
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Reprod. Health , 04 November 2022
Sec. HIV and STIs
Volume 4 - 2022 | https://doi.org/10.3389/frph.2022.993916
This article is part of the Research Topic Insights in HIV and STIs: 2021 View all 5 articles
 Josée Uwamariya1*
Josée Uwamariya1* Marcel Nshunguyabahizi1Jean Népomuscène Nshimyumuremyi1Gerardine Mukesharurema1Emmanuel Ndayishimiye1Innocent Kamali1Jean d’Amour Ndahimana1Bethany Hedt-Gauthier2
Marcel Nshunguyabahizi1Jean Népomuscène Nshimyumuremyi1Gerardine Mukesharurema1Emmanuel Ndayishimiye1Innocent Kamali1Jean d’Amour Ndahimana1Bethany Hedt-Gauthier2 Vincent K. Cubaka1
Vincent K. Cubaka1 Dale A. Barnhart1,2
Dale A. Barnhart1,2
Introduction: In sub-Saharan Africa, youth living with HIV, especially those who have lost one or both parents, face economic, socially and psychological challenges that hinder adherence to ART, ultimately leading to poor health outcomes. Partners In Health/Inshuti Mu Buzima implemented an Adolescent Support Group (ASG) to support HIV-positive youth aged 15–25 years. During the evaluation of the ASG program, we sought to better understand youths' lived experiences to improve our delivery of HIV care.
Methods: We conducted qualitative in-depth, semi-structured individual interviews with youth enrolled in the ASG program. All interviews were conducted in-person or by telephone. Thematic analysis applying the framework approach with parallel inductive coding in Kinyarwanda and English was used.
Results: We interviewed 35 youth who ranged in age from 16 to 29 years. The main themes related to the lived experiences of youth were (a) Experiences living with HIV, including disclosure, stigma, interactions with the health care system, and medication adherence; (b) external challenges, defined as challenges that were not related to the implementation of the ASG program; and (c) personal vision. Almost all youth reported acquiring HIV from their mothers and disclosure of HIV status occurred around the age of 10. Disclosure was often unintentional and followed by internalized and enacted stigma. Many reported poor past medication adherence which improved following enhanced counselling. External challenges were overwhelmingly economic in nature, and orphanhood was a root cause of other challenges such as difficulty accessing education, lack of transport to health facility, and lack of insurance fees. Despite these challenges, youth have an optimistic view of the future with dreams of health, economic attainment, marriage, and children.
Conclusion: Healthcare providers should empower caregivers to support HIV disclosure. Supporting youth as they face many economic challenges could help address socio-economic barriers to good health and promote holistic well-being.
In 2019, approximately 3,4 million youth between the ages of 15 and 24 years were living with HIV globally (1). These youth are less likely than older adults to get tested for HIV, to adhere to treatment plan and to be retained in care (2). Worldwide, HIV mortality reduced by 39% in all age categories from 2010 to 2019, however the prevalence rise by almost 25% among youth (3). Youth living with HIV are susceptible to social stigma, anxiety regarding the future, insufficient social support, and have a fear of HIV status disclosure, leading to profound experiences of internalized stigma (4). Ultimately, these dynamics often lead to poor health, including poor HIV-related outcomes, such as poor adherence to treatment plan, high viral loads, and high loss to follow-up, as well as poor mental health outcomes, including depression, lack of self-acceptance, and low self-esteem (5).
However, youth's clinical outcomes can vary based on contextual factors. In Africa, where HIV is the fifth leading cause of death among male youths and second among female youth (1), recognized contextual factors hindering good health among youth with HIV include living in extended families where children have less privacy to take medication; long distances to health facilities and lack of resources for transportation; limited availability of healthcare providers trained in delivering youth-friendly services, and ineffective disclosure leading to poor psychological outcomes (6, 7). Rwanda has made great strides in promoting widespread access to ART and improving the quality of HIV services to ensure that patients have improved adherence and retention (8). However, adherence is still a documented challenge among adolescents aged 10 to 17, partly due to psychological symptoms such as depression (9). Many of these challenges likely persist among older youth.
To better support youth living with HIV, Partners In Health/Inshuti Mu Buzima (PIH/IMB) implemented Adolescent Support Groups (ASGs), a complex intervention that included both peer support groups and group-based economic incentives, in health facilities in rural Rwanda. Despite its name, this program did not only target adolescents and was instead designed to support youth 15–25. In the mixed-methods evaluation of this program, the clinical benefits were not statistically significant, although the youth members identified many non-clinical benefits and suggested many key areas for improvement (3, 10). However, during interviews with youth members, we also identified several key themes that were not specific to youths' experiences in the ASG program but provided more general insights into their experiences as young people living with HIV in rural Rwanda. This paper explores the ASG members' lived experiences, with a focus on their experiences living with HIV, challenges they face, and their personal vision. By better understanding these experiences, we hope to identify ways to improve delivery of HIV care for children and youth.
This is an explorative qualitative study using in-depth, semi-structured individual interviews with youth enrolled in the ASG program.
In Rwanda, 84% of young people between the ages of 15–24 are literate (11). HIV prevalence remains stable around 3% in the general population and 1% among youth (12). In Rwanda, 85,6% of the population is insured by community based health insurance (CBHI), also known as mutuelle de santé (13). CBHI members pay a contribution of 3$ per year, however poor families' contribution is covered by the government and employees contribute 0.5% of their monthly net salary to the CBHI scheme (14). The community based health insurance (CBHI) policy and the provision of HIV treatment free of charge to all to positive people had increased the accessibility to HIV testing, diagnosis and treatment (15).
The ASG program was implemented in 34 rural health facilities in Burera, Kayonza and Kirehe districts, Rwanda. These health centers are supported by PIH/IMB, an international non-governmental organization that supports health system strengthening through collaborations that include constructing and staffing of hospitals and increasing access to HIV and TB treatment since 2005. PIH/IMB supports the HIV program of the three districts through mentorship of HIV nurses at primary health facilities and provision of transportation fees to help some HIV patients keep their appointments. In Rwanda, HIV care and treatment services are provided in 96% of all health facilities (16). Since 2016, ART has been prescribed to every HIV positive patients regardless of their CD4 count and pharmacy visits are currently scheduled monthly for new patients and every six month for patients >15 years who have been on ART for at least 18 months, demonstrated good adherence, and achieved viral load suppression (17).
The ASG program was designed and implemented by PIH/IMB in collaboration with health care providers at participating primary-level health facilities. The program was first launched in Kayonza in July 2017 and was scaled up to Burera and Kirehe in July 2018. Healthcare providers in charge of the HIV program were requested to select 10 to 15 economically vulnerable youth aged 15–24 years old to participate in the ASG program, giving a particular attention to orphans and school dropouts. The ASG program combines peer support and economic empowerment; the peer support aspect of the program involves organized monthly nurse-facilitated meetings where all group members convened and discussed medication adherence and social economic challenges. The economic empowerment aspect of the program involves providing incentives to the group based on the achievement of predefined three main indicators: (1) quarterly pharmacy visit attendance, (2) biannual achieving group savings targets and (3) annual viral suppression.
Interviewed participants were youth living with HIV who had participated in an ASG. Youth were purposively sampled from over-performing ASGs, under-performing ASGs, or from among ASG dropouts, where group performance was evaluated retrospectively using data from an electronic medical record (EMR) system (10).
Between June and early July 2021, interviews were conducted in-person and scheduled to coincide with regular ASG meetings and to avoid interrupting youth's usual daily activities. During the meeting, trained data collectors explained the purpose of the study and asked group members aged 15 years or older to voluntarily participate in one-on-one interviews anticipated to last between 45 min to 60 min. In each group, a maximum of three members were selected to participate in the interviews. If more than three members volunteered, we randomly selected three members by drawing slips of paper out of a container. Selected participants provided written consent and were immediately interviewed in a private room at the clinic. Data collectors used an interview guide that was designed based on a review of the literature and in collaboration with the PIH/IMB staff who implemented the ASG project.
After July, cross-district travel in Rwanda was restricted due to a surge of COVID-19, so we shifted to conducting telephone-based interviews. During telephone-based data collection, nurses' in charge of HIV at each health center provided our data collection team with phone numbers of ASG members or ASG dropouts. We generated a random calling order for each ASG group as well as for ASG dropouts and data collectors contacted the top three members by phone to explain the study and invite them to participate. If interested, we scheduled one-on-one phone interviews and the interviewee provided oral consent prior to the interview. All interviews were conducted in Kinyarwanda and audio-recorded.
All interviews were transcribed and translated into English. A thematic analysis applying the framework approach was carried out (18). The research team, which included three native Rwandans who had conducted the interviews and one native English speaker (an American epidemiologist living in Rwanda), conducted all coding. No member of the research team had been involved in the implementation of the ASG or the youths' clinical care. We constructed a codebook using inductive parallel coding where each interview was independently coded by two coders, one using the Kinyarwanda transcript and the other using the English translations (19). Identified codes were discussed and harmonized during two full-team meetings, one occurring after the end of in-person data collection and the second occurring after the end of all data collection. After a codebook was developed, two team members conducted deductive coding on the English translations and made final revisions to the codebook as needed. Key demographic data was extracted in youth interviews to Excel to report medians, ranges or percent. The analysis process was facilitated by MAXQDA 2020 Software (20).
This study received approval from Inshuti Mu Buzima Research Committee (IMBRC), Rwanda National Ethics Committee (NO. 150/RNEC/2020) and Harvard University approvals (IRB20-0565). Informed consent were obtained for all adolescents who participated in the study. The ethic committees waived the requirement for caregiver consent for adolescents below 18 years old to avoid involuntary disclosure of adolescents' HIV status.
In total, we interviewed 35 participants. Seventeen interviews were conducted in-person and 18 over the telephone. The median age of respondents was 20 years (range: 16 to 29) and 20 (57%) were male. The main themes identified during the inductive coding that was linked to the lived experience of youth were (a) Experience living with HIV, (b) External challenges and (c) Personal vision.
Subthemes explored within the main theme of experiences living with HIV included disclosure of HIV status, stigma, interaction with health systems, and medication adherence. Illustrative quotes are provided for each of these subthemes in Table 1. Although almost all youths reported acquiring HIV from their mothers, the median age at disclosure was 10 years. Some participants reported that their HIV status was disclosed to them by caregivers, but often only after youths persistently asked why they must take medications. Other youths had simply observed their parents' taking medication and gradually understood. In these cases, youth often felt lied to and resented that their parents had not told them the truth (Quote 1.1.1; 1.1.2). Many others reported that they learned their HIV status from health care workers during group meetings at the health center. These meetings were designed to provide counselling about medication adherence without providing specific support for status disclosure (Quote 1.1.3). A few participants had learned of their HIV status through voluntary testing either during community HIV screening or at the health center following diseases recurrence (Quote 1.1.4; 1.1.5).

Table 1. Sub-themes and illustrative quotes from the main theme, “Experiences living with HIV”.
HIV disclosure was often followed by enacted stigma within families and communities. Youths reported being isolated and mistreated once the community became aware of their HIV status (Quote 1.2.1). This enacted stigma resulted in internalized stigma, where youths hated themselves, leading to poor mental health outcomes, including hopelessness, self-reported depression and suicidal ideation (Quote 1.2.2). Internalized stigma also led to a lack of self-acceptance (Quote 1.2.3). Although many youths reported that they have grown to accept their HIV status, they still said that HIV status is a personal secret that needs to be protected and often did not feel comfortable taking medication in front of others (Quote 1.2.4). Similarly, in our interviews they avoided describing themselves as people living with HIV, instead saying things like they “live with this problem” (Quote 1.2.5).
Though ASG members have experienced enacted and internalized stigma, their interactions with the health system were generally positive. Youths mentioned that the health centers consider them to be valuable stakeholders and involve them in different youth-related projects (Quote 1.3.1). Many youths emphasized good relationships with their nurses and felt comfortable discussing their treatment plan as well as medication related challenges (Quote 1.3.2; 1.3.3). Youths appreciated the timely service that they receive and recognized that they do not experience shortages of medication (Quote 1.3.4). The good relationship with nurses and timely service motivated youth to develop healthier behaviors including appointment keeping and medication adherence.
Many youths reported that their medication adherence had been bad in the past and that they used to skip medication doses and miss medical appointment as a result of lack of self-acceptance or fear of people seeing them at the HIV clinic (Quote 1.4.1). Some youth also simply forgot to take medication. Generally, education on the importance of medication adherence had improved their adherence and currently they take their medications as prescribed (Quote 1.4.2, 1.4.3). Although the current adherence situation had generally improved, youth reported that it was still very hard to take ARV medication when they have an empty stomach because it induces side effects (Quote 1.4.4). Other facilitators of medication adherence included multi-month prescriptions (Quote 1.4.5) and parental support (Quote 1.4.6).
External challenges, defined as challenges that were not related to the implementation of the ASG program, were overwhelmingly economic in nature (Table 2). They included orphanhood, difficulty accessing education, unstable housing, family conflict, supporting impoverished family members, food insecurity, lack of transport to health facilities, and lack of insurance fees. The majority of the interviewed youth had lost one or both parents. Orphanhood was a major root cause of socio-economic challenges, causing some youth to live alone and provide for themselves financially (Quote 2.1.1; 2.1.2).
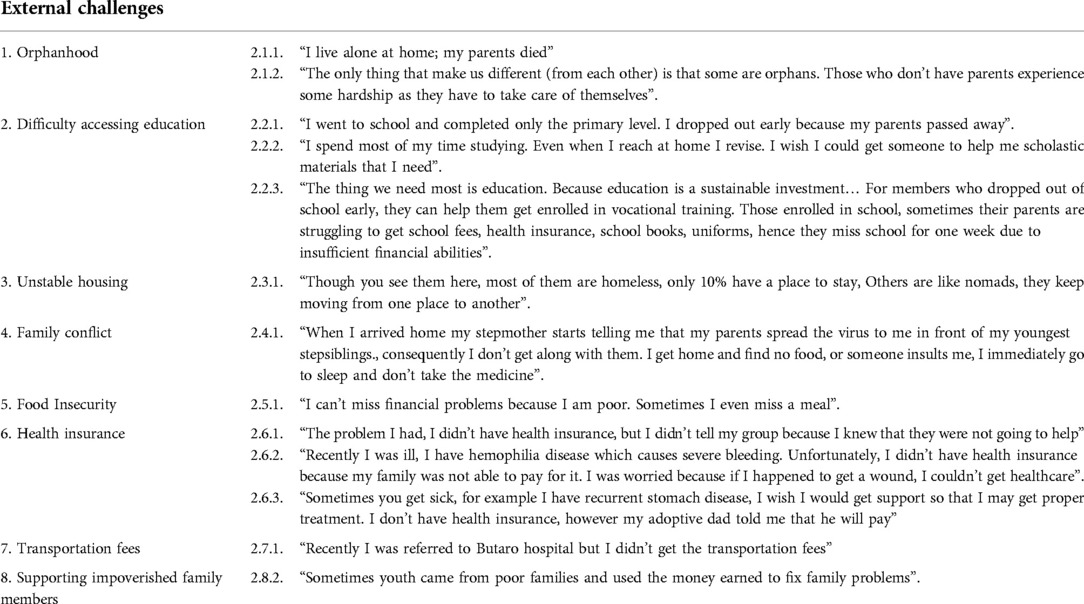
Table 2. Sub-themes and illustrative quotes from the main theme, “external challenges”.
Orphanhood was also associated with difficulty accessing education. Only few interviewed youths were still enrolled in school, with the majority having dropped out of primary school, and few others having dropped out of secondary school. Youth reported dropping out of school following the death of their parents because it was hard to get school fees or access other scholastic materials such as uniforms and books (Quote 2.2.1). Even youth who were still enrolled in school reported challenges accessing school fees and scholastic materials (Quote 2.2.2). Many youths recognized access to education as a sustainable investment and explicitly requested support to continue formal education or enroll in vocational training (Quote 2.2.3).
Many youths reported being homeless or living in unstable housing due to an inability to pay rent (Quote 2.3.1). Some youths with stable housing reported being in direct conflict with their caretakers, which consequently contributed to poor adherence to medication (Quote 2.4.1). Food insecurity was an additional challenge to youth, and this insecurity sometimes impacted their adherence (Quote 2.5.1). Youth coming from such extremely poor families reported having difficulty accessing health insurance and transportation fees, which affected their ability to seek care for both HIV and for other health issues (Quote 2.6.1; 2.6.2; 2.6.3; 2.7.1) Although youth often reported to experiencing economic hardships, they were also sometimes responsible for supporting impoverished families themselves (Quote 2.8.1).
Youths' personal vision for the future was optimistic and positive (Table 3). Their long-term vision demonstrated that they no longer perceived HIV as a death sentence but instead as a chronic, manageable conditions that was compatible with a fulfilling life and dreams and goals. Many youths wish to develop economically, have stable jobs, and improve their health, with a particular focus on attaining an undetectable viral load (Quote 3.1; 3.2). Many youths want to invest in their education and become experts in their chosen careers (Quote 3.3) while others want to create their own business and generate income (Quote 3.4). Youth wanted to be financially independent not just to improve their own lives but also to impact lives of people in their community through providing support in career development (Quote 3.5). Besides their professional and career goals, many youths reported that they want to get married and build families (Quote 3.6).
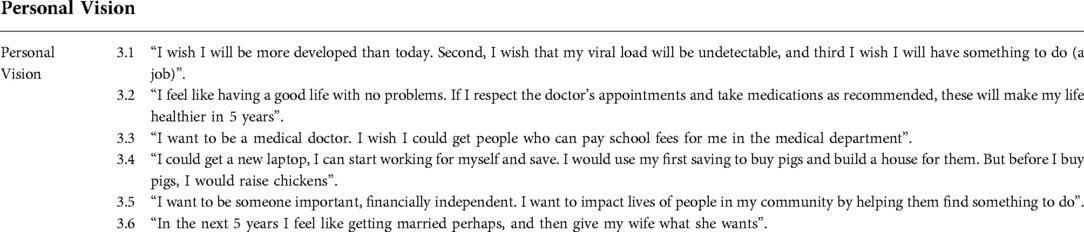
Table 3. Illustrative quotes from the main theme, “personal vision”.
Our qualitative interviews among youth living with HIV in rural Rwanda revealed complex interactions between early negative experiences with HIV, poverty, and poor medication adherence. At the same time, our findings suggest that support and education from health care professionals can help youth understand the importance of medication adherence and to reframe HIV as a manageable chronic condition.
Many of our participants reported delayed disclosure of HIV status and expressed that disclosure did not occur in a private, age-appropriate manner. Appropriate disclosure of HIV has positive clinical and psychological benefits that promote the quality of life including improved adherence, viral load suppression, self-acceptance, and self-esteem (21). Currently, the WHO recommends that school age children and younger children should be informed of their HIV status incrementally to accommodate their psychological maturity while preparing them for full disclosure (22). The current Rwanda guideline on disclosure recommends that school age children from 7 years old should be notified of their HIV status in presence of their caretakers after a carefully cognitive and psychological assessment (17). However, HIV-positive caregivers are frequently reluctant to disclose their own HIV status to their children due to fear of negative consequences as well as due to worries that the child will be unable to understand and accept their diagnosis or will disclose the family's HIV status to others (23). Interventions aiming at empowering caregivers to effectively disclose HIV to perinatally infected youth should take into consideration beliefs and cultural factors in order to develop an intervention tailored specifically to that population (23).
Although most of the youth reported good adherence at the time of our interviews, they also described prior episodes of poor adherence, usually as a result of lack of self-acceptance or fear of discrimination. A similar patterns of HIV disclosure being followed by depression, isolation, and medication cessation have been reported elsewhere in East Africa (5). Periods of non-adherence to ART can lead to opportunistic infections, development of ART-resistant virus, and to progression to AIDS (24). Even if youth begin to adhere ART appropriately at a later date, these earlier periods of non-adherence could led to drug resistance and potentially explain the very high prevalence of drug resistance among Rwandan youth (25) as well as the low prevalence of viral load suppression among ASG members (26). Currently, the WHO recommends that people with high viral load count should receive 3–6 months enhanced adherence counseling (EAC) sessions before diagnosing virological treatment failure (27). However, for perinatally infected youth who may have historically had poor adherence but currently report appropriate treatment adherence, more proactive monitoring for ART resistance may be warranted.
Our study identified that many interviewed youths had lost one or both parents. As has been reported elsewhere, perinatally infected youth are especially likely to live in extreme poverty due to orphanhood of one or both parents (5), which can prevent them from accessing medical treatment for HIV though free of charge (28), cause them to drop out of school (29), and caust them to struggle to afford healthy food and stable housing (30). In 2010, Rwanda endorsed a policy to shut down all orphanages. Since then, Rwandan orphans were placed with their extended families or in foster families. In general, living with extended families likely provides an improved safety net for orphans and vulnerable children. However, for orphans living with HIV in these circumstances may also force the youth to face challenges surrounding disclosure, stigmatization, and inability to take medication due to poor perception of HIV among their extended families (31). Health care providers should be aware that, although extended family placements could make it less obvious which Rwandan children living with HIV are orphans, these orphaned children still constitute a particularly vulnerable population in need of economic and emotional support.
Despite these challenges, our study revealed that the youth perceived that the HIV services provided by the health center were high-quality, and reported that good relationship with their healthcare providers helped them to develop ownership over their treatment journey, ultimately resulting in improved adherence to treatment and retention in care. Previously evidence has similarly shown that patient satisfaction among patients living with HIV lead to improved health outcomes, including adherence to ART and retention to care (32) and that good relationships between the healthcare providers and HIV-positive patients yields improved patients' quality of life, self-esteem and adherence (33).
This study does have several limitations. Our primary limitation is that all interviews were conducted among ASG participants, who may not be representative of all HIV-positive youth in rural Rwanda. In particular, these youths may have more positive views of the health care system, better medication adherence, or improved future orientation compared to youth who did not received a comparable intervention. Similarly, interviewed youth were 15 years of age or older, and their childhood experiences may not reflect the current experience of HIV-positive children, especially as targeted training around disclosure of HIV status to children had been implemented in Rwanda in 2008 when our study participants would have been aged between 2 and 16 years. Additionally, we transitioned to telephone-based interviews due to a surge during the COVID 19 pandemic, so the poorest ASG members who lacked access to mobile phones may have been excluded from some interviews. Finally, there was a possibility of social desirability bias where respondents may have underreported socially undesirable behaviors and over reported desirable attributes because the interviewing team were from the organization that supports HIV care in the respondents' health centers and the implementation of the ASG project.
Despite these limitations, our results highlight several challenges experienced by youths living with HIV and suggest a number of avenues to better support these youths. First, training healthcare providers to empower caregivers to appropriate disclosure HIV status to perinatally infected youth is a critical step for ensuring that children with HIV are prepared for success in their adolescence and beyond. Second, framing HIV as a manageable chronic condition and educating young people on the benefits of medication from an early age may help motivate youth to adhere, leading to better long-term health outcomes. Third, clinicians should recognize that perinatally infected youth could have developed antiviral resistance from prior periods of non-adherence, even if their current adherence is good, and should provide appropriate, compassionate counselling. Fourth, intentionally tracking adolescents' orphanhood status as part of their medical records and providing emotional and economic support is warranted, even when the child has been placed with an extended family. Providing these orphaned youths with community based-accompaniment, which has been previously demonstrated to improve health outcomes and mental health among adult HIV patients in Rwanda (34), may be one concrete strategy to ensure that the youth is receiving appropriate support from an adult. In order to address these issues in a systematic and sustainable manner, the government may also consider appointing an official to oversee outcomes among youth with HIV and implement improved training for health care providers providing HIV care that reinforces appropriate disclosure strategies, provides health education messaging for children and youth with HIV, and investigates a revision of drug resistance testing policies for perinatally-infected youth.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Rwanda National Ethics Committee. Written informed consent for participation was not provided by the participants’ legal guardians/next of kin because: the ethics committee waived the requirement for caregiver consent for adolescents below 18 years old to avoid involuntary disclosure of adolescents' HIV status.
DAB, VKC, and BHG conceptualized this study. JU, MN, and EN conducted, transcribed, and translated interviews. JU, DAB, MN, and EN coded and analyzed the data. JU drafted the initial manuscript and DB reviewed the manuscript. All authors contributed to the article and approved the submitted version.
We are very grateful to the youth who participated in the interviews. We are also grateful to the health center nurses, who supported the ASG program and facilitated our research.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. UNAIDS. Young people and HIV. New York City, USA: UNAIDS (2021). 20 p. https://www.unaids.org/en/resources/documents/2021/young-people-and-hiv
2. Ryscavage PA, Anderson EJ, Sutton SH, Reddy S, Taiwo B. Clinical outcomes of adolescents and young adults in adult HIV care. JAIDS J Acquir Immune Defic Syndr. (2011) 58(2):193–7. doi: 10.1097/QAI.0B013E31822D7564
3. Nshimyumuremyi JN, Mukesharurema G, Uwamariya J, Mutunge E, Goodman AS, Ndahimana Jd, et al. Implementation and adaptation of a combined economic empowerment and peer support program among youth living with HIV in rural Rwanda. J Int Assoc Provid AIDS Care. (2022) 21:232595822110640. doi: 10.1177/23259582211064038
4. Wolf HT, Halpern-Felsher BL, Bukusi EA, Agot KE, Cohen CR, Auerswald CL. ‘It is all about the fear of being discriminated (Against)…The person suffering from HIV will not be accepted’: a qualitative study exploring the reasons for loss to follow-up among HIV-positive youth in Kisumu, Kenya. BMC Public Health. (2014) 14(1):1154. doi: 10.1186/1471-2458-14-1154
5. Kimera E, Vindevogel S, Kintu MJ, Rubaihayo J, De Maeyer J, Reynaert D, et al. Experiences and perceptions of youth living with HIV in western Uganda on school attendance: barriers and facilitators. BMC Public Health. (2020) 20(1):79. doi: 10.1186/s12889-020-8198-7
6. MacCarthy S, Saya U, Samba C, Birungi J, Okoboi S, Linnemayr S. ‘How am I going to live?’: exploring barriers to ART adherence among adolescents and young adults living with HIV in Uganda. BMC Public Health. (2018) 18(1):1158. doi: 10.1186/s12889-018-6048-7
7. Ndayishimiye P, Uwase R, Kubwimana I, Niyonzima JdlC, Dine RD, Nyandwi JB, et al. Availability, accessibility, and quality of adolescent sexual and reproductive health (SRH) services in urban health facilities of Rwanda: a survey among social and healthcare providers. BMC Health Serv Res. (2020) 20(1):697. doi: 10.1186/s12913-020-05556-0
8. Nkiko D, Peterson J, Miller L, Morris M, Mukaminega M, van Zyl C. Improving quality of HIV services in Rwanda: The elizabeth glaser pediatric AIDS foundation experience. Kigali, Rwanda: Elisabeth Glaser Pediatric AIDS Foundation (2015). https://www.pedaids.org/wp-content/uploads/2017/11/ImprovingQualityofHIVservicesRwanda.pdf
9. Smith Fawzi MC, Ng L, Kanyanganzi F, Kirk C, Bizimana J, Cyamatare F, et al. Mental health and antiretroviral adherence among youth living with HIV in Rwanda. Pediatrics. (2016) 138(4):e20153235. doi: 10.1542/peds.2015-3235
10. Barnhart D, Uwamariya J, Nshimyumuremyi JN, Mukesharurema G, Anderson T, Ndahimana JD, et al. “Today I know who I want to be”: perspectives on a peer support and group-based economic incentives program for Rwandan youth living with HIV. Submitted. (2022).
11. National Institute of Statistics of Rwanda. Fourth population and house census, Rwanda. Kigali, Rwanda: National Instutute of Statistics of Rwanda (2012). https://www.statistics.gov.rw/publication/population-rwanda-results-4th-census-2012
12. Rwanda Population based HIV impact. Rwanda population based impact. Kigali, Rwanda: International Centre for AIDS Care and Treatment (2019). https://phia.icap.columbia.edu/wp-content/uploads/2019/10/RPHIA-Summary-Sheet_Oct-2019.pdf
13. Hakiba H. USAID Rwanda integrated health system.pdf. Kigali, Rwanda: Rwanda Integrated Health System (2022). https://pdf.usaid.gov/pdf_docs/PA00ZFC9.pdf
14. UNDP. An ongoing process. In: Ruberangeyo T, Ayebare C, de Bex AdL, editors. Sharing innovative experiences: Successful social protection floor. New York, USA: International Labour Organization (2011). https://www.social-protection.org/gimi/gess/ShowRessource.action?ressource.ressourceId=20840
15. Zeng W, Rwiyereka AK, Amico PR, Ávila-Figueroa C, Shepard DS. Efficiency of HIV/AIDS health centers and effect of community-based health insurance and performance-based financing on HIV/AIDS service delivery in Rwanda. Am J Trop Med Hyg. (2014) 90(4):740–6. doi: 10.4269/ajtmh.12-0697
16. Rwanda Biomedical Center. National strategic plan 2018–2024. Kigali, Rwanda: Rwanda Biomedical Center (2018). https://rbc.gov.rw/fileadmin/user_upload/stra2019/strategie2019/Rwanda%20Strategic%20Plan%20for%20HIV%20Extended%20to%202020.pdf
17. Rwanda Biomedical Center. National guidelines for prevention and management of HIV and STIs, edition 2016. Kigali, Rwanda: Rwanda Biomedical Center (2016). 176 p. http://rbc.gov.rw/fileadmin/user_upload/guide/SIGNED%20ENGLISH%20%202016%20VERSION.pdf
18. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. (2013) 13(1):117. doi: 10.1186/1471-2288-13-117
19. van Nes F, Abma T, Jonsson H, Deeg D. Language differences in qualitative research: is meaning lost in translation? Eur J Ageing. (2010) 7(4):313–6. doi: 10.1007/s10433-010-0168-y
20. VERBI Software. MAXQDA 2020 (computer software). Berlin, Germany: VERBI Software (2019). Available at: maxqda.com.
21. Hayfron-Benjamin A, Obiri-Yeboah D, Ayisi-Addo S, Siakwa PM, Mupepi S. HIV Diagnosis disclosure to infected children and adolescents; challenges of family caregivers in the central region of Ghana. BMC Pediatr. (2018) 18(1):365. doi: 10.1186/s12887-018-1330-5
22. Gyamfi E, Okyere P, Enoch A, Appiah-Brempong E. Prevalence of, and barriers to the disclosure of HIV status to infected children and adolescents in a district of Ghana. BMC Int Health Hum Rights. (2017) 17(1):8. doi: 10.1186/s12914-017-0114-6
23. Heeren GA, Jemmott JB 3rd, Sidloyi L, Ngwane Z. Disclosure of HIV diagnosis to HIV-infected children in South Africa: focus groups for intervention development. Vulnerable Child Youth Stud. (2012) 7(1):47–54. doi: 10.1080/17450128.2012.656733
24. Rudy BJ, Murphy DA, Harris DR, Muenz L, Ellen J. Patient-Related risks for nonadherence to antiretroviral therapy among HIV-infected youth in the United States: a study of prevalence and interactions. AIDS Patient Care STDS. (2009) 23(3):185–94. doi: 10.1089/apc.2008.0162
25. Ndahimana Jd, Riedel DJ, Mwumvaneza M, Sebuhoro D, Uwimbabazi JD, Kubwimana M, et al. Drug resistance mutations after the first 12 months on antiretroviral therapy and determinants of virological failure in Rwanda. Trop Med Int Health. (2016) 21(7):928–35. doi: 10.1111/tmi.12717
26. Barnhart D, Nshimyumuremyi JN, Mukesharurema G, Anderson T, Ndahimana Jd, Vincent K, Cubaka VK, et al. Receipt of a combined economic and peer support intervention and clinical outcomes among HIV-positive youth in rural Rwanda: A retrospective cohort. San Francisco, USA: Plos Global Public Health (2022). https://journals.plos.org/globalpublichealth/article?id=10.1371/journal.pgph.0000492
27. Diress G, Dagne S, Alemnew B, Adane S, Addisu A. Viral load suppression after enhanced adherence counseling and its predictors among high viral load HIV seropositive people in north wollo zone public hospitals, Northeast Ethiopia, 2019: retrospective cohort study. AIDS Res Treat. (2020) 2020:1–9. doi: 10.1155/2020/8909232
28. Bermudez LG, Ssewamala FM, Neilands TB, Lu L, Jennings L, Nakigozi G, et al. Does economic strengthening improve viral suppression among adolescents living with HIV? Results from a cluster randomized trial in Uganda. AIDS Behav. (2018) 22(11):3763–72. doi: 10.1007/s10461-018-2173-7
29. Pufall EL, Nyamukapa C, Robertson L, Mushore PG, Takaruza A, Gregson S. Migration as a risk factor for school dropout amongst children made vulnerable by HIV/AIDS: a prospective study in eastern Zimbabwe. Vulnerable Child Youth Stud. (2015) 10(3):179–91. doi: 10.1080/17450128.2015.1034799
30. Marfatia Y, Naswa S. Adolescent HIV/AIDS: issues and challenges. Indian J Sex Transm Dis. (2010) 31(1):1. doi: 10.4103/0253-7184.68993
31. Mutiso DN, Mutie DPM. Challenges affecting orphans and vulnerable children (OVCS) in Embu County. Int J Sociol. (2018) 1(1):18–36.
32. Dang BN, Westbrook RA, Black WC, Rodriguez-Barradas MC, Giordano TP. Examining the link between patient satisfaction and adherence to HIV care: a structural equation model. PLoS One. (2013) 8(1):e54729. doi: 10.1371/journal.pone.0054729
33. Dean Wantland W-TC. Engagement with health care providers affects self- efficacy, self-esteem, medication adherence and quality of life in people living with HIV. J AIDS Clin Res. (2013) 04(01):3. doi: 10.4172/2155-6113.1000256
Keywords: HIV, youth, HIV status disclosure, orphans and vulnerable children, Rwanda
Citation: Uwamariya J, Nshunguyabahizi M, Nshimyumuremyi JN, Mukesharurema G, Ndayishimiye E, Kamali I, Ndahimana Jd, Hedt-Gauthier B, Cubaka VK and Barnhart DA (2022) Rediscovering life after being diagnosed with HIV: A qualitative analysis of lived experiences of youth living with HIV in rural Rwanda. Front. Reprod. Health 4:993916. doi: 10.3389/frph.2022.993916
Received: 14 July 2022; Accepted: 6 October 2022;
Published: 4 November 2022.
Edited by:
Elizabeth Bukusi, Kenya Medical Research Institute (KEMRI), KenyaReviewed by:
Pamela Abbott, University of Aberdeen, United Kingdom© 2022 Uwamariya, Nshunguyabahizi, Nshimyumuremyi, Mukesharurema, Ndayishimiye, Kamali, Ndahimana, Hedt-Gauthier, Cubaka and Barnhart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josee Uwamariya am9zZWV1d2FAeWFob28uY29t
Specialty Section: This article was submitted to HIV and STIs, a section of the journal Frontiers in Reproductive Health
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.