
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Reprod. Health, 27 October 2023
Sec. HIV and STIs
Volume 5 - 2023 | https://doi.org/10.3389/frph.2023.1253384
This article is part of the Research TopicImproving the Delivery of Pre-exposure Prophylaxis (PrEP) to Eliminate Vertical HIV TransmissionView all 14 articles
 Philisiwe Ntombenhle Khumalo1*
Philisiwe Ntombenhle Khumalo1* Siphiwesihle Sibonisiwe Mkhonta1
Siphiwesihle Sibonisiwe Mkhonta1 Kikanda Kindandi1
Kikanda Kindandi1 Sindy Matse2Phinda Brian Dlamini1
Sindy Matse2Phinda Brian Dlamini1 Vincent Tukei1Rhoderick Machekano3Godfrey Woelk3
Vincent Tukei1Rhoderick Machekano3Godfrey Woelk3
Introduction: In Eswatini, HIV incidence among women of childbearing age is 1.45%. Eswatini introduced oral pre-exposure prophylaxis (PrEP) for HIV prevention in 2016 and requires that all HIV-negative pregnant and post-natal women (PPW) visiting health care facilities be offered PrEP.
Methods: Between September-November 2021, we conducted a survey among HIV-negative PPW from 16 purposively selected healthcare facilities in the Hhohho and Shiselweni regions in Eswatini. We interviewed consenting HIV-negative PPW using a structured questionnaire to collect data on PrEP knowledge, attitudes, intentions, and practices, as well as information on partner HIV status and stigma. Multivariate logistic regression was used to determine predictors of PrEP use and intention, adjusted for significant covariates.
Results: Of 1,484 PPW women approached, 1,149 consented and were interviewed, of whom 704 (61.3%) were post-partum and 445 (38.7%) pregnant. The median age was 25 years [Interquartile Range (IQR) = 21–30 years], with 533 (46.4%) 18–24 years old. Among the 1,149 women, 930 (80.7%) had ever heard about PrEP; 635 (55.3%) had knowledge about PrEP; 183 (15.9%) were currently using PrEP; and 285 (24.8%) had ever used PrEP. Increased odds of PrEP use were associated having HIV-positive male partner (aOR:7.76, 95%CI 3.53- 17.04); positive attitudes to PrEP (aOR:1.56, 95%CI: 1.02–2.40); and high self-efficacy (aOR:1.49, 95%CI:1.13–1.98). Among 864 women who never used PrEP, 569 (65.3%) intended to use PrEP in the future. Odds of intention to use PrEP were higher among women with low levels of education (aOR:2.23, 95% CI: 1.32–3.77); who ever heard about PrEP (aOR:1.69, 95%CI: 1.12–2.56); and had high self-efficacy (aOR:1.57, 95%CI: 1.31–1.87). Regarding stigma, among all women, 759 (66%) either agreed or strongly agreed that people would think they have HIV if they were to use PrEP; 658 (57.3%) reported they would be labelled as having multiple sex partners; 468 (40.7%) reported that their partner would think they are having risky sex with other people. Of 102 women who had discontinued PrEP, a majority stopped due to side effects 32 (35.2%).
Conclusion: Only about 50% of women had knowledge of PrEP, and PrEP uptake among PPW was low, though intention to use appeared high. More efforts to reduce stigma and promote PrEP use, including adequate information on side effects, are needed.
In 2016, the World Health Organization (WHO) strongly recommended offering oral pre-exposure prophylaxis (PrEP) containing tenofovir disoproxil fumarate (TDF) and emtricitabine (FTC), as an additional prevention choice for people at substantial risk of HIV infection as part of combination HIV prevention (1). Oral PrEP reduces the risk of HIV acquisition if used correctly as part of a combination prevention strategy. Several controlled trials have provided rigorous evidence that oral daily PrEP is protective against HIV infection among heterosexual sero-discordant couples (2, 3); women (4); men who have sex with men (MSM) (5); and injecting drug users (6). Evidence also shows that PrEP is safe to use by pregnant or lactating women (7–10). However, there are few surveys on knowledge and use of PrEP for HIV among pregnant and lactating women (11), and most of them have been conducted in South Africa. Data from the existing surveys showed low levels of awareness and knowledge about PrEP among pregnant and lactating women (12–14).
Eswatini has an HIV prevalence of 24.8% among adults 15 years and older, with a prevalence of 30.4% among women overall (15), and 35.4% among pregnant women aged 15–49 years (16). This is much higher than the prevalence among similarly-aged men of 18.7% (15). The annual HIV incidence rate among adults 15–49 years is 0.77% (0.20% among males and 1.45% among females) (15). With the high HIV prevalence and incidence rates, pregnant and post-natal women (PPW) in Eswatini are at substantial risk of HIV infection (11). Women who get infected with HIV during pregnancy or breastfeeding risk transmitting HIV to their infants (11). In 2019, the Eswatini Ministry of Health scaled-up the provision of PrEP as part of combination HIV prevention, with a particular focus on HIV-negative PPW, adolescent girls and young women (AGYW) aged 16–24 years, men aged 30–34 years, HIV-negative partners in sero-discordant sexual relationships, clients with sexually transmitted infections (STIs), and key populations (sex workers, men who have sex with men and transgender clients) (11). In Eswatini, clients are eligible for PrEP if at substantial risk after an assessment; age is 16 years and above; HIV test is negative on the day of PrEP initiation; there is no presence of symptoms indicating acute HIV infection (AHI) in combination with an exposure for HIV in the previous 14 days; willing to attended PrEP visits until 28 days after risk period; no contraindication to TDF + lamivudine (3TC); and bodyweight is 30 kilograms (kg) and above. PPW women are considered to be at substantial risk for HIV infection and are offered PrEP upon testing HIV-negative and having no contraindications for PrEP.
In Eswatini there is paucity of data on facilitators and barriers among PPW. Understanding the levels of knowledge, intention, use and potential gaps related to PrEP among PPW could help to identify opportunities for education and program implementation. The information could also be used to monitor the impact of social behavior change activities aiming to improve knowledge, attitudes and practices related to PrEP in antenatal and postpartum women. This study aimed to determine oral PrEP related levels of knowledge, attitudes, intention and practices PPW in Eswatini, and also to determine factors associated with use and intention to use PrEP among PPW.
We conducted a cross-sectional survey among HIV- negative PPW between September 2021 and November 2021. All HIV-negative women receiving antenatal care (ANC) and postnatal care (PNC) services in the study sites were invited to participate in the study. Individual interviews were conducted using a structured questionnaire covering topics on socio-demographic characteristics, HIV risk behaviors, PrEP knowledge, PrEP access and sources of information, PrEP experiences (e.g., adherence, discontinuity, and side effects), intention to use PrEP and PrEP stigma. Only women who provided written informed consent were interviewed.
The study was conducted in 16 purposively selected PEPFAR-supported health facilities and regions (Hhohho and Shiselweni) in Eswatini which were offering oral PrEP to PPW. By November 2020 there were 55 health facilities providing PrEP to PPW in Hhohho and Shiselweni regions, of which 34 were in Hhohho and 21 were Shiselweni region. Among the health facilities, six were public health units (PHUs) and 49 were clinics. Public health units provide primary healthcare services and are the basis for outreach services in Eswatini while clinics only provide primary healthcare services. Since there was a small number of PHUs, all six PHUs were included in the study and five clinics were randomly selected from each region using a random number generator in Microsoft Excel. Nine sites were selected from Hhohho region and seven sites were from Shiselweni region. The study sites comprised of four sites located in urban areas and 12 sites located in rural areas.
The sample size calculation aimed to provide a sufficient sample size to estimate the proportion of PPW with knowledge about PrEP with ±3% precision (half width of 95% Wilson confidence intervals) or better. Since the proportion of PPW with knowledge about PrEP in Eswatini was unknown, the sample size calculation assumed that 50% PPW would have knowledge about PrEP. In addition, the sample size had to be large enough to allow a detection of significant differences of at least 10% with 80% power in knowledge and attitudes between current PrEP users and non-users, and also large enough to perform multivariate analysis to determine factors associated with PrEP use and intention to use PrEP. A sample size of at least 1,064 was required to be able to meet the study objectives. We also factored in 10% refusal and non-response rate. Probability proportional to size was used to select the number of PPW to be interviewed from each site.
The study population comprised of HIV-negative PPW seeking antenatal and post-natal care in the study sites. Women were eligible to participate in the study if they were accessing antenatal or post-natal services at the sites; were 18 years or older; were pregnant or reported to have delivered within 24 months; had a documented HIV-negative status; willing to provide consent to participate, and able to read and/or speak one of the study languages of English and SiSwati. Women were excluded if they had an illness that could prevent their participation, which included display of pain, inability to focus on the conversation or to talk or to sit throughout the interview.
Women were recruited within Maternal Child and Neonatal Health (MNCH) departments in the study sites with the support of healthcare workers (HCWs) who worked in the study sites. The HCWs informed potential study participants about the study after providing them with the required clinical services for the day. Interested women were referred to trained research assistants (RAs) who were stationed in the study sites. After obtaining written informed consent, RAs interviewed the women in a quiet space using a structured questionnaire designed in EpiInfo 7, entering the responses directly into the database on Wi-Fi enabled tablets. The questionnaire had built-in controls and checks to assure data accuracy and quality.
A questionnaire was developed specifically for the study by adapting already validated questions from similar Knowledge, Attitude and Practices (KAP) surveys in multiple populations (12, 14, 17, 18). Adaptation included removing or rephrasing words and statements which did not apply to the study population. The interviewer-administered questionnaire collected data on socio-demographic characteristics, HIV risk behaviors, PrEP awareness and knowledge, PrEP access and sources of information, PrEP experiences (e.g., adherence, discontinuity, side effects), PrEP attitudes, PrEP motivation, PrEP self-efficacy, PrEP willingness, PrEP potential uptake (intention), and PrEP stigma. The questionnaire was translated from English to SiSwati, and participants had the interview in English or SiSwati depending on their preference.
Socio-demographic characteristics and sexual behavior questions were adapted from a PrEP demonstration survey conducted in Nigeria (17) and from a survey of knowledge and PrEP use among pregnant and breastfeeding women (PBFW) in South Africa (12). Socio-demographic variables included age, level of education, marital status, employment status, health related decision making and characteristics of male partners such as their age, HIV status, and employment. Sexual behavioral variables included number of sexual encounters, number of sexual partners, condom use, use of post exposure prophylaxis (PEP) for HIV, and testing and treatment for sexually transmitted illnesses (STIs).
Questions about PrEP awareness, sources of information and places to access PrEP were adapted from the survey of knowledge and PrEP use among PBFW in South Africa (12). Participants were asked if they have ever heard about PrEP, and where they have heard about PrEP. They were also asked where they would like to get information about PrEP and access PrEP pills in the future.
The questions about PrEP experience were adapted from the PrEP demonstration survey in Nigeria, the Durbar Mahila Samanwaya Committee (DMSC) case study and the Ashodaya Samithi Demo and Feasibility Project, and from the AIDS Clinical Trials Group (ACTG) Adherence Baseline Questionnaire (17). Participants were asked to self-report on the use of PrEP, experience of side effects, adherence to PrEP medication, PrEP disclosure and reasons for discontinuing PrEP for those who had discontinued PrEP.
For the study PrEP users were defined as women who were using PrEP at the time of the survey and PrEP non users were women who had never used PrEP and those who had previously used PrEP but had stopped taking PrEP at the time of the survey. Two questions were used to determine use of PrEP (1) Have you ever taken PrEP pills and (2) Are you currently taking PrEP pills. The response options were “Yes”, “No” and “Do not remember/ Refused to answer”. Only respondents who answered “Yes” were considered to have ever used or were currently using PrEP.
Knowledge about PrEP: was measured using four items as follows: (1) Consistent use of PrEP reduces HIV risk among HIV-negative individuals, (2) People using PrEP are recommended to continue using condoms, (3) Inconsistent use of PrEP decreases its effectiveness and (4) PrEP does not help prevent other STIs. The items were adapted from a survey of PrEP functional knowledge among MSM conducted in 2018 and were validated as part of scale on “Functional Knowledge of HIV Prevention Strategies” in the survey “Prioritizing U, 2015” (18). The response options were “True”, “False”, and “Do not know”. If a respondent answered “True” to ALL of the four items, then they were considered to have knowledge about PrEP otherwise considered not having knowledge about PrEP.
Before introducing respondents to PrEP scales, a summary of the meaning of PrEP was orally presented as follows. “There is a new way to prevent HIV infection for people who may be exposed to the virus. It is called Pre-Exposure Prophylaxis or PrEP. It involves an HIV-negative person taking a pill daily, on an ongoing basis (starting before an exposure and continuing after for as long as the person is at risk) to reduce their risk of HIV infection. Research suggests that PrEP is generally safe and is highly effective (over 90%) in preventing HIV infection if taken every day. It is much less effective if not taken every day and does not protect against other sexually transmitted infections. Taking PrEP would require a visit to a doctor every three months in order to be tested for HIV, STIs and side effects (19).”
PrEP Attitudes: was measured using a 5-items scale which sought to assess the participant's beliefs around PrEP's safety and effectiveness at preventing HIV (Supplementary Table S1). The items were taken from the article on applying the Information-Motivation-Behavioral Skills Model to understand PrEP intentions and use among MSM (20).The response options were 1 = Strongly disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly agree. The scale was constructed by summing the item scores and dividing by the number of items. The scale score range was 1–5, and a higher scale score indicated a higher level of positive PrEP attitudes. Using Factor Analysis, the scale was reliable to measure attitudes towards PrEP with Cronbach's Alpha (α) = 0.7.
PrEP Self-efficacy: was measured using a 5-items scale (α = 0.8) which sought to assess the participant's perceived ability to take PrEP consistently and as required (19) (Supplementary Table S1). The response options were: 1 = Not at all confident, 2 = Slightly confident, 3 = Somewhat confident, 4 = Fairly confident, 5 = Completely confident. The scale was constructed by summing the item scores and dividing by the number of items. The scale score range was 1–5, and a higher scale score indicated a higher level of self-efficacy (belief in self to use PrEP correctly).
PrEP Motivation: was measured using a 6-items scale (α = 0.6) which sought to assess circumstances under which participants would take or not take PrEP (19). These included assessing if clients would want to take PrEP if they knew about PrEP side effects, if they had to disclose to their sexual partners about taking PrEP, if they knew someone taking PrEP, if they had social support and if they trusted the efficacy of PrEP to prevent HIV transmission (Supplementary Table S1). The response options were: 1 = Strongly disagree, 2 = Disagree, 3 = Neutral, 4 = Agree, 5 = Strongly agree. The scale was constructed by summing the item scores and dividing by the number of items. The scale score range was 1–5, and a higher scale score indicated a higher level of motivation to use PrEP.
PrEP Stigma: was measured using a 13-items scale (α = 0.8) which covered fear of being perceived as promiscuous and fear of being shunned or rejected within social circles (Supplementary Table S1). The items were adapted from “The Pre-Exposure Prophylaxis (PrEP) Stigma Scale” (14, 21). The response options were: 1 = Strongly agree, 2 = Agree, 3 = Neutral, 4 = Disagree and 5 = Strongly Disagree. The scale was constructed by summing the item scores and dividing by the number of items. The scale score range was 1–5, a lower score indicated a higher level of stigma about PrEP.
PrEP Intention: was measured using three items as follows: (1) During the next three months, I will talk to a health care provider about PrEP; (2) During the next three months, I will seek out more information about PrEP and (3) During the next three months, I will get a prescription for PrEP (20). The response options were: 1 = No, definitely not; 2 = No, probably not; 3 = Yes, probably; 4 = Yes, definitely. A women was considered to have intention to use PrEP if they responded with either option “3 = Yes, probably” or option “4 = Yes, definitely” across all the three statements.
PrEP Willingness: was measured using a 6-items scale (α = 0.8) adapted from a study on willingness to take PrEP for HIV prevention among Thai MSM (22) (Supplementary Table S1). The items assessed participants' willingness to take PrEP if available, even if they would still have to use condoms, if it could cause temporary mild side effects, if they had to pay for it and if they would still need to test regularly for HIV. The response options were: 1 = No, definitely not; 2 = No, probably not; 3 = Yes, probably; 4 = Yes, definitely. The scale was constructed by summing the item scores and dividing by the number of items. The scale score range was 1–4, a higher score indicated a higher level of willingness to use PrEP.
Data analysis was performed using the Statistical Package for Social Sciences (SPSS) version 26.0. Categorical variables were summarized using frequencies and percentages of participants. Continuous variables were summarized using means and standard deviations or medians and interquartile ranges, as appropriate. Factor analysis was used to confirm reliability among the scale items. Scales were considered reliable if the Cronbach's alpha was 0.5 and above. Pearson's chi-squared test was used to measure the association among categorical variables, and a rank-sum test was used to measure association between continuous variables. The precision around PrEP awareness, knowledge, use and intention estimates was assessed by 95% confidence intervals. Additionally, we used multivariate logistic regression to identify predictors of PrEP use and intention to use PrEP. Odds ratios and their respective 95% confidence intervals were used to quantify the effects. Variables for the multivariate model, were initially compiled informed by background knowledge, and these included region, age, education, marital status, decision making about health-related issues, HIV testing, male partner's characteristics, sexual risk behavior, self-efficacy, social support, perceived benefits and barriers of PrEP and stigma association with taking PrEP (14, 23–25). The potential factors were subsequently screened using simple (i.e., univariate) logistic regression and included in the multivariate model if the association with the respective dependent variable had a p-value of 0.05 or lower. Missing cases were excluded in a listwise fashion.
The protocol was implemented with human subject oversight provided by the Eswatini Health and Human Research Review Board (EHHRRB) (IRB: 00011253) in Eswatini, and the Advarra IRB (IORG0000468) in the United States of America. In addition, administrative approvals were obtained from the Eswatini National AIDS Program; Regional Health Management Teams, and senior management teams at the study sites. No monetary incentives were provided to the women for being part of this study. To enhance confidentiality, study participants were assigned unique study identification numbers to identify and link study records.
A total of 1,484 PPW were referred to the Research Assistants by Healthcare Workers (HCWs) in study sites, and 252 (17.0%) were not eligible to participate in the study, 1,157 (78.0%) consented to participate in the study and 75 (5.0%) did not consent. Of the 75 women who did not consent to participate, 23 (30.7%) refused (did not want/ not interested/not comfortable), 46 (61.3%) did not have enough time to sit through the interview/in a hurry to leave health facility, 6 (8.0%) had their children crying endlessly. Among the 1,157 PPW who consented to participate in study, 1,149 completed the interview. Figure 1 presents the flow of study participant screening and enrollment.
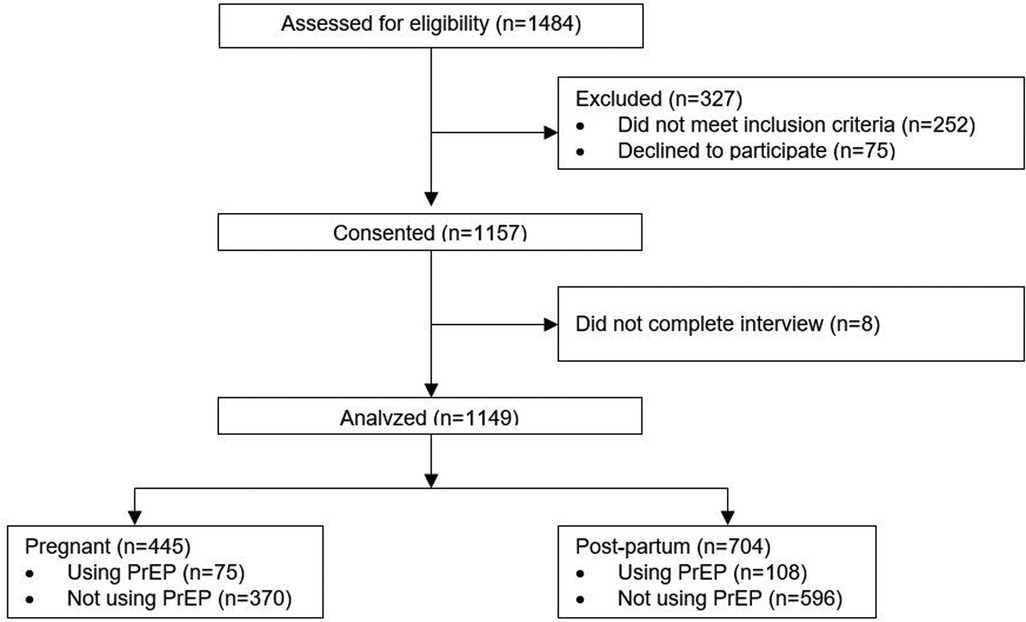
Figure 1. Flow of study screening and enrollment.
A total of 1,149 PPW women were interviewed for the study: 704 (61.3%) women were post-partum and 445 (38.7%) were pregnant (Table 1). The median age was 25 years [Interquartile Range (IQR) = 21–30 years], with 46.4% (533) 18–24 years old. Most women (n = 902, 78.8%) said that they are the ones who usually make decisions regarding their health, 100 (8.7%) had their male partners making the decisions, 111 (9.7%) their parents. Nearly two-thirds, 748 (65.3%) had HIV-negative male partners, 83 (7.2%) had HIV-positive male partners and 318 (27.7%) did not know the HIV status of their male partners. Of the women who reported that their male partners were HIV-positive, 70 (84.3%) reported that the HIV-positive male partners were on antiretroviral therapy (ART).
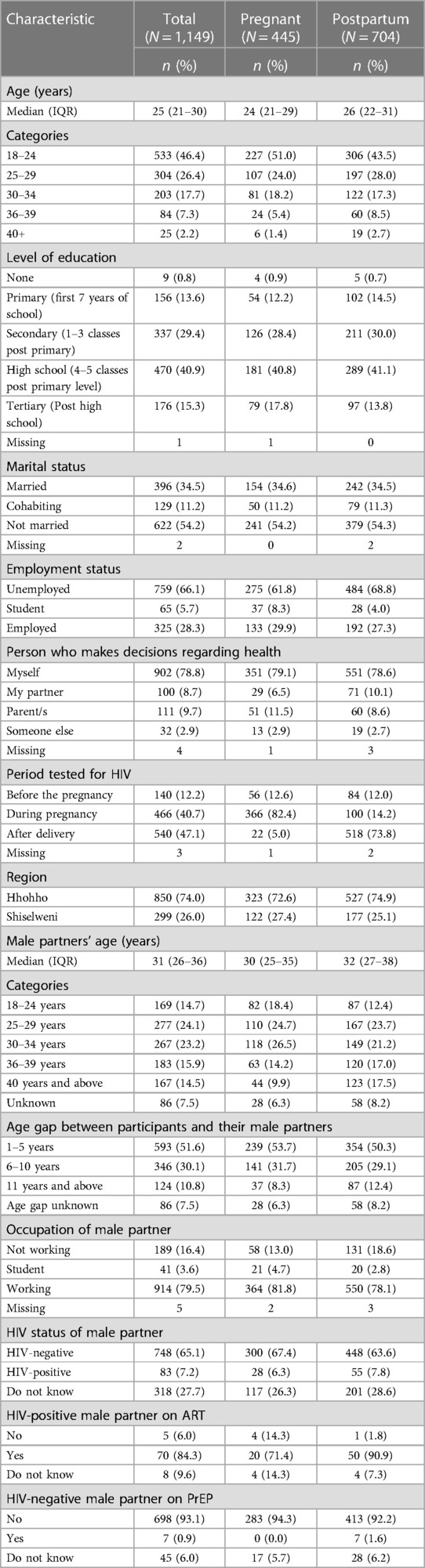
Table 1. Characteristics of study participants.
Of the 1,149 women interviewed, 353 (30.8%) reported to have used a condom in their last sex encounter while 154 (21.8%) reported to have used a condom every time they had sex in the last month and 415 (58.6%) had never used a condom during sex in the last month (Table 2). About 370 (32.3%) had tested for a sexually transmitted infection (STI) in the past 6 months; 55 (4.8%) had been treated for a Sexually Transmitted Infection (STI) in the past 3 months; 28 (2.5%) had engaged in anal sex in the past 3 months; and 127 (11.1%) had taken post-exposure prophylaxis (PEP) following a potential exposure to HIV in the past six months.
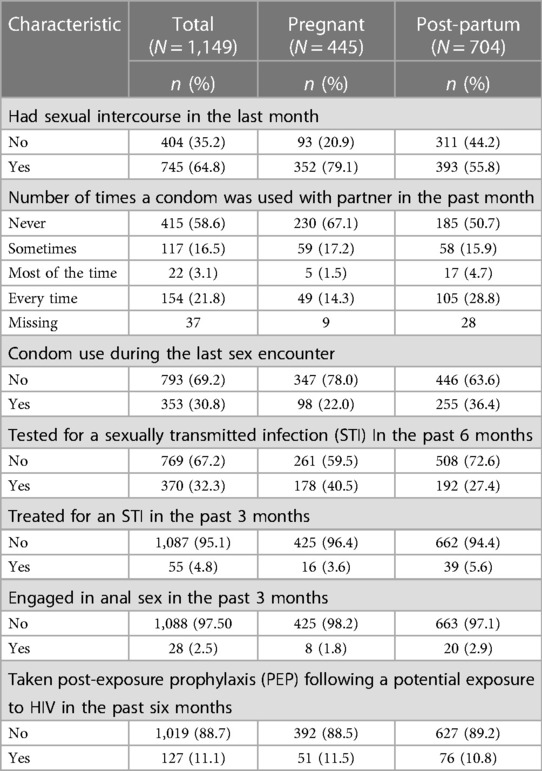
Table 2. Sexual behavior.
Over 80% (n = 930, 80.7%) of the women had ever heard about oral PrEP for HIV prevention, while 219 (19.3%) had never heard about PrEP. Most women, 706 (76.2%) heard about PrEP at a clinic or hospital, followed by 150 (16.2%) who had heard about PrEP at a community or outreach event (Supplementary Table S2). Similarly, the most preferred source of information about PrEP among the women was a clinic or hospital (n = 1,039, 90.4%), followed by the community or outreach event (n = 151, 13.1%). The clinic or hospital was also preferred by a majority (n = 1,112, 96.8%) of the women for accessing PrEP pills, followed by the community or outreach event (n = 101, 8.8%). The proportion of PPW who knew all four facts (1) Consistent use of PrEP reduces HIV risk among HIV-negative individuals, (2) People using PrEP are recommended to continue using condoms, (3) Inconsistent use of PrEP decreases its effectiveness and (4) PrEP does not help prevent other STIs) about PrEP was 635 (55.3%) (95 CI: 52.3, 58.2).
The women had positive attitudes towards PrEP. A majority of the women, 1,032 (89.8%) either agreed or strongly agreed that taking PrEP is safe; 974 (84.8%) agreed that PrEP is effective for preventing HIV; and 859 (74.8%) felt that it was not going to be difficult to adhere to PrEP every day (Table 3). Regarding stigma, a majority of the women either agreed or strongly agreed that if they were to use PrEP people would think they have HIV (n = 759, 66.0%), and that people would think that they have sex with a lot of different people (n = 658, 57.3%) (Table 3). Nearly half of the women (n = 511, 44.5%) felt that if they brought-up the subject of PrEP with their partners, then their partners would think that they are having risky sex with other people.
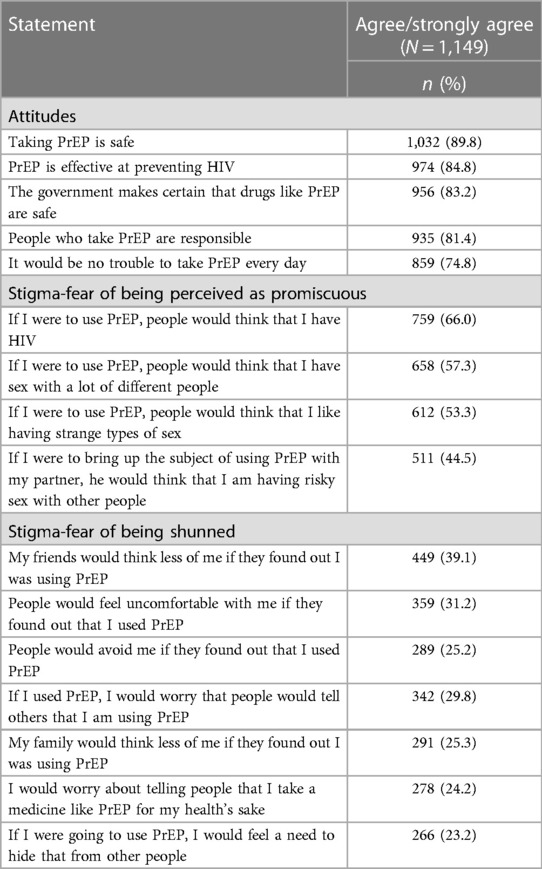
Table 3. PrEP attitudes and stigma among respondents.
Among all the 1,149 PPW interviewed for the study, the number of PPW who have ever used PrEP was 285 (24.8%), and the number of PPW who were currently using PrEP was 183 (15.9%) (Supplementary Table S3). Among the 285 women who have ever used PrEP, 102 (35.8%) had stopped using PrEP. Seventy eight (76.5%) PPW had stopped taking PrEP within the past 12 months, and 12 (13.3%) in more than a year. Thirty-five (35.2%) PPW had stopped taking PrEP due to side effects; and 59 (64.8%) stopped due to other reasons including unavailability of PrEP pills (n = 15, 27.8%), perceived lack of HIV acquisition risk (n = 7, 13.0%) and partners/husbands' refusal (n = 6, 11.1%). When asked if they would like to re-start taking PrEP, 62 (60.8%) wanted to start taking PrEP again, among which 23 (42.6%) wanted to protect themselves from getting infected with HIV, 8 (14.8%) because they did not trust their partners, and the remaining due to a variety of reasons. Of the 183 PPW who were still on PrEP during the survey; 63 (34.4%) reported to have experienced side effects as a result of taking PrEP; 142 (77.6%) had disclosed to their male partners about taking PrEP; 91 (49.7%) had disclosed to their parents; and 54 (29.5%) had disclosed to other family members (Supplementary Table S3). When asked if they would want to continue taking PrEP in the next month, 174 (95.6%) wanted to continue using PrEP for the next month and 8 (4.4%) did not.
Using multivariate logistic regression, we determined factors associated with the use of PrEP. We first used univariate logistic regression to measure association of potential factors to “PrEP use” and only included in the final multivariate model factors that were significant with a p = value of 0–05 or lower. PrEP use, comparing women on PrEP against women not on PrEP, was associated with HIV status of male partner, PrEP attitudes, and self-efficacy (Table 4). Women with an HIV-positive male partner were more likely to use PrEP compared to women with a HIV-negative partner [adjusted odds ratio [aOR] = 7.8, 95% confidence interval (CI) (3.5, 17.0)]. PPW with positive PrEP attitudes [aOR = 1.6, 95% CI (1.0, 2.4)]; and high self-efficacy about taking PrEP correctly [aOR = 1.5, 95% CI (1.1, 2.0)] were more likely to use PrEP.
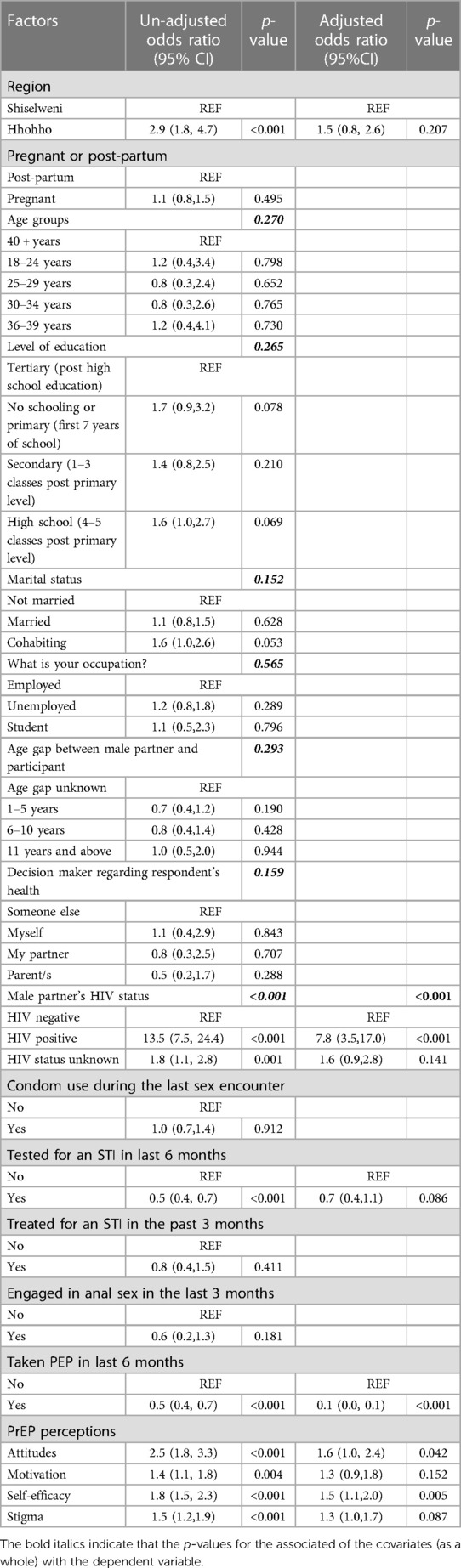
Table 4. Factors associated with PrEP use among pregnant and post-partum women.
Regarding intention to use PrEP, among 864 PPW who had never used PrEP, 65.3% intended to use PrEP in the future and 34.1% did not. The intention to use PrEP, comparing women who intended to use PrEP against women who did not intend to use PrEP, was associated with level of education, PrEP awareness, willingness to use PrEP, and self-efficacy (Table 5). PPW who had attained high school education [aOR = 1.7, 95% CI (1.1, 2.8)], secondary education [aOR = 2.2, 95% CI (1.3, 3.9)] and had primary education or no schooling [aOR = 2.0, 95% CI (1.1, 3.9)] are more likely to intend to use PrEP compared to those who have attained tertiary education. PPW who have ever heard about PrEP [aOR = 1.7, 95% CI (1.1, 2.6)]; high willingness to use PrEP [aOR = 3.1, 95% CI (2.3, 4.1)]; and with high self-efficacy (believe that they are capable of taking PrEP as required) [aOR = 1.6, 95% CI (1.3, 1.9)] are more likely to intend to use PrEP.
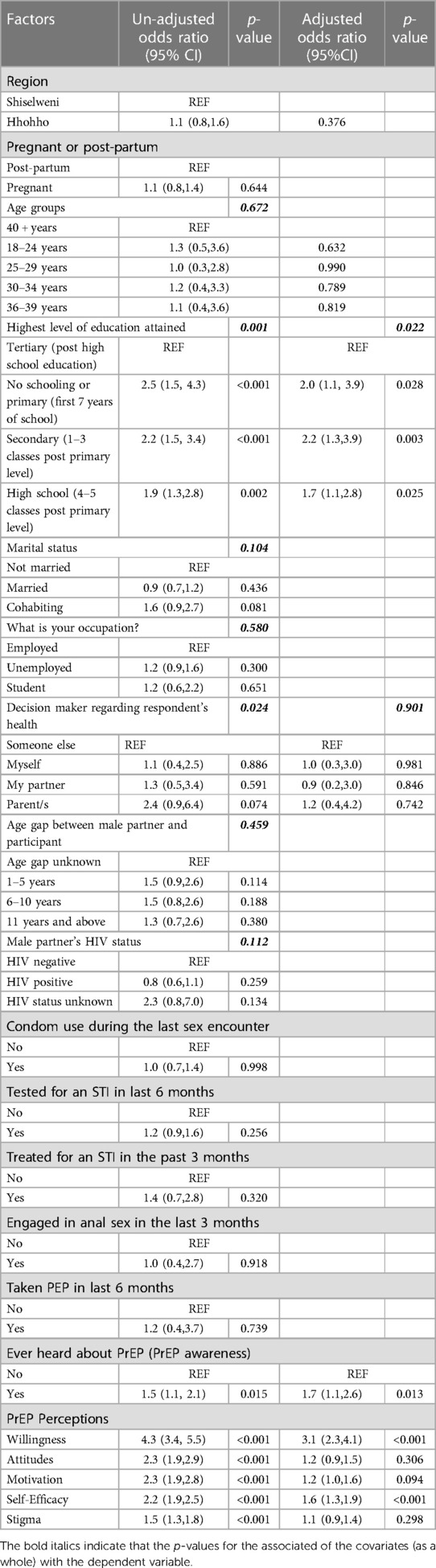
Table 5. Factors associated with intention to use PrEP among pregnant and post-partum women.
This study identified that a majority of the PPW had ever heard of PrEP, however, about 19% did not know anything about it. Additionally, only about half of PPW possessed the correct knowledge about PrEP. This is an indication of gaps in health education, particularly within health facilities, which is where the women were recruited for the study. Whilst this study shows slightly higher proportions of PPW aware and also having correct knowledge about PrEP, several studies in similar populations in different settings in Sub-Saharan Africa and the United States of America have reported relatively low awareness and knowledge about PrEP (12, 26–32). In South Africa, in a study among pregnant women from Cape Town knowledge about PrEP was only 33% (12) and in a study among young pregnant women aged 18–24 years old in KwaZulu Natal, none of the women had ever heard about PrEP before the survey (32). In Zambia, knowledge about PrEP among pregnant and breastfeeding was only 36% (28). In the United States approximately two thirds of pregnant women had never heard of PrEP before participating in the study (26). Of note is that even if the women were aware about PrEP, a majority tended to have incorrect knowledge about PrEP as an option for HIV prevention and also tended to have concerns about potential effects to their babies during pregnancy or breast feeding (27, 31).
Limited PrEP awareness and knowledge among the PPW is concerning because if women possess little or no knowledge on PrEP, then they are less likely to utilize the service even if it is offered at the healthcare facilities. From the studies it emerged clearly that high acceptability of PrEP is associated with knowledge about its efficacy in preventing the acquisition of HIV, and once PrEP was explained to the women, most of them reported positive attitudes towards PrEP and an interest to initiate PrEP (27, 29, 30, 32). PrEP programs targeting women at ANC or PNC need to develop appropriate interventions to increase health education on HIV PrEP among PPW both within health facilities and communities. Health education should aim to increase accurate PrEP knowledge and also motivate PPW to use PrEP as PPW are considered to be at high-risk of acquiring HIV.
In this study, the most cited source of PrEP information for women was the health facility. This finding indicates possible locations for health education interventions which could be implemented when the clients come for other health services. It could also be an indication of missed opportunities for health education outside the health facility environment. Extending PrEP promotion to the community can help to reach populations who do not regularly attend health facilities (34). Other studies have reported similar findings where health facilities and healthcare workers are the most cited sources of PrEP information (12, 28, 30, 31, 34). In this regard, HCWs play a critical role in delivering PrEP in antenatal and postpartum care to PPW. However, studies from South Africa and France showed that less than half of HCWs knew about PrEP, described inaccurate PrEP knowledge regarding effectiveness, and lacked clinical detail (35–38). The limited PrEP knowledge among HCWs will hinder their ability to educate patients correctly about PrEP and the confidence to prescribe PrEP There is therefore a need to address this gap by providing trainings to HCWs on information about PrEP safety, efficacy, and how to prescribe it to pregnant and breastfeeding women, and other population groups.
The study also revealed that there was stigma attached to PrEP use. Most women agreed that if they were to use PrEP, people would think they have HIV, have sex with a lot of different people and/or like having strange types of sex. The PPW also agreed that their partners would think they were having risky sex with other people. A similar study conducted in Uganda, South Africa and Zimbabwe, mentioned that participants would refrain from taking PrEP because of its association with antiretroviral therapy and HIV related stigma (39). Likewise, findings from Malawi and Zambia showed that PrEP stigma was linked to being perceived as promiscuous and being on ART due to the appearance of PrEP packaging (29). This stigma associated with PrEP leads to challenges in PrEP initiation, retention, and adherence (14, 30, 34, 40–43). Interventions to address stigma and public education on HIV/AIDS prevention should address the social and cultural norms that undermine PrEP's optimal use (44, 46). HIV prevention programs should also consider introducing long-lasting injectable PrEP, as it comes with benefits of administration only once every two months and invisibility as no pills are required to be carried and taken by the individual (44–46).
Despite WHO's recommendation to offer PrEP to all population groups at substantial risk of HIV infection, the uptake is persistently low (11). In this study, only a quarter of PPW women have ever used PrEP and an even lower percentage were on PrEP at the time of the study. On the other hand, a large proportion of the women engaged in sex with men who were HIV-positive or had unknown HIV status, and many of the women's sexual encounters did not involve the use of condoms. This low coverage of PrEP among the women engaged in unprotected sex is worrying and may explain the continued high incidence of HIV in Eswatini. The factors associated with PrEP use identified by this study included having a known HIV-positive male partner, a male partner with unknown HIV status, positive attitudes towards PrEP, high self-efficacy, having tested for an STI in the last 6 months, and having taken PEP in the last 6 months. This finding aligns with previous studies conducted in Zambia and Kenya among PPW where factors associated with PrEP use were: being a sero-different couple, having a partner of unknown HIV status, having a positive attitude towards PrEP (47), and a reactive syphilis test result (7). Some studies identified other pertinent factors for PrEP use such as: engaging in sex without a condom in the past six months, having experienced intimate partner violence (7, 29), the desire to safely conceive a child (23), being a drug injector, being homeless (48) and rape (29). Worth noting is that most factors associated with PrEP use are factors know to be associated with the risk of HIV acquisition. Literature has shown that understanding the risk of HIV infection strengthens the desire to seek information about PrEP (12) and that women with perceived risk for HIV acquisition had high interest to use PrEP (49). For this reason, it is imperative for HCW to be aware of risk factors for HIV acquisition in order to provide the opportunity to discuss expanded HIV prevention options with women who are at risk of HIV exposure.
Among PPW using PrEP in this study, more than a quarter experienced various side effects, with dizziness and headaches being the most reported. Consequently, 36% of these women stopped taking PrEP due to the side effects. This finding resonates with already existing literature on PrEP where side effects were stated as some of the reasons for stopping PrEP (50, 51). However, studies from Zimbabwe and Mozambique had contradictory findings where the experience of side effects was not perceived as a major reason for discontinuing the use of PrEP, and in such cases women developed coping strategies of dealing with side effects (23, 52). It is critical for HCWs to provide information about PrEP side effects to PPW during initiation and follow up, so that they cope with side effects without stopping PrEP.
Our study found other reasons for PrEP discontinuation including; unavailability of PrEP and being stopped by partner or husband. Consistent findings from regional studies reported PrEP stock-outs and needing partner or husband approval to take PrEP as barriers to PrEP uptake, adherence and retention (23, 39, 47). The lack of autonomy among women to make decisions concerning their health may present a barrier to PrEP uptake. Thus, male involvement in promoting PrEP uptake beyond healthcare spaces including the community and key leaders such as traditional leaders, religious leaders, political leaders and employers could increase the use of PrEP in this target population (56) Also, political will is key in developing interventions and policy reviews to address challenges contributing to PrEP drugs stock-outs.
Some reasons for stopping PrEP unique to other studies were: changes in partner relationships and doubting safety of PrEP in pregnancy (41), changing risk perception, lack of social support, PrEP stigma, pill fatigue, and loss of interest (43, 51). These findings suggest that appropriate education and messaging about PrEP use, effectiveness, and side effects to communities might improve PrEP uptake and persistence. In so doing, partners and family members would also be enlightened about the importance of PrEP and supporting PrEP users. Also, conceptualizing PrEP as an intervention that can be paused and later restarted based on HIV risk may help ease the pill burden (54).
From this study, among women who never used PrEP, 65%, intended to use PrEP in the future. The odds of intention to use PrEP were high among women with low levels of education, awareness of PrEP, high self-efficacy and high willingness to use PrEP. These findings are similar to other studies where women with awareness of PrEP and high self-efficacy showed increased willingness to use PrEP (28, 55). On the contrary, Scott et al. in a research among PPW found that self-efficacy was not associated with PrEP uptake intention (56). Further, positive attitudes, subjective norms (support or approval from significant other), maternal status and breastfeeding were other factors associated with PrEP use intention reported from existing evidence (28, 55). To increase intention to use PrEP, it is imperative to sensitize women on risk factors for HIV infection, to be empowered with knowledge and make informed choices about using PrEP.
The main strength of this study is that it includes a large sample size of PPW from 16 health facilities. The results reported in this study are specific to PPW, providing important insights to inform scale-up of PrEP services to PPW. However, the study also has some limitations. The main limitation of this study is that it only sampled from the population of those already accessing the health care facility, therefore it may not represent the perspective of those who do not access health care facilities. Additionally, the study relies on self-reported information about PrEP during the interviews which may be biased.
The study showed that there are gaps in PrEP awareness and knowledge and that PrEP uptake among PPW was low. While PPW generally believed that PrEP is safe and effective to prevent HIV, they were concerned about possible side effects and encountering negative experiences if they were to disclose about taking PrEP to their sex partners. There is a need to strengthen health education about PrEP for PPW. This should include improving the integration of PrEP counselling into existing clinic visits at ANC and PNC and offering clients with options for HIV prevention. The program can also improve efforts to identify and educate sero-discordant couples; continue implementing couples' HIV testing to ensure that the women have knowledge of their risk; and identify outreach strategies to be implemented at community level to reduce stigma and misinformation around PrEP. These strategies can reach women who may become pregnant (intentionally or otherwise), and possibly increase acceptability of PrEP early in the antenatal course. In addition, the study suggests that many women are ready for PrEP since more than two thirds of the women had the intention of initiating PrEP. Accordingly, program implementers should use this opportunity to expand PrEP activities nation-wide.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Eswatini Health and Human Research Review Board (EHHRRB) and Advarra IRB. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
PK: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. SM: Writing – review & editing, Writing – original draft. KK: Conceptualization, Investigation, Validation, Writing – review & editing. SM: Conceptualization, Investigation, Writing – review & editing. PD: Conceptualization, Investigation, Writing – review & editing. VT: Writing – review & editing. RM: Conceptualization, Investigation, Validation, Writing – review & editing. GW: Conceptualization, Investigation, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study was made possible through funding from the U.S. President's Emergency Plan for AIDS Relief (PEPFAR) through the United States Agency for International Development (USAID) under the Eswatini ASPIRE Project Contract No: 72067421C00005 and the University of California, Los Angeles (UCLA) AIDS Institute, Dance Marathon Fund. The contents herein are solely the responsibility of the authors and do not necessarily represent the official views of USAID, PEPFAR, the U.S. government or UCLA.
The authors would like to gratefully thank the study participants and staff in study sites for their valuable contribution and support during the implementation of the study. We would also like to thank the hard work and dedication of the study team and Research Assistants who assisted with data collection for the study. We thank the Eswatini Ministry of Health, the Regional Health Management Teams in both Hhohho and Shiselweni regions and the study sites managers for their collaboration with this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frph.2023.1253384/full#supplementary-material
1. World Health Organization (WHO). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach—2nd ed.2016 29 January 2021 (cited 2021 29 January). Available at: https://apps.who.int/iris/bitstream/handle/10665/208825/9789241549684_eng.pdf?sequence=1
2. Baeten JM, Donnell D, Ndase P, Mugo NR, Campbell JD, Wangisi J, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med. (2012) 367(5):399–410. doi: 10.1056/NEJMoa1108524
3. Thigpen MC, Kebaabetswe PM, Paxton LA, Smith DK, Rose CE, Segolodi TM, et al. Antiretroviral preexposure prophylaxis for heterosexual HIV transmission in Botswana. N Engl J Med. (2012) 367(5):423–34. doi: 10.1056/NEJMoa1110711
4. Bekker L-G, Roux S, Sebastien E, Yola N, Amico KR, Hughes JP, et al. Daily and non-daily pre-exposure prophylaxis in African women (HPTN 067/ADAPT Cape Town trial): a randomised, open-label, phase 2 trial.Lancet HIV. (2018) 5(2):e68–78. doi: 10.1016/S2352-3018(17)30156-X
5. Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. (2010) 363(27):2587–99. doi: 10.1056/NEJMoa1011205
6. Choopanya K, Martin M, Suntharasamai P, Sangkum U, Mock PA, Leethochawalit M, et al. Antiretroviral prophylaxis for HIV infection in injecting drug users in Bangkok, Thailand (the Bangkok Tenofovir Study): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet (London, England). (2013) 381(9883):2083–90. doi: 10.1016/S0140-6736(13)61127-7
7. Dettinger JC, Kinuthia J. Perinatal outcomes following maternal pre-exposure prophylaxis (PrEP) use during pregnancy: results from a large PrEP implementation program in Kenya. J Int AIDS Soc. (2019) 22(9):e25378. doi: 10.1002/jia2.25378
8. Mugo NR, Hong T, Celum C, Donnell D, Bukusi EA, John-Stewart G, et al. Pregnancy incidence and outcomes among women receiving preexposure prophylaxis for HIV prevention: a randomized clinical trial. JAMA. (2014) 312(4):362–71. doi: 10.1001/jama.2014.8735
9. Mofenson LM, Baggaley RC, Mameletzis I. Tenofovir disoproxil fumarate safety for women and their infants during pregnancy and breastfeeding. AIDS. (2017) 31(2):213–32. doi: 10.1097/QAD.0000000000001313
10. Mugwanya KK, Hendrix CW, Mugo NR, Marzinke M, Katabira ET, Ngure K, et al. Pre-exposure prophylaxis use by breastfeeding HIV-uninfected women: a prospective short-term study of antiretroviral excretion in breast milk and infant absorption. PLoS Med. (2016) 13(9):e1002132. doi: 10.1371/journal.pmed.1002132
11. World Health Organization. WHO TECHNICAL BRIEF: Preventing HIV during pregnancy and breastfeeding in the context of PrEP2017 19 November 2020 (cited 2020 19 November). Available at: https://apps.who.int/iris/bitstream/handle/10665/255866/WHO-HIV-2017.09-eng.pdf?sequence=1
12. DiTullio DJ, Farley E, Gomba Y, Coates TJ, Bekker L-G, Myer L, et al. Factors associated with knowledge of pre-exposure prophylaxis in pregnant women in Cape Town, South Africa. Int J STD AIDS. (2019) 30(11):1063–70. doi: 10.1177/0956462419863216
13. Amico KR, Wallace M, Bekker LG, Roux S, Atujuna M, Sebastian E, et al. Experiences with HPTN 067/ADAPT study-provided open-label PrEP among women in Cape Town: facilitators and barriers within a mutuality framework. AIDS Behav. (2017) 21(5):1361–75. doi: 10.1007/s10461-016-1458-y
14. Moran A, Mashele N, Mvududu R, Gorbach P, Bekker L-G, Coates TJ, et al. Maternal PrEP use in HIV-uninfected pregnant women in South Africa: role of stigma in PrEP initiation, retention and adherence. AIDS Behav. (2022) 26:205–17. doi: 10.1007/s10461-021-03374-x
15. The Government of the Kingdom of Eswatini. Swaziland Population-based HIV impact assessmnet 3 (SHIMS3): Summary sheet. Mbabane, Eswatini (2022).
16. The Government of the Kingdom of Eswatini. Eswatini annual sexual and reproductive health report. In: Mbabane E, editors. Sexual and reproductive health unit. Ministry of Health (2018). p. 35.
17. PREPWatch. PrEP Demonstration Project Tools by Category 2020. Available at: https://www.prepwatch.org/demo-project-tools-category/#surveys
18. Kahle EM, Sullivan S, Stephenson R. Functional knowledge of pre-exposure prophylaxis for HIV prevention among participants in a web-based survey of sexually active gay, bisexual, and other men who have sex with men: cross-sectional study. JMIR Public Health Surveill. (2018) 4(1):e13. doi: 10.2196/publichealth.8089
19. Shrestha R, Altice FL, Huedo-Medina TB, Karki P, Copenhaver M. Willingness to use Pre-exposure prophylaxis (PrEP): an empirical test of the information-motivation-behavioral skills (IMB) model among high-risk drug users in treatment. AIDS Behav. (2017) 21(5):1299–308. doi: 10.1007/s10461-016-1650-0
20. Walsh JL. Applying the information-motivation-behavioral skills model to understand PrEP intentions and use among men who have sex with men. AIDS Behav. (2019) 23(7):1904–16. doi: 10.1007/s10461-018-2371-3
21. Klein H, Washington TA. The Pre-exposure prophylaxis (PrEP) stigma scale: preliminary findings from a pilot study. Int Public Health J. (2019) 11(2):185–95.32089789
22. Wheelock A, Eisingerich AB, Ananworanich J, Gomez GB, Hallett TB, Dybul MR, et al. Are Thai MSM willing to take PrEP for HIV prevention? An analysis of attitudes, preferences and acceptance. PLoS One. (2013) 8(1):e54288. doi: 10.1371/journal.pone.0054288
23. Gombe MM, Cakouros BE, Ncube G, Zwangobani N, Mareke P, Mkwamba A, et al. Key barriers and enablers associated with uptake and continuation of oral pre-exposure prophylaxis (PrEP) in the public sector in Zimbabwe: qualitative perspectives of general population clients at high risk for HIV. PLoS One. (2020) 15(1):e0227632. doi: 10.1371/journal.pone.0227632
24. Mugwanya KK, Pintye J, Kinuthia J, Abuna F, Lagat H, Begnel ER, et al. Integrating preexposure prophylaxis delivery in routine family planning clinics: a feasibility programmatic evaluation in Kenya. PLoS Med. (2019) 16(9):e1002885. doi: 10.1371/journal.pmed.1002885
25. Joseph Davey DL, Mvududu R, Mashele N, Lesosky M, Khadka N, Bekker LG, et al. Early pre-exposure prophylaxis (PrEP) initiation and continuation among pregnant and postpartum women in antenatal care in Cape Town, South Africa. J Int AIDS Soc. (2022) 25(2):e25866. doi: 10.1002/jia2.25866
26. Groves AK, Vadaketh J, Raziano VT, Nkwihoreze H, Short WR, Momplaisir F. Preexposure prophylaxis acceptability among pregnant individuals and implications for human immunodeficiency virus prevention. Obstet Gynecol. (2022) 139(4):537–44. doi: 10.1097/AOG.0000000000004709
27. Joseph Davey D, Farley E, Towriss C, Gomba Y, Bekker LG, Gorbach P, et al. Risk perception and sex behaviour in pregnancy and breastfeeding in high HIV prevalence settings: programmatic implications for PrEP delivery. PLoS One. (2018) 13(5):e0197143. doi: 10.1371/journal.pone.0197143
28. Hamoonga TE, Mutale W, Hill LM, Igumbor J, Chi BH. Salient beliefs and intention to use pre-exposure prophylaxis among pregnant and breastfeeding women in Zambia: application of the theory of planned behaviour. Glob Public Health. (2023) 18(1):2184483. doi: 10.1080/17441692.2023.2184483
29. Maseko B, Hill LM, Phanga T, Bhushan N, Vansia D, Kamtsendero L, et al. Perceptions of and interest in HIV pre-exposure prophylaxis use among adolescent girls and young women in Lilongwe, Malawi. PLoS One. (2020) 15(1):e0226062. doi: 10.1371/journal.pone.0226062
30. Hirschhorn LR, Brown RN, Friedman EE, Greene GJ, Bender A, Christeller C, et al. Black cisgender women’s PrEP knowledge, attitudes, preferences and experience in Chicago. J Acquir Immune Defic Syndr. (2020) 84(5):497. doi: 10.1097/QAI.0000000000002377
31. Bradley EL, Hoover KW. Improving HIV preexposure prophylaxis implementation for women: summary of key findings from a discussion series with women’s HIV prevention experts. Women’s Health Issues. (2019) 29(1):3–7. doi: 10.1016/j.whi.2018.08.004
32. Vazquez L, Moll AP, Kacin A, Ndlovu NE, Shenoi SV. Perceptions of HIV preexposure prophylaxis among young pregnant women from rural KwaZulu-Natal, South Africa. AIDS Patient Care STDS. (2019) 33(5):214–9. doi: 10.1089/apc.2018.0242
33. Geldsetzer P, Bärnighausen K, Hettema A, McMahon SA, Dalal S, Chase RP, et al. A stepped-wedge randomized trial and qualitative study of uptake of HIV pre-exposure prophylaxis among the general population in eswatini. Sci Transl Med. (2020) 12(562):1–27. doi: 10.1126/scitranslmed.aba4487
34. Auerbach JD, Kinsky S, Brown G, Charles V. Knowledge, attitudes, and likelihood of pre-exposure prophylaxis (PrEP) use among US women at risk of acquiring HIV. AIDS Patient Care STDS. (2015) 29(2):102–10. doi: 10.1089/apc.2014.0142
35. Zimba C, Maman S, Rosenberg NE, Mutale W, Mweemba O, Dunda W, et al. The landscape for HIV pre-exposure prophylaxis during pregnancy and breastfeeding in Malawi and Zambia: a qualitative study. PloS one. (2019) 14(10):e0223487. doi: 10.1371/journal.pone.0223487
36. Davey DL J, Daniels J, Beard C, Mashele N, Bekker L-G, Dovel K, et al. Healthcare provider knowledge and attitudes about pre-exposure prophylaxis (PrEP) in pregnancy in Cape Town, South Africa. Aids Care. (2020) 32(10):1290–4. doi: 10.1080/09540121.2020.1782328
37. . Human immunodeficiency virus Pre-exposure prophylaxis knowledge, attitudes, and self-efficacy among family planning providers in the southern United States: bridging the gap in provider training. In: Ramakrishnan A, Sales JM, McCumber M, Powell L, Sheth AN, editors. Open forum infectious diseases. Oxford University Press US (2022).
38. Gilles M, Tetart M, Huleux T, Thill P, Meybeck A, Robineau O. HIV pre-exposure prophylaxis (PrEP) knowledge among general practitioners in 2020: a French survey. Infect Dis Now. (2023) 53(3):104649. doi: 10.1016/j.idnow.2023.104649
39. Muhumuza R, Ssemata AS, Kakande A, Ahmed N, Atujuna M, Nomvuyo M, et al. Exploring perceived barriers and facilitators of PrEP uptake among young people in Uganda, Zimbabwe, and South Africa. Arch Sex Behav. (2021) 50(4):1729–42. doi: 10.1007/s10508-020-01880-y
40. Moseholm E, Gilleece Y, Collins B, Kowalska JD, Vasylyev M, Elía MJP, et al. Achievements and gaps to provide pre-exposure prophylaxis (PrEP) for women across the European region–results from a European survey study. J Virus Erad. (2021) 7(1):100026. doi: 10.1016/j.jve.2020.100026
41. Pyra M, Johnson AK, Devlin S, Uvin AZ, Irby S, Stewart E, et al. HIV pre-exposure prophylaxis use and persistence among black ciswomen:“women need to protect themselves, period”. J Racial Ethn Health Disparities. (2022) 9(3):820–9. doi: 10.1007/s40615-021-01020-9
42. Bjertrup PJ, Mmema N, Dlamini V, Ciglenecki I, Mpala Q, Matse S, et al. PrEP reminds me that I am the one to take responsibility of my life: a qualitative study exploring experiences of and attitudes towards pre-exposure prophylaxis use by women in Eswatini. BMC Public Health. (2021) 21(1):1–8. doi: 10.1186/s12889-021-10766-0
43. Duby Z, Bunce B, Fowler C, Jonas K, Bergh K, Govindasamy D, et al. “These girls have a chance to be the future generation of HIV negative”: experiences of implementing a PrEP programme for adolescent girls and young women in South Africa. AIDS Behav. (2023) 27(1):134–49. doi: 10.1007/s10461-022-03750-1
44. Montgomery ET, Atujuna M, Krogstad E, Hartmann M, Ndwayana S, O’Rourke S, et al. The invisible product: preferences for sustained-release, long-acting pre-exposure prophylaxis to HIV among South African youth. J Acquir Immune Defic Syndr. (2019) 80(5):542. doi: 10.1097/QAI.0000000000001960
45. Minnis AM, Atujuna M, Browne EN, Ndwayana S, Hartmann M, Sindelo S, et al. Preferences for long-acting Pre-exposure prophylaxis (PreP) for HIV prevention among South African youth: results of a discrete choice experiment. J Int AIDS Soc. (2020) 23(6):e25528. doi: 10.1002/jia2.25528
46. World Health Organization. WHO recommends the dapivirine vaginal ring as a new choice for HIV prevention for women at substantial risk of HIV infection Geneva 2021 (cited 2023 26 April 2023). Available at: https://www.who.int/news/item/26-01-2021-who-recommends-the-dapivirine-vaginal-ring-as-a-new-choice-for-hiv-prevention-for-women-at-substantial-risk-of-hiv-infection
47. Hamoonga TE, Mutale W, Hill LM, Igumbor J, Chi BH. “PrEP protects us”: behavioural, normative, and control beliefs influencing pre-exposure prophylaxis uptake among pregnant and breastfeeding women in Zambia. Front Reprod Health. (2023) 5:1084657. doi: 10.3389/frph.2023.1084657
48. Bazzi AR, Biancarelli DL, Childs E, Drainoni M-L, Edeza A, Salhaney P, et al. Limited knowledge and mixed interest in pre-exposure prophylaxis for HIV prevention among people who inject drugs. AIDS Patient Care STDS. (2018) 32(12):529–37. doi: 10.1089/apc.2018.0126
49. Hill LM, Maseko B, Chagomerana M, Hosseinipour MC, Bekker LG, Pettifor A, et al. HIV Risk, risk perception, and PrEP interest among adolescent girls and young women in Lilongwe, Malawi: operationalizing the PrEP cascade. J Int AIDS Soc. (2020) 23:e25502. doi: 10.1002/jia2.25502
50. Arnold-Forster D, Horne R, Nutland W, Wayal S, Rayment M, Rae C, et al. Perceptions and practicalities influencing pre-exposure prophylaxis adherence among men who have sex with men in England. AIDS Behav. (2022) 26(8):2768–82. doi: 10.1007/s10461-022-03624-6
51. Celum CL, Gill K, Morton JF, Stein G, Myers L, Thomas KK, et al. Incentives conditioned on tenofovir levels to support PrEP adherence among young South African women: a randomized trial. J Int AIDS Soc. (2020) 23(11):e25636. doi: 10.1002/jia2.25636
52. Falcao J, Ahoua L, Zerbe A, di Mattei P, Baggaley R, Chivurre V, et al. Willingness to use short-term oral pre-exposure prophylaxis (PrEP) by migrant miners and female partners of migrant miners in Mozambique. Cult Health Sex. (2017) 19(12):1389–403. doi: 10.1080/13691058.2017.1316424
53. Mweemba O, Zimba C, Chi BH, Chibwe KF, Dunda W, Freeborn K, et al. Contextualising men’s role and participation in PMTCT programmes in Malawi and Zambia: a hegemonic masculinity perspective. Glob Public Health. (2022) 17(9):2081–94. doi: 10.1080/17441692.2021.1964559
54. Haberer JE, Bangsberg DR, Baeten JM, Curran K, Koechlin F, Amico KR, et al. Defining success with HIV pre-exposure prophylaxis: a prevention-effective adherence paradigm. AIDS. (2015) 29(11):1277. doi: 10.1097/QAD.0000000000000647
55. Chittamuru D, Frye V, Koblin BA, Brawner B, Tieu HV, Davis A, et al. PrEP stigma, HIV stigma, and intention to use PrEP among women in New York city and Philadelphia. Stig. Health. (2020) 5(2):240–6. doi: 10.1037/sah0000194
Keywords: pregnant and post-natal women, HIV pre-exposure prophylaxis, PrEP, uptake, intention, Eswatini
Citation: Khumalo PN, Mkhonta SS, Kindandi K, Matse S, Dlamini PB, Tukei V, Machekano R and Woelk G (2023) Uptake of and intention to use oral pre-exposure prophylaxis for HIV among pregnant and post-natal women in Eswatini: a cross-sectional survey. Front. Reprod. Health 5:1253384. doi: 10.3389/frph.2023.1253384
Received: 5 July 2023; Accepted: 11 October 2023;
Published: 27 October 2023.
Edited by:
Irene Njuguna, Kenyatta National Hospital, KenyaReviewed by:
Jerusha Nyabiage Mogaka, University of Washington, United States© 2023 Khumalo, Mkhonta, Kindandi, Matse, Dlamini, Tukei, Machekano and Woelk. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philisiwe Ntombenhle Khumalo cGtodW1hbG9AcGVkYWlkcy5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.