
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Reprod. Health , 20 January 2021
Sec. Assisted Reproduction
Volume 2 - 2020 | https://doi.org/10.3389/frph.2020.618838
This article is part of the Research Topic Luteal Phase Support for Assisted Reproduction View all 5 articles
 Panagiotis Drakopoulos1*†
Panagiotis Drakopoulos1*† Caroline Roelens1†Michel De Vos1,2
Caroline Roelens1†Michel De Vos1,2 Shari Mackens1AnnaLisa Racca1Herman Tournaye1,2
Shari Mackens1AnnaLisa Racca1Herman Tournaye1,2 Christophe Blockeel1,3
Christophe Blockeel1,3In vitro fertilization (IVF) treatment routinely involves ovarian stimulation (OS) with gonadotropins in combination with GnRH analogs to prevent premature luteinization and ovulation (1). However, it is well-established that the use of GnRH analogs during OS may impair corpus luteum function, resulting in suboptimal endometrial receptivity (2). Thus, luteal phase support (LPS) with progestins is an essential part of IVF treatment and is mandatory to support implantation and to increase pregnancy rates after fresh embryo transfer (3).
Progestins can be administered using various routes, either vaginally, intramuscularly (IM), rectally, orally, or subcutaneously, with differential impact on the pharmacokinetics of progestins. Indeed, serum progesterone (P) levels are higher when progestins are administered using the IM route compared to the vaginal one. On the other hand, although micronized P capsules had initially been developed for oral use, they can be administered vaginally, offering an effective alternative to oral and IM injections: serum P concentrations may be lower after vaginal compared to IM administration, but endometrial P levels are higher because of the uterine first pass effect, while several disadvantages of the IM route (i.e., injection site pain and discomfort, risk of infection) are avoided (4). On a similar note, vaginal micronized P is preferred over oral administration due to the rapid absorption and avoidance of the first-pass metabolism (5, 6). However, there are a number of downsides to the vaginal route of P administration, since vaginal irritation, discharge and bleeding may occur (7). Furthermore, suboptimal serum P levels in a subgroup of women who are prescribed vaginal P may be associated with reduced pregnancy rates (8). Therefore, vaginal micronized P administration should not be seen as a panacea.
In this regard, the concept of oral progestin administration in assisted reproduction technology (ART) has recently been revitalized, given that dydrogesterone (6-dehydro-retroprogesterone) has been extensively used for the treatment of other conditions associated with P deficiency since the 1960s (9). Dydrogesterone is a stereo-isomer of P, with an additional double bond between carbons 6 and 7, characterized by a better oral bioavailability and higher specificity for P receptors compared with oral micronized P (10, 11). A recent study demonstrated that after natural conception dydrogesterone supplementation from 6 to 20 weeks of gestation significantly reduced the incidence of preeclampsia (PE) in high-risk patients (12), while these findings were replicated by another retrospective study showing a reduction in PE rate after dydrogesterone supplementation in assisted reproductive techniques and intra-uterine insemination (13).
Several small-scale clinical studies have shown that oral dydrogesterone is at least as efficacious as micronized vaginal progesterone in supporting pregnancy following fresh embryo transfer (14–16). These findings revived the interest in oral dydrogesterone for LPS and paved the way for large Phase III prospective RCTs (Lotus I and Lotus II studies), which led to the recent approval of oral dydrogesterone for LPS in IVF–ART.
In particular, Lotus I was an international Phase III non-inferiority RCT including 1,034 patients undergoing IVF and fresh embryo transfer, which showed that dydrogesterone 30 mg (10 mg three times daily) resulted in comparable ongoing pregnancy rates (pregnancy rates at 12 weeks of gestation of 37.6 and 33.1% in the oral dydrogesterone and micronized vaginal P group, respectively) compared to vaginal micronized P 600 mg (200 mg three times daily) (17). Similarly, Lotus II RCT compared oral dydrogesterone 30 mg (10 mg three times daily) with 8% micronized vaginal P gel (90 mg once daily) and demonstrated non-inferiority, with ongoing pregnancy rates at 12 weeks' gestation of 38.7% in the oral dydrogesterone group and 35.0% in the micronized vaginal progesterone gel group (18). The main conclusion of the two RCTs was that oral dydrogesterone is safe (no evidence for an increased risk for fetal malformation), well-tolerated and as efficient as vaginal P.
Frozen-thawed embryo transfer (FET) has become an increasingly important part of IVF treatment, with large clinical trials and meta-analyses demonstrating similar live birth rates to those associated with fresh embryo transfer (19). To date, several methods of endometrial preparation for FET have been developed, with hormone replacement therapy (HRT)-FET cycles being the most commonly used, in view of the reduced need for treatment monitoring and easier scheduling. In HRT-FET cycles estrogen and progesterone are administered consecutively, in order to mimic the endocrine conditions of the endometrium of a normal menstrual cycle. However, from an physiological point of view, LPS in HRT-FET is completely different compared to LPS in a fresh IVF cycle due to the lack of ovulation and absence of endogenous corpora lutea, suggesting that transformation of the endometrium into a receptive state for the implanting embryo is completely dependent on exogenous P supplementation (20).
While there is robust evidence demonstrating the efficacy of oral dydrogesterone for LPS in fresh IVF cycles as mentioned above, very few small studies using inconsistent doses have evaluated the role of dydrogesterone in HRT-FET cycles [(21–24); Table 1]. In the only RCT performed up to date, Zarei et al. (22) reported lower pregnancy rates in the oral dydrogesterone group compared to the micronized vaginal P group, using doses of 20 and 800 mg, respectively. However, the lack of data with regard to the optimal dosing of oral dydrogesterone in FET-HRT, highlights the need for further studies. In view of the advancing understanding of the impact of an absent corpus luteum in FET-HRT cycles and the associated elevated risk for PE (25), dydrogesterone with its potential immunomodulatory effects (26) represents an interesting research track. Of great importance will be the development of a clinically applicable dose monitoring test for dydrogesterone and/or its metabolites, as an optimal LPS presumably lies in its individualization (8).
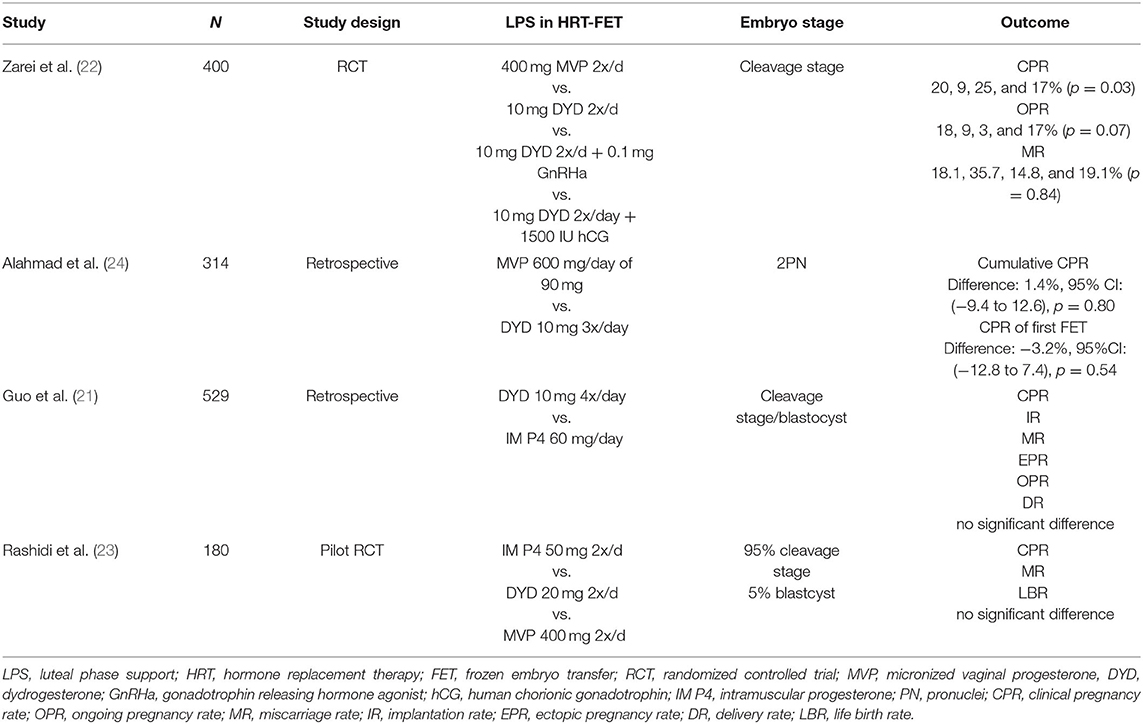
Table 1. Overview of evidence of dydrogesterone use in HRT-FET cycles.
Collectively, there is evidence that dydrogesterone has high oral bioavailability and specificity for P receptors (27), suggesting that it is effective at a dose 10–20 times lower than that of micronized P (25). Dydrogesterone has a good safety and tolerability profile with few side effects, making the ideal candidate for LPS in ART. Oral dydrogestrone is as effective as vaginal progesterone for LPS in women undergoing fresh IVF, whilst more evidence is warranted for its use in HRT cycles. The well-known widespread preference of women for an oral compound may pave the way for dydrogesterone to become the new standard. Furthermore, preliminary observations showing a decreased risk of PE after dydrogesterone supplementation in natural and intrauterine insemination cycles (12, 13) may be of paramount value in HRT-FET cycles, which are known to have a higher incidence of PE (28).
All authors contributed to this work and approved the final version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Ovarian Stimulation T, Bosch E, Broer S, Griesinger G, Grynberg M, Humaidan P, et al. ESHRE guideline: ovarian stimulation for IVF/ICSI(dagger). Hum Reprod Open. (2020) 2020:hoaa009. doi: 10.1093/hropen/hoaa009
2. Beckers NG, Laven JS, Eijkemans MJ, Fauser BC. Follicular and luteal phase characteristics following early cessation of gonadotrophin-releasing hormone agonist during ovarian stimulation for in-vitro fertilization. Hum Reproduct. (2000) 15:43–9. doi: 10.1093/humrep/15.1.43
3. Delcour C, Robin G, Delesalle AS, Drumez E, Plouvier P, Dewailly D, et al. Weekly intramuscular progesterone for luteal phase support in women receiving oocyte donation is associated with a decreased miscarriage rate. Reproduct Biomed Online. (2019) 39:446–51. doi: 10.1016/j.rbmo.2019.05.001
4. Miles RA, Paulson RJ, Lobo RA, Press MF, Dahmoush L, Sauer MV. Pharmacokinetics and endometrial tissue levels of progesterone after administration by intramuscular and vaginal routes: a comparative study. Fertility Sterility. (1994) 62:485–90. doi: 10.1016/S0015-0282(16)56935-0
5. Bulletti C, de Ziegler D, Flamigni C, Giacomucci E, Polli V, Bolelli G, et al. Targeted drug delivery in gynaecology: the first uterine pass effect. Hum Reproduct. (1997) 12:1073–9. doi: 10.1093/humrep/12.5.1073
6. Cicinelli E, de Ziegler D. Transvaginal progesterone: evidence for a new functional 'portal system' flowing from the vagina to the uterus. Hum Reproduct Update. (1999) 5:365–72. doi: 10.1093/humupd/5.4.365
7. van der Linden M, Buckingham K, Farquhar C, Kremer JA, Metwally M. Luteal phase support for assisted reproduction cycles. Cochrane Database Syst Rev. (2015) 2015:CD009154. doi: 10.1002/14651858.CD009154.pub3
8. Labarta E, Mariani G, Holtmann N, Celada P, Remohi J, Bosch E. Low serum progesterone on the day of embryo transfer is associated with a diminished ongoing pregnancy rate in oocyte donation cycles after artificial endometrial preparation: a prospective study. Hum Reproduct. (2017) 32:2437–42. doi: 10.1093/humrep/dex316
9. Backer MH Jr. Isopregnenone (Duphaston): a new progestational agent. Obstet Gynecol. (1962). 19:724–9.
10. Schindler AE. Progestational effects of dydrogesterone in vitro, in vivo and on the human endometrium. Maturitas. (2009) 65(Suppl. 1):S3–11. doi: 10.1016/j.maturitas.2009.10.011
11. Rizner TL, Brozic P, Doucette C, Turek-Etienne T, Muller-Vieira U, Sonneveld E, et al. Selectivity and potency of the retroprogesterone dydrogesterone in vitro. Steroids. (2011) 76:607–15. doi: 10.1016/j.steroids.2011.02.043
12. Tskhay V, Schindler A, Shestakova M, Klimova O, Narkevich capital A C. The role of progestogen supplementation (dydrogesterone) in the prevention of preeclampsia. Gynecol. Endocrinol. (2020) 36:698–701. doi: 10.1080/09513590.2019.1706085
13. Ali AB, Ahmad MF, Kwang NB, Shan LP, Shafie NM, Omar MH. Dydrogesterone support following assisted reproductive technique (ART) reduces the risk of pre-eclampsia. Horm Mol Biol Clin Investig. (2016) 27:93–6. doi: 10.1515/hmbci-2015-0063
14. Ganesh A, Chakravorty N, Mukherjee R, Goswami S, Chaudhury K, Chakravarty B. Comparison of oral dydrogestrone with progesterone gel and micronized progesterone for luteal support in 1,373 women undergoing in vitro fertilization: a randomized clinical study. Fertility Sterility. (2011) 95:1961–5. doi: 10.1016/j.fertnstert.2011.01.148
15. Chakravarty BN, Shirazee HH, Dam P, Goswami SK, Chatterjee R, Ghosh S. Oral dydrogesterone vs. intravaginal micronised progesterone as luteal phase support in assisted reproductive technology (ART) cycles: results of a randomised study. J Steroid Biochem Mol Biol. (2005) 97:416–20. doi: 10.1016/j.jsbmb.2005.08.012
16. Tomic V, Tomic J, Klaic DZ, Kasum M, Kuna K. Oral dydrogesterone vs. vaginal progesterone gel in the luteal phase support: randomized controlled trial. Eur J Obstetr Gynecol Reproduct Biol. (2015) 186:49–53. doi: 10.1016/j.ejogrb.2014.11.002
17. Tournaye H, Sukhikh GT, Kahler E, Griesinger G. A phase III randomized controlled trial comparing the efficacy, safety and tolerability of oral dydrogesterone vs. micronized vaginal progesterone for luteal support in in vitro fertilization. Hum Reproduct. (2017) 32:2152. doi: 10.1093/humrep/dex266
18. Griesinger G, Blockeel C, Sukhikh GT, Patki A, Dhorepatil B, Yang DZ, et al. Oral dydrogesterone vs. intravaginal micronized progesterone gel for luteal phase support in IVF: a randomized clinical trial. Hum Reproduct. (2018) 33:2212–21. doi: 10.1093/humrep/dey306
19. Roque M, Haahr T, Geber S, Esteves SC, Humaidan P. Fresh vs. elective frozen embryo transfer in IVF/ICSI cycles: a systematic review and meta-analysis of reproductive outcomes. Hum Reproduct Update. (2019) 25:2–14. doi: 10.1093/humupd/dmy033
20. Ghobara T, Gelbaya TA, Ayeleke RO. Cycle regimens for frozen-thawed embryo transfer. Cochrane Database Syst Rev. (2017) 7:CD003414. doi: 10.1002/14651858.CD003414.pub3
21. Guo W, Chen X, Ye D, He Y, Li P, Niu J, et al. [Effects of oral dydrogesterone on clinical outcomes of frozen-thawed embryo transfer cycles]. Nan Fang Yi Ke Da Xue Xue Bao. (2013) 33:861–5.
22. Zarei A, Sohail P, Parsanezhad ME, Alborzi S, Samsami A, Azizi M. Comparison of four protocols for luteal phase support in frozen-thawed Embryo transfer cycles: a randomized clinical trial. Arch Gynecol Obstet. (2017) 295:239–46. doi: 10.1007/s00404-016-4217-4
23. Rashidi B, Ghazizadeh M, Tehrani Nejad E, Bagheri M, Gorginzadeh M. Oral dydrogesterone for luteal support in frozen-thawed embryo transfer artificial cycles: a pilot randomized controlled trial. Asian Pacific J Reproduct. (2016) 5:490–4. doi: 10.1016/j.apjr.2016.10.002
24. Alahmad A, Neumann K, Depenbusch M, Schultze-Mosgau A, Osterholz-Zaleski T, Hajek J, et al. Oral dydrogesterone vs. micronized vaginal progesterone for artificial frozen-thawed embryo transfer cycles. Hum Reproduct. (2019) 34:i442.
25. Schindler AE, Campagnoli C, Druckmann R, Huber J, Pasqualini JR, Schweppe KW, et al. Classification and pharmacology of progestins. Maturitas. (2003) 46(Suppl. 1):S7–16. doi: 10.1016/j.maturitas.2003.09.014
26. Griesinger G, Tournaye H, Macklon N, Petraglia F, Arck P, Blockeel C, et al. Dydrogesterone: pharmacological profile and mechanism of action as luteal phase support in assisted reproduction. Reproduct Biomed Online. (2019) 38:249–59. doi: 10.1016/j.rbmo.2018.11.017
27. Stanczyk FZ, Hapgood JP, Winer S, Mishell DR Jr. Progestogens used in postmenopausal hormone therapy: differences in their pharmacological properties, intracellular actions, and clinical effects. Endocr Rev. (2013). 34:171–208. doi: 10.1210/er.2012-1008
Keywords: luteal (phase) support, dydrogesterone, progesterone, endometrium, IVF
Citation: Drakopoulos P, Roelens C, De Vos M, Mackens S, Racca A, Tournaye H and Blockeel C (2021) The Future of Luteal Phase Support in ART and the Role of Dydrogesterone. Front. Reprod. Health 2:618838. doi: 10.3389/frph.2020.618838
Received: 18 October 2020; Accepted: 23 December 2020;
Published: 20 January 2021.
Edited by:
Shevach Friedler, Barzilai Medical Center, IsraelReviewed by:
Maria Costanza Chiti, Cliniques Universitaire Saint-Luc, BelgiumCopyright © 2021 Drakopoulos, Roelens, De Vos, Mackens, Racca, Tournaye and Blockeel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Panagiotis Drakopoulos, cGFuYWdpb3Rpc2RyYWtvcG91bG9zQGhvdG1haWwuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.