
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Reprod. Health , 29 November 2021
Sec. Gynecology
Volume 3 - 2021 | https://doi.org/10.3389/frph.2021.783247
This article is part of the Research Topic Genitourinary Syndrome of Menopause View all 7 articles
 Ana Paula Ferreira Costa1*
Ana Paula Ferreira Costa1* Ayane Cristine Alves Sarmento1
Ayane Cristine Alves Sarmento1 Pedro Vieira-Baptista2,3
Pedro Vieira-Baptista2,3 José Eleutério Jr.4
José Eleutério Jr.4 Ricardo Ney Cobucci5
Ricardo Ney Cobucci5 Ana Katherine Gonçalves1,6
Ana Katherine Gonçalves1,6Menopause is a physiological and progressive phenomenon secondary to decreased ovarian follicular reserve that significantly affects the genital tract. Although postmenopausal vulvovaginal atrophy primarily affects postmenopausal women, it is also seen in premenopausal women. The hypoestrogenic condition results in hormonal and anatomical changes, with the main symptoms, are dryness, burning and genital irritation, decreased lubrication, urinary urgency, dysuria, and recurrent urinary tract infections. This review aims to update hormone therapy for urogenital atrophy, both local and systemic, and discusses the importance of understanding and the need for active treatment of this condition. The main therapeutic objective is the relief of symptoms, and hormonal therapy (HT) is still the most effective choice for treating clinical manifestations, despite the side effects of its use. HT should be used in an individualized way to the needs of the women and appropriate to the stage in which she is menopausal, perimenopausal, or after menopause.
Menopause is a gradual and physiological event due to ovarian failure and consequent hypoestrogenism, which significantly affects the lower genital tract. Several denominations are used to describe the alterations noticed in the lower genital tract, such as atrophic vaginitis, vulvovaginal atrophy (VVA), and, lately, genitourinary syndrome of menopause (GSM) (1–3).
Vulvovaginal atrophy of any degree is present in 15% of premenopausal women and in 40–54% of postmenopausal women (4, 5). Women may experience some or all signs and symptoms (vaginal dryness, dyspareunia, sensations of discomfort, burning and irritation, vulvovaginal pruritus, dysuria, and increased frequency of genitourinary infections). The condition is often underdiagnosed due to sexual embarrassment or general disregard associated with it as a liability of natural aging, especially if the symptoms are mild (4, 5).
The main therapeutic objective is the relief of symptoms. Local (vaginal) hormones are the most used option to fulfill this objective. They promote the renovation of the epithelium and vaginal flora, and improvement of the urogenital and sexual complaints (3, 5).
Several hormonal treatment options are currently available, including systemic hormonal therapies (oral and transdermal), low-dose vaginal estrogen, prasterona therapies (2, 3, 5), and Selective Estrogen Receptor Modulators (SERMs) as Ospemifene. This article aims to contribute to knowledge about subjective and objective measurements available for assessing vulvar, vaginal, and lower urinary tract atrophy, as well as future possibilities; so, the hormonal treatment options have been available over the years for this syndrome.
Systemic estrogen therapy is in preference if vasomotor symptoms are also present, whereas local vaginal estrogen therapy (vaginal estrogen ovules or tablets, creams, or a vaginal ring) is preferred when genitourinary symptoms are the only complaint (3–8). Patients receiving systemic ET for other menopausal symptoms frequently have persistent urogenital symptoms requiring supplemental vaginal ET.
Exogenous estrogen use restores normal the vaginal pH, increases epithelial thickness, and revascularizes the epithelium, thus increasing vaginal lubrication. As a result, systemic hormonal therapy relieves symptoms of VVA, including dryness, irritation, pruritus, dyspareunia, and urinary urgency, and may also decrease the incidence of lower urinary tract infections, thus improving the quality of life of these women (5, 9, 10).
In some cases, systemic estrogen therapy is not effective. One of the reasons for this is the fact that, within the intestine, estrogen levels are controlled by a group of intestinal bacteria called estrobolome. When there is an imbalance in the intestine, estrobolome releases an excess enzyme, beta-glucuronidase, which causes harmful estrogens to continually circulate through our system. Depending on the diversity and amount of intestinal bacteria, we may have a low beta-glucuronidase (insufficient reabsorption and a deficit of estrogen in the body) or a high beta-glucuronidase (excess of estrogen being reabsorbed) (11).
Progesterone is a modulator of normal reproductive functions. These functions include ovulation, uterine and mammary gland development, and neurobehavioral expression associated with sexual responsiveness. Oral micronized progesterone is molecularly identical to human progesterone and provides additional therapeutic benefits for sleep and endometrial hyperplasia protection. However, there is reason to believe that progesterone has a more favorable safety profile than medroxyprogesterone; large safety trials of progesterone as postmenopausal monotherapy are lacking (12–14).
In postmenopause, there is a decline in the production of androgens, which are also responsible, among others, for sexual function; the administration of testosterone for the treatment of symptoms related to menopause has been studied, with an emphasis on decreasing libido and sexual desire (15).
Testosterone use in postmenopausal women is considered effective in improving sexual function. However, it is a necessary note that each result has its limitations, mainly related to personal and cultural factors, as the studies evaluated women of diversity. Oral testosterone is less used as it undergoes hepatic passage, and there is a decrease in the half-life of the drug, thus needing to be ingested several times a day (three to four times) to maintain the serum level. In addition, oral 17-alpha-alkylated forms of testosterone can cause hepatotoxicity, even at physiological levels, thus increasing the risk of hepatitis, cholestasis, and benign and malignant liver neoplasms (16). It is known that the plasma concentration of total testosterone observed in women in their 40's represents half of that seen in their 20's. However, it should be noted that there is no well-defined biochemical criterion to characterize an androgenic insufficiency since it was not possible to directly correlate the plasma levels of total and free testosterone with the complaints of the patients, reinforcing the need to dose them (17).
Low-dose vaginal ET is the most used pharmacological treatment for VVA, being also the most effective and safer option. During the low-dose vaginal ET use, systemic estrogen absorption is minimal, and serum estradiol remains within postmenopausal levels (7–14).
The application of vaginal ET must be adjusted according to tolerability of each woman. However, ET usually starts with nightly application between 2 and 3 weeks and decreases to two to three times per week. The posology of formulations of vaginal ET is evidenced in Table 1. In general, women prefer an improvement of symptoms within a few weeks of initiating treatment. However, many women require 8 to 12 weeks to relieve symptoms. The use of a progestogen is not required for endometrial protection in women receiving low-dose vaginal ET. Nonetheless, periodic endometrial surveillance or progestogen use can be considered for women at high-risk endometrial neoplasia (7–14).
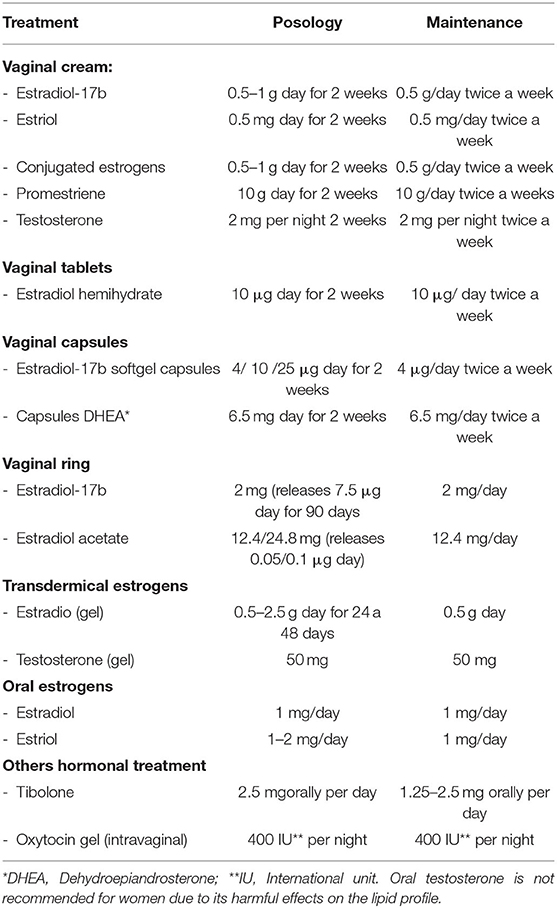
Table 1. Hormonal therapy options.
According to a systematic review conducted by Biehl et al. (18), use of vaginal ET for 1 year was associated with complications, such as vulvovaginal mycosis, vaginal bleeding, endometrial hyperplasia, and endometrial cancer. Another complication that usually not requires treatment is the development of mild transient candidiasis (19). Vaginal ET does not seem to increase the risk of venous thromboembolism, but data on high-risk patients are lacking (7–14). Essentially, non-hormonal treatments are preferred initial strategies for the survivors of hormone-dependent cancers (breast and endometrial cancers). However, after a detailed evaluation of benefits and risks, low-dose vaginal ET, for a short time, could be considered in women with unmanageable symptoms affecting their quality of life (7, 14). Vaginal ET use was not associated with significant absorption, which may provide indirect evidence of safety. Research confirmed this information when observed that vaginal ET is considerable safety in women with breast cancer, receiving aromatase inhibitors (20). Another clinical trial evaluated the efficacy and safety of an ultra-low dose of vaginal gel estriol (0.005%) and demonstrated that the treatment group displayed improved VMI, pH, dryness, global symptoms, and exploratory signs as FSFI scores. Furthermore, serum estrogen, LH, and FSH levels remained unchanged (21). Multiple vaginal estrogen products with similar efficacy are available (Table 1).
Dehydroepiandrosterone is a steroid produced in the adrenal glands and converted into sex hormones (estrogens and androgens). A represents an inactive precursor, being transformed into active androgens, only in peripheral tissues that contain the enzymes necessary to continue the steroidogenesis process; thus, each tissue builds its own hormonal identity (intracrinology), avoiding unnecessary exposure to circulating active steroids (22, 23). The vaginal tissue-specific enzymes transform DHEA into the appropriate small amounts of estrogens and androgens for a strictly intracellular and local action, improving the vaginal pH and vaginal maturation index. Furthermore, improvement in sexual arousal and libido has also been reported. The only side effect reported was vaginal discharge due to the melting of the insert (23).
Clinical trial realized using DHEA showed that vaginal prasterone different doses (3.25 and 6.5 mg/day) increased in blood DHEA levels in a dose-dependent manner while serum estradiol was increased only in those insignificant prasterone concentrations. Despite an increase in the level, it is important to cite that the sex steroid levels remained within the lowest levels for postmenopausal women. More studies are necessary to clarify the long-term effects of this treatment (24) (Table 1).
Although there are few studies about its efficacy, intravaginal testosterone has been used as hormonal therapy that has shown positive effects in relieving vaginal atrophy symptoms and decreased libido. Some research showed that a single intravaginal dose of 2 mg in premenopausal women resulted in supra physiologic testosterone levels with no change in serum estradiol; another study appointed that these hormone treatments reduced the vaginal pH and increased the vaginal cell score and the number of lactobacilli. Finally, a meta-analysis concluded that the effect of vaginal testosterone on sexual function and sexuality scores was similar to estrogen therapy. Thus, larger studies are needed to assess safety and efficacy (25–28) (Table 1).
Tibolone, a synthetic steroid, is rapidly converted to three active metabolites (3α-OH, 3β-OH, and 1Δ4), all of which are biologically active and contribute to the hormonal profile of the parent compound. It has been used in postmenopausal women to relieve vasomotor symptoms and improve vaginal atrophy, changing the vaginal maturation index and increasing the sex drive through its part androgenic properties. Moreover, urinary incontinence problems of nocturia and urgency were found to be improved (5, 18, 29, 30) (Table 1).
Oxytocin has been evaluated as an alternative due to concerns about the use of estrogen therapy. It is a peptide hormone produced in the hypothalamus, and it is best known for its role in labor and lactation. Some studies suggest that applying oxytocin produces a healthier and more vaginal epithelium, with normal vaginal pH levels and a significant reduction in symptoms. However, other research is necessary for confirmation of these results (31–35).
Hormonal therapy must be individualized to the needs of women and is conditioned by the stages of menopause. Low-dose vaginal estrogens, vaginal DHEA, and systemic estrogen therapy are effective for moderate to severe GSM. Treatment by administering hormone systemic, in particular, is commonly used to combat vasomotor symptoms, preserve bone mass, improve sleep, prevent the deterioration of cognitive function, and stimulate libido. The vaginal formulations promote the renovation of the epithelium and vaginal flora and improve the urogenital and sexual complaints, decreasing the vaginal dryness. Tibolone is another option used to relieve vasomotor symptoms and improve vaginal atrophy, changing the VMI and increasing the sex drive through its androgenic properties. Oxytocin has been evaluated as an alternative due to concerns about the use of estrogen therapy. However, other research is necessary for confirmation of these results.
AC and AG: conceived and designed the study. AC, AS, AG, and JE: drafted and revised the article where appropriate. AS and AC: prepared the table. AG, PV-B, JE, and RC: carried out the final revision of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Portman DJ, Gass ML. Vulvovaginal atrophy terminology consensus conference panel. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the international society for the study of women's sexual health and the North American menopause society. Menopause. (2014) 21:1063–8. doi: 10.1097/GME.0000000000000329
2. Pérez-López FR, Vieira-Baptista P, Phillips N, Cohen-Sacher B, Fialho SCAV, Stockdale CK. Clinical manifestations and evaluation of postmenopausal vulvovaginal atrophy. Gynecol Endocrinol. (2021) 37:740–5. doi: 10.1080/09513590.2021.1931100
3. Gandhi J, Chen A, Dagur G, Suh Y, Smith N, Cali B, et al. Genitourinary syndrome of menopause: an overview of clinical manifestations, pathophysiology, etiology, evaluation, and management. Am J Obstet Gynecol. (2016) 215:704–11. doi: 10.1016/j.ajog.2016.07.045
4. Keil K. Urogenital atrophy: diagnosis, sequelae, and management. Curr Womens Health Rep. (2002) 2:305–11.
5. Palacios S, Combalia J, Emsellem C, Gaslain Y, Khorsandi D. Therapies for the management of genitourinary syndrome of menopause. Post Reprod Health. (2020) 26:32–42. doi: 10.1177/2053369119866341
6. Nappi RE, Kingsberg S, Maamari R, Simon J. The CLOSER (CLarifying Vaginal Atrophy's Impact OnSEx and Relationships) survey: implications of vaginal discomfort in postmenopausal women and in male partners. J Sex Med. (2013) 10:2232–41. doi: 10.1111/jsm.12235
7. The North American Menopause Society. Management of symptomatic vulvovaginal atrophy: 2013 position statement of the North American menopause society. Menopause. (2013) 20:888–902 doi: 10.1097/GME.0b013e3182a122c2
8. The NAMS 2017 Hormone Therapy Position Statement Advisory Panel. The 2017 hormone therapy position statement of The North American menopause society. Menopause. (2017) 24:728–53. doi: 10.1097/GME.0000000000000921
9. Perez-Lopez FR, Phillips N, Vieira-Baptistac P, Cohen-Sacherf B, Fialhog SCAV, Stockdale CK. Management of postmenopausal vulvovaginal atrophy: recommendations of the international society for the study of Vulvovaginal disease. Gynecol Endocrinol. (2021) 37:746–52. doi: 10.1080/09513590.2021.1943346
10. Genazzani AR, Monteleone P, Giannini A, Simoncini T. Hormone therapy in the postmenopausal years: considering benefits and risks in clinical practice. Hum Reprod Update. (2021) 27:1115–50. doi: 10.1093/humupd/dmab026
11. Ruo SW, Alkayyali T, Win M, Tara A, Joseph C, Kannan A, et al. Role of gut microbiotadysbiosis in breast cancer and novel approaches in prevention, diagnosis, and treatment. Cureus. (2021) 13:e17472. doi: 10.7759/cureus.17472
12. Hitchcock CL, Prior JC. Oral micronized progesterone for vasomotor symptoms—a placebo-controlled randomized trial in healthy postmenopausal women. Menopause. (2012) 19:886–93. doi: 10.1097/gme.0b013e318247f07a
13. Gompel A, Plu-Bureau G. Progesterone, progestins and the breast in menopause treatment. Climacteric. (2018) 21:326–32. doi: 10.1080/13697137.2018.1476483
14. Prior JC, Hitchcock CL. Progesterone for hot flush and night sweat treatment – effectiveness for severe vasomotor symptoms and lack of withdrawal rebound. Gynecol Endocrinol. (2018) 28:7–11. doi: 10.3109/09513590.2012.705390
15. Traish AM, Feeley RJ, Guay AT. Testosterone therapy in women with gynecological and sexual disorders: a triumph of clinical endocrinology from 1938 to 2008. J Sex Med. (2009) 6:334–51 doi: 10.1111/j.1743-6109.2008.01121.x
17. Santoro N, Epperson CN, Mathews SB. Menopausal symptoms and their management. Endocrinol Metab Clin North Am. (2015) 44:497–515. doi: 10.1016/j.ecl.2015.05.001
18. Biehl C, Plotsker O, Mirkin S. A systematic review of the efficacy an safety of vaginal estrogen products for the treatment of genitourinary syndrome of menopause. Menopause. (2019) 26:431–53. doi: 10.1097/GME.0000000000001221
19. Faubion SS, Sood R, Kapoor E. Genitourinary syndrome of menopause: management strategies for the clinician. Clin Proc. (2017) 92:1842–9. doi: 10.1016/j.mayocp.2017.08.019
20. Pavlovic RT, Jankovic SM, Milovanovic JR, Stefanović SM, Folić MM, Milovanović OZ, et al. The safety of local hormonal treatment for vulvovaginal atrophy in women with estrogen receptor-positive breast cancer who are on adjuvant aromatase inhibitor therapy: meta-analysis. Clin Breast Cancer. (2019) 19:e731–40. doi: 10.1016/j.clbc.2019.07.007
21. Hirschberg AL, Sanchez-Rovira P, Presa-Lorite J, Campos-Delgado M, Gil-Gil M, Lidbrink E, et al. Efficacy and safety of ultra-low dose 0005% estriol vaginal gel for the treatment of vulvovaginalatrophy in postmenopausal women with early breast cancer treated with nonsteroidal aromatase inhibitors: a phase II, randomized, double-blind, placebo-controlled trial Menopause. (2020) 27:526–34. doi: 10.1097/GME.0000000000001497
22. Labrie F, Martel C. A low dose (65 mg) of intravaginal DHEA permits a strictly local action while maintaining all serum estrogens or androgens as well as their metabolites within normal values. Horm Mol Biol Clin Investig. (2017) 29:39–60. doi: 10.1515/hmbci-2016-0042
23. Guay AT. Screening for androgen deficiency in women: methodological and interpretive issues. FertilSteril. (2002) 77:83–8. doi: 10.1016/S0015-0282(02)02965-5
24. Barton DL, Sloan JA, Shuster LT, Gill P, Griffin P, Flynn K, et al. Evaluating the efficacy of vaginal dehydroepiandosterone for vaginal symptoms in postmenopausal cancer survivors: NCCTG N10C1 (Alliance). Support Care Cancer. (2018) 26:643–50. doi: 10.1007/s00520-017-3878-2
25. Fischer G, Bradford J. Vulvovaginal candidiasis in postmenopausal women: the role of hormone replacement therapy. J Low Genit Tract Dis. (2011) 15:263–7. doi: 10.1097/LGT.0b013e3182241f1a
26. Simon JA, Goldstein I, Kim NN, Davis SR, Kellogg-Spadt S, Lowenstein L, et al. The role of androgens in the treatment of genitourinary syndrome of menopause (GSM): international society for the study of women's sexual health (ISSWSH) expert consensus panel review. Menopause. (2018) 25:837–47. doi: 10.1097/GME.0000000000001138
27. Apperloo M, Midden M, van der Stege J, Wouda J, Hoek A, Schultz WW. Vaginal application of testosterone: a study on pharmacokinetics and the sexual response in healthy volunteers. J Sex Med. (2006) 3:541–9. doi: 10.1111/j.1743-6109.2006.00212.x
28. Fernandes T, Pedro AO, Baccaro LF. Hormonal, metabolic, and endometrial safety of testosterone vaginal cream versus estrogens for the treatment of vulvovaginal atrophy in postmenopausal women: a randomized, placebo-controlled study. Menopause. (2018) 25:641–7. doi: 10.1097/GME.0000000000001059
29. Pitsouni E, Grigoriadis T, Douskos A, Kyriakidou M, Falagas ME. AthanasiouS. Efficacy of vaginal therapies alternative to vaginal estrogens on sexual function and orgasm of menopausal women: a systematic review and meta-analysis of randomized controlled trials. Eur J Obstet Gynecol Reprod Biol. (2018) 229:45–56. doi: 10.1016/j.ejogrb.2018.08.008
30. Swanson SG, Drosman S, Helmond FA, Stathopoulos VM. Tibolone for the treatment of moderate to severe vasomotor symptoms and genital atrophy in postmenopausal women. Menopause. (2016) 13:917–25. doi: 10.1097/01.gme.0000247016.41007.c9
31. Breuil V, Trojani MC, Ez-Zoubir A. Oxytocin and bone: review and perspectives. Int J Mol Sci. (2021) 22:8551. doi: 10.3390/ijms22168551
32. Jonasson AF, Edwall L, Uvnas-Moberg K. Topical oxytocin reverses vaginal atrophy in postmenopausal women: a double-blind randomized pilot study. Menopause. (2011) 17:120–5. doi: 10.1258/mi.2011.011030
33. Hyun-Kyung K, So-Yeon K, Youn-Jee C, Jang-Heub K, Mee-Ran K. The recent review of the genitourinary syndrome of menopause. J Menopausal Med. (2015) 21:65–71. doi: 10.6118/jmm.2015.21.2.65
34. Al-saqi SH, Uvnäs-moberg K, Jonasson AF. Intravaginally applied oxytocin improves postmenopausal vaginal atrophy. Post Reprod Health. (2015) 21:88–97. doi: 10.1177/2053369115577328
Keywords: menopause, vulvovaginal atrophy, hormone therapy, estrogen, DHEA, testosterone, oxytocin
Citation: Costa APF, Sarmento ACA, Vieira-Baptista P, Eleutério J Jr, Cobucci RN and Gonçalves AK (2021) Hormonal Approach for Postmenopausal Vulvovaginal Atrophy. Front. Reprod. Health 3:783247. doi: 10.3389/frph.2021.783247
Received: 25 September 2021; Accepted: 29 October 2021;
Published: 29 November 2021.
Edited by:
Pradeep Tanwar, The University of Newcastle, AustraliaCopyright © 2021 Costa, Sarmento, Vieira-Baptista, Eleutério, Cobucci and Gonçalves. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Paula Ferreira Costa, YW5hLXBhdWxhLXJmQGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.