 Ying Meng
Ying Meng Gui H. Wen
Gui H. Wen Hong Luo
Hong Luo Xiu C. Tan
Xiu C. Tan
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Reprod. Health , 04 November 2022
Sec. Assisted Reproduction
Volume 4 - 2022 | https://doi.org/10.3389/frph.2022.1032062
This article is part of the Research Topic Reviews in Assisted Reproduction: 2022 View all 6 articles
Objective: The aim of this study was to evaluate six vaginal douching agents (Iodine, Saline, Iodine followed by saline, chlorhexidine acetate followed by saline, Ozone, Potassium permanganate) on oocytes pick-up related pelvic infection (OPU-PI) and IVF outcome in patients underwent assisted reproduction technology (ART).
Design: Through searching PubMed, Embase, Cochrane Library, Web of Science, Ovid, CINAHL CNKI, only human clinical trials were collected to study the effects of the six vaginal douching agents on OPU-PI and IVF outcomes. The included studies were evaluated for methodological quality by the Cochrane bias risk assessment tool, and the data analysis software was used to analyze the data accordingly.
Results: The clinical trials were collected between the earliest available date and June 2022. Eight studies were included, the total sample size used in the study was 12,567. The results of the network meta-analysis showed that Ozone can significantly decrease OPU-PI; Iodine followed by saline can be a antiseptic protocol ranked first without affecting the quality of oocytes and Chlorhexidine acetate followed by saline can improve patients' clinical pregnancy rate.
Conclusion: Based on Ranking Plot of the Network, this review reports the best evidence available regarding different vaginal douching agents used before OPU.
Infertility is common, with recent publications quoting a 9% to 18% prevalence in the general population (1). Approximately 12.7% of reproductive age women seek treatment for infertility each year (2), many of whom will ultimately require assisted reproductive technology (ART). Ultrasound-guided oocyte retrieval is an essential part of ART. Even though oocyte retrieval is seen as a safe and efficient procedure, it is considered a process that potentially occur surgery- or infection-related complications (3). The incidence of oocyte pick-up related pelvic infection (OPU-PI) has been reported as 0.02% by the European Society of Human Reproduction and Embryology data, other studies report an incidence rate of up to 0.3–1.5% (4, 5). It is widely agreed that pre-operative vaginal preparation cannot rule out the infection in all cases because every imaginable effort is made to minimize the risk of pelvic infections (6). However, the use of antiseptic solutions on vaginal douching before OPU in ART is controversial. Two major concerns regarding the use of antiseptic solutions in patients actively undergoing OPU with in vitro fertilization (IVF) are benefits for reducing complications related to OPU and the toxicity impact on quality of oocytes (7, 8).
A recent study showed that preoperative vaginal douching with distilled water led to a significantly higher rate of postoperative infection than did preoperative vaginal irrigation with Iodine (9). However, some douching agents were confirmed associated with epithelial disruption and inflammation, and may reduce the anti-inflammatory effects of beneficial lactobacilli (10). It is therefore particularly important to find a vaginal douching product used before OPU with effectiveness against infections and whether it affects IVF outcome should be considered.
There is no uniform standard of vaginal preparation before OPU, different vaginal douching agents were used in different countries/regions. Network meta-analysis is a technique that uses direct or indirect comparisons to compare the effects of multiple interventions on a disease and to estimate the rank order of each treatment (11). Therefore, in this study we used network meta-analysis to compare different vaginal preparation (Iodine, saline, Iodine followed by saline, chlorhexidine acetate followed by saline, potassium permanganate and ozone) in order to assess the effect of these agents on OPU-PI and IVF outcome and to provide patients and clinicians with a better advice about the effects of these vaginal irrigation agents. The aim is to evaluate the effects of these vaginal douching agents on OPU-PI and IVF outcome and to provide evidence-based recommendations for patients and clinicians.
This systematic review and network meta-analyses are reported according to the PRISMA statement guidelines. The review was registered with the PROSPERO database (Registration number: CRD42022306779).
The researchers searched seven electronic databases (Pubmed, EMBASE, Cochrane Central Register of Controlled Trials, Web of Science, CINAHL, Ovid and CNKI) from their creation to 30 June 2022. The search strategy was constructed around the PICOS tool: (P) Population: patients need vaginal prep before oocyte retrieval in IVF-ET; (I) Intervention: using Iodine to wash the vagina before oocyte retrieval; (C) Comparator: using other vaginal irrigation agents to wash the vagina; (O) Outcomes: OPU-PI and IVF outcome (including fertilization rate and clinical pregnancy rate). (S) Study type: human clinical trials. The detailed search strategy is shown in Table 1 (Pubmed is used as an example).
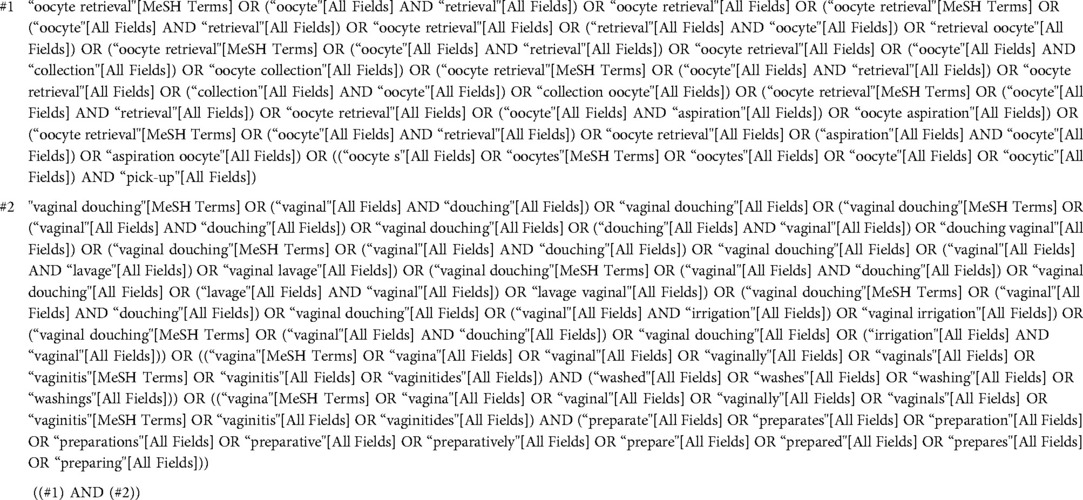
Table 1. Search strategy on pubmed.
(1) Experimental group with iodine used to wash the vagina as an intervention for patients need vaginal prep before oocyte retrieval. (2) Control group with other vaginal douching agents used to wash the vagina before oocyte retrieval. (3) Human clinical trials. (4) Outcome indicators including at least one of the following: OPU-PI and IVF outcome (including number of oocytes, fertilization rate, clinical pregnancy rate).
(1) Studies with incomplete or unreported data (2) Studies from non-trials [including systematic reviews, animal studies, protocols, conference abstracts, case reports or meta-analysis.
The literature was screened and excluded using the literature management soft-ware Endnote X9. Two researchers first screened the titles of the literature for duplication, non-trial studies, review papers, conference papers, protocols and meta-analysis. The abstracts of the literature were then read by two researchers to identify literature for inclusion and to exclude literature. Finally, the remaining literature was read in full by both researchers and further identified for inclusion. During this process, both researchers independently screened the literature and finally compared the remaining literature, if it was the same then it was finally included, if it was different then it was discussed and resolved by a third researcher.
A eight-item, standardized and pre-selected data extraction form was used to record data for inclusion in the study under the following headings: (1) author, (2) year of publication, (3) country, (4) population, (5) sample size, (6) details of the intervention, and (7) outcome (Table 2).
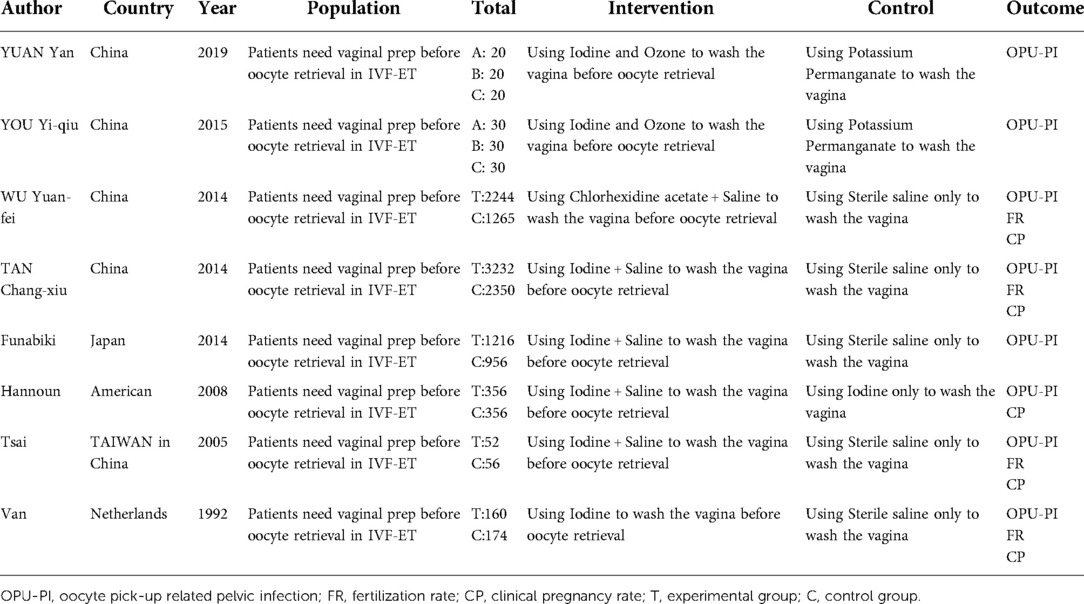
Table 2. Characteristics of the studies included in the meta-analysis.
Two researchers independently assessed the risk of bias (ROB), in accordance with the Cochrane Handbook version 5.1.0 tool for assessing ROB in RCTs. The following domains were included: (1) randomized sequence generation, (2) treatment allocation concealment, blinding of (3) participants and (4) personnel, (5) incomplete outcome data, (6) selective reporting and (7) other sources of bias. Trials were categorized into three levels of ROB: high risk (five or more components of high ROB potentially existed), moderate risk (three or four components of high ROB potentially existed) and low risk (two or less components of high ROB potentially existed) (12).
We used Stata software (version 15.1) and performed NMA aggregation and analysis using Markov chain Monte Carlo simulation chains in a Bayesian-based framework according to the PRISMA NMA instruction manual (13). We will use the nodal method to quantify and demonstrate the agreement between indirect and direct comparisons, calculated through the instructions in the Stata software, and if the P-value > 0.05. the consistency test passes (14).
Stata software is used to present and describe network diagrams of different movement interventions. In the generated network diagrams, each node represents a different motor intervention and a different control condition, and the lines connecting the nodes represent direct head-to-head comparisons between interventions. The size of each node and the width of the connecting lines are proportional to the number of studies (15). All variables in this study are categorical variables and are expressed as odds ratios (OR) with 95% confidence intervals (CI) and analysis. As there are certainly potential differences across studies, we chose a random effects model for analysis rather than a fixed effects model (16).
A total of 231 documents were retrieved from the electronic database, and an additional 6 documents were manually searched. After eliminating duplicates, the remaining 152 documents were read for titles and abstracts, and 137 documents were again excluded. The remaining 15 documents were read in full and 7 documents were again excluded (for reasons including: not a clinical trial, no vaginal douching were done, other outcomes evaluated and full-text unavailable), leaving a final remaining 8 documents to be included in this study (Figure 1).
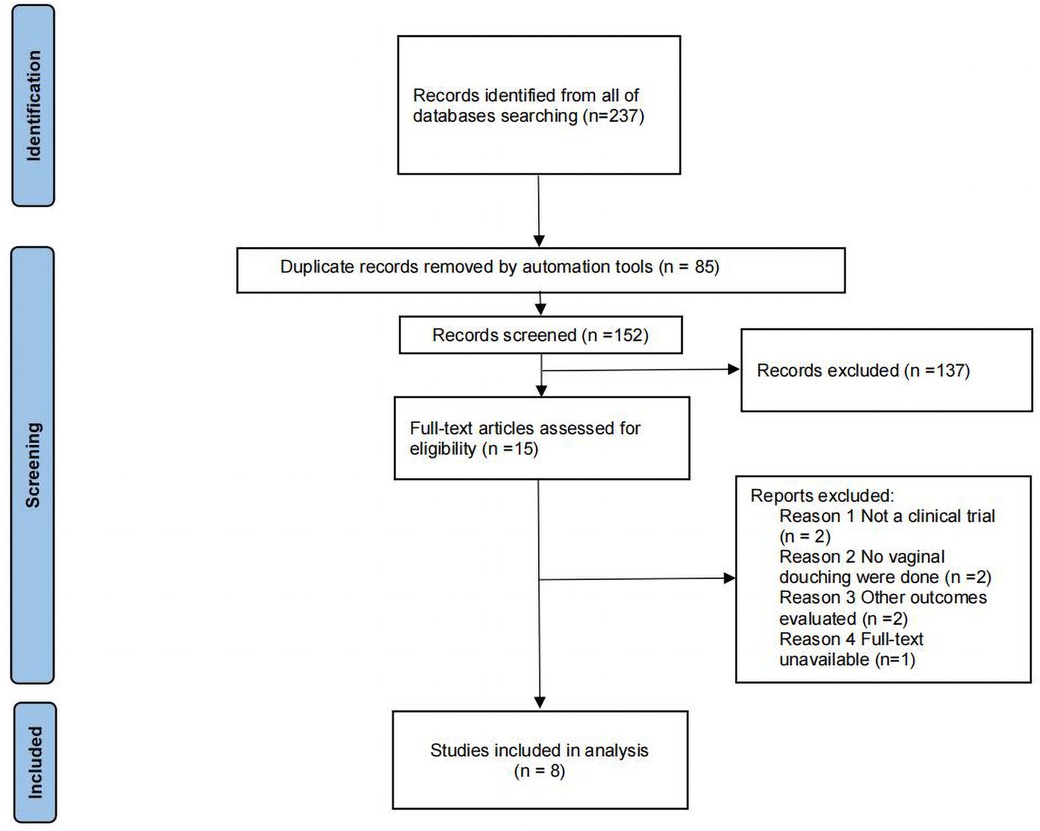
Figure 1. Flow diagram of literature selection.
All of the included studies were defined as low risk and simultaneously achieved avoiding selection bias and attrition bias, but as the intervention in these studies was vaginal douching, it was difficult to achieve simultaneous blinding of subjects and measurers as both the patients themselves and their relatives had to sign an informed consent form before the experiment was conducted. Specific details will be presented in Figures 2, 3.
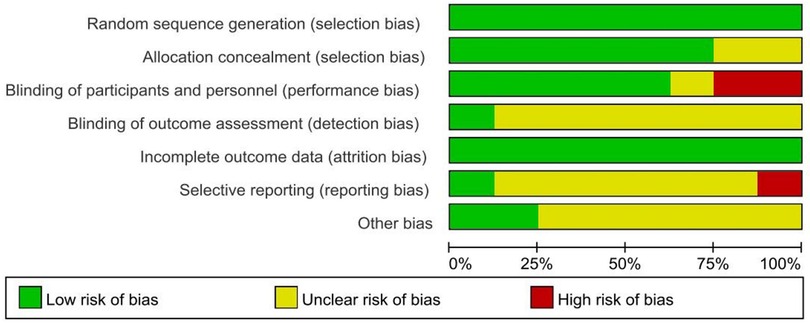
Figure 2. Risk of bias graph.
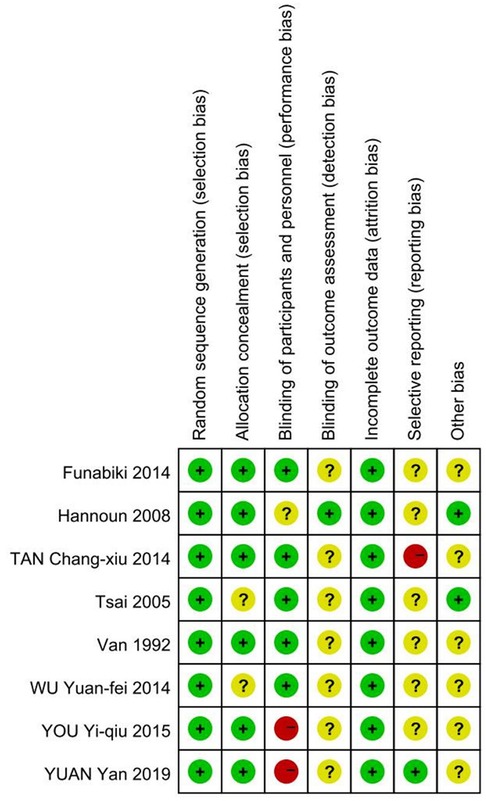
Figure 3. Risk of bias summary.
In total, we included studies from 8 clinical trials, which included 12,567 patients need vaginal prep before oocyte retrieval in IVF-ET. The vaginal douching agents in intervention groups included Ozone (2 studies) (17, 18), Iodine only (3 studies) (17–19), Iodine followed by saline(4 studies) (20–23) and Chlorhexidine acetate followed by saline (24). Interventions in the control group included using Potassium Permanganate (2 studies) (17, 18), sterile saline (5 studies) (19–21, 23, 24), iodine (1 study) (22) to wash the vagina before OPU. All of the studies reported OPU-PI as an outcome indicator, 5 studies reported clinical pregnancy rate as an outcome indicator and 4 studies reported fertilization rate as an outcome indicator. There were 5 studies from China and other 3 studies were from America, Japan and Netherlands, respectively. The characteristics of the included studies are shown in Table 2.
The full NMA figure will be shown in Figures 4A, 5A, 6A.
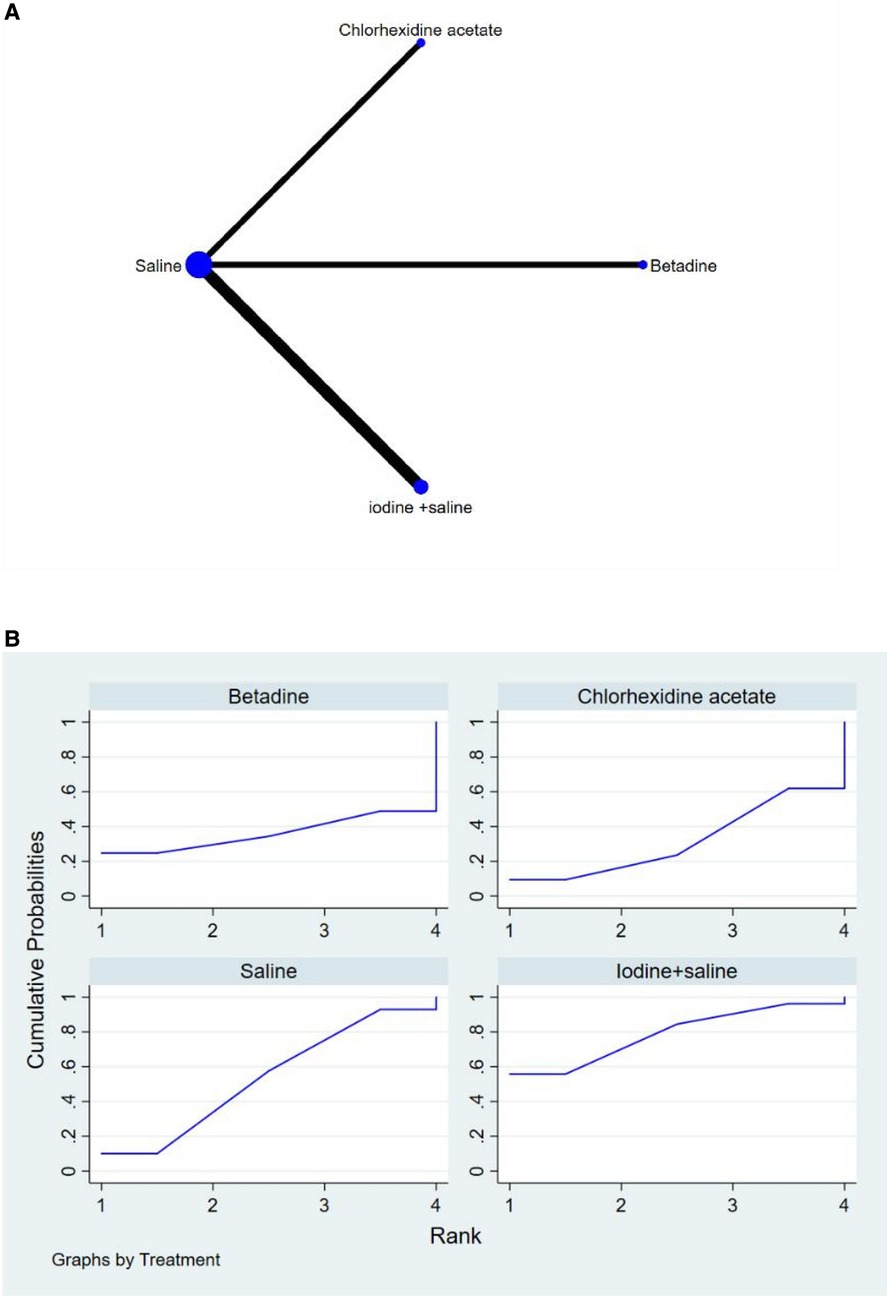
Figure 4. (A) NMA figure for FR (B) SUCRA plot for FR.
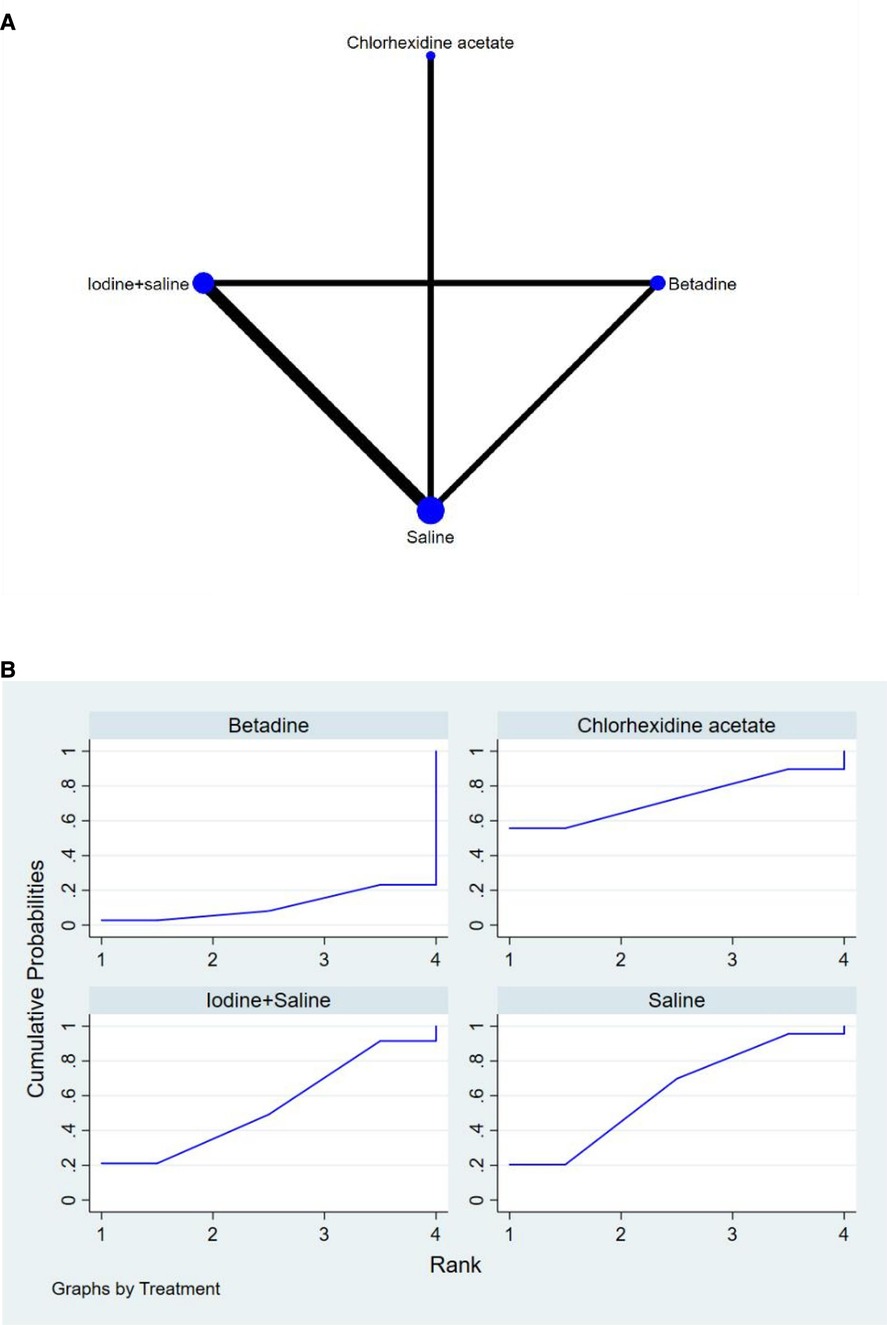
Figure 5. (A) NMA figure for CP (B) SUCRA plot for CP.
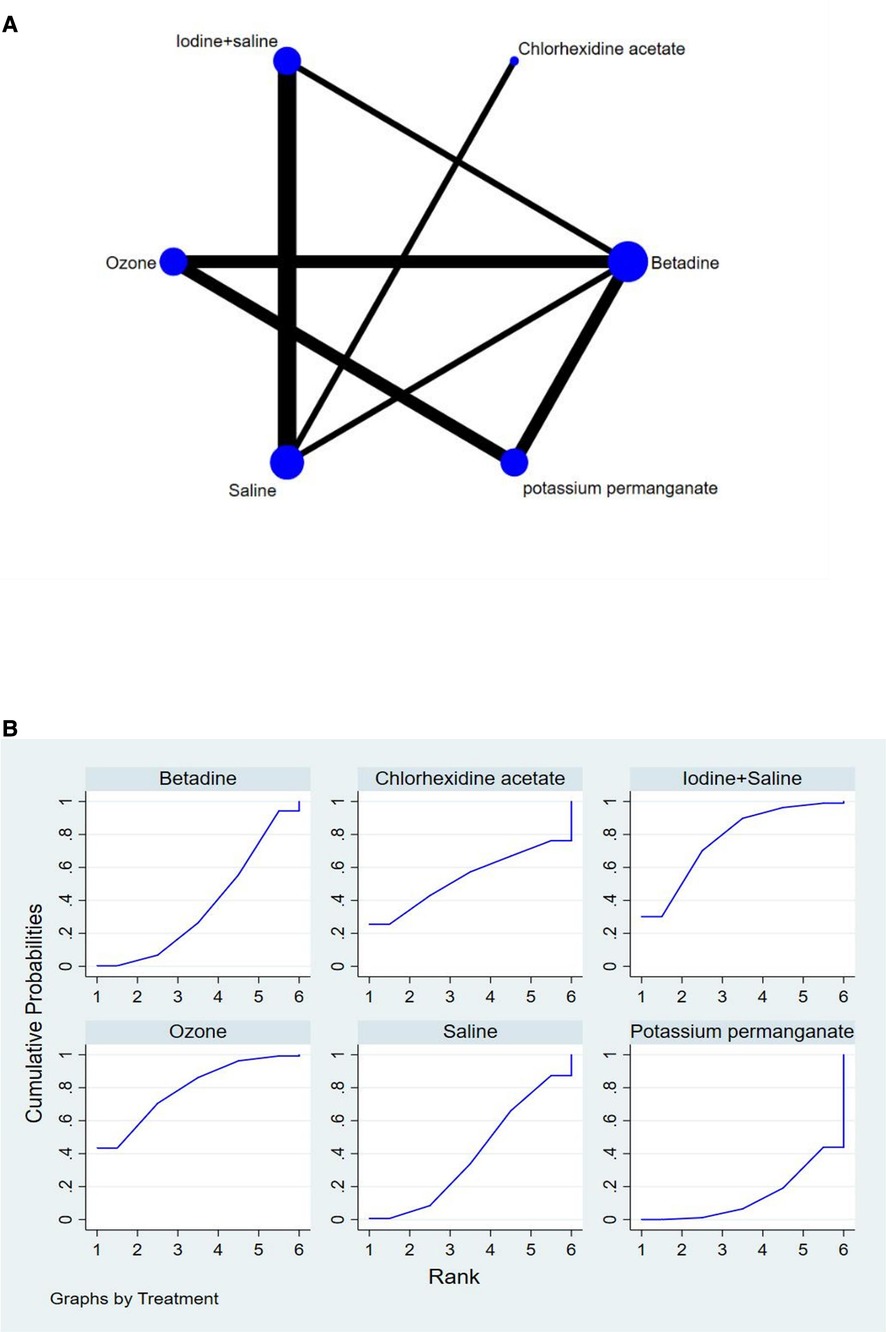
Figure 6. (A) NMA figure for OPU-PI (B) SUCRA plot for OPU-PI.
All P-values for indirect and direct comparisons between all studies were tested for consistency and inconsistency, and all P-values were greater than 0.05, indicating that the effect of consistency between studies was acceptable.
The results of the Network meta-analysis showed that relative to the 4 different vaginal douching agents, Betadine, Chlorhexidine acetate followed by saline, Saline, Iodine followed by saline. The probability ranking of the different vaginal douching agents in terms of improving fertilization rate was ranked first in the SUCRA for Iodine followed by saline (SUCRA was shown in Figure 4B). A comparison between the two different interventions will be shown in Table 3.
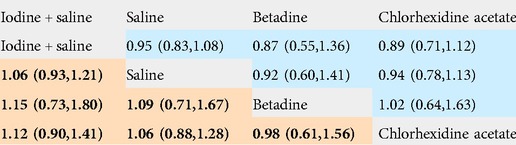
Table 3. League table on FR.
All P-values for indirect and direct comparisons between all studies were tested for consistency and inconsistency, and all p-values were greater than 0.05, indicating that the effect of consistency between studies was acceptable.
The results of the network meta-analysis showed that relative to the 4 different vaginal douching agents, Betadine, Chlorhexidine acetate followed by saline, Saline, Iodine followed by saline. The probability ranking of the different vaginal douching agents in terms of improving clinical pregnancy rate was ranked first in the SUCRA for Chlorhexidine acetate followed by saline (SUCRA was shown in Figure 5B). A comparison between the two different interventions will be shown in Table 4.
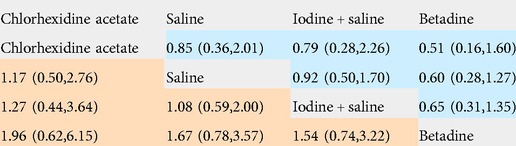
Table 4. League table on CP.
All P-values for indirect and direct comparisons between all studies were tested for consistency and inconsistency, and all p-values were greater than 0.05, indicating that the effect of consistency between studies was acceptable.
The results of the network meta-analysis showed that relative to the 6 different vaginal douching agents, Betadine, Chlorhexidine acetate followed by saline, Saline, Iodine followed by saline, Ozone [MD = 0.09, 95% CI =(0.01, 0.76)], Potassium permanganate. The probability ranking of the different vaginal douching agents in terms of reducing OPU-PI rate was ranked first in the SUCRA for Ozone (SUCRA was shown in Figure 6B). A comparison between the two different interventions will be shown in Table 5.

Table 5. League table on OPU-PI.
We constructed separate funnel plots for all outcome indicators to test for possible publication bias. Visual inspection of the funnel plots did not reveal any significant publication bias (25). Details as shown in Figure 7.
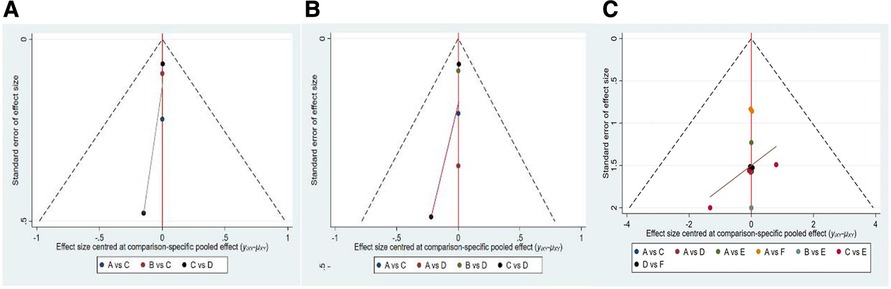
Figure 7. Funnel plot on publication bias (A) FR (B) CP (C) OPU-PI.
In this study we compared different vaginal douching agents to decrease OPU-PI and improve IVF outcome in people who need vaginal prep before oocyte retrieval. A total of 8 studies including 6 different vaginal preparation protocols were included, including 12,567 patients, which is a fairly large sample size. Our study showed that using iodine followed by sterile saline to wash vagina before OPU was the best intervention in terms of increasing fertilization rate, Chlorhexidine acetate followed by saline was the best solution in terms of increasing clinical pregnancy rate, but using Ozone to wash vagina showed better results in terms of decreasing the OPU-PI. Overall, however, we believe that there are three appropriate vaginal douching agents for ensuring the security of OPU while improving IVF outcome in patients who need IVF treatment.
As an important part of fertility treatment, OPU is generally viewed as a low-risk of procedure. Symptomatic pelvic infection following transvaginal oocyte retrieval is a rare, but serious complication (26). Cleansing of the vagina/cervix is therefore widely believed should be done prior to OPU to minimize bacterial vaginal/cervical contamination (27). Many kinds of disinfection protocols before OPU were reported but there is no evidence on the safety of those antiseptic methods, and how different vaginal douching agents may influence reproductive outcomes and post-OPU complications (28). Our results demonstrate that ozone has a statistically significant beneficial effect on the decreasing OPU-PI compared to other agents, which is consistent with the results of other animal studies (29, 30). As a highly reactive molecule, ozone is emerging as a new antifungal agent for vaginal/pelvic infection in recent years (31). One of the common causes of OPU-PI is Candida albicans, a study tested that ozone was highly effective on the yeast form of Candida albicans and it can inhibit the formation of germ tubes in Candida albicans (32). Besides Candida albicans, other clump of bacteria such as Staphylococcus aureus, Escherichia coli, and M. urealyticum that may cause the acute pelvic inflammatory disease were also confirmed sensitive to ozone (33). In addition, Merhi Z et al. found that ozone therapy could have beneficial effect on tubal occlusion, protect patients from endometritis and vaginitis, and might also protect ovaries from ischemia and oocyte loss and finally might lead to less formation of pelvic adhesions (34). Taken together, the key findings of the study present evidence that ozone may aid in decreasing the vagina flora and protect the fertility preservation of infertility patients.
In addition, fertilization rate seems to be a significantly important part of IVF outcome. Some disinfection agents previously confirmed that might act on the oocyte's cell membrane (35) and might have also been associated with epithelial toxicity (36), which can not be safe for oocytes (37), and the quality of oocytes were significant positive predictors of fertilization rate (38). Also, If there were inadequate numbers of mature oocytes are available after OPU, fertilization failure (TFF) occurs and can reoccur in subsequent cycles (39). If povidone–iodine preparations were used before OPU, the remained iodine could contaminate the aspirates and in that way damage the oocytes, or they might be imbibed by the cervical plug and thus gain access to the uterine cavity (40). Another possibility is that traces of Betadine which remain in the cervical mucus plug may be introduced into the uterine cavity with embryo transfer (41). In our study, it was shown that the fertilization rate are lower when betadine solution which is not rinsed with saline solution are employed. Iodine followed by thoroughly saline douching was the most effective agents on improving fertilization rate among the different agents included in this study. The results are the same as the original study (42). Even though the vaginal anatomy is such that traces of Iodine can remain, the results of this study attributed to the fact that all the antiseptic solution should be completely flushed away before oocyte retrieval.
The increase in the clinical pregnancy rate is difficult to explain. The increase in the clinical pregnancy rate has been attributed to the low risk of pregnancy loss rate, controlled ovarian hyperstimulation (COH) protocol, cycle type and serum hCG level 14 days after transfer (43, 44). In addition, even the unicornuate uterus could affects the clinical pregnancy rate in IVF-ET (45). Therefore, the high clinical pregnancy rate not only depends on the vaginal preparations before OPU. At the same time, we got the conclude that Chlorhexidine acetate followed by saline washing may be the most beneficial agents in improving the clinical pregnancy.
Overall our study has some clinical implications, firstly Ozone and Iodine followed by saline have a significant effect in decreasing OPU-PI without compromising the outcome of IVF treatment, and furthermore doctors can make a decision on which vaginal douching agents to use before OPU based on the data of this study.
Firstly our study included 8 studies and 12,567 patients, which is a very large sample size, and we also built on the original review on the vaginal douching agents for people who need oocyte retrieval in IVF-ET by including saline, Iodine, Iodine followed by saline, Ozone, Potassium permanganate and Chlorhexidine acetate followed by saline, which provides newer and more comprehensive evidence-based recommendations.
Secondly, our study shares some limitations with the studies on which it is based. Although we made every effort to control for study heterogeneity when including these original studies, heterogeneity between studies was unavoidable (e.g., the proportion of studies by region and between clinical characteristics).
Finally, in our study, readers should interpret the results with caution because of the small number of studies and the limited head-to-head direct comparative evidence for some interventions. It also highlights the need for further expansion of relevant studies.
In our study, Ozone is the most recommended antiseptic solution for patients who want to decrease infection rate after OPU; Iodine followed by thoroughly saline douching is the most recommended agents for patients who want to ensuring the quality of oocytes.
Overall, however, we recommended using Iodine followed by thoroughly saline washing as the antiseptic solutions for clinicians in order to decreasing OPU-PI after OPU without affecting IVF outcome.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
YM, interpreted the data and wrote the initial manuscript; JL, involved in the data analysis; LW, was responsible for the collection of all relevant papers; GHW, project development; HL, was responsible for the supervision of the study; XCT, manuscript review; NY, manuscript editing; HP, literature search; LL, data collection; YZ, literature quality assessment. All authors contributed to the article and approved the submitted version.
This research was supported by the Chongqing Science and Technology Bureau (No. cstc2017shms-zdyfX0020).
We thank all the reviewers for their assistance and support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
OPU-PI, Oocytes pick-up related pelvic infection; IVF, In vitro fertilization; ART, Assisted reproduction technology; ROB, Risk of bias; OR, Odds ratios; CI, Confidence intervals; FR, Fertilization Rate; CP, Clinical pregnancy rate; TFF, Fertilization failure; COH, Controlled ovarian hyperstimulation.
1. Hanson B, Johnstone E, Dorais J, Silver B, Peterson C, Hotaling J, et al. Female infertility, infertility-associated diagnoses, and comorbidities: a review. J Assist Reprod Genet. (2017) 34(2):167–77. doi: 10.1007/s10815-016-0836-8
2. Carson S, Kallen A. Diagnosis and management of infertility: a review. Jama. (2021) 326(1):65–76. doi: 10.1001/jama.2021.4788
3. Özaltın S, Kumbasar S, Savan K. Evaluation of complications developing during and after transvaginal ultrasound - guided oocyte retrieval. Ginekol Pol. (2018) 89(1):1–6. doi: 10.5603/GP.a2018.0001
4. Andersen A, Gianaroli L, Felberbaum R, de Mouzon J, Nygren K. Assisted reproductive technology in Europe, 2001. Results generated from European registers by ESHRE. Hum Reprod. (2005) 20(5):1158–76. doi: 10.1093/humrep/deh755
5. Levi-Setti P, Cirillo F, Scolaro V, Morenghi E, Heilbron F, Girardello D, et al. Appraisal of clinical complications after 23,827 oocyte retrievals in a large assisted reproductive technology program. Fertil Steril. (2018) 109(6):1038–43. e1. doi: 10.1016/j.fertnstert.2018.02.002
6. Bhandari H, Agrawal R, Weissman A, Shoham G, Leong M, Shoham Z, et al. Minimizing the risk of infection and bleeding at trans-vaginal ultrasound-guided ovum pick-up: results of a prospective web-based world-wide survey. J Obstet Gynecol India. (2015) 65(6):389–95. doi: 10.1007/s13224-014-0619-z
7. Simon EG, Laffon M. Maternal care after vaginal delivery and management of complications in immediate post-partum–guidelines for clinical practice. J Gynecol Obstet Biol Reprod (Paris). (2015) 44(10):1101–10. doi: 10.1016/j.jgyn.2015.09.024
8. Southern AP, Jwayyed S. Iodine toxicity. Treasure Island (FL), StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC: StatPearls (2022).
9. Yoshida T, Akitani F, Hayashi K, Shioda K. Effectiveness of 10% povidone-iodine formulation on preoperative vaginal irrigation. J Obstet Gynaecol Res. (2021) 47(3):935–40. doi: 10.1111/jog.14615
10. Hesham H, Mitchell A, Bergerat A, Hung K, Mitchell C. Impact of vaginal douching products on vaginal Lactobacillus, Escherichia coli and epithelial immune responses. Sci Rep. (2021) 11(1):23069. doi: 10.1038/s41598-021-02426-5
11. Rouse B, Chaimani A, Li T. Network meta-analysis: an introduction for clinicians. Intern Emerg Med. (2017) 12(1):103–11. doi: 10.1007/s11739-016-1583-7
12. Higgins J, Altman D, Gøtzsche P, Jüni P, Moher D, Oxman A, et al. The cochrane Collaboration's Tool for assessing risk of bias in randomised trials. Br Med J. (2011) 343:d5928. doi: 10.1136/bmj.d5928
13. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
14. Salanti G, Ades A, Ioannidis J. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. J Clin Epidemiol. (2011) 64(2):163–71. doi: 10.1016/j.jclinepi.2010.03.016
15. Chaimani A, Higgins J, Mavridis D, Spyridonos P, Salanti G. Graphical tools for network meta-analysis in STATA. PloS one. (2013) 8(10):e76654. doi: 10.1371/journal.pone.0076654
16. Jackson D, Riley R, White I. Multivariate meta-analysis: potential and promise. Stat Med. (2011) 30(20):2481–98. doi: 10.1002/sim.4172
17. Yan Y. Analysis of methods and status quo of vaginal preparation before oocyte retrieval in IVF. J Pract Gynecol Endocrinol. (2019) 6(06):103–5.
18. Yiqiu Y, Liping W, Yan C. Study on the relationship between the method of vaginal preparation before oocyte retrieval and the success rate of IVF. Mod Diagn Treat. (2015) 26(15):3470–2. Available at: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=XDZD201515074&DbName=CJFQ2015
19. van Os H, Roozenburg B, Janssen-Caspers H, Leerentveld R, Scholtes M, Zeilmaker G, et al. Vaginal disinfection with povidon iodine and the outcome of in-vitro fertilization. Hum Reprod. (1992) 7(3):349–50. doi: 10.1093/oxfordjournals.humrep.a137647
20. Changxiu T, Honggui W, Ling L. Effect of different vaginal irrigation methods on pregnancy outcomes of embryo transfer in vitro fertilization. Chin J Eugenics Genet. (2013) 21(10):119–23. doi: 10.1080/09513590802360751
21. Funabiki M, Taguchi S, Hayashi T, Tada Y, Kitaya K, Iwaki Y, et al. Vaginal preparation with povidone iodine disinfection and saline douching as a safe and effective method in prevention of oocyte pickup-associated pelvic inflammation without spoiling the reproductive outcome: evidence from a large cohort study. Clin Exp Obstet Gynecol. (2014) 41(6):689–90. doi: 10.12891/ceog18772014
22. Hannoun A, Awwad J, Zreik T, Ghaziri G, Abu-Musa A. Effect of betadine vaginal preparation during oocyte aspiration in in vitro fertilization cycles on pregnancy outcome. Gynecol Obstet Investig. (2008) 66(4):274–8. doi: 10.1159/000156378
23. Tsai Y, Lin M, Chen S, Chung M, Loo T, Huang K, et al. Vaginal disinfection with povidone iodine immediately before oocyte retrieval is effective in preventing pelvic abscess formation without compromising the outcome of IVF-ET. J Assist Reprod Genet. (2005) 22(4):173–5. doi: 10.1007/s10815-005-4915-5
24. Yuanfei W, Na Z, Xiaohong W. Selection of vaginal irrigation solution before embryo transfer and oocyte retrieval in vitro fertilization. Contemp Nurses. (2014)(10):64–5. Available at: https://kns.cnki.net/kcms/detail/detail.aspx?FileName=DDHS201410039&DbName=CJFQ2014
25. Wallace B, Schmid C, Lau J, Trikalinos T. Meta-Analyst: software for meta-analysis of binary, continuous and diagnostic data. BMC Med Res Methodol. (2009) 9:80. doi: 10.1186/1471-2288-9-80
26. El-Toukhy T, Hanna L. Pelvic infection after oocyte retrieval: a preventable complication or an inevitable risk? J Obstet Gynaecol. (2006) 26(7):701–3. doi: 10.1080/01443610600940273
27. Edelstein S, Ben Shachar I, Ben-Amram H, Biswas S, Marcus N. Assisted reproductive technology as a transcutaneous route for bacterial contamination of ovarian endometrioma with coagulase-negative Staphylococcus: case report and review of the literature. Infect Dis Obstet Gynecol. (2019) 2019:4149587. doi: 10.1155/2019/4149587
28. D'Angelo A, Panayotidis C, Amso N, Marci R, Matorras R, Onofriescu M, et al. Recommendations for good practice in ultrasound: oocyte pick up. Hum Reprod Open. (2019) 2019(4):hoz025. doi: 10.1093/hropen/hoz025.eCollection2019.
29. Zobel R, Tkalčić S, Stoković I, Pipal I, Buić V. Efficacy of ozone as a novel treatment option for urovagina in dairy cows. Reprod Domest Anim. (2012) 47(2):293–8. doi: 10.1111/j.1439-0531.2011.01857.x
30. Gautam G, Nakao T. Prevalence of urovagina and its effects on reproductive performance in Holstein cows. Theriogenology. (2009) 71(9):1451–61. doi: 10.1016/j.theriogenology.2008.12.027
31. Tara F, Zand-Kargar Z, Rajabi O, Berenji F, Akhlaghi F, Shakeri M, et al. The effects of ozonated olive oil and clotrimazole cream for treatment of vulvovaginal candidiasis. Altern Ther Health Med. (2016) 22(4):44–9. PMID: 2754849227548492
32. Zargaran M, Fatahinia M, Zarei Mahmoudabadi A. Candida albicansThe efficacy of gaseous ozone against different forms of Candida albicans. Curr Med Mycol. (2017) 3(2):26–32. doi: 10.29252/cmm.3.2.26
33. Wei A, Feng H, Jia X, Tang H, Liao Y, Li B, et al. Ozone therapy ameliorates inflammation and endometrial injury in rats with pelvic inflammatory disease. Biomed Pharmacother. (2018) 107:1418–25. doi: 10.1016/j.biopha.2018.07.137
34. Merhi Z, Garg B, Moseley-LaRue R, Moseley A, Smith A, Zhang J. Ozone therapy: a potential therapeutic adjunct for improving female reproductive health. Med Gas Res. (2019) 9(2):101–5. doi: 10.4103/2045-9912.260652
35. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Centers for disease control and prevention (CDC) hospital infection control practices advisory committee. Am J Infect Control. (1999) 27(2):97–132. quiz 3-4; discussion 96. doi: 10.1016/S0196-6553(99)70088-X
36. Hu M, Zhou T, Dezzutti CS, Rohan LC. The effect of commonly used excipients on the epithelial integrity of human cervicovaginal tissue. AIDS Res Hum Retrovir. (2016) 32(10-11):992–1004. doi: 10.1089/aid.2016.0014
37. Hershlag A, Feng HL, Scholl GS. Betadine (povidone-iodine) is toxic to murine embryogenesis. Fertil Steril. (2003) 79(5):1249–50. doi: 10.1016/S0015-0282(03)00159-6
38. Jawed S, Rehman R, Ali MA, Abdullah UH, Gul H. Fertilization rate and its determinants in intracytoplasmic sperm injection. Pak J Med Sci. (2016) 32(1):3–7. doi: 10.12669/pjms.321.8329
39. Wang M, Zhu L, Liu C, He H, Wang C, Xing C, et al. A novel assisted oocyte activation method improves fertilization in patients with recurrent fertilization failure. Front Cell Dev Biol. (2021) 9:672081. doi: 10.3389/fcell.2021.672081
40. Haas DM, Morgan S, Contreras K, Kimball S. Vaginal preparation with antiseptic solution before cesarean section for preventing postoperative infections. Cochrane Database Syst Rev. (2020) 4(4):Cd007892. doi: 10.1002/14651858.CD007892.pub7
41. Bradbury RA, Christie-David D, Smith HC, Byth K, Eastman CJ. Prior iodine exposure and impact on thyroid function during controlled ovarian hyperstimulation: a prospective study. Aust N Z J Obstet Gynaecol. (2022) 62(1):133–9. doi: 10.1111/ajo.13419
42. Younis JS, Ezra Y, Laufer N, Ohel G. Late manifestation of pelvic abscess following oocyte retrieval, for in vitro fertilization, in patients with severe endometriosis and ovarian endometriomata. J Assist Reprod Genet. (1997) 14(6):343–6. doi: 10.1007/BF02765839
43. Hu L, Du J, Lv H, Zhao J, Chen M, Wang Y, et al. Influencing factors of pregnancy loss and survival probability of clinical pregnancies conceived through assisted reproductive technology. Reprod Biol Endocrinol. (2018) 16(1):74. doi: 10.1186/s12958-018-0390-6
44. Ma LY, Xu XT, Dou Q, Zhao DM, Xiang YG, Li PF, et al. Influencing factors of pregnancy outcome of in vitro fertilization-embryo transfer. J Sichuan Univ Med Sci Ed. (2022) 53(1):133–6. doi: 10.12182/20220160205
Keywords: vaginal douching, oocyte retrieval, pelvic infection, IVF outcome, network meta analysis
Citation: Meng Y, Wen GH, Luo H, Tan XC, Wang L, Liao J, Peng H, Lan L, Yang N and Zhao Y (2022) Which vaginal douching agent is the best choice before oocyte retrieval? A systematic review and network meta-analysis. Front. Reprod. Health 4:1032062. doi: 10.3389/frph.2022.1032062
Received: 31 August 2022; Accepted: 17 October 2022;
Published: 4 November 2022.
Edited by:
Jan Tesarik, MARGen Clinic, SpainReviewed by:
Akmal El-Mazny, Cairo University, Egypt© 2022 Meng, Wen, Luo, Tan, Wang, Liao, Peng, Lan, Yang and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gui Hong Wen MzU2NzI3MjEyQHFxLmNvbQ==
Specialty Section: This article was submitted to Assisted Reproduction, a section of the journal Frontiers in Reproductive Health
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.