 Emmanuel Ndagijimana1*
Emmanuel Ndagijimana1* Emmanuel Biracyaza
Emmanuel Biracyaza Manasse Nzayirambaho
Manasse Nzayirambaho- 1Department of Epidemiology and Biostatistics, School of Public Health, University of Rwanda, Kigali, Rwanda
- 2School of Rehabilitation, Faculty of Medicine, Université de Montréal, Montréal, QC, Canada
Background: Risky sexual behaviors (RSBs) remain public health concerns in adolescents from sub-Saharan Africa (SSA), and these practices may increase vulnerability to reproductive health problems if no early healthcare strategies are implemented. While previous studies reported that adolescents are engaged in these RSBs due to diverse influences such as the teenage stage, urbanization, and change in the environment they experience, there is a shortage of studies on RSB among adolescents in SSA. This study assessed the magnitude of RSBs and the RSB-associated factors among in-school adolescents.
Methods: School-based cross-sectional study was conducted among 263 Saint Andre school students in Kigali, Rwanda, from July 3, 2020, to September 30, 2020. Systematic random sampling techniques were employed. All data were entered into Epi-Data and analyzed using SPSS version 25. Chi-square tests and multivariable logistic regression analyses were applied to determine factors associated with risky sexual behaviors. Confidence intervals (CIs) of 95% and 5% for statistical significance were maintained.
Results: Of 263 participants, 109 (41%) experienced RSB in their lifetime. Among them, 66 respondents (60.55%) utilized contraceptive methods to prevent sexual and reproductive problems that can be caused by unprotected sexual intercourse. The students who experienced domestic violence had increased odds of experiencing RSB [odds ratio (OR) = 4.22; 95% CI: 1.6–11.23] than their counterparts. Those in grade 11 (OR = 2.68; 95% CI: 1.06–6.78) and grade 12 (OR = 4.39; 95% CI: 1.82–10.56) were more likely to practice RSB than those in grade 10. Alcohol users were almost more likely to experience RSB (OR = 3.9; 95% CI: 1.97–5.5) than their counterparts. Those who lived away from their biological parents had higher likelihood of experiencing RSB (OR = 2.5; 95% CI: 1.14–4.42) than those who lived with one or both parents. Students who experienced peer pressure were more likely to engage in RSB (OR = 3.9; 95% CI: 2.01–7.51) than their counterparts.
Conclusion: Promoting specific intervention programs built upon the factors associated with RSB among high school students needs to be prioritized.
Background
Most of the students from secondary schools are often aged between 11 and 24 years. This age interval, characterized by physical maturation, is considered to have sexually active people (1, 2). A report from the United Nations International Children’s Emergency Fund (UNICEF) has recently documented that adolescence is the period that constitutes three stages of age, namely, early adolescence (from 10 to 13 years old), middle adolescence (from 14 to 16 years old), and late adolescence (from 17 to 19 years old), while those aged 20–24 years are considered young adults (3). During this transitional period between childhood and adulthood, physical maturity precedes psychological and social maturity. Thus, it is in this transition that adolescents are highly exposed to risky sexual behavior (RSB) if parents do not provide early sexual health education to their children at a younger age. RSB refers to the engagement in sexual practices and sometimes unprotected sexual intercourse (4). A similar research stated several examples of RSB, such as unprotected intercourse without male or female condom use, unprotected mouth-to-genital contact, starting sexual practices at a young age, having multiple sexual partners, and having a high-risk partner. According to previous studies (5–7), these practices might increase vulnerability to reproductive health problems. RSB can also be measured across six indicators, namely, the first experience of sex was involuntary, coercive sex in the past year, reported not using a condom at sexual debut, and reported not using a condom during the last intercourse, starting sexual practices at young age, and possession of multiple sex partners. Previous studies also reported that 42.4% had more than one sexual partner and had received cash or in-kind compensation for sex in the past year. Based on this literature, all the study participants presented more than one indicator in their previous sexual practices that allowed us to conclude RSB (8, 9).
RSB has significant effects not only on the children but also on family functioning, community resilience, and the development of the country (4–6). These behaviors left the patricians of these RSBs almost maimed, with tremendous effects on biological or physiological health, mental health, and social health. Consequently, these behaviors are extreme circumstances, and there is a need for a multidisciplinary team to prevent teenagers from these behaviors and their impact (psychosocial and physiological effects) on their lifestyle.
In most high schools, the majority of the students are teenagers. Adolescence is a stage that people encounter once throughout a lifetime. It refers to a period in which they may experience RSB, which may have adverse sexual and reproductive health outcomes (4, 10, 11). Further, healthy sexual development substantially contributes to the quality of life of the sexual users or holistic personal wellbeing. However, unaware youths and adolescents may develop diverse RSBs that may put their lives in danger (4, 6, 12). In low- and middle-income countries (LMICs), the incidence of RSB, including unprotected sexual intercourse or barebacking and early sexual initiation, is increasing; however, efforts are being made by the nations to increase awareness and attenuate the prevalence of sexual reproductive problems (10). More than 50% new sexually transmitted diseases (STDs) are documented every year as a result of RSB in young adults aged less than 24 years old (13). Further, young adults also experience high-risk behaviors, including substance users (smoking, alcohol) and gender-based violence, which lead to the RSB (7, 8). In Ethiopia and many other developing countries, a high proportion of sexual reproductive health (SRH) problems such as HIV are the result of RSB, mainly in young people. In particular, research on the AIDS epidemic established that sub-Saharan Africa (SSA) accounts for 60% of all people living with HIV/AIDS due to the RSB, which has hampered the quality of life (12, 14).
It is important to note that knowledge of HIV/AIDS, sociodemographic characteristics, education of the mother, family structure, family income per month, year of education, occupation of the mother, age of the start of sexual intercourse, peer pressure, substance use, and coercion are the factors responsible for the risky sexual behaviors among the high school students (5, 15). Further, students with poor knowledge of HIV/AIDS have greater odds of engaging in risky sexual behaviors. During transition from childhood, adolescents experience rapidly changing lifestyles by being exposed to the internet and mass media that influence them to easily engage in these practices (13, 15). In addition, the empirical evidence in Botswana has reported that young people are sexually active and they often experience their first sexual encounter at an average age below 18 years, which is considered risky sexual intercourse since they are not mature (11). Similar authors stated that 90% of the boys aged 10–14 years had their first sexual experience unintentionally, while 50% of the boys did sexual practices after planning. Additionally, more than half of girls aged 15–24 years experienced their first sexual intercourse unintentionally. Unfortunately, more than half of teenage girls experience unwanted pregnancies; however, some of the adolescents who are engaged in RSB use contraceptives (16). Regarding the factors associated with the RSB, peer pressure was reported to result in school dropout among the students from primary and secondary schools (13, 17).
In Rwanda, upper-secondary education encompasses grades 10–12 (Senior 4 to Senior 6), and the students of these grades are often 15–19 years old. However, depending on various characteristics, the students may be older than 20 years. Many young adults in Rwanda are engaged in sexual behaviors that increase their risk of sexual reproductive problems such as HIV, gonorrhea, syphilis, and Papillomavirus, which hinder the quality of life of the affected people (11, 18). Rwanda, like many other countries, is trying to cope with the problem of sexual behavior, especially in the young population, on the same scale as drug abuse or alcohol. This is because engagement of young people in RSBs has a negative impact on the population in general and on reproductive health in particular (19, 20). Although the present literature on RSB and its risk factors is limited, we hypothesize that the prevalence of RSB is high and sociodemographic factors are related to RSB in Rwanda, as previously reported in the other SSA countries. This study determined the magnitude of RSB and the factors associated with RSB among students from secondary schools in Rwanda.
Materials
Study design
An institution-based cross-sectional study design was applied among the students from Collège Saint André, a secondary school in Kigali, Rwanda. Students registered for grades Seniors 4–6 were systematically selected and enrolled in the study.
Settings and participants
The study surveyed high school students from Collège Saint André, which is one of the biggest secondary schools in the city of Kigali, Rwanda. This study used a quantitative approach to assess the level of sexual intercourse and to identify its associated factors among this target population using an individual self-administered questionnaire. The total number of younger students in the school was estimated to be 596 out of a total of 599 students.
Sampling procedures
A total of 596 students were found in Collège Saint André. A sampling frame containing the lists of all students under each grade level (10th, 11th, and 12th) was developed based on the lists obtained from the students’ record office in the academic year 2019 (Figure 1). Then, the sample size was calculated using a single population proportion. Formula was used to calculate the sample size, where “n” stands for the sample size, “N” stands for the total population, and “e” is the margin error (0.05%). Therefore, . Using this information, the calculated sample size was n = 239. Considering the possible nonresponses, we added 10% of extra participants; then, the total sample size of our study participants was 263. In each selected class, the sample was drawn proportionally to the size of the class (total sample size divided by the number of available students in each class). The lists of all students in each class were used to reach the participants. Each student on the list of the class was given a number. Then, all numbers were written on pieces of paper and put into a basket. The researcher picked the numbers randomly from the basket, one by one, until the calculated sample size for each class was reached. After obtaining the total sample size, the systematic random sampling technique was applied to select the interviewees.

Figure 1. Schematic staging of sampling procedures.
Study variables
The outcome variable for our study was experiencing RSB. The explanatory variables were sociodemographic factors (such as student’s age, gender, religion, and education), parental characteristics (like education of the mother and father), substance use, living arrangements, environmental variables (mode of study, peer pressure, access to channel media, or social media), and grades of the student, and communication with parents about sexual intercourse.
Data collection
The trained graduates from undergraduate programs at the University of Rwanda performed data collection from July 3, 2020 to September 30, 2020, and all the data collectors were under the supervision of the authors. Research questionnaires were administered among the eligible participants based on their grades or classes. Indeed, before the students filled out the research questionnaires, they were informed about the research purpose. The filled questionnaires were submitted to the data collectors.
Data analysis
Prior to statistical analyses, the collected data from the students were entered into Microsoft Excel. Double data entry was done, and the consistency of the entered data was cross-checked by comparing the two separately entered data entries on Epi-Data. Data were cleaned and entered into Epi-Data version 3.0.2 and exported to the Statistical Package for Social Sciences (SPSS) version 25 for statistical analyses. Descriptive and analytical analyses were performed. Statistical parameters such as means, frequency, and percentage were employed for descriptive analysis. In analytical analyses, bivariate logistic regression was applied to identify factors associated with RSB among the students. All significant predictors were exported to multivariate logistic regression models to obtain the significantly associated variables with respect to 95% confidence interval, and p < 0.05 were considered statistical significant.
Ethics
All procedures applied in the study involving human participants were in agreement with the guidelines and regulations established in the Declaration of Helsinki 1964 and its later amendments or comparable ethical standards (21). Ethical clearance was sought from the committee of the Institutional Review Board (IRB), College of Medicine and Health Sciences of the University of Rwanda (No. CMHS/IRB/415/2019). Participants aged more than 18 years provided written consent. Students aged less than 18 years provided their consent to participate, and their parents or legal guardians provided written and signed informed consent forms. Confidentiality and voluntariness were secured and treated anonymously.
Results
Demographic characteristics of the respondents
The mean and standard deviation (SD) for the age of enrolled students were 17.39 and 1.11 years, respectively. The majority (185, 70.34%) of the respondents were in the age range of 17–18 years. The majority (n = 179, 68.1%) of the respondents were boys, and a higher number of the respondents were from grade 6 or grade 12 (n = 94, 35.7%). Our findings showed that most of the respondents had their mothers with university studies (n = 106, 40.3%) and this is similar to the education of their fathers (n = 103, 39.16%). More than half (n = 147, 55.9%) studied while spending time at school (or boarding), and only 144 respondents (43.4%) were substance users. Of 263 respondents, 117 respondents (44.5%) experienced domestic violence and 174 respondents (66.16%) were influenced by their peers to engage in sexual behaviors (Table 1).

Table 1. Descriptive characteristics of the students (N = 263).
Proportion of sexual intercourse practices among young students
Our findings indicated that 41% (n = 109) of our respondents were engaged in RSB, and these behaviors could expose them to sexual and reproductive health problems. Further, the proportion of respondents engaged in RSB was 0.47 or 47% among boys and 0.3 or 30% among girls (Figure 2).
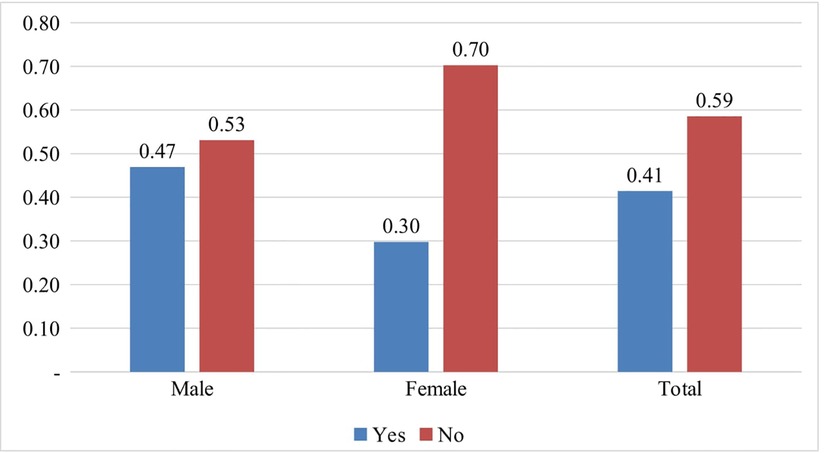
Figure 2. Prevalence in engagement in risky sexual behaviors among the students.
Risky sexual behaviors among study participants from secondary schools
Our results indicated that the majority (n = 77, 70.64%) of the students engaged in RSB were aged 17–18 years. Most (n = 84, 77.06%) of the students engaged in risky sexual behaviors were boys. A higher proportion of the students engaged in risky sexual behaviors was those who resided in Kigali (n = 70, 64.22%). Regarding the mode of the study, our results showed that a majority (n = 74, n = 67.89%) of the respondents engaged in risky sexual behaviors were students not enrolled in boarding. The incidence of RSB was higher in substance users (n = 68, 79.82%) than nonsubstance users. Concerning parents’ education, our results demonstrated that the students whose mothers had secondary (n = 48, 44.12%) and university (n = 47, 43.12%) studies had a greater prevalence of experiencing RSB than the other groups. For living arrangements, high prevalence (n = 80, 73.39%) of risky sexual behaviors was found in those who lived with one or both parents. A higher occurrence of RSB was found in students who experienced peer influence (n = 89, 81.56%) than those who did not. The prevalence of experiencing risky sexual behaviors was higher in students who did not get opportunities to communicate with their parents or guardians (n = 78, 71.56%) than those who communicated with their parents about these behaviors. Moreover, bivariate analysis found that students having ever had sex is associated with gender, study mode, religion, study mode, living arrangements, education of the parents, peer influence, domestic violence, communication about the RSB, and substance use, and these factors were significantly associated with RSB among the students (Table 2).

Table 2. Proportion of risky behavior practices by demographic characteristics and predictors associated with risky sexual intercourse among students.
Multivariate logistic regression models for assessing the factors associated with RSB among students of secondary school
In multivariable logistic regression analyses, the gender of the student, year of education, domestic violence, type of schooling, parental education, drinking alcohol, religion, peer pressure, lack of communication between parents and children about sexual issues, and poor parental monitoring were factors significantly associated with RSB among secondary school students in the study area. Girls were roughly four times more likely to engage in risky sexual behaviors [odds ratio (OR) = 3.73; 95% confidence interval (CI): 1.6–7.84] than boys. Respondents who experienced domestic violence had greater odds to experience RSB (OR = 4.22; 95% CI: 1.6–11.23) than their counterparts. Those in grade 11 (OR = 2.68; 95% CI: 1.06–6.78) and grade 12 (OR = 4.39; 95% CI: 1.82–10.56) were more likely to encounter RSB than those in grade 10. The likelihood of being at RSB among female students who consumed alcohol was seven times higher than those who did not consume alcohol (OR = 3.9; 95% CI: 1.97–5.5). Regarding religion, Muslims were less likely to experience RSB (OR = 0.09; 95% CI: 0.01–0.63) than Catholics. Those whose fathers had formal education were less likely to engage in RSB (OR = 0.54; 95% CI: 0.3–0.97) than those whose fathers had no formal education. Also, those whose fathers had primary education were less likely to experience RSB (OR = 0.12; 95% CI: 0.1–0.31) than those fathers no formal education. Students whose mothers had secondary education were five times more likely to experience RSB (OR = 5.1, 95% CI: 1.54–16.8) than those whose mothers had no formal education. Further, students who lived away from their parents had more likelihood of experiencing RSB (OR = 2.5; 95% CI: 1.14–4.42) than those living with one or both genetic parents. Those who were under peer pressure influence were about four times more likely to engage in RSB (OR = 3.9; 95% CI: 2.01–7.51) than their counterparts. The students who did not have opportunities to communicate on the SRH issues with their parents or guardians in the last year were more likely to engage in RSB (OR = 0.81; 95% CI: 0.7–0.98) than their counterparts (Table 3).

Table 3. Factors associated with RSB among sexually active school students in Kigali, Rwanda.
Discussion
This study determined the prevalence of RSB and its associated factors among high school students from College Saint André. Our results revealed that 41% of respondents were engaged in RSB. Our results are in agreement with the previous studies conducted in SSA countries, such as Ethiopia and Kenya, where the prevalence varies between 40% and 50% (22). Among the students with risky sexual behaviors, 39.45% had unprotected sexual intercourse. These results collaborated with previous studies that the students exposed to risky sexual behaviors do not use contraceptive methods, which may lead to sexual and reproductive health problems (23, 24).
Moreover, girls were more likely to experience RSB in secondary schools. Our results are in harmony with the previous studies conducted in Tanzania, Nigeria, and South Africa and in contrast to the result of a study conducted in Ethiopia (12, 16, 25). Interestingly, the students who faced peer pressure are more likely experience RSB, which is in line with previous studies in Ethiopia, South Africa, and Assela (7, 12, 26), and this might be due to their need to share life experiences with their peers. These results contradicted the previous study carried out in Addis Ababa that documented no significant association with peer influences, which might be due to the self-efficacy of the students toward external forces (27). In congruence with previous studies (28), another notable finding of our study is that substance users were more prone to experience risky sexual behaviors than their counterparts. These behaviors associated with RSB might put young people at risk for HIV, STDs, and early pregnancies (in girls). These findings are similar to those of previous studies conducted in Thailand, Kenya, Ethiopia, Nigeria, and Tanzania (26, 29–31).
Our results indicated that the students whose families are in the third Ubudehe category had greater odds of experiencing risky sexual behaviors. This was because the adolescents from the third category are children of citizens who were gainfully employed, employers of laborers, small farmers with subsistence farming, or owners of small- and medium-scale businesses. Our results are in collaboration with prior studies that conveyed that students from rich families had greater risks of experiencing risky sexual behaviors (24, 32). Our results also conflict with prior studies that conveyed that students from wealthy families have fewer odds of experiencing risky sexual behaviors (7, 27). Thus, material satisfaction and the economic class of the family contribute significantly to RSB among young students. These findings are relevant to prior studies that reported that poverty and economic depravity, in particular, are the risk factors for RSB and premarital sexual practices among young people, especially girls (23, 33). In agreement with previous studies conducted in SSA countries that indicated students living with their parents and experiencing domestic violence had a greater risk of being engaged in RSB than their counterparts (6, 12, 34), our study revealed that living without biological parents or experiencing domestic violence are associated with an increased prevalence of RSB. This was because the students who do not live with their genetic parents also do not get sexual and reproductive health education and easily experience a lack of coparenting and parental monitoring. Practicing RSB for the studies might be due to experiencing a lack of parenting or poor parenting or parental monitoring as well as psychosocial effects associated with domestic violence and the absence of the parents (35, 36).
In addition, the students who experienced peer pressure were more likely to have had sexual intercourse than their counterparts. Our results are consistent with preceding studies (12, 28, 37). The students whose parents had high education and university studies were less likely to experience RSB than their counterparts. These results are supported by previous studies (9, 12, 31). Besides, the nonboarding students were more engaged in RSB than the boarding students. Our results challenged previous studies that agreed that boarding students were more engaged in RSB than nonresidents because the boarding school environment provides greater freedom and, consequently, perhaps more permissive sexual attitude (38). The reason for our results is that the school has school leaders who are in charge of discipline and they effectively communicate with the parents and guardians to improve the behaviors of the students.
Limitations and future directions
Although this study expands and builds on the current literature with the associated factors of RSB and its impact on young adults, the authors encountered several shortcomings that need to be further considered. The study had a small sample size where it targeted only students from one secondary school, which may not be generalized to all students of all national schools. Indeed, the study was limited to participants from a secondary school from an urban area and may not be representative of all young adults out of school in the area that need attention when generalizing the findings to other young adults, particularly teenagers. Second, as the findings from the present study are based on the cross-sectional data, causal relationships could not be inferred and the results should be taken with caution. It is in that regard the longitudinal study design is recommended to determine the causal relationships. Additional work using a large sample is critical to investigating similar studies using qualitative methods with the aim to understand their perspectives on risky sexual practices. Further, we recommend the concurrent and longitudinal studies to survey the medication of sociodemographic and psychosocial factors of RSB using the longitudinal study design. A notable strength of the present study is that unlike previous studies it was conducted in a school; however, the previous explored the sexual reproductive health of adolescents.
Conclusion
Our study documented the considerable prevalence of RSB among young students. The lack of parental monitoring, lack of discussion between youth and their parents, religion, peer pressure, substance use, parental education, mode of study, access to media channels, gender of the child, and performance in the class were significantly associated with RSB among secondary school students. Discussion between parents or caregivers and children on sexual reproductive health and sexual practices and their harmful influence is substantial. We recommend that sexual risk prevention programmes for adolescents be designed and implemented in educational institutions; additionally, it is critical to strengthen family education and sexual behaviour education beginning in primary school. This is to equip youths with correct information to enable them make informed choices about responsible sexual life. There is a need to promote specific intervention programs built upon those factors that are associated with an increased likelihood for early sexual introduction and risky sexual behavior. Parents are recommended to educate their children about SRH when they are too young, and this can enrich their knowledge about sexual health and enhance their informed decision about SRH issues. As a result, our findings suggest that psychological and behavioral programs for young people be reinforced in order to address RSK behaviors.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Institutional Review Board (IRB), College of Medicine and Health Sciences of the University of Rwanda. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. The animal study was reviewed and approved by the Institutional Review Board (IRB), College of Medicine and Health Sciences of the University of Rwanda. Written informed consent was obtained from the owners for the participation of their animals in this study.
Author contributions
EN conceived and designed the study, collected data, and participated in statistical analyses. EB contributed to the conceptualization, formal analysis, interpretation of the results, and drafted the manuscript. MN has contributed to the conception, preparation of the manuscript, study design, supervision of the work, and advising the present manuscript. All authors reviewed, edited, and approved the final manuscript for submitting to the journal for publication. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors thank the study participants for their participation and for facilitating the fieldwork throughout the study time. The governmental authorities and the director of the College Saint Andre are acknowledged for authorizing this work to be conducted.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Dhawan J, Gupta S, Kumar B. Sexually transmitted diseases in children in India. Indian J Dermatol Venereol Leprol. (2010) 76(5):489–93. doi: 10.4103/0378-6323.69056
2. Arruda EPT, Brito LGO, Prandini TR, Lerri MR, Dos RR, Barcelos TMR, et al. Sexual practices during adolescence. Rev Bras Ginecole Obstet. (2020) 42(11):731–8. doi: 10.1055/s-0040-1713411
4. Kassa GM, Degu G, Yitayew M, Misganaw W, Muche M, Demelash T, et al. Risky sexual behaviors and associated factors among Jiga high school and preparatory school students, Amhara Region. Ethiopia Int Sch Res Not. (2016) 2016:1–7. doi: 10.1093/imrn/rnv113
5. Kumar D, Goel N, Bakshi R, Sharma M, Ghosh A. Sexual behavior of adolescent students in Chandigarh and their perceptions regarding family life education. J Fam Med Prim Care. (2017) 6(2):399. doi: 10.4103/2249-4863.219989
6. Keto T, Tilahun A, Mamo A. Knowledge, attitude and practice towards risky sexual behaviors among secondary and preparatory students of Metu town, south western Ethiopia. BMC Public Health. (2020) 20(1):1–8. doi: 10.1186/s12889-020-09371-4
7. Li S, Huang H, Xu G, Cai Y, Huang F, Ye X. Substance use, risky sexual behaviors, and their associations in a Chinese sample of senior high school students. BMC Public Health. (2013) 13(1):295. doi: 10.1186/1471-2458-13-295
8. Alem G, Teklewoini M. Risky sexual behavior practice and associated factors among secondary and preparatory school students of Aksum town, northern Ethiopia, 2018. BMC Res Notes. (2019) 12:698. doi: 10.1186/s13104-019-4714-1
9. Arega W, Zewale T, Bogale K. Premarital sexual practice and associated factors among high school youths in Debretabor town, South Gondar zone, North West Ethiopia, 2017. BMC Res Notes [Internet]. (2019) 12(1):314. doi: 10.1186/s13104-019-4348-3
10. Jaworska N, MacQueen G. Adolescence as a unique developmental period. J Psychiatry Neurosci. (2015) 40(5):291–3. doi: 10.1503/jpn.150268
11. Mabiala Babela JR, Massamba A, Bantsimba T, Senga P. Sexual behaviour among adolescents in Brazzaville, Congo. J Gynecol Obstet Biol Reprod. (2008) 37:510–5. doi: 10.1016/j.jgyn.2007.11.033
12. Laddunuri MM. The sexual behaviour of secondary school adolescent students in Tanzania: patterns and trends. Int J Caring Sci. (2013) 6(3):472–82. Available at: http://www.internationaljournalofcaringsciences.org/docs/21.%20Madan%20Lad.pdf (Accessed on 22nd December 2022).
13. Yi S, Poudel KC, Yasuoka J, Palmer PH, Yi S, Jimba M. Role of risk and protective factors in risk sexual behaviours. BMC Public Health. (2010) 10(477):1–8. doi: 10.1186/1471-2458-10-477
14. Lanari D, Mangiavacchi L, Pasqualini M. Adolescent sexual behaviour and academic performance of Italian students. Genus. (2020) 76(1). doi: 10.1186/s41118-020-00093-4
15. Girmay A, Mariye T, Gerensea H. Early sexual debut and associated factors among secondary school students of central zone of Tigray, northern Ethiopia, 2018. Pan Afr Med J. (2019) 34:1. doi: 10.11604/pamj.2019.34.1.17139
16. Wakasa BF, Oljira L, Demena M, Regassa LD, Daga WB. Risky sexual behavior and associated factors among sexually experienced secondary school students in Guduru. Ethiopia Prev Med Rep. (2021) 23:101398. doi: 10.1016/j.pmedr.2021.101398
17. Sari DE, Rokhanawati D. The correlation between age of first dating and sexual behavior of adolescents and young adults in Indonesia. J Heal Technol Assess Midwifery. (2018) 1(1):23–8. doi: 10.31101/jhtam.441
18. Grose RG, Chen JS, Roof KA, Rachel S, Yount KM. Sexual and reproductive health outcomes of violence against women and girls in lower-income countries: a review of reviews. J Sex Res. (2021) 58(1):1–20. doi: 10.1080/00224499.2019.1707466
19. Gibbs A, Crone ET, Willan S, Mannell J. The inclusion of women, girls and gender equality in national strategic plans for HIV and AIDS in Southern and Eastern Africa. Glob Public Health. (2012) 7(10):1120–44. doi: 10.1080/17441692.2012.701319
20. Williams TP, Chopra V, Chikanya SR. “It isn’t that we’re prostitutes”: child protection and sexual exploitation of adolescent girls within and beyond refugee camps in Rwanda. Child Abus Negl. (2018) 86(February):158–66. doi: 10.1016/j.chiabu.2018.09.015
21. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310(20):2191–4. doi: 10.1001/jama.2013.281053
22. Babalola S, Awasum D, Quenum-Renaud B. The correlates of safe sex practices among Rwandan youth: a positive deviance approach. Afr J AIDS Res. (2002) 1(1):11–21. doi: 10.2989/16085906.2002.9626540
23. Ritchwood TD, Ford H, DeCoster J, Sutton M, Lochman JE. Risky sexual behavior and substance use among adolescents: a meta-analysis. Child Youth Serv Rev. (2016) 137(32):10160–3. doi: 10.1016/j.childyouth.2015.03.005
24. Duru CB, Emelumadu OF, Iwu AC, Ohanle I, Agunwa CC, Nwaigbo E, et al. Socio-demographic determinants of family planning service utilization among women of reproductive age in urban communities of Imo State, Nigeria. OALib. 2018;05(05):1–21. doi: 10.4236/oalib.1104627
25. Masatu MC, Kazaura M, Ndeki S, Mwampambe R. Predictors of risky sexual behavior among adolescents in Tanzania. AIDS Behav. (2007) 13(1):94–9. doi: 10.1007/s10461-007-9292-x
26. Zuma K, Setswe G, Ketye Y, Mzolo T, Rehle T, Mbelle N. Age at sexual debut: a determinant of multiple partnership among South African youth. Afr J Reprod Heal. (2010) 14(2):47–54. PMID: 21243918
27. Mclaughlin C, Kaplan V. Risky business: The effect of family income on teen risky sexual behavior. Durham, North Carolina, United States: Duke University (2008). p. 1–31. Available at: http://econ.duke.edu/uploads/media_items/kaplan-mclaughlin-2.original.pdf. (Accessed on November 22, 2022)
28. Noll M, Noll PRES, Tiggemann CL, Custodio DC, Silveira EA. Health-risk behavior differences between boarding and non-resident students: Brazilian adolescent national school health survey. Arch Public Health. (2020) 78(1):1–9. doi: 10.1186/s13690-019-0383-8
29. Durowade KA, Babatunde OA, Omokanye LO, Elegbede OE, Ayodele LM, Adewoye KR, et al. Early sexual debut: prevalence and risk factors among secondary school students. Afr Health Sci. (2017) 17(3):614–22. doi: 10.4314/ahs.v17i3.3
30. Liu A, Kilmarx P, Jenkins RA, Manopaiboon C, Mock PA, Jeeyapunt S, et al. Sexual initiation, substance use, and sexual behavior and knowledge among vocational students in northern Thailand. Int Fam Plan Perspect. (2006) 32(3):126–35. doi: 10.1363/3212606
31. Odii A, Atama CS, Igwe I, Idemili-Aronu NJ, Onyeneho NG. Risky sexual behaviours among adolescent undergraduate students in Nigeria: does social context of early adolescence matter? Pan Afr Med J. (2020) 37(188):1–11. doi: 10.11604/pamj.2020.37.188.22968
32. Kobulsky J, Cederbaum J, Wildfeuer R, Grest C, Clarke L, Kordic T. Comparing the prevalence of sexual behaviors and victimization among adolescents based on child welfare system involvement. Child Abus Negl [Internet]. (2022) 134:105883. doi: 10.1016/j.chiabu.2022.105883
33. Amoateng A, Kalule-Sabiti I, Arkaah Y. The effect of socio-demographic factors on risky-sexual behaviours of adolescents in the north west province of South Africa. Afr Popul Stud. (2014) 28(1):487–98. doi: 10.11564/28-1-502
34. Gemechu AG, Ayana LA, Waqtole ZD, Tola EK, Beyene MD. Risky sexual behavior and its associated factors among daily laborers in Arjo-Didessa sugar factory, Jimma Arjo, Southwest Ethiopia: An institution-based cross-sectional study. SAGE Open Med [Internet]. (2021) 15(9):2050312121994358. doi: 10.1177/20503121219943
35. Capuano S, Simeone S, Scaravilli G, Raimondo D, Balbi C. Sexual behaviour among Italian adolescents: knowledge and use of contraceptives. Eur J Contracept Reprod Heal Care [Internet]. (2009) 14(4):285–9. doi: 10.1080/13625180902926920
36. Mukanyangezi MF, Manzi O, Tobin G, Rulisa S, Bienvenu E, Giglio D. Sexual risk behaviour in a cohort of HIV-negative and HIV-positive Rwandan women. Epidemiol Infect. (2019) 147:e54. doi: 10.1017/S0950268818003023
37. Abebe M, Tsion A, Netsanet F. Living with parents and risky sexual behaviors among preparatory school students in Jimma zone, South west Ethiopia. Afr Health Sci. (2013) 13(2):498–506. doi: 10.4314/ahs.v13i2.42
Keywords: school-based interventions, risk factors, sexual health, sexual behavior, unprotected sex/barebacking
Citation: Ndagijimana E, Biracyaza E and Nzayirambaho M (2023) Risky sexual behaviors and their associated factors within high school students from Collège Saint André in Kigali, Rwanda: An institution-based cross-sectional study. Front. Reprod. Health 5:1029465. doi: 10.3389/frph.2023.1029465
Received: 27 August 2022; Accepted: 27 January 2023;
Published: 3 March 2023.
Edited by:
Narges Sheikhansari, University of Exeter, United KingdomReviewed by:
Bang-on Thepthien, ASEAN Institute for Health Development, ThailandTafadzwa Dzinamarira, University of Rwanda, Rwanda
© 2023 Ndagijimana, Biracyaza and Nzayirambaho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Emmanuel Biracyaza YmlyYWN5YXphZW1tYXVzQGdtYWlsLmNvbQ== Emmanuel Ndagijimana bmRhZ2lqZW1tYW51ZWwyMDE3QGdtYWlsLmNvbQ==
Specialty Section: This article was submitted to Reproductive Epidemiology, a section of the journal Frontiers in Reproductive Health