 Dominica Dhakwa1*†
Dominica Dhakwa1*† Fungai H. Mudzengerere2†
Fungai H. Mudzengerere2† Mulamuli Mpofu3
Mulamuli Mpofu3 Emmanuel Tachiwenyika1Florence Mudokwani2Blessing Ncube2
Emmanuel Tachiwenyika1Florence Mudokwani2Blessing Ncube2 Mutsa Pfupajena2
Mutsa Pfupajena2 Tendai Nyagura4
Tendai Nyagura4 Getrude Ncube5
Getrude Ncube5 Taurayi A. Tafuma2
Taurayi A. Tafuma2- 1Family Health International 360, Harare, Zimbabwe
- 2Zimbabwe Health Interventions, Harare, Zimbabwe
- 3Family Health International 360, Gaborone, Botswana
- 4United States Agency for International Development Zimbabwe Mission, Harare, Zimbabwe
- 5AIDS and TB Department, Ministry of Health and Child Care, Harare, Zimbabwe
Background: Gaps still exist in reducing new HIV infections among adolescent girls and young women (AGYW) aged 10–24 years. High Internet coverage and mobile phone penetration rates present opportunities for the use of mobile health (mHealth) to support access to health services. We present results of an FHI 360 and Zimbabwe Health Interventions-implemented mHealth intervention for reproductive health (RH) and HIV testing service (HTS) referral among AGYW aged 10–19 years between October 2019 and September 2020.
Methods: Adolescent girls and young women referred for RH and HTS under the Determined, Resilient, Empowered, AIDS-free, Mentored, and Safe (DREAMS) program had automatic reminders sent to their phones to facilitate access to services through short message service (SMS) and also using a paper-based system. These data were captured in a web-based District Health Information System (DHIS) database, which captured the referral completion status of the AGYW. Data for AGYW referred for RH and HTS for the period October 2018 to September 2019 for the paper-based system and October 2018 to September 2020 for the mHealth were extracted from District Health Information System version 2 (DHIS2) database and analyzed using SPSS to generate descriptive statistics. The Chi-square test was used to assess differences in referral completion rates by age-group; marital status, district, and type of service, as well as differences between mHealth and paper-based referral completion rates within each of the groups for the variables above.
Results: A total of 8,800 AGYW referred for RH and HTS, where 4,355 and 4,445 were referred through the mHealth and paper-based systems, respectively. About 95.2% (4,148/4,355) and 87.8% (3,903/4,445) referred through mHealth and the paper-based system, respectively completed referrals. The median time for referral completion was 1 day (Range = 0–9 days) for mHealth and 11 days (Range = 0–28 days) for the paper-based system. AGYW referred through mHealth were 17.995 times
more likely to complete the referral system than those referred through the paper-based system (OR =17.995; p <0.001).
Conclusion: Compared to the paper-based referral system the mHealth solution resulted in a higher, service referral completion rates and shorter turnaround time. We recommend expansion of the mHealth solution to all DREAMS supported districts to increase uptake of RH and HTS among AGYW aged 10–19 years.
Introduction
Despite reductions in HIV infections globally, gaps still exist in addressing the HIV pandemic among adolescent girls and young women (AGYW) (1). Thus, innovations like promoting a complete service referral network (SRN) through mobile health (mHealth) are critical for any HIV programming among this vulnerable group. mHealth is the use of mobile and wireless technologies to support health interventions, and literature has shown that mHealth interventions have demonstrable efficiency in supporting completion of patient referral ensuring treatment adherence especially among the youths (2). Community-based strategies like mHealth can help accelerate progress toward HIV epidemic control (3, 4). The use of mHealth through mobile devices like smartphones and tablets provides interactive programs and interventions are appealing to the young generations (5). The rise in the use of technology by youths globally presents greater opportunities for mHealth. Over 80% of youths aged between 18–29 years are believed to own a phone in developed countries, while in low and middle-income countries, the use of the Internet and owning a smartphone are also on the rise (6, 7). This makes mHealth a powerful tool capable of transforming the lives of the youths to meet their reproductive health (RH) and HIV testing service (HTS) needs. In Sub-Sahara Africa, short message service (SMS) has been used for reminding clients to undergo HIV testing and to pick up their medicine refills for those on antiretroviral therapy (ART) (8). Additionally, mHealth reduces documentation errors, is efficient in reducing the turnaround time, gives quality data, and is effective in reducing the missed appointments (9).
Family Health International (FHI360) and Zimbabwe Health Interventions (ZHI) with funding from the United States Agency for International Development (USAID) have been implementing the Determined, Resilient, Empowered, AIDS-free, Mentored, and Safe (DREAMS) program in Zimbabwe since 2015. The program aims to reduce HIV incidence among 10–19 year-old AGYW. Under the Zimbabwe DREAMS project, referrals for services were done using a paper-based system where out of school club facilitators (OOSCFs) generated referral slips which the AGYW handed over to the service providers upon presenting themselves for services. The referral slips were completed in duplicate where AGYW were given one of the slips which the service providers signed as confirmation for referral completion and services rendered on presentation. Tracking referral completions was done through the collection and reconciliation of the slips between the referral organization and the service provider. This referral system had the following challenges: poor communication between service providers, loss of referral slips, lack of feedback from the service providers, and long turnaround time for completion of the referral cycle to access services (10, 11). Under the project, mHealth was introduced on October 1, 2019. The community OOSCFs screen AGWY for eligibility into the DREAMS programs, and those who are eligible are enrolled, and their demographic details are captured into District Health Information System version 2 (DHIS2). AGYW are referred for HTS and RH services through the generation of a referral slip, which is also captured in DHIS2. The AGYW's contact telephone number is linked to the DHIS database where reminders are sent for services not accessed. Once services are accessed, information from the service providers is updated into DHIS2. This study assessed the effectiveness of mHealth in improving service linkages among AGYW. It also evaluates the turnaround time to referral completion among AGYW referred through the mHealth and the paper-based referral systems. In addition, the study explored factors associated with services referral completion among AGYW.
Methodology
This analysis used aggregate and routine program data, extracted from the DHIS2 project database. Routine program data of AGYW enrolled in the DREAMS program and referred for RH and HIV prevention services for the period October 2018–September 2020 were extracted by the data capture clerk from DHIS2. We extracted aggregate data on the following data elements: age, marital status, district, referred health facility, date of referral, and referral outcome.
Determined, Resilient, Empowered, AIDS-Free, Mentored, and Safe Program
Zimbabwe has been implementing the DREAMS program since 2015. The program is aimed at reducing HIV incidence among AGYW aged 10–24 years old. In Zimbabwe, the program is being implemented in six districts, namely Bulawayo, Chipinge, Gweru, Makoni, Mazowe, and Mutare. The DREAMS core package combines evidence-based approaches that go beyond health, but addresses the structural drivers that directly and indirectly increase girls' risk for contracting HIV. These include poverty, gender inequality, sexual violence, and lack of education. Thus, the program offers in-school and community-based service delivery to build social assets for the AGYW. The program also promotes changing harmful community norms that put AGYW at risk of gender-based violence (GBV). Through layering of services, the DREAMS program delivers clinical and post-GBV services. The clinical services that are delivered through the DREAMS program include HIV testing, Sexually Transmitted Infections (STI) screening, Pre-exposure prophylaxis (PrEP), Post-Exposure prophylaxis (PEP), and reproductive health.
Enrolment of AGYW Into the DREAMS Program
The OOSCFs, who are community cadres employed under the DREAMS program, identified AGYW aged between 10 and 19 years who are at risk of contracting HIV. Using the enrolment standard operating procedures (SOPs), written consent was sought from AGYW prior to the administration of the DREAMS eligibility screening tool. The DREAMS eligibility screening tool captures demographic details, orphanhood status, indulgence in sex, experience of any GBV, alcohol misuse, and if the AGYW had experienced any of this, then they are eligible for enrollment into the program and hence referred for services. If the AGYW are eligible, a unique identification code is generated, which will be used for enrolment into the program. The DREAMS program enrolment tool was administered, which captured the demographic and social details, exposure to GBV and HIV risk assessment. Provision or referral for appropriate services was conducted based on AGYW vulnerabilities. Data on screening and enrolment of the beneficiaries were captured in the program database (DHIS2) by Monitoring and Evaluation (M&E) staff.
Referral Process for Services
Adolescent girls and young women identified from the community who were screened and enrolled into the DREAMS program and deemed at risk of contracting HIV were either offered services onsite or referred to another implementing partner for services. A referral slip was generated and given to the AGYW, with the duplicate copy remained with the OOSCF for tracking purposes. Upon accessing services at the referral site, the referral slips were collected by a health worker who offered HTS or RH services. The issuing partner will then follow up to determine completion of referral with the service providers. Data on referral slips were later captured in DHIS2 where reminders for those who have not accessed services were generated, and notifications sent through SMS.
Since October 2019, referrals were made through the mHealth platform where slips generated manually were immediately captured into DHIS2 upon being issued to the AGYW. If services were not accessed, continuous and automated SMS reminders were sent until the AGYW access the service and an update is made in DHIS2. Referrals are made to both the public and private service providers. Among the public service providers are the Ministry of Health and Childcare (MOHCC) and Zimbabwe National Family Planning Council (ZNFPC) run facilities. Private sector service providers are mainly non-governmental organizations who conduct outreach activities.
Sampling and Data Collection
All AGYW who were enrolled and referred for HTS and RH services in the six districts using the paper-based referral system from October 1, 2018 to September 30, 2019, and those referred through mHealth from October 1, 2019 to September 30, 2020 were included in the analysis. Data were extracted from the project's DHIS2 system.
Data Analysis
Data were extracted from the DHIS2 database, exported to Microsoft Excel spreadsheet, and analyzed using SPSS (IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, NY, USA) for generating descriptive statistics. The Chi-square-test was used to test if there were differences in the completion of referrals within the following variable groups: age-group, marital status, district, service, organization referred to, and location of service within both the mHealth and the paper-based referral systems. We also used the Chi-square to assess for differences in the referral completion rates between mHealth and paper-based referral systems within each sub-group of the variables listed above. Logistics regression was used to estimate the factors associated with service completion. Cox Proportional Hazard analysis was used to test the difference in time to completion of service referral between the two systems (mHealth vs. paper-based system).
Ethical Consideration
Ethics approval was obtained from the Medical Research Council of Zimbabwe (MRCZ/E/254). Routine monitoring and evaluation program data were analyzed. Personal identification information of beneficiaries was excluded from the analysis.
Results
A total of 8,800 AGYW aged 10–19 years were referred for HTS and RH, where 4,355 were referred through mHealth and 4,445 through the paper-based system. Of these, 1,821 (20.7%) were from Bulawayo district while 10.9% (959/8,800) were from Mazowe district (Table 1). The majority 96.2% (8,66/8,800) were aged 15–19 years. Nearly two-thirds, 60.4% (5,315/ 8,800) of the AGYW were referred for RH services. About 91.4% (8,043/8,800) were single while 4.4% were married and 4.2% were divorced.
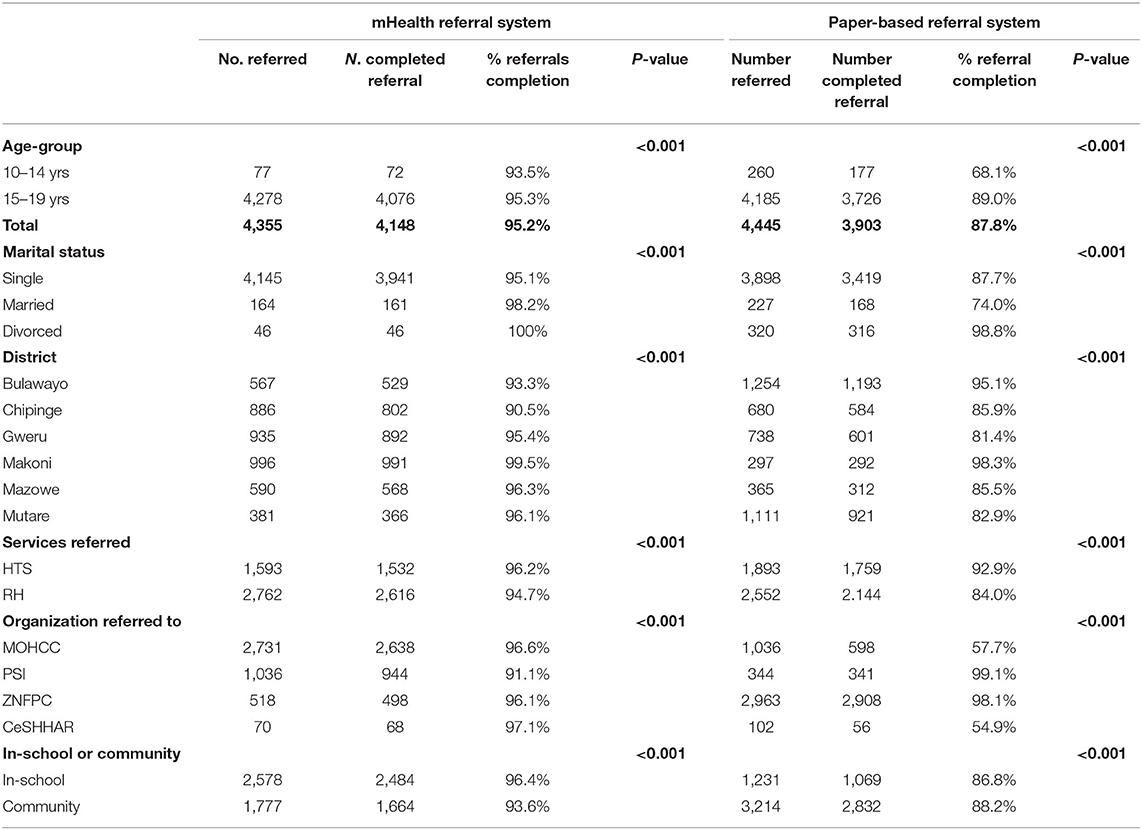
Table 1. mHealth and paper-based referral system results.
From Table 1, there was a significant difference in referral completion by age-group, marital status, district, and organization for referrals done by both mHealth and the paper-based system (p <0.001).
Less than half, 42.8% (3,766/8,800) of the AGYW were referred to the MOHCC for HTS and RH while the rest were referred to private organizations.
Services Referral Completion
About 95.2% (4,148/4,355) of AGYW was referred through mHealth, which was significantly higher than the 87.8% (3,903/4,445) of the AGYW referred through the paper-based system (p <0.001; Table 2).
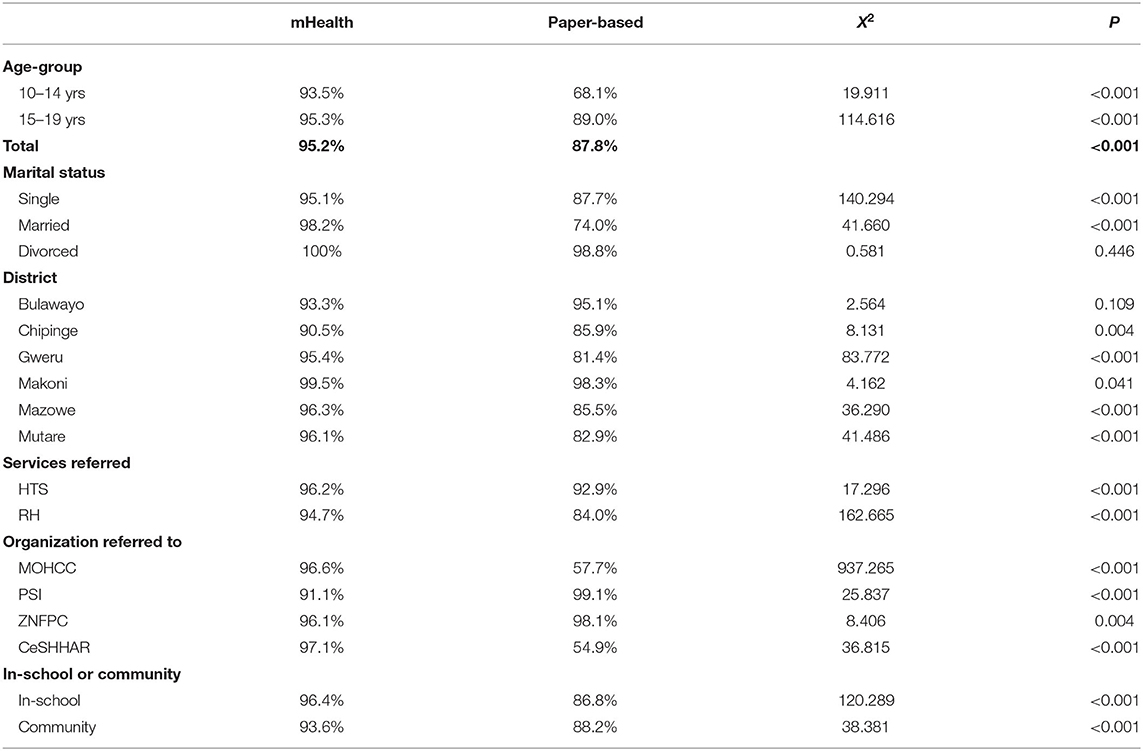
Table 2. Differences in referral completion between mhealth and the paper-based system.
Within all age-groups, type of service, and some districts, referral completion was higher within the mHealth referral system compared to the paper-based system (p < 0.001). Though referral completion was higher in the mHealth system among the divorced and those in Bulawayo district, the difference was not statistically significant (p = 0.446 and p = 0.109, respectively).
Time to Service Referral Completion
Almost half 47.2% (1,957/4,148) of the AGYW referred through the mHealth platform completed the service referral on the same day, compared to 0.8% (36/4,398) for the paper-based system (Figure 1). This rises to 96.1% (3,984/4,148) of the AGYW referred through the mHealth platform within 5 days compared to 20.7% (912/4,398) for those referred through the paper-based system.
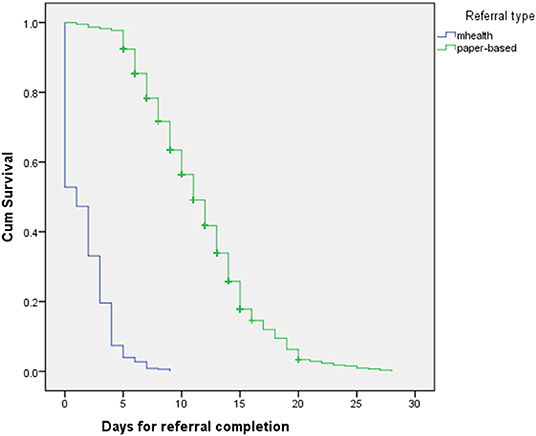
Figure 1. Time to referral completion for mHealth and paper-based system.
The median time for referral completion was 1 day, (range = 0–9 days) for mHealth while it was 11 days (range = 0–28 days) for paper-based system. There was a significant difference in the time to completion service referral network for mHealth and the paper-based systems (X2 = 5868.786, p < 0.001). Also, the Cox regression analysis showed a significant difference in the time to completion of the referral network between mHealth and paper-based systems, Exp (B) = 12.157, 95% CI (11.308; 13.070).
Factors Associated With Service Referral Completion
Adolescent girls and young women referred through mHealth were 17.995 times more likely to complete referral than those referred through the paper-based system [OR = 17.995 (95% CI =13.520: 23.952)]. AGYW aged 10–14 years old were 75.2% less likely to complete service referral than those aged 15–19 years [OR = 0.248; 95% CI (0.169; 0.363)]. Single AGYW were also less likely to complete SRN than the married and the divorced [OR = 0.137; 95% CI (0,049; 0.381); p < 0.001].
Discussion
Results from this study showed high referral completion rates among AGYW referred using mHealth than those referred using a paper-based system. mHealth services that integrate SMS reminders help to remind AGYW to access services unlike referral slips which can easily be misplaced. The high mobile phone penetration rate among AGYW also assured that enrolled clients will receive SMS reminders. While the use of mHealth was successful within DREAMS in Zimbabwe, this contrasts findings from a study conducted in Uganda, where the use of mHealth had little effect in improving access and completion of services referred due to limited data bundles and support systems for online follow-up and reporting (12). In Zimbabwe, the use of mHealth timeously reminded AGYW to seek services early, and these results are similar to findings from studies conducted in other low-income settings (13). While mHealth has benefits as shown in this study, a similar study in 2016 found that the use of mHealth had a cost implication as the beneficiaries had challenges of mobile data to access the system, which was resolved by the use of SMS reminders that were cost-effective (14). The use of SMS to remind AGYW improved accessing services and reduced the referral completion turnaround time, similar to the findings from studies from other African countries (8, 15).
There were high HTS and RH service referral completion rates regardless of the marital status of the AGYW, which can be attributed to the integration of HTS and RH for AGYW as reported from other Sub-Saharan countries (16). There was high service uptake among AGYW enrolled in the in-school program compared to the out of school program. The DREAMS program through the in-school activities equips AGYW with knowledge and refers them for services. In Kenya and South Africa, in-school AGYW were to have a lower vulnerability (17, 18).
Most of the AGYW referred using the mHealth innovation accessed HTS and RH services within 5 days, compared to less than a quarter among those referred using the paper-based system. Those enrolled into the mHealth platform received constant reminders, which could have prompted service uptake. Moreover, availability of service directories, which are booklets with names and contact details of service providers, and the use of mHealth in tracking and following clients equipped the AGYW with the tools to access services. The study findings are consistent with the findings for other health interventions from South Africa, where mHealth was preferred among AGYW because it is user-friendly, appeals to youth, and has led to short turnaround times for accessing family planning and HIV self-test services in South Africa (19, 20).
Limitations
This study has limitations. Completion of service referrals is based on data on referrals captured in DHIS, and some referral slips could have been lost before capture. The analysis was limited to AGYW enrolled into the DREAMS project covering only six districts in a country with more than 57 districts, which makes it difficult to generalize findings beyond study districts. In addition, the analysis used routinely collected program data thereby limiting analysis to variables captured in the database.
Conclusion and Recommendations
The study highlights the utility of mHealth in increasing the uptake of HTS and RH services among AGYW. The use of mHealth was effective in reducing the turnaround time from the time of referral to completion among AGYW referred for HTS and RH services and should be expanded to other districts and also to other health services targeting especially youth.
Data Availability Statement
The original contributions generated for in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical Research Council of Zimbabwe. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
DD, BN, and FM development of the manuscript. TT and GN review of manuscript. ET manuscript development and review. MM data analysis and review of manuscript. TN manuscript development. MP development of manuscript and review. FHM development of manuscript, data analysis, and review of manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
FHI 360 and Zimbabwe Health Interventions receives financial support from the USAID (AID - 61- A- 16 – 00001), and the authors are grateful for the support of the Zimbabwe Ministry of Health and Child Care. Appreciation also goes to the study participants and the DREAMS project staff who worked tirelessly to make this study a success.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frph.2021.656351/full#supplementary-material
Abbreviations
AGYW, Adolescent Girls and Young women; AIDS, Acquired Immunodeficiency Syndrome; ART, Antiretroviral Therapy; CeSHHAR, Center for Sexual Health and HIV and AIDS Research; DREAMS, Determined Resilient Empowered AIDS-Free Mentored and Safe; DHIS2, District Health Information System version 2; FHI360, Family Health International; FP, Family Planning; GBV, Gender-based Violence; HIV, Human Immunodeficiency Virus; HTS, HIV Testing Services; IQR, Interquartile Range; mHealth, Mobile health; MOHCC, Ministry of Health and Child Care; MRCZ, Medical Research Council of Zimbabwe; NGO, Non-governmental Organizations; OOSCF, Out of School Club Facilitators; PEP, Post-Exposure Prophylaxis; PrEP, Pre-Exposure Prophylaxis; PSI, Population Services International; RH, Reproductive Health; SMS, Short Messages Services; SRN, Service Referral Network; SPSS, Statistical Package for the Social Sciences; STI, Sexually Transmitted Infection; TB, Tuberculosis; USAID, United States Agency for International Development; ZHI, Zimbabwe Health Interventions; ZNFPC, Zimbabwe National Family Planning Council.
References
1. Butts SA, Parmley LE, Alcaide ML, Rodriguez VJ, Kayukwa A, Chitalu N, et al. Let us fight and support one another: adolescent girls and young women on contributors and solutions to HIV risk in Zambia. Int J Womens Health. (2017) 9:727–37. doi: 10.2147/IJWH.S142232
2. Evans C, Turner K, Suggs L, Occa A, Juma A, and Blake H. Developing a mHealth intervention to promote uptake of HIV testing among African communities in the UK: a qualitative study. BMC Public Health. (2016) 16:656. doi: 10.1186/s12889-016-3580-1
3. WHO. Consolidated Guidelines on HIV Testing Services, 5Cs: Consent, Confidentiality, Counselling, Correct Results and Connection. Geneva: World Health Organisation (2015).
4. Donner J, and Mechael P. mHealth in Practice: Mobile Technology for Health Promotion in the Developing World. London: Bloomsbury (2013).
5. Mulawa MI, LeGrand S, and Hightow-Weidman LB. eHealth to enhance treatment adherence among youth living with HIV. Curr HIV/AIDS Rep. (2018) 15:336–49. doi: 10.1007/s11904-018-0407-y
6. Lenhart A Pew Research Center. Teen, Social Media and Technology Overview. Lenhart A Pew Research Center, Washington DC (2015).
7. Pew Research Center. Emerging Nations Embrace Internet, Mobile Technology. Pew Research Center, Washington DC (2014).
8. Odeny T, Bukusi E, Cohen C, Yuhas K, Camlin C, and McClelland R. Texting improves testing: a randomised trial of 2 way SMS to increase postpartum prevention of mother to child transmission retention and infant testing. AIDS. (2014) 28:2307–12. doi: 10.1097/QAD.0000000000000409
9. De Tolly K, Skinner D, Nembaware V, and Benjamin P. Investigation into the use of short message services to expand uptake of human immunodeficiency virus testing, and whether content and dosage have impact. J Telemed E-Health. (2012) 18:18–23. doi: 10.1089/tmj.2011.0058
10. Kamau KJ, Osuga BO, and Njuguna S. Challenges facing implementation of referral system for quality health care services in Kiambu County, Kenya. Health Syst Policy Res. (2017) 4:1. doi: 10.21767/2254-9137.100067
11. Ramdas PD. A Framework for a Referral System for Health Service Delivery in Kwazulu-Natal. Province of Kwa Zulu-Natal Health Services, Pietermaritzburg (2003).
12. Linnemayr S, Huang H, Luoto J, Kambugu A, Thirumurthy H, Haberer JE, et al. Text messaging for improving antiretroviral therapy adherence: no effects after 1 year in a randomized controlled trial among adolescents and young adults. Am J Public Health. (2017) 107:1944–50. doi: 10.2105/AJPH.2017.304089
13. Evans C, Turner K, Blake H, Juma A, Suggs S, and Occa A. Text messaging to encourage uptake of HIV testing amongst African communities: findings from a theory based feasibility study. HIV Med. (2015) 16(Suppl. 2):54. doi: 10.1111/hiv.12265
14. Saberi P, Siedle-Khan R, Sheon N, and Lightfoot M. The use of mobile health applications among youth and young adults living with HIV: focus group findings. AIDS Patient Care STDs. (2016) 30:254–60. doi: 10.1089/apc.2016.0044
15. De Tolly K, Skinner D, Nembaware V, and Benjamin P. Investigation into the use of short message services to expand uptake of human immunodeficiency virus testing, and whether content and dosage have impact. J Telemed E-Health. (2012) 18:18–23 doi: 10.1177/0956474812441141
16. Mathur S, Pilgrim N, Patel SK, Okal J, Mwapasa V, Chipeta E, et al. HIV vulnerability among adolescent girls and young women: a multi-country latent class analysis approach. Int J Public Health. (2020) 65:399–411. doi: 10.1007/s00038-020-01350-1
17. Gourlay A, Birdthistle I, Mthiyane NT, Orindi BO, Muuo S, Kwaro D, et al. Awareness and uptake of layered HIV prevention programming for young women: analysis of population-based surveys in three DREAMS settings in Kenya and South Africa. BMC Public Health. (2019) 19:1417. doi: 10.1186/s12889-019-7766-1
18. Pulerwitz J, and Mathur S. Emerging evidence on AGYW HIV risk and prevention from the DREAMS partnership: the role of gender. In: International AIDS Conference 24 July 2018. Amsterdam (2018).
19. Jonas K, Duby Z, Maruping K, Dietrich J, Slingers N, Harries J, et al. Perceptions of contraception services among recipients of a combination HIV-prevention interventions for adolescent girls and young women in South Africa: a qualitative study. Reprod Health. (2020) 17:122. doi: 10.1186/s12978-020-00970-3
Keywords: mHealth, referral, AGYW, services, dreams, community
Citation: Dhakwa D, Mudzengerere FH, Mpofu M, Tachiwenyika E, Mudokwani F, Ncube B, Pfupajena M, Nyagura T, Ncube G and Tafuma TA (2021) Use of mHealth Solutions for Improving Access to Adolescents' Sexual and Reproductive Health Services in Resource-Limited Settings: Lessons From Zimbabwe. Front. Reprod. Health 3:656351. doi: 10.3389/frph.2021.656351
Received: 20 January 2021; Accepted: 10 May 2021;
Published: 28 September 2021.
Edited by:
Lynda Stranix-Chibanda, University of Zimbabwe, ZimbabweReviewed by:
Franco Cavallo, University of Turin, ItalyDaniel B. Lee, University of Michigan, United States
Copyright © 2021 Dhakwa, Mudzengerere, Mpofu, Tachiwenyika, Mudokwani, Ncube, Pfupajena, Nyagura, Ncube and Tafuma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dominica Dhakwa, ZGRoYWt3YUBmaGkzNjAub3Jn
†These authors have contributed equally to this work and share first authorship