 Mohammed Yuya
Mohammed Yuya Hassen Abdi Adem
Hassen Abdi Adem Nega Assefa
Nega Assefa Addisu Alemu1‡
Addisu Alemu1‡ Abdurezak Adem Umer
Abdurezak Adem Umer Lemessa Oljira
Lemessa Oljira- 1School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 2School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
- 3Department of Public Health, College of Medicine and Health Sciences, Dire Dawa University, Dire Dawa, Ethiopia
Background: Globally, two-thirds of pre-mature deaths and one-third of the total disease burden in adults are associated with problems that began in adolescent and youth. Global and national acting educational and health policies, strategies, and programs designed to promote, implement, and improve adolescent and youth sexual and reproductive health services utilization should be responsive, consider the knowledge of reproductive rights and risk factors. This study assessed the level and predictors of knowledge of reproductive rights among Haramaya University students in Ethiopia.
Methods: An institution-based cross-sectional study was conducted among randomly selected Haramaya University students from March 1 to 24, 2018. A self-administered pre-tested structured questionnaire was used to collect data from participants. Data were entered using EpiData version 3.1 and analyzed using SPSS version 24. Bivariable and multivariable logistic regression analyses were conducted to identify factors associated with knowledge of reproductive rights. Adjusted odds ratio (AOR) with 95% CI was used to report association and significance was declared at P-value < 0.05.
Results: Of 822 total students invited to the study, 812 (98.8%) respondents participated in the study. A total of 424 students (52.2%, 95% CI: 48.8, 55.4%) had an above-average level of knowledge on reproductive rights. Participants who were in the fourth and above year of the study [AOR = 2.37 (1.58, 3.54)], whose father's had higher education [AOR = 1.89 (1.27, 2.80)], who came from rich families [AOR = 1.54 (1.07, 2.21)], in the health faculty [AOR = 3.37 (2.17, 5.23)], utilized reproductive health services [AOR = 2.81 (2.21, 4.98)] and participated in reproductive health club [AOR = 1.77 (1.27, 2.47)] were significantly associated with knowledge of reproductive rights.
Conclusion: Around half of the participants knew reproductive rights. In this study, lack of awareness (information) on reproductive health issues and absence of reproductive health services utilization were strong independent predictors of knowledge of reproductive rights.
Introduction
Reproductive rights are the basic rights of all couples and individuals to decide freely and responsibly the number, spacing, and timing of their children and to have the information and means to do so, and the right to attain the highest standard of sexual and reproductive health (1, 2). It includes the right to decide on reproduction and sexuality free from discrimination, coercion, and violence (2, 3), and is the cornerstone to empowering people to make informed healthcare decisions (1, 2).
Reproductive right literacy is a key life-saving public health intervention to reduce adolescent and youth morbidity and mortality in today's world (1, 3). Globally, universal access to reproductive right literacy increases opportunities for youth to have informed choice and appropriate decisions regarding their sexual and reproductive well-being, which decreases early marriage and childbirth by 11%, unintended pregnancy by 70%, unsafe abortion by 14%, and HIV/AIDS by 34% (1, 2). In Africa, reproductive right literacy of adolescents and youth prevents the unmet need for contraceptives by 30%, sexual violence by 32%, and HIV/AIDS by 50% (3).
Youths are individuals in a period of transition from childhood to adulthood, between the ages of 15 and 24 years, during which they undergo biological and psychological transitions to attain reproductive capability and become sexually active (4, 5). Inadequate information on reproductive rights exposes youths to multiple problems that have several negative impacts on their health in the adulthood period (6). For instance, unprotected sex, sexually transmitted infections, unwanted pregnancy, violence, and risky behaviors contribute to 17% of the global burden of disease in all ages. Youths are highly vulnerable to unprotected sex, the second leading risk factor for morbidity and deaths in developing countries (2, 3, 7–9). The magnitude of unintended pregnancy is 21% in Ethiopia (10), 26.1% in Addis Ababa, and 41.5% in the Oromia region (11). The median childbearing age range from 15 to 19 years and thus, 45% of total births in Ethiopia occur among adolescent and young women.
In Ethiopian higher education institutions, less than half (46%) of students had reproductive health literacy and 26.9% had knowledge about sexually transmitted infections, 16.5% know about family planning, 14.3% knew access to healthcare services and only 8.6% knew the right to choose when and with whom to have sex (12). In another study, 45.5% of students know reproductive rights; 21.8% had not discussed the sexual and reproductive issues with their partners or healthcare providers or peers (13). A survey conducted in Haramaya University revealed that among sexually active participants, 11.6% had multiple sexual partners and 16.3% of males had sex with commercial sex workers (14). Another study shows, two of six participants did not know the meaning of reproductive health literally (15).
Several barriers that make youth unable to deal with sexual and reproductive violence include shame, guilt, embarrassment, not want to know by friends and family; lack of confidentiality; and fear of being not believed and culturally stigmatized and discriminated (8). The other barrier is lack of information on sexual health among youth may lead to different types of health risks and social problems (16). Globally, studies show higher socioeconomic status is related to the better chance of having sexual and reproductive information (2, 3, 9, 17, 18) through accessing different media and visiting health facilities and seeking related healthcare services, which directly or indirectly invest on sexual and reproductive health issues (2, 3, 8, 9, 17–20). On the other hand, previous studies conducted in Ethiopia were more focused on the utilization of sexual and reproductive health services (18, 20, 21) which could be difficult to increase unless we boosted youth sexual and reproductive health literacy (1–3, 9).
However, overall little information was available on knowledge of reproductive rights and associated factors in Ethiopia and the study setting. In addition, addressing sexual and reproductive health needs and problems of youths has been a priority intervention in population and development policies of low- and middle-income countries including Ethiopia. Moreover, acting worldwide and national educational and public health policies, strategies, and activities developed to promote and improve the level of knowledge of sexual and reproductive health and related rights for the better outcome and fighting preventable adolescents and youth morbidity and deaths would be essential (1–3, 9). Therefore, this study assessed the level and predictors of knowledge of reproductive rights among Haramaya University students in eastern Ethiopia in 2018.
Materials and Methods
Study Design and Setting
An institution-based cross-sectional study was conducted at Haramaya University in Ethiopia from March 1 to 24, 2018. Haramaya University is found in the East Hararghe Zone at 510 km East of Addis Ababa, Capital of Ethiopia. Haramaya University, the second oldest University in Ethiopia, was established in 1954. During the study period, University has two campuses, 11 colleges, and 55 departments running 188 academic programs for a total of 16,437 regular students in the undergraduate program's study. University has one teaching tertiary hospital and four medium clinics providing basic health services for the students, staff, and surrounding communities. Haramaya University has different youth clubs such as reproductive health and anti-HIV/AIDs clubs (22).
Population and Eligibility Criteria
All undergraduate students in Haramaya University were the source population. Randomly selected undergraduate students in Haramaya University during the study period constituted the study population. Students enrolled in the regular undergraduate program and aged 18 years and above were included while critically sick participants who could not respond and absented from the regular class sessions were excluded.
Sample Size and Sampling Procedure
The sample size was calculated using Epi Info version 7.1 using a single population proportion with the following assumptions: confidence level with 95%, assumed 54.4% proportion of knowledge of reproductive rights among university students (13) 5% margin of error, the significance level of 0.05 design effect of 2 with a 10% non-response proportion. Accordingly, a minimum of 822 students was required to conduct the study.
A multistage stratified sampling technique was used to select the study participants. First, Haramaya University was stratified by campus (Main Campus and Harar Campus) and then, the sample size was proportionally allocated to each campus. Then, allocated samples to each campus was proportionally allocated to their respective college, school, department, and program/unit found under each campus along with their years of the study, using the actual number of learning undergraduate students reviewed from the latest students lists or registrations available in the Associate Registrar Office of Haramaya University during the study period, 2018. We prepared a sampling frame for each faculty/college and finally, the participants were drawn by systematic sampling technique (Supplementary File 1).
Data Collection Tool and Measurement
Pre-tested structured questionnaires adapted from related published literature (13) were used to collect data from participants. The questionnaire contains information on sociodemographic factors (age, sex, ethnicity, religion, marital status, address, family size, paternal and maternal education, paternal and maternal main occupation, and the wealth index of the family) school-related factors (type of school attended in lower education, college of the study, and year of the study) and reproductive factors (history of sexual experience, age and time at first sex, number of sexual partners, heard about sexual and reproductive health information and their main source of information, participating on the reproductive health club, discussion about sexual and reproductive health issues, and advised on sexual and reproductive health issue and utilization of sexual and reproductive health service) and knowledge of reproductive rights (Supplementary File 2).
Knowledge of Reproductive Rights
It was measured using 24 dichotomous yes/no items asking about knowledge of reproductive rights. The response of each item was re-coded “1” when participants responded a right response and “0” point when the participant responded a wrong response and then, composite index score was summed from a total of 24 points, and participants who scored the mean and above were considered to know reproductive rights and not unless otherwise (13).
Wealth Index
It was assessed by a standard instrument containing 36 dichotomous (yes/no) items asking about three domains of the family's wealth level (domestic animals, durable assets, other productive assets, and housing conditions). We observed high internal consistency among items (Cronbach α = 0.81) and principal component analysis using the varimax rotation method to compute estimate composite wealth index factors and the wealth status of the participants.
Data Collection Procedure
Data were collected paper-based through a self-administrated interview conducted over near a month. Ten health professionals holding Bachelor of Science degree in Nursing facilitated the overall data collection and two public health experts holding master's degrees in Public Health were supervised data collection with the principal investigator. The study participants have filled the questionnaire at the same time in lecture halls.
Data Quality Control
To maintain the data quality, questionnaires were adapted from standard tools and related published works of literature. We pre-tested the tools on 5% of the total sample (41 undergraduate students) to check the validity of the questionnaire in Dire Dawa University, Ethiopia. Data were entered using EpiData version 3.1 software. In field, strict supervision of data collectors and validation of collected data were carried out by supervisors and principal investigators.
Data Processing and Analysis
After checking for completeness, data were entered into EpiData version 3.1 and analyzed using SPSS version 24. Descriptive statistics such as frequencies, the measure of central tendency, and measures of dispersion were used to characterize the participants. Before any analysis, the internal consistency of items used to measure each composite index was checked by reliability analysis (using Cronbach's α). Principal component analysis with the varimax rotation method was used to estimate composite wealth index score and wealth status of the family of participant. All predictors with P-value < 0.25 in the bivariable analysis were considered in our multivariable analysis (23, 24). Multivariable logistic regression analyses were conducted (using the backward stepwise method) to identify factors associated with knowledge of reproductive rights. Adjusted odds ratio (AOR) (95% CI) was used to report strengthen of association and significance was declared at P-value < 0.05.
Results
Characteristics of Participants
A total of 812 (98.8%) students were involved in the study. About 521 (64.2%) participants were male. The majority, 710 (87.4%) of participants were in the age group of between 20 and 24 years. The mean age ± SD of the participants was 21.35 ± 1.40 years. Four out of 10 (40.6%) participants had mothers who have no formal education, 33.3% were students from a poor family and 72.9% attended their education at governmental schools before joining University (Table 1).
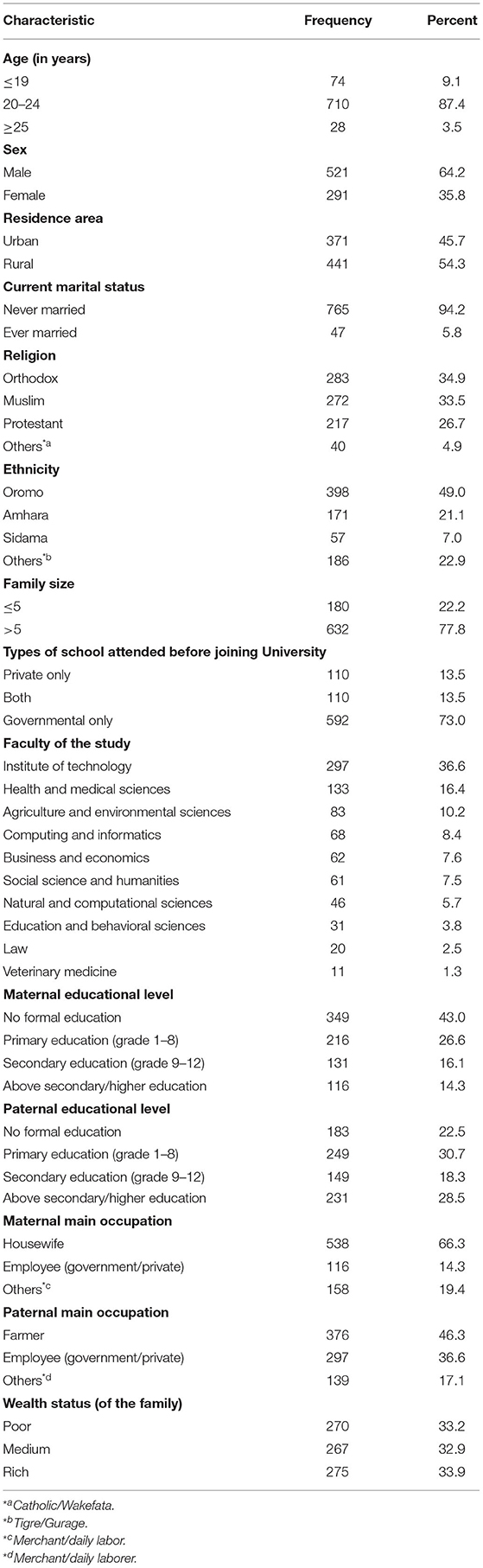
Table 1. Sociodemographic characteristics of Haramaya University students, Eastern Ethiopia, 2018 (n = 812).
Nearly one-third, 264 (32.5%) of the participants had sexual experience. Over three-fourth (77.6%) of participants visited health facilities in the university; 35.6% were counseled on reproductive health issues; 33.7% of participants used reproductive healthcare; and 49.1% of them discussed reproductive health issues with their parents (Table 2).
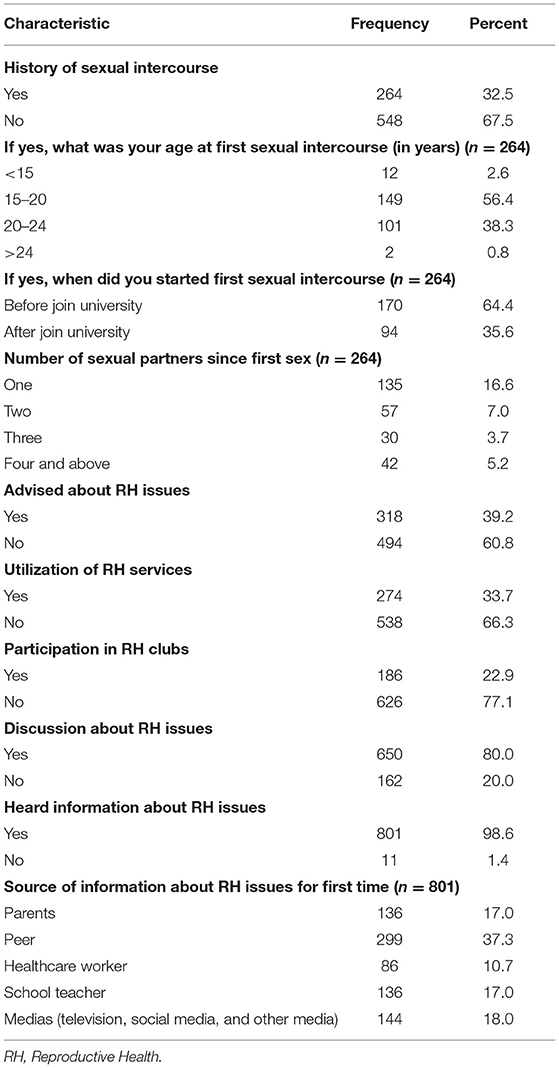
Table 2. Reproductive health related factors of Haramaya University students, Eastern Ethiopia, 2018 (n = 812).
Knowledge of Reproductive Rights
Initially, we checked for the internal consistency among 24 yes/no items used to assess the level of knowledge of reproductive rights. We found internally consistent items (Cronbach's α = 0.73). The mean (±SD) score of knowledge of reproductive rights was 14.36 ± 3.65. About 424 (52.2%) participants knew reproductive rights (95% CI: 48.8, 55.4%) in the setting.
Predictors of Knowledge of Reproductive Rights
In the bivariable analysis, residence area, maternal education, type of the school, year of the study, faculty, and wealth status, utilization of reproductive health service and participating on the reproductive health club, counseling on reproductive health issues, and discussion on reproductive health issue were associated with knowledge of reproductive rights at P-value < 0.05. All independent variables with P-value < 0.25 in the bivariable analysis were included in our multivariable analysis model (Table 3).
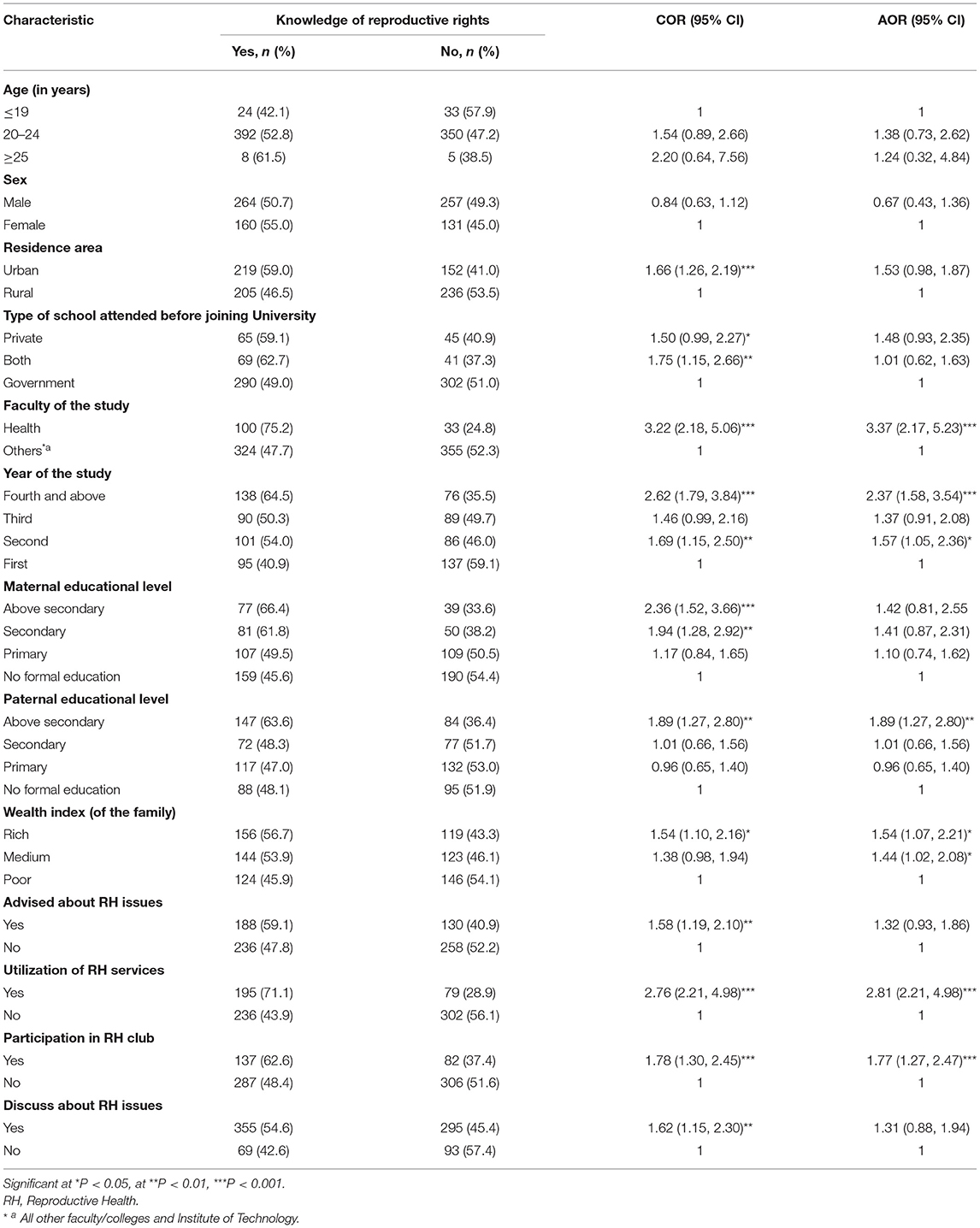
Table 3. Factors associated with knowledge of reproductive rights among Haramaya University students, Eastern Ethiopia, 2018 (n = 812).
In the multivariable analysis, the odds of knowledge of reproductive rights was two [AOR = 2.37 (1.58, 3.54)] and one and a half [AOR = 1.57 (1.05, 2.36)] times higher among students in the second and fourth and above year of the study compared to students in the first year. The odds of knowledge of reproductive rights was nearly two times [AOR = 1.89 (1.27, 2.80)] higher among students whose fathers had higher education compared to those whose fathers had no formal education. The odds of knowledge of reproductive rights was 44% [AOR = 1.44 (1.02, 2.08)] and 54% [AOR = 1.54 (1.07, 2.21)] higher among students who came from medium and rich families compared to those who came from poor families. The odds of knowledge of reproductive rights was three times [AOR = 3.37 (2.17, 5.23)] higher among students who were in the health faculty compared to those in non-health faculties. The odds of knowledge of reproductive rights was nearly three times [AOR = 2.81 (2.21, 4.98)] higher among students who ever used reproductive health services compared to those who did not use them. The odds of knowledge of reproductive rights was nearly two times [AOR = 1.77 (1.27, 2.47)] higher among students who participated in reproductive health clubs compared to those who did not (Table 3).
Discussion
We investigated the magnitude of knowledge of reproductive rights and associated factors among Haramaya University students. In this study, more than half (52.2%) of the participants know about reproductive rights. Knowledge of reproductive rights among Haramaya University students was positively and significantly associated with being in the fourth and above year of the study, paternal higher education, being from the health faculty, coming from the rich and medium families, utilization of reproductive health service, and participation in the reproductive health club.
This study revealed that around one out of two (52.2%) students knew reproductive rights. This finding is somewhat similar to institution-based cross-sectional studies conducted in Wolaita Sodo, southern Ethiopia (54.5%) (13), southwest Nigeria (60.3%) (19), and Nepal (83.3%) (25). However, this finding is higher than a community-based cross-sectional study conducted in the Shire, northern Ethiopia (47.1%) (26). This variation might be explained by the methodological differences across the conducted studies. For instance, the Nigerian study used fewer items to measure the level of knowledge of reproductive rights (19), and also the Nepal study with better sexual reproduction knowledge use the scale with a lower number of items to assess the knowledge of reproductive rights (25). Moreover, the observed variation could also be due to the differences in the study settings and the differences in educational status, set-up, and sociocultural characteristics of the study population across the studies.
In this study, knowledge of reproductive rights was 2-folds higher among students in the fourth and above years of the study compared to those in the first year. This could be explained by the fact that the chance of getting information, and participating in and discussing reproductive health issues rise as the duration of stay in the campus increased as seen in the Shire, northern Ethiopia (26), and Thailand (27).
Paternal educational level has a significant association with knowledge of reproductive rights. Students whose fathers had higher education were nearly 2-folds more likely to know reproductive rights than those whose fathers had no education. This is supported by a cross-sectional study conducted in Riyadh, Saud Arabia revealed that students who discussed with educated families were more likely to know reproductive rights than students who discussed with uneducated families (16).
In this study, the wealth status of the family had a significant association with knowledge of reproductive rights. Knowledge of reproductive rights was around 2- and 3-folds higher when the participants came from medium and rich families compared to those who came from poor families. This finding was lower than the cross-sectional study conducted in East Gojjam, northern Ethiopia, which was 3-folds higher odds of knowledge of reproductive rights (15). This discrepancy in the effect size between studies could be since that students who had a family with a higher socioeconomic class could have a higher income and a better chance of access to different media and information. In addition, this finding could be supported by the cross-sectional study conducted in Wolaita Sodo, southern Ethiopia which reported students who came from the urban area were more likely to know reproductive rights than those who came from the rural area. Since most of the urban populations are high in economic status than rural populations (13).
In this study, knowledge of reproductive rights was 3-folds higher among students who were in the health faculty compared to the non-health faculties. This is consistent with the cross-sectional study done in Wolaita Sodo University, which reported 3-folds higher knowledge of reproductive rights among students who come from the health faculty (13).
In this study, uptake of reproductive health services was positively and significantly associated with the higher odds of knowledge of reproductive rights. Students who used reproductive health services were three times more likely to know reproductive rights. This was lower than the finding of a cross-sectional study done in southern Ethiopia and the possible reason for the discrepancy could be due to the higher chance of receiving counseling by healthcare workers before utilization and giving more attention to know what they use (13).
In this study, participating in the reproductive health club was associated with nearly 2-folds higher odds of knowledge of reproductive rights. This could be since those who participated in reproductive health clubs could get new and updated information and policies established on reproductive health and related rights early on time which supported by cross-sectional studies done in South Africa (4), the Shire, northern Ethiopia (26) and Wolaita Sodo, southern Ethiopia (13).
As a strength, this study used a large sample size and multistage stratified sampling given we included participants from different parts of the country. This study also shared the limitation of cross-sectional studies; the difficulty of determining the causal relationship between variables and the study findings also could not be generalized to undergraduate students in private universities in Ethiopia. The cross-sectional studies require the potential abilities of respondents to remember information retrospectively, recall bias also other limitations of this study. However, scientific procedures were employed to minimize possible effects. In addition, a pre-test of the data tool, supervision, and adequate training for data collectors and supervisors were utilized.
Conclusions
This study revealed that about half (52.2%) of Haramaya University students knew reproductive rights. In this study, being in the fourth and above year of the study, paternal higher education, being from medium and rich families, in the health faculty, using reproductive health services, and participating in reproductive health clubs were factors associated with knowledge of reproductive rights. Based on the findings, Ethiopian higher education institutions should collaborate with the ministry of health in providing reproductive and sexual rights-related courses for non-health discipline students. The district health office should collaborate with Haramaya University in providing quality reproductive health services for youth students. Public health facilities at different levels should encourage students to actively participate in reproductive health issues in collaboration with existing higher education facilities. Healthcare service providers at all levels should focus on providing quality reproductive health services and arranging special education and counseling programs for all discipline students on sexual and reproductive rights. Very importantly, continuous support and promotion of youth health clubs would be essential, sustainable, and feasible options to promote knowledge and access to sexual and reproductive healthcare services and rights.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Institutional Health Research Ethical Review Committee of College of Health and Medical Sciences, Haramaya University approved the protocol of the study (Ref. No: IHRERC/028/2018). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
MY, HAA, NA, LO, AA, and AAU participated in the conception of the idea, designing the study, data collection and analysis, writing up the draft results, reanalyzed the data, drafted, edited, and revised the manuscript. All authors agree to take responsibility and be accountable for the contents of the article, agree on the journal to which the article will be submitted, and read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank participants, data collectors, and supervisors for their endless cooperation and contribution during conducting the study. The authors would also appreciate Haramaya University for providing the opportunity to conduct the study and providing the background information.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frph.2021.641008/full#supplementary-material
Abbreviations
AOR, adjusted odds ratio; HIV, human immune deficiency virus; IHRERC, Institution Health Research Ethical Review Bureau; RH, reproductive health; WHO, World Health Organization.
References
1. WHO. World Health Organization Recommendations on Adolescent Sexual and Reproductive Health and Rights. Geneva: World Health Organization; Licence: CC BY-NC-SA 3.0 IGO (2018).
2. IPPF UNFPA. Global Sexual and Reproductive Health Service Package for Men and Adolescent Boys. London: IPPF; New York, NY: UNFPA (2017).
3. UNFPA. The Power of 1.8 Billion: Adolescents, Youth and the Transformation of the Future Sub-Saharan Africa. UNFPA (2014).
4. Griffin S. Literature Review on Sexual and Reproductive Health Rights: Universal Access to Services, Focussing on East and Southern Africa and South Asia. Panos, London: Department for International Development (2006).
5. WHO. Key Issues in the Implementation of Programs for Adolescent Sexual and Reproductive Health. Geneva: WHO (2004).
6. Santosa MJ, Ferreirab E, Ferreirac M. Knowledge of and Attitudes Toward Sexual and Reproductive Health Among College Students. Amsterdam: Elsevier (2016). p. 188–94.
7. International Council. Sexuality and Human Rights Discussion paper International Council on Human Rights Policy. International Council (2009).
8. Mbeba RM, Mkuye MS, Magembe GE, Yotham WL, Mellah Ao, Mkuwa SB. Barriers to sexual reproductive health services and rights among young people in Mtwara district, Tanzania: a qualitative study. Pan Afr Med J. (2012) 13(Supp 1):13.
9. WHO. Global Accelerated Action for the Health of Adolescents (AA-HA!): Guidance to Support Country Implementation. Annexes 1-6 and Appendices I-IV. Geneva: World Health Organization. Licence: CC BY-NC-SA 3.0 IGO (2017).
10. EDHS. Central Statistical Agency (CSA) [Ethiopia] and ICF 2016. Addis Ababa; Rockville, MD: CSA; ICF: Ethiopia Demographic and Health Survey (2016).
11. Fite RO, Mohammedamin A, Abebe TW. Unintended pregnancy and associated factors among pregnant women in Arsi Negele Woreda, West Arsi Zone, Ethiopia. BMC Res Notes. (2018) 11:671. doi: 10.1186/s13104-018-3778-7
12. Yemaneh Y, Gezahagn R, Yechale M, Assefa M, Abrha K, Abdias A, et al. Assessment of knowledge, attitude and practice towards reproductive health service among Mizan Tepi Universtiy Tepi Campus Students, Sheka Zone, South Nations Nationalities and Peoples Regional State, South West Ethiopia, 2017. J Hosp Med Manag. (2017) 3:11. doi: 10.4172/2471-9781.100030
13. Adinew YM, Worku AG, Mengesha ZB. Knowledge of reproductive and sexual rights among University students in Ethiopia. BioMed Central. (2013) 13:12. doi: 10.1186/1472-698X-13-12
14. Derese A, Seme A, Misganaw C. Assessment of substance use and risky sexual behaviour among Haramaya University Students, Ethiopia. Sci J Public Health. (2014) 2:102–10. doi: 10.11648/j.sjph.20140202.19
15. Abajobir AA, Seme A. Reproductive health knowledge and services utilization among rural adolescents in East Gojjam Zone, Ethiopia. BioMed Central. (2014) 14:138. doi: 10.1186/1472-6963-14-138
16. AlQuaiz AM, Kazi A, Muneef MA. Determinants of sexual health knowledge in adolescent girls in schools of Riyadh-Saudi Arabia. BMC Women's Health. (2013) 13:19. doi: 10.1186/1472-6874-13-19
17. Asghar K. Socio-Economic and Cultural Determinants of Attitude Towards Reproductive Health Rights in Punjab. Pakistan: University of Agriculture. (2010).
18. Alehegn BG, Mulunesh TT, Yilkal TA, Abebaw AG. Sexual and reproductive health services utilization and associated factors among preparatory school students in Mecha District, Northwest Ethiopia: cross sectional study. J Gynecol Women Health. (2018) 11:555824. doi: 10.19080/JGWH.2018.11.555824
19. Ogunla MA. An assessment of the awareness of sexual and reproductive rights among adolescents in South Western Nigeria. Afr J Reprod Health. (2014) 9:99–112. doi: 10.2307/3583164
20. Dida N, Darega B, Takele A. Reproductive health services utilization and its associated factors among Madawalabu University students, Southeast Ethiopia: cross-sectional study. BMC Res Notes. (2015) 8:8. doi: 10.1186/s13104-015-0975-5
21. Atnafu A, Kebede A, Tessema GA, Emiru K, Berihun T, Asmamaw T, et al. Sexual and reproductive health services utilization and associated factors among university students, Northwest Ethiopia: cross sectional study. J Gynecol Women Health. (2019) 15:555915. doi: 10.19080/JGWH.2019.15.555915
22. HU. Haramaya University Office of the Vice-President for Academic Affairs. Statistics on Academic Programs, Student Enrollment, Staff Profile, and Teaching Resources (2010-2017). Haramaya: Haramaya University (2017).
23. Zhang Z. Model building strategy for logistic regression: purposeful selection. Ann Transl Med. (2016) 4:111. doi: 10.21037/atm.2016.02.15
24. Mickey RM, Greenland S. The impact of confounder selection criteria on effect estimation. Am J Epidemiol. (1989) 129:125–37. doi: 10.1093/oxfordjournals.aje.a115101
25. Bhattarai M, Dhakal R. Knowledge regarding reproductive rights among undergraduate students. Sch J App Med Sci. (2015) 3:2461–5.
26. Gebretsadik GG, Weldearegay GG. Knowledge on reproductive and sexual rights and associated factors among youths, Shire town, Tigray, Northern Ethiopia. Int J Res Pharm Sci. (2016) 6:30–7.
Keywords: knowledge, reproductive rights, youths, students, Haramaya University, Ethiopia
Citation: Yuya M, Adem HA, Assefa N, Alemu A, Umer AA and Oljira L (2021) Level and Predictors of Knowledge of Reproductive Rights Among Haramaya University Students, Eastern Ethiopia: A Cross-Sectional Study. Front. Reprod. Health 3:641008. doi: 10.3389/frph.2021.641008
Received: 13 December 2020; Accepted: 18 October 2021;
Published: 24 November 2021.
Edited by:
Oliver Chukwujekwu Ezechi, Nigerian Institute of Medical Research (NIMR), NigeriaReviewed by:
Daniel B. Lee, University of Michigan, United StatesNatsayi Chimbindi, Africa Health Research Institute (AHRI), South Africa
Copyright © 2021 Yuya, Adem, Assefa, Alemu, Umer and Oljira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hassen Abdi Adem, aGFzc2VueGlxcWEzMkBnbWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship