-Raddad LJ. Epidemiology of Treponema pallidum, Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, and herpes simplex virus type 2 among female sex workers in the Middle East and north Africa: systematic review and meta-analytics. J Glob Health. (2019) 9:020408. doi: 10.7189/jogh.09.020408
75. Lowe S, Mudzviti T, Mandiriri A, Shamu T, Mudhokwani P, Chimbetete C, et al. Sexually transmitted infections, the silent partner in HIV-infected women in Zimbabwe. South Afr J HIV Med. (2019) 20:849. doi: 10.4102/sajhivmed.v20i1.849
76. Traeger MW, Cornelisse VJ, Asselin J, Price B, Roth NJ, Willcox J, et al. Association of HIV preexposure prophylaxis with incidence of sexually transmitted infections among individuals at high risk of HIV infection. JAMA. (2019) 321:1380–90. doi: 10.1001/jama.2019.2947
77. Armstrong-Mensah E, Ebiringa DP, Whitfield K, Coldiron J. Genital Chlamydia Trachomatis infection: prevalence, risk factors and adverse pregnancy and birth outcomes in children and women in sub-Saharan Africa. Int J MCH AIDS. (2021) 10:251–7. doi: 10.21106/ijma.523
78. Gallo MF, Steiner MJ, Warner L, Hylton-Kong T, Figueroa JP, Hobbs MM, et al. Self-reported condom use is associated with reduced risk of chlamydia, gonorrhea, and trichomoniasis. Sex Transm Dis. (2007) 34:829–33. doi: 10.1097/OLQ.0b013e318073bd71
79. CDC. Centers for Disease Control and Prevention. Condom Effectiveness. Condom fact sheet in brief. (2021). Available online at: https://www.cdc.gov/condomeffectiveness/brief.html (accessed August 29, 2023).
80. Mabaso M, Makola L, Naidoo I, Mlangeni LL, Jooste S, Simbayi L. HIV Prevalence in South Africa through gender and racial lenses: results from the 2012 population-based national household survey. Int J Equity Health. (2019) 18:167. doi: 10.1186/s12939-019-1055-6
81. Kharsany AB, Karim QA. HIV Infection and AIDS in sub-Saharan Africa: current status, challenges and opportunities. Open AIDS J. (2016) 10:34–48. doi: 10.2174/1874613601610010034
82. Fonck K, Kaul R, Keli F, Bwayo JJ, Ngugi EN, Moses S, et al. Sexually transmitted infections and vaginal douching in a population of female sex workers in Nairobi, Kenya. Sex Transm Infect. (2001) 77:271–5. doi: 10.1136/sti.77.4.271
83. Ness RB, Hillier SL, Kip KE, Richter HE, Soper DE, Stamm CA, et al. Douching, pelvic inflammatory disease, and incident gonococcal and chlamydial genital infection in a cohort of high-risk women. Am J Epidemiol. (2005) 161:186–95. doi: 10.1093/aje/kwi025
84. Nsereko E, Moreland PJ, Dunlop AL, Nzayirambaho M, Corwin EJ. Consideration of cultural practices when characterizing the vaginal microbiota among African and African American women. Biol Res Nurs. (2021) 23:91–9. doi: 10.1177/1099800420940788
85. Joesoef MR, Sumampouw H, Linnan M, Schmid S, Idajadi A, St Louis ME. Douching and sexually transmitted diseases in pregnant women in Surabaya, Indonesia. Am J Obstet Gynecol. (1996) 174:115–9. doi: 10.1016/s0002-9378(96)70382-4
86. Scholes D, Stergachis A, Ichikawa LE, Heidrich FE, Holmes KK, Stamm WE. Vaginal douching as a risk factor for cervical Chlamydia trachomatis infection. Obstet Gynecol. (1998) 91:993–7. doi: 10.1016/s0029-7844(98)00095-7
87. La Ruche G, Messou N, Ali-Napo L, Noba V, Faye-Ketté H, Combe P, et al. Vaginal douching: association with lower genital tract infections in African pregnant women. Sex Transm Dis. (1999) 26:191–6. doi: 10.1097/00007435-199904000-00001
88. Tsai S, Shepherd E, Vermund H. Does douching increase risk for sexually transmitted infections? A prospective study in high-risk adolescents. Am J Obstet Gynecol. (2009) 200(38):e1–8. doi: 10.1016/j.ajog.2008.06.026
89. Hesham H, Mitchell AJ, Bergerat A, Hung K, Mitchell CM. Impact of vaginal douching products on vaginal Lactobacillus, Escherichia coli and epithelial immune responses. Sci Rep. (2021) 11:23069. doi: 10.1038/s41598-021-02426-5
90. Brown JM, Poirot E, Hess KL, Brown S, Vertucci M, Hezareh M. Motivations for intravaginal product use among a cohort of women in Los Angeles. PLoS One. (2016) 11:e0151378. doi: 10.1371/journal.pone.0151378
91. Yıldırım R, Vural G, Koçoğlu E. Effect of vaginal douching on vaginal flora and genital infection. J Turk Ger Gynecol Assoc. (2020) 21:29–34. doi: 10.4274/jtgga.galenos.2019.2018.0133
92. Mayaud P, ka-Gina G, Cornelissen J, Todd J, Kaatano G, West B, et al. Validation of a WHO algorithm with risk assessment for the clinical management of vaginal discharge in Mwanza, Tanzania. Sex Transm Infect. (1998) 74:S77–84. PMID: 10023356
93. Vallely M, Toliman P, Ryan C, Rai G, Wapling J, Gabuzzi J, et al. Performance of syndromic management for the detection and treatment of genital Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis among women attending antenatal, well woman and sexual health clinics in Papua New Guinea: a cross-sectional study. BMJ Open. (2017) 7:e018630. doi: 10.1136/bmjopen-2017-018630
94. Pettifor A, Walsh J, Wilkins V, Raghunathan P. How effective is syndromic management of STDs? A review of current studies. Sex Transm Dis. (2000) 27:371–85. doi: 10.1097/00007435-200008000-00002
95. Zemouri C, Wi TE, Kiarie J, Seuc A, Mogasale V, Latif A, et al. The performance of the vaginal discharge syndromic management in treating vaginal and cervical infection: a systematic review and meta-analysis. PLoS One. (2016) 11:e0163365. doi: 10.1371/journal.pone.0163365
96. Sonkar SC, Wasnik K, Kumar A, Sharma V, Mittal P, Mishra PK, et al. Evaluating the utility of syndromic case management for three sexually transmitted infections in women visiting hospitals in Delhi, India. Sci Rep. (2017) 7:1465. doi: 10.1038/s41598-017-01422-y
97. Barry MS, Ba Diallo A, Diadhiou M, Mall I, Gassama O, Ndiaye Guèye MD, et al. Accuracy of syndromic management in targeting vaginal and cervical infections among symptomatic women of reproductive age attending primary care clinics in Dakar, Senegal. Trop Med Int Health. (2018) 23:541–8. doi: 10.1111/tmi.13046
98. Teasdale CA, Abrams EJ, Chiasson MA, Justman J, Blanchard K, Jones HE. Incidence of sexually transmitted infections during pregnancy. PLoS One. (2018) 13:e0197696. doi: 10.1371/journal.pone.0197696
99. Connolly S, Wall KM, Parker R, Kilembe W, Inambao M, Visoiu AM, et al. Sociodemographic factors and STIs associated with Chlamydia trachomatis and Neisseria gonorrhoeae infections in Zambian female sex workers and single mothers. Int J STdD AIDS. (2020) 31:364–74. doi: 10.1177/0956462419894453
100. Swartzendruber A, Steiner RJ, Adler MR, Kamb ML, Newman LM. Introduction of rapid syphilis testing in antenatal care: a systematic review of the impact on HIV and syphilis testing uptake and coverage. Int J Gynaecol Obstet. (2015) 130:S15–21. doi: 10.1016/j.ijgo.2015.04.008
101. Fonjungo PN, Boeras DI, Zeh C, Alexander H, Parekh BS, Nkengasong JN. Access and quality of HIV-related point-of-care diagnostic testing in global health programs. Clin Infect Dis. (2007) 62:369–74. doi: 10.1093/cid/civ866
102. Mashamba-Thompson TP, Morgan RL, Sartorius B, Dennis B, Drain PK, Thabane L. Effect of point-of-care diagnostics on maternal outcomes in human immunodeficiency virus-infected women: systematic review and meta-analysis. Point Care. (2017) 16:67–77. doi: 10.1097/POC.0000000000000135
103. Kuupiel D, Bawontuo V, Mashamba-Thompson TP. Improving the accessibility and efficiency of point-of-care diagnostics services in low- and middle-income countries: lean and agile supply chain management. Diagnostics (Basel). (2017) 7:58. doi: 10.3390/diagnostics7040058
104. Marks M, Mabey DC. The introduction of syphilis point of care tests in resource limited settings. Expert Rev Mol Diagn. (2017) 17:321–5. doi: 10.1080/14737159.2017.1303379
105. Manoto SL, Lugongolo M, Govender U, Mthunzi-Kufa P. Point of care diagnostics for HIV in resource limited settings: an overview. Medicina (Kaunas). (2018) 54:3. doi: 10.3390/medicina54010003
106. Murtagh M. Point-of-Care Diagnostic Tests (POCTs) for Sexually Transmitted Infections (STIs) WHO. World Health Organization. (2019). Available online at: http://www.who.int/reproductivehealth/topics/rtis/pocts/en (accessed September 3, 2023).
Keywords: prevalence, sexually transmitted infections, syndromic management, vaginal discharge, Mozambique
Citation: Manjate A, Sergon G, Kenga D, Golparian D, Tyulenev Y, Loquilha O, Mausse F, Guschin A, Langa JC, Passanduca A, Sacarlal J and Unemo M (2024) Prevalence of sexually transmitted infections (STIs), associations with sociodemographic and behavioural factors, and assessment of the syndromic management of vaginal discharge in women with urogenital complaints in Mozambique. Front. Reprod. Health 6:1323926. doi: 10.3389/frph.2024.1323926
Received: 23 October 2023; Accepted: 4 April 2024;
Published: 18 April 2024.
Edited by:
Marissa L. Becker, University of Manitoba, CanadaReviewed by:
Lyle McKinnon, University of Manitoba, Canada© 2024 Manjate, Sergon, Kenga, Golparian, Tyulenev, Loquilha, Mausse, Guschin, Langa, Passanduca, Sacarlal and Unemo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Magnus Unemo bWFnbnVzLnVuZW1vQHJlZ2lvbm9yZWJyb2xhbi5zZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.